spots with keys
TRANSCRIPT

SPOTTERS
Dr Mohit GoelJRII30 Dec. 2013

SPOT 1
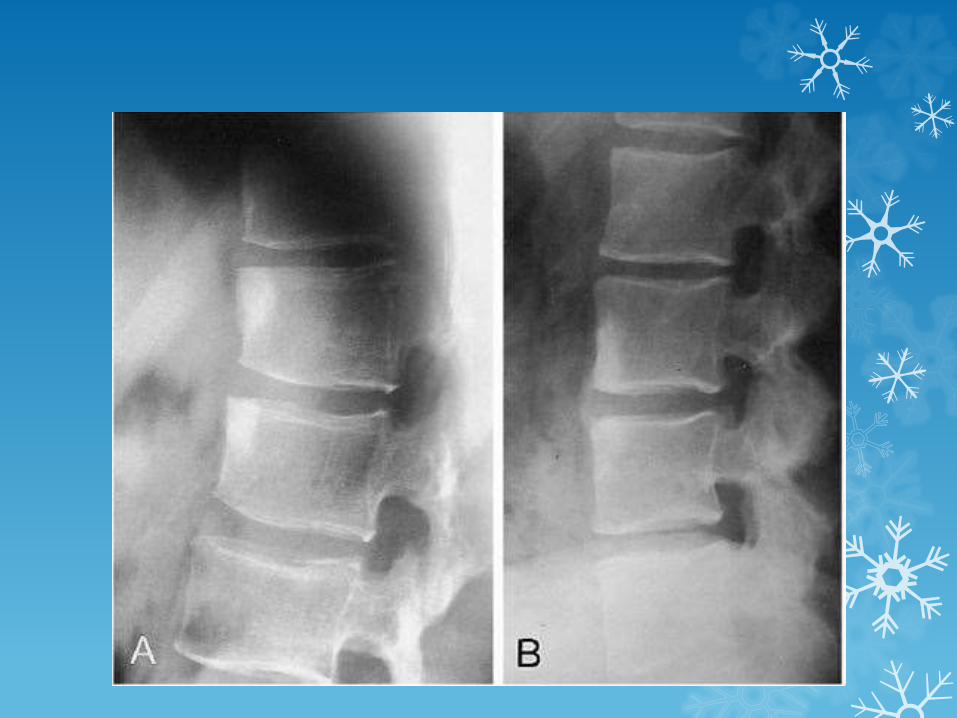
Shiny corner sign
The shiny corner sign, also known as a Romanus lesion, is an early spinal finding in ankylosing spondylitis.
These represent small erosions at the superior and inferior endplates (corners on lateral radiograph) of the vertebral bodies, with surrounding reactive sclerosis.
Eventually the vertebral bodies become squared

SPOT 2

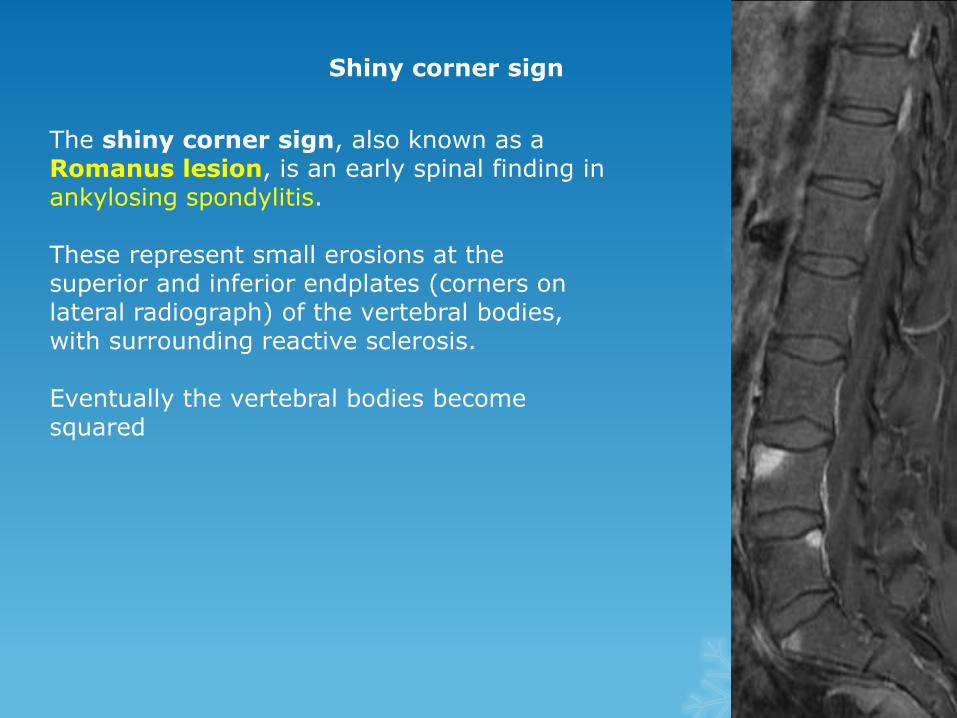
Anteroposterior view of the hand in this patient with sarcoiddemonstrates classic changes of bony involvement with this granulomatous process.
Note the lacelike pattern of destruction, which is seen most prominently in the proximal phalanges and in the distal third phalanx.
Soft tissue swelling and some areas of severe bony dissolution are also noted, which occur in more advanced patterns of sarcoid.
These changes are typically limited to the hands but can rarely occur in other parts of the skeleton.
Sarcoid.

SPOT 3

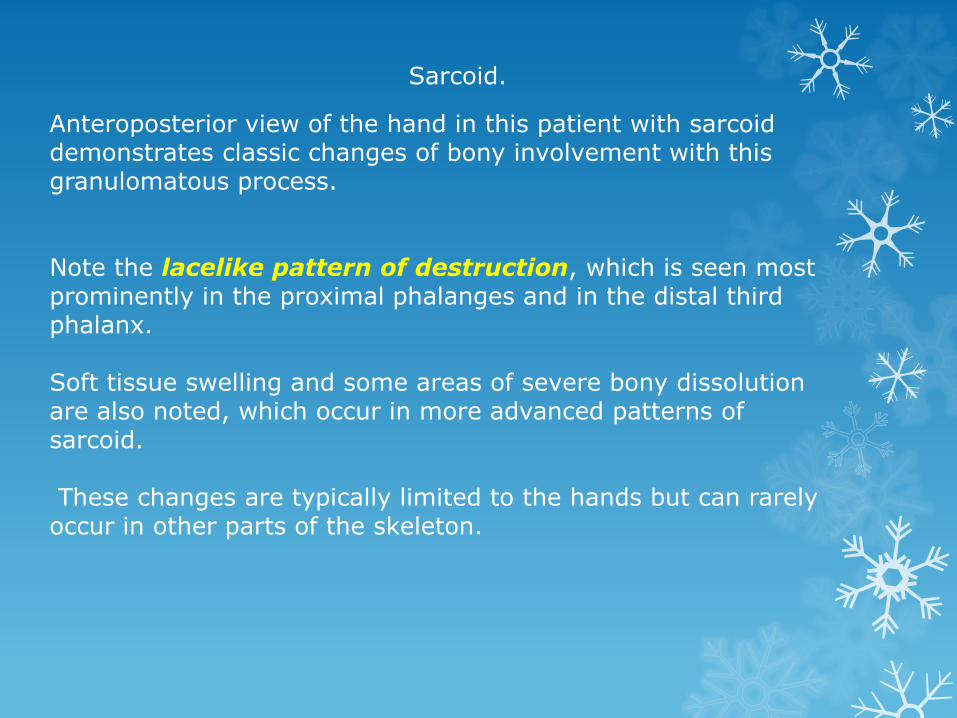
Patient was known to have long-standing bronchiectasis shows extensive lamellar periosteal new bone formation around the shafts of the distal radius, ulna, metacarpals, and proximal phalanges.
Hypertrophic osteoarthropathy is characterised by a proliferative periostisisinvolving the long bones. When associated with a lung condition it is also termed hypertrophic pulmonary osteoarthropaty(HPOA). It is usually painful and associated with clubbing

