staffing escalation for nursing - inpatient areas · trust policy and procedure document ref. no:...
TRANSCRIPT
Source: Deputy Chief Nurse Issue Date: January 2017 Page 1 of 13 Status: Approved Review Date: January 2019
Trust Policy and Procedure Document Ref. No: PP(17) 342
Staffing Escalation for Nursing - Inpatient areas
For use in: All areas of the Trust
For use by: All Trust staff
For use for: To advise and inform hospital staff of the Trusts policy regarding safe staffing levels on inpatient adult wards.
Document owner: Deputy Chief Nurse
Status: Approved
Contents
Page
Section 1 Introduction
1.1 Policy Statement and Rationale 2
Section 2 Policy and Procedure
2.1 Nursing establishment and skill mix 3
2.2 Managing staffing requirements at ward level 3
2.3 Flow Chart for the daily management of nurse staffing in inpatient
areas
4
2.4 Escalation levels and trigger points 5
2.5 Mitigation cascade 6
2.6 Reporting 6
Section 3 Duties and Responsibilities
3.1 Duties and Responsibilities 7
Section 4 Nursing Red Flags
4.1 Definition 7
4.2 Nursing Red Flag escalation process 9
References 10

Source: Deputy Chief Nurse Issue Date: January 2017 Page 2 of 13 Status: Approved Review Date: January 2019
SECTION 1 INTRODUCTION
1.1 Policy Statement and Rationale
West Suffolk NHS Foundation Trust is committed to be the healthcare provider of first choice by providing excellent quality, safe, effective and caring services. The impact of nursing, midwifery and care staffing capacity and capability, on the quality of care experienced by patients and on patient outcomes has been well documented, with multiple studies linking low staffing levels to poorer patient outcomes (DH, Hard Truths 2014).
This policy provides guidance on a shift by shift, day by day approach to the management of staffing levels in inpatient areas.
The purpose of this document is to:
Provide guidance to staff in reaching decisions regarding the organisation of staffing on any inpatient area when the number of staff falls below planned levels on a shift by shift basis.
Ensure that staffing decisions are based on the acuity/ dependency of patients across the Trust.
Minimise clinical risk associated with reduced staffing levels.
Indicate possible actions available to staff, providing a clear process for mitigation of risks and determines a risk rating following mitigation.
Explain the roles and responsibilities of team members in managing staffing issues.
Improve utilisation of existing staff and reduce reliance on temporary staff.
Enable accurate and consistent reporting.
Provide assurance to the Board that in-patient staffing and other clinical risk is managed appropriately on a shift by shift basis.
Source: Deputy Chief Nurse Issue Date: January 2017 Page 3 of 13 Status: Approved Review Date: January 2019
SECTION 2 POLICY AND PROCEDURE
2.1 Nursing establishment and skill mix
The Executive Chief Nurse holds executive responsibility for skill mix and staffing levels for wards and is required to take to open Board twice yearly a review of establishments which needs to be approved by the Trust Board.
This establishment is determined by utilising an evidence based tool and leads to planned day and night time shift staffing numbers (both registered and non-registered staff).
Each clinical ward should have a level of staff with specific skills and competencies on each shift, i.e. the ability to coordinate, IV skilled etc. as agreed with the Ward Manager /Matron.
In areas where workload is known to vary according to the day of the week planned staff numbers for day and night shifts and skill mix should reflect this.
Staff will work a combination of long and short shifts or long days in order to meet the clinical requirement. Variations to these shifts may be worked but must be with the agreement of the Ward Manager/Matron and a record kept (e-rostering).
2.2 Managing staffing requirements at ward level
The Ward Manager/Ward Coordinator are responsible for ensuring staffing levels are such that all patient care needs are met on a shift by shift basis and that any risks are escalated to their divisional bleep holder immediately.
Where there is a change from the usual plan required for a shift e.g. planned staffing not fully required due to reduction in patient admissions to ward area, this should be identified to the divisional bleep holder so that staff can be redeployed if needed.
One to one close observation (special) should be requested to and recorded by the Divisional Bleep holder.
The day and night shift planned and actual staffing levels should be clearly displayed
in every area.
To maintain safe staffing levels it is expected that nursing staff will move to work on
other wards which may be outside of their Division.
To ensure patient safety, short notice sickness will be covered initially by the
supervisory Ward Manager when they are on duty, they will work clinically to fill
essential gaps until other arrangements can be made.
When agency nurses are required they will be allocated to a ward where WSH staff
are working. No shifts will be staffed by agency nurses alone.
Newmarket and Glastonbury have flowcharts to escalate staffing issues see
appendix 1.

