stroke mdg icp south - hsc knowledge exchange bab-carey... · icp south – stroke tia clinic...
TRANSCRIPT

Barbara Carey
Stroke MDG – ICP South

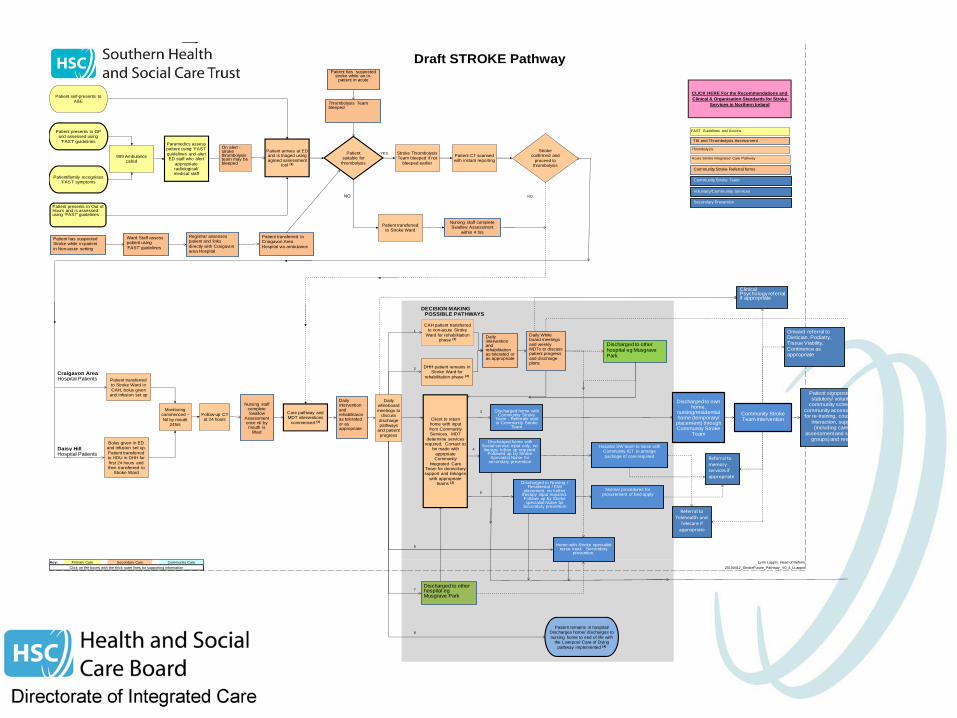
Integrated stroke service pathway
ICP-South

Total Patient Journey
YES YES
YES
NO NO
DECISION MAKING POSSIBLE PATHWAYS
1
2
Craigavon AreaHospital Patients
3
??
Daisy Hill 4
Hospital Patients
5
6
Key: Lynn Lappin, Head of Reform
20100412_StrokeFuture_Pathway_V0_4_LLappin
7
8
Click on the boxes with the thick outer lines for supporting information
Draft STROKE Pathway
CLICK HERE For the Recommendations and
Clinical & Organisation Standards for Stroke
Services in Northern Ireland
Primary Care Secondary Care Community Care
Patient presents to GP and assessed using
'FAST' guidelines
Patient/family recognises 'FAST' symptoms
999 Ambulance called
Paramedics assess patient using 'FAST'
guidelines and alert ED staff who alert
appropriate radiological/medical staff
Patient arrives at ED and is triaged using agreed assessment
tool (1)
Patient suitable for
thrombolysis
Stroke Thrombolysis Team bleeped if not
bleeped earlier
Patient CT scanned with instant reporting
Stroke confirmed and
proceed to thrombolysis
Monitoring commenced -
Nil by mouth 24hrs
Follow-up CT at 24 hours
Daily whiteboard
meetings to discuss
discharge pathways
and patient
progress
Client to return home with input
from Community Services. MDT
determine services required, Contact to
be made with
apprpriate Community
Integrated Care Team for domiciliary support and linkages
with appropriate teams (2)
CAH patient transferred to non-acute Stroke
Ward for rehabilitation phase (2)
Patient transferred to Stroke Ward in
CAH, bolus given and infusion set up
Bolus given in ED and infusion set up.
