spontaneous and artefitial abortion robin malina jozef záhumenský
TRANSCRIPT

Spontaneous and artefitial abortion
Robin MalinaJozef Záhumenský

HUMAN REPRODUCTION TODAY• Succes of human reproduction is the cause of
overpopulation– This is the greatest hazard to the health and the environmental
and economical future of humankind• One of the momentous social problems worldwide is the
high and increasing number of unwanted pregnancies among teenage girls
• From another vantage point, the problem of human reproduction that haunts many women and men (and their physicians) is relative infertility, which may affect 20percent of couples
• Pregnancy failure caused by embryonic or fetal wastage can occur at every possible step of human reproduction

HUMAN REPRODUCTION TODAY
• the reproductive variables that ordinarily would lead to some sort of reproductive equilibrium include– Age of puberty– Frequency of embryonal or fetal death– Neonatal mortality– The duration of lactation amenorhea
• in humans, these constraints have been modified, even if unwittingly, such that the natural history of reproduction in our species has been diverted by social overlay

Reproduction in primitive societies• the reproductive success of the primitive nomadic
hunter-gatherer !Kung tribe was is contrasted to their relatives who have become farmers
• the nomadic branch of the tribe has fewer infants per woman when compared with the farmers– This likely is due to later childbearing in the nomads
because of lean body mass, which is associated with delayed menarche
– Their prolonged lactation, dictated by their mobility, prohibits quick return to ovulation
– the farmer tribe women can limit lactation because of increased availability of soft food and animal milk for their infants

Reproduction in modern women
• change in body composition and mass favors earlier menarche and ovulation
• Artificial feeding of the newborn, resulting in decreased duration of lactation with associated anovulation and amenorrhea after childbirth
• More frequent and longer infant survival

Reproduction in modern women• Because women in the United States today, on
average, choose to have two pregnancies and to breast feed for only a few weeks, no more than 20 ovarian (menstrual) cycles are eliminated by pregnancy and the anovulation/amenorrhea of lactation. In the absence of pharmacological or surgical intervention, therefore, modern women experience nearly 500 ovulatory cycles, each of which is accompanied by massive progesterone secretion/withdrawal intervals and attendant menstruation, because of their intellectual capacity to choose infertility

Normal duration of pregnancy
• The mean duration of pregnancy calculated from the first day of the last normal menstrual period is very close to 280 days, or 40 weeks
• It is customary to estimate the expected date of delivery by adding 7 days to the date of the first day of the last normal menstrual period and counting back 3 months (Naegele rule)

Abortion• The definition of abortion is the termination of
pregnancy by any means before the fetus is sufficiently developed to survive. In the EU this definition is confined to the termination of pregnancy before 22 weeks based upon the date of the first day of the last normal menses. Another commonly used definition is the delivery of a fetus-neonate that weighs less than 500 g.
• SPONTANEOUS ABORTION– When abortion occurs without medical or mechanical
means to empty the uterus, it is referred to as spontaneous. Another widely used term is miscarriage.

Pathology
• Hemorrhage into the decidua basalis• necrotic changes in the fetal tissues• The retained fetus may undergo maceration• Internal organs degenerate and undergo
necrosis

Etiology
• 80% of abortion occur in the I. trimester– Leading causes are chromosomal anomalies
• 60 percent has chromosomal abnormalities• The risk of spontaneous abortion increases with with maternal
and paternal age• approximately one fourth of chromosomal abnormalities were
due to maternal gametogenesis errors and 5 percent to paternal errors. In a study of fetuses and newborns with trisomy 13, Robinson and colleagues (1996) reported that in 21 of 23 cases, the extra chromosome was of maternal origin
– The most common morphological finding in early spontaneous abortions is an abnormality of development of the zygote, embryo, early fetus, or at times the placenta

Etiology of euploid abortions
• Infections– Toxoplasmosis– Herpes simplex– Ureaplasma urealyticum– Cytomegalovirus– Syphilis (causes late abortions in II. trimester)
• Listeria monocytogenes and chlamydia trachomatis causes no abortions

Etiology of euploid abortions
• Chronic maternal illnes– Severe tuberculosis– Disseminated cancer– Serious hypertension– Hypothyreoidism– IDDM with bad compensation

