sympathetic ans connections origin ganglia · (1/24) schlemmer lecture: pharmacology of adrenergic...
TRANSCRIPT

(1/24) Schlemmer Lecture: Pharmacology of Adrenergic Agonists Sympathetic ANS Connections
- Origin: Sympathetic preganglionic fibers originate in the thoracic (T1-T12) lumbar (L1-L5) segments.
- Ganglia: Most of the fibers are arranged as 2 paravertebral ganglia near the spinal column. These ganglia are referred to as the Sympathetic Chain
o Adrenal Gland: Considered a specialized sympathetic ganglion, it receives input from T5-T11.
- Transmission: In both cases, preganglionic input is at nicotinic (nAChR) receptors (NN) modulated by the ACh NT. They vary in their output
o Direct: The Sympathetic chain has directed innervation to its prescribed organs, releasing NE to a and b receptors. This produces immediate action. As an example, innervation of the SA node of the heart, increasing heart rate for a brief period.
o Indirect: The adrenal gland also releases NE, but predominantly E. Its secretions, also referred to as ‘adrenaline,’ enters the circulation and is responsible for the persisting effect of sympathetic stimulation
Adrenergic Nervous System: Receptor Characteristics [a: 1,2 b: 1,2,3] - Endogenously, the a and b adrenergic receptors are acted upon by NE and E catecholamines. Both a and b are G-
protein linked receptors; and depending on their localization, may have opposite mechanistic effects, though they bear the same “fight or flight” goal. As a general example, constriction one place, contraction another, but producing the same physiological effect on blood pressure.
- Alpha1 Receptors (a1): A GPCR-(Gq) postsynaptic receptor found mostly on vascular smooth muscle that, when activated, leads to a stimulatory response mediated by Ca2+. a1 receptors are also frequently found on a variety of effector organs.
o Known For: Stimulatory Constriction at Smooth Muscle o Biomolecular Activity: PLC(+), IP3Ý, Calmodulin(+), Ca2+, Constrict! o Location: Eye, GI tract, Genitalia, Blood Vessels, Liver, Apocrine glands, skin
- Alpha2 Receptors (a2): A GPCR-(Gi) receptor mostly found presynaptically as autoreceptors to elicit negative feedback within the presynaptic cell, shutting down the release of NE. It can also be found postsynaptically.
o Known For: Autoreceptor activity in the brain o Biomolecular Activity: [cAMPß], NE Releaseß o Location: Brain (medulla), platelets, Eye, GI tract, Pancreas (islets), blood vessels, sympathetic terminals
- Beta1 Receptors (b1): A GPCR-(Gs) postsynaptic receptor found mostly in the heart that, when activated, lead to stimulatory heart muscle activity mediated by Ca2+. They are also found in the Kidney.
o Known For: Stimulatory activity in the Heart o Biomolecular Activity: Adenylyl cyclase(+), [cAMPÝ], Ca2+, Contract! o Location: Heart (SA, AV, V-Myocardium), Kidney (Juxtaglomerular cells)
- Beta2 Receptors (b2): A GPCR-(Gs) postsynaptic receptor found on a variety of effector organs, but most notably in bronchial smooth muscle of the lungs. The b2 system is best associated with relaxation of vascular smooth muscle, such as in blood vessels and the lungs.
o Known For: Bronchodilation in the lungs, inhibition of labor, vasodilation for skeletal arterioles o Biomolecular Activity: Adenylyl cyclase(+), [cAMPÝ], Protein Kinase A(+), Relax! o Location: Lungs (Bronchial Muscles), Uterine smooth muscle, Bladder, Arterioles, GI, Liver, Eye,
Muscles, Pancreas - Beta3 Receptors (b3): A GPCR-(Gs) postsynaptic receptor found mainly in Adipose tissue and the urinary bladder.
These are not well characterized and will not be test on. o Known For: Not being tested on. o Location: Adipose tissue (Fat Cells), Bladder (detrusor muscle) - will not be tested on.