Patient transferred to HDU in DHH for
first 24 hours and then transferred to
Stroke Ward
DHH patient remains in Stroke Ward for
rehabilitation phase (2)
Patient transferred to Stroke Ward
Care pathway and MDT interventions
commenced (3)
Patient remains in hospital/Discharges home/ discharges to
nursing home to end of life with the Liverpool Care of Dying
pathway implemented (4)
Patient self-presents to A&E
FAST Guidelines and Actions
Thrombolysis
Acute Stroke Integrated Care Pathway
Patient presents to Out of Hours and is assessed using 'FAST' guidelines
Discharged to own home,
nursing/residentialhome (temporary/
placement) through Community Stroke
Team
Community Stroke Team intervention
Patient signposted to statutory/ voluntary/
community schemes/ community access officer for re-training, couselling,
interaction, support (including carer's
assessment and support groups) and respite
Discharged to other hospital eg Musgrave Park
TIA and Thrombolysis Assessment
Community Stroke Referral forms
Community Stroke Team
Voluntary/Community Services
Secondary Prevention
On alert -stroke thrombolysis team may be bleeped
Nursing staff complete Swallow Assessment
within 4 hrs
Nursing staff complete Swallow
Assessment once nil bymouth is
lifted
Daily intervention and rehabilitaion as tolerated or as appropriate
Referral to Telehealth and
Telecare if appropriate
Patient has suspected stroke while an in-
patient in acute
