spinal trauma: the legend of the c-spine collar - a case report
TRANSCRIPT

Spinal Trauma:The Legend of the C-Spine Collar
Trauma Grand Rounds 14/04/15
Dr Emma McVeighEmergency Medicine Registrar

Case Report
27 year old female presents 18/7 post high speed ski injury in Japan
c/o persistent central intrascapular pain worse on lifting
Denies any focal or peripheral neurology Systemically well

Mechanism/ Hx of Injury
Injury at approximately 60kph Hyperflexion injury with axial loading c/o “excruciating 10/10 pain” at time of injury over cervical and thoracic
spine No paraesthesiae/ No weakness Patient mobilised 10min post-injury and continued to ski down slope C/o severe intermittent pain localised Cervico-Thoracic junction over
next 1/52 Some relief from simple analgesia Continued to ski again 2/7 post injury Went surfing twice Returned to work for 2/52 in a physical occupation

HxPc
Urged to present to ED on the advice of friends due to persistent pain
Maximal pain over T1 post lifting/mobilising lasting for several hours
Intermittent Naproxen 1000mg SR provided relief No paraesthesia No weakness No incontinence

O/E:
Vitals: Stable GCS: 15 Mobilising No focal neurology No peripheral neurology Tender to palpation over cervico-thoracic
junction to mid-thoracic spine All other examination grossly normal



Epidemiology
US 10,000 Spinal fractures/ year Peak incidence 15-35yo, 61%Male Associated w/ RTAs and Sports injuries USA nationwide study 8634 spinal fractures 2000-2008 Alpine tertiary centre 728 fractures 2000-2006
– Subluxation/dislocation 73 patients Skiers = C-spine Vs Snowboarders= Lumbar
– Cervical 19.6%– Thoracic10.9%– Lumbar 6%

Anatomy of the Spine
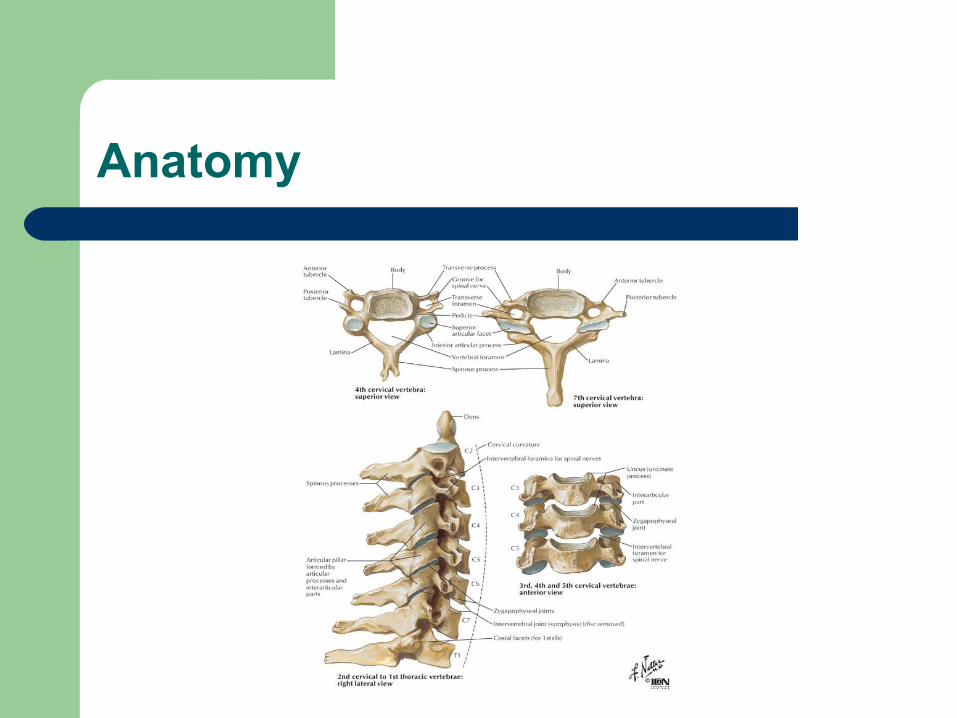
Anatomy

Anatomy

Classification
Flexion injury Flexion – Rotation injury Extension injury Vertical (Axial) Compression Injury Multiple or complex injuries

