summary report 1 novembeer 2018 agenda nu mber: 14 title
TRANSCRIPT

SUMMAR
TRUST B
Title of R
AccountaOfficer
Recomm
ConsultaUndertak
RevieweExecutiv
RevieweCommittapplicab
RevieweBoard (wapplicab
Next Ste
Executiv
The purp
A su
RY REPOR
BOARD (IN
Report
able
mendation
ation ken to Date
d by ve Team
d by Boardtee (where le)
d by Trust where
le)
ps
ve Summar
ose of this r
ummary of
RT
PUBLIC)
Risk an
Bernade
The Boa
ReviOctoAssuthe and man
Appr
Noterisks
Note
e Corpora
Circulate
d Quality A
Financeperforma
People &Committ
Trust Bo
Contproviassobeing
To co
IncorMana
To ccommTrust
ry
report is to
the propos
d Assuran
ette George
ard is reco
iew the Bober 2018/1urance Framproposed pwhether the
naged;
rove propos
e the Corpos that have a
e the curren
ate Risk Reg
ed to Execu
Assurance
e Committeeance risks
& Organisatee – workfo
oard
tinue to subides compre
ociated withg effectively
omplete the
rporate theagement St
continue tomittees to pt are manag
provide:
ed principa
1
nce Manage
e, Interim Di
ommended
Board Assu19, and thmework repprincipal risere is suffic
sed revision
orate Risk Ra trust wide
nt position o
gister and P
utive Direct
Committee
e – financia
tional Deveforce risks
bmit the Boehensive as
h the delivey managed.
e RAG ratin
e updated trategy (RM
o submit thprovide assged approp
al risks held
1 Novembe
ement Rep
irector of Int
to:
urance Frae more deport as at Asks are appcient assura
ns to Princip
Register (rise impact sco
of the Risk M
Principal Ris
tors
– quality ris
l and
elopment
oard Assurassurance toery of the
g of the ass
Risk AppMS)
he Corporasurance thariately.
d on the B
er 2018 A
ort
tegrated Go
mework suetailed singAppendix 1 propriately dnce that the
pal risks;
ks currentlyoring 12);
Managemen
sks circulate
sks
ance Frameo the Board
Trust’s str
surances re
petite State
te Risk Reat the most
oard Assur
Agenda Nu
overnance
ummary rele page foand consid
described aey are bein
y scoring 15
nt Improvem
ed for revie
25.10.1
23.10.1
29.10.1
16.10.1
04.10.1
ework to en that the prrategic obje
eceived by t
ement into
egister to significant
rance Fram
1
umber: 14
eport as armat Boardder whetheand scoredg effectively
5 or more o
ment Plan
w.
18
18
18
18
18
nsure that irincipal risksectives, are
the Board
o the Risk
board leverisks to the
mework, and
at d r
d, y
r
it s e
k
el e
d

2
present the detailed single page format of the Board Assurance Framework at Appendix 1;
A summary of the risks held on the Corporate Risk Register;
A position report on the current Risk Management Improvement Plan.
The Board Assurance Framework has been developed in consideration of the strategic objectives and sub aims outlined in the Trust’s 2018/19 Operational Plan that was approved by the Board in May 2018. The Trust’s Operation Plan 2018/19 identified four strategic objectives; Quality, People, Partnerships and Resources and fourteen sub aims associated with these objectives.
The principal risks to delivery of each of the sub aim have been identified and are provided in Appendix 1. Further review of the principal risks has taken place and proposed revisions are contained in this report. Members are asked to approve the proposed revisions.
There are 29 open risks on the Corporate Risk Register and these have been cross-referenced against the Trust’s Strategic Objectives, CQC domains and to the relevant Board Committees. A dashboard view of the Corporate Risk Register is provided in Appendix 2.
Following risk review:
1 existing risk has increased in score (4301);
1 divisional risk has been escalated onto the Corporate Risk register (6443);
1 risk has been closed (6655);
3 risks have reduced in score and been de-escalated from the Corporate Risk Register (Highlighted in grey Appendix 3 and Table 2 – IDs 6827, 6857, 6855).
A summary update on the progress of the Risk Management Improvement Plan is provided in this report and details the next steps to further enhance the revised approach to risk management in the Trust.

3
Risk and Assurance Management Report
1 Introduction / Background
1.1 This report aims to provide members with details of the newly approved principal risks held on the revised Board Assurance Framework (BAF). It also provides a summary of all risks held on the Corporate Risk register (CRR) which comprises risks scoring 15 and above or risks that have a trust wide impact.
1.2 The body of this report contains a detailed view of changes to the CRR, including newly identified, closed, escalated and de-escalated risks. It further provides a breakdown of the number of risks by Director, Strategic Objective, CQC domain and Assuring committee and will note overdue mitigating actions. Corporate Risk Register Risks are reviewed monthly to facilitate the refresh and updates to the register.
1.3 The Corporate Risk Register and Principal risks are provided to the Shaping Our Futures (SOF) Provider Board on a quarterly basis. Risks held by the Trust which impact on the system are included in the System Wide Risk Register along with those held by partner organisations.
1.4 An update is also provided on the progress of the Risk Management Improvement Plan, aimed at strengthening risk management at all levels of the organisation.
Key terms used in this report:
Board Assurance Framework (BAF): Key document which records the principal risks to strategic objectives. The BAF also provides the Board with sources of assurance that controls are working effectively.