Source: Deputy Chief Nurse Issue Date: January 2017 Page 4 of 13 Status: Approved Review Date: January 2019
2.3 Flow chart for the daily management of safer staffing and escalation
08:00 Divisional bleep holder collects ward staffing numbers for the late and night shift
for that day and the early shift, where appropriate, the following day and makes decisions to move staff as required within Division and contacts WSP (bank) to cover
any gaps.
ACTION POINT: Any patient safety risks identified that cannot be mitigated by bleep holder are discussed with Matron or Deputy Chief Nurse
By 09:00 Divisional bleep holder contacts WSP to update any staffing requests with
them. Ward staffing not meeting core levels are reviewed and actions taken according to escalation levels (Escalation support tool 2.4).
ACTION POINT: 12:00hrs Bed meeting is attended by all Divisional bleep holders
358 bleep holder updates electronic staffing situation report that informs the Capacity Report RAG rating.
When ward staffing is not meeting core, levels are reviewed and actions taken according to escalation levels (in 2.4) by Divisional bleep holders.
By 15.00 Trust wide RAG on Capacity Report to be updated by 358 bleepholder
Action point: 15:00 Divisional bleep holders to develop a plan for staffing over the night shift and early shift for following day & communicate with the Patient Flow Team at 20:00 who have responsibility for overnight staffing escalation.

Source: Deputy Chief Nurse Issue Date: January 2017 Page 5 of 13 Status: Approved Review Date: January 2019
2.4 Trust Nurse Staffing Escalation support tool Level One or more of following:
Decision made by Action
Level 1 GREEN
Safe staffing levels achieved across most wards to meet activity and patient acuity /dependency requirements Nursing Red Flags resolved at ward level 90% of wards (18 - 20) at planned staffing levels
Ward (supported by Divisional bleep holder)
Monitor and inform Matrons of areas not at plan.
Level 2 AMBER
Staffing levels fall below template and some shifts are not covered for next 24 hours Rising staffing pressures with gaps in the roster that cannot be mitigated for Gaps across one division area or widely spread across Trust Nursing Red Flags resolved at Divisional level 70% - 90% of wards (14 - 18) at planned staffing levels
Divisional bleep holders
Advise WSP of staff cover required.
Ward Manager & band 6s on management days to support delivery of care into ward numbers.
Staff moved within Division - risk is shared but manageable in line with patient acuity review
Regular review by Divisional bleep holder
Matrons all aware
Level 3 RED
Numerous gaps in staffing across more than one Division
High levels of activity requiring opening of escalation areas
All mitigation for Amber status taken and risk remains Nursing Red Flags not resolved at Divisional level
60% - 70% of wards (12 - 14) at planned staffing levels
Divisional bleep holders (supported by Senior Matrons)
Staff moved across Divisions
Use Health Roster to review time owing to the Trust from members of staff and utilise these where possible
Deputy Chief Nurse fully aware of the situation and advise on redeployment
Level 4 BLACK
Numerous staffing gaps. High levels of activity requiring opening of escalation areas Mitigation actions taken but risks remain high 60% or less of wards (<12) at planned staffing levels Black escalation status can only be declared by Executive Chief Nurse or deputy in the absence of.
In hours:
Executive Chief Nurse
Out of hours:
Silver on call
Patient Flow Team
Escalate to Gold if required
Notify: (In hours) Executive Chief Nurse (Out of hours) Silver on call
Matrons and Deputy Chief Nurse are deployed to ward areas
Deploy available RNs from non-ward based roles to wards
Cancel non-mandatory training sessions
Additional agency nurses will be considered at this point if the above mitigation does not reduce the level
All mitigation actions reviewed.
Executive Chief Nurse to consider number of beds open