SPOT 4
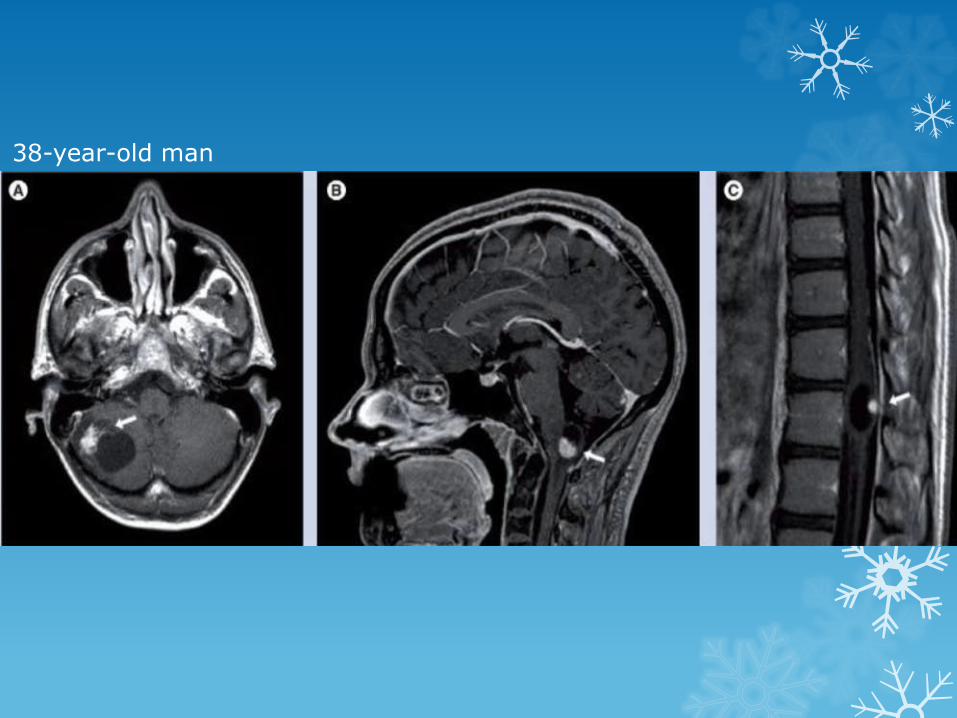
38-year-old man

Von Hippel-Lindau disease (VHL)

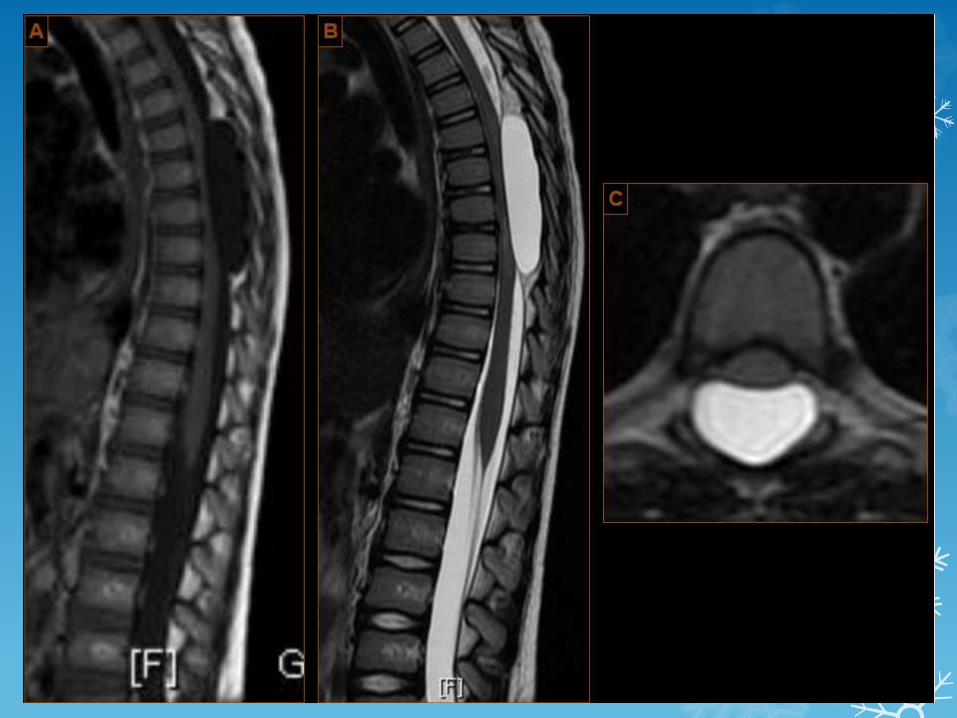
SPOT 5

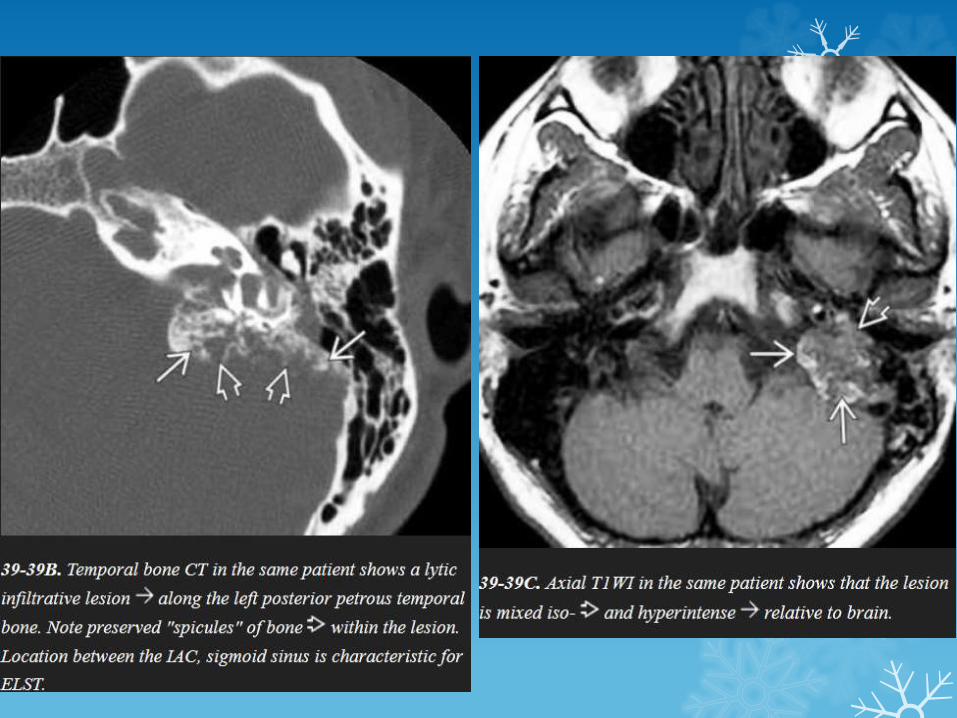
CT MRI

Endolymphatic sac tumors (ELSTs)


