state approaches to ensuring healthy pregnancies through
TRANSCRIPT

APRIL | 2021
State Approaches to Ensuring Healthy Pregnancies Through Prenatal Care
HEALTH

iii NATIONAL CONFERENCE OF STATE LEGISLATURES
NATIONAL CONFERENCE OF STATE LEGISLATURES © 2021
The National Conference of State Legislatures is the bipartisan organization dedicated to serving the lawmakers and staffs of the nation’s 50 states, its commonwealths and territories.
NCSL provides research, technical assistance and opportunities for policymakers to exchange ideas on the most pressing state issues, and is an effective and respected advocate for the interests of the states in the American federal system. Its objectives are:
• Improve the quality and effectiveness of state legislatures.
• Promote policy innovation and communication among state legislatures.
• Ensure state legislatures a strong, cohesive voice in the federal system.
The conference operates from offices in Denver, Colorado and Washington, D.C.
State Approaches to Ensuring Healthy Pregnancies
Through Prenatal CareBY KHANH NGUYEN

1 NATIONAL CONFERENCE OF STATE LEGISLATURES
IntroductionEnsuring healthy births and a strong start for children remains a top priority for state policymakers. Healthy pregnancies are a key mechanism to promote healthy births and healthy babies. Prenatal care—the health care received during pregnancy—can prevent or minimize complications from pregnancy risks such as hypertension, anemia, infections, depression and gestational diabetes, which can lead to preterm birth, low birth weight babies, malnutrition and even death. Babies of mothers who do not get prenatal care are three times more likely to be low birth weight and five times more likely to die.
In addition to the human and societal cost, the economic cost of pregnancy compli-cations can be significant. For example, preterm births cost an estimated $25 billion a year—or roughly $65,000 per preterm birth. Disparities also exist in prenatal care initiation, quality and access across different populations, such as by race, geography or education. This brief provides an overview of factors influencing prenatal care ac-cess and utilization, recommended models of care, and state-level solutions and pol-icy options.
NATIONAL CONFERENCE OF STATE LEGISLATURES iv
Preterm birth is when a baby is born too early, before 37 weeks of pregnancy have been completed.
Low birth weight refers to babies born weighing less than 5 pounds, 8 ounces (2,500 grams).
Very low birth weight refers to babies born weighing less than 3 pounds, 4 ounces (1,500 grams).These conditions increase the risk of complications such as breathing problems, feeding difficulties, hearing and vision problems, cerebral palsy and developmental delay.

NATIONAL CONFERENCE OF STATE LEGISLATURES 2
NATIONAL CONFERENCE OF STATE LEGISLATURES iv
Prenatal Care in the United StatesPregnancy is a unique time during which the body expe-riences extra stress while sup-porting fetal growth. In ad-dition to physical, emotional and hormonal changes, preg-nant women also experience increased risk of certain in-fections and chronic illnesses, and have particular nutritional needs. Prenatal care consists of regular health checkups as well as screening and moni-toring for pregnancy risks. Prenatal care providers also provide counseling and education around healthy pregnancy behaviors and manage illnesses or complications that may arise.
The U.S. Department of Health and Human Services’ Office of Women’s Health and the Maternal and Child Health Bureau within the Health Resources and Services Administration (HRSA) recommend early and reg-ular prenatal care that addresses the individual needs of each woman. According to these recommenda-tions, women should start prenatal care as soon as they know or suspect they are pregnant, ideally within the first trimester, or first 12 weeks of pregnancy. Subsequent visits typically progress from monthly to bi-weekly to weekly.
Women who receive early and regular prenatal care are more likely to have healthy infants, but the exact delivery and frequency of care should take into consideration the “medical, nutritional, psychosocial, cul-tural and educational needs of the patient,” according to the American College of Obstetricians and Gyne-cologists (ACOG).
Core components of prenatal care include:• Assessing the health and well-being of the mother and fetus.• Providing relevant prenatal education on how to stay healthy and give the baby a healthy start.
Maternal Depression, an Often Overlooked ConditionMaternal mental health conditions—which include depression, anxiety and other illnesses—are the most common complications of pregnancy and the 12 months following delivery, affecting 1 in 5 women. Maternal depression, which includes depression during and after pregnancy, can have serious consequences for mothers and their children. While postpartum depression has gained visibility in recent years, depression during pregnancy, or antepartum depression, remains an issue for many women. According to the American College of Obstetricians and Gynecologists (ACOG), 14% to 23% of women suffer from some type of depression during pregnancy.Antepartum depression can significantly affect mothers and developing babies. Several studies have linked antepartum depression with preterm birth and low birth weight. Preterm births are both more costly than full-term births and increase the likelihood of physical and intellectual developmental delays.The cost of preterm births, during and after delivery, is substantial. According to the March of Dimes, caring for a preterm baby in the first year of life costs employers approximately $55,000, whereas care for a baby born without complications costs about $5,000. Nearly half of all births in the United States are paid for by Medicaid, which covers a greater share of preterm births than private insurance. ACOG recommends screening for depression at least once during the perinatal period in order to mitigate the effects of untreated depression during this crucial time.
NATIONAL CONFERENCE OF STATE LEGISLATURES iv
• Anemia• Depression• Diabetes• Environmental
exposures
• Folic acid intake
• Genetics• Health risk
behaviors, including smoking, alcohol use and other drug use
• High blood pressure
• Infections• Medications• Vaccinations • Violence
Prenatal Care Addresses Key Factors Affecting Pregnancy Including:

3 NATIONAL CONFERENCE OF STATE LEGISLATURES
• Completing recommended tests and screenings, such as for gesta-tional diabetes or birth defects.
• Detecting medical and psychosocial issues and intervening as needed.
• Providing appropriate preventive care, such as immunizations.
Women with certain underlying conditions and risk factors may require more frequent care and additional monitoring. For example, pregnancy risks are higher for women carrying twins or multiples, women with ex-isting chronic conditions, women older than 35, and women with a histo-ry of pregnancy complications, such as premature birth or preeclampsia.
Disparities in Prenatal Care-Access and UtilizationNearly one-quarter of U.S. women do not receive timely or recommend-ed prenatal care, often as the result of unequal access and utilization that may in turn result in disparities in birth outcomes (Figure 1). These are evident in disparities such as those by race, education and geogra-phy, which may also be interrelated and co-occurring.
DISPARITIES BY RACE
Racial disparities in maternal and infant outcomes are significant. For example, the rates of preterm births among Black and American Indian/Alaska Native women are significantly higher than those for other
Fig. 1 — Timing of Prenatal Care InitiationUnited States, 2019
Percent of live births
78+16+6+L6.4
First trimester2nd trimesterThird trimester or no care
Source: 2021 March of Dimes Foundation
16
77.6
Source: 2021 March of Dimes Foundation

NATIONAL CONFERENCE OF STATE LEGISLATURES 4
groups (Figure 2). In addition, the rate of low birth weight babies born to Black women is almost dou-ble the rate for white women (Figure 3). Preterm birth and low birth weight are risk factors for in-fant mortality, and there are notable racial dispar-ities in infant mortality rates. For example, Indige-nous infants are also one and a half to two times more likely to die than white infants, and Black in-fants are two to three times more likely to die than white infants.
Given that prenatal care is one of the key strategies to reduce these pregnancy complications, experts are also concerned about racial disparities in when women start getting care and how much care they receive. Black, Hispanic and American Indian/Alas-ka Native women are less likely than white women to initiate prenatal care in the first trimester (Fig-ure 4). When they do begin prenatal care, they are also less likely than white women to receive 80% or more of expected visits.
Both societal and health system factors contribute to high rates of poor health outcomes and mater-nal mortality for Black women, who are more like-
Fig. 2 — Preterm Birth by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
15.0
12.5
10.0
7.5
5.0
2.5
0.0
HispanicWhiteBlack
Source: 2021 March of Dimes Foundation
9.8 9.2
14.0
11.7
8.8
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
Fig. 3 — Low Birth Weight by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
15.0
12.5
10.0
7.5
5.0
2.5
0.0
HispanicWhiteBlack
7.5 7.0
13.9
8.2 8.3
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
8.5
Fig. 4 — Early Prenatal Care by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
100
80
60
40
20
0
HispanicWhiteBlack
72.4
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
82.4
67.364.4
80.5 77.5
10.1
Source: 2021 March of Dimes Foundation
Source: 2021 March of Dimes Foundation
Fig. 2 — Preterm Birth by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
15.0
12.5
10.0
7.5
5.0
2.5
0.0
HispanicWhiteBlack
Source: 2021 March of Dimes Foundation
9.8 9.2
14.0
11.7
8.8
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
Fig. 3 — Low Birth Weight by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
15.0
12.5
10.0
7.5
5.0
2.5
0.0
HispanicWhiteBlack
7.5 7.0
13.9
8.2 8.3
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
8.5
Fig. 4 — Early Prenatal Care by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
100
80
60
40
20
0
HispanicWhiteBlack
72.4
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
82.4
67.364.4
80.5 77.5
10.1
Source: 2021 March of Dimes Foundation
Source: 2021 March of Dimes Foundation
Fig. 2 — Preterm Birth by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
15.0
12.5
10.0
7.5
5.0
2.5
0.0
HispanicWhiteBlack
Source: 2021 March of Dimes Foundation
9.8 9.2
14.0
11.7
8.8
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
Fig. 3 — Low Birth Weight by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
15.0
12.5
10.0
7.5
5.0
2.5
0.0
HispanicWhiteBlack
7.5 7.0
13.9
8.2 8.3
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
8.5
Fig. 4 — Early Prenatal Care by Race/EthnicityUnited States, 2017-2019 Average
Percent of live births
100
80
60
40
20
0
HispanicWhiteBlack
72.4
American Indian/Alaska NativeAsian/Pacific IslanderOverall Average
82.4
67.364.4
80.5 77.5
10.1
Source: 2021 March of Dimes Foundation
Source: 2021 March of Dimes Foundation
Source: 2021 March of Dimes Foundation Source: 2021 March of Dimes Foundation
Source: 2021 March of Dimes Foundation
5 NATIONAL CONFERENCE OF STATE LEGISLATURES
ly to experience barriers to obtaining quality care. Increasing research has also shown how chronic stress such as that caused by experiencing racism and discrimination can increase risk for conditions such as hypertension among Black communi-ties. Black mothers report facing racial discrimina-tion and differential treatment from health care providers, which may raise the risk that health emergencies go unaddressed. These factors, cou-pled with access barriers, may increase risk for complications.
DISPARITIES BY EDUCATION
Educational attainment also contributes to dispar-ities in prenatal care access and pregnancy out-comes. Maternal and infant mortality rates gener-ally decrease with greater educational attainment, although Black women with a college degree or higher are still five times more likely to die from pregnancy-related causes than white women with a similar education.
As illustrated in Figure 5, women with higher edu-cational attainment are more likely to initiate pre-natal care during the first trimester and less likely to start as late as the third trimester or forego pre-natal care altogether.
Fig. 5 — Timing of Prenatal Care (PNC) Initiation by Maternal Education*
United States, 2016
Bachelor’s degree or higherLess than a high school education
Source: CDC
Initiation of PNC in the first trimester
100
80
60
40
20
0
87.6
62.7
3.311.2
Late or no PNC
*Among women aged 25 and over (age limited to allow for completion of education)
Source: CDC