Referral to memoryservices if appropriate
Clinical Psychology referral if appropriate
Discharged home with Community Stroke
Team - Referrals sent to Community Stroke
Team
Home with Stroke specialist nurse input. Secondary
prevention.
Daily interventionand rehabilitation as tolerated or as appropriate
Daily White board meetings and weekly MDTs to discuss patient progress and discharge plans
Discharged home with Social service input only, no therapy follow up required.
Followed up by Stroke Specialist Nurse for
secondary prevention
Hospital SW team to liaise with Community ICT to arrange
package of care required
Discharged to Nursing /Residential / EMI
placement, no further therapy input required. Followe up by Storke specialist Nurse for
Secondary prevention
Normal procedures for procurement of bed apply
Onward referral to Dietician, Podiatry, Tissue Viability, Continence as appropriate
Discharged to other hospital eg Musgrave Park
Patient has suspected Stroke while in-patient
in Non-acute setting
Ward Staff assess patient using
'FAST' guidelines
Thrombolysis Team bleeped
Registrar assesses patient and links
directly with Craigavon area Hospital
Patient transferred to Criagavon Area
Hospital via ambulance
http://thelrc.files.wordpress.com/2013/02/mind_the_gap_logo_by_rrward1.png
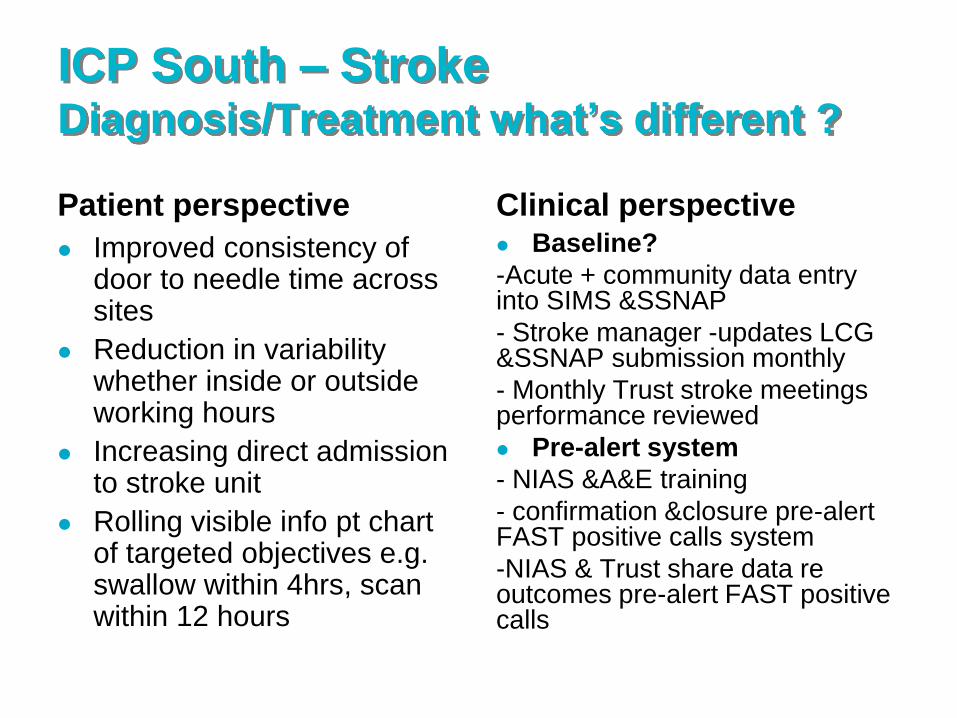
ICP South – Stroke Diagnosis/Treatment what’s different ?
Patient perspective