SPOT 6
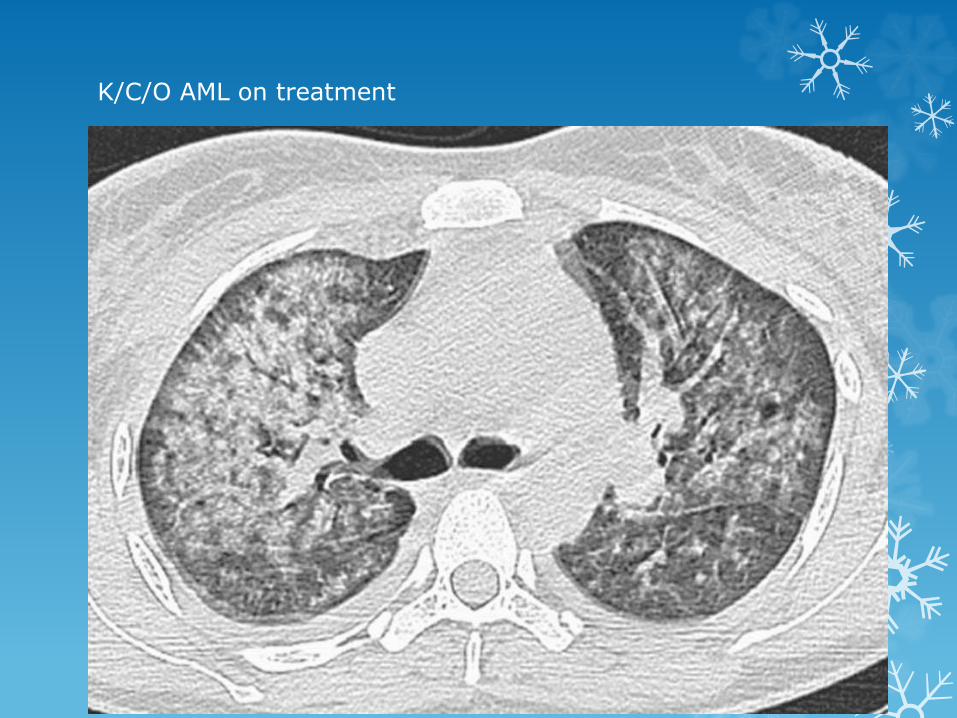
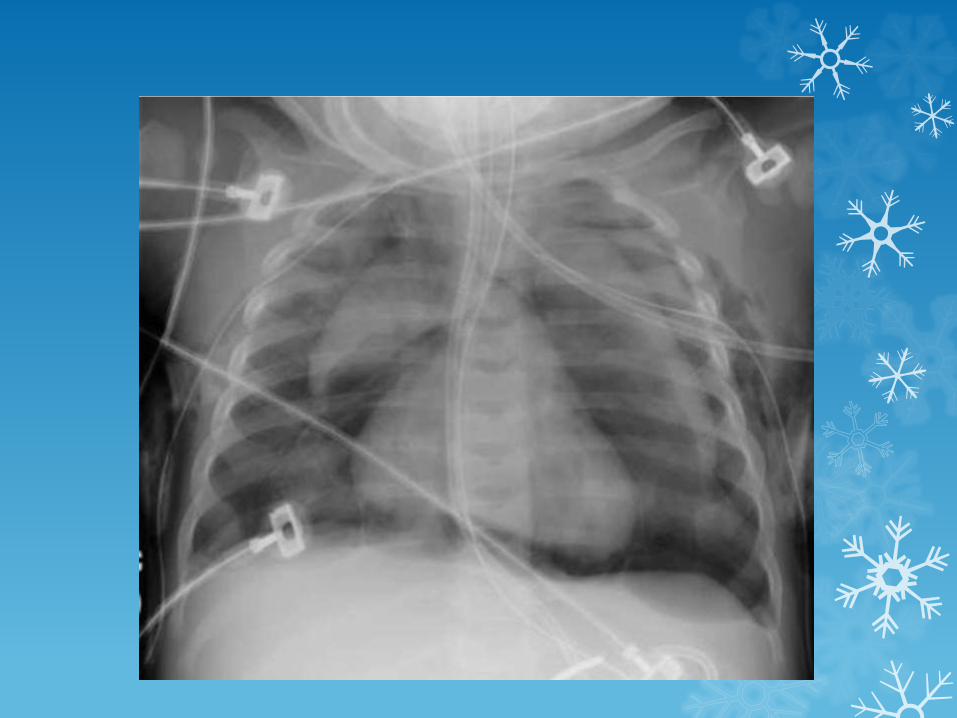
K/C/O AML on treatment
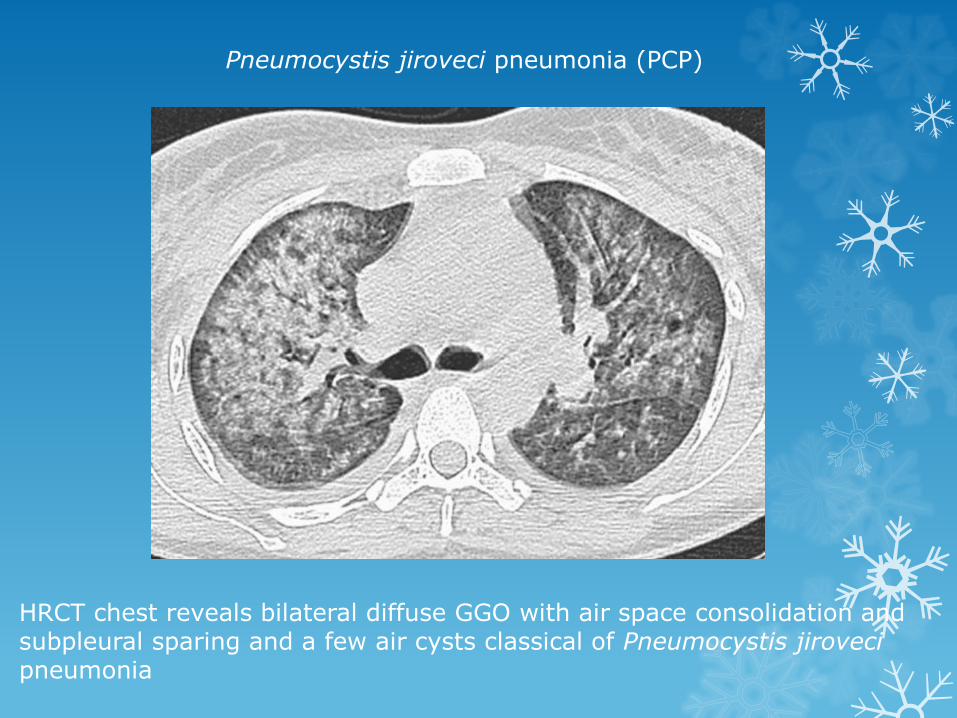
HRCT chest reveals bilateral diffuse GGO with air space consolidation and subpleural sparing and a few air cysts classical of Pneumocystis jirovecipneumonia
Pneumocystis jiroveci pneumonia (PCP)

SPOT 7
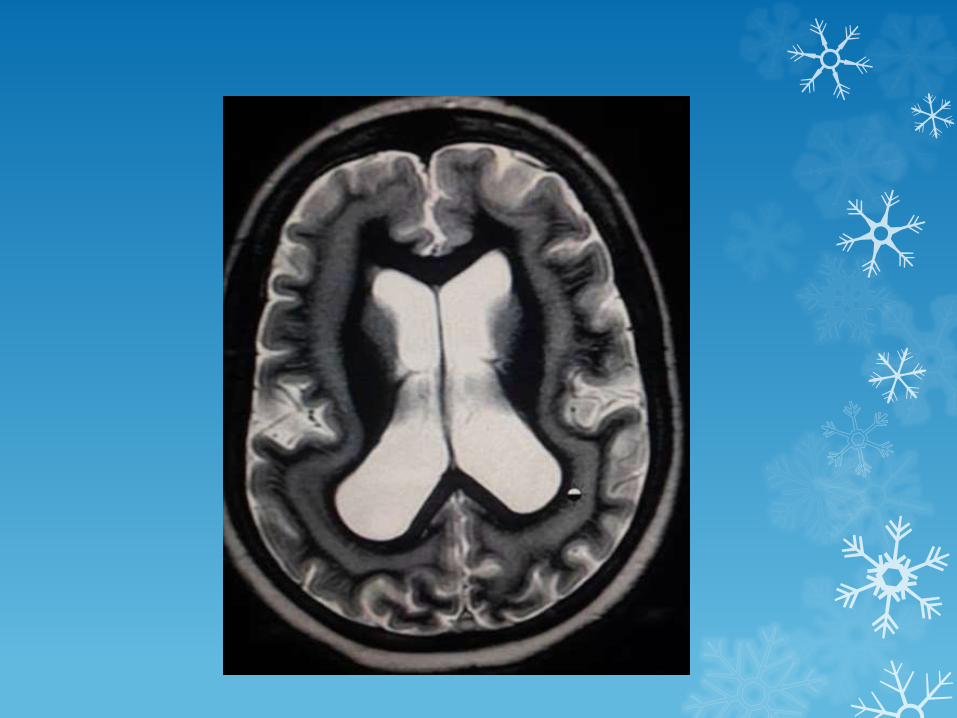
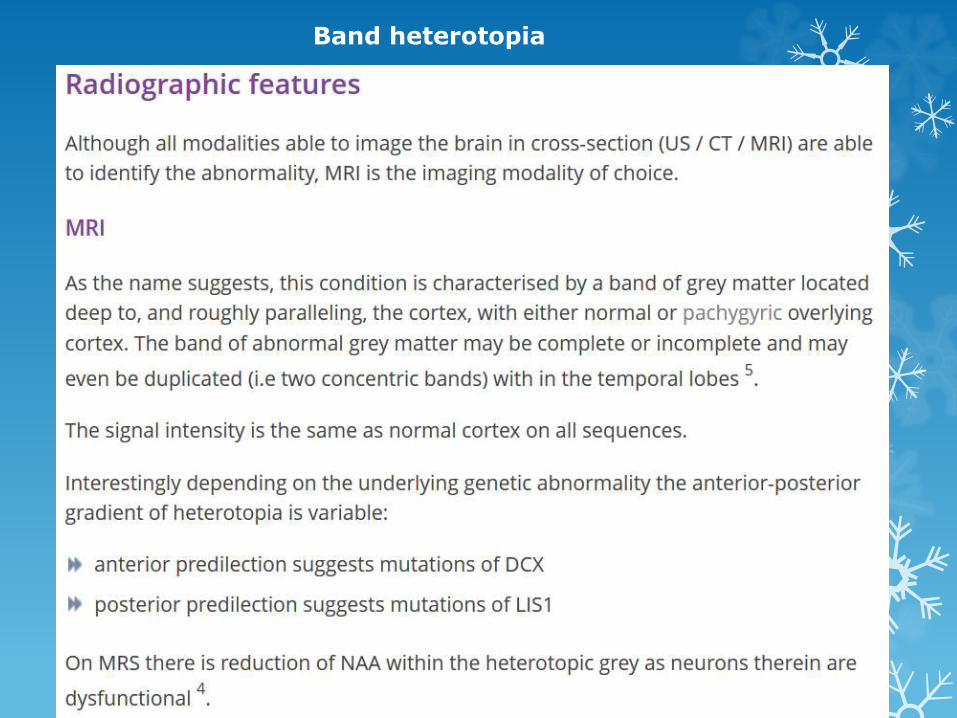
Band heterotopia