NATIONAL CONFERENCE OF STATE LEGISLATURES 6
DISPARITIES BY GEOGRAPHY
Pregnant women living in rural areas may face challenges accessing care due to transportation, health care provider shortages and lack of specialty care services. Figure 6 illustrates the low ratio of obstetric provid-ers in rural areas across the country, sometimes referred to as maternity care deserts.
Women experiencing these access barriers have lower rates of prenatal care initiation in the first trimes-ter and poorer birth outcomes such as preterm birth. Additionally, rural women have higher rates of early elective delivery—by inducing and augmenting labor—and low-risk cesarean delivery. These procedures may unnecessarily increase risk of adverse outcomes for low-risk pregnant women. Decisions to deliver early may be due to concerns of not reaching the hospital in time because of the travel time needed to reach facilities with obstetric services.
Federal Action and ResourcesPolicymakers and institutions at the local, state and federal levels play a role in promoting healthy pregnan-cies overall and addressing disparities in maternity care.
The Affordable Care Act (ACA) added the Women’s Health Amendment to the Public Health Service Act, re-quiring health insurance plans to cover women’s health preventive services, including prenatal care, with-out cost sharing. These pre-pregnancy and prenatal preventive services include folic acid supplements, expanded tobacco intervention, counseling and screening for a number of conditions, such as anemia, ges-tational diabetes and preeclampsia.
In 2018, Congress passed H.R. 315, the Improving Access to Maternity Care Act. This law required HRSA to identify, collect and publish data around maternity care health professional target areas to address provid-er shortages.
Federal health agencies such as the Office of Women’s Health (OWH), the Centers for Disease Control and Prevention (CDC), and HRSA’s Maternal and Child Health Bureau (MCHB) also play a vital role in promoting healthy pregnancies.
Fig. 6 — Distribution of Obstetric Providers by U.S. County
OB Providers (OB/GYN, Certified Nurse-Midwife) per 10,000 Births and Number of Counties
None (1,241)Fewer than 30 (131)30-60 (399)Greater than 60 (1,365)
Source: March of Dimes 2018, Nowhere to Go: Maternity care deserts across the U.S.

