75 - spine trauma and spinal cord injury - semantic … · 645 spine trauma and 75 spinal cord...
TRANSCRIPT

645
75 Spine Trauma and Spinal Cord Injury
Michelle Lin and Swaminatha V. Mahadevan
PATHOPHYSIOLOGY
In the setting of spinal trauma, the bone, ligaments, spinal cord, and vascular structures may be injured. Anatomically, the vertebral bony spine can be divided into structural columns. The cervical spine is traditionally divided into two columns—anterior and posterior. The anterior column consists of the load-bearing vertebral bodies, intervertebral disks, anterior longitudinal ligament, and posterior longitudinal ligament (Fig. 75.1). The posterior column consists of the more poste-rior structures, including the pedicles, laminae, and transverse and spinous processes (Fig. 75.2).
In contrast, the thoracic and lumbar vertebral spines are divided into three columns based on the modified Denis model—anterior, middle, and posterior (Fig. 75.3). The anterior column consists of the anterior longitudinal ligament, the anterior two thirds of the vertebral body, and the interver-tebral disk. The middle column consists of the posterior longitudinal ligament, the posterior third of the vertebral body, and the intervertebral disk. Any disruption of the middle column predisposes a patient to significant spinal cord injury because the middle column abuts the spinal canal. The posterior column consists of the remaining posterior structures.
The C1 and C2 vertebrae are anatomically unique (Fig. 75.4). C1 (atlas) is a ring-link structure without a vertebral body. It articulates superiorly with the occipital condyles. This articulation allows 50% of normal neck flexion and extension. C2 (axis) projects the dens superiorly to articulate with C1. The transverse ligament tethers the dens to the anterior arch of C1. This atlantoaxial articulation allows 50% of normal neck rotation left and right.
The spinal cord spans from the foramen magnum to the L1 level, whereupon the spinal cord tapers into the conus medul-laris and cauda equina, a collection of peripheral lower lumbar and sacral nerve roots. Because the spinal cord is thickest in the cervical spine, there is relatively less spinal canal space in the cervical levels than in the thoracic or lumbar spine. Thus spinal cord injuries occur more frequently with cervical spine trauma than with thoracic or lumbar spine trauma. The neurologic dermatomes can help localize the injury (Table 75.1).
The vertebral arteries branch off the subclavian arteries and course superiorly within the transverse foramina of C2 to C6. These arteries then merge to form the basilar artery.
• Patientswithspinalpainandspinefracturesshouldreceiveathoroughneurologicexaminationtolookforspinalcordinjury.
• Spinefracturesareassociatedwithahighincidenceofconcurrentnoncontiguousspinefracturesandspinalcordinjuries.
• TheNationalEmergencyX-radiographyUtilizationStudycriteriaortheCanadianCervical-SpineRulecriteriacanbeusedtoidentifylow-riskpatientswhodonotneedcervicalspineimaging.
• Imagingwithplainfilmsversuscomputedtomographyofthecervicalspineshouldbebasedonthepretestprobabilityofasignificantinjuryandtheirradiationriskwithcomputedtomography.
• Spinalshock,ortransientphysiologictransectionofthespinalcordasaresultoftrauma,isdifferentfromneurogenicshock,whichisphysiologicsympathectomyoftheupperspinalcordleadingtoperipheralvasodilation.
• Patientswithaspinalcordinjurycausedbyblunttraumaareoftengivenhigh-dosecorticosteroidswithin8hoursofinjury,althoughsuchtherapyiscontroversial.
KEY POINTS
EPIDEMIOLOGY
The estimated annual cost of spine injuries, including inability to work and health care costs, exceeds $5 billion in the United States.1
In the emergency department (ED), all trauma victims are screened for vertebral fractures, ligamentous disruptions, and spinal cord injuries because of the potentially devastating neurologic consequences of overlooking these injuries. Patients with a delayed diagnosis of spinal fracture are 7.5 times more likely to sustain secondary neurologic deficits.2 Neurologic deficits from spinal cord injury may be subtle and can easily be missed if not specifically evaluated. Adding to these difficulties, plain film radiographs of the spine, though an adequate screening tool for other fractures, can miss 23% to 42% of cervical spinal fractures3,4 and 13% to 50% of lumbar fractures.5,6

SECTION VIII TRAUMATIC DISORDERS
646
Patients with spinal cord injuries may have a spectrum of findings ranging from subtle neurologic deficits to grossly obvious paralysis. Spinal cord injuries should be suspected in any trauma victim who complains of neck or back pain, espe-cially pain exacerbated by movement. Neurologic symptoms suggesting spinal cord injury include numbness, tingling, par-esthesias, focal weakness, and paralysis. Other worrisome symptoms include urinary or fecal incontinence and urinary retention. Unconscious patients and those with impaired con-sciousness secondary to intoxication may harbor occult spinal cord injuries. Physical examination should focus on the spine and areas where associated injuries may occur (Tables 75.2 to 75.4).