Source: Deputy Chief Nurse Issue Date: January 2017 Page 6 of 13 Status: Approved Review Date: January 2019
2.5 Mitigation Appropriate mitigation where there are individual unplanned staffing gaps should be taken in the following order:
Mitigation action Responsible person for this decision
WSP used if within staffing budget Ward Manager Matron 888 OOH
Move own staff within Division Divisional bleep holder Matron 888 OOH
Review staff not in ward numbers (supervisory shifts – not including student nurses), Ward Manager into numbers.
Divisional bleep holder Matrons 888 OOH
Move staff across the Divisions Deputy Chief Nurse 888 OOH
Consider downgrading registered nurse vacant shift to nursing assistant if safe to do so
Deputy Chief Nurse 888 OOH
Utilise Assistant Practitioners where available to fill RN gaps moving across division where appropriate
Deputy Chief Nurse 888 OOH
Deploy available non ward based registered nurses to ward areas
Deputy Chief Nurse Service Managers 888 OOH
Temporary staffing from usual/ Agency staff to be booked
General Managers Executive Chief Nurse
2.6 Reporting
Monthly data on staffing fill rates to plan for nurses, midwives and care staff has been presented on NHS Choices website from June 2014 onwards. Patients and the public will be able to see how hospitals are performing on this indicator in an easy and accessible way. The data will sit alongside a range of other safety indicators. This data will be submitted via UNIFY on the 10th of each month with the preceding month’s data. The Trust Board will receive ward level information on actual versus planned nurse staffing
and triggers of nurse red flags every month and every six months a detailed review of staffing using evidence based tools will be reported to the Trust Board. The Trust will also publish their actual versus planned staff fill rates on a ward by ward basis on the Trust website.

Source: Deputy Chief Nurse Issue Date: January 2017 Page 7 of 13 Status: Approved Review Date: January 2019
SECTION 3 DUTIES AND RESPONSIBILITIES
The following roles listed below each have a responsibility in managing staffing levels and plans on a daily basis, and escalating issues in a timely fashion
Role Responsibility
Divisional Bleep holder
A Ward Sister who holds the bleep for their Division. Responsible for collating staffing numbers and nurse sensitive issues (patients requiring 1:1, high acuity etc.) including responding to reports of Nursing Red Flags. They move staff within their Division to mitigate any risk. Any outstanding risks they are unable to manage within their Division are escalated to the Matron and Service Manager.
Ward Sister/Charge Nurse
Responsible for rostering effectively and minimising planned staffing gaps including responding to reports of Nursing Red Flags.
Clinical site practitioner 888
Responsible for holding the Divisional bleep’s OOH –following staffing plan identified by the Divisional Bleep holder/matron and uses clinical judgement to manage any further issues that arise, including responding to reports of Nursing Red Flags out of hours. To assess staffing plan for night on Friday’s for weekends.
Senior Manager on call Silver
Responsible for supporting the Clinical Site practitioner regarding Trust staffing overnight, and also when patient flow is compromised. Responsible for determining additional actions when staffing at Black and escalating risks to Exec on call. Attend 3pm bed meetings. To assess staffing plan for night on Fridays for weekends.
Deputy Chief Nurse
Review and lead on actions being taken when staffing is at Red/Black status within their Divisions. Attend 3pm bed meetings where possible. To assess staffing plan for night on Fridays for weekends.
Executive Chief Nurse
Responsible for the agreement of use of agency staff. Responsible for determining additional actions when staffing at Black (in hours) and advising others as appropriate. To authorise the continuation of the number of beds open when staffing issues cannot be rectified and where patient care and safety is compromised.