Corporate Risk Register (CRR): A register of all operational risks with scores of 15 or more or those deemed to have an organisational wide impact.
Current risk Score: Assessment of risk score using 5x5 risk matrix, taking into account current mitigation
Divisional Risk Register: All risks scoring 1-12.
Principal risk: A risk which threatens achievement of the Trust’s strategic objectives.
Risk scores:
1-3=’Low risk’
4-6=’Moderate risk’
8-12=’High risk’
15-25=’Extreme risk’
Target risk score: The estimated achievable risk score when all actions are completed.

4
2 Principal risks – Board Assurance Framework (BAF)
2.1 The 2018/19 Board Assurance Framework and the principal risks have been developed in consideration of the strategic objectives and sub aims outlined in the Trust’s 2018/19 Operational Plan that was approved by the Board in May 2018.
2.2 The Trust’s Operation Plan 2018/19 identified four strategic objectives; Quality, People, Partnerships and Resources and fourteen sub aims associated with these objectives. The principal risks to delivery of each of the sub aim have been identified and scored, and presented to Board on the 4th October 2018 for approval.
2.3 The current Board Assurance Framework, including detail and rationale for scoring is provided in Appendix 1 Board Assurance Framework Single Page Format Report.
2.4 The Board approved the risks but requested that the Executive Team review the scoring of all the principal risks identified. This review as taken place with Executive Leads and the resultant proposed scores amendments are highlighted in Table 1.
2.5 Members are requested to approve the revised scoring, risk descriptions and rationales for scores for 3 of the Principal as proposed by Executive leads, detailed in Table 1 below.
Table 1
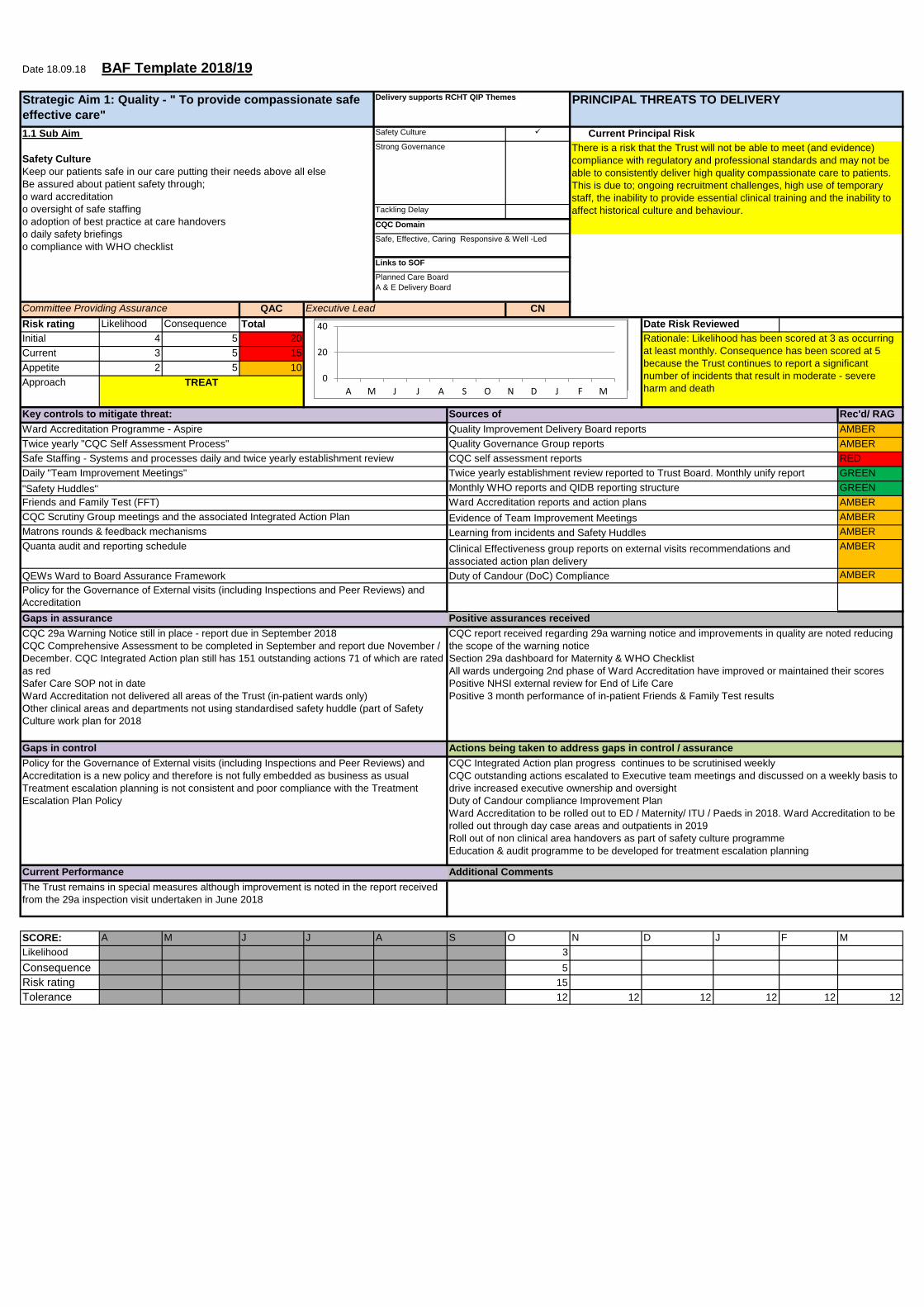
Principal risk Proposed Revision ID 7013 Strategic Aim 1: Quality Sub Aim 1.1 Safety Culture Keep our patients safe in our care putting their needs above all else Be assured about patient safety through; o ward accreditation o oversight of safe staffing o adoption of best practice at care handovers o daily safety briefings o compliance with WHO checklist
Change to Risk Description - There is a risk that the Trust will not be able to meet (and evidence) compliance with regulatory and professional standards and may not be able to consistently deliver high quality compassionate care to patients. This is due to; ongoing recruitment challenges, high use of temporary staff, the inability to provide essential clinical training and the inability to affect historic culture and behaviour. Change to rationale but score remains the same 5(c) x 3(l) = 15 Rationale: Likelihood has been scored at 3 as occurring at least monthly , consequence has been scored at 5 because the Trust continues to report a significant number of incidents that result in moderate - severe harm and death
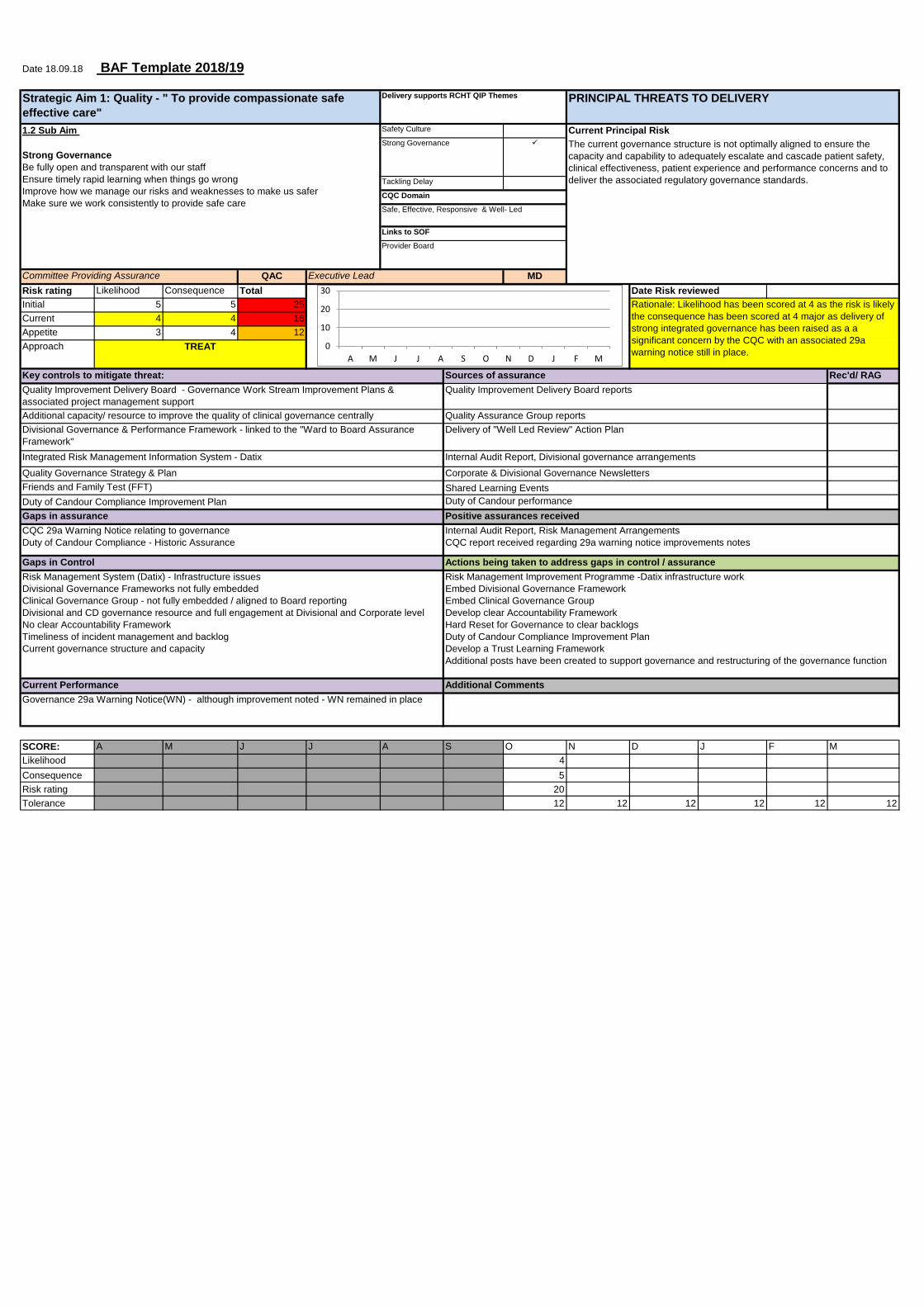
ID 7014 Strategic Aim 1: Quality Sub Aim 1.2 Strong Governance Be fully open and transparent with our staff Ensure timely rapid learning when things go wrong Improve how we manage our risks and weaknesses to make us safer Make sure we work consistently to provide safe care Risk Description The current governance structure is not optimally aligned to ensure the capacity and capability to adequately escalate and cascade
Changes to Rationale & Score – originally scored as a 5(c) x 4 (l) = 20 as the consequence was linked to safety and SIs this has now been tied into the risk above – risk score and rationale for this risk now relate to compliance as per the risk description Revised rationale Likelihood has been scored at 4 as the risk is likely the consequence has been scored at 4 major as delivery of strong integrated governance has been raised as a significant concern by the CQC with an associated 29a warning notice still in place.

5
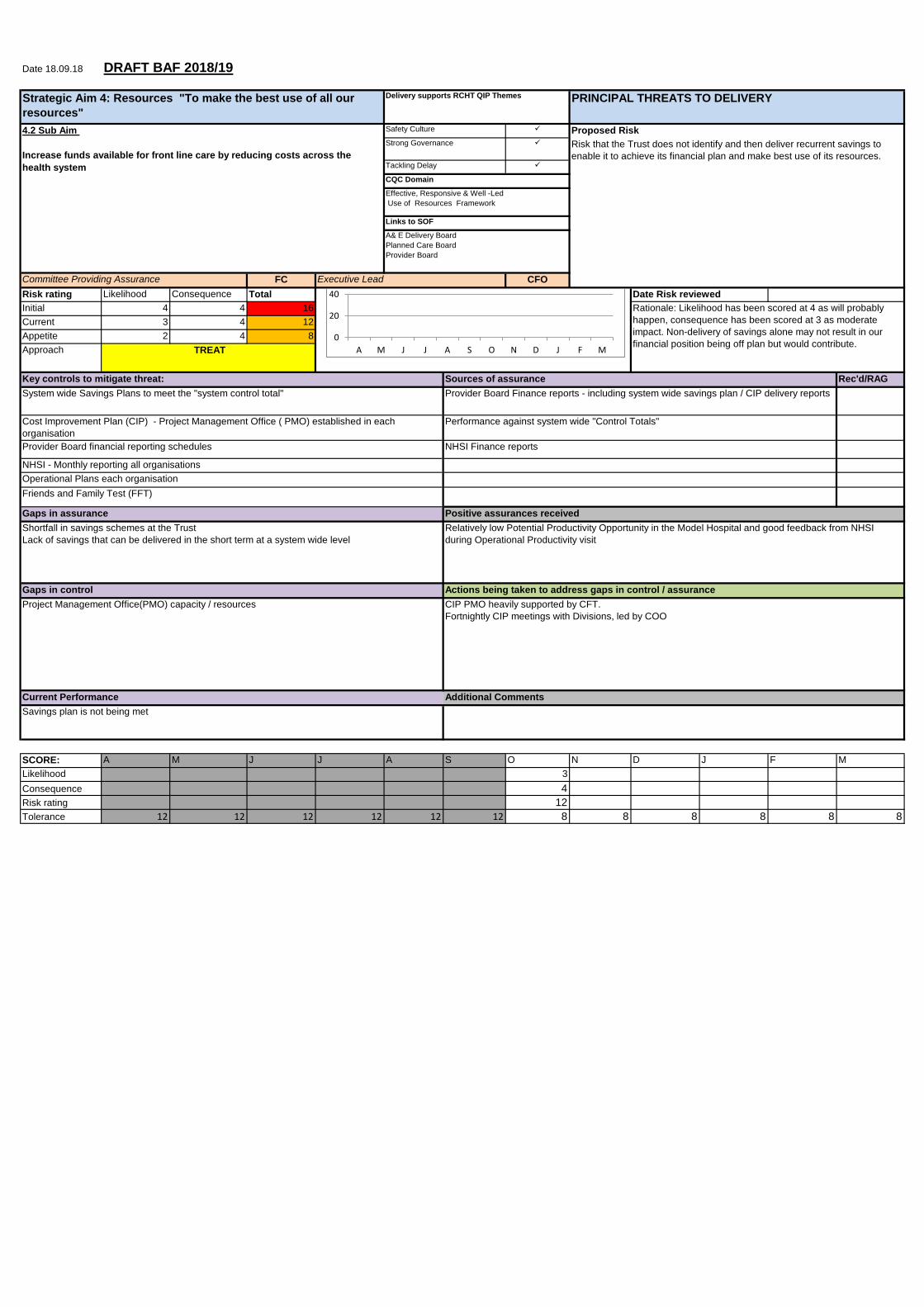
patient safety, clinical effectiveness, patient experience and performance concerns and to deliver the associated regulatory governance standards. ID 6752 Strategic Aim 4: Resources Sub aim 4.4 Ensure investments in technology and facilities improve experience for staff and outcomes for patients Risk Description Risk that the Trust is not able to access or prioritise capital resources to enable it to ensure that service continuity is maintained, statutory regulations are adhered to and services are improved through the use of technology.
Changes to score The risk score has been proposed for increase from 4(c) x 3(l) = 12 to 4(c) x 4 (l) = 16 Rationale as there is no decision on emergency capital bid as at 12 October 2018. £1.5m+ pressure on Mortuary works as well as £0.5m on MRI contingency and £1m on St Michael's Hospital. Partly offset by underspends on Cath Lab and E Notes projects. Risks also remain on medical capital equipment and fire safety. Risk relates to the breach of the Capital Resource Limit.
2.6 In order to align with revised Executive Leads’ portfolios, it is proposed that the Principal risk relating to Strong Governance (Strategic sub-aim 1.2) is assigned to the Chief Nurse.
2.7 The principal risks have been displayed in a ‘heat map’ to provide members with a profile of Principal risks to the delivery of strategic objectives. Each risk is represented by two circles plotted on the 5x5 risk matrix; the blue circle notes the current risk score and the grey represents the target risk score. Arrows show the direction of planned risk reduction.

