state of illinois department of central management services …€¦ · · 2014-04-30benefit...
TRANSCRIPT

BenefitChoiceOptions
State of Illinois
State of IllinoisDepartment of Central Management Services • Bureau of Benefits
Enrollment Period May 1 - June 2, 2014 • Effective July 1, 2014 - June 30, 2015

Benefit Choice isMay 1 - June 2, 2014
Benefit Choice Forms must be submitted to your Group Insurance Representative (GIR) no later than
Monday, June 2nd! If you do not want to change yourcoverage, you do not need to submit a form.
IMPORTANT: Enrollment in the Medical Care Assistance Plan (MCAP)and/or the Dependent Care Assistance Plan (DCAP) is optional. Eligibleemployees MUST submit a new MCAP and/or DCAP enrollment form no
later than June 2nd in order to be enrolled effective July 1, 2014.
It is each member’s responsibility to knowplan benefits and make an informed decision
regarding coverage elections.
Online Group InsuranceBenefit Statements. Go tothe Benefits website and
click on this button. . .
Go to the ‘Latest News’ section of the Benefits website atwww.benefitschoice.il.gov
for group insurance updates throughout the plan year.

www.benefitschoice.il.gov 1
Table of ContentsMessage to Plan Members. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Member Responsibilities. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Benefit Choice Changes for Plan Year 2015. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
What You Should Know for Plan Year 2015 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Member and Dependent Monthly Contributions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6-7
Health Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Opt Out and Annuitant Waiver . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Health Plan Descriptions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10-11
Out-of-Pocket Maximums Description and Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Map of Health Plans in Illinois Counties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Benefits Comparison Charts. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14-16
Federally Required Notices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Plan Participants Eligible for Medicare . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18-19
Behavioral Health Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Prescription Benefit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21-23
Dental Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24-25
Vision Plan. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Life Insurance Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Flexible Spending Accounts (FSA). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Medical Care Assistance Plan (MCAP) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Dependent Care Assistance Plan (DCAP). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
Program Initiatives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
Get HIP (Health Improvement Program) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Plan Administrators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32-33
Transition of Care after Health Plan Change:Members and their dependents who elect tochange health plans and are then hospitalizedprior to July 1 and are discharged on or afterJuly 1, should contact both the current andfuture health plan administrators and primarycare physicians as soon as possible tocoordinate the transition of services.
Members or dependents involved in anongoing course of treatment or who haveentered the third trimester of pregnancy shouldcontact the new plan to coordinate thetransition of services for treatment.
COBRA Participants: During the Benefit ChoicePeriod, COBRA participants have the samebenefit options available to them as all othermembers with the exception of life insurancecoverage, which is not available to COBRAparticipants. COBRA health and dental rates forthe 2015 plan year will be available on or afterMay 1, 2014, by calling (217) 558-6194.
Important Reminders

FY2015 Benefit Choice Options2
The Benefit Choice Period will be May 1 throughJune 2, 2014, for eligible members. Membersare employees (full-time employees, part-timeemployees working 50% or greater andemployees on leave of absence), COBRAparticipants, and annuitants and survivors notenrolled in, or eligible for, participation underthe Medicare Advantage Program (see page 5for more information). Elections will be effectiveJuly 1, 2014.
Unless otherwise indicated, all Benefit Choicechanges should be made on the Benefit ChoiceElection Form available on the Benefits website.Members should complete the form only ifchanges are being made. Your agency/university group insurance representative (GIR)will process the changes based upon theinformation indicated on the form. Membersmay obtain GIR names and locations by eithercontacting the agency’s personnel office orviewing the GIR listing on the Benefits websitelocated at www.benefitschoice.il.gov.
Members may make the following changesduring the Benefit Choice Period:
• Change health plans.
• Add or drop dental coverage.
• Add or drop dependent coverage. Note:Survivors may add a dependent only if thatdependent was eligible for coverage as adependent under the original member.
• Add, drop, increase or decrease MemberOptional Life insurance coverage.
• Add or drop Child Life, Spouse Life and/orAD&D insurance coverage.
• Elect to opt out (applies only to full-timeemployees (including those on a leave ofabsence), annuitants and survivors). Theelection to opt out of the State’s coveragewill terminate the health, vision, dental,behavioral health and prescription coveragefor the member and any covereddependents. Note: Members must provide
proof of other comprehensive healthcoverage in order to opt out.
o Effective with this Benefit Choice Period,annuitants and survivors electing to opt outof the State’s coverage will remain enrolledin the dental coverage. Annuitants andsurvivors who do not wish to continuedental coverage must check the appropriatebox on the Benefit Choice form indicatingtheir desire to drop the dental coverage.
• Elect to waive health, dental, vision andprescription coverage (part-time employees50% or greater, annuitants and survivors).
• Re-enroll in the Program if previously optedout of or waived coverage. Members havethe option of not electing dental coverageupon re-enrollment into the health plan.
• Re-enroll in the Program if coverage iscurrently terminated due to nonpayment ofpremium while on leave of absence(employees only – subject to eligibility criteria).Any outstanding premiums plus the Julypremium must be paid before coverage willbe reinstated. Note: Survivors and annuitantsare not eligible to re-enroll if previouslyterminated due to nonpayment of premium.
• Enroll in MCAP and/or DCAP. Employeesmust enroll each year; previous enrollment inthe program does not continue into the newplan year. Note: Survivors and annuitantsare not eligible for MCAP or DCAP.
Documentation Requirements
• Documentation, including the SSN, isrequired when adding dependent coverage.
• An approved statement of health is requiredto add or increase Member Optional Lifecoverage or to add Spouse Life or Child Lifecoverage.
• If opting out, proof of other comprehensivehealth coverage provided by an entity otherthan the Department of Central ManagementServices, is required.
Message to Plan Members

www.benefitschoice.il.gov 3
You must notify the group insurancerepresentative (GIR) at your employing agency,university or retirement system if:
• You and/or your dependents experience achange of address.
• Your dependent loses eligibility.Dependents that are no longer eligible underthe Program (including divorced spouses orpartners of a dissolved civil union ordomestic partner relationship) must bereported to your GIR immediately. Failure toreport an ineligible dependent is considereda fraudulent act. Any premium payments youmake on behalf of the ineligible dependentwhich result in an overpayment will not berefunded. Additionally, the ineligibledependent may lose any rights to COBRAcontinuation coverage.
• You go on a leave of absence or have timeaway from work. When you go on a leave ofabsence and are not receiving a paycheck orare ineligible for payroll deductions, you arestill responsible to pay for your groupinsurance coverage. You should immediatelycontact your GIR for your options, if any, tomake changes to your current coverage.Requested changes will be effective the dateof the written request if made within 60 days ofbeginning the leave. You will be billed by CMSfor the cost of your current coverage. Failure topay the bill may result in a loss of coverageand/or the filing of an involuntary withholdingorder through the Office of the Comptroller.
• You have or gain other coverage. If you havegroup coverage provided by a plan other thanthe Program, or if you or your dependents gainother coverage during the plan year.
• You experience a change in Medicare status.A copy of the Medicare card must beprovided to the Medicare Coordination ofBenefits Unit when a change in your or yourdependent's Medicare status occurs. Failureto notify the Medicare Coordination ofBenefits Unit at Central Management Servicesof your Medicare eligibility may result insubstantial financial liabilities. The MedicareUnit’s address and phone number can befound on page 30.
• You get married or enter into a civil unionpartnership; or your marriage, domesticpartnership or civil union partnership isdissolved.
• You have a baby or adopt a child.
• Your employment status changes fromfull-time to part-time or vice versa, or theemployment status of your dependentchanges.
• You have a financial or medical power ofattorney (POA) who you would like to beable to make decisions and get informationon your behalf if you are incapacitated.
o Financial POA – used by your agent tochange your health plan elections. Thefinancial POA document would allow anagent to make health, dental and lifeinsurance plan elections on your behalfand should be sent to your agency orretirement system group insurancerepresentative.
o Medical POA – used by your agent tospeak with your health, dental and visionplans about your coverage and claims. Amedical POA generally gives an agent theauthority to make medical decisions onyour behalf; therefore, in order for youragent to speak with your health, dentaland/or vision plan(s), you would need themedical POA document to each plan forthem to have on file.
Contact your GIR if you are uncertain whether ornot a life-changing event needs to be reported.
Member Responsibilities
Beneficiary DesignationsYou should periodically review allbeneficiary designations and make theappropriate updates. Remember, you mayhave death benefits through variousstate-sponsored programs, each having aseparate beneficiary form:
• State of Illinois life insurance
• Retirement benefits
• Deferred Compensation
FY2015 Benefit Choice Options4
Benefit Changes for Plan Year 2015(Enrollment Period May 1 – June 2, 2014)
It is each member’s responsibility to know theirplan benefits in order to make an informeddecision regarding coverage elections.Members should carefully review all theinformation in this booklet to be aware of thebenefit changes for the upcoming plan year.The Benefit Choice Period will be May 1 throughJune 2, 2014. All elections will be effective July 1,2014.Managed Care Plan (HMO/OAP) Changes• Managed Care (HMO and OAP all tiers)
emergency room visit copayment increasesto $250
• Managed Care (HMO and OAP all tiers)outpatient surgery copayment increases to$250
• HMO and OAP Tier I, physician office visitcopayment increases to $20
• HMO and OAP Tier I, specialist office visitand home health visit copayment increases to$30
• HMO and OAP Tier I, home health visitcopayment increases to $30
• HMO and OAP Tier I, inpatient admissioncopayment increases to $350
• OAP Tier II, inpatient surgery copaymentincreases to $400
• OAP Tier III, inpatient admission copaymentincreases to $500
• New combined OAP Tier I and Tier II out-of-pocket maximum (individual) of $6,250
• New combined OAP Tier I and Tier II out-of-pocket maximum (family) of $12,750
• OAP Tier III, out-of-pocket maximum(individual and family) removed
• Prescription deductible increases to $100 perindividual per plan year
• Retiree health plan contributions increase to2% for retirees enrolled in Medicare Parts Aand B and to 4% for all other retirees
Quality Care Health Plan (QCHP) Changes• Individual plan year deductibles increase $25
per salary range (see chart on page 16)• Family plan year deductible caps increase to
2.5 times the individual plan year deductible(see chart on page 16)
• In-network coinsurance for services decreasesfrom 90% to 85%
• Emergency room visit copayment increasesto $450
• In-network hospital admission deductibleincreases to $100
• Out-of-network hospital admission deductibleincreases to $500
• Prescription deductible increases to $125 perindividual per plan year
• Retiree health plan contributions increase to2% for retirees enrolled in Medicare Parts Aand B and to 4% for all other retirees
Quality Care Dental Plan (QCDP) Changes
• Dental deductible increases to $175 per planparticipant per plan year
Vision Changes
• Vision eye exams, lenses and standard framecopayment increases to $25
• Vision replacement lenses, including contactlenses, available once every 12 months(previously every 24 months)