Source: Deputy Chief Nurse Issue Date: January 2017 Page 8 of 13 Status: Approved Review Date: January 2019
SECTION 4 NURSING RED FLAGS 4.1 Definition
Nursing Red Flags (NICE, 2014) are identified as:
Unplanned omission in providing patient medications.
Delay of more than 30 minutes in providing pain relief.
Patient vital signs not assessed or recorded as outlined in the care plan.
Delay or omission of regular checks on patients to ensure that their fundamental
care needs are met as outlined in the care plan, i.e. intentional rounding.
A shortfall of more than 8 hours or 25% (whichever is reached first) of registered
nurse time available compared with the actual requirement for the shift.
Less than two Registered Nurses present on a ward during any shift.
Nursing Red Flags will be recorded on e-rostering by nurse in charge or Divisional bleep holder. If unable to record on e-rostering at the time a message must be left for the Ward Manger to enter this retrospectively. Actions to be taken regarding Red Flags are listed in section 4.2 Nursing Red Flag Escalation Process.

Source: Deputy Chief Nurse Issue Date: January 2017 Page 9 of 13 Status: Approved Review Date: January 2019
4.2 Nursing Red Flag Escalation Process
Yes No
Yes No
Red Flag resolved
Review Ward Based Resolution
Red Flag identified
Record Red flag on HealthRoster and inform Divisional Bleep
holder
Bleep holder to liaise with ward to provide support
Red Flag resolved
Ward senior nurse and bleep holder escalate in line with escalation support tool

Source: Deputy Chief Nurse Issue Date: January 2017 Page 10 of 13 Status: Approved Review Date: January 2019
Source: Deputy Chief Nurse Issue Date: January 2017 Page 11 of 13 Status: Approved Review Date: January 2019
References
NICE 2015 Safe Staffing and effiency – http://pathways.nice.org.uk/pathways/safe-staffing-for-nursing-in-adult-inpatient-wards-in-acute-hospitals Spilsbury et al 2011 Evaluation of the Development and Impact of Assistant Practitioners Supporting the Work of Ward-Based Registered Nurses n Acute NHS (Hospital) Trusts in England http://www.netscc.ac.uk/hsdr/files/project/SDO_FR_08-1619-159_V01.pdf p142
Version and Status Approved
Date Ratified 15 August 2016
Ratified by Trust Executive Group
Name of Originator / author, job title and Department
Tracey Oats, Deputy Chief Nurse, Nursing & Governance Directorate
Name of Responsible Committee Trust Executive Group
Issue Date January 2017
Review Date January 2019
Notes To be reviewed by TEG in December 2016