3 Co
3.1 TmoD
3.2 F
3.3 Thodg3
T
orporate Ris
his report imore or whic
n the TrusDashboard –
ollowing ris
‐ 1 exis
‐ 1 divi‐ 1 risk‐ 3 risk
Regis
he reducedowever resivision and rey. Furtherbelow:
able 3 Sum
sk Registe
ncludes all ch have a Tt Corporate
– October 2
sk review:
sting risk ha
isional risk k has been cks have redster (Highlig
d score risksponsibility
subsequenr details of r
mmary of Ch
r (CRR)
risks held Trust wide ime Risk Reg018).
as increase
has been eclosed (665
duced in scoghted in gre
ks have beefor manag
nt Care Grorisks and ra
hanges to C
on the Cormpact). Forgister (see
d in score (
scalated o55); ore and bee
ey Appendix
en proposedgement of oup. Theseationale for
CRR
porate Riskr context, th
Appendix
(4301);
nto the Cor
en de-escax 3 and Tab
d and agreethese risks
e are noted changes to
k Register (ere are cur3 – Corpo
porate Risk
lated from tble 2 – IDs 6
ed for remos remains w
in Append risk score
(risks scorinrrently 29 risorate Risk R
k register (6
the Corpora6827, 6857,
oval from thwithin the
dix 3, highligare shown
6
ng 15 or sks held Register
6443);
ate Risk , 6855).
he CRR; relevant ghted in in Table

7
Risk Risk Owner/ Executive Lead
Action Taken Date to achieve reduced/ target risk score
4301 – Variability in ED Performance
Toby Slade – CD Urgent and Emergency Care Chief Operating Officer
Increased in Score – Risk Score increased from 16-20 - Crowding increasing and department now experiencing sustained pressure on subsequent days not allowing for recovery. The Team consistently uses the Emergency Department Crowding Standard Operating Procedure (SOP), to maintain patient safety. ED escalation triggers have been developed and four hourly board rounds are being undertaken. 2018/19 Winter Plan currently being tested system wide.
To be reviewed December 2018 following the implementation of the Winter Plan.
6443 – Patient monitoring in the Emergency Department
Owen McCormack – ED Consultant Chief Operating Officer (COO)
Increased in Score- This score was reduced to 12 in August 2018 by the COO as a result of agreement in principal to purchase new monitoring equipment. As this equipment is not yet in place the score has been increased to 15 until the equipment is purchased and installed.
December 2018
6655 Lack of ICU beds
Ken Mccune - Consultant Vascular Surgeon Chief Operating Officer
Risk Closed - at COMCELL it was agreed to amalgamate this risk into the ITU capacity/flow risk 6365 as this would apply to specialties access
6827 - Management of Spinal Patients referred to Therapy services
Vicki Slade – NAHP Service Improvement Medical Director
Reduced in Score – This score was reduced from 15 to 12 – As a network solution to support the management of these patients has been agreed
6587 – Implications of modernising radiotherapy NHS England consultation
Louise Hunt – Cancer Services Manager Director of Strategy & Performance
Reduced in Score – Risk score reduced from 15 to 12 by the Director of Strategy and Performance following discussion with the Risk Owner – on the basis that there is uncertainty on the timescales associated with NHSE’s consultation outcome decision.
6855 – Delayed/failed discharges resulting from sub-standard NEPTS ambulance performance
Nick Masters – Patient Transport Manager Chief Operating Officer
Reduced in Score – Risk reduced from 15 to 10. This risk was added and initially scored at 15. This was challenged whilst the likelihood of the risk occurring remains almost certain (5) as RCHT have limited control on the delivery of the EZEC contract. The consequence/ impact on the Trust is being controlled through the use of the Life star contract limiting the impact to a minor (2) to the Trust of failed discharges.

8
3.4 In order to provide greater visibility of the current mitigation and planned actions in place for the most significant risks, a ‘deep dive’ data extract of all risks scoring 16 or more has been presented at each Board level Committee. The aim of this is to provide greater assurance that management of these risks is appropriate.
3.5 Table 4 below shows the number of risks on the Corporate Risk Register by the Lead Director responsible for the risk:
Table 4 Risks Assigned to Executive Lead
3.6 Table 5 shows the number of risks on the Corporate Risk Register against the Trust Strategic Objective in order to provide clear linkage with the Board Assurance Framework:
Table 5 Risks Linked to Strategic Objective
3.7 Table 6 below shows the number of Corporate Risk Register risks on the by relating primary Assurance Committee responsible for oversight of the risks. Please note,
0
2
4
6
8
10
12
Chief Nurse ChiefOperatingOfficer
Director ofFinance
Director ofHR & OD
MedicalDirector
Corporate Risks Assigned to Executive Lead
Chief Nurse
Chief Operating Officer
Director of Finance
Director of HR & OD
Medical Director
0
5
10
15
20
25
30
Quality: Toprovide
compassionate,safe, effective
care
Resources: Makethe best use of allof our resources
People: Attractdevelop and
retain excellentstaff
Corporate Risks Linked to Strategic Objective
Quality: To providecompassionate, safe, effectivecare
Resources: Make the best useof all of our resources
People: Attract develop andretain excellent staff

9
some risks are presented to multiple Committees to facilitate sharing of risk information where multiple impacts have been identified.
Table 6 Risks by Assuring Committee
3.8 The October Corporate Risk Register dashboard lists 40% (n.12) of risks with no recorded actions and 3.3% (n.1) of risks with overdue actions. In response, the Risk Manager has carried out a targeted review of all risks held on the Corporate Risk register to improve the recording and management of all planned mitigating actions. This project has led to a 100% reduction in the total number of risks with no planned mitigating actions with targeted action plans for all risks held on the Corporate Risk Register.
3.9 Two risks have actions have breached their anticipated completion dates and risk owners are being supported to ensure that actions are completed within expected timescales.
3.10 The Corporate Risk Register and Principal risks are provided to the Shaping Our Futures (SOF) Provider Board on a quarterly basis. Risks held by the Trust which impact on the system are included in the System Wide Risk Register along with those held by partner organisations.
0
5
10
15
20
25
30
FIC POD QAC
Corporate Risks by Primary Assuring Committee
FIC
POD
QAC

10
4 Risk Management Improvement Plan
4.1 Following the findings of two internal audits, the Trust implemented a Risk Management Improvement Plan, aimed at improving both the risk management approach and associated processes within the Trust.
4.2 A range of work streams were identified to address this:
Review risk management strategy and policy and associated documentation with focus on simplifying the approach. The revised Risk Management Strategy was approved by the Board in June 2018. Communication and support to key staff within divisions has taken place;
Strengthening the management of risk at a senior level; an Executive Risk review, dedicated Board risk and assurance session and risk workshop was delivered to the Operational Executive Group. Attendance at the Divisional Governance Boards to present the revised approach to risk;
Cleansing the current risk register and working with divisional and specialty teams to ensure their Risk Registers reflect their wicked issues. Using a ‘top down’ approach, the Corporate Risk Register underwent an intensive cleanse. Following this, risks scoring 12 have been reviewed with risk owners. The implementation of the revised clinical structure will allow Care Groups to have improved visibility of their risks in order to carry out data cleanses in conjunction with the Risk Management Team; monthly Risk Surgeries are planned to increase support and training to further cleanse the Risk Registers ;
Provide “Board to Ward” clear line of sight through alignment of BAF, Corporate Risk Register and Ward Based Risks. All risks held on the Corporate Risk Register and scoring 12 have been aligned to the Trust’s strategic objectives, to provide greater line of sight. Linkage of the remaining risks will take place as part of the data cleanse in conjunction with Care Groups;
Ongoing risk management advice and coaching for key support posts. A forum has taken place with key governance staff in the Trust to strengthen understanding of the revised approach to risk management. Monthly risk surgeries are being scheduled with the interim care group leaders ;
Deliver organisational wide training on the basics of risk management through an accessible rapid roll out programme. A training needs analysis has been carried out to identify requirements for organisation-wide staff training. An integrated governance approach to training is currently under consideration.
5 Recommendations
5.1 The Board is recommended to:
Review the Board Assurance Framework Summary Report as at October 2018/19, and the more detailed single page format Board Assurance Framework report as at Appendix 1 and consider whether the principal risks are appropriately described and scored, and whether there is sufficient assurance that they are being effectively managed;
Approve proposed revisions to Principal risk ;
Note the Corporate Risk Register (risks currently scoring 15 or more or risks that have a
trust wide impact scoring 12);

11
Note the current position of the Risk Management Improvement Plan
Appendix 1 Single Page Format, Board Assurance Framework Appendix 2 Corporate Risk Register Dashboard October 2018 Bernadette George Director of Integrated Governance

14.2_Appendix 1 Corporate Risk Register Dashboard October 2018
Oct-18
Corporate Risks Register and Principal Risks Oversight Dash Board
Lead Director / Division Current Date risk
Identified ≤6 8 9 10 12 15 16 ≥20 # Dates to achieve target risk score Strategic Objectives Primary Assuring Committee CQC Domain
QAC 7013 Quality Strategic Aim 1.1 Safety Culture ‐ Compliance with regulatory standards Chief Nurse 15 Oct‐18 Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Caring, Effective, Responsive,
Safe, Well Led
QAC 7014 Quality Strategic Aim 1.2 Strong Governance ‐ Governance structure is not optimally aligned Medical Director 16 Oct‐18 Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe, Well
Led
QAC 7016 Quality Strategic Aim 1.3 Tackling Delay ‐ Winter period resilience Chief Operating Officer 16 Oct‐18 Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe, Well
Led
POD 7017 People Strategic Aim 2.1 Safety Culture ‐ Lack of a coherent People Strategy Director of HR & OD 16 Oct‐18 People: Attract develop and retain excellent staff People & Organisational
Development Committee
Caring, Effective, Responsive,
Safe, Well Led
POD 7018 People Strategic Aim 2.2 Safety Culture/Strong Governance ‐ Staff engagement Director of HR & OD 12 Oct‐18 People: Attract develop and retain excellent staff People & Organisational
Development Committee
Caring, Effective, Responsive,
Safe, Well Led
POD 7019 People Strategic Aim 2.3 Safety Culture ‐ Develop Leadership cabability Director of HR & OD 12 Oct‐18 People: Attract develop and retain excellent staff People and Organisational
Development Committee
Effective, Responsive, Safe, Well
Led
FIC 7020 Partnership Strategic Aim 3.1 Tackling Delay‐ Insufficient Health and Social Care Provision outside of RCHT Director of Strategy & Performance 16 Oct‐18 Partnership: Offer integrated care as close to
home as possible
Finance Committee Caring, Effective, Responsive,
Safe, Well Led
FIC 7021 Partnership Strategic Aim 3.2 Strong Governance ‐ County Wide Children's Service Planning Director of Strategy & Performance 12 Oct‐18 Partnership: Offer integrated care as close to