Etiology of euploid abortions
• DRUG USE AND ENVIRONMENTAL FACTORS.– Tobacco – 14 and more cigarettes daily increases
twofold the risk of abortion– Alcohol - the abortion rate is doubled in women
drinking twice weekly and trebled in women who consumed alcohol daily compared with nondrinkers
– Caffeine - coffee consumption at greater than four cups per day appears to slightly increase the risk of abortion

Etiology of euploid abortions
• DRUG USE AND ENVIRONMENTAL FACTORS– there is evidence that arsenic, lead,
formaldehyde, benzene, and ethylene oxide may cause abortion
• Video display terminals and exposure to the accompanying electromagnetic fields do not increase the risk of abortion (computers, xerox copier, TVs…)

Etiology of euploid abortions
• Immunological factors– Autoimmune factors• Lupus anticoagulans• Anticardiolipin antibodies
– Alloimmune factors• Maternal and paternal HLA comparison

Etiology of euploid abortions
• Inherited factors– Inherited trombophilias– Developmental uterine dephects• Uterus septus

Categories of spontaneous abortions
• THREATENED ABORTION (abortus imminens)– The clinical diagnosis of threatened abortion is
presumed when any bloody vaginal discharge or bleeding appears during the first half of pregnancy.
– It is an extremely commonplace occurrence, and one out of four or five women has vaginal spotting or heavier bleeding during early gestation.
– Of those women who bleed in early pregnancy, approximately half will abort.

Categories of spontaneous abortions
• INEVITABLE ABORTION (abortus in cursu)– Inevitability of abortion is signaled by gross
rupture of the membranes in the presence of cervical dilatation. Under these conditions, abortion is almost certain
• INCOMPLETE ABORTION (abortus incompletus)– When the placenta, in whole or in part, is retained
in the uterus, bleeding ensues sooner or later, to produce the main sign of incomplete abortion.

Categories of spontaneous abortions
• MISSED ABORTION – This is defined as retention of dead products of
conception in utero
• RECURRENT ABORTION (abortus habitualis)– three or more consecutive spontaneous abortions
• SEPTICAL ABORTION – Misscariage complicated with inflamation and
signs of general infection
Artefitial (induced) abortion
• Induced abortion is the medical or surgical termination of pregnancy before the time of fetal viability
• About 88 percent of abortions were performed before 13 weeks, 55 percent before 8 weeks, and 16 percent at 6 weeks or less.

Legal aspects – Czech republic
• Before end of the 12 weeks of pregnancy – social indication (maternal choice)
• Before end of the 24 weeks of pregnancy – medical indication – fetal or maternal disease with parental agreement– CAVE – fetus over 500 g – BIRTH not ABORTION
• Everytime – Maternal indication – live threating conditions

Indications
• When continuation of pregnancy may threaten the life of the woman or seriously impair her health
• When pregnancy has resulted from rape or incest
• When continuation of pregnancy is likely to result in the birth of a child with severe physical deformities or mental retardation

ELECTIVE (VOLUNTARY) ABORTION
• Elective or voluntary abortion is the interruption of pregnancy before viability at the request of the woman but not for reasons of impaired maternal health or fetal disease. Most abortions done today fall into this category.
• The number of the interruption in Czech republic is continually decreased
Abortion techniques
• Surgical procedures– Dilatation of internal oss and vacuumexpiration or
currettage
• Medical procedures– Prostaglandins – Antiprogestins – Metothrexate

Counseling before Elective Abortion
• Three choices available to a woman considering an abortion
• include continued pregnancy with its risks and parental responsibilities;
• continued pregnancy with its risks and responsibilities of arranged adoption;
• or the choice of abortion with its risks.• Knowledgeable and compassionate counselors should
objectively describe and provide information about these choices so that a woman or couple can make an informed decision.