PRESENTING SIGNS AND SYMPTOMS
Patients with vertebral fractures usually have significant midline spinal tenderness on palpation. High-risk findings include spinal soft tissue swelling, ecchymosis, and step-off misalignment of the spine. Pain radiating along a dermatomal distribution suggests an associated radiculopathy. Thoracic spine fractures are uncommon because the articulating ribs provide stability to the spinal column; however, the thoraco-lumbar junction (encompassing the T10 to L2 vertebral levels) is commonly injured because the spine curvature changes from the kyphotic thoracic spine to the lordotic lumbar spine.
Fig. 75.1 Bony anatomy of a typical lower cervical vertebra (C3-C7): superior axial view with the anterior aspect oriented upward and the posterior aspect oriented downward.
Spinous process
Lamina
Spinal canal
Superior articular facet
Pedicle
Transverse process
Transverse foramen
Lower cervical spine
Vertebral body
Nucleus pulposus(disk)
Annulus fibrosus(disk)
Fig. 75.2 Bony anatomy of a typical thoracic and lumbar vertebra (T1-L5): superior axial view with the anterior aspect oriented upward and the posterior aspect oriented downward.
Spinous process
Lamina
Spinal canal
Superior articular facet
Pedicle
Transverse process
Vertebral body
Thoracic/lumbar spine
Nucleus pulposus(disk)
Annulus fibrosus(disk)
Fig. 75.3 Schematic diagram illustrating the lateral view of the anatomic columns of the cervical and thoracic/lumbar spine.Notethatthecervicalspine’santeriorcolumniscomposedofthesamestructuresasthethoracic/lumbarspine’santeriorandmiddlecolumns.
Vertebral bodyIntervertebral disk
Spinous processTransverse processSpinal canal
Cervical spine columns:
Thoracic-lumbar spinecolumns
Anterior Posterior
PosteriorMiddleAnterior
Fig. 75.4 Bony anatomy of the upper cervical spine (C1 and C2): posterolateral view.TheC1lateralmassesarticulatewiththeoccipitalcondyles.TheC2densprojectscephalad,articulateswiththeC1anteriorarch,andisstabilizedbytheC1transverseligament.
Spinous process
Transverseligament
Superior articular facet
Transverse processTransverse foramen
Pedicle
Dens
Lateral mass
Transverse processTransverse foramen
Anterior archC1 atlas
C2 axis
Posterior arch

Table 75.1 Individual Spinal Sensory Dermatomes, Motor Function, and Reflex Arcs
SPINAL LEVEL SENSORY DISTRIBUTION MOTOR FUNCTION REFLEX
C2 Occiput
C3 Thyroidcartilage
C4 Suprasternalnotch Spontaneousrespiration
C5 Infraclaviculararea Shouldershrugging Biceps
C6 Thumb Elbowflexion Triceps
C7 Indexfinger Elbowextension
C8 Littlefinger Fingerflexion(withT1)
T4 Nippleline
T10 Umbilicus
L1 Inguinalligament Hipflexion(withL2)
L2 Medialthigh Hipflexion
L3 Medialthigh Hipadduction
L4 Medialfoot Hipabduction Patellar
L5 Webspacebetweenbigtoeandsecondtoe Footdorsiflexion
S1 Lateralfoot Footplantarflexion(withS2) Achilles
S2 Perianalarea(withS3,S4) Footplantarflexion
S3-4 Perianalarea Rectalsphinctertone
Table 75.2 Physical Examination Findings Associated with Vertebral Fractures and Spinal Cord Injuries
INJURYPHYSICAL EXAMINATION AREA ASSOCIATED FINDINGS
Vertebralfracture
Spine Tendernessoftheneckand/orback.Examinetheentirespinebecausevertebralfracturesmayoccurinmultiples.