home as possible
Finance Committee Caring, Effective, Responsive,
Safe, Well Led
FIC 7022 Partnership Strategic Aim 3.3 Tackling Delay ‐ Organisational Digital Strategy Director of Strategy & Performance 15 Oct‐18 Partnership: Offer integrated care as close to
home as possible
Finance Committee Effective, Responsive, Well Led
FIC 7024 Partnership Strategic Aim 3.4 Safety Culture/Strong Gov ‐ Engagement with research Director of Strategy & Performance 6 Oct‐18 Partnership: Offer integrated care as close to
home as possible
Finance Committee Effective, Responsive, Well Led
FIC 6749 Resources Strategic Aim 4.1 Resources Strong Gov/Safety Culture/Tackling Delay ‐ Achieve Financial Target Director of Finance 20 Oct‐18 Resources: Make the best use of all of our
resources
Finance Committee Effective, Responsive, Well Led
FIC 6751 Resources Strategic Aim 4.2 Safety Culture/Strong Gov/Tackling Delay Identify and Delivery Recurrent Savings Director of Finance 12 Oct‐18 Resources: Make the best use of all of our
resources
Finance Committee Effective, Responsive, Well Led
FIC 7029 Resources Strategic Aim 4.3 Strong Gov/Tackling Delay ‐ Transformational schemes within the health economy Director of Finance 12 Oct‐18 Resources: Make the best use of all of our
resources
Finance Committee Effective, Responsive, Well Led
FIC 6752 Resources Strategic Aim 4.4 Tackling Delay ‐ Risk of not accessing or prioritising capital resources Director of Finance 16 Oct‐18 Resources: Make the best use of all of our
resources
Finance Committee Effective, Responsive, Well Led
QAC 4301 Variability in ED performance Chief Operating Officer 20 Jun‐12 Dec‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe
QAC 1101 Lack of appropriate CAMHS support for young people admitted with mental health issues Chief Nurse 20 May‐15 Sep‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Responsive, Well Led
QAC 6418 Referral to Treatment Performance Chief Operating Officer 20 Aug‐17 Oct‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Responsive
QAC 6487 High Stroke Mortality Rate in comparison to benchmarks Medical Director 16 Oct‐17 Sep‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Responsive, Safe
QAC 3744 Equipment not fit for purpose (ED CT dual slice head scanner) Chief Operating Officer 16 Oct‐11 Mar‐19Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective
QAC 6245 Serious Incident Administration and non compliance with CQC Regulation 12 Medical Director 16 Apr‐17 Jul‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Responsive, Safe, Well Led
QAC 4523 MRI capacity (particularly inpatients) ‐ ageing MRI 1+2 scanners, increased demand Chief Operating Officer 16 Dec‐12 Mar‐19Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe
QAC 4966 High acuity patients will not be able to be treated in a high dependency area due to small resus area Medical Director 16 Sep‐13 Sep‐18Quality: To provide compassionate, safe, effective
care, Resources: Make the best use of all of our
Quality Assurance Committee Effective, Responsive, Safe
QAC 5536 Failure to comply with Duty of Candour regulations as a result of low staff awareness and performance management Medical Director 16 Mar‐15 Dec‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Caring, Responsive, Well Led
FIC 6863 PAS Financial Risk Director of Finance 16 Jul‐18 Sep‐18Resources: Make the best use of all of our
resources
Finance Committee Effective, Responsive, Well Led
FIC 6874 CT scanner and lasers end of life Director of Finance 16 Jul‐18 Oct‐18Quality: To provide compassionate, safe, effective
care, Resources: Make the best use of all of our
Finance Committee Effective, Responsive, Well Led
QAC 6780 Medical Equipment Maintenance (medicine and ED) Medical Director 16 Apr‐18 Sep‐18Quality: To provide compassionate, safe, effective
care, Resources: Make the best use of all of our
Quality Assurance Committee Effective, Responsive, Safe
QAC 6365 Patient Flow ‐ Delayed discharges from Critical Care Chief Operating Officer 16 Jan‐18 Oct‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe
QAC 6849 Lack of flow in MAA due to use of area for inpatient beds Chief Operating Officer 15 Jun‐18 Sep‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Caring, Effective, Responsive,
Safe
FIC 6882 Lack of a Digital Strategy and Roadmap in RCHT Director of Finance 15 Jul‐18 Sep‐18Quality: To provide compassionate, safe, effective
care, Resources: Make the best use of all of our
Finance Committee Effective, Safe, Well Led
QAC 6903 Patients transferred from MAU to oncology assigned to oncologist without being seen Medical Director 15 Jul‐18 Sep‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Caring, Effective, Safe
QAC 6766 Delayed or not sent discharge summaries Medical Director 15 Mar‐18 Dec‐18Quality: To provide compassionate, safe, effective
care, Resources: Make the best use of all of our
Quality Assurance Committee Effective, Responsive, Safe
QAC 6770 Inability to assure whether prospectively booked follow‐up patients are booked within their To Be Seen Date Chief Operating Officer 15 Mar‐18 Dec‐18
Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Safe
POD 5609 Mandatory Training and PDR Compliance Director of HR & OD 15 Jun‐15 Jun‐18Quality: To provide compassionate, safe, effective
care
People and Organisational
Development Committee
Caring, Effective, Safe
QAC 5930 Provision of the cervical cancer screening programme via PHE contract for Cornwall and Plymouth patients Chief Operating Officer 15 Apr‐16 Nov‐18
People: Attract develop and retain excellent staff,
Quality: To provide compassionate, safe, effective
Quality Assurance Committee Effective, Responsive, Safe, Well
Led
QAC 6170 Breaches of complaints timescales Chief Nurse 15 Jan‐18 Aug‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe
QAC 6278 Respiratory outpatient capacity Chief Operating Officer 15 May‐17 Oct‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Responsive, Safe
QAC 6685 N3 Wide Area Network Ceasing to exist Director of Finance 15 Feb‐18 Sep‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Safe
QAC 6691 ED Oceano ‐ missing clinical information from ED & MIU attendance summaries sent to GPs Medical Director 15 Feb‐18 Aug‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe
QAC 6730 Outpatient Clinic Letters delay Chief Operating Officer 15 Mar‐18 Dec‐18Quality: To provide compassionate, safe, effective
care, Resources: Make the best use of all of our
Quality Assurance Committee Effective, Responsive, Safe
QAC 6443 Patient Monitoring in the ED Chief Operating Officer 15 Aug‐17 Dec‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe
QAC 6584 NICE Quality standard 158 ‐ Critically ill patients may not receive adequate rehabilitation physiotherapy Chief Nurse 15 Jan‐18
Due for Review
October 18
Quality: To provide compassionate, safe, effective
care People: Attract develop and retain excellent
Quality Assurance Committee Effective, Responsive, Safe
POD 3093 Improving communication and engagement with staff Director of HR & OD 12 Aug‐10 Due for Review
October 18
People: Attract develop and retain excellent staff, People and Organisational
Development Committee
Caring, Well Led
POD 5821 Culture and leadership Improvement Director of HR & OD 12 Jan‐16
2Due for Review
October 18
People: Attract develop and retain excellent staff, People and Organisational
Development Committee
Caring, Well Led
QAC 6827 Reduced Management of Spinal Patients referred to Therapy servicess Medical Director 12 May‐18 Nov‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe
QAC 6587 Reduced Implications of modernising radiotherapy NHS England consultation Director of Strategy and
Performance
12 Dec‐17 Sep‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Well Led
QAC 6855 Reduced Delayed/failed discharges resulting from sub‐standard NEPTS ambulance performance Chief Operating Officer 10 Mar‐18
Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Well Led
Key Indicates movement in the quarter; Diamond indicates current score; Circle indicates target risk score # Hash symbol column indicates no. of overdue actions Indicates no open actions. Indicates Principal Risk held on BAF Indicates closed risk or reduced score and removed from CRR
Principal Risks
Corporate Risk Register and Principal Risks
Closed Risks
Corporate Risk Register
Page 1 of 2

14.2_Appendix 1 Corporate Risk Register Dashboard October 2018
Oct-18
Corporate Risks Register and Principal Risks Oversight Dash Board
Lead Director / Division Current Date risk
Identified ≤6 8 9 10 12 15 16 ≥20 # Dates to achieve target risk score Strategic Objectives Primary Assuring Committee CQC Domain
Key Indicates movement in the quarter; Diamond indicates current score; Circle indicates target risk score # Hash symbol column indicates no. of overdue actions Indicates no open actions. Indicates Principal Risk held on BAF Indicates closed risk or reduced score and removed from CRR
Corporate Risk Register and Principal Risks
QAC 6655 Closed Lack of ICU beds Chief Operating Officer 16 Dec‐17 Oct‐18Quality: To provide compassionate, safe, effective
care
Quality Assurance Committee Effective, Responsive, Safe
Page 2 of 2
Date 18.09.18 BAF Template 2018/19
QAC CN
Risk rating Likelihood Consequence Total
Initial 4 5 20
Current 3 5 15
Appetite 2 5 10
Approach
Sources of
assurance
Rec'd/ RAG
AMBER
AMBER
RED
GREEN
GREEN
AMBER
AMBER
AMBER
AMBER
AMBER
SCORE: A M J J A S O N D J F M
Likelihood 3
Consequence 5
Risk rating 15
Tolerance 12 12 12 12 12 12
QEWs Ward to Board Assurance Framework
Policy for the Governance of External visits (including Inspections and Peer Reviews) and
Accreditation
Duty of Candour (DoC) Compliance
Gaps in assurance Positive assurances received
CQC Scrutiny Group meetings and the associated Integrated Action Plan
Matrons rounds & feedback mechanisms
Quanta audit and reporting schedule
Evidence of Team Improvement Meetings
Learning from incidents and Safety Huddles
Clinical Effectiveness group reports on external visits recommendations and
associated action plan delivery
Daily "Team Improvement Meetings" Twice yearly establishment review reported to Trust Board. Monthly unify report
"Safety Huddles" Monthly WHO reports and QIDB reporting structure
Friends and Family Test (FFT) Ward Accreditation reports and action plans
Ward Accreditation Programme - Aspire
Twice yearly "CQC Self Assessment Process" Quality Governance Group reports
Safe Staffing - Systems and processes daily and twice yearly establishment review CQC self assessment reports
Quality Improvement Delivery Board reports
Date Risk Reviewed
Rationale: Likelihood has been scored at 3 as occurring
at least monthly. Consequence has been scored at 5
because the Trust continues to report a significant
number of incidents that result in moderate - severe
harm and death TREAT
Key controls to mitigate threat:
Safe, Effective, Caring Responsive & Well -Led
Links to SOF
Planned Care Board
A & E Delivery Board
Committee Providing Assurance Executive Lead
Strategic Aim 1: Quality - " To provide compassionate safe
effective care"
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
1.1 Sub Aim
Safety Culture
Keep our patients safe in our care putting their needs above all else
Be assured about patient safety through;
o ward accreditation
o oversight of safe staffing
o adoption of best practice at care handovers
o daily safety briefings
o compliance with WHO checklist
Safety Culture Current Principal Risk
Strong Governance There is a risk that the Trust will not be able to meet (and evidence)
compliance with regulatory and professional standards and may not be
able to consistently deliver high quality compassionate care to patients.