• Techniques for Early Abortion• Abortion can be performed either
medically or surgically as shown in
Table 6-6.
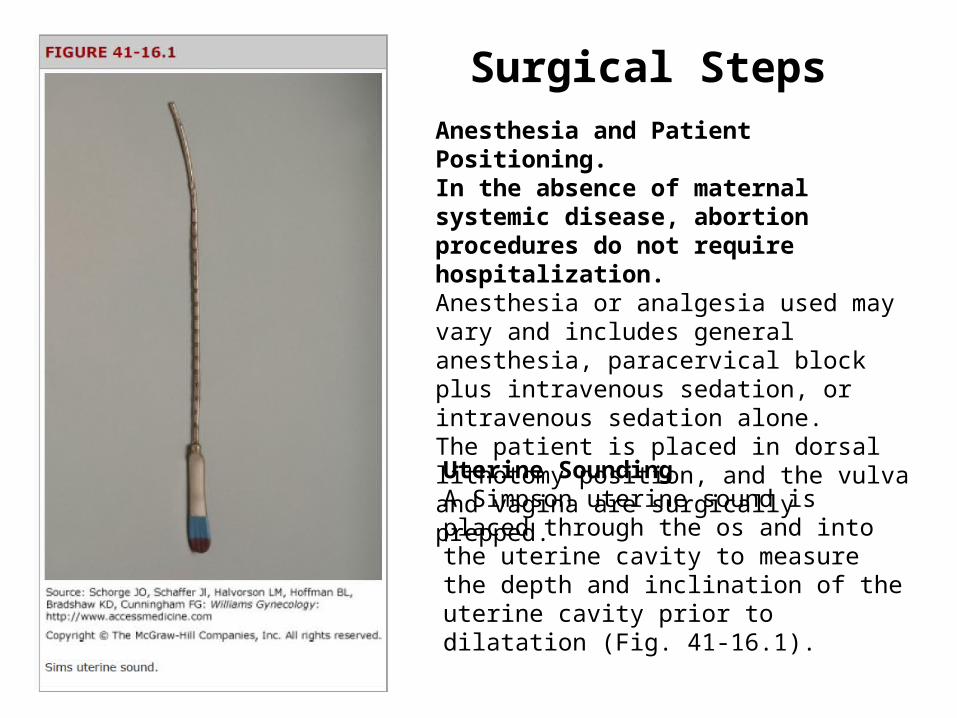
Surgical StepsAnesthesia and Patient Positioning. In the absence of maternal systemic disease, abortion procedures do not requirehospitalization. Anesthesia or analgesia used may vary and includes general anesthesia, paracervical block plus intravenous sedation, or intravenous sedation alone. The patient is placed in dorsal lithotomy position, and the vulva and vagina are surgically prepped.
Uterine Sounding A Simpson uterine sound is placed through the os and into the uterine cavity to measure the depth and inclination of the uterine cavity prior to dilatation (Fig. 41-16.1).


Cervical Dilatation. A Graves speculum is placed in the vagina to allow access to the cervix. In cases of incomplete or inevitable abortion, the cervical os already will be dilated. Alternatively, metal Pratt, Hegar, or Hank dilators (Fig. 41-17.4) of sequentially increasing diameter are placed through the external and internal os to gently dilate the cervix. The uterus is especially vulnerable to perforation during this step. For this reason, the metal dilator should be grasped as one would apencil. The heel of the hand and fourth and fifth fingers rest on the perineum and buttock. Gentle pressure from only thethumb and first two fingers is used to push the dilator through the cervical os (Fig. 41-17.5).

Uterine Evacuation. The cannula is inserted through the open cervix and into the endometrial cavity. The suction unit is turned on, and uterine contents are removed. The suction cannula is moved toward the fundus and then back toward the os and is turned circumferentially to cover the entire surface of the uterine cavity.Tissue is collected in a container at the distal end of the tubing and is sent for pathologic evaluation to exclude hydatidiform mole. Occasionally, the Karman cannula may become obstructed with excess tissue. The suction unit is turned off prior to cannula removal. Once the cannula opening is cleared of obstructing tissue, it may be reinserted, and curettage completed.

Sharp Curettage. Although no more tissue is aspirated, a gentle curettage should follow to remove any remaining placental or fetal fragments

Postoperative
Recovery from suction D&C is typically fast and without complication. Patients may resume normal activities as they desire, but abstinence from intercourse usually is encouraged during the first 2-3 weeks following surgery.
Ovulation may resume as early as 2 weeks after an early pregnancy ends. Therefore, if contraception is desired, methods should beinitiated soon after abortion.