state of the art: integrase inhibitors clinical...
TRANSCRIPT

State of the ART:
Integrase Inhibitors Clinical Data
Juan BerenguerHospital General Universitario Gregorio Marañón (IiSGM)Madrid, Spain

Disclosures
• Consulting fees and honoraria
– Gilead, Janssen, MSD, ViiV Healthcare
• Grant support
– Gilead, MSD, ViiV Healthcare
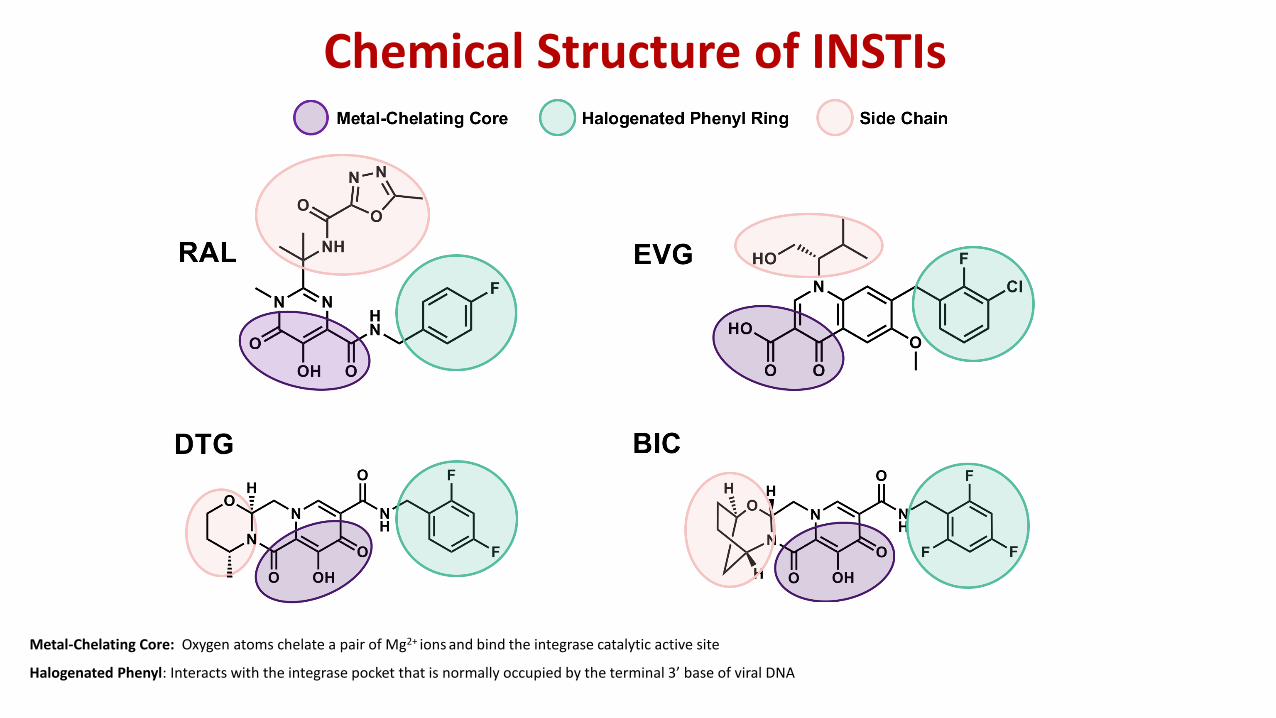
Chemical Structure of INSTIs
Metal-Chelating Core: Oxygen atoms chelate a pair of Mg2+ ions and bind the integrase catalytic active site
Halogenated Phenyl: Interacts with the integrase pocket that is normally occupied by the terminal 3’ base of viral DNA

ART-naïve patients

RAL or EFV with TDF/FTC in Treatment-Naive PtsFinal 5-Year Results From STARTMRK
Rockstroh JK, et al. J Acquir Immune Defic Syndr 2013; 63(1):77-85.

ATVr, DRVr, or RAL with FTC/TDF in ART-naïve patients (ACTG A5257)Open label, 1809 participants
Cumulative Incidence of Virologic or Tolerability Failure
Difference in 96 wk cumulative incidence (97.5% CI)
-20 0-10 10 20
15% (10%, 20%)
7.5% (3.2%, 12%)
7.5% (2.3%, 13%)
ATV/r vs RAL
DRV/r vs RAL
ATV/r vs DRV/r
Favors RAL
Favors RAL
Favors DRV/r
Lennox JL, et al. Ann Intern Med 2014; 161(7):461-471.

RAL 1200 mg QD* or RAL 400 mg BID with TDF/FTCONCEMRK Study
Cahn P, et al. The Lancet HIV 2017; 4(11):e486-e494* two 600 mg reformulated tablets

Dolutegravir-Based Regimens in Treatment-Naïve PtsHIV RNA <50 Copies/mL (Week 48)
Raffi F, et al. Lancet. 2013;381:735-743.Walmsley S, et al. N Engl J Med. 2013;369:1807-1818.Clotet B, et al. Lancet. 2014;383:2222-2231.
No resistance selected for any dolutegravir-based regimen
-20 -10 0 10 20
DTG + FTC/TDF or ABC/3TC (n=411)
RTG + FTC/TDF or ABC/3TC (n=411)
SPRING-2
Adjusted Treatment Difference (%)
2.5%
Week 48HIV RNA <50
Copies/mL (%)
88
85
Favors Comparator Favors Dolutegravir
DTG + ABC/3TC (n=414)
EFV/FTC/TDF (n=419)
SINGLE7.4%88
81
DTG + FTC/TDF or ABC/3TC (n=242)
DRV/r + FTC/TDF or ABC/3TC (n=242)
FLAMINGO7.1%90
83