www.benefitschoice.il.gov 5
• Medicare Advantage ‘TRAIL’ Program:Effective February 1, 2014, the State began anew Medicare Advantage Program, referredto as the ‘TRAIL’ (Total Retiree AdvantageIllinois) for annuitants and survivors enrolled inboth Medicare Parts A and B.
Each fall, annuitants and survivors who meetthe criteria for enrollment in the MedicareAdvantage ‘TRAIL’ Program will be notified ofthe TRAIL Enrollment Period by theDepartment of Central ManagementServices. These members will be required tochoose a Medicare Advantage plan or optout of State coverage (which includes health,prescription and vision coverage) and will nolonger be able to make changes duringsubsequent Benefit Choice Periods.
For more information regarding the MedicareAdvantage ‘TRAIL’ Program, includingeligibility criteria, go towww.cms.illinois.gov/thetrail.
• Federal Healthcare Reform: As a result of thePatient Protection and Affordable Care Act,the out-of-pocket maximum amount for theopen access plans (OAPs) have increased.Additionally, Tier III no longer has an out-of-pocket maximum. OAP Tiers I and II havecombined charges contributing to the out-of-pocket maximum. Refer to page 12 for moreinformation.
• Dependent Eligibility Verification Audit: In aneffort to control costs and ensure enrollmentfiles are accurate, the State of Illinois will beconducting a dependent eligibility verificationaudit of State employees during FY2015. Formore information, refer to page 30.
• Annuitant and Survivor Opt Out Option:Effective July 1, 2014, annuitants and survivorselecting to opt out of the health coverage(which includes the termination of vision andprescription coverage) will remain enrolled inthe dental and life insurance coverage.Members who opt out of the health coverageand do not want the dental coverage must
mark the appropriate box on the BenefitChoice Election form indicating they do notwant the dental coverage. Further informationregarding the Opt Out Programs is availableon page 9.
• Monthly Health Plan Contributions forRetirees, Annuitants and Survivors: All retirees,annuitants and survivors are charged apercentage of their combined annuity value tocover the costs of the basic program of grouphealth benefits. Effective July 1, 2014, retireesthat are ineligible for premium-free MedicarePart A will be charged 4% of their monthlyannuity value; retirees that are eligible for andenrolled in Medicare Parts A and B will becharged 2% of their monthly annuity value. Seepage 7 for more information.
• Weight-Loss Benefit: As a commitment to anemployee’s overall wellness, eligible planparticipants are entitled to receive a rebatetowards the cost of an approved weight-lossprogram. The maximum rebate is $200 onceevery three plan years. Employees who utilizea weight-loss program are eligible for theweight-loss benefit through the Department.
The weight-loss benefit is available to allemployees who are eligible for benefitsunder the State Employees Group InsuranceProgram. Active employees who opt out orwaive health coverage under the Program arenot eligible for this benefit, nor aredependents, annuitants or survivors.
Documentation required to receivereimbursement include receipts indicatingpayment for the weight-loss program, alongwith the employee’s name, address, agency’sname and telephone number. For moreinformation about this benefit, contact theMember Services Unit at the Bureau ofBenefits.
• Express Scripts Mail Order: Express Scripts isnow the mail order pharmacy for the QualityCare Health Plan (QCHP), HealthLink OAP planand Coventry OAP plan.
What You Should Know forPlan Year 2015
FY2015 Benefit Choice Options6
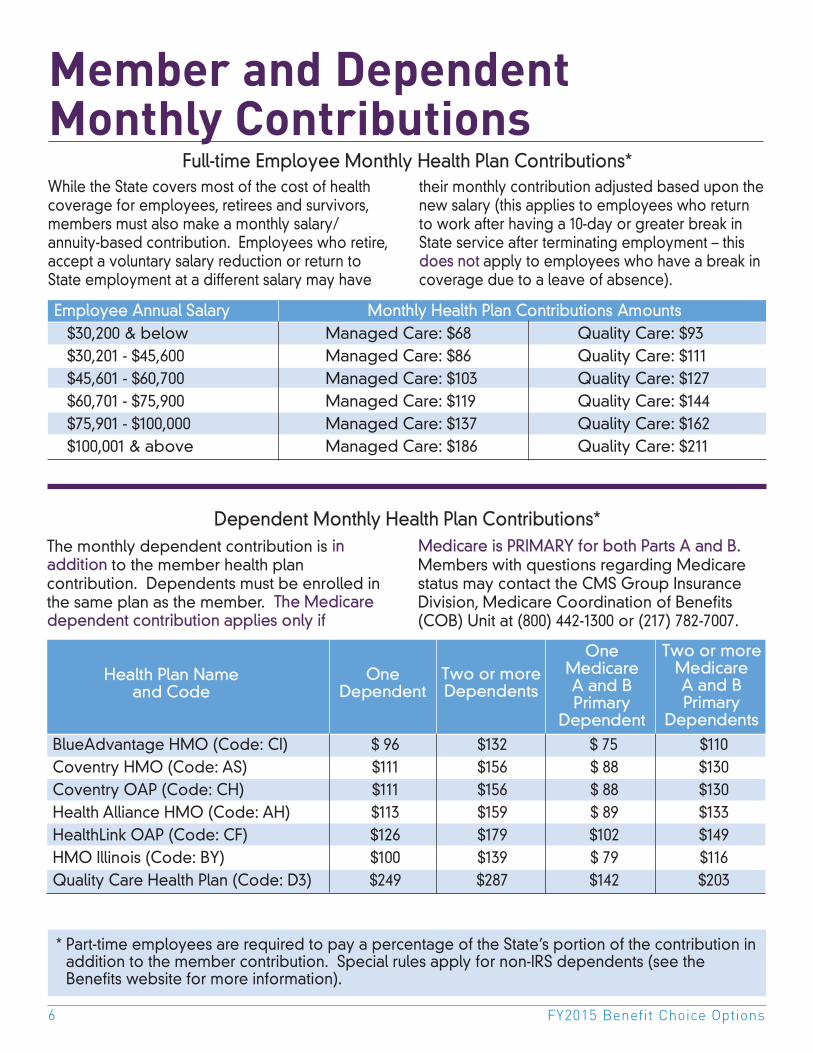
The monthly dependent contribution is inaddition to the member health plancontribution. Dependents must be enrolled inthe same plan as the member. The Medicaredependent contribution applies only if
Medicare is PRIMARY for both Parts A and B.Members with questions regarding Medicarestatus may contact the CMS Group InsuranceDivision, Medicare Coordination of Benefits(COB) Unit at (800) 442-1300 or (217) 782-7007.
Employee Annual Salary Monthly Health Plan Contributions Amounts$30,200 & below Managed Care: $68 Quality Care: $93$30,201 - $45,600 Managed Care: $86 Quality Care: $111$45,601 - $60,700 Managed Care: $103 Quality Care: $127$60,701 - $75,900 Managed Care: $119 Quality Care: $144$75,901 - $100,000 Managed Care: $137 Quality Care: $162$100,001 & above Managed Care: $186 Quality Care: $211
Member and Dependent Monthly ContributionsWhile the State covers most of the cost of healthcoverage for employees, retirees and survivors,members must also make a monthly salary/annuity-based contribution. Employees who retire,accept a voluntary salary reduction or return toState employment at a different salary may have
their monthly contribution adjusted based upon thenew salary (this applies to employees who returnto work after having a 10-day or greater break inState service after terminating employment – thisdoes not apply to employees who have a break incoverage due to a leave of absence).
* Part-time employees are required to pay a percentage of the State’s portion of the contribution inaddition to the member contribution. Special rules apply for non-IRS dependents (see theBenefits website for more information).
BlueAdvantage HMO (Code: CI) $ 96 $132 $ 75 $110Coventry HMO (Code: AS) $111 $156 $ 88 $130Coventry OAP (Code: CH) $111 $156 $ 88 $130Health Alliance HMO (Code: AH) $113 $159 $ 89 $133HealthLink OAP (Code: CF) $126 $179 $102 $149HMO Illinois (Code: BY) $100 $139 $ 79 $116Quality Care Health Plan (Code: D3) $249 $287 $142 $203
Health Plan Name and Code
OneDependent
Two or moreDependents
OneMedicareA and BPrimary
Dependent
Two or moreMedicareA and BPrimary
Dependents
Full-time Employee Monthly Health Plan Contributions*
Dependent Monthly Health Plan Contributions*
www.benefitschoice.il.gov 7
Member Only $11.00 Member plus 1 Dependent $17.00 Member plus
2 or more Dependents $19.50
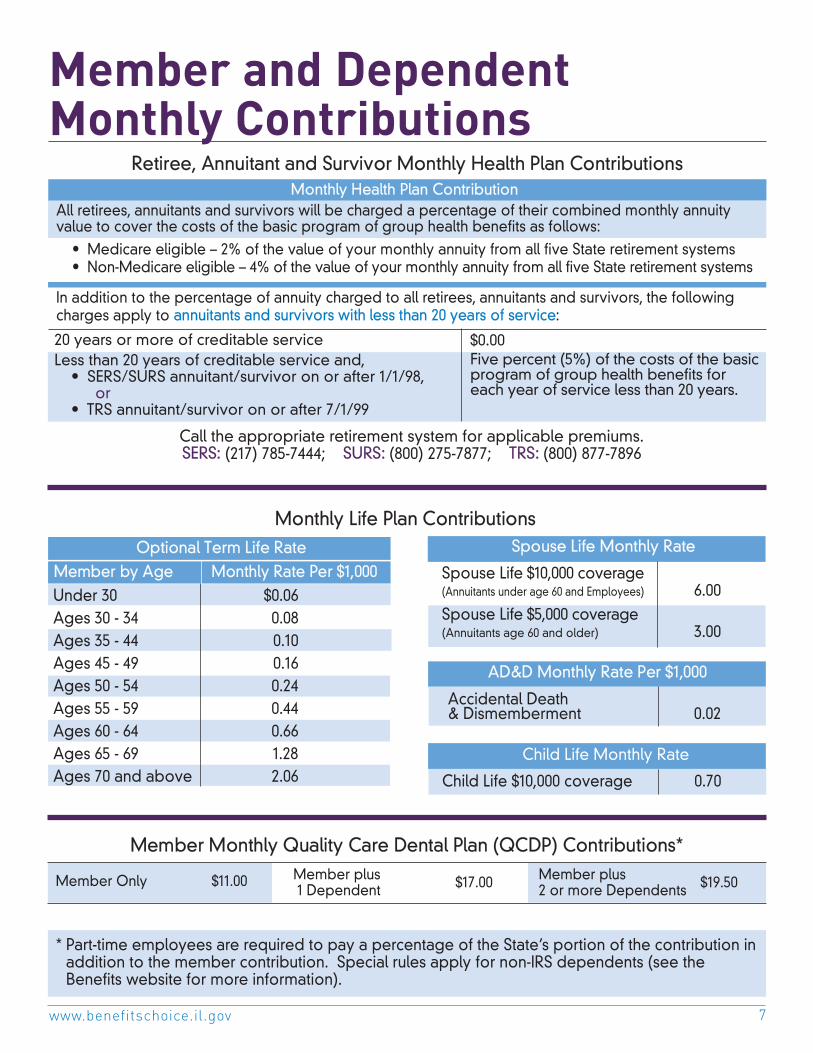
Member and Dependent Monthly Contributions
Call the appropriate retirement system for applicable premiums.SERS: (217) 785-7444; SURS: (800) 275-7877; TRS: (800) 877-7896
Under 30 $0.06Ages 30 - 34 0.08Ages 35 - 44 0.10Ages 45 - 49 0.16Ages 50 - 54 0.24Ages 55 - 59 0.44Ages 60 - 64 0.66Ages 65 - 69 1.28 Ages 70 and above 2.06
Spouse Life Monthly Rate
Spouse Life $10,000 coverage(Annuitants under age 60 and Employees) 6.00Spouse Life $5,000 coverage(Annuitants age 60 and older) 3.00
Monthly Life Plan Contributions
Member by Age Monthly Rate Per $1,000
Accidental Death& Dismemberment 0.02
AD&D Monthly Rate Per $1,000
Child Life Monthly Rate
Child Life $10,000 coverage 0.70
* Part-time employees are required to pay a percentage of the State’s portion of the contribution inaddition to the member contribution. Special rules apply for non-IRS dependents (see theBenefits website for more information).
20 years or more of creditable serviceLess than 20 years of creditable service and,
• SERS/SURS annuitant/survivor on or after 1/1/98,or
• TRS annuitant/survivor on or after 7/1/99
$0.00Five percent (5%) of the costs of the basicprogram of group health benefits foreach year of service less than 20 years.
Monthly Health Plan ContributionAll retirees, annuitants and survivors will be charged a percentage of their combined monthly annuityvalue to cover the costs of the basic program of group health benefits as follows:
• Medicare eligible – 2% of the value of your monthly annuity from all five State retirement systems• Non-Medicare eligible – 4% of the value of your monthly annuity from all five State retirement systems
In addition to the percentage of annuity charged to all retirees, annuitants and survivors, the followingcharges apply to annuitants and survivors with less than 20 years of service:
Member Monthly Quality Care Dental Plan (QCDP) Contributions*
Retiree, Annuitant and Survivor Monthly Health Plan Contributions
Optional Term Life Rate