Neurologic Seespinalcordinjurybelow.Chest Thoracic spine fractures:Checkforchesttenderness,unequalbreathsounds,andarrhythmia,
whicharesuggestiveofanassociatedintrathoracicinjuryormyocardialcontusion.Abdomen/pelvis Thoracolumbar and lumbar spine fractures:Checkforabdominalorpelvictenderness.For
instance,upto50%ofpatientswithatransverseprocessfracture7and33%ofpatientswithaChancefracture8haveconcurrentintraabdominalpathology.Atransverseareaofecchymosisonthelowerabdominalwall(seatbeltsign)increasesthechanceofanabdominopelvicinjury.
Extremity Thoracolumbar and lumbar spine fractures:Checkforcalcanealtendernessbecause10%ofcalcanealfracturesareassociatedwithalowthoracicorlumbarfracture.Mechanistically,theseareasarefracturedasaresultofaxialloading.
Spinalcordinjury
Neurologic,motor(anteriorcolumn)
Assessmotorfunctiononascaleof0to5(seeTable75.3).Motor levelisdefinedasthemostcaudalsegmentwithatleast3/5strength.Injuriestothefirsteightcervicalsegmentsresultintetraplegia(previouslyknownasquadriplegia);lesionsbelowtheT1levelresultinparaplegia.
Neurologic,sensory(spinothalamictract)
Assesssensoryfunctionviapinprickandlighttouchonthefollowingscale:0=absent;1=impaired;2=normal.Thesensory levelisdefinedasthemostcaudalsegmentofthespinalcordwithnormalsensoryfunction.Thehighestintactsensorylevelshouldbemarkedonthepatient’sspinetomonitorforprogression.
Neurologic,sensory(dorsalcolumn)
Assessvibratorysensoryfunctiononascaleof0to2byusingatuningforkoverbonyprominences.Assesspositionsense(proprioception)byflexingandextendingthegreattoe.
Neurology,deeptendonreflex
Onascaleof0to4,assessthedeeptendonreflexesintheupper(biceps,triceps)andlower(patellar,Achilles)extremities(seeTable75.4).
Anogenital Assessrectaltone,sacralsensation,signsofurinaryorfecalretentionorincontinence,andpriapism.Alsochecktheanogenitalreflexes:ananal wink(S2-S4)ispresentiftheanalsphinctercontractsinresponsetostrokingtheperianalskinarea.Thebulbocavernosus reflex(S3-S4)iselicitedbysqueezingtheglanspenisorclitoris(orpullingonaninsertedFoleycatheter),whichresultsinreflexivecontractionoftheanalsphincter.
Head-to-toeexamination
Aspinalcordinjurymaymaskapatient’sabilitytoperceiveandlocalizepain.Imagingofhigh-riskareas,suchastheabdomen,andareasofbruisingorswellingmayberequiredtoexcludeoccultinjuries.

SECTION VIII TRAUMATIC DISORDERS
648
Spinal shock is a neurologic phenomenon resulting from physiologic transection of the spinal cord. It results in flaccid paralysis and loss of reflexes below the level of the spinal cord lesion. Spinal shock is temporary, commonly lasting for 24 to 48 hours, although it can persist for weeks. Patients suffering from spinal shock may appear (clinically) to have a complete spinal cord injury only to “miraculously” recover once the spinal shock has passed. Termination of spinal shock is identi-fied by return of segmental reflexes; anogenital reflexes are the earliest to recover.
Neurogenic shock may occur in patients with cervical or high thoracic spinal cord injuries. It is a neurocardiovascular phenomenon resulting from impairment of the descending sympathetic pathways in the spinal cord. As a result, vasomo-tor tone is lost and visceral and peripheral vasodilation and hypotension ensue. Diminished sympathetic innervation to the heart also occurs and results in relative bradycardia despite the presence of hypotension.