7 NATIONAL CONFERENCE OF STATE LEGISLATURES
OWH has an information hub that provides health information for women across numerous topic areas and has a robust section on pregnancy and prenatal care.
CDC provides data, research, preventive care guidelines and recommendations. For example, the CDC con-ducts national surveillance of pregnancy-related deaths by reviewing copies of death certificates for wom-en who died during pregnancy or within one year of pregnancy from 52 jurisdictions (50 states, New York City and Washington, D.C.). This data helps the public and health professionals understand the causes and trends of maternal death.
The Pregnancy Risk Assessment Monitoring System (PRAMS), a joint surveillance and data collection proj-ect between the CDC and state health departments, is a key tool for states to improve the health of moth-ers and infants by reducing adverse outcomes. Forty-seven states participate in PRAMS, along with New York City, Puerto Rico, the District of Columbia and the Great Plains Tribal Chairmen’s Health Board. PRAMS participants represent about 83% of all U.S. births.
PRAMS collects state-specific, population-based data used by researchers to study emerging maternal health issues. State and local governments use this data to plan programs and policies. For example, Min-nesota lawmakers reviewed PRAMS data before passing SB 699, which approved Medicaid payment for doula services. The state used PRAMS data to better understand how doula services could be targeted to rural and underserved women, particularly to improve prenatal care to American Indian mothers.
HRSA’s MCHB plays a large role in bolstering perinatal—the period between 22 weeks gestation and seven days postpartum—care by administering programs, supporting research and investing in workforce train-ing to improve the health and well-being of mothers and infants. Among other programs and initiatives, MCHB administers the Title V Maternal and Child Health Services Block Grant, providing funding to 59 states and jurisdictions. Title V is one of the largest federal block grant programs and provides support for health programs benefitting 92% of all pregnant women. This interactive webpage shows the contact in-formation for each state’s Maternal and Child Health director as well as national Title V data. Data available include maps that show the number of states reporting on different measures such as risk-appropriate perinatal care. Individual state profiles also summarize each state’s selected priorities and outcomes such as rates of early prenatal care and low birth weight.

NATIONAL CONFERENCE OF STATE LEGISLATURES 8
HRSA’s State Maternal Health Innovation Program also funds nine states to strengthen their capacity to address disparities in maternal health and improve maternal health outcomes. For example, each funded state established a Maternal Health Task Force to create and implement a strategic plan that translates rec-ommendations on addressing maternal mortality and severe maternal morbidity from ideas into action. In addition, the Alliance for Innovation on Maternal Health, or AIM program, assists state-based teams in im-plementing evidence-based maternal safety bundles within hospitals and other types of birthing facilities to improve patient outcomes and reduce maternal mortality and severe maternal morbidity.
State Strategies to Ensure Healthy PregnanciesWith the help of tools such as PRAMS and HRSA-funded programs, states have implemented several strat-egies to improve maternity care overall and address disparities. These strategies include those that directly and indirectly address prenatal care. They include efforts to expand access to different types of providers, care settings and coverage options, as well as those related to improving the quality of care.
Workforce and Access to ServicesBarriers to accessing maternity care affect women’s ability to receive timely and adequate prenatal care. These barriers include finding a trusted provider the woman can communicate with, accessing the location where maternity services are provided and having insurance coverage for services.
There are several reasons women choose to seek prenatal care with different types of providers, such as pregnancy risk level, proximity to the provider, insurance coverage or trust. While pregnant women typi-cally receive prenatal care from obstetricians, family practice physicians or certified nurse-midwives (pro-viders with medical training), some states have expanded access to additional provider types, care settings and models of care to increase prenatal care visits and improve birth outcomes.

9 NATIONAL CONFERENCE OF STATE LEGISLATURES
COMMUNITY HEALTH WORKERS
State or community-based programs may employ community health workers (CHWs) to improve access to health care services and promote health in high-risk communities. CHWs work to address many health concerns, particularly those related to chronic diseases, and are a recommended model of care to reach high-risk women in low-income communities, rural communities and communities of color. CHWs typically live in the communities in which they work and provide support in women’s homes or neighborhoods. As trusted members of the community who generally share the same language and culture, CHWs can help women navigate pregnancy and provide prenatal education, emotional support and care coordination.
Almost all states have laws or administrative policies addressing the CHW workforce, and oversight and development of state CHW programs typically fall under the purview of state health departments. For ex-ample, Illinois enacted a bill in 2014 creating the Community Health Worker Advisory Board under the department of public health. With CHWs included as members, the board was tasked with summarizing best practices, curriculum and training programs for a CHW certification program as well as summarizing recommendations for reimbursement and securing funding. In 2011, the Texas Legislature established an advisory committee and commissioned a study to maximize access to CHWs and to explore public and private funding sources. Texas statute provides authority to operate the CHW training and certification program to the department of health, which continues to oversee the state’s CHW workforce.
DOULAS
Some states also increased access to doula care to provide supplemental support for pregnant women.
Doulas are professional labor assistants who provide physical and emotional support during pregnancy, childbirth and the postpartum period. Doulas do not provide medical care or deliver the baby. Some stud-ies have shown that continuous support from doulas during childbirth may be associated with decreased use of pain relief medication during labor, decreased incidence of cesarean deliveries, decreased length of labor and decreased negative childbirth experiences, particularly for Black women.