EVG/COBI/FTC/TDF vs. EFV/FTC/TDF in Rx-Naïve Pts (GS-102*)Efficacy Endpoint: HIV-1 RNA <50 c/mL (FDA Snapshot) Weeks 48 and 96
Zolopa A, et al. J Acquir Immune Defic Syndr 2013; 63(1):96-100. *Double-blind study
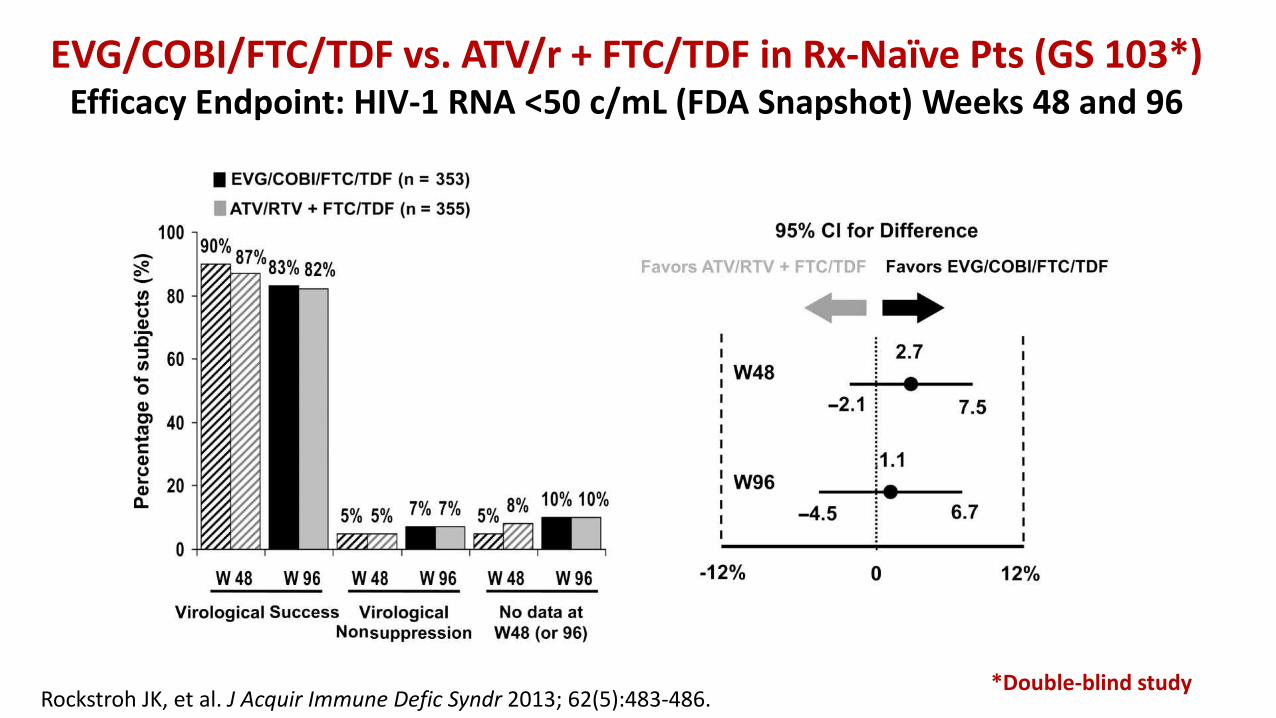
EVG/COBI/FTC/TDF vs. ATV/r + FTC/TDF in Rx-Naïve Pts (GS 103*) Efficacy Endpoint: HIV-1 RNA <50 c/mL (FDA Snapshot) Weeks 48 and 96
Rockstroh JK, et al. J Acquir Immune Defic Syndr 2013; 62(5):483-486.*Double-blind study

E/C/F/TAF vs. E/C/F/TDF in ART-Naïve Pts (104 and 111)
Primary Endpoint : Non-inferiority (12% margin) of E/C/F/TAF to Stribild based on HIV-1 RNA <50 copies/mL at Wk 48 FDA Snapshot
Secondary Endpoints: Efficacy, safety and tolerability observed through Week 96, Week 144
Sax PE, et al. The Lancet 2015; 385(9987):2606-2615.Wohl D, et al. JAIDS Journal of Acquired Immune Deficiency Syndromes 2016; 72(1):58-64.
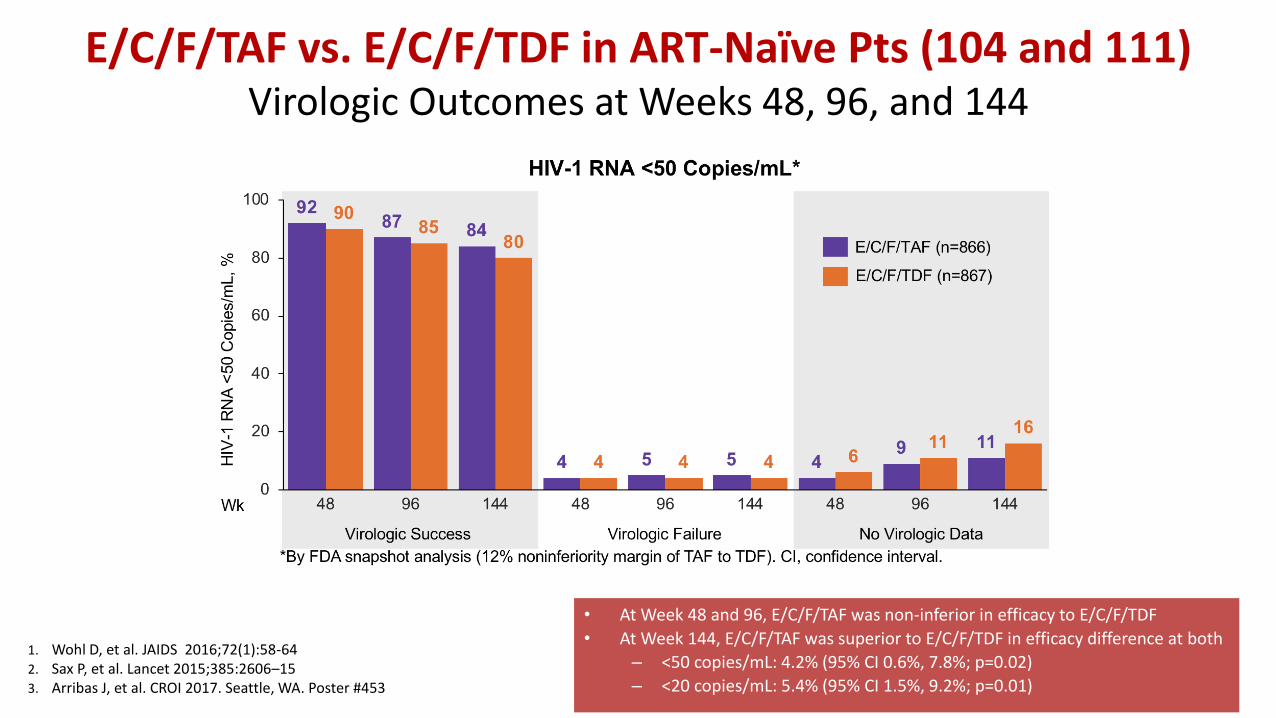
E/C/F/TAF vs. E/C/F/TDF in ART-Naïve Pts (104 and 111)Virologic Outcomes at Weeks 48, 96, and 144
• At Week 48 and 96, E/C/F/TAF was non-inferior in efficacy to E/C/F/TDF
• At Week 144, E/C/F/TAF was superior to E/C/F/TDF in efficacy difference at both
– <50 copies/mL: 4.2% (95% CI 0.6%, 7.8%; p=0.02)
– <20 copies/mL: 5.4% (95% CI 1.5%, 9.2%; p=0.01)
1. Wohl D, et al. JAIDS 2016;72(1):58-642. Sax P, et al. Lancet 2015;385:2606–153. Arribas J, et al. CROI 2017. Seattle, WA. Poster #453