DIFFERENTIAL DIAGNOSIS AND MEDICAL DECISION MAKING
INDICATIONS FOR CERVICAL SPINE IMAGING
In the year 2000, in the hope of reducing the number of low-risk patients undergoing cervical spine plain film radiography, a multicenter study by the National Emergency X-radiography Utilization Study (NEXUS) group validated a set of five low-risk criteria for determining which patients do not require radiographic imaging if all the criteria are met (Box 75.1). This clinical decision tool demonstrated a sensitivity of 99.6% and a specificity of 12.9% for detecting clinically significant cervical spine fractures. It was thus extrapolated that 4309 (12.6%) of the 34,069 patients enrolled could have avoided plain film radiography.9
Following development of the NEXUS criteria, the Cana-dian Cervical-Spine Rule (CCR) was developed (Fig. 75.5). The validated sensitivity and specificity for this decision rule were 99.4% and 45.1%, respectively.10
The CCR study excluded the following subjects: patients younger than 16 years; patients with an abnormal Glasgow Coma Scale score, abnormal vital signs, injuries more than 48 hours old, penetrating trauma, paralysis, and history of vertebral disease; patients seen previously for the same injury;
Table 75.3 Graded Assessment of Motor Function
GRADE ASSESSMENT ON PHYSICAL EXAMINATION
0 Noactivecontraction
1 Tracevisibleorpalpablecontraction
2 Movementwithgravityeliminated
3 Movementagainstgravity
4 Movementagainstgravityandresistance
5 Normalpower
Table 75.4 Graded Assessment of Deep Tendon Reflexes
GRADE ASSESSMENT ON PHYSICAL EXAMINATION
0 Reflexesabsent
1 Reflexesdiminishedbutpresent
2 Normalreflexes
3 Reflexesincreased
4 Clonuspresent
BOX 75.1 NEXUS Low-Risk Criteria for a Cervical Spine Injury
Apatientdoesnotrequirecervicalspineradiographicimagingifallfiveofthefollowinglow-riskconditionsaremet:1. Noposteriormidlineneckpainortenderness2. Nofocalneurologicdeficit3. Normallevelofalertness4. Noevidenceofintoxication5. Noclinicallyapparent,painfuldistractinginjury*
*Definedasaconditionthoughtbythecliniciantobeproducingpainsuf-ficienttodistractpatientsfromasecond(neck)injury.
FromHoffmanJR,MowerWR,WolfsonAB,etal.Validityofasetofclini-cal criteria to rule out injury to the cervical spine in patients with blunttrauma.NEnglJMed2000;343:94-9.NEXUS,NationalEmergencyX-radiographyUtilizationStudy.
and pregnant patients. Because these cases were not studied, the CCR guidelines should not be applied to such patients.
CHOOSING THE IMAGING MODALITY TO EVALUATE THE CERVICAL SPINE (Fig. 75.6)When patients have at least one high-risk criterion for a spinal fracture, imaging begins with either plain films or computed tomography (CT) scans. The pros and cons of both imaging approaches are listed in Table 75.5.
Patients with symptoms suggestive of a spinal cord injury should undergo CT and magnetic resonance imaging (MRI) of suspicious areas of the spine. Although plain films and CT do not directly reveal spinal cord injuries, they may supply indirect evidence of such injuries. Spinal cord injury without radiographic abnormality (SCIWORA) is a traumatic myelop-athy in which no abnormalities can be identified on plain films or CT.
Computed TomographyWith increasing evidence in the literature showing that CT is much more sensitive (98%) than plain film radiography (53%) in detecting cervical spine fractures, future recommendations will probably recommend cervical spine CT as the first-line diagnostic approach for most patients because of the neuro-logic significance of a missed cervical spine injury.11 Conven-tional radiography is especially difficult to interpret in the high cervical spine (occiput, C1, C2) and cervicothoracic

CHAPTER 75 SpInE TRAUMA AnD SpInAl CORD InjURy
649
Fig. 75.5 Canadian Cervical-Spine Rule (CCR) algorithm for clinical clearance of the cervical spine.Thegreen boxsignifiesalow-risk,negativework-upandclinicalcervicalspineclearance.Orange boxessignifyamoderate-riskcondition,andthered boxsignifiesahigh-riskcondition,bothofwhichrequireplainfilmradiography.ED,Emergencydepartment;GCS,GlasgowComaScale;RR,respiratoryrate;SBP,systolicbloodpressure.(DatafromStiellIG,ClementCM,McKnightRD,etal.TheCanadianC-SpineRuleversustheNEXUSlow-riskcriteriainpatientswithtrauma.NEnglJMed2003;349:2510-8.)