FY2015 Benefit Choice Options8
Health PlanThe State of Illinois offers its employees,annuitants and survivors health benefits throughthe State Employees Group Insurance Program(medical, prescription and behavioral health).Vision coverage is included at no additionalcost when enrolled in the health coverage.With limited exceptions, the State makesmonthly contributions toward your healthpremiums. Active employees, annuitants andsurvivors should refer to pages 6-7 for themonthly contribution amounts.
As an employee, annuitant or survivor of theState, you are offered various health insurancecoverage options:
F Quality Care Health Plan (QCHP)
F Managed Care Plans (two types)
• Health Maintenance Organizations (HMOs)• Open Access Plans (OAPs)
The health insurance options differ in the benefitlevels they provide, the doctors and hospitalsyou can access and the cost to you. See theBenefits Comparison charts on pages 14-16 forinformation to help you determine which plan isright for you.
Opting Out of Coverage*: Full-timeemployees, retirees, annuitants and survivorshave the option of opting out of healthcoverage if they have other comprehensivehealth coverage provided by an entity otherthan the Department of Central ManagementServices. Full-time employees who do nothave other comprehensive health coveragemust remain enrolled in the State’s health plan.
Full-time employees who elect to opt out willhave their health, dental, vision, behavioralhealth and prescription coverage terminated.Annuitants and survivors who opt out will haveall coverage terminated, except dental and lifeinsurance. Annuitants and survivors who donot want the dental coverage may only cancelthe coverage during a Benefit Choice Period.See page 9 for more information regardingopting out.
Waiving Coverage*: Part-time employees,retirees, annuitants and survivors, have theoption to waive all coverage which willterminate health, dental, vision, behavioralhealth and prescription coverage. Memberselecting to waive coverage do not need toprovide proof of other coverage.
If you change health plans during the BenefitChoice Period, or re-elect health coverage afteropting out or waiving coverage, your newhealth insurance ID cards will be mailed to youdirectly from your health insurance carrier, notfrom the Department of Central ManagementServices. If you need to have services but havenot yet received your ID cards, contact yourhealth insurance carrier.
Except for annuitants and survivors who becomeenrolled in Medicare Parts A and B prior toSeptember 30, 2014, members who select ahealth plan during the Benefit Choice Period willremain in that plan the entire plan year unlessthey experience a qualifying change in statusthat allows them to change plans.
* Members who must pay an amount in addition to thecontribution required of all members may waivecoverage. Members who are responsible for themember monthly contribution only must opt out ofcoverage which will require proof of other coverage.
Total Retiree Advantage Illinois (TRAIL)Medicare Advantage Program
Annuitants and survivors who become enrolledin Medicare Parts A and B and meet all thecriteria for enrollment in the MedicareAdvantage Program will be notified of theTRAIL Enrollment Period by the Department ofCentral Management Services. These memberswill be required to choose a MedicareAdvantage plan or opt out of all Statecoverage (which includes health, behavioralhealth, prescription and vision coverage) in thefall with an effective date of January 1, 2015. Formore information regarding the MedicareAdvantage ‘TRAIL’ Program, go to:
www.cms.illinois.gov/thetrail

www.benefitschoice.il.gov 9
Opt OutIn accordance with Public Act 92-0600, full-timeemployees, retirees, annuitants and survivors mayelect to Opt Out of the State Employees HealthInsurance Program if proof of other major medicalinsurance by an entity other than the Departmentof Central Management Services is provided.This election will terminate health, prescription,behavioral health, dental (see note below) andvision coverage for the member and anyenrolled dependents.
Note: Annuitants and survivors will remainenrolled in the dental coverage unless they electto cancel the coverage during the annual openenrollment period.
Members opting out of the Program continue tobe enrolled with the same Basic and OptionalLife insurance coverage, if applicable.
If you opt out of the Program you will not beeligible for the:
– Free influenza immunizations offeredannually
– COBRA continuation of coverage– Smoking Cessation Benefit– Weight-Loss Benefit
However, if you are an employee, you will stillbe eligible for the:
– Flexible Spending Account (FSA) Program– Commuter Savings Program (CSP)– Paid maternity/paternity benefit, if eligible– Employee Assistance Program – Adoption Benefit Program
Opt Out With Financial IncentiveSERS, JRS, GARS, SURS and TRS Annuitants noteligible for Medicare
In accordance with Public Act 98-0019, membersnot eligible for Medicare receiving a retirementannuity from any of the five state retirementsystems who are enrolled in the StateEmployees Health Insurance Program and haveother comprehensive medical coverage mayelect to OPT OUT of the health insuranceprogram and receive a financial incentive.Opting out includes health, dental, vision,
prescription and behavioral health coverage forthe annuitant and any dependents. Make sureto mark the 'Opt Out with Financial Incentive'box on the Benefit Choice Election Form if youare interested in this option. The retirementsystem responsible for your group insuranceenrollment will send you additional forms tocomplete that are required for this election.Members with less than 20 years of creditableservice are eligible for a $150/month financialincentive; members with 20 years or more ofcreditable service are eligible for a $500/monthfinancial incentive. Note: Annuitants whoretired under TRS cannot count the time workedfor a public school district in their creditableservice time for financial incentive purposes.
Annuitant Waiver Public Act 93-553 allows annuitants who arecurrently enrolled as a dependent of theirState-covered spouse to remain a dependentand waive coverage in their own right, therebydecreasing the cost of coverage for anannuitant with less than 20 years of service.
New annuitants who have been enrolled for ayear or more as a dependent and wish toremain enrolled as a dependent oncebecoming an annuitant must indicate on theParticipation Election Form (provided by theretirement system) their desire to waive health,dental and vision coverage as an annuitant. Theannuitant’s spouse cannot carry Spouse Life onthe annuitant; however, the annuitant will haveBasic Life coverage and may apply foradditional Optional Life coverage, if eligible.
Re-enrolling in the Health PlanIndividuals who opt out or waive under any ofthese Public Acts may re-enroll in the Programonly during an annual open enrollment period orwithin 60 days of experiencing an eligiblequalifying change in status. Any outstandingpremiums must be paid before you will beallowed to re-enroll. Note: Survivors andannuitants are not eligible to re-enroll if previouslyterminated for nonpayment of premium.
Opt Out and Annuitant Waiver

FY2015 Benefit Choice Options10
QCHP is the medical plan that offers acomprehensive range of benefits. Under theQCHP, plan participants can choose anyphysician or hospital for medical services;however, plan participants receive enhancedbenefits, resulting in lower out-of-pocket costs,when receiving services from a QCHP networkprovider. Plan participants can access planbenefit and participating QCHP networkinformation, explanation of benefits (EOB)statements and other valuable healthinformation online.
The QCHP has a nationwide network thatconsists of physicians, hospitals and ancillaryproviders. Notification to Cigna is required forcertain medical services in order to avoidpenalties. Contact Cigna at (800) 962-0051 fordirection.
QCHP utilizes Magellan for behavioral healthbenefits and Express Scripts for prescriptionbenefits. Effective July 1, 2014, the prescriptiondeductible that applies to each plan participantwill be $125.
Health Plan DescriptionsThere are several health plans available basedon geographic location. All plans offercomprehensive benefit coverage. Healthmaintenance organizations (HMOs) havelimitations including geographic availability anddefined provider networks, whereas the twoopen access plans (OAPs) and the Quality CareHealth Plan (QCHP) have nationwide networksof providers available to their members.
All health plans require a determination ofmedical appropriateness prior to specializedservices being rendered. HMO plans requirethe member to obtain a copy of the authorized
referral prior to services being rendered. ForQCHP and OAPs, it is the member’sresponsibility to confirm authorization ofmedical services has been obtained by thehealth plan provider to avoid penalties ornonpayment of services. Important note: OAPsare self-referral plans. It is the member’sresponsibility to ensure that the providerand/or facility from which they are receivingservices are in Tier I or Tier II to avoid significantout-of-pocket costs. For more detailedinformation, refer to each health plan’s summaryplan document (SPD).
• Health Maintenance Organizations (HMOs)
Members who elect an HMO plan will needto select a primary care physician (PCP) froma network of participating providers. A PCPcan be a family practice, general practice,internal medicine, pediatric or an OB/GYNphysician. The PCP will direct all healthcareservices and will make referrals forspecialists and hospitalizations. When careand services are coordinated through thePCP, only a copayment will apply. There areno annual plan deductibles for medicalservices obtained through an HMO.
The minimum level of HMO coverageprovided by all plans is described on thechart on page 14.
Please note that some HMOs provideadditional coverage, over and above theminimum requirements. Effective July 1, 2014,the prescription deductible that applies toeach plan participant will be $100.
If a member is enrolled in an HMO and theirPCP leaves the HMO plan’s network, themember has three options (must be electedwithin 60 days of the event):
– Choose another PCP within that plan;– Change to a different managed care
plan; or – Enroll in the Quality Care Health Plan.
Quality Care Health Plan (QCHP) Managed Care Plans
www.benefitschoice.il.gov 11
• Open Access Plans (OAPs)
Open access plans combine similar benefitsof an HMO with the same type of coveragebenefits as a traditional health plan.Members who elect an OAP will have threetiers of providers from which to choose toobtain services. The benefit level isdetermined by the tier in which thehealthcare provider is contracted. Membersenrolled in an OAP can mix and matchproviders and tiers.
Effective July 1, 2014, the prescriptiondeductible that applies to each plan participantwill be $100, regardless of the tier used.
F Tier I offers a managed care networkwhich provide enhanced benefits andrequire copayments which mirror HMOcopayments.
F Tier II offers another managed carenetwork, in addition to the managed carenetwork offered in Tier I, and alsoprovides enhanced benefits. Tier IIrequires copayments, coinsurance and issubject to an annual plan year deductible.
F Tier III covers all providers which are not inthe managed care network of Tiers I or II(i.e., out of network providers). Using TierIII can offer members flexibility in selectinghealthcare providers, but involve higherout-of pocket costs. Tier III has a higherplan year deductible and has a highercoinsurance amount than Tier II services.In addition, certain services, such aspreventive/wellness care, are not coveredwhen obtained under Tier III. Furthermore,plan participants who use out-of-networkproviders will be responsible for anyamount that is over and above thecharges allowed by the plan for services(i.e., allowable charges), which couldresult in much higher out-of-pocket costs.When using out-of-network providers, it isrecommended that the participant obtaina preauthorization of benefits to ensurethat medical services/stays will meetmedical necessity criteria and be eligiblefor benefit coverage.
Members who use providers in Tiers II and III willbe responsible for the plan year deductible. Inaccordance with the Affordable Care Act,beginning July 1, 2014, these deductibles willaccumulate separately from each other and willnot ‘cross accumulate.' This means thatamounts paid toward the deductible in one tierwill not apply toward the deductible in theother tier.
Specific benefits are described on the chart onpage 15 and may also be found in the summaryplan document (SPD) on the OAP administrator’swebsite.
Health Plan Descriptions (cont.)
Managed Care Plans