NATIONAL CONFERENCE OF STATE LEGISLATURES 10
At least 20 states recently introduced and several passed legislation related to doula care. For example, Vir-ginia passed legislation in 2020 related to doula certification and Indiana passed legislation in 2019 provid-ing that Medicaid pregnancy services may include reimbursement for doula services.
The New York State Health Department launched a pilot program in 2019 to expand Medicaid coverage for doula services in parts of the state with high rates of maternal and infant mortality. The doula pilot is part of Governor Cuomo’s initiative to reduce maternal mortality and racial disparities in birth outcomes.
MIDWIVES
In some cases, women choose midwives for prenatal care and delivery support—seeking a holistic philos-ophy of care, often with fewer medications, lower cost and greater convenience. Midwives include a range of professionally trained providers who support women to maintain healthy pregnancies and have optimal births, such as certified professional midwives and direct entry midwives. This may also be appealing for women with low-risk pregnancies who lack access and transportation to obstetric hospitals. Most states regulate midwives through licensure or certification, but several states do not regulate midwives or allow direct entry midwives to practice.
Oklahoma and the District of Columbia recently provided licensure for midwives to ensure quality and ac-countability while allowing pregnant women expanded options for prenatal care and delivery.
HOME VISITING
One key strategy to reduce access barriers and provide additional support to populations with a higher burden of adverse pregnancy outcomes is through home visiting programs. The federally funded Maternal,
Infant, and Early Childhood Home Visiting (MIECHV) Program funds states and territories to develop ev-idence-based home visiting programs to support pregnant women and parents with young children up to kindergarten entry. These programs are volun-tary and are commonly led by nurses, social work-ers or other trained professionals. Home visiting improves maternal and child health and has been shown to reduce infant mortality, preterm births and emergency room visits.
New Jersey passed legislation in 2016 establishing a three-year Medicaid home visitation demonstra-tion project to provide information, support and es-sential referrals to health and social services during pregnancy, infancy and early childhood.
Colorado’s Prenatal Plus program also serves the state’s Medicaid members, matching high-risk preg-nant women with a team that helps them maintain regular prenatal care as well as obtain additional support, such as nutrition counseling, mental health services and coordinated care. The program was found to be successful in lowering the rate of low birth weight infants—babies born to program partic-ipants had a low birth weight rate 22.5% lower than the expected rate for women without Prenatal Plus services.
South Carolina’s Nurse-Family Partnership, funded in part by Medicaid, is the nation’s first maternal and child health home visiting program to use a pay-for-success model. Under this financing system, funders