• Age ≥ 16 years• GCS score of 15• Normal vital signs (RR, 10-24 breaths/min; SBP > 90 mm Hg)• Injury within 48 hours• Blunt (not penetrating) neck trauma mechanism• No acute paralysis• No known vertebral disease• Not evaluated previously for the same injury• Not pregnant
• Age ≥ 65 years• Dangerous mechanism � Fall from ≥3 feet or 5 stairs � Axial loading to the head � Motor vehicle crash at >62 mph (100 km/hr) � Motor vehicle crash with rollover or ejection � Motorized recreational vehicle crash � Bicycle crash• Extremity paresthesias
Yes
Yes
• Simple rear-end motor vehicle crash• In a sitting position in the ED• Ambulatory at any time after the trauma• Delayed onset of neck pain• Absence of midline cervical spine tenderness
No
Fulfills ALL eligibility requirements?
Presence of ≥1 high-risk finding?
Presence of ≥1 low-risk finding?
Yes
Able to rotate neck 45° left and right actively?
Yes
Low risk:Cervical spine clinically cleared
High risk:Obtain imaging
No Moderate risk:Obtain imaging
No Moderate risk:Obtain imaging
junction (C6, C7, T1), where coincidentally most cervical spine fractures occur.12 It is important to obtain sagittal CT reconstructions, in addition to the traditional axial views, to adequately assess spinal alignment.
Cost analyses have shown that cervical spine CT scans are actually less expensive than conventional radiography in high-risk patients. These studies factored personnel time, delays in patient management while obtaining films, and the neurologic sequelae of initially missing a cervical spine injury. Cost savings are especially evident if the patient is already under-going CT imaging of other body parts, such as head scanning for a closed head injury. With multidetector scanners being more readily available, an additional cervical spine scan would add less than 5 minutes of scan time at a relatively small cost.13
The risk for cancer from irradiation serves as the major deterrent against universally performing CT in all patients with neck trauma. It is estimated that up to 2% of cancers in the United States are attributable to CT studies.14 The thyroid gland, breast tissue, and lens are exposed to especially high levels of radiation in cervical spine CT, thus placing the patient at high risk for the development of thyroid cancer, breast cancer, and cataracts. Patients receive an effective dose of 0.2 millisievert (mSv) and 6 mSv for cervical spine plain films and CT, respectively. In contrast, the effective dose of a posteroanterior and lateral chest radiograph is just 0.1 mSv.15 The overall lifetime carcinogenic risk from CT imaging, however, varies depending on the patient’s age at the time of irradiation. Younger patients have greater risk, partly because they have more years of life left for the development of cancer.

SECTION VIII TRAUMATIC DISORDERS
650
Fig
. 75.6
D
iag
nost
ic a
lgo
rith
m f
or
a p
atie
nt w
ith
neck
pai
n re
sult
ing
fro
m b
lunt
tra
uma.
CC
R,
Can
adia
nC
ervi
cal-
Sp
ine
Rul
e;C
T,
com
put
edt
omog
rap
hy;
MR
I,m
agne
ticr
eson
ance
imag
ing;
NE
XU
S,
Nat
iona
lEm
erge
ncy
X-r
adio
grap
hyU
tiliz
atio
nS
tud
y.
Nor
mal
film
sLo
w r
isk:
Cer
vica
l spi
ne c
lear
edN
euro
surg
ical
or
orth
oped
icsp
ine
cons
ulta
tion
Abn
orm
alC
TY
esY
es
If co
ncur
rent
neur
olog
icde
ficit
Spi
nal c
ord
inju
ry r
isk:
Obt
ain
cerv
ical
spi
ne M
RI
Can
the
patie
nt a
ctiv
ely
flex
and
exte
nd th
e ne
ck 3
0°?
No
Abn
orm
alfil
ms
App
ly s
emiri
gid
cerv
ical
col
lar
and
refe
r fo
r fle
xion
-ext
ensi
onfil
ms
in 7
-10
days
Neu
rolo
gic
or o
rtho
pedi
csp
ine
cons
ulta
tion
Yes
Obt
ain
flexi
on-e
xten
sion
plai
n fil
ms
No
Low
ris
k:O
btai
n pl
ain
film
s
Nor
mal
film
s
Abn
orm
alfil
ms
Low
ris
k:C
linic
ally
cle
ar c
ervi
cal s
pine
Yes
Low
ris
k:C
ervi
cal s
pine
cle
ared
Is c
linic
al c
lear
ance
pos
sibl
e by
NE
XU
S o
r C
CR
crit
eria
?