E/C/F/TAF vs. E/C/F/TDF in ART-Naïve Pts (104 and 111)Week 144 Safety Summary
AEs leading to discontinuations were significantly less on E/C/F/TAF compared to E/C/F/TDF at Week 144Arribas J, et al. CROI 2017. Seattle, WA. Poster #453

Bictegravir/FTC/TAF vs Dolutegravir-Containing Regimens for Treatment-Naive Pts
• GS-1489: randomized, double-blind, active-controlled phase III trial[1]
Slide credit: clinicaloptions.com1. Gallant J, et al. Lancet. 2017;390:2063-2072. 2. Sax PE, et al. Lancet. 2017;390:2073-2082.
Bictegravir/FTC/TAF*
(n = 314)
Dolutegravir/ABC/3TC†
(n = 315)
ART-naive, HLA-B*5701–negative
pts with eGFRCG ≥ 50 mL/min
(N = 629)
All pts also received placebo tablets for comparator regimen (eg, pts in GS-1489 who received BIC/FTC/TAF also received DTG/ABC/3TC
placebo). *BIC/FTC/TAF 50/200/25 mg PO QD. †DTG/ABC/3TC 50/600/300 mg PO QD. ‡DTG + FTC/TAF 50 + 200/25 mg PO QD
Wk 48
▪ GS-1490: randomized, double-blind, active-controlled phase III trial[2]
Bictegravir/FTC/TAF*
(n = 320)
Dolutegravir + FTC/TAF‡
(n = 325)
ART-naive pts with
eGFRCG ≥ 30 mL/min
(N = 645)
Wk 48

BIC/FTC/TAF vs DTG-Containing RegimensKey Efficacy Findings
No resistance for any regimen components detected for either group
Slide credit: clinicaloptions.com
No resistance for any regimen components detected for either group
GS-1489: Wk 48 Virologic Efficacy[1] GS-1490: Wk 48 Virologic Efficacy[2]
Pts
(%
)
Pts
(%
)
100
80
60
40
20
0HIV-1 RNA
< 50 c/mL
HIV-1 RNA
≥ 50 c/mL
No Virologic
Data
BIC/FTC/TAF (n = 314)
DTG/ABC/3TC (n = 315)
92 93
1 3 7 4
100
80
60
40
20
0HIV-1 RNA
< 50 c/mL
HIV-1 RNA
≥ 50 c/mL
No Virologic
Data
BIC/FTC/TAF
DTG + FTC/TAF
89 93
4 16
0
99 > 99
1 < 16
0
PP1°
Treatment difference: -0.6%
(95% CI: -4.8% to 3.6%)Treatment difference (1o): -3.5%
(95% CI: -7.9% to 1.0%)
1. Gallant J, et al. Lancet. 2017;390:2063-2072. 2. Sax PE, et al. Lancet. 2017;390:2073-2082.

BIC/FTC/TAF vs DTG-Containing RegimensKey Safety Findings
• No d/c for renal AEs and no proximal tubulopathy for any regimen
Slide credit: clinicaloptions.com
Outcome Through Wk 48
GS-1489[1] GS-1490[2]
BIC/FTC/TAF(n = 314)
DTG/ABC/3TC(n = 315)
BIC/FTC/TAF(n = 320)
DTG + FTC/TAF(n = 325)
Diarrhea, % 13 13 12 12
Headache, % 11 14 13 12
Nausea, % 10 23* 8 9
Insomnia, % 4 6 5 4
Upper respiratory tract infection, % 6 11 5 7
Median eGFRCG ∆ from BL, mL/min -10.5 -10.8 -7.3 -10.8†
Mean BMD ∆ from BL, % spine/hip -0.83/-0.78 -0.60/-1.02 NR NR
D/c for AE, n (%) 0 4 (1) 5 (2) 1 (< 1)
*P < .0001; †P = .02
1. Gallant J, et al. Lancet. 2017;390:2063-2072. 2. Sax PE, et al. Lancet. 2017;390:2073-2082.

Guidelines: Recommended Regimens for First-line ART
Recommendations may differ according to renal function, HLA-B*5701 status, HBsAg status, osteoporosis status, other comorbidities
DHHS1 GESIDA2 EACS3 IAS-USA4
INSTI
▪ DTG/ABC/3TC▪ DTG + (TAF or TDF)/FTC▪ EVG/COBI/(TAF or TDF)/FTC▪ RAL + (TAF or TDF)/FTC ▪ BIC/TAF/FTC
▪ DTG/ABC/3TC▪ DTG + TAF/FTC▪ RAL + TAF/FTC
▪ DTG/ABC/3TC▪ DTG + (TAF or TDF)/FTC▪ EVG/COBI/(TAF or TDF)/FTC▪ RAL + (TAF or TDF)/FTC
▪ DTG/ABC/3TC▪ DTG + TAF/FTC▪ RAL + TAF/FTC ▪ EVG/COBI/TAF/FTC
NNRTI ▪ NONE ▪ NONE ▪ RPV/TAF/FTC, RPV/TDF/FTC ▪ NONE
PI ▪ NONE ▪ DRVc or DRVr + TAF/FTC or TDF/FTC ▪ NONE
1. DHHS ART Guidelines. March 2018. 2. GESIDA January 2018, 3. EACS October 2017, 4 Günthard HF, et al. JAMA. 2016;316:191-210.

