sympathetic ophthalmia*
TRANSCRIPT

SYMPATHETIC OPHTHALMIA* FOLLOWING PURULENT ENDOPHTHALMITIS (POSTCATARACT EXTRACTION)
MILTON M. SCHEFFLER, M.D. Chicago, Illinois
CASE REPORT
T. P., a 54-year-old white man, was admitted to the Illinois Eye and Ear Infirmary on January 27, 1949, for a cataract extraction of the left eye. The vision of the left eye had been failing for four years, and pre-operative examination revealed a mature cataract with vision limited to light perception and good projection. The lens of the right eye was clear and corrected vision was 20/30. The laboratory findings were normal, the tear passages were patent, and the con-junctival culture was sterile.
A cataract extraction, left eye, was performed January 29, 1949, utilizing a limbus-based flap, two McLean sutures, and complete iridectomy. During delivery of the lens, the capsule ruptured in the wound lips. The nucleus was expressed and the capsule removed by capsule forceps. The sutures were tied, the anterior chamber was irrigated, and the iris pillars were replaced. Interrupted 4-0 black silk sutures closed the conjunctival flap, and the eye was dressed with atropine sul-fate and sulfacetimide ointment.
For the first two days postoperatively, the course was uneventful. There was a mild striate keratitis. The anterior chamber was well formed. There was a black pupil with no lens material visible, and the iris pillars seemed to be in good position.
On the third postoperative day, a decided change was noted. The bulbar conjunctiva became chemotic. The wound was well closed. Purulent material was present about the corneoscleral sutures with corneal infiltration around the nasal suture. The entire cornea was hazy. A marked aqueous beam with many cell clumps and fibrin, and a three-
* From the Department of Ophthalmology, University of Illinois School of Medicine and the Illinois Eye and Ear Infirmary.
mm. hypopyon was visible in the anterior chamber.
The pupil was dilated to five mm. and no fundus details could be visualized. The impression was that an infection of the anterior segment had occurred along the suture tract. Cultures showed hemolytic Staphylococcus aureus, and sensitivity tests indicated that this organism was sensitive to penicillin and streptomycin.
The patient was given penicillin systemi-cally and subconjunctivally as well as streptomycin locally, in addition to atropine, heat, and foreign protein. On the fourth postoperative day, the patient was given .800 units of streptomycin and 2,500 units of penicillin intravitreally. Penicillin without adrenalin was given subconjunctivally twice daily in the amounts of 250,000 units. This was found to invoke a severe local reaction so that the dosage was reduced to 25,000 units. A total of 750,000 units was given subconjunctivally.
Within a few days purulent exudate filled the area of the coloboma and no red reflex was obtained. The visual acuity was limited to light perception and faulty projection. With continuation of the therapy, the inflammatory process gradually subsided.
On discharge three weeks postoperatively, the left eye revealed a two-plus bulbar reaction, the lower three fourths of the cornea was clear, the iris was atrophic with the pupil bound down and spanned by a gray membrane which also covered the colobom-atous area, no red reflex was visible, tactile tension was soft, and visual acuity was light perception with faulty projection.
The corrected visual acuity of the right eye remained 20/30. Other than the development of a hyphema following discharge, the eye gradually became phthisical, soft and remained tender and slightly injected.
1427
1428 MILTON M. SCHEFFLER
Fig. 1 (Scheffler). High-power view of nodule in skin following uveal pigment sensitivity test. Reaction is similar to that seen in the choroid.
On April 12, 1949, approximately two and one-half months postoperatively, the patient presented himself at the eye clinic of Research and Educational Hospital with the complaints of blurred vision in the right eye of three days' duration. Vision in the right eye was still 20/30, but the globe showed a one-plus bulbar injection, clear cornea, no keratic precipitates, a questionable aqueous ray, fluffy gray Koeppe nodules, and normal fundus. The left eye had not changed except for a marked aqueous beam and cell clumps in the anterior chamber.
The impression was an early sympathetic ophthalmia, and enucleation of the left eye was performed. Therapy for the right eye consisted of aureomycin and salicylates, orally, intravenous typhoid, and atropine locally.
On his discharge, April 18, 1949, there was one-plus ciliary injection, fine keratic precipitates on the lower one third of the cornea, a one-plus aqueous ray with few cell clumps, a few Koeppe nodules on the iris, and no pathologic condition of the fundus.
X-ray studies of the chest revealed some pleural adhesions and the sinuses were
slightly cloudy. There was a two-plus reaction to first strength purified protein derivative. Wassermann reaction and blood agglutinations for brucellosis and tularemia were negative. The uveal pigment skin test was positive, showing an accumulation of lymphocytes and epithelioid cells with pigment phagocytosis (fig. 1). By June 14, 1949, the activity of the right eye had completely subsided, and the final visual acuity remained 20/30.
PATHOLOGIC DESCRIPTION
The enucleated left eye macroscopically measured 18.5 mm. vertically, 20 mm. horizontally, and 22.5 mm. anteroposteriorly. The globe was shrunken with wrinkling of the sclera, especially in the circumcorneal area.
Microscopically, the cornea was quite
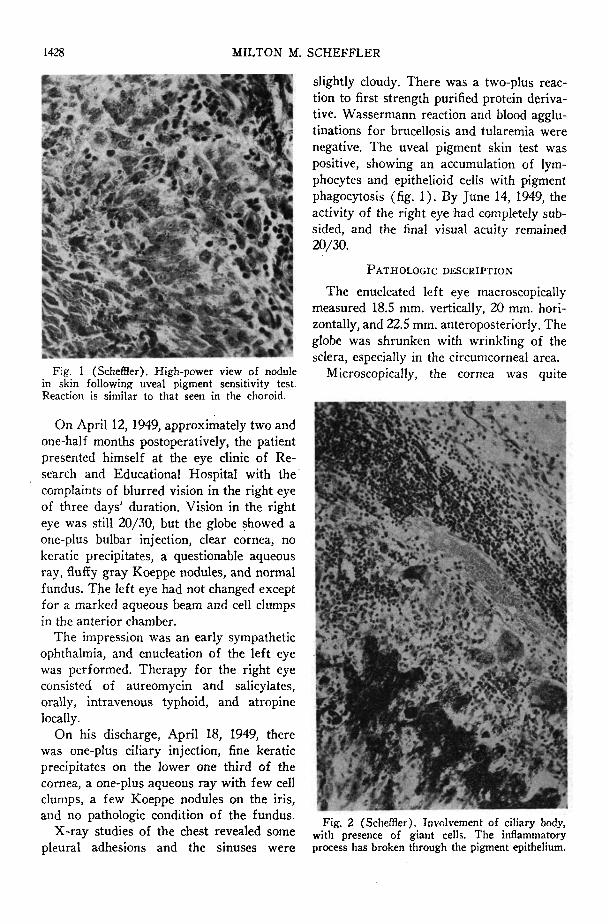
Fig. 2 (Scheffler). Involvement of ciliary body, with presence of giant cells. The inflammatory process has broken through the pigment epithelium.