No
Mod
erat
e-hi
gh r
isk:
Obt
ain
cerv
ical
spi
ne C
T
Yes
• A
ge ≥
65
year
s•
Sig
nific
ant m
echa
nism
• S
igni
fican
t nec
k te
nder
ness
• C
hron
ic c
ortic
oste
roid
trea
tmen
t•
His
tory
of v
erte
bral
dis
ease
• B
ody
habi
tus
likel
y to
pre
clud
e ad
equa
te p
lain
film
acq
uisi
tion
• G
oing
to C
T fo
r an
othe
r bo
dy a
rea
• A
neu
rolo
gic
defic
it co
nsis
tent
with
a c
ervi
cal
spi
nal c
ord
inju
ry•
A th
orac
ic o
r lu
mba
r sp
ine
inju
ry
Pre
senc
e of
≥ 1
hig
h-ris
k or
cos
t-ef
fect
ive
crite
ria?
Nor
mal
CT
Is a
neu
rolo
gic
defic
it pr
esen
t?N
oIs
sig
nific
ant p
ersi
sten
t cer
vica
lsp
ine
tend
erne
ss p
rese
nt?
No
Low
ris
k:C
linic
ally
cle
ar c
ervi
cal s
pine

CHAPTER 75 SpInE TRAUMA AnD SpInAl CORD InjURy
651
Magnetic Resonance ImagingMRI is the best available modality for detection and charac-terization of spinal cord injury, but it is less sensitive than CT for cervical spine fractures. In an acute trauma patient with potential spinal injury, indications for emergency MRI include (1) complete or incomplete neurologic deficits suspicious for a spinal cord injury, (2) deterioration of spinal cord neurologic function, and (3) signs of unstable ligamentous injury. Abnor-mal MRI findings may include the presence of spinal canal compromise, disk herniation, and spinal cord edema or hemorrhage.
OLDER AND OSTEOPENIC PATIENTSPatients older than 65 years old and those taking corticoste-roids on a long-term basis are probably osteopenic. They can sustain spinal fractures with mild trauma, such as a fall from a standing position, and often exhibit minimal associated pain. Specifically, patients older than 65 years have an increased risk for cervical spine fracture (relative risk of 2.09).16 In addition, acute back pain in chronic corticosteroid users is correlated with 99% specificity for a spinal compression frac-ture.17 Thus, imaging should be performed in these potentially osteopenic patients in the setting of neck or back pain.
CLINICAL CLEARANCE OF THE CERVICAL SPINENot all patients require cervical spine imaging. To clinically clear a cervical spine, the patient’s neck should be reevaluated for tenderness. First, unfasten the cervical collar. Next, palpate the posterior aspect of the patient’s neck while applying the other hand to the patient’s forehead to prevent spontaneous and reflexive head lifting. In the absence of significant midline tenderness, remove your hands and instruct the patient to actively lift the head off the gurney and place the neck through a range of motion by looking right, left, caudad, and cephalad. Do not assist the patient.
If the patient is able to move spontaneously and easily without pain or neurologic symptoms, the patient’s neck is considered to be “clinically cleared” and the collar may be removed.
Furthermore, children are more radiosensitive. If irradiated after 40 years of age, the risk reaches its nadir, with an esti-mated lifetime attributable risk for death from cancer of less than 0.2%.14
Because of such concerns for radiation exposure, low-risk patients should undergo conventional radiography. Only patients with radiographic evidence of an injury on plain films should subsequently undergo CT scanning. For moderate- to high-risk patients, cervical spine CT should be the first-line imaging modality, especially for patients scheduled for CT scanning of another body part.
Flexion-Extension Plain Film RadiographyA normal cervical CT image adequately excludes a cervical spine fracture but cannot sufficiently evaluate ligamentous instability. In patients who have sustained significant flexion, extension, or rotational injury to the neck and have persistent neck pain, ligamentous stability should be assessed within 10 days either in the ED or by a neurosurgeon or orthopedic spine specialist.
In the ED, patients who are awake and alert and can actively flex and extend their neck 30 degrees may undergo flexion-extension plain film radiography to evaluate for spinal stability. Vertebral body subluxation or focal widening of the spinous processes suggests an unstable ligamentous injury. Because no serious adverse outcomes have resulted from voluntary neck movement by an awake, alert patient without neurologic deficits, manual manipulation of the patient’s neck should be avoided during flexion-extension radiography.
Many acutely injured patients have such severe associated cervical muscle spasms that they have limited neck mobility. As a result, flexion-extension films are often inadequate, and these patients should be immobilized in a semirigid cervical collar (e.g., a Philadelphia or Miami J collar) and undergo delayed flexion-extension plain film radiography after 7 to 10 days, when the cervical muscle spasm diminishes.