FY2015 Benefit Choice Options12
Out-of-Pocket MaximumAfter the out-of-pocket maximum has beensatisfied, the plan will pay 100% of coveredexpenses* up to the allowable charge for theremainder of the plan year. Charges that applytoward the out-of-pocket maximum for each typeof plan varies and are outlined in the chart below.
Certain charges are always the member’sresponsibility and do not count toward the out-of-pocket maximum, nor are they covered after theout-of-pocket maximum has been met. Chargesthat do not count toward the out-of-pocketmaximum include:
• Amounts over allowable charges for the plan;
• Noncovered services;
• Charges for services deemed to be notmedically necessary;
• Penalties for failing to precertify/providenotification; and
• Prescription deductibles and copayments*
* Effective July 1, 2014, prescription deductibles andcopayments paid by Coventry HMO members andHealth Alliance HMO members will apply toward theout-of-pocket maximum; therefore, once the out-of-pocket maximum has been met, charges forprescription medications will be covered at 100% forthe remainder of the plan year.
The following are the types of charges that applyto the out-of-pocket maximum by plan type:
• Quality Care Health Plan: The types of chargesthat apply toward the out-of-pocket maximum forQCHP include the annual plan year deductible,QCHP additional deductibles and coinsurance.
• HMO Plans: HMO plans apply medicalcopayments and coinsurance paid fordurable medical equipment toward the out-of-pocket maximum*.
• OAP Plans: Beginning July 1, 2014, the manner inwhich the OAP out-of-pocket maximums arecalculated will change. Eligible charges fromTiers I and II will be added together whencalculating the out-of-pocket maximum. Thecharges that will count toward this out-of-pocketmaximum will include copayments andcoinsurance from Tier I and Tier II providers,and the annual plan year deductible from Tier II.
Tier III will no longer have an out-of-pocketmaximum.
PLAN
QCHP
HMO
OAP Tier I
OAP Tier II
Out-of-PocketMaximum Limits
In-NetworkIndividual $1,500Family $3,750Out-of-NetworkIndividual $6,000Family $12,000
Individual $3,000Family $6,000
Individual $6,250Family $12,750
Annual Plan Year
Deductible
X
N/A**
N/A
X
AdditionalDeductibles
(QCHP)/Copayments
X
X
X
X
Coinsurance
X
X
X
X
Amounts over Allowable Charges(QCHP out-of-network
providers andOAP Tier III providers)
Amounts over the plan’s allowable charges are the
member’s responsibility and do not go toward the
out-of-pocket maximum.
Charges That Apply Towards Out-Of-Pocket Maximum
Note: Effective July 1, 2014, eligible charges that the member pays toward the annual plan deductible (i.e., Tier II),copayments and/or coinsurance for OAP Tiers I and II will be added together for the out-of-pocket maximumcalculation. OAP Tier III does not have an out-of-pocket maximum.
** Beginning July 1, 2014, Coventry HMO and Health Alliance HMO will apply the annual prescription deductible towardthe out-of-pocket maximum.

www.benefitschoice.il.gov 13
Map of Health Plans by Illinois County
Refer to the code key belowfor the health plan code foreach plan by county.
Jo Daviess Stephenson Winnebago Boone Mc Henry Lake
CarrollOgle
De KalbKane
CookDu PageWhiteside Lee
Kendall
Rock Island Henry Bureau
Putnam
La SalleGrundy
Will
Kankakee
Livingston
Mercer
Henderson
Warren KnoxStark
Marshall
Hancock Mc Donough Fulton
Peoria Woodford
Tazewell McLean Ford
Iroquois
Adams
Schuyler
Brown Cass MenardLogan De Witt
Piatt
Champaign Vermilion
EdgarDouglas
Moultrie
Macon
Christian
SangamonMorganScottPike
Calhoun
GreeneMacoupin
Jersey
MontgomeryShelby
Coles
ClarkCumberland
MadisonBond
Fayette Effingham Jasper Crawford
St. ClairClinton Marion
Clay Richland Lawrence
Monroe
Randolph Perry
Washington Jefferson
Wayne
Edwards
Wabash
Jackson
FranklinHamilton White
Williamson Saline Gallatin
Union Johnson Pope Hardin
Alexander
Pulaski Massac
Mason
July 1, 2014 through June 30, 2015
BlueAdvantage HMO . . . CI Coventry HMO . . . . . . . . ASCoventry OAP. . . . . . . . . CHHealth Alliance HMO . . . AHHealthLink OAP . . . . . . . . CFHMO Illinois . . . . . . . . . . . BYQuality Care Health
Plan (QCHP) . . . . . D3
AH, AS, BY, CF, CH, CI, D3
BY, CF, CH, CI, D3
AH, AS, CF, CH, D3
AH, AS, CF, CH, CI, D3
AH, AS, BY, CI, CH, CF, D3
Striped areas represent counties in whichHMO Illinois or BlueAdvantage HMO do not have provider coverage; membersin these counties may have access to HMO Illinois or BlueAdvantage HMOproviders in a neighboring county.

FY2015 Benefit Choice Options14
HMO Plan Design
Plan year maximum benefit UnlimitedLifetime maximum benefit Unlimited
Hospital Services
Inpatient hospitalization 100% after $350 copayment per admissionAlcohol and substance abuse 100% after $350 copayment per admissionPsychiatric admission 100% after $350 copayment per admissionOutpatient surgery 100% after $250 copaymentDiagnostic lab and x-ray 100%Emergency room hospital services 100% after $250 copayment per visit
Professional and Other Services(Copayment not required for preventive services)
Physician Office visit 100% after $20 copayment per visitPreventive Services, including immunizations 100%Specialist Office visit 100% after $30 copayment per visitWell Baby Care (first year of life) 100%Outpatient Psychiatric and Substance Abuse 100% after $20 or $30 copayment per visitPrescription drugs $8 copayment for generic($100 deductible applies; formulary $26 copayment for preferred brandis subject to change during plan year) $50 copayment for nonpreferred brandDurable Medical Equipment 80% Home Health Care $30 copayment per visit
The HMO coverage described below representsthe minimum level of coverage an HMO isrequired to provide. Benefits are outlined ineach plan’s summary plan document (SPD). It isthe member’s responsibility to know and follow
the specific requirements of the HMO planselected. Contact the plan for a copy of theSPD. A $100 prescription deductible applies toeach plan participant (see page 21 for details).
Some HMOs may have benefit limitations based on a calendar year.
HMO Benefits

www.benefitschoice.il.gov 15
The benefits described below represent theminimum level of coverage available in an OAP.Benefits are outlined in the plan’s summary plandocument (SPD). It is the member’s responsibility
to know and follow the specific requirements ofthe OAP plan. Contact the plan for a copy of theSPD . A $100 prescription deductible applies toeach plan participant (see page 21 for details).
Benefit Tier I Tier II Tier III (Out-of-Network)100% Benefit 90% Benefit 60% Benefit
Plan Year Maximum Benefit Unlimited Unlimited UnlimitedLifetime Maximum Benefit Unlimited Unlimited UnlimitedAnnual Out-of-Pocket MaxPer Individual Enrollee $6,250 (includes eligible charges from Tier I and Tier II combined) Not ApplicablePer Family $12,750 (includes eligible charges from Tier I and Tier II combined)Annual Plan Deductible
$0 $250 per enrollee* $350 per enrollee*(must be satisfied for allservices)
Hospital Services
Inpatient 100% after $350 copayment 90% of network charges 60% of allowable charges after per admission after $400 copayment $500 copayment per admission
per admissionInpatient Psychiatric 100% after $350 copayment 90% of network charges 60% of allowable charges after
per admission after $400 copayment $500 copayment per admissionper admission
Inpatient Alcohol and 100% after $350 copayment 90% of network charges 60% of allowable charges after Substance Abuse per admission after $400 copayment $500 copayment per admission
per admissionEmergency Room 100% after $250 copayment 100% after $250 copayment 100% after $250 copayment
per visit per visit per visitOutpatient Surgery 100% after $250 copayment 90% of network charges 60% of allowable charges after
per visit after $250 copayment $250 copaymentDiagnostic Lab and X-ray 100% 90% of network charges 60% of allowable charges
Physician and Other Professional Services(Copayment not required for preventive services)
Physician Office Visits 100% after $20 copayment 90% of network charges 60% of allowable charges Specialist Office Visits 100% after $30 copayment 90% of network charges 60% of allowable charges Preventive Services, 100% 100% Covered under Tier I andincluding immunizations Tier II onlyWell Baby Care 100% 100% Covered under Tier I and(first year of life) Tier II onlyOutpatient Psychiatric 100% after $20 or $30 90% of network charges 60% of allowable chargesand Substance Abuse copayment
Other ServicesPrescription Drugs – Covered through State of Illinois administered plan, Express Scripts; $100 deductible applies
Generic $8 Preferred Brand $26 Nonpreferred Brand $50 Durable Medical Equipment 80% of network charges 80% of network charges 60% of allowable charges Skilled Nursing Facility 100% 90% of network charges Covered under Tier I and
Tier II onlyTransplant Coverage 100% 90% of network charges Covered under Tier I and
Tier II onlyHome Health Care 100% after $30 copayment 90% of network charges Covered under Tier I and
Tier II only
Open Access Plan (OAP) Benefits
* An annual plan deductible must be met before Tier II and Tier III plan benefits apply. Benefit limits are measured on a planyear. Amounts over the plan’s allowable charges do not count toward the out-of-pocket maximum.
FY2015 Benefit Choice Options16
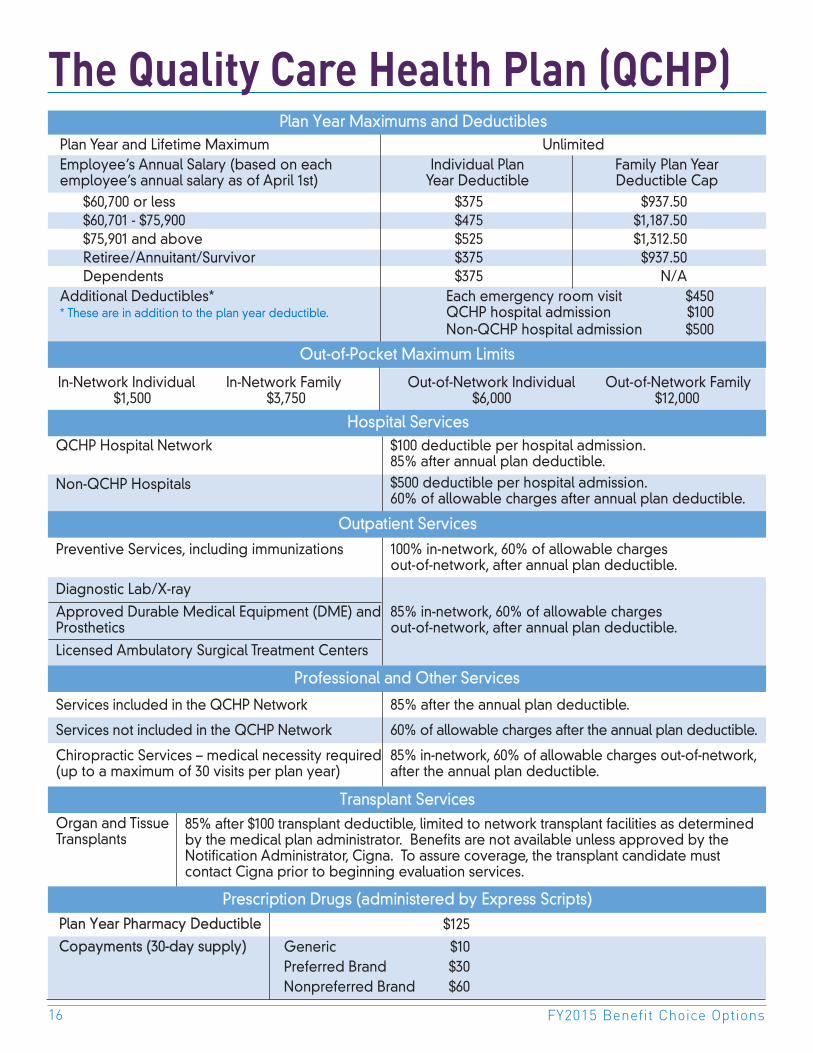
The Quality Care Health Plan (QCHP)
Plan Year Pharmacy Deductible $125
Copayments (30-day supply) Generic $10Preferred Brand $30Nonpreferred Brand $60
Plan Year Maximums and DeductiblesPlan Year and Lifetime Maximum UnlimitedEmployee’s Annual Salary (based on each Individual Plan Family Plan Yearemployee’s annual salary as of April 1st) Year Deductible Deductible Cap
$60,700 or less $375 $937.50$60,701 - $75,900 $475 $1,187.50$75,901 and above $525 $1,312.50Retiree/Annuitant/Survivor $375 $937.50Dependents $375 N/A
Additional Deductibles* Each emergency room visit $450* These are in addition to the plan year deductible. QCHP hospital admission $100
Non-QCHP hospital admission $500
QCHP Hospital Network
Non-QCHP Hospitals
Preventive Services, including immunizations
Diagnostic Lab/X-ray
Approved Durable Medical Equipment (DME) andProsthetics
Licensed Ambulatory Surgical Treatment Centers
Services included in the QCHP Network
Services not included in the QCHP Network
Chiropractic Services – medical necessity required(up to a maximum of 30 visits per plan year)
Organ and TissueTransplants
$100 deductible per hospital admission.85% after annual plan deductible.$500 deductible per hospital admission.60% of allowable charges after annual plan deductible.
100% in-network, 60% of allowable chargesout-of-network, after annual plan deductible.
85% in-network, 60% of allowable chargesout-of-network, after annual plan deductible.
85% after the annual plan deductible.
60% of allowable charges after the annual plan deductible.
85% in-network, 60% of allowable charges out-of-network,after the annual plan deductible.
Prescription Drugs (administered by Express Scripts)
Out-of-Pocket Maximum Limits
85% after $100 transplant deductible, limited to network transplant facilities as determinedby the medical plan administrator. Benefits are not available unless approved by theNotification Administrator, Cigna. To assure coverage, the transplant candidate mustcontact Cigna prior to beginning evaluation services.
Professional and Other Services
Transplant Services
Outpatient Services
Hospital Services
In-Network Individual In-Network Family Out-of-Network Individual Out-of-Network Family$1,500 $3,750 $6,000 $12,000

