systematic approach to abdominal pain dr devinder singh bansi bm dm frcp consultant...
TRANSCRIPT
Systematic Approach to Abdominal Pain
Dr Devinder Singh Bansi BM DM FRCP
Consultant GastroenterologistImperial College Healthcare NHS Trust
What Do They Have? As you go through this
presentation, think about each of these cases: An 18 mo old that suddenly
became inconsoleable from AP while playing
A 20 yo man with 12 hours of diffuse crampy AP that migrated to RLQ that became sharp
78 yo woman with h/o chronic steroid use with sudden sharp AP and a rigid exam

Scale of the ProblemGI symptoms in primary careScale of the ProblemGI symptoms in primary care
7.1-9.6% of all primary consultations are with regard to GI complaints
Gastric pain: 5.0 per 1000/yr Regurgitation: 2.0 Abdominal pain: 6.1 Nausea: 2.9 Diarrhoea: 6.7 Constipation: 8.1
– Thompson WG, Gut 2000: 46: 78-82

Scale of the Problem:Abdominal pain in the general populationScale of the Problem:Abdominal pain in the general population
Community prevalence 15-20% 75% of these abdominal complaints
non-consulting 25% consulting
23.5% stay in primary care
1-2% referred to secondary care

Scale of the Problem:Abdominal pain in general practiceScale of the Problem:Abdominal pain in general practice
578 cases of non-acute abdominal pain presenting to 11 general practices
Follow up 15 months Females predominated in the younger age groups 80% visited GP <3 times during F/U 83% managed entirely in the practices 64% received a prescription Only 20% were additionally investigated in anyway by the GP Hardly any differences in dx between patients who had
complaints less than 1 week or more than 1 week before presenting to their GP
Family Practice Vol 10: 4. 387-400

Scale of the Problem:Prevalence of GI diseaseScale of the Problem:Prevalence of GI disease
Peptic ulcer: 1.9 per 1000/yr Oesophagitis: 2.9 IBD: 1.5 GI cancer: 1.6
Functional dyspepsia: 12 GORD: 5.8 IBS: 10.5
80% of chronic GI disease has a functional background
Thompson WG . Gut 2000: 46: 78-82
Scale of the problem;Acute abdominal painScale of the problem;Acute abdominal pain
Acute abdominal pain is not uncommon.
Approximately 5 admissions to the MRI/day with acute abdominal pain from a population base of 500,000.
1 case per GP per month for an average list size of 2,000.
Acute Abdominal Pain Approximately 6% of ED visits Admission rates vary by
population, up to about 65% in high risk elderly populations
Most common diagnosis is NONSPECIFIC (ie, “I dunno”)
Use H+P, risk factors, and directed studies to arrive at diagnosis
MUST rule out emergency conditions
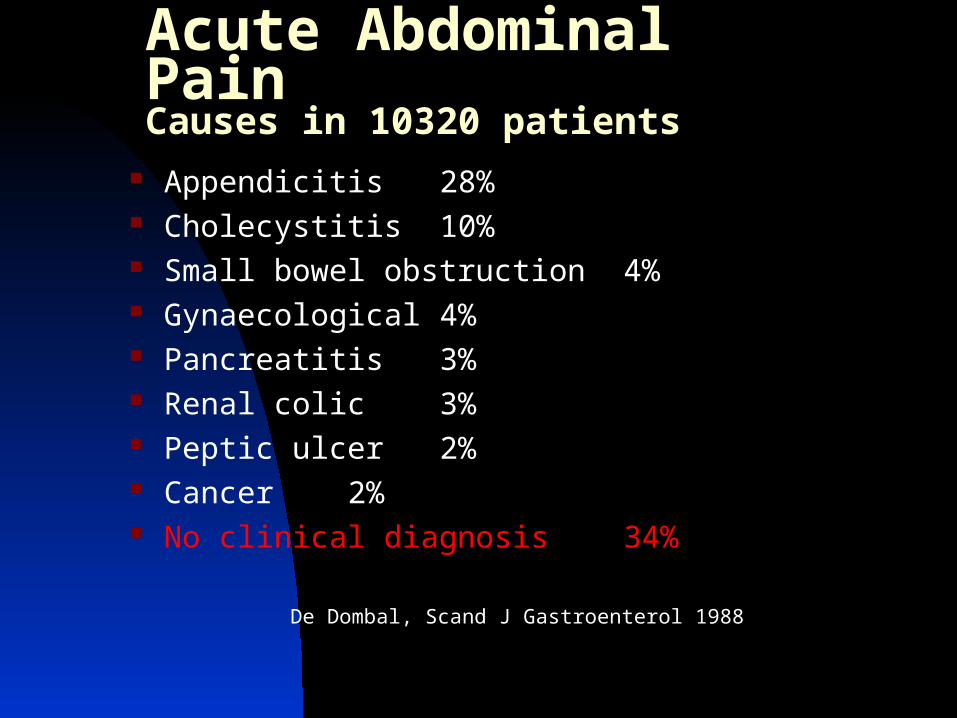
Acute Abdominal PainCauses in 10320 patients
Appendicitis 28% Cholecystitis 10% Small bowel obstruction 4% Gynaecological 4% Pancreatitis 3% Renal colic 3% Peptic ulcer 2% Cancer 2% No clinical diagnosis 34%
De Dombal, Scand J Gastroenterol 1988
Abdominal Pain Across the Ages
Ages 0-2 Colic, GE, viral illness, constipation
Ages 2-12 Functional, appendicitis, GE, toxins
Teens to adults Addition of genitourinary problems
Elderly Beware of what seems like
everything!
Special Populations
Elderly/ nursing home patients
Immunocompromised
Post operative patients
Infants