Table 75.5 Advantages and Disadvantages of Plain Film Imaging and Computed Tomography of the Cervical Spine
PLAIN FILM RADIOGRAPHY COMPUTED TOMOGRAPHY
Advantages Lessirradiationofthethyroid,breast,andlensCanbeperformedatthebedside
98%sensitivityindetectingfracturesMorecost-effectivethanplainfilmsLessdelayinpatientmanagement,especiallyifthepatientis
alreadygoingtoCTscannerforimagingofanotherbodypart
Disadvantages Only53%sensitivityindetectingfracturesThree-viewfilmsareinadequate>50%ofthetime,
especiallyfilmsofthecervicocranialandcervicothoracicjunction
Inefficientuseofradiologypersonnel,whoareoftenrepeatingfilmsbecauseofimageinadequacy
AsuspiciousfractureoronedetectedonplainfilmsrequiresadditionalevaluationbyCTforconfirmationandfurtherdelineation
Moreirradiationofthethyroid,breast,andlensRequiresthepatienttobehemodynamicallystablebecause
ofbeingtransportedoutoftheemergencydepartmenttotheCTscanner

SECTION VIII TRAUMATIC DISORDERS
652
FACTS AND FORMULAS
Tenpercentofspinalfractureshaveasecondnoncontigu-ousfracturealongthevertebralspine.
Ten percent of patients with a calcaneal fracture have anassociatedthoracicorlumbarfracture.
The most commonly fractured cervical spine level is C2,especiallyintheelderly.
Approximately 20% of computed tomography–confirmedburstfracturesinthethoracicandlumbarspineappearaswedgefracturesonplainfilmradiography.18
High-dosemethylprednisoloneisadministeredasa30-mg/kgbolusandthenasa5.4-mg/kg/hrinfusionfor24hours(if started within 3 hours of injury) or for 48 hours (ifstartedwithin8hoursofinjury).
Considerearlyendotrachealintubationinspinalcordinjurypatients with a negative inspiratory force of less than−25cmH2Ooravitalcapacityoflessthan15mL/kg.
Table 75.6 Classic Upper Cervical Spine Injury Patterns (C1-C2)*
INJURY MECHANISM STABILITY FIGURE COMMENTS
Atlantooccipitaldislocation
Flexion Unstable 75.7,A OfteninstantlyfatalMorecommoninchildrenbecauseofsmall,horizontallyoriented
occipitalcondylesDislocationcanbeanterior(mostcommon),superiorlydistracted,or
posterior
Anterioratlantoaxialdislocation
Flexion Unstable 75.7,B AssociatedwithruptureofthetransverseligamentMostcommonlyoccursinpatientswithrheumatoidarthritisand
ankylosingspondylitisfromligamentlaxityWideningofthepredentalspaceseenonlateralplainfilms
Jeffersonfracture(C1burstfracture)
Axialcompression
Unstable 75.7,C 33%withassociatedC2fractureLowincidenceofneurologicinjurybecauseofawideC1spinalcanalUsuallyinvolvesfracturesofboththeanteriorandposteriorC1
arches,oftenwith3or4fracturefragmentsComplication:transverseligamentrupture,especiallyiftheC1lateral
massesare≥7mmwiderthanexpected(MRIrecommended);vertebralarteryinjury(CTangiographyrecommended)
C1posteriorarchfracture
Extension Stable 75.7,C AnassociatedC2fracture(occurs50%oftime)makesaposteriorarchfractureunstable
Onplainfilms,nodisplacementoflateralmassesontheodontoidviewandnoprevertebralsofttissueswelling,unlikeaJeffersonburstfracture
C2densfracture Flexion Variable 75.7,D Type I (stable):AvulsionofthedenswithanintacttransverseligamentType II (unstable):Fractureatthebaseofthedens;10%havean
associatedruptureofthetransverseligament—MRIprovidesadefinitivediagnosisofligamentrupture
Type III (stable):Fractureofthedensextendingintothevertebralbody
Hangman’sfracture(C2spondylolisthesis)
Extension Unstable 75.7,E BilateralC2pediclefracturesAtriskfordisruptionofthePLL,C2anteriorsubluxation,andC2-C3
diskruptureLowriskforspinalcordinjurybecauseofC2anteriorsubluxation,
whichwidensthespinalcanal
Extensionteardropfracture
Extension Unstable 75.7,F SmalltriangularavulsionoftheanteroinferiorvertebralbodyattheinsertionpointoftheALL
OccursmostfrequentlyattheC2levelbutcanoccurinthelowercervicalspine
Complication:centralcordsyndromeasaresultoftheligamentumflavumbucklingduringhyperextension
RequiresCTdifferentiationfromaveryunstableflexionteardropfracture(see“flexionteardropfracture”inTable75.7)
*Listedinprogressiveorderfromtheocciput,toC1,toC2.ALL,Anteriorlongitudinalligament;CT,computedtomography;MRI,magneticresonanceimaging;PLL,posteriorlongitudinalligament.