SPOT 8


4th ventricle ependymoma

SPOT 9



SPOT 10

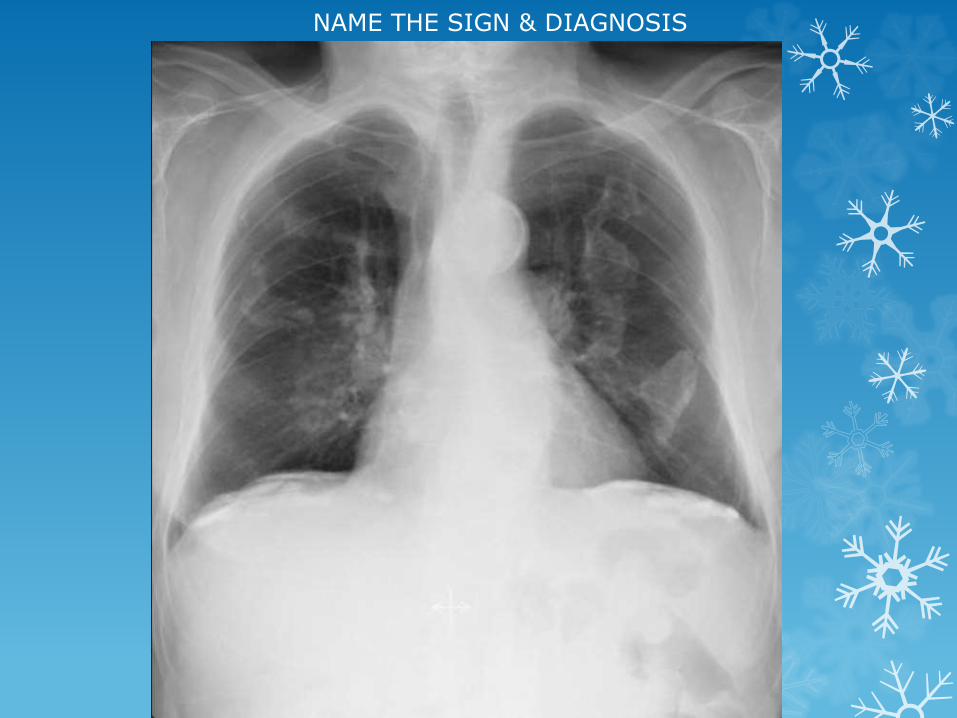
NAME THE SIGN & DIAGNOSIS

Corkscrew sign - midgut volvulus

SPOT 11
NAME THE SIGN & DIAGNOSIS
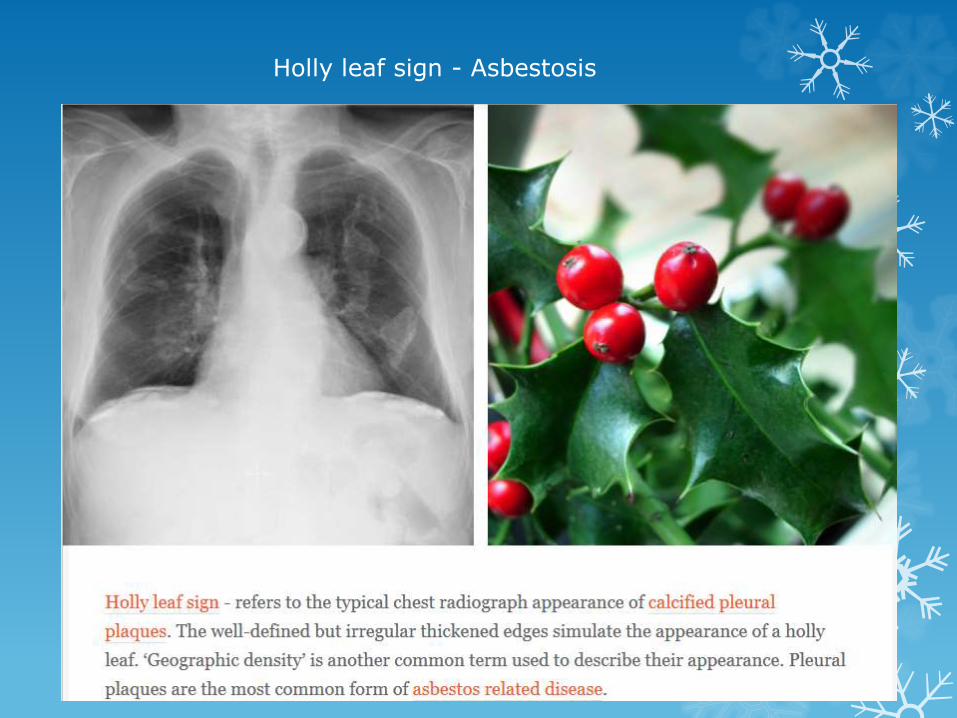
Holly leaf sign - Asbestosis