Switch

Switching to INSTI-based ART in the setting of virologic suppression
Current regimen New regimen Effects (in addition to maintaining viral suppression*)
Reference
EFV + 2nRTIsRAL + 2nRTIs(Switch-ER)
Improves dislipidemia & CNS AEs Nguyen A, AIDS 2011
bPI + 2nRTIsRAL + 2nRTIs(Switchmrk)(Spiral)
Improves dislipidemia, *if fully active nRTIsEron JJ, Lancet 2010Martinez E, AIDS 2010

Switching to INSTI-based ART in the setting of virologic suppression
Current regimen New regimen Effects (in addition to maintaining viral suppression*)
Reference
EFV + 2nRTIsRAL + 2nRTIs(Switch-ER)
Improves dislipidemia & CNS AEs Nguyen A, AIDS 2011
bPI + 2nRTIsRAL + 2nRTIs(Switchmrk)(Spiral)
Improves dislipidemia, *if fully active nRTIsEron JJ, Lancet 2010Martinez E, AIDS 2010
bPI + 2nRTIsDTG + 2nRTIs(Neat 002)
Improves dislipidemia Gatell JM, 9th IAS 2017
bPI + 2nRTIsnnRTI + 2nRTIsINSTI + 2nRTIs
DTG/ABC/3TC(Striiving)
More frequent AEs Improvement treatment satisfaction questionnaires
Trottier B, Antivir Ther 2017
bPI or nnRTI or INSTI + 2nRTIsDTG + RPV(Sword 1&2)
Improvement in renal biomarkers and BMDLlibre JM, Lancet 2018McComsey, AIDS 2018

Switching to INSTI-based ART in the setting of virologic suppression
Current regimen New regimen Effects (in addition to maintaining viral suppression*)
Reference
EFV + 2nRTIsRAL + 2nRTIs(Switch-ER)
Improves dislipidemia & CNS AEs Nguyen A, AIDS 2011
bPI + 2nRTIsRAL + 2nRTIs(Switchmrk)(Spiral)
Improves dislipidemia, *if fully active nRTIsEron JJ, Lancet 2010Martinez E, AIDS 2010
bPI + 2nRTIsDTG + 2nRTIs(Neat 002)
Improves dislipidemia Gatell JM, 9th IAS 2017
bPI + 2nRTIsnnRTI + 2nRTIsINSTI + 2nRTIs
DTG/ABC/3TC(Striiving)
More frequent AEs Improvement treatment satisfaction questionnaires
Trottier B, Antivir Ther 2017
bPI or nnRTI or INSTI + 2nRTIsDTG + RPV(Sword 1&2)
Improvement in renal biomarkers and BMDLlibre JM, Lancet 2018McComsey, AIDS 2018
EFV/TDF/FTC; TDF/FTC/COBI/EVGATVr + TDF/FTC; bPI + 2nRTIseGFR 30-69 mL/min
EVG/C/F/TAF(Study 112)Single arm
Improvement in BMD & renal biomarkersPozniak A, JAIDS 2016Gupta S, IAS 2015 / Post F, CROI 2016 / McDonald C, ASM 2016 / Stein D, ASM 2016 / Podzamczer D, IAS 2017
ATVr + TDF/FTCWomen
EVG/C/F/TAF Improvement in BMD & renal biomarkers Hodder S, CROI 2017
GeSIDA Guidelines – January 2018 http://gesida-seimc.org/wp-content/uploads/2018/01/gesida_TAR_adultos_v3-1.pdf

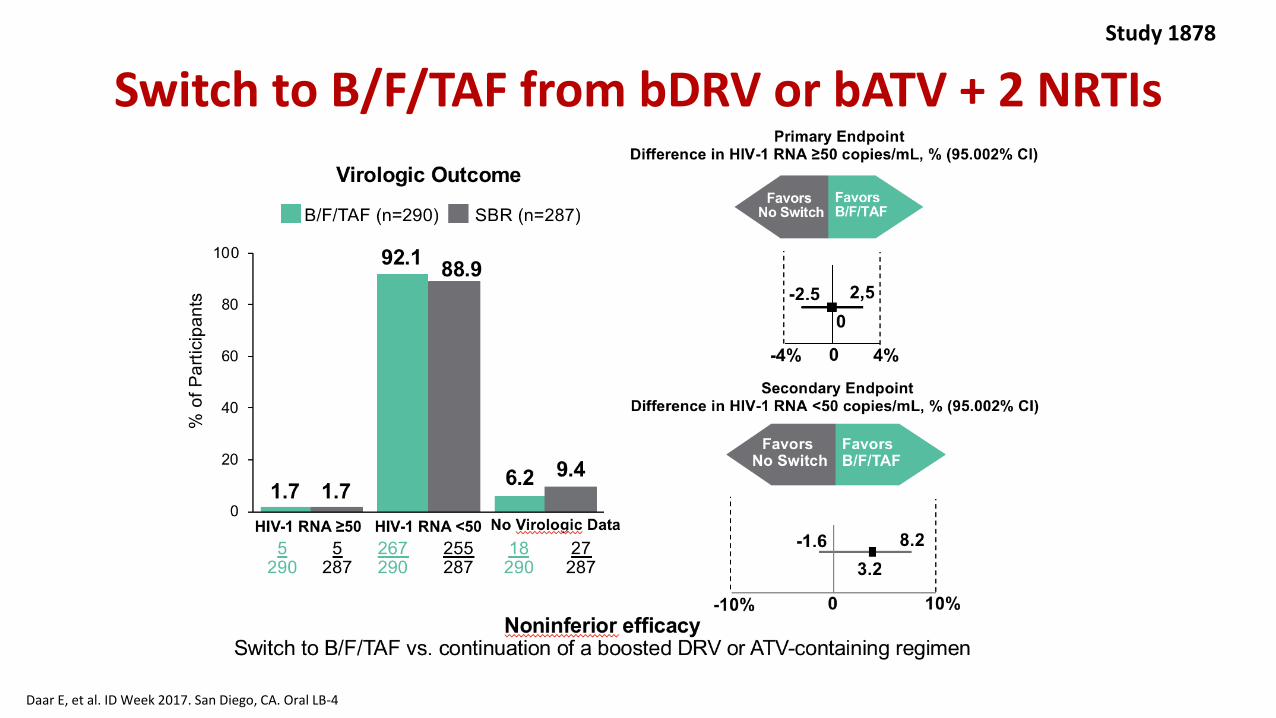
Switch to B/F/TAF from bDRV or bATV + 2 NRTIsStudy 1878
Daar E, et al. ID Week 2017. San Diego, CA. Oral LB-4
Switch to B/F/TAF from bDRV or bATV + 2 NRTIsStudy 1878
Daar E, et al. ID Week 2017. San Diego, CA. Oral LB-4