Source: Deputy Chief Nurse Issue Date: January 2017 Page 12 of 13 Status: Approved Review Date: January 2019
Appendix 1
Rosemary Ward, Newmarket Hospital Staffing – Guidance for 933 Bleep
Holder.
Rosemary Ward staffing at core
staffing levels: Early: 2:3, Late:
2:2, Night: 2:1 Yes
Update 933 template. No
further action required.
No.
Confirm level of staffing
deficit. Update staffing board
in Hospital Control Centre.
With support of Medical
Manager of the Day and Senior
Matron, identify WSFT staff
available to provide Rosemary
Ward with support.
(Liaise with Bleep Holder 888
during Out of Hour periods).
Update Rosemary Ward. Book
taxi, if required, to transport
member of WSFT to and from
Rosemary Ward.
Inform WSFT member of
staff of need to transfer to
Rosemary Ward.
Ask Nurse in Charge of WSFT
ward to ensure blue flag entered
on Healthroster, to reflect move
of team member to Rosemary
Ward.
07:00 – 08:00. 933 Bleepholder
to contact Nurse-in-Charge on
Rosemary Ward to confirm staffing
numbers (#6381).
Source: Deputy Chief Nurse Issue Date: January 2017 Page 13 of 13 Status: Approved Review Date: January 2019
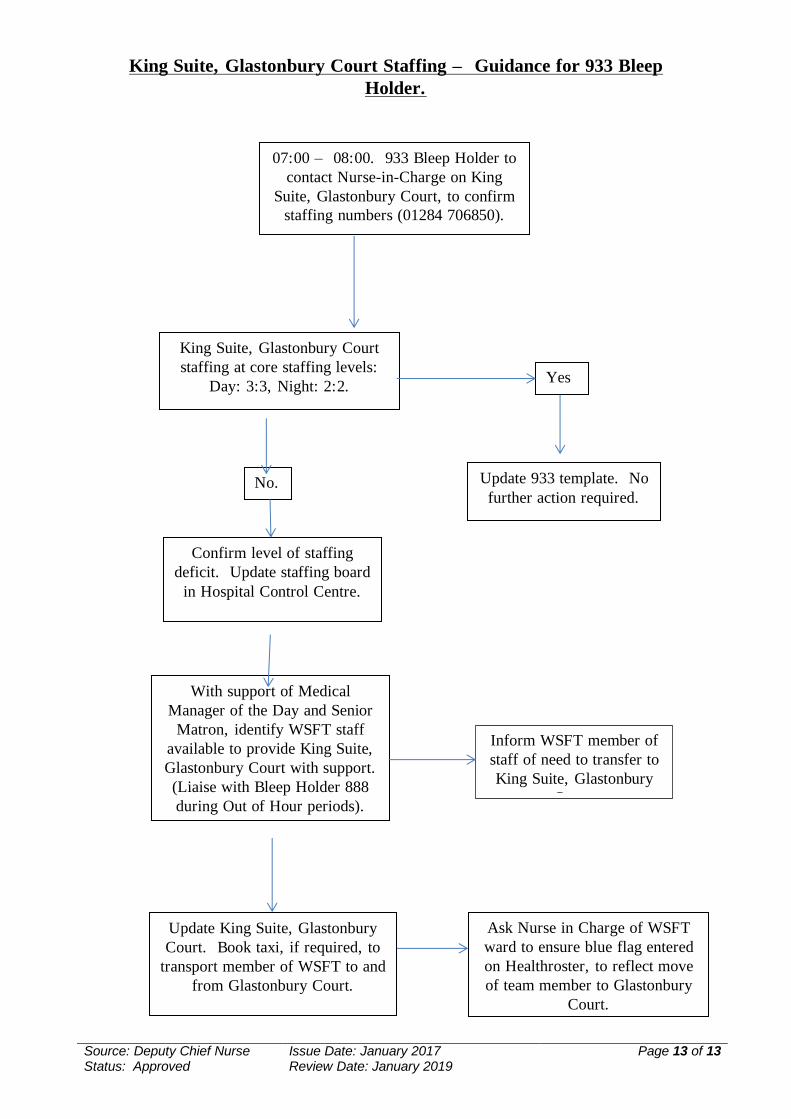
King Suite, Glastonbury Court Staffing – Guidance for 933 Bleep
Holder.
Yes
King Suite, Glastonbury Court
staffing at core staffing levels:
Day: 3:3, Night: 2:2.
Update 933 template. No
further action required. No.
Confirm level of staffing
deficit. Update staffing board
in Hospital Control Centre.
With support of Medical
Manager of the Day and Senior
Matron, identify WSFT staff
available to provide King Suite,
Glastonbury Court with support.
(Liaise with Bleep Holder 888
during Out of Hour periods).
Update King Suite, Glastonbury
Court. Book taxi, if required, to
transport member of WSFT to and
from Glastonbury Court.
Inform WSFT member of
staff of need to transfer to
King Suite, Glastonbury
Court.
Ask Nurse in Charge of WSFT
ward to ensure blue flag entered
on Healthroster, to reflect move
of team member to Glastonbury
Court.
07:00 – 08:00. 933 Bleep Holder to
contact Nurse-in-Charge on King
Suite, Glastonbury Court, to confirm
staffing numbers (01284 706850).