SPOT 12
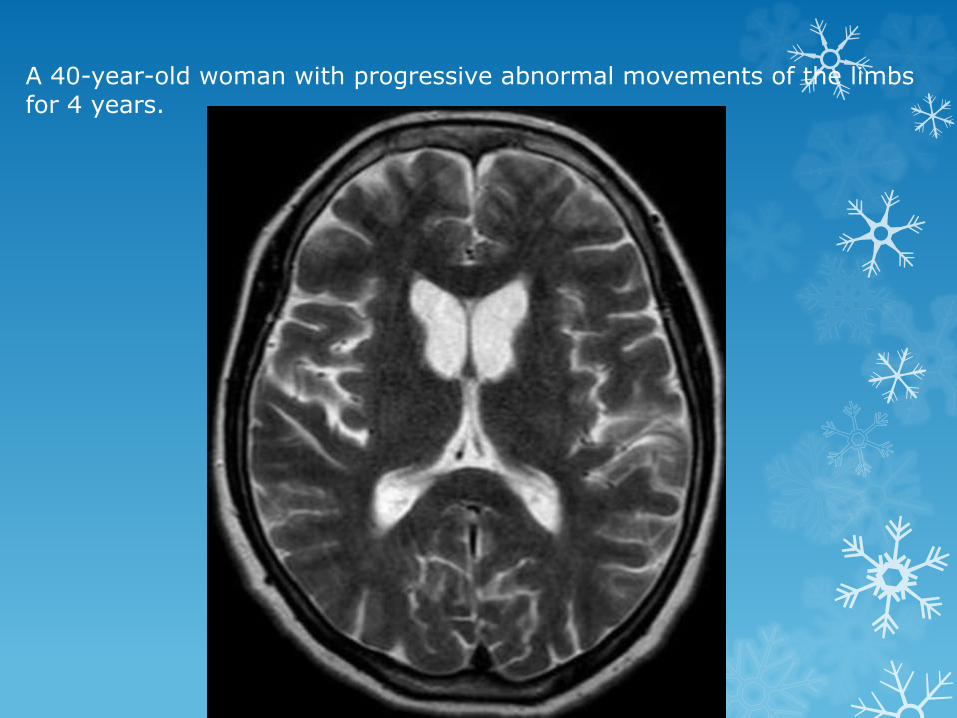
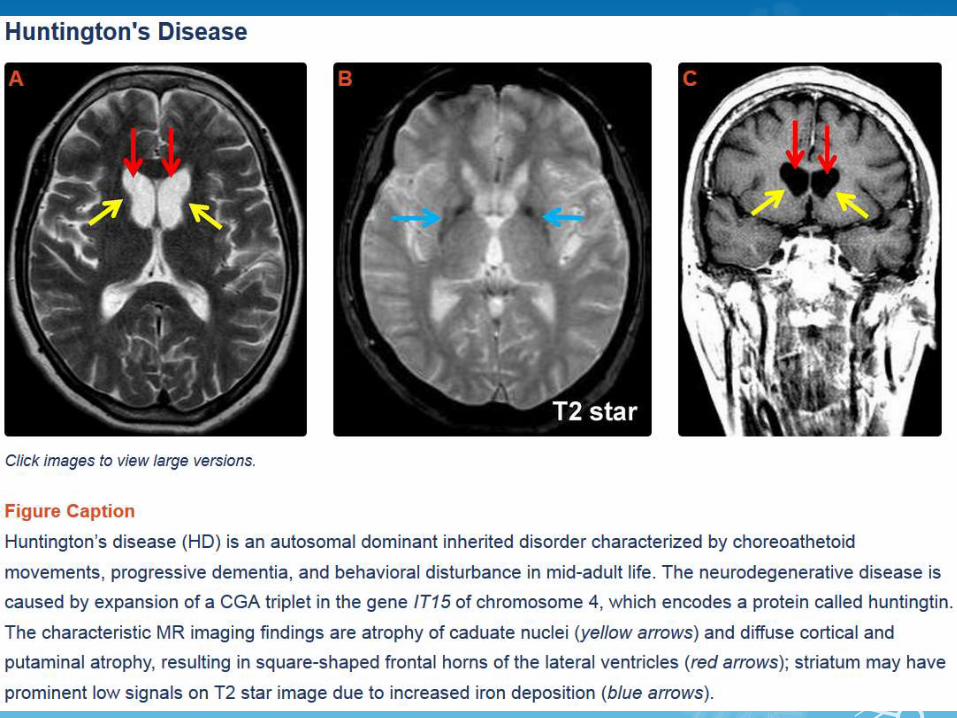
A 40-year-old woman with progressive abnormal movements of the limbs for 4 years.

SPOT 13

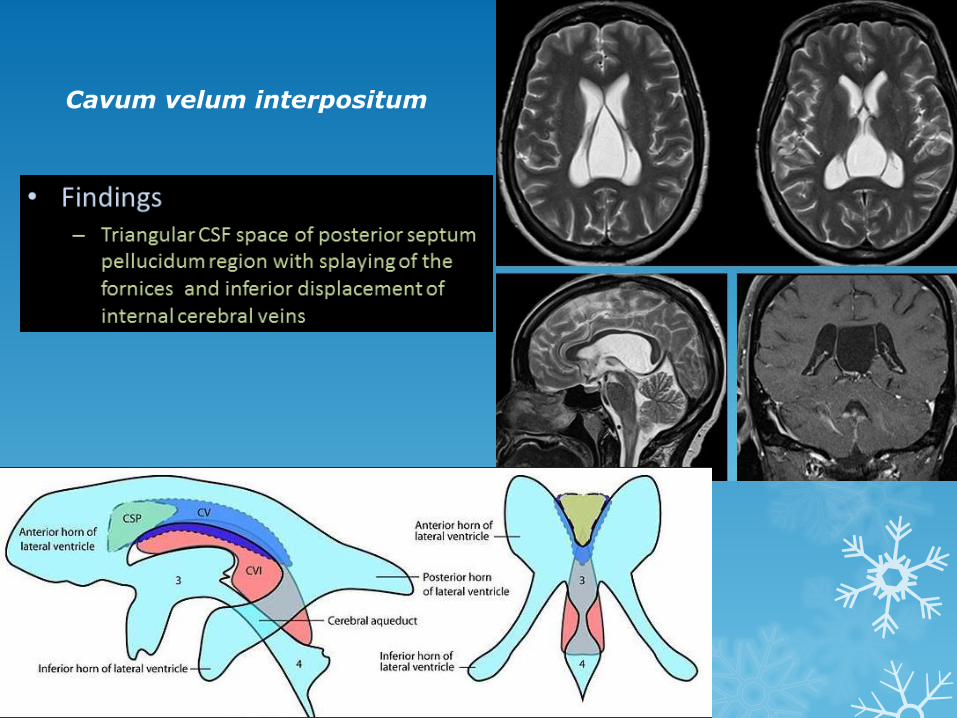
Cavum velum interpositum

SPOT 14
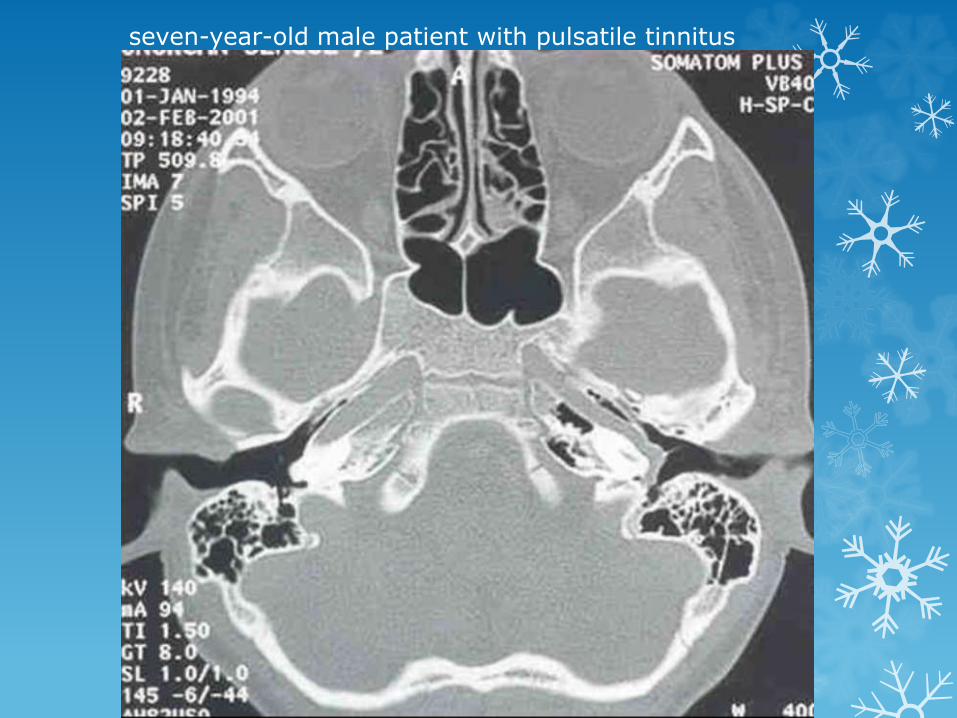
seven-year-old male patient with pulsatile tinnitus

Aberrant internal carotid artery
Some authors suggest that the reason could be the absence of the hypotympanic bony plate because of a congenital failure of ossification. With age, as the artery elongates and becomes tortuous, it protrudes through the defect into the tympanic cavity.
Others suggest that the cervical ICA never develops and an aberrant carotid artery forms when the inferior tympanic artery (a branch of the ascending pharyngeal artery) enlarges to supply the territory of a cervical carotid artery. The inferior tympanic artery runs through the middle ear and then joins the horizontal petrous carotid artery. The so-called aberrant carotid artery is, in fact, the markedly hypertrophied inferior tympanic artery.