This is due to; ongoing recruitment challenges, high use of temporary
staff, the inability to provide essential clinical training and the inability to
affect historical culture and behaviour.Tackling Delay
CQC Domain
Current Performance
The Trust remains in special measures although improvement is noted in the report received
from the 29a inspection visit undertaken in June 2018
Additional Comments
CQC 29a Warning Notice still in place - report due in September 2018
CQC Comprehensive Assessment to be completed in September and report due November /
December. CQC Integrated Action plan still has 151 outstanding actions 71 of which are rated
as red
Safer Care SOP not in date
Ward Accreditation not delivered all areas of the Trust (in-patient wards only)
Other clinical areas and departments not using standardised safety huddle (part of Safety
Culture work plan for 2018
CQC report received regarding 29a warning notice and improvements in quality are noted reducing
the scope of the warning notice
Section 29a dashboard for Maternity & WHO Checklist
All wards undergoing 2nd phase of Ward Accreditation have improved or maintained their scores
Positive NHSI external review for End of Life Care
Positive 3 month performance of in-patient Friends & Family Test results
Gaps in control
Policy for the Governance of External visits (including Inspections and Peer Reviews) and
Accreditation is a new policy and therefore is not fully embedded as business as usual
Treatment escalation planning is not consistent and poor compliance with the Treatment
Escalation Plan Policy
Actions being taken to address gaps in control / assurance
CQC Integrated Action plan progress continues to be scrutinised weekly
CQC outstanding actions escalated to Executive team meetings and discussed on a weekly basis to
drive increased executive ownership and oversight
Duty of Candour compliance Improvement Plan
Ward Accreditation to be rolled out to ED / Maternity/ ITU / Paeds in 2018. Ward Accreditation to be
rolled out through day case areas and outpatients in 2019
Roll out of non clinical area handovers as part of safety culture programme
Education & audit programme to be developed for treatment escalation planning
0
0.5
1
A0
20
40
A M J J A S O N D J F M
Date 18.09.18 BAF Template 2018/19
QAC MD
Risk rating Likelihood Consequence Total
Initial 5 5 25
Current 4 4 16
Appetite 3 4 12
Approach
Rec'd/ RAG
SCORE: A M J J A S O N D J F M
Likelihood 4
Consequence 5
Risk rating 20
Tolerance 12 12 12 12 12 12
Internal Audit Report, Risk Management Arrangements
CQC report received regarding 29a warning notice improvements notes
Quality Assurance Group reports
Risk Management System (Datix) - Infrastructure issues
Divisional Governance Frameworks not fully embedded
Clinical Governance Group - not fully embedded / aligned to Board reporting
Divisional and CD governance resource and full engagement at Divisional and Corporate level
No clear Accountability Framework
Timeliness of incident management and backlog
Current governance structure and capacity
Risk Management Improvement Programme -Datix infrastructure work
Embed Divisional Governance Framework
Embed Clinical Governance Group
Develop clear Accountability Framework
Hard Reset for Governance to clear backlogs
Duty of Candour Compliance Improvement Plan
Develop a Trust Learning Framework
Additional posts have been created to support governance and restructuring of the governance function
Gaps in Control Actions being taken to address gaps in control / assurance
Shared Learning Events
Duty of Candour performance
Safe, Effective, Responsive & Well- Led
Integrated Risk Management Information System - Datix
Duty of Candour Compliance Improvement Plan
Quality Improvement Delivery Board reports
Links to SOF
Provider Board
Date Risk reviewed
Key controls to mitigate threat: Sources of assurance
Committee Providing Assurance Executive Lead
Gaps in assurance Positive assurances received
TREAT
Divisional Governance & Performance Framework - linked to the "Ward to Board Assurance
Framework"
Quality Governance Strategy & Plan
Friends and Family Test (FFT)
Delivery of "Well Led Review" Action Plan
Governance 29a Warning Notice(WN) - although improvement noted - WN remained in place
Current Performance Additional Comments
Quality Improvement Delivery Board - Governance Work Stream Improvement Plans &
associated project management support
Rationale: Likelihood has been scored at 4 as the risk is likely
the consequence has been scored at 4 major as delivery of
strong integrated governance has been raised as a a
significant concern by the CQC with an associated 29a
warning notice still in place.
Additional capacity/ resource to improve the quality of clinical governance centrally
Internal Audit Report, Divisional governance arrangements
Corporate & Divisional Governance Newsletters
CQC 29a Warning Notice relating to governance
Duty of Candour Compliance - Historic Assurance
Strategic Aim 1: Quality - " To provide compassionate safe
effective care"
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
1.2 Sub Aim
Strong Governance
Be fully open and transparent with our staff
Ensure timely rapid learning when things go wrong
Improve how we manage our risks and weaknesses to make us safer
Make sure we work consistently to provide safe care
Safety Culture
The current governance structure is not optimally aligned to ensure the
capacity and capability to adequately escalate and cascade patient safety,
clinical effectiveness, patient experience and performance concerns and to
deliver the associated regulatory governance standards.
Strong Governance
Current Principal Risk
Tackling Delay
CQC Domain
0
0.5
1
A0
10
20
30
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
QAC COO
Risk rating Likelihood Consequence Total
Initial 5 4 20
Current 4 4 16
Appetite 3 3 9
Approach
Rec'd/ RAG
SCORE: A M J J A S O N D J F M
Likelihood 4
Consequence 4
Risk rating 20
Tolerance 9 9 9 9 9 9
As at September 2018 IPR; RTT = 80.9% A & E 83.4%,Cancer - Quarterly Standards met
Critical care occupancy levels 99% (124% L3 and 65%L2)
Diagnostic performance 90%
Planned Care Board reports
SDEC KPI Reports
ICNARC reports
Five Steps to Safer Surgery monthly audit reports
Gaps in assurance Positive assurances received
RTT performance
Cancer performance
Critical Care occupancy levels
Diagnostic performance
Winter planning arrangements
CQC report received regarding 29a warning notice and improvements in critical care discharges
noted
Proposed Principal Risks
Rationale: Likelihood has been scored at 4 as the winter
resilience risk is likely Consequence has been scored as
4 major , as a result of quality of care provided and
regulatory compliance impact.
There is risk that the Trust will not be resilient over the winter period, this
will adversely impact on the quality of care delivered and the overall
patient experience leading to cancelled or delayed treatment. Impacting
the Trusts ability to deliver a range of regulatory performance standards
including the A & E 4 hour standard, the cancer, diagnostics & RTT
standards.
Strong Governance
Outpatient Transformation Work is not yet impacting
RTT recovery outsourcing plans are not delivering required volumes
RTT Recovery Plans at specialty level
Cancer Recovery Programme
Critical Care Discharge Improvement Plan
Diagnostic Recovery Plan
SAFER work stream - to expedite discharges
Creating additional community bed capacity & packages of care
Exercise to test Winter Plans
OPD Transformation project is being refreshed to deliver clear KPI's
Harm Review Panel / oversight
Friends and Family Test (FFT)
Same Day Emergency Care Initiative
"Bronze Control" daily to support flow
Actions being taken to address gaps in control / assuranceGaps in control
Critical Care Discharges Improvement Plan
Quality Improvement Delivery Board (QIDB) - Tackling Delays Work stream - Project
resource dedicated to delivery
Safe, Effective , Responsive & Well-Led
Current Performance Additional Comments
Tackling Delay
CQC Domain
Links to SOF
QIDB reports
Referral to Treatment (RTT) & Cancer - Improvement Plan project resource
Integrated Performance Report
Key controls to mitigate threat: Sources of assurance
Outpatient Transformation Work stream- Project resources dedicated to delivery
RTT & Cancer Performance reports
SAFER care bundle project work stream
A& E Delivery Board
Planned Care Board
Committee Providing Assurance Executive Lead
Planned Care Board reports
Ophthalmology and Cardiology Improvement Plans
A& E Delivery Board reports
Strategic Aim 1: Quality - " To provide compassionate safe
effective care"
Delivery supports RCHT QIP Themes
Performance Metrics - Performance Assurance Framework
TREAT
PRINCIPAL THREATS TO DELIVERY
1.3 Sub Aim
Tackling Delays
Achieve the agreed standards for emergency and planned care
Deliver cancer services in line with cancer standards
Deliver an improved outpatient service
Increase the proportion of patients who receive same day emergency care
Safety Culture
Date Risk reviewed
0
0.5
1
A0
20
40
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
P&OD HRD
Risk rating Likelihood Consequence Total
Initial 5 4 20
Current 4 4 16
Appetite 2 4 8
Approach
Rec'd/ RAG
SCORE: A M J J A S O N D J F M
Likelihood 4
Consequence 4
Risk rating 16
Tolerance 8 8 8 8 8 8
As at September 2018 IPR; Mandatory training compliance 82.6%
Appraisal completion 75.4%
Sickness rate 3.87%
Turnover Rate 10.5% (3% Junior Doctor rotation)
Current Performance Additional Comments
Gaps in control
Proposed Risk
Gaps in assurance Positive assurances received
Absence of a fully aligned , comprehensive "People Strategy" that draws together the
HR, OD and Engagement components that are currently sitting in disparate documents
Development of a fully aligned People Strategy
Delivery of the Resourcing Plan
ESR review and data validation exercise
Agency controls need reviewing
Develop enhanced performance monitoring and reporting mechanisms for all HR, OD and
Engagement KPI's
Actions being taken to address gaps in control / assurance
Safe, Effective, Caring, Responsive & Well-
Led
There is a risk that the lack of a coherent aligned "People Strategy" for
the Trust will result in the inability to provide the right people in the right
place at the right time for the right cost'; posing a significant risk to the
Trust's ability to meet its care, financial and performance obligations.
Junior Doctor Contract - exception reporting
Agency Staff usage remains high
Vacancy levels are high
Mandatory training compliance is not being met
ESR data quality and functionality is questionable
Friends and Family Test (FFT)
Staff training records -monthly
Delivery against the Resourcing Plan
Staff training
Junior Doctor - Action Plans to deliver themes from exception reports
Resourcing Plan
Learning & Development Strategy
Finance Committee reportsStaff Health & Wellbeing Strategy
ESR reports
Human Resources Dashboard - monthly
Key controls to mitigate threat: Sources of assurance
Operational Workforce Group reports
Workforce Plan is targeting recruitment to reduce vacancies, developing new roles to
deliver the functions of hard to recruit to posts
Staff Health & Wellbeing Group reports
Operational Work Force Group - Monitors vacancy levels and use of agency staff &
reports to the Finance Committee
People and Organisational Development Committee reports
Committee Providing Assurance Executive Lead
Date Risk reviewed
Rationale: Likelihood has been scored at 3
Consequence has been scored at 5 because there is a
considerable risk of the current recruitment and
resourcing plan not delivering. TREAT
Strategic Aim 2: People - " Attract, develop and retain
excellent staff "
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
2.1 Sub Aim
Ensure we recruit and retain staff, who have the right skills and
experience to provide safe, effective care.
Safety Culture
Strong Governance
Tackling Delay
CQC Domain
Links to SOF
A& E Delivery Board
Planned Care Board
0
0.5
1
A0
20
40
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
P&OD HRD
Risk rating Likelihood Consequence Total
Initial 4 4 16
Current 3 4 12
Appetite 2 4 8
Approach
Rec'd/ RAG
SCORE: A M J J A S O N D J F M
Likelihood 3
Consequence 4
Risk rating 12
Tolerance 8 8 8 8 8 8
As at September 2018 IPR; Mandatory training compliance 82.6%
Appraisal completion 75.4%
Sickness rate 3.87%
Turnover Rate 10.5% ( 3% Junior Doctor rotation)
Gaps in assurance
Proposed Risk
Positive assurances received
Absence of a fully aligned , comprehensive "People Strategy" that draws together the HR, OD
and Engagement components that are currently sitting in disparate documents
Development of a "Recognition Component" to form part of the "People Strategy"
Finalise the "OD & Engagement Component " to form part of the "People Strategy"
Gaps in control Actions being taken to address gaps in control / assurance
Current Performance Additional Comments
Communication & Engagement Strategy & additional senior HR capacity
Outputs from "Improve Well " initiative Friends and Family Test (FFT)
Team Improvement Meeting daily rolled out to all areas
"Improve Well" Application introduced
Staff Survey results
Gaps in communication and engagement
Absence of a "Recognition Component " to form part of the "People Strategy"
An accepted "OD Component " to form part of the "People Strategy"
Gaps in communication and engagement
Delivery of actions arising from Medical Engagement Survey (MES)Freedom to Speak up Guardians & Champions established
Delivery of actions arising from the National and Local Staff SurveysBoard Walkabouts
NHSI Cultural Survey - SCORE results & Action Plan progressExecutive leadership to Improving Working Lives Group
Improving Working Lives Group reports
NHSI Culture Survey - SCORE findings and Action Plans
Committee Providing Assurance Executive Lead
Rationale: Likelihood has been scored at 3 Consequence
has been scored at 4 as staff engagement is a major risk .