www.benefitschoice.il.gov 17
Federally Required NoticesNotice of Creditable CoveragePrescription Drug Information for State of IllinoisMedicare Eligible Plan Participants
This Notice confirms that the State of IllinoisGroup Insurance Program has determined thatthe prescription drug coverage it provides iscreditable. This means that your existingprescription coverage is on average as goodas or better than the standard Medicareprescription drug coverage (Medicare Part D).You can keep your existing group prescriptioncoverage and choose not to enroll in aMedicare Part D plan. Unless you qualify forlow-income/extra-help assistance, you shouldnot enroll in a Medicare Part D plan.
With this Notice of Creditable Coverage, youwill not be penalized if you later decide toenroll in a Medicare prescription drug plan.However, you must remember that if you dropyour entire group coverage through the StateEmployees Group Insurance Program andexperience a continuous period of 63 days orlonger without creditable coverage, you maybe penalized if you enroll in a Medicare Part Dplan later. If you choose to drop your StateEmployees Group Insurance coverage, theMedicare Special Enrollment Period forenrollment into a Medicare Part D plan is twomonths after the loss of creditable coverage.
If you keep your existing group coverage, it isnot necessary to join a Medicare prescriptiondrug plan this year. Plan participants whodecide to enroll into a Medicare prescriptiondrug plan; however, may need a personalizedNotice of Creditable Coverage in order toenroll into a prescription plan without a financialpenalty. Participants who need a personalizedNotice may contact the State of IllinoisMedicare Coordination of Benefits Unit at(800) 442-1300 or (217) 782-7007.
Summary of Benefits andCoverage (SBC) and UniformGlossaryUnder the Affordable Care Act, health insuranceissuers and group health plans are required toprovide you with an easy-to-understandsummary about a health plan’s benefits andcoverage. The regulation is designed to helpyou better understand and evaluate your healthinsurance choices.
The forms include a short, plain languageSummary of Benefits and Coverage (SBC) anda uniform glossary of terms commonly used inhealth insurance coverage, such as"deductible" and "copayment.”
All insurance companies and group healthplans must use the same standard SBC form tohelp you compare health plans. The SBC formalso includes details, called “coverageexamples,” which are comparison tools thatallow you to see what the plan would generallycover in two common medical situations. Youhave the right to receive the SBC whenshopping for, or enrolling in, coverage or if yourequest a copy from your issuer or grouphealth plan. You may also request a copy ofthe glossary of terms from your healthinsurance company or group health plan. AllState health plan SBC’s are available on theBenefits website.
Notice of Privacy PracticesThe Notice of Privacy Practices were updatedon the Benefits website effective April 1, 2013.You have a right to obtain a paper copy of thisNotice, even if you originally obtained theNotice electronically. We are required to abidewith terms of the Notice currently in effect;however, we may change this Notice. If wematerially change this Notice, we will post therevised Notice on our website atwww.benefitschoice.il.gov.

FY2015 Benefit Choice Options18
What is Medicare? Medicare is a federal health insurance programfor the following:
• Participants age 65 or older• Participants under age 65 with certain
disabilities• Participants of any age with End-Stage
Renal Disease (ESRD)
Medicare has the following parts to help coverspecific services:
• Medicare Part A (Hospital Insurance): Part Acoverage is premium-free for participantswith enough earned credits based on theirown work history or that of a spouse atleast 62 years of age (when applicable) asdetermined by the Social SecurityAdministration (SSA).
• Medicare Part B (Outpatient and MedicalInsurance): Part B coverage requires amonthly premium contribution. With limitedexception, enrollment is required formembers who are retired or who have lost“current employment status” and areeligible for Medicare.
• Medicare Part C (also known as MedicareAdvantage): Part C is insurance that helpspay for a combination of the coverageprovided in Medicare Parts A, B and D (ifthe plan covers prescription drugs). Anindividual must already be enrolled inMedicare Parts A and B in order to enrollinto a Medicare Part C plan. Medicare PartC requires a monthly premium contribution.
• Medicare Part D (Prescription DrugInsurance): Medicare Part D coveragerequires a monthly premium contribution,unless the participant qualifies for extra-helpassistance as determined by the SSA.
In order to apply for Medicare benefits, planparticipants are instructed to contact their localSSA office or call (800) 772-1213. Planparticipants may also contact the SSA via theinternet at www.socialsecurity.gov to sign upfor Medicare Part A.
State of Illinois MedicareRequirementsEach plan participant must contact the SSA andapply for Medicare benefits upon turning theage of 65. If the SSA determines that a planparticipant is eligible for Medicare Part A at apremium-free rate, the State requires that theplan participant accept the Medicare Part Acoverage.
If the SSA determines that a plan participant isnot eligible for premium-free Medicare Part Abased on his/her own work history or the workhistory of a spouse at least 62 years of age(when applicable), the plan participant mustrequest a written statement of the Medicareineligibility from the SSA. Upon receipt, thewritten statement must be forwarded to theState of Illinois Medicare COB Unit to avoid afinancial penalty. Plan participants who areineligible for premium-free Medicare Part Abenefits, as determined by the SSA, are notrequired to enroll into Medicare Parts A or B.
To ensure that healthcare benefits arecoordinated appropriately and to preventfinancial liabilities with healthcare claims, planparticipants must notify the State of IllinoisMedicare COB Unit when they become eligiblefor Medicare and submit a copy of his or herMedicare identification card to the State ofIllinois Medicare COB Unit. The Medicare COBUnit can be reached by calling (800) 442-1300 or(217) 782-7007.
Plan Participants (Members and Dependents)
Eligible for Medicare

www.benefitschoice.il.gov 19
Plan Participants Eligible for Medicare (cont.)
Members with CurrentEmployment StatusMembers (as well as his or her applicabledependents) who are actively working thatbecome eligible for Medicare due to turning age65 or due to a disability (under the age of 65)must accept the premium-free Medicare Part Acoverage, but may delay the purchase ofMedicare Part B coverage. The State of IllinoisGroup Insurance Program will remain the primaryinsurance until the date the member retires orloses “current employment status” (such as nolonger working due to a disability-related leaveof absence). Upon such an event, Medicare PartB is required by the State.
Civil union partner dependents who areeligible for premium-free Medicare Part A uponturning the age of 65 are required by the Stateto enroll in Medicare Part B. Once enrolled,Medicare will be the primary payer for thepartner’s coverage regardless of the member’scurrent employment status.
Members without CurrentEmployment StatusMembers (as well as his or her applicabledependents) who are retired or who have lostcurrent employment status (such as no longerworking due to a disability related leave ofabsence) that are eligible for Medicare due toturning age 65 or due to a disability (under theage of 65) are required to enroll in the MedicareProgram. In most cases, Medicare is theprimary payer for health insurance claims overthe State of Illinois Group Insurance Program.
Failure to enroll and maintain enrollment inMedicare Parts A and B when Medicare is theprimary payer will result in a reduction ofbenefits under the State of Illinois GroupInsurance Program and will result in additionalout-of-pocket expenditures for health-relatedclaims.
Plan Participants Eligible forMedicare on the Basis ofEnd-Stage Renal Disease (ESRD)Plan participants of any age who are eligible forMedicare benefits based on End-Stage RenalDisease (ESRD) must contact the State of IllinoisMedicare COB Unit for information regardingMedicare requirements and to ensure propercalculation of the 30-month coordination ofbenefit period.
Plan Participants with Additional InsurancePlan participants that are actively working (orretired) with additional insurance (other thanwhat is provided through the State of IllinoisGroup Insurance Program) must submit a copyof their insurance identification card along withthe effective date of coverage to the State ofIllinois Medicare COB Unit in order to ensurethe proper coordination of benefits forhealthcare claims.
Plan participants can contact the State of IllinoisMedicare COB Unit concerning any questionsvia phone at (800) 442-1300 or (217) 782-7007.
Total Retiree Advantage Illinois (TRAIL)Medicare Advantage Program
Annuitants and survivors (as well as their covered dependents) who become enrolled in MedicareParts A and B and meet all the criteria for enrollment in the Medicare Advantage Program will benotified of the TRAIL Enrollment Period by the Department of Central Management Services. Thesemembers will be required to choose a Medicare Advantage plan or opt out of State coverage(which includes health, behavioral health, prescription and vision coverage) in the fall with aneffective date of January 1, 2015. For more information regarding the Medicare Advantage ‘TRAIL’Program, go to: www.cms.illinois.gov/thetrail

FY2015 Benefit Choice Options20
To access website links to plan administrators, visitthe Benefits website at www.benefitschoice.il.gov.
Quality Care Health PlanMagellan Behavioral Health is the planadministrator for behavioral health servicesunder the Quality Care Health Plan (QCHP).Behavioral health services are included in anenrollee’s annual plan deductible and annualout-of-pocket maximum. Covered services forbehavioral health which meet the planadministrator’s medical necessity criteria arepaid in accordance with the benefit scheduleon page 16 for in-network and out-of-networkproviders. For authorization procedures, see theBenefits Handbook or call Magellan at(800) 513-2611. Please contact Magellan forspecific benefit information.
Managed Care PlansBehavioral health services are provided underthe managed care plans. Covered services forbehavioral health must meet the managed careplan administrator’s medical necessity criteriaand will be paid in accordance with themanaged care benefit schedules on pages14-15. Please contact the managed care plan forspecific benefit information.
Behavioral Health Services
Employee Assistance Program
There are two separate programs that providevaluable resources for support and informationduring difficult times for active employees and theirdependents: the Employee Assistance Program(EAP) and the Personal Support Program (PSP). TheEAP benefit applies to employees only and doesnot apply to annuitants.
The Employee Assistance Program (EAP) is foractive employees NOT represented by thecollective bargaining agreement between the Stateand AFSCME Council 31. These employees mustcontact the EAP administered by MagellanBehavioral Health.
The Personal Support Program (PSP) is forbargaining unit employees represented byAFSCME Council 31 and covered under the mastercontract agreement between the State of Illinoisand AFSCME. These employees must access EAPservices through the AFSCME Personal SupportProgram.
Both programs are free, voluntary and provideproblem identification, counseling and referralservices to employees and their covereddependents regardless of the health plan chosen.All calls and counseling sessions are confidential,except as required by law. No information will bedisclosed unless written permission is receivedfrom the employee. Management consultation isavailable when an employee’s personal problemsare causing a decline in work performance. Seepage 33 for website and other contact information.