11 NATIONAL CONFERENCE OF STATE LEGISLATURES
provide upfront capital to expand social services and the state pays for all or part of the program if it mea-surably improves the lives of participants, as evaluated by an independent party. South Carolina’s program pairs low-income, first-time pregnant women with a home visiting registered nurse to improve pregnan-cy outcomes, among other goals. The program aims to reduce disparities by income and race; most of the women served are women of color. The program reported successful outcomes, with 90% of babies born full term and 89% of babies born at a healthy weight.
In 2018, Utah created a pay-for-success nurse home visiting pilot program within the department of health. The state will pay back investors once specific outcomes are achieved, such as postpartum depres-sion screening and lower rates of preterm birth.
OTHER INNOVATIVE PROGRAMS AND MODELS OF CARE
States have found innovative ways to reduce barriers to quality prenatal care. Texas established the Med-icaid Medical Transportation Program, requiring the maternal mortality and morbidity task force to estab-lish a pilot program for providing medical transportation services to pregnant women and new mothers.
California passed the Dignity in Pregnancy and Childbirth Act in 2019, which made legislative findings re-lating to implicit bias and racial disparities in maternal mortality rates. The law also requires hospitals and alternative birth centers to implement an implicit bias program for all perinatal health care providers with-in those facilities.
Implicit bias training is emerging as a state strategy to address racial disparities in perinatal care and birth outcomes. Maryland required the state’s Cultural and Linguistic Health Care Professional Competency Pro-gram to establish and provide an evidence-based implicit bias training program for perinatal health care professionals. The bill also requires certain health care professionals to complete the training on or before Jan. 1, 2022. Illinois directed the department of public health to develop best practices for implicit bias training and education in cultural competency for birthing facilities.
Many states have a Healthy Start program or coalition, which is funded by HRSA and administered by states and communities. Healthy Start programs aim to reduce infant mortality rates, increase access to early prenatal care and remove barriers to health care access. Florida’s Healthy Start program was created legislatively in 1991 and screens all pregnant women to identify those at risk of poor birth and health out-comes. The program offers care coordination and education on prenatal care, parenting, interconception care—the time between pregnancies—and stress management.
Medical practices in at least 46 states have adopted the Centering Pregnancy model, an innovative model of care that uses group prenatal care to bring together expectant mothers for a series of enhanced prena-tal visits. In addition to medical care, participating women receive guidance about nutrition, breastfeeding, labor and delivery. The program also builds community and peer support. Where implemented, Centering Pregnancy can decrease the rate of preterm and low-weight births, reducing costly neonatal intensive care unit (NICU) admissions; increase mothers’ engagement in their own care; and reduce racial disparities in preterm birth.
Providing services through telehealth is another innovative approach states employ to address access to care, particularly in rural areas. Arkansas and Virginia operate telehealth programs for high-risk pregnant women. These programs consist of video conferencing with maternal and fetal medicine specialists, and each have demonstrated significant outcome improvements, such as fewer deliveries of very low birth weight infants and shorter stays in NICUs.
NATIONAL CONFERENCE OF STATE LEGISLATURES 12
NATIONAL CONFERENCE OF STATE LEGISLATURES iv
COVID-19 May Change Prenatal Care Delivery Beyond the PandemicThe COVID-19 pandemic caused major disruptions in routine and preventive care access, including for pregnant women, particularly during the early months of the outbreak. Health care providers limited in-person appointments to reduce the spread of the virus and patients avoided health care facilities for fear of infection. Pregnant women may be at increased risk of severe illness from COVID-19 as well as other adverse outcomes such as preterm birth. The Centers for Disease Control and Prevention recommend that pregnant women take additional precautions to avoid infection.The American College of Obstetricians and Gynecologists emphasized the importance of keeping all prenatal care appointments, although in-person visits may be fewer or farther in between. Tests and procedures that were typically more spread out or conducted over separate visits may be condensed into fewer in-person visits and other care and consultation provided by phone or online. State efforts to expand telehealth coverage and access during the pandemic have allowed pregnant women to continue care, with many providers considering a permanent shift in prenatal care practice. For example, providers at Michigan Medicine have adjusted to only a handful of in-person visits, with all others going virtual. They also indicated that their revised schedule may be appropriate for low-risk pregnancies beyond the pandemic, particularly if patients have basic vitals monitoring devices at home.
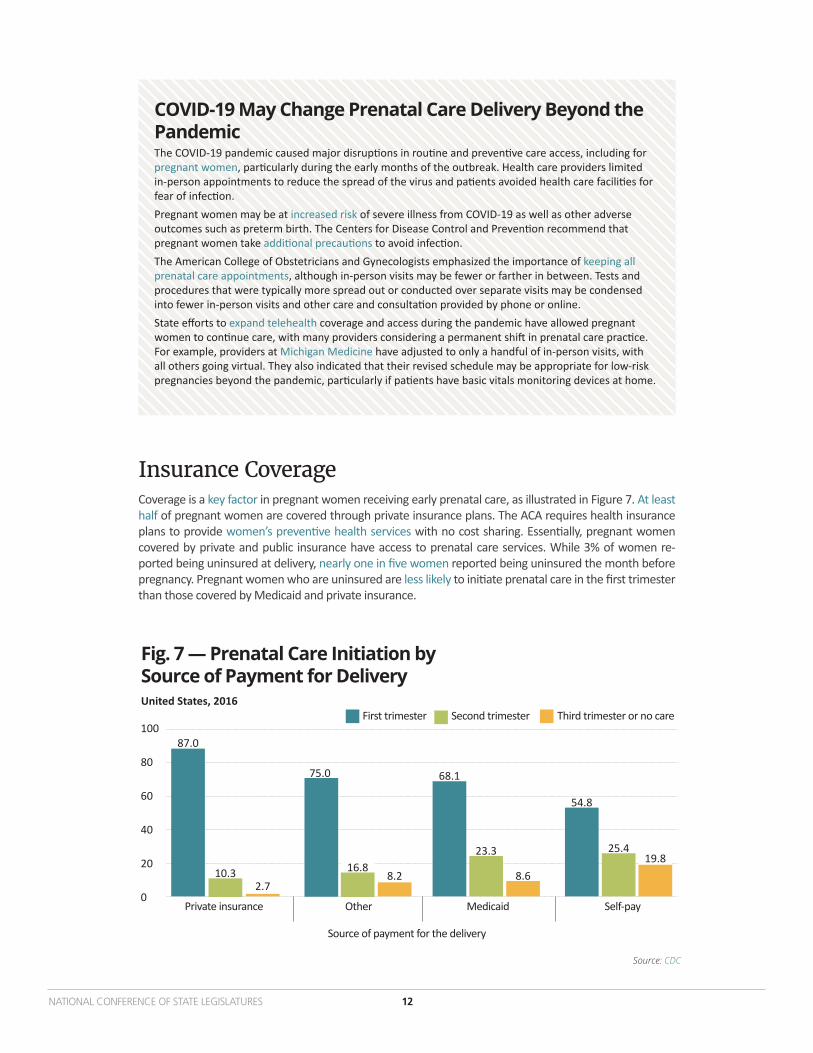
Insurance CoverageCoverage is a key factor in pregnant women receiving early prenatal care, as illustrated in Figure 7. At least half of pregnant women are covered through private insurance plans. The ACA requires health insurance plans to provide women’s preventive health services with no cost sharing. Essentially, pregnant women covered by private and public insurance have access to prenatal care services. While 3% of women re-ported being uninsured at delivery, nearly one in five women reported being uninsured the month before pregnancy. Pregnant women who are uninsured are less likely to initiate prenatal care in the first trimester than those covered by Medicaid and private insurance.
Fig. 7 — Prenatal Care Initiation by Source of Payment for DeliveryUnited States, 2016
Private insurance
100
80
60
40
20
0
87.0
2.7
75.0
8.2
Source of payment for the delivery
68.1
8.6
54.8
19.8
Other Medicaid Self-pay
First trimester Third trimester or no careSecond trimester
25.423.316.810.3
Source: CDC