SPOT 15

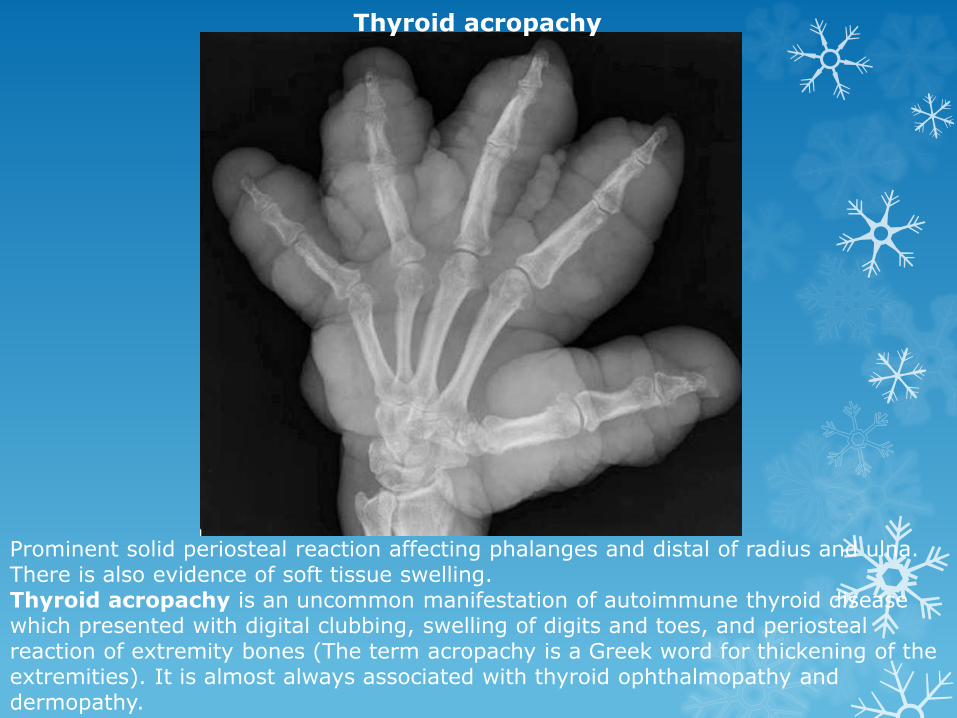
Prominent solid periosteal reaction affecting phalanges and distal of radius and ulna. There is also evidence of soft tissue swelling.Thyroid acropachy is an uncommon manifestation of autoimmune thyroid disease which presented with digital clubbing, swelling of digits and toes, and periosteal reaction of extremity bones (The term acropachy is a Greek word for thickening of the extremities). It is almost always associated with thyroid ophthalmopathy and dermopathy.
Thyroid acropachy

SPOT 16


SPOT 17


Intraorbital Lymphatic Malformation
There is an intraconal multilobulated mass with a fluid-fluid level and mild right globe proptosis.
Vascular lesions account for 5-20% of all orbital masses, and the two most common orbital vascular lesions are venous malformations (formerly known as cavernous hemangiomas) and lymphatic malformations (LM) ( formerly known as lymphangiomas).

Intraorbital venous-lymphatic malformations are present at birth, but tend not to be discovered clinically until early childhood when they enlarge as a result of either intralesional hemorrhage or lymphoid hyperplasia and result in acute proptosis.
Radiologic imaging of intraorbital LMs demonstrates unencapsulated, irregular, lobulated, and multicompartmental masses.
These lesions can have cystic as well as more solid components. The cystic elements of these masses commonly exhibit fluid-fluid levels as a result of intralesionalhemorrhage
Ultrasound images of LMs demonstrate heterogeneous, ill-defined lesions with anechoic cystic portions and extraconal extension.
On CT, these masses exhibit ill-defined borders, irregular attenuations, and variable enhancement with peripheral rim enhancement in cystic regions. Additionally, calcified phleboliths can be seen on CT in venous portions of these lesions.
MR imaging -LMs demonstrate iso- to slightly high signal intensities on T1-weighted images and very high signal intensities on T2-weighted images.

SPOT 18
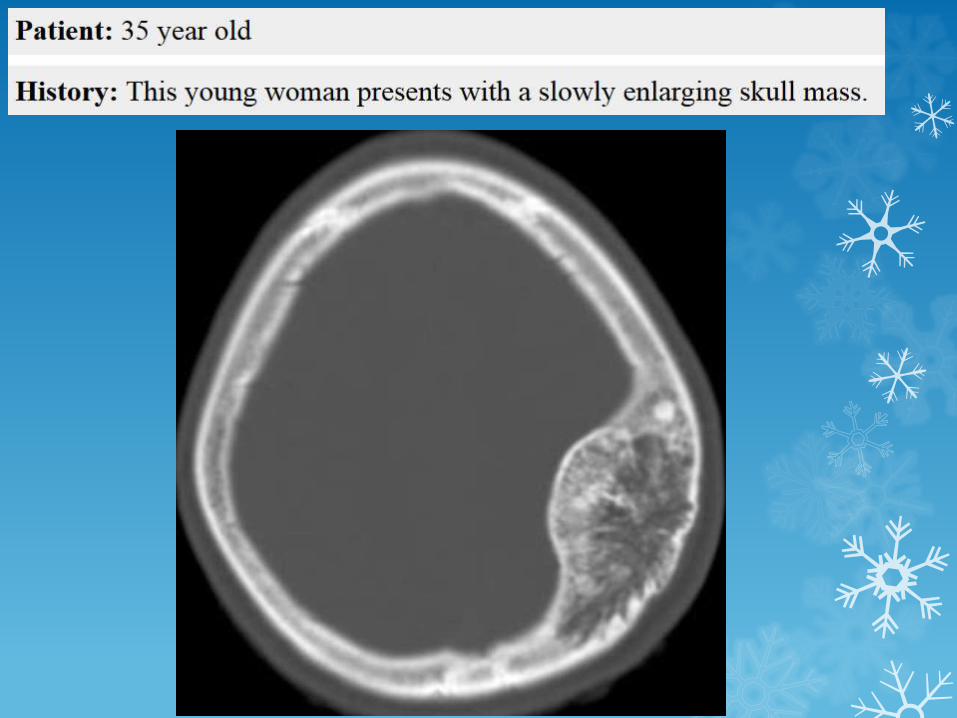

CT reveals a well corticated skull mass with coarse internal trabeculation in a "starburst" arrangement.
Intraosseous Hemangioma of skull

SPOT 19

SPOT 20
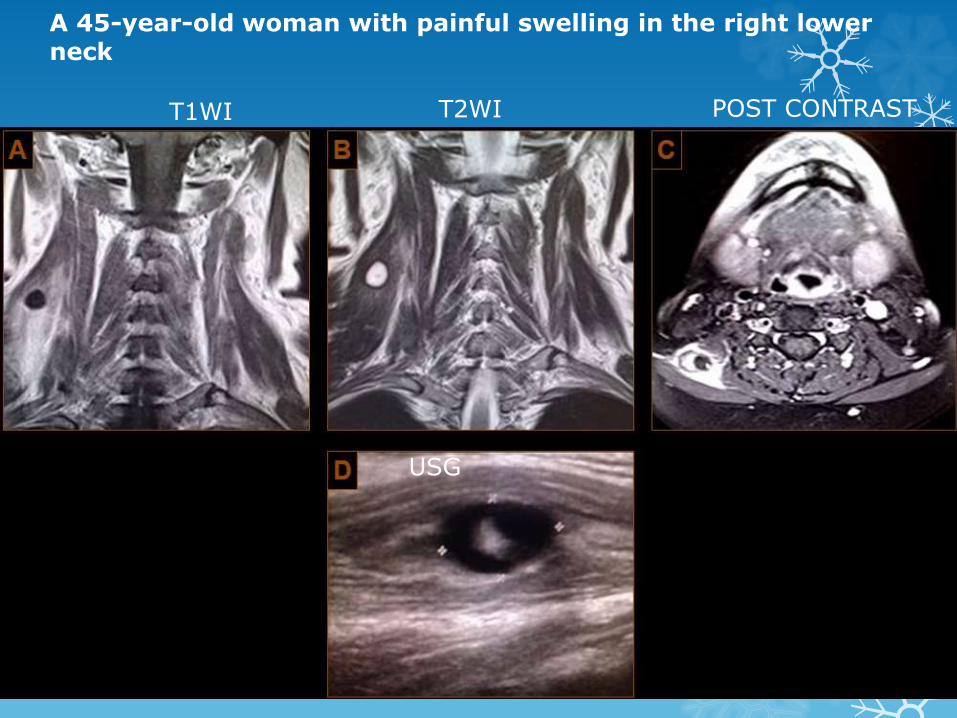
A 45-year-old woman with painful swelling in the right lower neck
T1WI T2WI POST CONTRAST
USG