www.benefitschoice.il.gov 21
Plan participants enrolled in any State healthplan have prescription drug benefits included inthe coverage. Plan participants who haveadditional prescription drug coverage,including Medicare, should contact their plan’sprescription benefit manager (PBM) forcoordination of benefits (COB) information.Copayments and a prescription deductibleapply to each plan participant each plan yearfor all health plans. Please note that when apharmacy dispenses a brand drug for anyreason and a generic is available, the planparticipant must pay the cost differencebetween the brand product and the genericproduct, plus the generic copayment.
To compare formulary lists, cost-savingsprograms and to obtain a list of pharmacies thatparticipate in the various health plan networks,plan participants should visit the website ofeach health plan they are considering.
Fully-insured managed care plans (i.e.,BlueAdvantage HMO, Health Alliance HMO,Coventry Health Care HMO and HMO Illinois)use a separate prescription benefit manager(PBM) to administer their prescription benefits.Members who elect one of these plans mustutilize a pharmacy participating in the plan’spharmacy network or the full retail cost of themedication will be charged. Partialreimbursement may be provided if the planparticipant files a paper claim with the health
plan. Most plans do not cover over-the-counterdrugs or drugs prescribed by medicalprofessionals (including dentists) other than theplan participant’s primary care physician (PCP).Drugs prescribed by a specialist would becovered provided that the plan participant wasreferred to the specialist by their PCP. Membersshould direct prescription benefit questions tothe respective health plan administrator.
Self-insured managed care plans (i.e.,HealthLink OAP and Coventry Health CareOAP) and the Quality Care Health Plan (QCHP)have prescription benefits administeredthrough the prescription benefit manager(PBM), Express Scripts. Prescription benefits areindependent of other medical services and arenot subject to the medical plan year deductibleor out-of-pocket maximums. In order to receivethe best value, plan participants enrolled in oneof these plans should carefully review thevarious options through which they may receivetheir medication (outlined on page 22). Mostdrugs purchased with a prescription from aphysician or a dentist are covered; however,over-the-counter drugs are not covered, even ifpurchased with a prescription. If a planparticipant elects a brand name drug and ageneric is available, the plan participant mustpay the cost difference between the brandproduct and the generic product, in addition tothe generic copayment.
Prescription Benefit
Formulary Lists: All prescription medications are compiled on a preferred formulary list (i.e., drug list)maintained by each health plan's PBM. Formulary lists categorize drugs in three levels: generic,preferred brand and nonpreferred. Each category has a different copayment amount. Coverage forspecific prescription drugs may vary depending upon the health plan. Formulary lists are subject tochange any time during the plan year.
Certain health plans notify plan participants by mail when a prescribed medication they are currentlytaking is reclassified into a different formulary list category. If a formulary change occurs, planparticipants should consult with their physician to determine if a change in prescription is appropriate.

FY2015 Benefit Choice Options22
Nonmaintenance MedicationIn-Network Pharmacy - Retail pharmacies thatcontract with Express Scripts and accept thecopayment amount for medications arereferred to as in-network pharmacies. Planparticipants who use an in-network pharmacymust present their Express Scripts IDcard/number or they will be required to paythe full retail cost. If, for any reason, thepharmacy is not able to verify eligibility (submitclaim electronically), the plan participant mustsubmit a paper claim to Express Scripts. Themaximum supply of nonmaintenancemedication allowed at one fill is 60 days,although two copayments will be charged forany prescription that exceeds a 30-day supply.A list of in-network pharmacies, as well as claimforms, are available on the Benefits website.
Out-of-Network Pharmacy - Pharmacies that donot contract with Express Scripts are referred toas out-of-network pharmacies. In most cases,prescription drug costs will be higher when anout-of-network pharmacy is used. If amedication is purchased at an out-of-networkpharmacy, the plan participant must pay the fullretail cost at the time the medication isdispensed. Reimbursement of eligible chargesmay be obtained by submitting a paper claimand the original prescription receipt to ExpressScripts. Reimbursement will be provided at theapplicable brand or generic in-network priceminus the appropriate in-network copayment.Claim forms are available by visiting theBenefits website or the Express Scripts website.
Maintenance MedicationThe Maintenance Medication Program (MMP)was developed to provide an enhancedbenefit to plan participants who usemaintenance medications. Maintenancemedication is medication that is taken on aregular basis for conditions such as high bloodpressure and high cholesterol. To determine
whether a medication is considered amaintenance medication, contact aMaintenance Network pharmacist or contactExpress Scripts. A list of pharmaciesparticipating in the Maintenance Network isavailable at www.benefitschoice.il.gov. Whenplan participants use the Maintenance Networkfor maintenance medications, they will receivea 90-day supply of medication (equivalent to 3fills) for only two and a half copayments.
The Maintenance Network is a network of retailpharmacies that contract with Express Scripts toaccept the copayment amount for maintenancemedication. Pharmacies in this network mayalso be an in-network retail pharmacy asdescribed in the Nonmaintenance Medicationsection. If a plan participant uses an in-networkpharmacy not part of the Maintenance Network,only the first two 30-day fills (or first 60-day fill)will be covered at the regular copaymentamount. Subsequent 30-day fills will becharged double the copayment rate.
Mail Order PharmacyThe mail order pharmacy provides participantsthe opportunity to receive medications directlyat their home. Both maintenance andnonmaintenance medications may be obtainedthrough the mail order process.
To utilize the mail order pharmacy, planparticipants must submit an original prescriptionfrom the attending physician. For maintenancemedication, the prescription should be writtenfor a 90-day supply, and include up to three90-day refills, totaling one year of medication.The original prescription must be attached to acompleted mail order form and sent to theaddress indicated on the form. When planparticipants use the mail order pharmacy, theywill receive a 90-day supply of medication(equivalent to 3 fills) for only two and a halfcopayments. Order forms and refills can beobtained by contacting Express Scripts.
Self-insured Plans Prescription Benefit(QCHP, HealthLink OAP and Coventry Health Care OAP)

www.benefitschoice.il.gov 23
Self-insured Plans Prescription Benefit(QCHP, HealthLink OAP and Coventry Health Care OAP)
Special Note Regarding Medications for Nursing Home/Extended Care Facility QCHP Patients
Due to the large amounts of medication generally administered at nursing home and extended carefacilities, many of these types of facilities cannot maintain more than a 30-day supply of prescriptionsper patient.
In order to avoid being charged a double-copayment for a 30-day supply, the patient or person who isresponsible for the patient’s healthcare (such as a spouse, power of attorney or guardian) shouldsubmit a letter requesting an ‘exception’ to the double copayment for their medication. The requestshould be in the form of a letter, and must include the patient’s name, a list of all medications thepatient is taking and the dosage of each medication. The effective date of the exception is the receiptdate of the request. Requests must be submitted to the Group Insurance Division, Member ServicesUnit, 801 South 7th Street, P.O. Box 19208, Springfield, Illinois 62794-9208.
Note: Since each request is based on a specific list of medications, any newly prescribedmedication(s) must be sent as another request.
Prescription Drug Step TherapyMembers who have their prescription benefitsadministered through QCHP or one of theself-insured open access plans whoseprescription benefit manager (PBM) is ExpressScripts, are subject to a coverage tool calledprescription drug step therapy (PDST) forspecific drugs. PDST requires the member tofirst try one or more specified drugs to treat aparticular condition before the plan will coveranother (usually more expensive) drug thattheir doctor may have prescribed. PDST isintended to reduce costs to both the member
and the plan by encouraging the use ofmedications that are less expensive but can stilltreat the member’s condition effectively.
Members who are taking a medication thatrequires step therapy will receive a letterexplaining that the plan will not cover thatparticular medication unless the alternativemedication is tried first. The letter will also havedirections on how a member’s physician mayrequest a coverage review if the physicianbelieves they should take the originalmedication without trying the alternativemedication first.
Express Scripts: (800) 899-2587Website: www.express-scripts.com≈

FY2015 Benefit Choice Options24
Dental PlanAll members and enrolled dependents have thesame dental benefits available regardless of thehealth plan selected. During the Benefit ChoicePeriod, members have the option to add or dropdental coverage. The election to add or dropdental coverage will remain in effect the entire planyear, without exception.
Dental Benefit
The Quality Care Dental Plan (QCDP) is a dental planthat offers a comprehensive range of benefitsadministered by Delta Dental of Illinois. The QCDPreimburses only those services listed on the DentalSchedule of Benefits (available on the Benefitswebsite). Listed services are reimbursed at apredetermined maximum scheduled amount. Eachplan participant is subject to an annual plandeductible for all dental services, except those listedin the Schedule of Benefits as ‘Diagnostic’ or‘Preventive’. Effective July 1, 2014, the annual planyear deductible will be $175 per participant per planyear. Once the annual deductible has been met,each plan participant is subject to a maximum annualdental benefit. Each plan participant has a maximumdental benefit of $2,500 (including orthodontia) whenservices are rendered by an in-network provider;however; participants who use an out-of-networkprovider are limited to a maximum benefit of $2,000(including orthodontia). For Example: If aparticipant’s out-of-network plan year maximum ismet, there would be no further coverage availablefor out-of-network services; however, the participantwould be allowed to utilize an in-network providerto exhaust the $500 remaining under the $2,500in-network plan year maximum.
Plan participants enrolled in the dental plan canchoose any dental provider for services; however,plan participants may pay less out-of-pocket whenthey receive services from a network dentist. Thereare two separate networks of dentists that a planparticipant may utilize for dental services in addition
to out-of-network providers: the Delta Dental PPOSM
network and the Delta Dental PremierSM network.
• Delta Dental PPOSM Network If you go to aPPO-level dentist you can maximize your dentalbenefits and minimize your out-of-pocketexpenses because these providers accept alower negotiated PPO fee (less any deductible).If the PPO fee is lower than the amount listed onthe Schedule of Benefits, the PPO dentist cannotbill you for the difference.
• Delta Dental PremierSM Network If you go to aPremier-level dentist, your out-of-pocket expensesmay also be less because Premier providersaccept the allowed Premier-level fee (less anydeductible). If the allowed fee is lower than theamount listed on the Schedule of Benefits, thePremier dentist cannot bill you for the difference.
• Out-of-Network If you go to a dentist who doesnot participate in either the PPO or Premiernetwork, you will receive benefits as provided bythe Schedule of Benefits. You will likely pay morethan you would if you went to a Delta Dentalnetwork dentist. Out-of-network dentists willcharge you for the difference between theirsubmitted fee and the amount listed on theSchedule of Benefits.
Annual Deductible forPreventive Services N/A
Annual Deductible forAll Other Covered Services
$175
Plan Year Maximum Benefit*In-Network Plan YearMaximum Benefit $2,500Out-of-Network Plan Year Maximum Benefit $2,000
Deductible and Plan Year Maximum
* Orthodontics + all other covered services = Plan Year Maximum Benefit
It is strongly recommended that plan participants obtain a pretreatment estimate for any service over $200,regardless of whether that service is to be received from an in-network or an out-of-network provider.Failure to obtain a pretreatment estimate may result in unanticipated out-of-pocket costs. A pretreatmentestimate is a review by Delta Dental of a dental provider’s proposed treatment, including diagnostic,x-ray and laboratory reports, as well as the expected charges. This treatment plan is sent to DeltaDental for verification of eligible benefits. Obtaining a pretreatment estimate to verify coverage willhelp you make decisions regarding your dental services and help you avoid unanticipatedout-of-pocket costs. Questions regarding a pretreatment estimate can be addressed by Delta Dental.