TREAT
CQC Domain
Links to SOF
There is a risk that staff do not know about or feel that they are able to
contribute to the continued improvement of the organisation caused by
insufficient communication and engagement of staff in decision making,
linked to the pace of change required. This could adversely affect the
improvements planned to safety, governance, unnecessary delays and the
day to day delivery of high quality and compassionate care.
Medical Engagement Survey (MES) findings and Action plans
Key controls to mitigate threat: Sources of assurance
People and OD Committee reportsWorkforce Plan
Date Risk reviewed
Strategic Aim 2: People - " Attract, develop and retain excellent
staff "
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
2.2 Sub Aim
Create an open, learning environment where all staff feel valued and able to
contribute to our Quality Improvement Plan
Safety Culture
Safe, Effective, Caring, Responsive & Well -
Led
Strong Governance
Tackling Delay
A& E Delivery Board
Planned Care Board
0
0.5
1
A0
20
40
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
P&OD HRD
Risk rating Likelihood Consequence Total
Initial 4 4 16
Current 3 4 12
Appetite 2 4 8
Approach
Rec'd/RAG
SCORE: A M J J A S O N D J F M
Likelihood 3
Consequence 4
Risk rating 12
Tolerance 8 8 8 8 8 8
Recognition that current structures are not working
HR KPI's, financial KPI's and NHS constitutional standards are not being delivered consistently
Current Performance Additional Comments
Absence of a fully aligned , comprehensive "People Strategy" that draws together the HR, OD and
Engagement components that are currently sitting in disparate documents
Finalise the "OD & Engagement Component " to form part of the "People Strategy"
Restructuring of the Divisions to increase leadership capacity and capability. Create a flatter hierarchy to support
leadership cultural development.
Recruit to new roles to further enhance leadership capacity and capability
Gaps in assurance
Gaps in control Actions being taken to address gaps in control / assurance
Positive assurances received
An accepted "OD Component " to form part of the "People Strategy"
Leadership culture
Leadership capability
Delivery of the Lead & FMLM Programmes Ward Accreditation Programme
Leadership training - key management roles - LEAD & FMLM Programmes
New Executive leadership post created to drive culture and leadership capability
Workforce Plan
Well- Led & Use of Resources- delivery of Action PlanWell Led Assessment/ Review
LEAD programme - completed by key staff groups in leadership rolesLearning & Development Strategy
Ward Accreditation reportsBoard Development Programme
Committee Providing Assurance Executive Lead
Rationale: Likelihood has been scored at 3 Consequence has
been scored at 4 because leadership capability is a major risk
hence the restructuring plan.
TOLERATE/ TREAT
Performance against the Workforce PlanFriends and Family Test (FFT)
Key controls to mitigate threat: Sources of assurance
People and OD Committee reports
Strong Governance
Tackling Delay
A& E Delivery Board
Planned Care Board
CQC Domain
Links to SOF
Date Risk reviewed
Strategic Aim 2: People - " Attract, develop and retain excellent
staff "
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
2.3 Sub Aim
Enhance our leadership capability to drive optimal patient care
Safety Culture Proposed Risk
Safe, Effective, Responsive & Well-Led
There is a risk that the Trust does not recruit to and develop the leadership
capability at the pace required to drive & deliver the Quality Improvement Plan &
deliver optimum patient care.
0
0.5
1
A0
20
40
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
TB DS&P
Risk rating Likelihood Consequence Total
Initial 4 4 16
Current 4 4 16
Appetite 2 4 8
Approach
Rec'd/ RAG
RED
AMBER
RED
RED
AMBER
AMBER
AMBER
SCORE: A M J J A S O N D J F M
Likelihood 4
Consequence 4
Risk rating 16
Tolerance 8 8 8 8 8 8
‘Stranded’ (7 day+) and ‘superstranded’ (21day+) and DTOC data (which are effectively a
subset of these). We also have information on patients who are medically fit for discharge
(broader than DTOCs as includes tertiary patients, internal delays etc.).
Current Performance Additional Comments
1. Gold Command initiative has highlighted ability of the system to 'respond' - needs to be sustained.
Accountable Care System Plans
Scope of Sustainable Transformation Plan (STP) has increased - not fully aligned to existing
Programme Board remit.
Gaps in control Actions being taken to address gaps in control / assurance
1. Resetting of Organisational Strategy to clarify what RCHT is here to provide.
Executive Lead
The joint infrastructure is not generating service improvement at this point and the number of
patients inappropriate cared for in the acute environment has not reduced.
SOF Leadership Arrangements - Programme Director
SOF Governance Structures
Integrated Performance Report
"Tackling Delays" Work streams
A & E Delivery Board reports
Gaps in assurance Positive assurances received
Tackling Delays KPI reports
Key controls to mitigate threat:
Frailty Strategy
Committee Providing Assurance
Sources of assurance
Safe, Effective , Caring , Responsive & Well-
Led
Rationale: Likelihood has been scored at 4. Consequence has
been scored at 4 because RCHT continues to accommodate
patients at the Treliske site who would be better cared for at
home or in the community. This can lead to harm and patient
deterioration.TREAT
Planned Care Board reports
Planned Care Board
A & E Delivery Board
Proposed Risk
Links to SOF
QIDB reports
Falls Work stream Falls & frailty KPI performance
Risk that acute primary, community and social care provision outside of the
Treliske environment is insufficient, meaning that patients do not always receive
care and support in the most appropriate therapeutic environment.
Provider Board - Committee in Common Arrangements - RCHT and CFT
Trust Board Assurance reports regarding progression of SOF
Date Risk reviewed
Strategic Aim 3: Partnership " Offer integrated care as close
to home as possible "
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
3.1 Sub Aim
Offer more acute services out of hospital and support locality teams to care for
frail and vulnerable people at home
Safety Culture
Tackling Delay
Strong Governance
CQC Domain
0
0.5
1
A0
20
40
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
TB DS&P
Risk rating Likelihood Consequence Total
Initial 3 4 12
Current 3 4 12
Appetite 2 4 8
Approach
Rec'd/RAG
RED
RED
RED
AMBER
RED
AMBER
SCORE: A M J J A S O N D J F M
Likelihood 3
Consequence 4
Risk rating 12
Tolerance 8 8 8 8 8 8
Gaps in control Actions being taken to address gaps in control / assurance
Current Performance Additional Comments
There is a memorandum of understanding between RCHT, CFT and KCCG to work together to drive
improvement in healthcare pathways which feed into "One Vision" work streams e.g. Neurodevelopmental
pathway . The start of this work is the review mentioned previously
The "One Vision" programme is being led by Kernow Council & alternate delivery models are in
development by the Kernow Council
RCHT Management representative attends and exerts influence through the One Vision -Executive Board
Engagement on healthcare initiatives done via One Vision where appropriate E.g. Handi app promoted at
Royal Cornwall Show as part of "One Vision" engagement
NHS Kernow Clinical Commissioning Group (CCG) has Commissioned a review of children's
services across Cornwall and the Isles of ScillyGaps in assurance Positive assurances received
The joint infrastructure is not generating service improvement at this point
Trust Clinical Lead Identified
Links with One Vision and Local Maternity System Programme Board (LMS)
Provider Board reports
New Developmental Pathways Groups
"One Vision" Partnership Board reports & minutes
CHAMS Partnership Group
"One Vision" Executive Board reports & minutes
"One" Vision Strategy & performance
Integrated Performance Report
Systems Assurance Group reports & minutes
Key controls to mitigate threat: Sources of assurance
"One Vision" Partnership Board - Programme resources - meets quarterly
"One Vision" Executive Board - meets monthly
Action Plan to deliver " Facing the Future" & progress of delivery
One Vision Board
Committee Providing Assurance Executive Lead
TREAT
Strategic Aim 3: Partnership " Offer integrated care as close to
home as possible "
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
3.2 Sub Aim
Implement "One Vision" for children's services
Safety Culture
Safe, Effective, Caring , Responsive & Well-Led
Risk that planning for county-wide children's services takes place without
the considered input of the Trust from the perspective of acute paediatric
care.
Strong Governance
Proposed Risk
Tackling Delay
CQC Domain
Links to SOF
Date Risk reviewed
Rationale: Likelihood has been scored at 3. Consequence
has been scored at 4 as failure to incorporate sufficient
clinical views is a possible risk with regard to the planning of
children's services.
0
0.5
1
A0
20
40
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
TB DS&P
Risk rating Likelihood Consequence Total
Initial 5 3 15
Current 5 3 15
Appetite 4 3 12
Approach
Rec'd/RAG
AMBER
AMBER
AMBER
AMBER
AMBER
AMBER
AMBER
SCORE: A M J J A S O N D J F M
Likelihood 5
Consequence 3
Risk rating 15
Tolerance 12 12 12 12 12 12
Current Performance Additional Comments
Gaps in control
Joint Trust Cybersecurity Group & programme resources Cybersecurity reports
There have been a number of IM&T related serious incidents in 2018 that has extended the
fragility of the current IM&T infrastructure.
Absence of TMG sign off for annual CITS RCHT Programme Plan
Gaps in assurance
Strategy in development for completion by 30 September 2018
More effective connectivity to Annual Plan and contract requirements
New initiatives to be discussed at E Health Programme Board before agreement at TMG
Identify how TMG will sign off annual CITS Programme as part of Annual Plan
Interviewing for CCIO on 1 August 2018
Positive assurances received
Actions being taken to address gaps in control / assurance
CITS Management Board review of annual CITS RCHT Programme Plan
Lack of RCHT Digital Strategy
Ineffective communication of National digital requirements e.g. NHS Standard Contract 2017/19
- Service Conditions - NHS Mail Relay issue / SI
Lack of RCHT Executive oversight and prioritisation of new digital initiatives / 'innovations'
Absence of RCHT TMG sign off for annual CITS Programme Plan
Lack of RCHT Chief Clinical Information Officer (CCIO)
Lack of regular engagement with CDs and Clinical Divisions, nurses and therapies
Sources of assurance
PAS Project Board & project resources PAS Project Board reports
Nerve Centre Project Board & project resources Nerve Centre Project Board reports
Frailty Strategy HSCN Project Board reports + Programme Plan
Rationale: Likelihood has been scored at 5. Consequence
has been scored at 3 because it is established that there is
currently no Trust-wide Digital Strategy and that this
inevitably leads to system disconnects.