13 NATIONAL CONFERENCE OF STATE LEGISLATURES
Medicaid is the single largest payer of maternity-related services, covering about 43% of all U.S. births. Medicaid also covers a greater share of births in rural areas; among women with lower levels of education-al attainment; among girls under 19; and among Hispanic, Black and American Indian/Alaska Native wom-en. Due to Medicaid’s role in covering births among populations with higher risk for pregnancy complica-tions and adverse birth outcomes, Medicaid can be one lever to address pregnancy-related morbidity and mortality as well as disparities in birth outcomes by ensuring coverage and access to preventive services.
Federal regulations allow states to cover pregnant women under the Medicaid state plan up to either 185% of the federal poverty level (FPL) or the highest income level in effect prior to transitioning to new income eligibility standards established by the ACA. Medicaid is required to provide coverage through 60 days postpartum.
Many states provide coverage for pregnant women up to 250% FPL, with a few covering over 300% FPL (for example, Wisconsin and Iowa) through Section 1115 waivers. These waivers can be an option to design programs to meet states’ unique needs, such as increasing eligibility limits if a state is already at its maxi-mum under the Medicaid State Plan (as long as the waivers are cost-neutral to the federal government).
Presumptive eligibility is another option for states to provide Medicaid coverage for pregnant women. It eliminates the waiting period for determining eligibility and provides women immediate access to prenatal care. States have the option of authorizing qualified entities to enroll individuals through presumptive eli-gibility, such as certain health care and social service providers. Currently, at least 30 states allow presump-tive eligibility for pregnant women.
Another option to address coverage and outcomes for women and infants is through Medicaid expansion. Women in states that have expanded Medicaid are more likely to have health coverage prior to and during the early months of pregnancy, and are more likely to start prenatal care early. Researchers also found that, overall, states that have expanded Medicaid have lower maternal and infant mortality rates, particu-larly among Black infants, compared to those that have not.
The Children’s Health Insurance Program (CHIP) provides additional options for states to cover pregnant women. States may not cover pregnant women at a higher income standard than the standard established for children. Colorado and Missouri are among states that currently offer coverage options for pregnant women through CHIP.
Data and QualityState efforts to improve quality of prenatal care include those to establish perinatal quality collaboratives (PQCs), advisory councils or task forces. A common thread across these different teams is the reliance on data and targeted recommendations to improve outcomes for each state and community.
One of the most common examples of using data to improve quality of prenatal care is via perinatal qual-ity collaboratives. PQCs identify health care processes that need to be improved and use quality improve-ment principles to address gaps in maternal and infant care, typically making changes as quickly as pos-sible. PQCs often work to reduce preterm births, severe pregnancy complications related to high blood pressure and hemorrhage, cesarean births among low-risk pregnant women, and disparities by race and geography.
Almost all states have PQCs available or in development, as illustrated in Figure 8. Arkansas and Delaware have more recently established PQCs, and Illinois recently expanded the scope of its PQC to develop an initiative to reduce racial and ethnic disparities during the immediate periods before, during and after delivery. The Illinois law also aims to improve timely identification and consultation for pregnant wom-en in birthing facilities, including allowing use of telemedicine for consultation. Finally, the law requires yearly education on severe maternal hypertension and obstetric hemorrhage management for obstetric providers.
Alabama’s PQC developed a Maternal Hypertension Initiative to establish protocols, processes and educa-tion to ensure providers quickly identify women with hypertension/preeclampsia and manage the condi-tion before further complications arise.