Switch to B/F/TAF from bDRV or bATV + 2 NRTIs
• No treatment-emergent resistance detected in BIC/FTC/TAF arm
• Lipid parameters significantly improved with switch vs baseline ART
– P = .002 for TG
– P = .033 for TC:HDL ratio
• Median eGFR decreased with switch vs continued baseline ART, but stabilized after Wk 4, consistent with known benign inhibition of creatinine tubular secretion by BIC
– Median change at Wk 48: -4.3 mL/min vs +0.2 mL/min (P < .001)
Study 1878
Daar E, et al. ID Week 2017. San Diego, CA. Oral LB-4

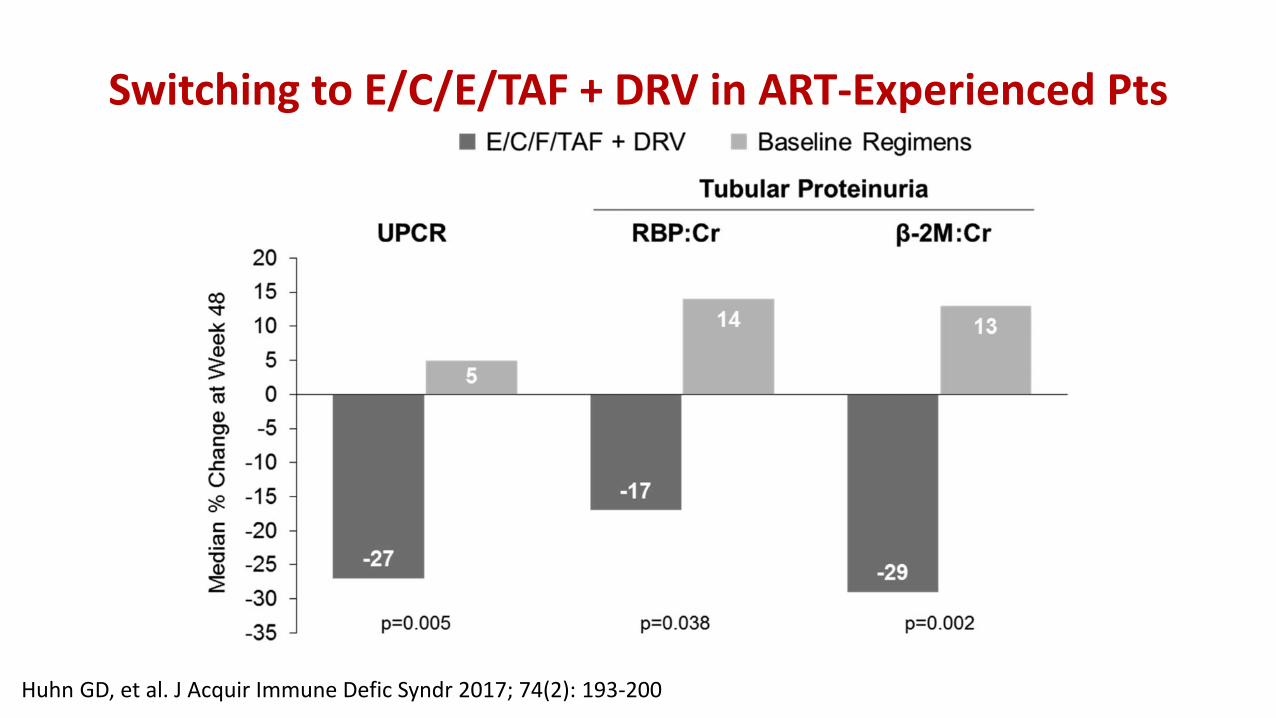
Switching to E/C/E/TAF + DRV in ART-Experienced Pts
Huhn GD, et al. J Acquir Immune Defic Syndr 2017; 74(2): 193-200
• Phase 3, open-label, randomized study with HIV+, virologically suppressed adults • 2 to 3-class drug resistance and at least 2 prior regimen failures • Primary endpoint: proportion of participants with HIV-1 RNA < 50 c/ml at week 24 [FDA snapshot algorithm].
Switching to E/C/E/TAF + DRV in ART-Experienced Pts
Huhn GD, et al. J Acquir Immune Defic Syndr 2017; 74(2): 193-200

Salvage therapy

Conference on Retroviruses and Opportunistic Infections; February 13-16, 2017; Seattle, WA
Slide 29 of 39
From JJ Eron, Jr, MD at San Antonio, Texas, August 21-23, 2017, Ryan White HIV/AIDS Program Clinical Conference, IAS−USA.
• Key eligibility criteria: on first-line 2 NRTIs + NNRTI regimen for ≥ 6 months, failing virologically (HIV-1 RNA ≥400 c/mL on 2
occasions); no primary viral resistance to PIs or INSTIs
• Stratification: by HIV-1 RNA (≤ or >100,000 copies/mL), number of fully active NRTIs in the investigator-selected study
background regimen (2 or <2)
• Primary endpoint: proportion with HIV-1 RNA <50 c/mL at Week 48 using the FDA snapshot algorithm (12% noninferiority
margin)
DAWNING Study – Dolutegravir in Second Line
Week 48primaryanalysis
Randomisation
FDA, US Food and Drug Administration; INSTI, integrase strand transfer inhibitor.
Open-label randomized noninferiority phase IIIb study
DTG + 2 NRTIsOpen label,
randomized
1:1LPV/RTV + 2 NRTIs
DTG + 2 NRTIs
Continuation phase
Week 24interim analysis
Week 52
Aboud et al. IAS 2017; Paris, France. Slides TUAB0105LB.