Adrenergic Receptor Regulation - If we continue to pour out NE, the receptors will adjust - Desensitization: A decreased response to continuous or repeated exposure to some drug agonists. This process is
also referred to as tolerance and refractoriness. The mechanism is most frequently internalization of receptors - Denervation: Completely different from desensitization, denervation refers to the loss of nerve supply
o Cause: If a motor nerve to an effector organ is cut, the nerve will degenerate resulting in the absence of transmitter binding.
o Denervation Supersensitivity: To compensate, the skeletal muscle or autonomic effector organ will experience a proliferation of receptors, causing it to become extremely sensitive to neurotransmitter.
Adrenoceptors are strong pharmacological targets, especially if there is drug selectivity for the numerous receptor subtypes. The different types of receptors on the same organ can have opposing effects.
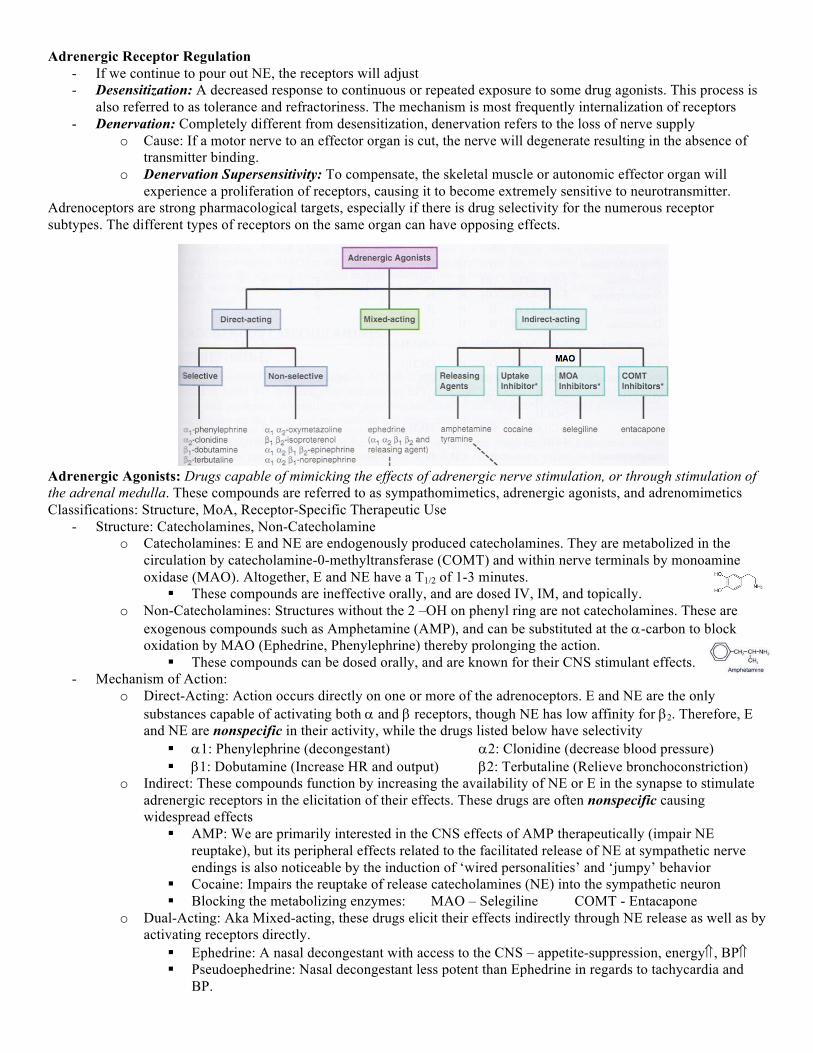
Adrenergic Agonists: Drugs capable of mimicking the effects of adrenergic nerve stimulation, or through stimulation of the adrenal medulla. These compounds are referred to as sympathomimetics, adrenergic agonists, and adrenomimetics Classifications: Structure, MoA, Receptor-Specific Therapeutic Use
- Structure: Catecholamines, Non-Catecholamine o Catecholamines: E and NE are endogenously produced catecholamines. They are metabolized in the
circulation by catecholamine-0-methyltransferase (COMT) and within nerve terminals by monoamine oxidase (MAO). Altogether, E and NE have a T1/2 of 1-3 minutes.