Stable Vs Unstable
Most important concept is that of “stability”White et Al.
Definition of Instability:“The loss of ability of the cervical spine under physiological loads to maintain relationships between the vertebrae in such a way, that spinal cord or nerve roots are not damaged or irritated and deformity or pain does not occur”Leemans and Calder 2012
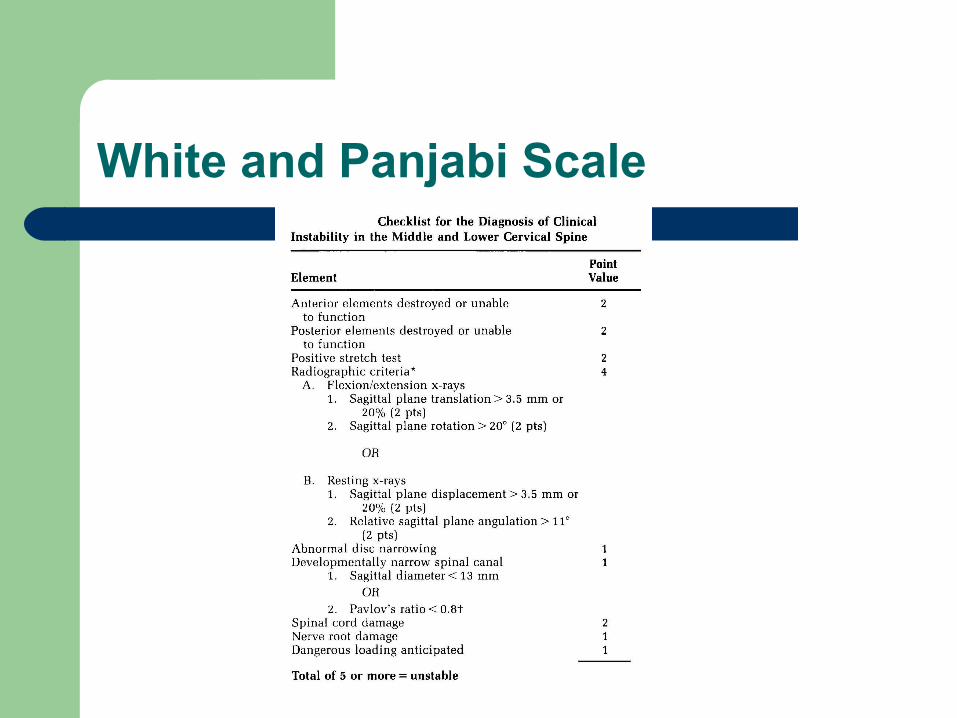
White and Panjabi Scale


An Approach to the Spinal Patient
1) Full spinal immobilization care until cleared
2) Detailed Hx and Exam Mechanism of injury Speed Other injuries
1) CT C-Spine (High Resolution)
2) Formal Radiologist/Orthopaedic/Neurosurgical opinion
3) Any doubt High risk injury / Neuro deficit MRI CT Abnormal MRI Normal Clear C-Spine

American Spinal Association Impairment Scale (ASIA)
Assessment of Potential C-spine Injury
Canadian c-spine rules
Nexus c-spine rules



C-Spine X-rays
A standard series of X-rays of the cervical spine consists of three views:– AP– Lateral – AP odontoid peg
Lateral view must show the top of the T1 vertebral body Odontoid peg view should show the lateral masses of the atlanto-axial articulation
In children aged <10, use a AP and lateral radiographs, No peg view CT imaging to clarify abnormalities or uncertainties
Indications: – Patients with neck pain or midline tenderness if aged ≥65 years– Any age if there was a dangerous mechanism of injury – Definitive diagnosis of cervical spine injury is needed urgently (eg, before surgery)– Any patients where it is considered unsafe to assess movement.

C-spine CT Scanning
CT scan is indicated immediately if: – GCS <13– Intubated– Multi-region trauma
CT is also indicated: – If plain films are inadequate/suspicious/definitely abnormal– High clinical suspicion
CT is superior to plain radiography– Sensitivity: 100%– Specificity: 99%.