Conference on Retroviruses and Opportunistic Infections; February 13-16, 2017; Seattle, WA
Slide 30 of 39
From JJ Eron, Jr, MD at San Antonio, Texas, August 21-23, 2017, Ryan White HIV/AIDS Program Clinical Conference, IAS−USA.
• DTG + 2 NRTIs is superior to LPV/RTV + 2 NRTIs with
respect to snapshot in the ITT-E (<50 c/mL) at Week
24, P<0.001
Snapshot Outcomes at Week 24: ITT-E and PP Populations
CI, confidence interval; ITT-E, intent-to-treat exposed; PP, per protocol.
82
69
86
72
0
20
40
60
80
100
Virologicsuccess
HIV
-1 R
NA
<50
c/m
L, %
DTG + 2 NRTIs (ITT-E, n=312)
LPV/RTV + 2 NRTIs (ITT-E,n=312)
DTG + 2 NRTIs (PP, n=282)
LPV/RTV + 2 NRTIs (PP,n=275)
Virologic outcomes Treatment differences (95% CI)
LPV/RTV DTG
13,8
14,5
-12 -10 -8 -6 -4 -2 0 2 4 6 8 10 12 14 16 18 20 22 24
ITT-E
PP
7.3 20.3
21.08.1
Aboud et al. IAS 2017; Paris, France. Slides TUAB0105LB.
Similar result regardless of BL VL, CD4 or # of active NRTI
Cahn et al. IAS 2013; Kuala Lumpur, Malaysia. Abstract WELBB03.
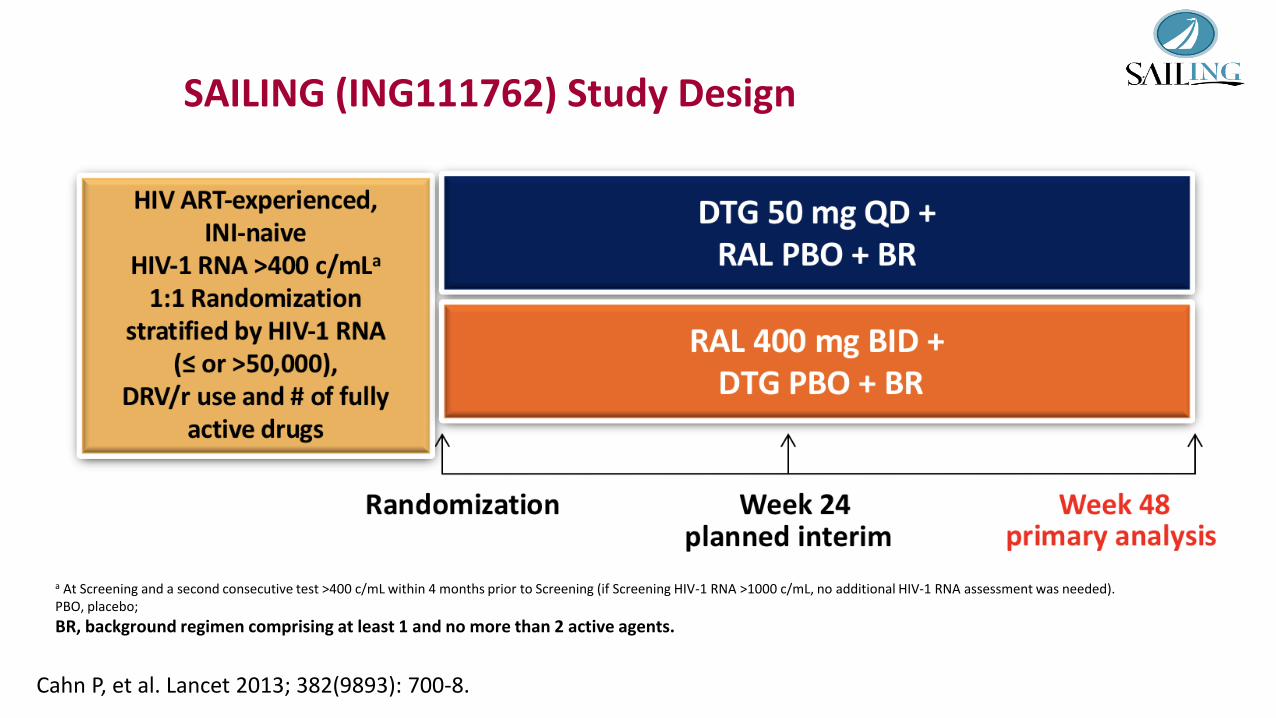
SAILING (ING111762) Study Design
a At Screening and a second consecutive test >400 c/mL within 4 months prior to Screening (if Screening HIV-1 RNA >1000 c/mL, no additional HIV-1 RNA assessment was needed). PBO, placebo;
BR, background regimen comprising at least 1 and no more than 2 active agents.
Cahn P, et al. Lancet 2013; 382(9893): 700-8.

Cahn et al. IAS 2013; Kuala Lumpur, Malaysia. Abstract WELBB03.
DTG 50 mg QD(n=354)
RAL 400 mg BID(n=361)
Age, median (y) 42 43Gender, female 30% 34%Race, white 50% 49%
African American/African heritage 41% 44%HIV-1 RNA, median (log10 c/mL) 4.17 4.21
>50,000 c/mL 30% 29%CD4+ count, median (cells/mm3) 205 193
<200 cells/mm3 49% 51%HBV/HCV coinfection 14% 18%Duration prior ART, median (y) 6.7 6.0≥3 Class resistance 47% 51%DRV/r in background regimenDRV/r use without primary PI mutations 72 (20%) 77 (21%)No DRV/r use or DRV/r use with primary PI mutations
282 (80%) 284 (79%)
Baseline Characteristics
Cahn P, et al. Lancet 2013; 382(9893): 700-8.

Cahn et al. IAS 2013; Kuala Lumpur, Malaysia. Abstract WELBB03.
Primary Endpoint: HIV-1 RNA <50 c/mL at Week 48
71
20
9
64
28
9
0
20
40
60
80
Virologic success Virologic non-response
No W48 data*
Pe
rce
nta
ge o
f su
bje
cts
(%)
DTG 50 mg QD (n=354) RAL 400 mg BID (n=361)
95% CI for differenceFavors
RALFavors
DTG
-20% 0 20%
7.40.7 14.2
-12%
Cahn P, et al. Lancet 2013; 382(9893): 700-8.