Improved consistency of door to needle time across sites
Reduction in variability whether inside or outside working hours
Increasing direct admission to stroke unit
Rolling visible info pt chart of targeted objectives e.g. swallow within 4hrs, scan within 12 hours
Clinical perspective Baseline?
-Acute + community data entry into SIMS &SSNAP
- Stroke manager -updates LCG &SSNAP submission monthly
- Monthly Trust stroke meetings performance reviewed
Pre-alert system
- NIAS &A&E training
- confirmation &closure pre-alert FAST positive calls system
-NIAS & Trust share data re outcomes pre-alert FAST positive calls
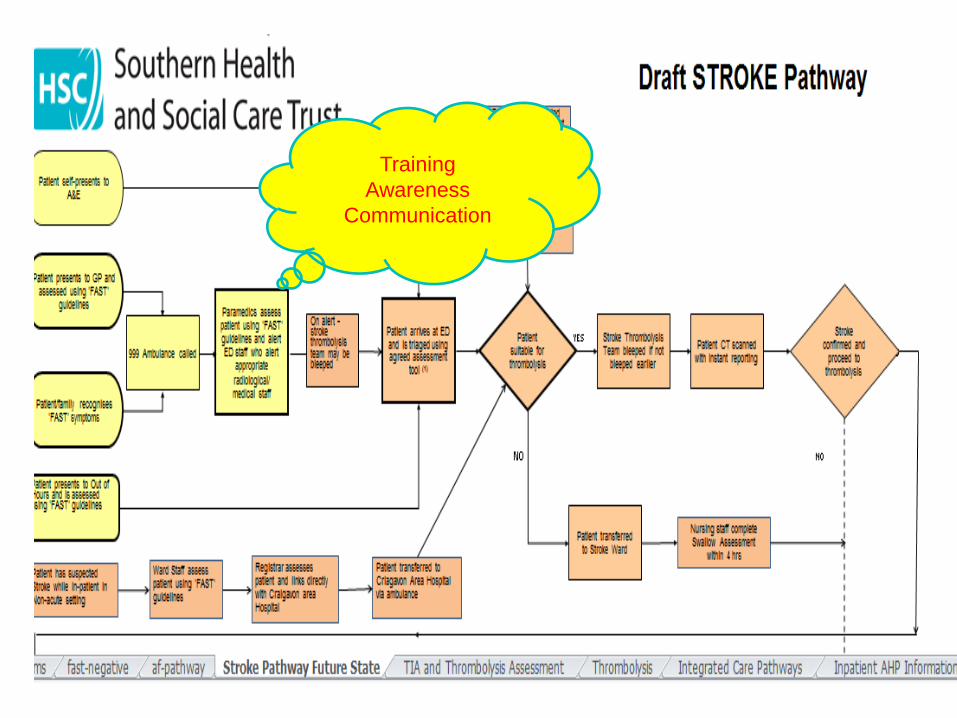
Training
Awareness
Communication
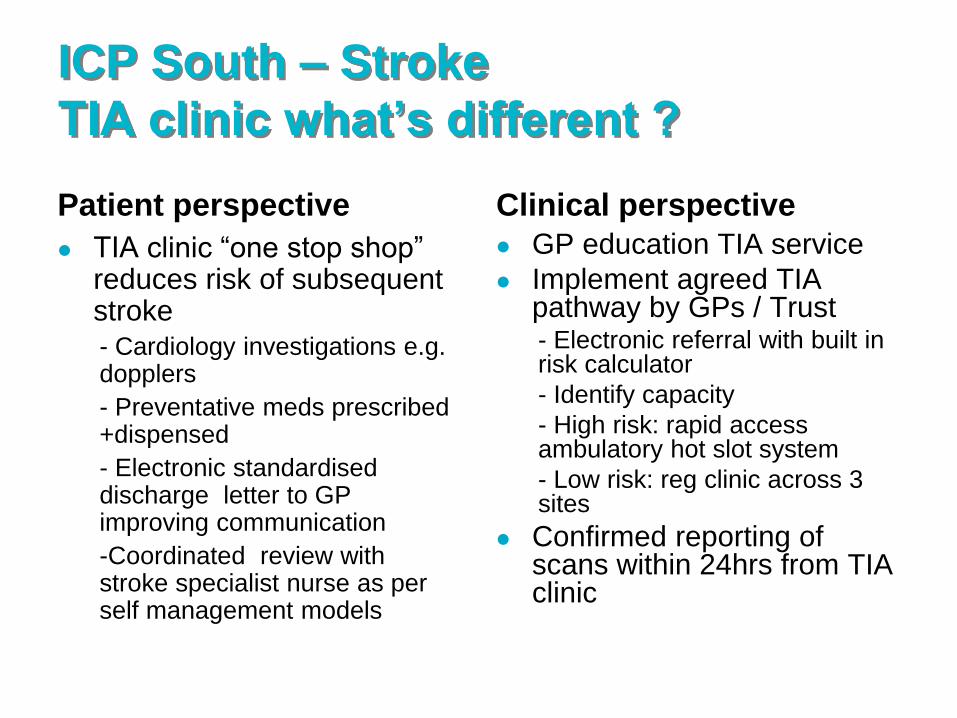
ICP South – Stroke
TIA clinic what’s different ?
Patient perspective
TIA clinic “one stop shop” reduces risk of subsequent stroke
- Cardiology investigations e.g. dopplers
- Preventative meds prescribed +dispensed
- Electronic standardised discharge letter to GP improving communication
-Coordinated review with stroke specialist nurse as per self management models
Clinical perspective
GP education TIA service
Implement agreed TIA pathway by GPs / Trust - Electronic referral with built in risk calculator
- Identify capacity
- High risk: rapid access ambulatory hot slot system
- Low risk: reg clinic across 3 sites
Confirmed reporting of scans within 24hrs from TIA clinic

ICP South – Stroke
Discharge What’s different ?