Levator Scapulae Cysticerosis
Levator Scapulae Cysticerosis

CASE 1

57-year-old patient


CASE 2
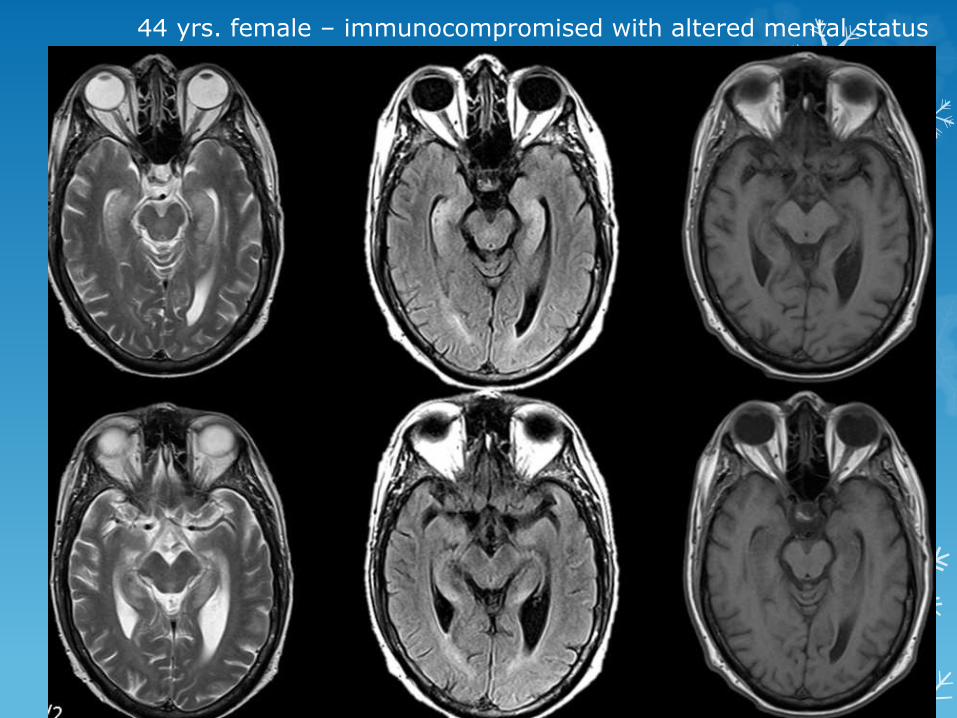
44 yrs. female – immunocompromised with altered mental status



CASE 3
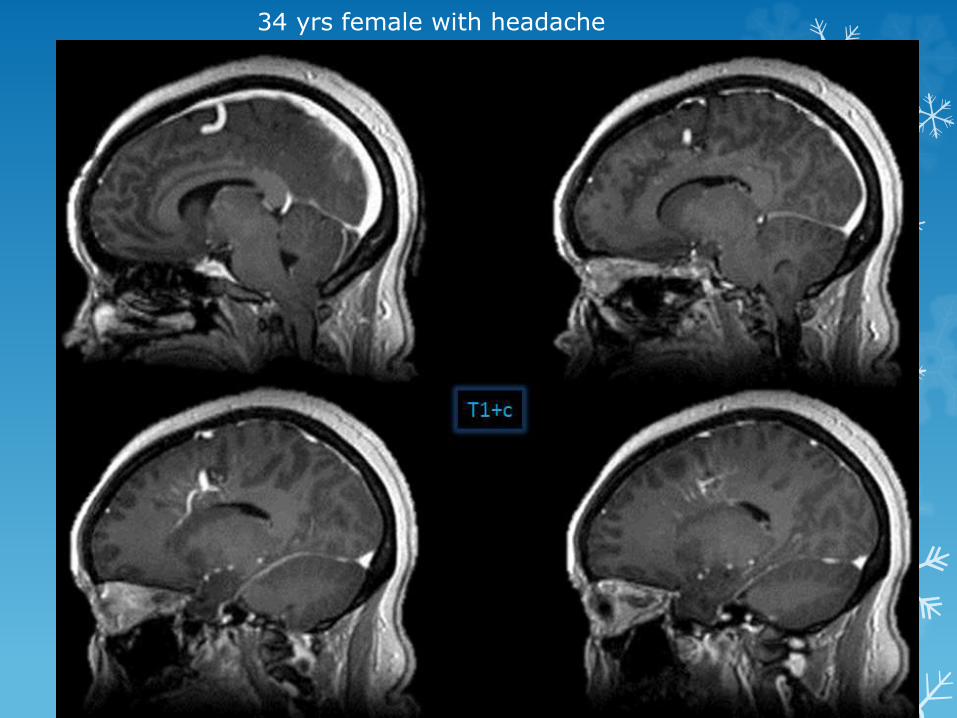
34 yrs female with headache


CASE 4
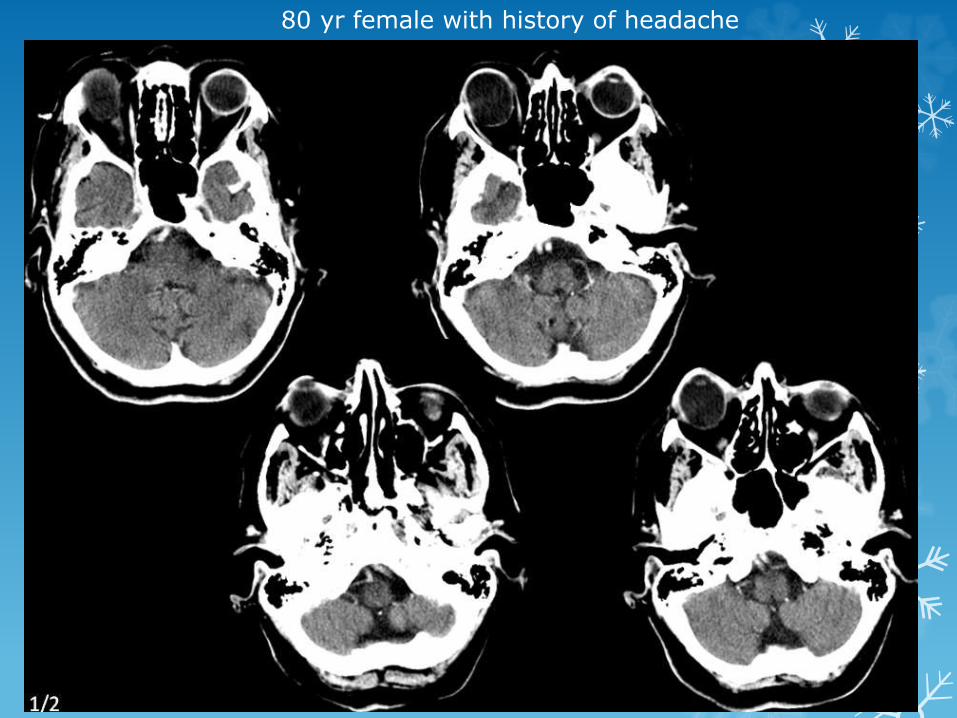
80 yr female with history of headache