VIKING-3: Rationale and Study Design
Castagna A, et al. J Infect Dis 2014; 210(3): 354-62
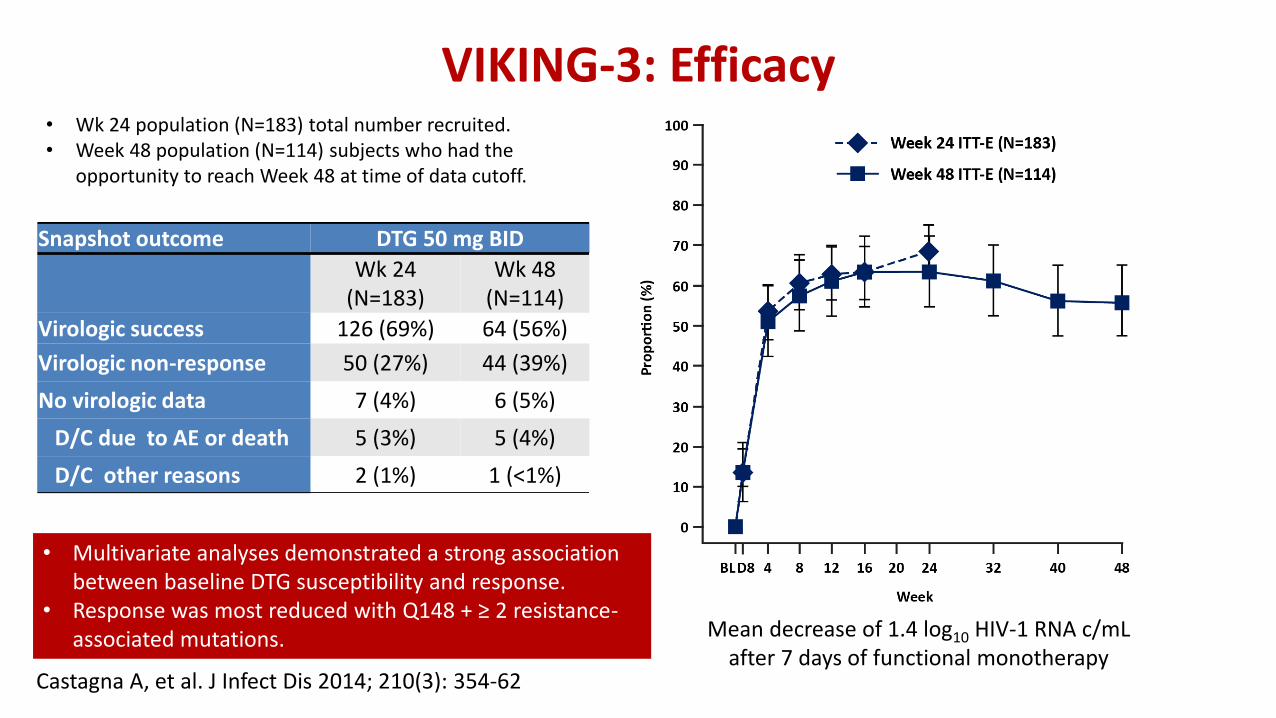
Snapshot outcome DTG 50 mg BID
Wk 24(N=183)
Wk 48 (N=114)
Virologic success 126 (69%) 64 (56%)
Virologic non-response 50 (27%) 44 (39%)
No virologic data 7 (4%) 6 (5%)
D/C due to AE or death 5 (3%) 5 (4%)
D/C other reasons 2 (1%) 1 (<1%)
• Wk 24 population (N=183) total number recruited.• Week 48 population (N=114) subjects who had the
opportunity to reach Week 48 at time of data cutoff.
VIKING-3: Efficacy
Mean decrease of 1.4 log10 HIV-1 RNA c/mL after 7 days of functional monotherapy
• Multivariate analyses demonstrated a strong association between baseline DTG susceptibility and response.
• Response was most reduced with Q148 + ≥ 2 resistance-associated mutations.
Castagna A, et al. J Infect Dis 2014; 210(3): 354-62

Women

EVG/COBI/FTC/TDF vs. ATV/r + FTC/TDF in ART-Naïve Women With HIV-1 Infection (WAVES Study)
37
• Key eligibility criteria HIV-1 RNA ≥500 copies/mL / eGFR ≥70 mL/min / No history of ART / Sensitivity to FTC, TDF, and ATV
• Primary endpoint: proportion of patients with HIV-1 RNA <50 copies/mL at Week 48 (FDA snapshot analysis)• Stratification
HIV-1 RNA (≤100,000, >100,000‒≤400,000, or >400,000 copies/mL) Race (black or nonblack)
Squires K, et al. Lancet HIV 2016; 3: e410-e420