www.benefitschoice.il.gov 25
Dental Plan (cont.)
Child Orthodontia BenefitThe child orthodontia benefit is available only tochildren who begin treatment prior to the age of 19.The maximum lifetime benefit for child orthodontiais $2,000 for members utilizing an in-networkprovider. Services obtained at an out-of-networkorthodontia provider will have a lifetime maximumbenefit of $1,500. This lifetime maximum is based onthe length of treatment (see 'Length of Orthodontia
Treatment' chart below). This lifetime maximumapplies to each plan participant regardless of thenumber of courses of treatment. Note: The annualplan year deductible must be satisfied each planyear that the plan participant is receivingorthodontia treatment unless it was previouslysatisfied for other dental services incurred duringthe plan year. This may reduce the maximumbenefit payable for orthodontia treatment.
Delta Dental: (800) 323-1743TDD/TTY: (800) 526-0844Website: http://soi.deltadentalil.com≈
Provider PaymentIf you use a Delta Dental network dentist, youwill not have to pay the dentist at the time ofservice (with the exception of applicabledeductibles, charges for noncovered services,charges over the amount listed on the Scheduleof Benefits and/or amounts over the annualmaximum benefit). Network dentists willautomatically file the dental claim for theirpatients. Out-of-network dentists can elect toaccept assignment from the plan or may
require other payment terms. Participants whouse an out-of-network dentist may have to paythe entire bill at the time of service and/or filetheir own claim form depending on thepayment arrangements the plan participant haswith their dentist.
Example of PPO, Premier and Out-of-NetworkDentist Payments (this is a hypothetical exampleonly and assumes all deductibles have beenmet).
Delta Dental PPO Dentist* Delta Dental Premier Dentist* Out-of-Network DentistDentist submitted fee $1,000 Dentist submitted fee $1,000 Dentist submitted fee $1,000PPO maximum $600 Premier maximum $900 No negotiated fee n/aallowed fee allowed feeSchedule of Benefits $781 Schedule of Benefits $781 Schedule of Benefits $781amount amount amountYour Out-of-Pocket $0 Your Out-of-Pocket $119 Your Out-of-Pocket $219Cost Cost Cost
Length of Treatment Maximum Benefit0 - 36 Months In-network $2,000 Out-of-network $1,5000 - 18 Months In-network $1,820 Out-of-network $1,3640 - 12 Months In-network $1,040 Out-of-network $780
Prosthodontic Limitations (Prosthodontics include full dentures, partial dentures, implants and crowns)• Prosthodontics to replace missing teeth are
covered only for teeth that are lost while theplan participant is covered by QCDP.
• Multiple procedures are subject to limitations.Please refer to the Dental Schedule of BenefitsPRIOR to the start of any procedure to clarifycoverage limitations.
* When utilizing a PPO or Premier dentist, if the maximum allowed fee is greater than the amount listed on the Schedule ofBenefits, the network dentist can bill the member the difference between the two amounts.
Plan participants can access QCDP networkinformation, explanation of benefits (EOB)statements and other valuable information onlineby registering with Delta Dental of Illinois MemberConnection.

FY2015 Benefit Choice Options26
Vision coverage is provided at no additional costto members enrolled in any of the State-sponsoredhealth plans. All members and enrolled dependentshave the same vision coverage regardless of thehealth plan selected. Eye exams are covered onceevery 12 months from the last date the exambenefit was used. The benefit for replacementlenses is also once every plan year from the lastdate used. Standard frames are available onceevery 24 months from the last date used.Copayments are required.
Service Network Out-of-Network** Benefit FrequencyProvider Benefit Provider Benefit
Eye Exam $25 copayment $30 allowance Once every 12 months
Spectacle Lenses* $25 copayment $50 allowance for single Once every 12 months(single, bifocal and trifocal) vision lenses
$80 allowance for bifocaland trifocal lenses
Standard Frames $25 copayment $70 allowance Once every 24 months(up to $175 retailframe cost; memberresponsible for balance over $175)
Contact Lenses $120 allowance $120 allowance Once every 12 months(All contact lenses are inlieu of spectacle lenses)
* Spectacle Lenses: Plan participant pays any and all optional lens enhancement charges. Network providers may offer additional discounts on lens enhancements and multiple pair purchases.
** Out-of-network claims must be filed within one year from the date of service.
EyeMed Vision Care: (866) 723-0512TDD/TTY: (800) 526-0844Website: www.eyemedvisioncare.com/stil≈
Vision Plan

www.benefitschoice.il.gov 27
Life Insurance Plan*
Basic Life insurance is provided at no cost to annuitants andactive employees. This term life coverage is provided in anamount equal to the annual salary of active employees.The Basic Life amount for annuitants under age 60 is equalto the annual salary as of the last day of active Stateemployment. For annuitants age 60 or older, the Basic Lifeamount is $5,000. The life insurance plan offers eligiblemembers the option to purchase additional life insurance tosupplement the Basic Life insurance provided by the State.
Member Optional LifeMember Optional Life coverage is available toeligible members. Annuitants under age 60 andactive employees can elect coverage in anamount equal to 1-8 times their Basic Lifeamount; annuitants age 60 and older can elect1-4 times their Basic Life amount. Membersenrolled with Member Optional Life coverageshould review the chart on page 7 to be awareof rate variations among age groups. Ratechanges due to age go into effect the first payperiod following the member’s birthday.
The maximum benefit allowed for MemberOptional Life plus Basic Life coverage is$3,000,000.
Accidental Death &DismembermentAccidental Death and Dismemberment (AD&D)coverage is available to eligible members ineither (1) an amount equal to their Basic Lifeamount or (2) the combined amount of theirBasic and Member Optional Life, subject to atotal maximum of five times the Basic Lifeinsurance amount or $3,000,000, whichever isless.
Spouse LifeSpouse Life coverage is available in a lump sumamount of $10,000 for the spouse of annuitantsunder age 60 and active employees. SpouseLife coverage decreases to $5,000 for annuitantsage 60 and older. A corresponding premiumapplies.
Child LifeChild Life coverage is available in a lump sumamount of $10,000 for each child. The monthlycontribution for Child Life coverage applies toall dependent children regardless of thenumber of children enrolled. Eligible childreninclude:
• Children age 25 and under
• Children in the Disabled category
Statement of HealthAdding/increasing Member Optional Life, aswell as adding Spouse and/or Child Lifecoverage, is subject to prior approval by thelife insurance plan administrator, Minnesota LifeInsurance Company. Members must completeand submit a statement of health form toMinnesota Life for review.
* Deferred Annuitants and Survivors have differentlife insurance benefits. Details are provided inthe Retiree, Annuitant and Survivor BenefitsHandbook available on the Benefits website.
Minnesota Life Insurance Co.: (888) 202-5525TDD/TTY: (800) 526-0844Website: https://web1.lifebenefits.com/
lbwcm/pd/illinois≈

FY2015 Benefit Choice Options28
Medical Care Assistance Plan(MCAP)What is it? The Medical Care Assistance Plan(MCAP) is a program that allows you to set asidemoney, before taxes, from your paycheck to payfor health-related expenses not covered byinsurance. If you, or someone in your family (i.e.,spouse and/or eligible dependents) goes to thedoctor or dentist, takes medication or wearsglasses, whether you have insurance or not, MCAPmay save you money. Please note thatdependents must qualify under the InternalRevenue Code in order for their healthcareexpenses to be eligible for reimbursement. Referto the Flexible Spending Accounts ReferenceGuide on the Benefits website for IRS dependenteligibility requirements.
How much should I contribute? Contributionsdepend on your family’s medical expenses whichinclude copayments and deductibles associatedwith doctor’s visits, prescriptions, medicallynecessary orthodontia (e.g., braces), vision examsand surgeries (e.g., LASIK surgery). The maximumannual amount you may elect is $2,500. Theminimum monthly amount for which an employeemay enroll is $20; the maximum monthly amount is$208.33 ($277.77 for university employees paid over9 months).
Examples of expenses you cannot claim:
• Cosmetic services, vitamins, supplements
• Insurance premiums
• Vision warranties and service contracts
• Over-the-counter medicines and drugs are noteligible for reimbursement without a prescription
Flexible Spending Accounts (FSA) Employee Benefit Only - Does NOT Apply to AnnuitantsDuring the Benefit Choice Period, employees mayenroll in a Flexible Spending Account (FSA)Program with an effective date of July 1, 2014. Thegreat advantage is that you pay no federal taxeson your contributions. For example, if you put in$1,000 and are in a 20% federal tax bracket, yousave $200 ($1,000 x 20% = $200) over the course ofthe plan year.
FSA plan elections do not automatically carry overeach year. You must complete a new FSAenrollment form each year to participate. The firstdeduction for an FSA enrollment will be taken on apretax basis from the first paycheck issued in July.Employees should carefully review their paycheckto verify the deduction was taken correctly. If youdo not see the deduction on your paycheck stub,please contact your payroll office immediately.
No MCAP Grace Period for the FY2015 plan year –MCAP accounts will no longer have a graceperiod for which to use remaining MCAP funds(the grace period previously allowed participantsfull access to all funds remaining in their MCAPaccount after the plan year ended until September15th of the following plan year). The Grace Periodwill still apply for the FY2014 plan year and anyservices rendered through September 15, 2014 willuse any remaining FY2014 funds.
New maximum $500 MCAP carryover –Beginning with the FY2015 plan year, MCAPparticipants who have a balance in their MCAPaccount after September 30th, will have up to$500* of that account balance automaticallycarried over to their next plan year MCAPaccount. This carried-over amount would beavailable for use throughout the new plan year.
For example, a participant re-enrolls in MCAP forthe FY2015 plan year for the maximum amount of$2,500. On October 1, 2015, the balanceremaining in their MCAP account is $350;therefore, if they enroll for $2,500 for the FY2016plan year they will have a total of $2,850 in theirMCAP account to use during the FY2016 planyear. Participants must re-enroll in MCAP to beeligible for the previous plan year’s carryoveramount. Those who do not re-enroll and have abalance in their MCAP account after the run-outperiod (i.e., September 30th) will forfeit thataccount balance.
*Participants who re-enroll in MCAP and have a balanceexceeding $500 after September 30, 2015, will forfeit anyamount exceeding this limit. This carryover amount is forMCAP accounts only and does not apply to DCAP accounts.
New and Important MCAP Changes for FY2015