Patient perspective
Access for all patients to a fully
resourced ESD team
-6/7 day rehab available
-Access to resident psychologist
-Improved services for young working
stroke patients
Named contact of specialist
stroke team for any issues
after discharge
Patient education: info leaflet
with CVS signposting to
include self management
Patient survey to monitor
Clinical perspective
Clarity re ESD alternative community stroke team model
Stroke manager to coordinate ESD team +performance - Traverse historical
boundaries
- In reach / Outreach capabilities
- Vocational rehab pathway
- Smoking cessation referral
- Standardisation of review and data entry
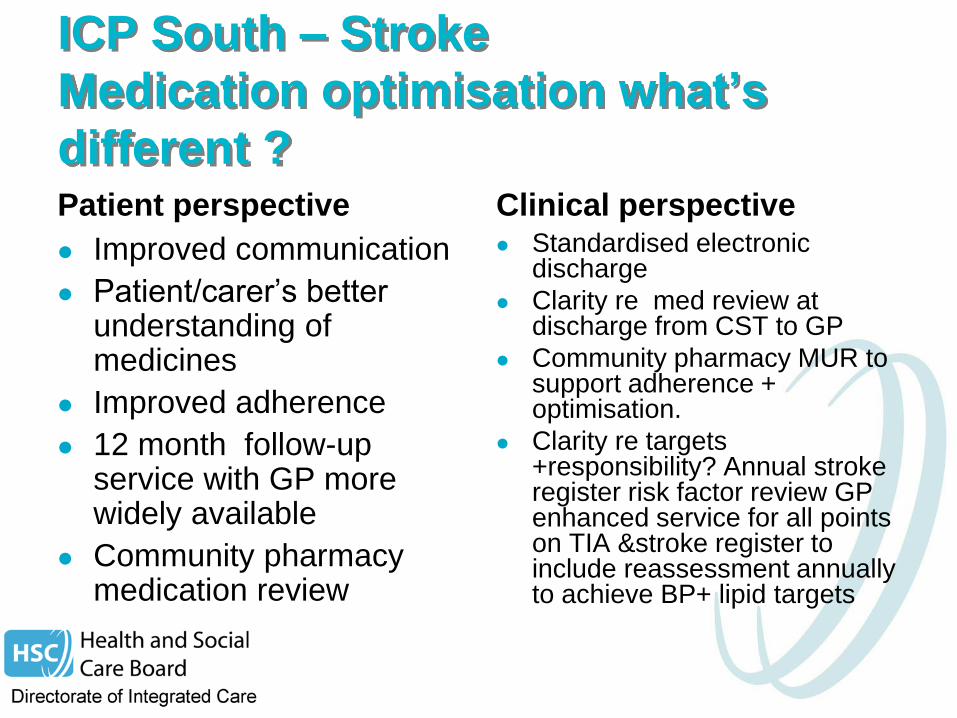
ICP South – Stroke
Medication optimisation what’s
different ? Patient perspective
Improved communication
Patient/carer’s better understanding of medicines
Improved adherence
12 month follow-up service with GP more widely available