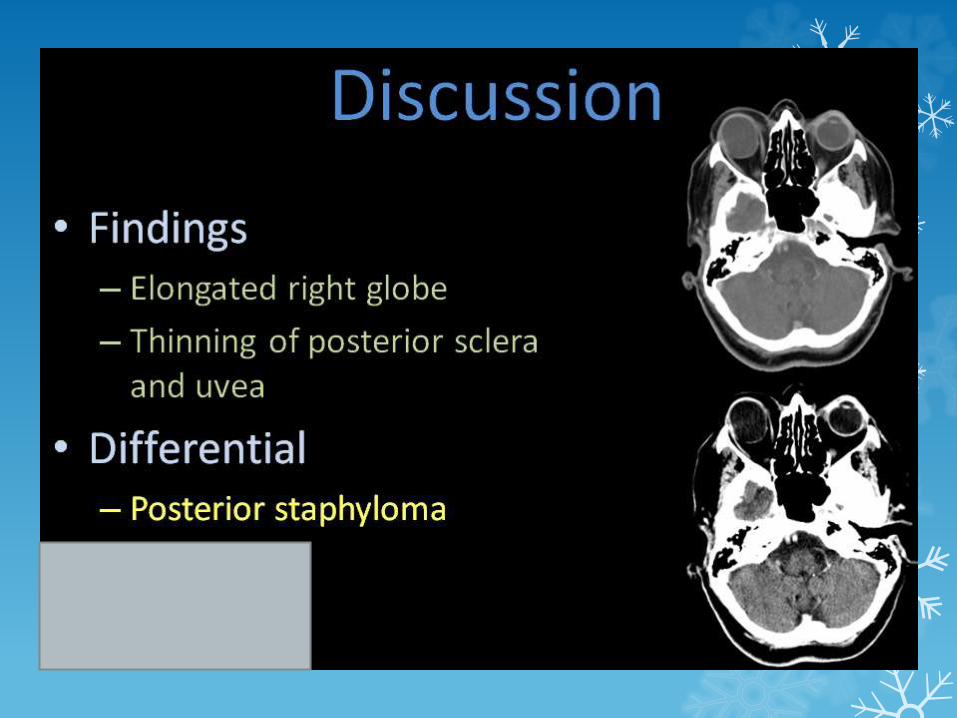

A staphyloma is the term given to an eye whose sclero-uveal coats are stretched (also known as ectasia). This most commonly occurs posteriorly, although anterior staphyloma also is recognised. As opposed to coloboma, staphyloma defect is located off-center from the optic disc, typically temporal to the disc.
A coloboma is collective term encompassing any focal discontinuity in the structure of eye, and should not be confused with staphylomas which are due to choroidal thinning.
CASE 5
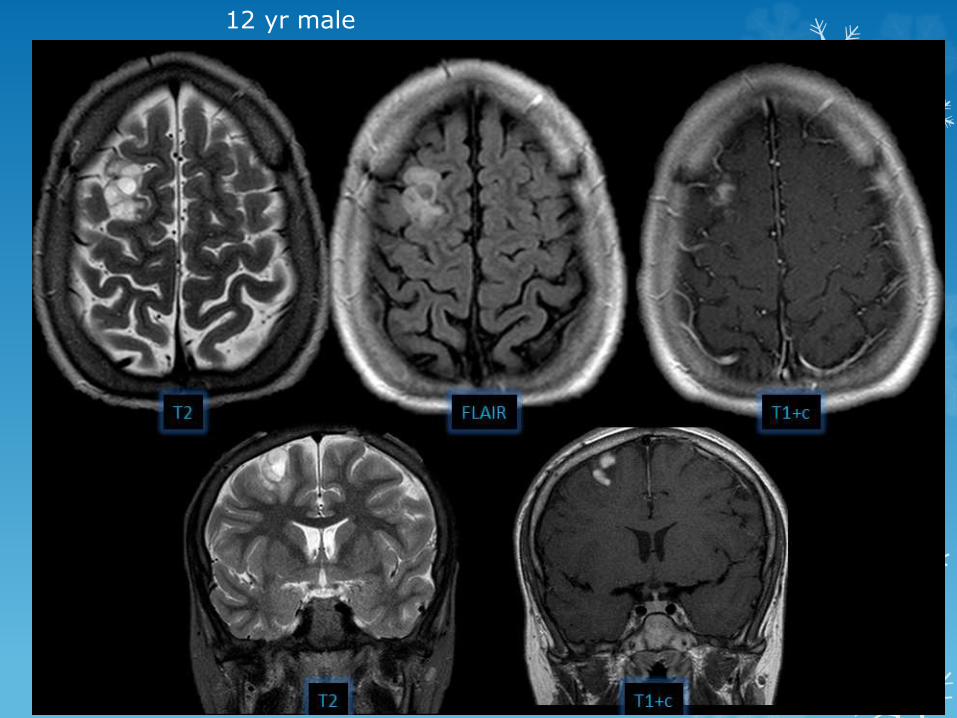
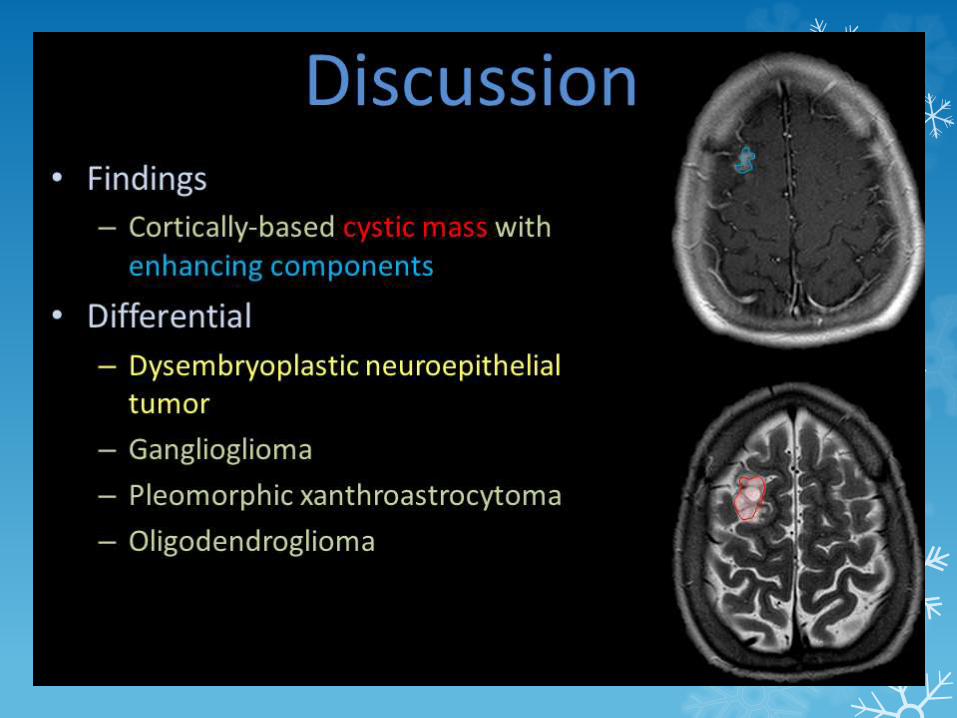
12 yr male

CASE 6

A 7-year-old boy presents with repeated transient ischemic attacks.
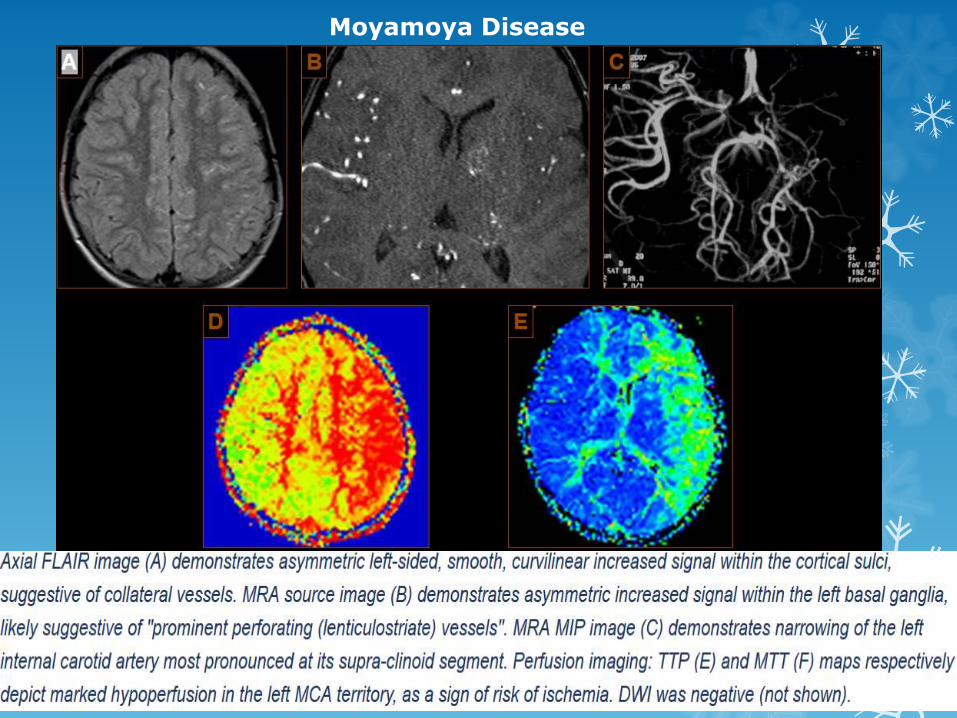
Moyamoya Disease
Moyamoya Disease

THANK YOU