Training staff - Accredited 5 day change management methodology programme - 20
August 2018
Executive Lead
Date Risk reviewed
E Health Programme Board & programme resources
E Notes Project Board & project resources
Key controls to mitigate threat:
TREAT
Effective, Responsive &
Well-Led
Falls Work stream
Strong Governance
Tackling Delay
Digital Transformation Board reports + Programme Plan
E Notes Project Board reports
E Health Programme Board reports + CITS Programme Plan
Committee Providing Assurance
PMO - Being established to standardise methodology and reporting documentation Virtual
PMO established - July 2018
Strategic Aim 3: Partnership " Offer integrated care as close
to home as possible "
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
3.3 Sub Aim
Adopt a "Digital First " approach to system wide transformation
Safety Culture Proposed Risk
CQC Domain
Links to SOF
E Health Board Programme Board
Risk that the lack of an organisational Digital Strategy will mean that the
Trust's IM&T infrastructure will be disconnected, sub-standard and not
support excellent clinical care.
0
0.5
1
A
0
5
10
1
0
0.5
1
A0
20
40
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
TB DS&P
Risk rating Likelihood Consequence Total
Initial 2 3 6
Current 2 3 6
Appetite 2 3 6
Approach
Rec'd/ RAG
AMBER
AMBER
AMBER
AMBER
AMBER
AMBER
AMBER
SCORE: A M J J A S O N D J F M
Likelihood 2
Consequence 3
Risk rating 6
Tolerance 6 6 6 6 6 6
Current Performance Additional Comments
Positive assurances received
CRN Regional Benchmark reports
Audit reports of research studies
Gaps in control Actions being taken to address gaps in control / assurance
Research is not fully embedded in all Directorates within the Trust
Research is de-prioritised at times of acute hospital pressure - to utilise Research Nurses for frontline
care
The Research Director and the Research Team continually promote research
The Medical Director is providing senior leadership and engagement to promote research
The Research Team schedule the programme to deliver the required activity across the year
Research Director has included research as a fundamental requirement in all Clinician's Job Descriptions
Proposed Risk
Governance Research Lead - Governance SMT meeting held monthly
Research Team's audit function to monitor status
Gaps in assurance
Dedicated research programmed activity (PA's)/time in Clinician's Job Plans RSMT reports and minutes
National Institute for Health Research's (NIHR) 7 High Level Objectives & the associated Trust Goals
CRN Performance Management Framework
Governance SMT reports and minutes
Research Director and full Research Team to embed research into all Clinical Teams & Directorates
Recruitment to trials is the responsibility of the Principal Investigator of the Research Project - this is
supported through the Research Nurse assigned to the project
Recruitment to clinical trials performance against target
Monthly CRN meeting & performance reports & minutes
Research Team's Business Continuity Plan Performance against NIHR 7 High level Objectives & Trust Goals
Key controls to mitigate threat: Sources of assurance
Research Senior Management Team (RSMT) meetings - weekly
Clinical Research Network ( CRN) meetings - monthly Research Development and Innovation - Annual report
Research Development and Innovation - Annual Business Plan
Committee Providing Assurance Executive Lead
Effective, Responsive & Well-Led
Lack of clinical buy-in/engagement with research will result in patients not having
an opportunity to take part in trails that may enhance their quality of life / wellbeing
now or in the future.
Date Risk reviewed
Rationale: Likelihood has been scored at 2. Consequence has
been scored at 3 because there is currently an acceptable level of
R&D activity within the Trust, although R&D income has reduced in
recent months.TOLERATE
Strategic Aim 3: Partnership " Offer integrated care as close to
home as possible "
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
3.4 Sub Aim
Make services better by encouraging patient involvement in research
Safety Culture
Strong Governance
Tackling Delay
CQC Domain
Links to SOF
Clinical Research Network South West Peninsula (CRN)
Academic Health science Network (AHSN)
0
0.5
1
A0
20
40
A M J J A S O N D J F M

Date 18.09.18 BAF Template 2018/19
FC CFO
Risk rating Likelihood Consequence Total
Initial 5 5 25
Current 4 5 20
Appetite 2 5 10
Approach
Rec'd/ RAG
SCORE: A M J J A S O N D J F M
Likelihood 4
Consequence 5
Risk rating 20
Tolerance 10 10 10 10 10 10
Financial plan not being met at month 4
Current Performance Additional Comments
Gaps in assurance Positive assurances received
Internal audit assessment of design of enhanced financial controls
Relatively low Potential Productivity Opportunity in the Model Hospital and good feedback from NHSI
during Operational Productivity visit
Loan funding approved
Urgent need to invest in services
Tracking and delivery of financial benefits of quality improvement
Changes to regulatory requirements with financial implications
Unavoidable agency spend with urgent service developments.
A fully resourced CIP PMO
Gaps in control Actions being taken to address gaps in control / assurance
Service developments are scrutinised by Executive Directors to confirm need
Review of quality improvement benefits so that they are costed
Recruitment initiatives included overseas recruitment and rebranding
CIP PMO heavily supported by CFT
Effective, responsive & Well-Led
Use of Resources Framework
Proposed Risk
Risk that the Trust does not achieve its financial target which will result in
lost income, additional debt and a longer period of time to recover to a
breakeven position.
Capital spend is monitored through, The Capital Deliver Group a sub group of the Finance
Committee
Benefits realisation of projects not yet tested
Shortfall in savings schemes
Internal audit assessment of existence of enhanced financial controls as being satisfactory
although more assurance required on application
Agency spend has risen significantly year on year even though agency controls remain in place
The Trust submits monthly cash forecasts to NHSI so that the cash need is clear.
Transformational savings opportunities are identified through "Shaping Our Futures" programme
to manage system wide control totals to return the whole health economy to financial balance.
Work force approvals processes are in place to control recruitment of all posts including agency
and locum staff.
The Trust's Workforce Plan is targeting recruitment to reduce vacancies and therefore reduce
the use of / spend against agency and locum staff.
CIP PMO established and regular CIP meeting scheduled to scrutinise and challenge service
level plans and delivery to the plans
Finance reports to the Trust Board
Standing Financial Instructions and Standing Orders including clear financial controls measures. Internal audit reports - re financial controls and processes
Operational Workforce Group - scrutiny of agency expenditure
Annual External Auditors Report - Head of External Audit's Opinion Report on the Trust's
Annual Report and Accounts
Annual Report and Accounts
Friends and Family Test (FFT)
Key controls to mitigate threat: Sources of assurance
Monthly Divisional Performance Review Meetings , including financial performance and Cost
Improvement Plan (CIP) delivery.
Finance Committee(FC) monthly reports - Including management of risks to delivery of
the financial plan, CIP delivery , income, expenditure & capital expenditure
Scheme of Delegation, clear processes for investment requests and business case approval to
ensure scrutiny of benefits prior to approval.
Trusts monthly submission to NHSI - cash forecasts
Committee Providing Assurance Executive Lead
Date Risk reviewed
Rationale: Likelihood has been scored at 4 as at month 4
financial plan was not being met Consequence has been
scored at 5 because of the financial value involved.
TREAT
Strategic Aim 4: Resources "To make the best use of all our
resources"
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
4.1 Sub Aim
Be a financially stable organisation
Safety Culture
Strong Governance
Tackling Delay
CQC Domain
Links to SOF
A& E Delivery Board
Planned Care Board
System - wide Saving Plan
0
20
40
A M J J A S O N D J F M
Date 18.09.18 DRAFT BAF 2018/19
FC CFO
Risk rating Likelihood Consequence Total
Initial 4 4 16
Current 3 4 12
Appetite 2 4 8
Approach
Rec'd/RAG
Gaps in control
SCORE: A M J J A S O N D J F M
Likelihood 3
Consequence 4
Risk rating 12
Tolerance 12 12 12 12 12 12 8 8 8 8 8 8
Savings plan is not being met
Current Performance Additional Comments
Shortfall in savings schemes at the Trust
Lack of savings that can be delivered in the short term at a system wide level
Gaps in assurance Positive assurances received
Relatively low Potential Productivity Opportunity in the Model Hospital and good feedback from NHSI
during Operational Productivity visit
Project Management Office(PMO) capacity / resources
Actions being taken to address gaps in control / assurance
CIP PMO heavily supported by CFT.
Fortnightly CIP meetings with Divisions, led by COO
Proposed Risk
Risk that the Trust does not identify and then deliver recurrent savings to
enable it to achieve its financial plan and make best use of its resources.