NATIONAL CONFERENCE OF STATE LEGISLATURES 14
States also set up advisory councils and task forces to improve the quality of perinatal care. Louisiana cre-ated the Healthy Moms, Healthy Babies Advisory Council within the Louisiana Department of Health. The legislation provided that the council, made up of experts and stakeholders committed to addressing racial and ethnic disparities in maternal health outcomes, will support the state PQC by incorporating a commu-nity-engaged approach to preventing maternal mortality and morbidity. Additionally, the legislation ex-panded public coverage options to provide access to provider services and other delivery-focused reforms that address maternal health outside the hospital setting.
Illinois created the Task Force on Infant and Maternal Mortality Among African Americans to establish best practices to decrease infant and maternal mortality among African Americans in Illinois. The task force’s duties include reviewing research to identify best practices and effective interventions for improving the quality and safety of maternity care, improving health outcomes during pregnancy, and addressing social determinants of health disparities in maternal and infant health outcomes.
Fig. 8 — Status of Perinatal Quality Collaboratives (PQC)in the United States
HI
ID
MT
WY
ND
SD
NM
NE
OK
IA
KS
TX
WI
MO
LA
IL
AR
KY
MS
IN
TN
MI
AL
OH
NC
FL
GA
SC
DC
MA
CT
NHVTAK
WA
OR
CA
NV
UT
CO
AZ
MN
WV VA
PA
NY
NJ
MD
DE
RI
ME
Information not available
State with PQC and CDC Division of Reproductive Health funding
PQC in development
PQC available Source: CDC

15 NATIONAL CONFERENCE OF STATE LEGISLATURES
NATIONAL CONFERENCE OF STATE LEGISLATURES iv
Substance Use Disorder During PregnancySubstance use during pregnancy can have serious consequences for the mother and developing infant. Prenatal alcohol use can cause miscarriage, stillbirth and a range of disabilities. Tobacco use increases risks of preterm birth, low birth weight, birth defects of the mouth and lip, and sudden infant death syndrome. Marijuana use is linked to low birth weight and may increase chances for developmental problems for the child. Opioid use is linked to poor fetal growth, preterm birth, stillbirth, certain birth defects and neonatal abstinence syndrome (NAS).While rates of substance use disorder (SUD) among pregnant women vary across different substances, the number of women with opioid use disorder (OUD) at labor and delivery quadrupled from 1999-2014. Additionally, polysubstance use, or the use of more than one substance, is common during pregnancy, particularly during early pregnancy. For example, 10% of pregnant women reported current alcohol use, and among those women, about 40% reported current use of one or more other substances.Prenatal care appointments can serve as critical touchpoints to screen pregnant women for SUD and refer women to timely treatment. Clinical guidelines from the American College of Obstetricians and Gynecologists include early universal screening (at the first prenatal visit), counseling and medication-assisted treatment (MAT) rather than stopping opioids during pregnancy. MAT has a higher chance of healthier outcomes and lower risk of relapse compared to withdrawal methods.States have moved to reverse the rising rates of perinatal SUD in recent years. For example, Washington required the department of health to educate pregnant individuals in opioid treatment programs about the risks of not treating OUD and required the state Medicaid authority to ensure pregnant individuals identified as at risk receive outreach related to OUD.Texas directed the department of state health services to improve screening, referral, care and access to MAT for pregnant women. Delaware established a perinatal quality collaborative to improve health outcomes for pregnant women and newborns, specifically identifying pregnant women with SUD and infants born with NAS as targets for quality care review. In order to encourage women to get treatment without fear of being arrested or losing their children, Montana passed a safe harbor law protecting pregnant women seeking or receiving evaluation, treatment or support services for SUD. Recent studies have found that states with policies that criminalized substance use during pregnancy or considered it child abuse or neglect were associated with significantly greater rates of NAS after enactment, while policies that required reporting of suspected use but did not include punitive penalties had no association with rates of NAS.
ConclusionInvestments in high quality prenatal care and policies to improve access for pregnant women can save lives, improve quality of life and save states money. States have employed many innovative strategies to increase access and utilization of prenatal care, particularly for women who are at higher risk of adverse pregnancy outcomes.

Tim Storey, Executive Director
7700 East First Place, Denver, Colorado 80230, 303-364-7700 | 444 North Capitol Street, N.W., Suite 515, Washington, D.C. 20001, 202-624-5400
ncsl.org© 2021 by the National Conference of State Legislatures. All rights reserved.
Khanh H. Nguyen, MSW, MPHSenior Policy Specialist, Health Program
This project is supported by the Maternal and Child Health Bureau (MCHB), Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number
U1XMC31659-02-00, Supporting State Maternal and Child Health Policy Innovation Program. This information or content and conclusions are those of the author and should not be construed as the official
position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.