Community pharmacy medication review
Clinical perspective Standardised electronic
discharge
Clarity re med review at discharge from CST to GP
Community pharmacy MUR to support adherence + optimisation.
Clarity re targets +responsibility? Annual stroke register risk factor review GP enhanced service for all points on TIA &stroke register to include reassessment annually to achieve BP+ lipid targets
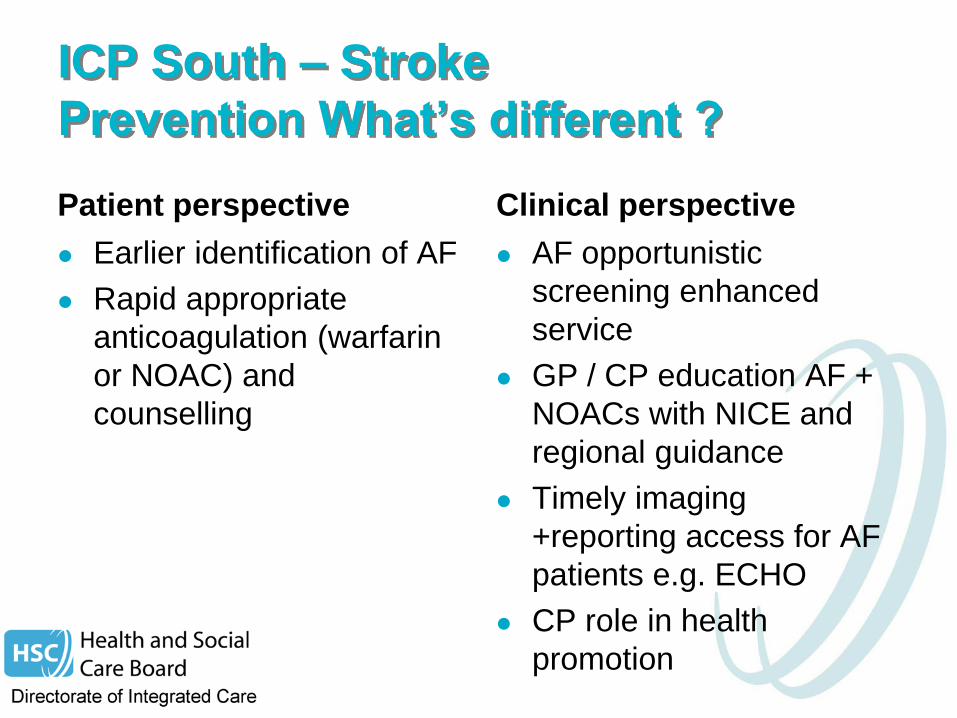
ICP South – Stroke
Prevention What’s different ?
Patient perspective
Earlier identification of AF
Rapid appropriate
anticoagulation (warfarin
or NOAC) and
counselling
Clinical perspective
AF opportunistic
screening enhanced
service
GP / CP education AF +
NOACs with NICE and
regional guidance
Timely imaging
+reporting access for AF
patients e.g. ECHO
CP role in health
promotion
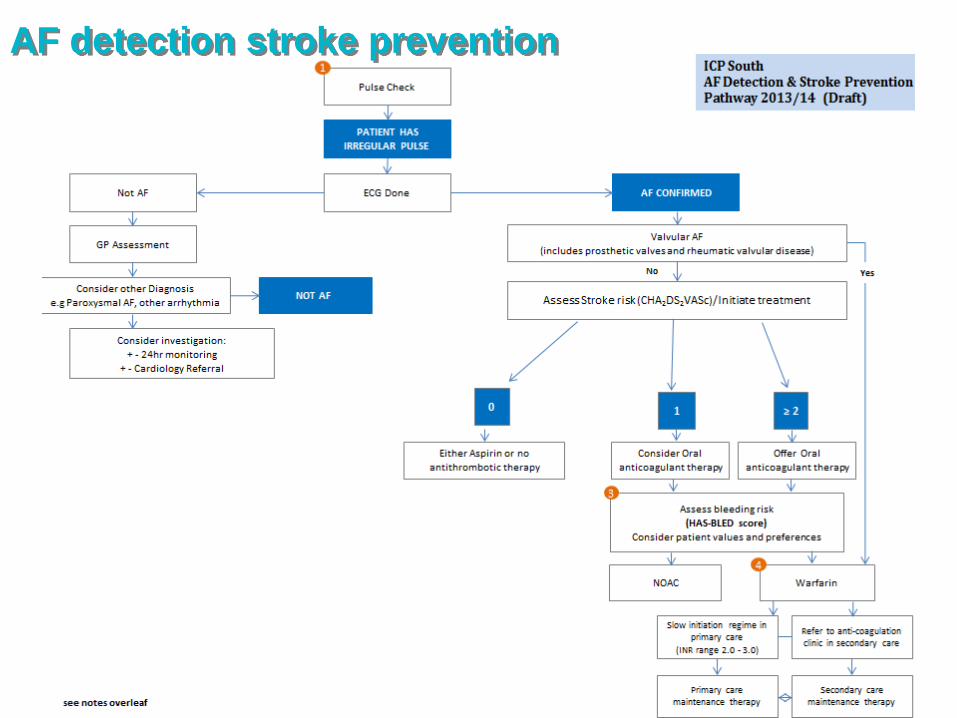
AF detection stroke prevention