SYMPATHETIC OPHTHALMIA 1429
scarred and vascularized above, with a healed linear penetrating scar just in front of the angle.
The anterior chamber was filled with an albuminous exudate, lymphocytes, and clumps of monocytes showing pigment phagocytosis. The angles were obliterated by broad peripheral anterior synechias.
The entire uveal tract was diffusely thickened and infiltrated with masses of lymphocytes, showing central zones of epithelioid cells with pigment phagocytosis. The infiltration tended to assume nodular characteristics. Only in the ciliary body was an occasional giant cell seen (fig. 2).
In the iris, the posterior layers were primarily involved, leaving the superficial layers comparatively clear. There was a tendency for the inflammatory process to break through the pigment epithelium (fig. 3). The pupil and the area of the surgical coloboma of the iris were occupied by a newly formed connective-tissue membrane continuous with the tissue filling the angle.
In the ciliary body, the vascular layer was involved. In some areas, the inflammatory cells had broken through and involved the pigment epithelium. The choroid was dif-
Fig. 3 (Scheffler). Thickened iris showing involvement of the posterior layers which in places have broken through the pigment epithelium.
fusely infiltrated in the external layers leaving the choriocapillary zone comparatively clear (figs. 4 and 5).
Some Dalen-Fuchs nodules were present in the pigment epithelium of the retina. A cyclitic membrane was present in the anterior one third of the vitreous cavity containing many new blood vessels and infiltrated with inflammatory cells. The posterior vitreous cavity was filled by an organized inflammatory mass to which the detached retina, folded on itself, was adherent (fig. 6).
Many of the emissaries of the sclera were filled with masses of cells similar to those found in the uveal tract. The superficial vessels in the sclera revealed cuffs of lymphocytes. The optic nerve was atrophic with glial proliferation. No lens material was visualized.
The pathologic diagnosis was sympathetic ophthalmia, secondary to a purulent endoph-thalmitis following a cataract extraction.

1430 MILTON M. SCHEFFLER
Fig. 5 (Scheffler), High-power view of a choroidal nodule. The epithelioid cells show pigment phagocytosis.
COMMENT
It was formerly thought that a purulent infection within the eye destroyed the uveal tract to such an extent that sympathetic uveitis was made unlikely. However, even in phthisical eyes some remnants of uveal tissue remain. Thus, the protection against sympathetic ophthalmia by suppuration in an injured eye, while generally true, is not absolute. When it does occur, it is sufficiently uncommon to warrant its presentation.
Theobold,1 in the laboratory of ophthalmic pathology at the Illinois Eye and Ear Infirmary, has not seen a case of sympathetic ophthalmia following a suppurative process. However, several cases have been reported in the literature.
Trowbridge2 reported three cases of puru-
Fig. 6 (Scheffler). Low-power view of organizing inflammatory mass in vitreous cavity with detached retina adherent to it.
lent infections of the eye followed by sympathetic ophthalmia. One case was similar to that presented here. Samuels3 reported three cases of panophthalmitis in a series of 101 cases of sympathetic ophthalmia. Woods4
has also reported several cases following a suppurative process.
In the case presented here, purulent endophthalmitis following cataract extraction without prolapse of uveal tissue resulted in phthisis bulbi in spite of antibiotic therapy and, two and one-half months later, the development of uveitis in the unoperated eye. Histologic study of the phthisical sympatho-genic eye showed the typical findings of sympathetic ophthalmia, and the uveal pigment skin test was positive.
55 East Washington Street (2).
REFERENCES
1. Theobold, G. D.: Personal communication. 2. Trowbridge. D. H., Jr.: Clinical and pathological factors in sympathetic ophthalmia. Am. J.
Ophth., 20:135, 1937. 3. Samuels, B.: Panophthalmitis and sympathetic ophthalmia. Arch. Ophth., 20:804, 1938. 4. Woods, A. C.: Sympathetic ophthalmia, Am. J. Ophth., 19 :9; 100; 1936.