Effective, Responsive & Well -Led
Use of Resources Framework
Provider Board financial reporting schedules NHSI Finance reports
Friends and Family Test (FFT)
NHSI - Monthly reporting all organisations
Operational Plans each organisation
Key controls to mitigate threat: Sources of assurance
System wide Savings Plans to meet the "system control total" Provider Board Finance reports - including system wide savings plan / CIP delivery reports
Cost Improvement Plan (CIP) - Project Management Office ( PMO) established in each
organisation
Performance against system wide "Control Totals"
Committee Providing Assurance Executive Lead
Date Risk reviewed
Rationale: Likelihood has been scored at 4 as will probably
happen, consequence has been scored at 3 as moderate
impact. Non-delivery of savings alone may not result in our
financial position being off plan but would contribute. TREAT
Strategic Aim 4: Resources "To make the best use of all our
resources"
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
4.2 Sub Aim
Increase funds available for front line care by reducing costs across the
health system
Safety Culture
Strong Governance
Tackling Delay
CQC Domain
Links to SOF
A& E Delivery Board
Planned Care Board
Provider Board
0
0.5
1
A0
20
40
A M J J A S O N D J F M
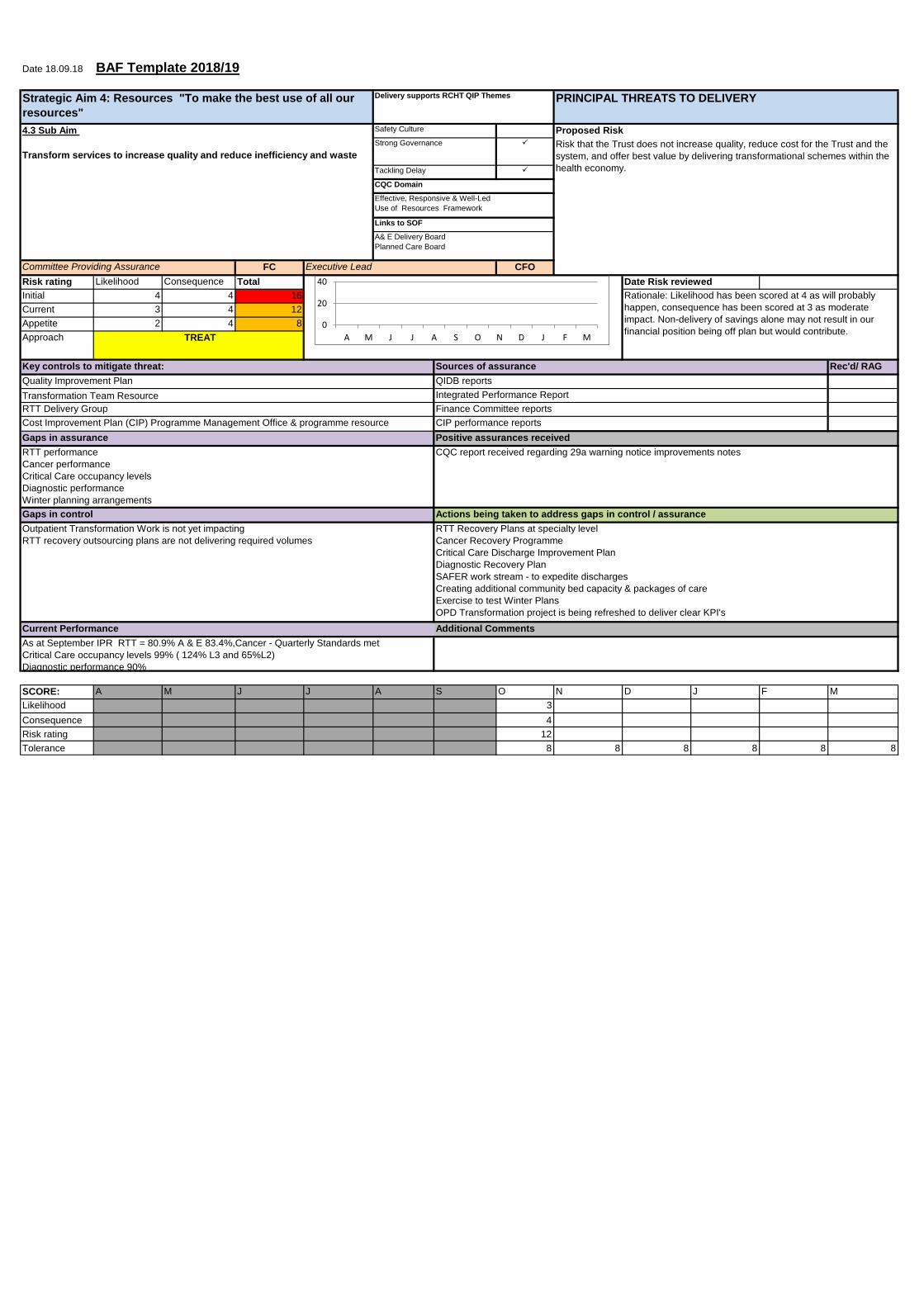
Date 18.09.18 BAF Template 2018/19
FC CFO
Risk rating Likelihood Consequence Total
Initial 4 4 16
Current 3 4 12
Appetite 2 4 8
Approach
Rec'd/ RAG
SCORE: A M J J A S O N D J F M
Likelihood 3
Consequence 4
Risk rating 12
Tolerance 8 8 8 8 8 8
As at September IPR RTT = 80.9% A & E 83.4%,Cancer - Quarterly Standards met
Critical Care occupancy levels 99% ( 124% L3 and 65%L2)
Diagnostic performance 90%
CQC report received regarding 29a warning notice improvements notes
Outpatient Transformation Work is not yet impacting
RTT recovery outsourcing plans are not delivering required volumes
Gaps in control Actions being taken to address gaps in control / assurance
RTT Recovery Plans at specialty level
Cancer Recovery Programme
Critical Care Discharge Improvement Plan
Diagnostic Recovery Plan
SAFER work stream - to expedite discharges
Creating additional community bed capacity & packages of care
Exercise to test Winter Plans
OPD Transformation project is being refreshed to deliver clear KPI's
Current Performance Additional Comments
CIP performance reports
Gaps in assurance
RTT performance
Cancer performance
Critical Care occupancy levels
Diagnostic performance
Winter planning arrangements
Positive assurances received
QIDB reports
RTT Delivery Group
Transformation Team Resource
Cost Improvement Plan (CIP) Programme Management Office & programme resource
Integrated Performance Report
Committee Providing Assurance
Links to SOF
Effective, Responsive & Well-Led
Use of Resources Framework
A& E Delivery Board
Planned Care Board
Rationale: Likelihood has been scored at 4 as will probably
happen, consequence has been scored at 3 as moderate
impact. Non-delivery of savings alone may not result in our
financial position being off plan but would contribute.
Date Risk reviewed
Executive Lead
CQC Domain
Proposed Risk
Risk that the Trust does not increase quality, reduce cost for the Trust and the
system, and offer best value by delivering transformational schemes within the
health economy.
Strong Governance
Tackling Delay
Key controls to mitigate threat: Sources of assurance
Quality Improvement Plan
TREAT
Finance Committee reports
Strategic Aim 4: Resources "To make the best use of all our
resources"
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
4.3 Sub Aim
Transform services to increase quality and reduce inefficiency and waste
Safety Culture
0
0.5
1
A0
20
40
A M J J A S O N D J F M
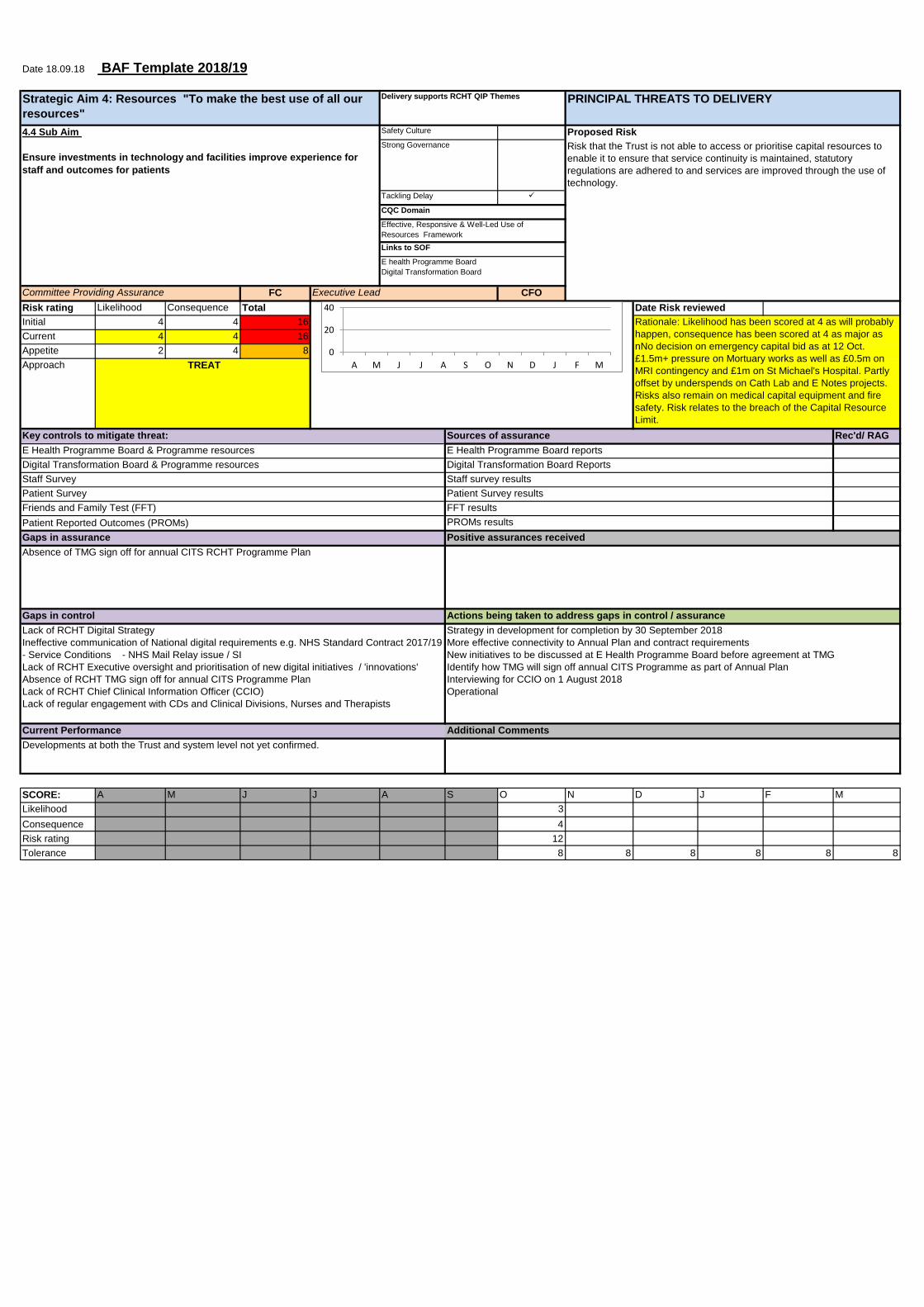
Date 18.09.18 BAF Template 2018/19
FC CFO
Risk rating Likelihood Consequence Total
Initial 4 4 16
Current 4 4 16
Appetite 2 4 8
Approach
Rec'd/ RAG
SCORE: A M J J A S O N D J F M
Likelihood 3
Consequence 4
Risk rating 12
Tolerance 8 8 8 8 8 8
Developments at both the Trust and system level not yet confirmed.
Current Performance Additional Comments
Gaps in assurance
Absence of TMG sign off for annual CITS RCHT Programme Plan
Positive assurances received
Lack of RCHT Digital Strategy
Ineffective communication of National digital requirements e.g. NHS Standard Contract 2017/19
- Service Conditions - NHS Mail Relay issue / SI
Lack of RCHT Executive oversight and prioritisation of new digital initiatives / 'innovations'
Absence of RCHT TMG sign off for annual CITS Programme Plan
Lack of RCHT Chief Clinical Information Officer (CCIO)
Lack of regular engagement with CDs and Clinical Divisions, Nurses and Therapists
Gaps in control Actions being taken to address gaps in control / assurance
Strategy in development for completion by 30 September 2018
More effective connectivity to Annual Plan and contract requirements
New initiatives to be discussed at E Health Programme Board before agreement at TMG
Identify how TMG will sign off annual CITS Programme as part of Annual Plan
Interviewing for CCIO on 1 August 2018
Operational
E Health Programme Board & Programme resources E Health Programme Board reports
Patient Survey results
Friends and Family Test (FFT) FFT results
Patient Survey
PROMs results Patient Reported Outcomes (PROMs)
Strong Governance
Tackling Delay
Digital Transformation Board Reports
Staff Survey Staff survey results
Digital Transformation Board & Programme resources
Links to SOF
Rationale: Likelihood has been scored at 4 as will probably
happen, consequence has been scored at 4 as major as
nNo decision on emergency capital bid as at 12 Oct.
£1.5m+ pressure on Mortuary works as well as £0.5m on
MRI contingency and £1m on St Michael's Hospital. Partly
offset by underspends on Cath Lab and E Notes projects.
Risks also remain on medical capital equipment and fire
safety. Risk relates to the breach of the Capital Resource
Limit.
Effective, Responsive & Well-Led Use of
Resources Framework
Key controls to mitigate threat: Sources of assurance
E health Programme Board
Digital Transformation Board
TREAT
Date Risk reviewed
Executive Lead
Strategic Aim 4: Resources "To make the best use of all our
resources"
Delivery supports RCHT QIP Themes PRINCIPAL THREATS TO DELIVERY
4.4 Sub Aim
Ensure investments in technology and facilities improve experience for
staff and outcomes for patients
Safety Culture
Committee Providing Assurance
Risk that the Trust is not able to access or prioritise capital resources to
enable it to ensure that service continuity is maintained, statutory
regulations are adhered to and services are improved through the use of
technology.
Proposed Risk
CQC Domain
0
0.5
1
A0
20
40
A M J J A S O N D J F M