Abdominal Pain in the Elderly
Diminished sensation of pain in the elderly
Comorbid diseases Polypharmacy Combinations of above result in many
more vague, nonspecific presentations Twice as likely to require surgery with
presentation over age 65 Social factors
Understanding the Types of Abdominal Pain
Visceral Stretch fibers in capsules or walls
of hollow viscus that enter both sides of spinal cord
Somatic Fibers dermatomally distributed
and enter unilaterally in the spinal cord
Referred Overlap of fibers from other
locations
Understanding the Types of Abdominal Pain
Visceral Crampy, achy, diffuse, Poorly localized
Somatic Sharp, lancinating Well localized
Referred Distant from site of generation Symptoms, but no signs

Understanding the Types of Abdominal Pain
Location, location, location Organs and their corresponding
fiber entry to the spinal cord C3-5 – liver, spleen, diaphragm T5-9 – gallbladder, stomach,
pancreas, small intestine T10-11– colon, appendix, pelvic
viscerat11-l1 – sigmoid, renal capsules, ureters, gonads
S2-4 - bladder

History Taking in Abdominal Pain Presentations
“OLD CARS”
O- onset L- location D- duration C- character A-alleviating/aggravating factors
associated symptoms R- radiation S- severity
History Taking for Abdominal Pain Presentations
PMH Similar episodes in past Other medical problems that increase disease
likelihood of problems (ex: DM and gastroparesis)
PSH Adhesions, hernias, tumors
MEDS Abx, NSAIDS, acid blockers, etc
GYN/URO LMP, bleeding, discharge
Social Tob/EtoH/drugs/home situation/agenda
Physical Exam in Abdominal Pain Presentations
General appearance “Sick versus not sick” Mobile versus still Obvious pain or discomfort “Doorway” impression
Vital signs “That’s why they’re called vital”

Physical Exam in Abdominal Pain Presentations
Inspection Distention, scars, bruises
Auscultation Present, hyper, or absent Actually not that helpful!
Palpation Often the most helpful part of exam Tenderness versus pain Start away from painful area first Guarding, rebound, masses

Physical Exam in Abdominal Pain Presentations
Signs Iliopsoas Murphy’s
Extra-abdominal exam Pelvic or scrotal exams Lungs, heart Remember it’s a patient, not a part
Rectal Adds very little (despite the angst) beyond
gross blood or melena
Laboratory Testing
Everybody likes a CBC, but…
Lacks sensitivity, no specificity Little to no change in diagnostic
probabilities Should not dramatically alter
approach (tender is still tender)
Laboratory Testing
Directed approach to lab studies There are no “standard belly labs” Pregnancy test in women of child
bearing age Urine dipsticks