Virologic Outcome at Week 48
• Mean CD4 cell increase: 196 cells/mm3 (EVG/COBI/FTC/TDF and ATV+RTV+FTC/TDF)
38Squires K, et al. Lancet HIV 2016; 3: e410-e420
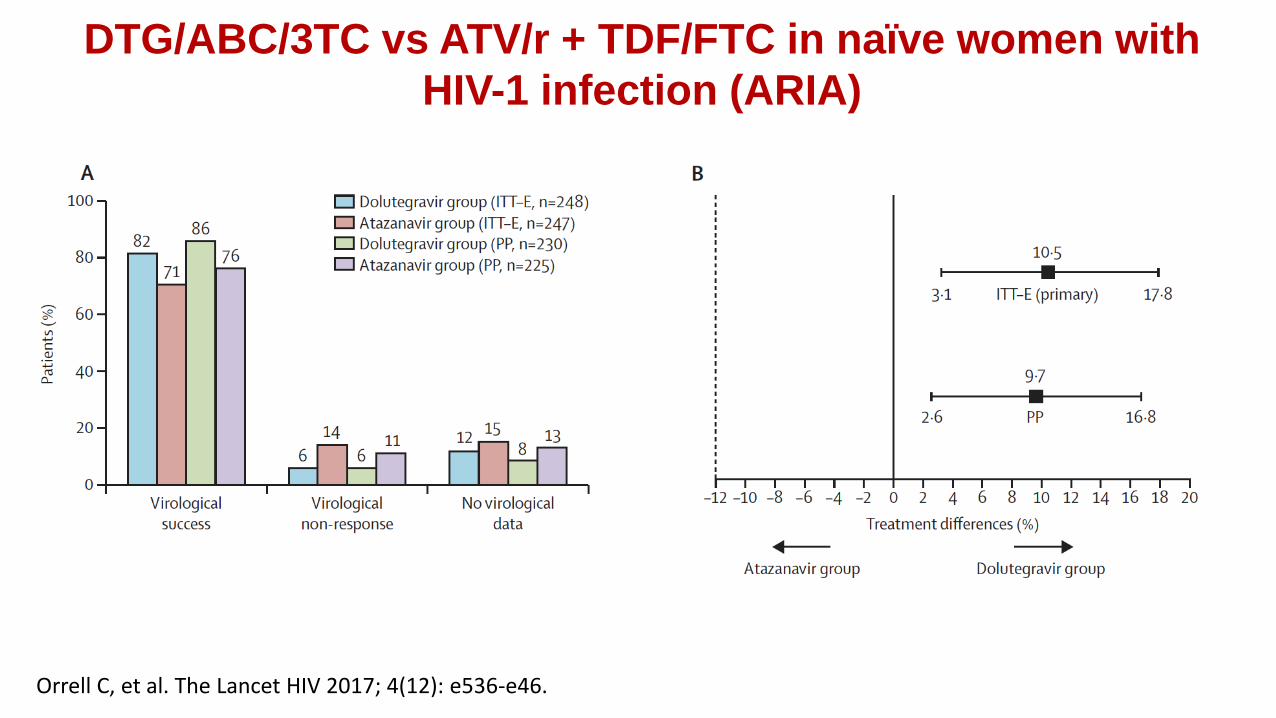
DTG/ABC/3TC vs ATV/r + TDF/FTC in naïve women with
HIV-1 infection (ARIA)
Orrell C, et al. The Lancet HIV 2017; 4(12): e536-e46.

Initial regimens for ART-naïve pregnant women
DHHS1 GESIDA2
N-RTI ▪ ABC/3TC▪ TDF/FTC or TDF/3TC
▪ ABC/3TC▪ TDF/FTC or TDF/3TC
INSTI ▪ RAL + 2nRTI ▪ RAL + 2nRTI
NNRTI ▪ NONE ▪ NONE
PI▪ ATV/r + 2nRTI▪ DRV/r + 2nRTI
▪ ATV/r + 2nRTI▪ DRV/r + 2nRTI
1. DHHS ART Guidelines. May 2018. 2. GESIDA March 2018.

Additional safety data

Risks of cardiovascular or CNS AEs and IRIS for DTG vs other antiretrovirals: meta-analysis of RCT
Hill AM et al. Curr Opin HIV AIDS 2018; 13: 102-111

Risks of cardiac or CNS AEs and IRIS for DTG vs other antiretrovirals: meta-analysis of RCT
• No significant effect of DTG on the risk of cardiac, IRIS or suicide-related serious adverse events.
• Higher risk of insomnia for DTG.
• Other completed RCT should be included in new evaluations of DTG safety.
• Continued pharmacovigilance, with regular meta-analyses, should be used to monitor safety.
Hill AM et al. Curr Opin HIV AIDS 2018; 13: 102-111

http://prais.paho.org/es/who-products-alert-potential-safety-issue-affecting-women-living-with-hiv-using-dolutegravir-at-the-time-of-conception/

Statement on dolutegravir – Geneva 18 May 2018
• The investigator of an independent NIH‐funded study has identified a potential safety issue with DTG, and reported it to WHO and ViiV Healthcare. – Neural tube defects (NTD) in infants born to women who were taking
DTG at the time of conception.
• The issue has been identified from a preliminary unscheduled analysis of an ongoing observational study in Botswana– 4 cases of NTD in 426 women who became pregnant while taking DTG– This rate of approximately 0.9% compares to a 0.1% risk of NTD in infants
born to women taking other ART medicines at the time of conception.
http://prais.paho.org/es/who-products-alert-potential-safety-issue-affecting-women-living-with-hiv-using-dolutegravir-at-the-time-of-conception/

Information on neural tube defects (NTD)
• The neural tube is the foundation of the spinal cord, brain and the bone and tissues that surround it.
• Neural tube defects (NTD)
– occur when the neural tube fails to completely form; this formation takes place between 0 and 28 days after conception.
– may be related to folate deficiency, other medications or family history.
– WHO recommends that women take daily supplements of folic acid before conception and during pregnancy to help prevent NTD.
http://prais.paho.org/es/who-products-alert-potential-safety-issue-affecting-women-living-with-hiv-using-dolutegravir-at-the-time-of-conception/

DHHS. Recommendations Regarding the Use of DTG in Women with HIV who are Pregnant or of Child-Bearing Potential
ART history Clinical Scenario • Recommendations/Comments
Not on DTG Pregnant < 8 weeks from LMP • Do not initiate a DTG-based regimen
Pregnant 8 weeks from LMP • DTG can be considered as part of an ARV regimen.
Desire pregnancy orNot using effective contraception
• Do not initiate a DTG-based regimen
Do not desire pregnancy andUsing effective contraception
• DTG can be considered as part of an ARV regimen.• Pregnancy testing prior to initiation of DTG.• Discuss the potential of DTG to the fetus and the effective use
of contraception.
https://aidsinfo.nih.gov/news/2109/recommendations-regarding-the-use-of-dolutegravir-in-adults-and-adolescents-with-hiv-who-are-pregnant-or-of-child-bearing-potential
LMP: last menstrual period

DHHS. Recommendations Regarding the Use of DTG in Women with HIV who are Pregnant or of Child-Bearing Potential
ART history Clinical Scenario • Recommendations/Comments
Currently on DTG Pregnant < 8 weeks from LMP • Switch DTG to al alternative option
Pregnant 8 weeks from LMP • DTG can be continued
Desire pregnancy orNot using effective contraception
Have effective options other than DTG• Switch DTG to al alternative optionDTG as part of salvage regimen with no alternative options• Continue DTG
Do not desire pregnancy andUsing effective contraception
• Continue DTG• Discuss the potential of DTG to the fetus and the effective use
of contraception
https://aidsinfo.nih.gov/news/2109/recommendations-regarding-the-use-of-dolutegravir-in-adults-and-adolescents-with-hiv-who-are-pregnant-or-of-child-bearing-potential
LMP: last menstrual period

Conclusions