C-spine MRI Scanning
Soft tissue structures
Intervertebral disc injury– Sensitivity: 93%
Posterior longitudinal injury– Sensitivity: 93%
Interspinous Ligament injury – Sensitivity: 100%
MRI is indicated for patients with neurological signs, even if plain films are negative
MRI can distinguish haematoma from oedema

Complications
Paralysis Neurogenic Shock Respiratory Failure Thrombosis Haemorrhage Infection Autonomic Hyper-reflexia

Case Report
Diagnosis of: – C7 Fracture
– T1 Spinous Process Fractures
– T7 Vertebral Body Compression Fracture

Initial Management
Full C-spine Precaution
Neurology Examination: Normal
4-hourly Neuro Observation
Further imaging including CT Cervical/Thoracic Spine and MRI Spine




Definitive Management
Transfer to RPH Spinal Unit in full spinal precautions awaiting Spinal Review
Initial decision for C7/T1 Fusion Remained in full spinal precaution 4.5/7 S/B Spinal Consultant 5/7 post diagnosis Decision for conservative mx in Thoracic
Aspen collar


Discussion: When can we clear the c-spine?
Controversial issue
C-spine clearance can be clinical +/- Radiological
Treatments are vastly different – Stability
Until patients are cleared they must be immobilized in a hard-collar, in line stabilisation and log rolled

Hard collars
Use of hard-collars is standard of care – Fear of not using the collar in undx SCIs or
worse….being judged by colleagues

Evidence?

Why do we use the collar?
American Association of neurological surgeons– Guidelines mandate use of hard collar– 1970s full Neurological Lesions 55%– In 1980s Partial lesion 61%.......at same time as
hard collars introduced
Correlation vs Causality

But it’s a harmless intervention…
Ulcers Raised ICP – ‘Brain tourniquet’ Actually could make fractures worse Intoxicated patient Airway management Painful Increased cost and time
– 4hr rule…

Is it harmful?
Myths of the cervical collar…1. Injured patients may have an unstable injury of the
cervical spine2. Further movement of the c-spine could cause addition
damage to the spinal cord over and above that already caused by the initial trauma
3. The application of a semi-rigid collar prevents potentially harmful movements of the c-spine
4. Immobilisation of the c-spine is a relatively harmless measure and can therefore be applied to a large number of patients with a relatively low risk of injury “as a precaution”.

Take Home Message…….
Mechanism of injury should arouse suspicion – i.e. falling while skiing at 60kph Vs tripping over
your shoelaces
Knowledge of anatomy and the concept of stability
Ax rules are useful but not very specific, a senior clinician’s gestalt is all important
The hard collar is not the be all and end all

THM cont…
Don’t transfer a trauma patient to RPH the same week as FSH changeover….
Don’t go skiing with two other emergency registrars…



THANKS!!!
References
[1] Sanders KM1, Seeman E, Ugoni AM, Pasco JA, Martin TJ, Skoric B, Nicholson GC, Kotowicz MA.Age- and gender-specific rate of fractures in Australia: a population-based study. Osteoporosis
International. 1999; 10 (3) 240-7
[2] Hubbard M.E., Jewell R.P., Dumont T.M., Rughani A.R. (2011). Spinal injury patterns among skiers and snowboarders. Neurosurgical FOCUS. Nov 2011; 31: 5
[3] White AA 3rd, Johnson RM, Panjabi MM. Biomechanical analysis of clinical stability in the cervical spine. Clin Orthop. 1975;(109):85-96. [Medline].
[4] Leemans and Calder. The Unstable Cervical Spine. In: (eds) Johnston I, Harrop-Griffiths W. and Gemmell L. AAGBI Topics in Anaesthesia 2012. Chichester, UK: Wiley-Blackhall 2012 p88-104
[5] Sundstrøm T, et al. Prehospital use of cervical collars in trauma patients: a critical review.Review article J Neurotrauma. 2014
[6] Wee B, Reynolds JH, Bleetman A; Imaging after trauma to the neck. BMJ. 2008 Jan 19;336(7636):154-7. Triage - assessment - investigation and early management of head injury in infants, children and
adults; NICE Clinical Guideline (September 2007)

Questions