www.benefitschoice.il.gov 29
* In addition to child care, DCAP can be used to pay for the dependent care expenses for any individual living with you that isphysically or mentally unable to care for themselves and is eligible to be claimed as a dependent on your taxes. Refer to theInternal Revenue Code to ensure your dependent qualifies as a tax dependent before enrolling in this program.
Special Note Regarding DCAP Reimbursement for Summer Day CampsEmployees who enroll children in a summer day camp should calculate their FY2015 daycare expensesand annual contribution carefully. Since the FY2014 plan year ends June 30th, any day camp expensesincurred during June 2014 will not be eligible for reimbursement through your FY2015 DCAP. For FY2015,the summer months of July and August 2014, as well as June 2015, will be eligible for reimbursement.
Plan Administratorto be determined
How do I use my MCAP account? Employees whoare enrolled in MCAP will be issued a stored-valuedebit card at no cost to the employee. The cardmay be used to pay for medical expenses andeligible over-the-counter medical-related purchases.Documentation will be required to substantiatecertain expenses paid with the debit card; therefore,you should review your online account carefully toensure you are aware of the documentationrequirements. Employees choosing not to use thedebit card may complete and submit a paper claimform for reimbursement of eligible expenses.
What is the deadline to submit MCAP claims forreimbursement? You will have until the end of therun-out period, which is September 30, 2015, to submitclaims for expenses that were incurred from July 1,2014, through June 30, 2015; otherwise, any money leftin your account will be forfeited. Please be aware thatFY2015 MCAP accounts will not have a grace periodfor which to use funds remaining in an MCAP account(the grace period previously ran until September 15theach year, but will not apply to FY2015).
Dependent Care AssistancePlan (DCAP)The Dependent Care Assistance Plan (DCAP) is forthe reimbursement of eligible child care expenses,such as daycare.* DCAP cannot be used fordependent healthcare expenses (employeesinterested in having their dependent's health-relatedexpenses reimbursed through a pretax programshould refer to the Medical Care Assistance Plan(MCAP) on page 28). In situations where parents arelegally separated or divorced, only the custodialparent can enroll in DCAP. The custodial parent isdefined by the IRS as the person who has the childthe most nights during the calendar year. See IRSPublication 503 for more information.
What is it? The Dependent Care Assistance Plan(DCAP) is a program that allows you to set asidemoney, before taxes, from your paycheck to payprimarily for child care expenses* of dependentchildren 12 years and under. If you (and your spouse,if married), work full-time and pay for daycare, daycamp or after-school programs, then DCAP may saveyou money. Please note that if you claim thedependent care tax credit, the credit will be reduced,dollar for dollar, by the amount you contribute toDCAP. Also, depending on your household income,it might be advantageous to claim child careexpenses on your federal income tax return insteadof using DCAP. You cannot claim the expenses onyour tax return and use DCAP. Please ask your taxadviser which plan is best for you.
How much should I contribute? Contributionsdepend on household needs—think about howmuch you spend on child care every year. Will youuse daycare or a private nanny? Perhaps your childis going to nursery school or day camp this year.The maximum annual amount you may elect is$5,000. The minimum monthly amount for which anemployee may enroll is $20; the maximum monthlyamount is $416.66 ($555.54 for university employeespaid over 9 months).
Examples of expenses you cannot claim:
• Overnight camp
• Daycare provided by another dependent
• Daycare provided “off the books”
• Kindergarten tuition
• Private primary school tuition
• Before and after-school care expenses fordependents age 13 and older.
You have until September 30, 2015, to submit claimsfor services incurred from July 1, 2014, through June30, 2015; otherwise, any money left in your accountwill be forfeited. All dependent care expensesmust be incurred prior to July 1, 2015, in order to beeligible for reimbursement.

FY2015 Benefit Choice Options30
Program InitiativesDependent EligibilityVerification Audit (DEVA)The Illinois Department of Central ManagementServices has retained the services of HMSEmployer Solutions (HMS) to conduct aDependent Eligibility Verification Audit (DEVA).The audit is being conducted to ensure thatonly eligible dependents are covered underthe State Employees Group Insurance Program.All State employees with dependent coveragewho receive health insurance through the Stateare being audited. The active State employeesaudit is scheduled to be administered in FY2015.
If you are required to participate in the audit,HMS will send a letter to your home. The letterwill explain the audit process and list therequired documentation. Documentation foreach dependent must be submitted by thedeadline in the letter in order to verify theeligibility of your dependents. Carefully readthe documentation requirements as they maydiffer from the initial enrollment documents yousubmitted to enroll your dependents. Failure tosubmit the required documentation will result intermination of your unverified dependents.
If, during the dependent eligibility verificationaudit, an employee is found to be covering anineligible dependent, the employee may besubject to a financial penalty, including but notlimited to, repayment of all premiums the Statemade on behalf of the employee and/ordependent, as well as expenses incurred bythe Program.
More information concerning the audit isavailable on the Benefits website.
Disease Management ProgramsDisease Management Programs are utilized bythe Quality Care Health Plan (QCHP) planadministrator and the managed care healthplans as a way to improve the health of planparticipants. Members and dependentsidentified with certain risk factors indicatingdiabetes, cardiac health and many other chronichealth conditions will be contacted by themedical plans to participate in these programs.These highly confidential programs are basedupon certain medical criteria and provide:
• Healthcare support available 24 hours aday, 7 days a week with access to a teamof registered nurses (RNs) and otherqualified health clinicians;
• Wellness tools, such as reminders ofregular health screenings;
• Educational materials pertaining to yourhealth condition, including identification ofanticipated symptoms and ways to bettermanage these conditions;
• Valuable information and access todiscounted services from weight-lossprograms.

www.benefitschoice.il.gov 31
Get HIP (Health Improvement Program)
Be Well, Get Well, Stay WellThe State offers many valuable wellnessprograms to help keep our members healthyand help unhealthy members get healthier. Thegoal is for all State members to lead better,more satisfying lives.
Stepping Up Our Wellness Program
The State is upgrading its current wellnessprogram to provide even more assistance toyou. The focus will be on improving lifestylechoices, including eating healthier, being morephysically active, ending tobacco use,managing stress more effectively, and gettingmore sleep. The goal is to help you avoidchronic health problems (or helpstabilize/improve them, if applicable), such asdiabetes, heart disease, high blood pressureand high cholesterol.
What You Can Do Now
Even before Wellness Program improvementsstart, you can take steps to be healthier and livebetter:
‰ Step 1: Get a checkup. It is vitally importantto have a preventive health exam each year,including (as applicable based on your ageand gender) a Pap smear, prostate exam,mammogram, colonoscopy, cancerscreening and immunizations. Your healthplan covers many preventive services at nocost to you, as required under FederalHealth Care Reform laws.
‰ Step 2: Take advantage of your medicalplan’s resources. Many State-offeredmedical plans have valuable wellnessresources such as health informationlibraries, online health coaching, dedicatednurse phone lines and wellnesspublications. Visit your plan’s website tofind out what’s available to you.
‰ Step 3: Know your numbers, know yourrisks. A smart step to getting healthier andstaying that way, is to…
• …Know your numbers: Get biometricscreenings from your doctor. These aresimple and quick tests that measure yourblood pressure, pulse rate, bloodglucose (sugar), total cholesterol, bodymass index (BMI), height and weight.You can get them when you go for anannual physical.
• …Take a Health Risk Assessment (HRA):Complete a private, confidential HRA onyour medical plan’s website. It asksbasic health-related questions like, “Didyou get a flu shot?” and “Do you wear aseat belt?” There are no right or wronganswers. The information youprovide—and HRA results—is not sharedwith the State. You’ll get instant resultsafter you complete an HRA, including apersonal action plan. (Using yourbiometric screening information will giveyou the most accurate results.) Shareyour results and action plan with yourdoctor. Discuss with him/her ways youcan maintain good health or improveyour health.
HIPHealth Improvement Program

FY2015 Benefit Choice Options32
Plan AdministratorsWho to contact for information
Plan Component Administrator’s Customer Service Website AddressName and Address Phone Numbers
EyeMed
Vision PlanOut-of-Network Claims (866) 723-0512 www.eyemedvisionP.O. Box 8504 (800) 526-0844 (TDD/TTY) care.com/stil
Mason, OH45040-7111
Quality Care Delta Dental of IllinoisDental Plan Group Number 20240 (800) 323-1743 http://soi.deltadentalil.com(QCDP) P.O. Box 5402 (800) 526-0844 (TDD/TTY)
Administrator Lisle, IL 60532Minnesota Life
Life Insurance Insurance Company (888) 202-5525 https://web1.lifebenefits.com/Plan 536 Bruns Lane, Unit 3 (800) 526-0844 (TDD/TTY) lbwcm/pd/illinois
Springfield, IL 62702
Flexible SpendingAccounts (FSA) Program (to be determined) (to be determined) (to be determined)
WageWorks (855) 428-0446Commuter Savings Claims Administrator (866) 353-8058 (TDD/TTY) www.wageworks.com
Program (CSP) P.O. Box 14326 (855) 291-0625 (fax)Lexington, KY 40512
Health/Dental Plans,Medicare COB Unit, CMS Group
FSA and CSP Unit, Insurance Division (217) 782-2548Premium Collection Unit, 801 South 7th Street (800) 442-1300 www.benefitschoice.il.govLife Insurance and the P.O. Box 19208 (800) 526-0844 (TDD/TTY)Benefit Programs for Springfield, ILAdoption, Smoking 62794-9208
Cessation andWeight Loss
Health Plan Toll-Free TDD/TTY Number Website AddressAdministrators Telephone Number
BlueAdvantage HMO (800) 868-9520 (866) 876-2194 www.bcbsil.com/stateofillinoisCoventry Health Care HMO (800) 431-1211 (217) 366-5551 www.chcillinois.comCoventry Health Care OAP (800) 431-1211 (217) 366-5551 www.chcillinois.com
Health Alliance HMO (800) 851-3379 (800) 526-0844 www.healthalliance.org/state ofillinois
HealthLink OAP (800) 624-2356 (800) 624-2356 www.healthlink.com/ext. 6280 illinois_index.asp
HMO Illinois (800) 868-9520 (866) 876-2194 www.bcbsil.com/stateofillinoisQuality Care Health Plan (Cigna) (800) 962-0051 (800) 526-0844 www.cigna.com/stateofil

www.benefitschoice.il.gov 33
Plan Contact For Administrator’s Customer ServiceComponent Name and Address Contact Information
Medical service CignaQCHP information, network QCHP Group #3181456 (800) 962-0051
Medical Plan providers, claim forms, (nationwide)Administrator ID cards, claim Cigna HealthCare (800) 526-0844 (TDD/TTY)
filing/resolution and P.O. Box 182223 www.cigna.com/stateofilpredetermination of Chattanooga, TN
benefits 37422-7223
QCHP Notification prior toNotification and hospital services (800) 962-0051Medical Case Noncompliance
Cigna (nationwide)Management penalty of $800 applies
QCHP Group #3181456 (800) 526-0844 (TDD/TTY)Administrator (out-of-network only)
Express ScriptsPrescription Group Number: 1400SD3 (800) 899-2587Drug Plan Information on 1400SCH, 1400SCF (nationwide)
Administrator prescription drug Paper Claims:QCHP (1400SD3) coverage, pharmacy Express Scripts
Coventry OAP network, mail order, P.O. Box 14711 (800) 759-1089 (TDD/TTY)
(1400SCH) specialty pharmacy, Lexington, KY 40512ID cards and claim filing Mail Order Prescriptions:
www.express-scripts.comHealthLink OAP Express Scripts(1400SCF) P.O. Box 66577
St. Louis, MO 63166-6577
Notification, Magellan Behavioral HealthQCHP authorization, claim QCHP Group #3181456 (800) 513-2611
Behavioral Health forms and claim (nationwide)Administrator filing/resolution P.O. Box 2216 (800) 526-0844 (TDD/TTY)
for behavioral Maryland Heights, MO www.MagellanHealth.comhealth services 63043
Employee Magellan Behavioral (866) 659-3848Assistance Confidential assistance Health (nationwide)
Program (EAP) and assessment -For Non-AFSCME (800) 456-4006 (TDD/TTY)services represented employees- www.MagellanHealth.com
Personal Support AFSCME Council 31 (800) 647-8776Program Confidential assessment -For AFSCME (statewide)
(PSP – AFSCME and assistance services represented employees- (800) 526-0844 (TDD/TTY)EAP) www.afscme31.org
DISCLAIMERThe State of Illinois intends that the terms of this plan are legally enforceable and that the plan is maintained for the exclusivebenefit of Members. The State reserves the right to change any of the benefits, program requirements and contributionsdescribed in this Benefit Choice Options Booklet. This Booklet is intended to supplement the Benefits Handbook. If there is adiscrepancy between the Benefit Choice Options Booklet, the Benefits Handbook and state or federal law, the law will control.
Plan AdministratorsWho to contact for information

Illinois Department of Central Management ServicesBureau of Benefits
PO Box 19208Springfield, IL 62794-9208
Printed by the authority of the State of Illinois(CMS-BEN2002-02-3,000-04/14)
Printed on recycled paper