§ These compounds are ineffective orally, and are dosed IV, IM, and topically. o Non-Catecholamines: Structures without the 2 –OH on phenyl ring are not catecholamines. These are
exogenous compounds such as Amphetamine (AMP), and can be substituted at the a-carbon to block oxidation by MAO (Ephedrine, Phenylephrine) thereby prolonging the action.
§ These compounds can be dosed orally, and are known for their CNS stimulant effects. - Mechanism of Action:
o Direct-Acting: Action occurs directly on one or more of the adrenoceptors. E and NE are the only substances capable of activating both a and b receptors, though NE has low affinity for b2. Therefore, E and NE are nonspecific in their activity, while the drugs listed below have selectivity
§ a1: Phenylephrine (decongestant) a2: Clonidine (decrease blood pressure) § b1: Dobutamine (Increase HR and output) b2: Terbutaline (Relieve bronchoconstriction)
o Indirect: These compounds function by increasing the availability of NE or E in the synapse to stimulate adrenergic receptors in the elicitation of their effects. These drugs are often nonspecific causing widespread effects
§ AMP: We are primarily interested in the CNS effects of AMP therapeutically (impair NE reuptake), but its peripheral effects related to the facilitated release of NE at sympathetic nerve endings is also noticeable by the induction of ‘wired personalities’ and ‘jumpy’ behavior
§ Cocaine: Impairs the reuptake of release catecholamines (NE) into the sympathetic neuron § Blocking the metabolizing enzymes: MAO – Selegiline COMT - Entacapone
o Dual-Acting: Aka Mixed-acting, these drugs elicit their effects indirectly through NE release as well as by activating receptors directly.
§ Ephedrine: A nasal decongestant with access to the CNS – appetite-suppression, energyÝ, BPÝ § Pseudoephedrine: Nasal decongestant less potent than Ephedrine in regards to tachycardia and
BP.

- Receptor-Specific Therapeutic Use o a1: Local constriction of arteries and veins
§ Decongestion: Mucous membranes and eyes. § Local Vasoconstriction: This helps dentists who administer local anesthetics. Constricted vessels
will prevent diffusion of the local anesthetics and also help prevent superficial bleeding. § Systemic Vasoconstriction: Help raise or support blood pressure in the ICU, treat sinus
tachycardia by evoke reflex bradycardia § Smooth Muscle Constriction: Treat urinary incontinence by increasing the pressure in the bladder
neck, telling the sphincters to hold onto urine better, causing less leaking, making it so we don’t have to walk around in Depends all day.
• What is causing this? The urge to urinate is from cholinergic stimulation… hmmm § Pupil Dilation: Radial smooth muscle of the iris is stimulated to contract (dilate)
o b2: Lung and Uterine Activity § Manage Acute Asthma Attacks: Can use short-acting b2 agonists (SABA) § Asthma Prophylaxis: Can use long-acting b2 agonists (LABA) in combo with ICS § Uterine-Relaxing Drugs (aka tocolytics): Used to prevent abortion, premature birth.
- Receptor- NON-specific Therapeutic Use o Anaphylactic Shock: Epinephrine (E) – Slam ‘em
§ Dilates bronchiole tubes, constricts blood vessels, reduces capillary permeability Note: This presentation was similar to: https://www.youtube.com/watch?v=KtmV-yMDYPI by Speed Pharmacology
• It is recommended you have coffee before continuing on to Dr. Orjala’s section, shit gets intense •