Imaging Plain films
Free air, obstruction, air-fluid, FBs Ultrasound
Rapid “yes or no” ED evaluations Formal studies May add doppler
Computed Tomography Revolutionized acute care Often better than we are!
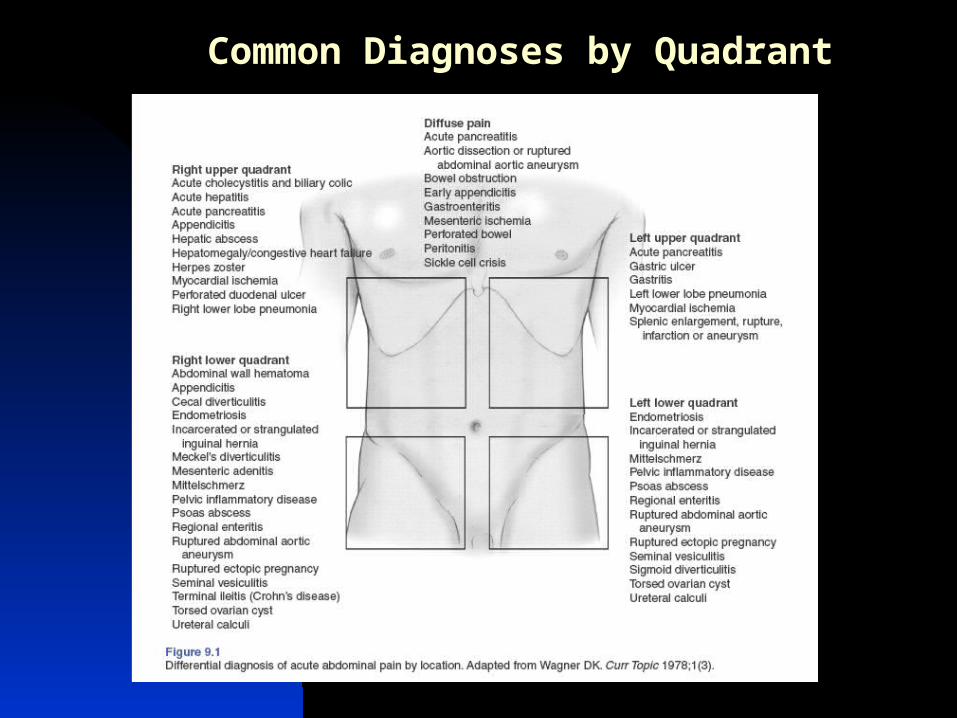
Common Diagnoses by Quadrant

Management of Abdominal Pain
Always right to start with ABC’s IV access Fluid administration Antiemetics Analgesics Directed testing and imaging Re-evaluations Antibiotics Consultants
Surgeons, OB/GYN, urologists, cardiologists, etc
Now How About Those Cases
18 mo old had classic presentation of intussusception, and symptoms may wax and wane; rectal would be to look for current jelly stool. Air enema for diagnosis and reduction. Involve consultants early in the course.
Now How About Those Cases
20 year old with classic presentation of appendicitis, which likely does not need CT scan. Most do not present so simply, quite a wide array of presentations. General surgery consultation, pain meds, IVF, and an operation would all be good, but don’t be shocked if CT requested.
Now How About Those Cases
78 yo has perforated abdomen, with age, multiple problems, and chronic steroids risks for perforation. Rapid resuscitation, plain films to confirm free air, antibiotics, pain medicine, and a surgeon as fast as you can would be good practice.
Pearls, Pitfalls and Myths
Do not restrict the diagnosis solely by the location of the pain.
Consider appendicitis in all patients with abdominal pain and an appendix, especially in patients with the presumed diagnosis of gastroenteritis, PID or UTI.
Do not use the presence or absence of fever to distinguish between surgical and medical causes of abdominal pain.
The WBC count is of little clinical value in the patient with possible appendicitis.
Any woman with childbearing potential and abdominal pain has an ectopic pregnancy until her pregnancy test comes back negative.
Pain medications reduce pain and suffering without compromising diagnostic accuracy.
An elderly patient with abdominal pain has a high likelihood of surgical disease.
Obtain an ECG in elderly patients and those with cardiac risk factors presenting with abdominal pain.
A patient with appendicitis by history and physical examination does not need a CT scan to confirm the diagnosis; they need an operation.
The use of abdominal ultrasound or CT may help evaluate patients over the age of 50 with unexplained abdominal or flank pain for the presence of AAA.

Simplified rules for the diagnosis of acute abdominal pain.
Think in terms of the area of the pain.
Common conditions are common. Disease prevalence changes with
age. Different patterns of disease
between men and women.