CLASSIC FRACTURE PATTERNS (Tables 75.6 to 75.8; Figs. 75.7 to 75.9)
CERVICAL SPINE INJURIESBased on the NEXUS study of 818 patients with cervical spine injury, fractures occurred most commonly at the level of C2 (24% of all fractures), C6 (20%), and C7 (19%). Anatomically, the most commonly fractured part of the cervi-cal spine was the vertebral body, which accounted for 30% of fractures at the C3 to C7 levels. It was more common than fractures of the spinous process (21%), lamina (16%), and articular process (15%). Subluxations occurred most com-monly at the C5-C6 (25%) and C6-C7 (23%) levels.19
THORACIC AND LUMBAR SPINE INJURIESSimilar to patients undergoing cervical spine assessment, low-risk patients may selectively be cleared clinically without radiographic imaging. Although no large studies of thoracic and lumbar spine injuries equivalent to the NEXUS and CCR

CHAPTER 75 SpInE TRAUMA AnD SpInAl CORD InjURy
653
Fig. 75.7 A,Cross-sectionalsagittalviewofanterioratlantooccipitaldislocationwithassociatedspinalcordinjury.B,Posterolateralviewofanterioratlantoaxialdislocationfromruptureofthetransverseligament.C,PosterolateralviewofaC1JeffersonburstfracturethroughtheanteriorandposteriorarchandanisolatedC1posteriorarchfracture.D,PosterolateralviewofthethreetypesofC2densfractures.E,Sagittalviewofahangman’sfracturewithbilateralC2pediclefracture.PLL,Posteriorlongitudinalligament.F,SagittalviewofaC2extensionteardropfracture.ALL,Anteriorlongitudinalligament.
Stretchedspinal cord
Anterior atlantoocciptaldislocation
Brain
Skull
A
C1 atlas
C2 axis
Dens
Anterior dislocationof C1 over C2
Rupturedtransverse ligament
B
Posterior arch
Transverse ligament
Lateral mass
Anterior archC1 burst fracture
C
Type I
Type II
Type III
Dens
D
Risk for C2subluxation
from PLL rupture
Bilateral C2pedicle fracture
Risk forC2-C3
disk rupture
C1
C2
E
Neckextension
Avulsion ofC2 body
ALL
C1
C2
F
projects have been conducted, recommendations can be extrapolated from the relevant literature.
Based on the NEXUS criteria, patients with (1) significant back pain or tenderness, (2) clinical evidence of drug- or alcohol-related intoxication, (3) lower extremity neurologic deficits, (4) Glasgow Coma Scale score lower than 15, or (5) a distracting injury cannot be cleared clinically for a thoracic
or lumbar fracture. Patients with alcohol intoxication, for example, should not be cleared clinically until they are sober and found to fulfill no other high-risk criteria.
Furthermore, based on the CCR criteria and the American Healthcare Research and Quality “red flag” indications for imaging, injured patients who are (1) older than 65 years with any degree of back pain or tenderness, (2) are receiving

SECTION VIII TRAUMATIC DISORDERS
654
below the level of injury. During the first few days following injury, this diagnosis cannot be made with certainty because of the possibility of concurrent spinal shock.
INCOMPLETE INJURYA spinal cord injury is incomplete if motor function, sensa-tion, or both are partially present below the level of the injury. Signs of an incomplete injury may include (1) the presence of any sensation or voluntary movement in the lower extremi-ties or (2) evidence of sacral sparing. Signs of sacral sparing include perianal sensation, voluntary anal sphincter contrac-tion, and voluntary great toe flexion.
chronic corticosteroid therapy, or (3) have a history of verte-bral disease should undergo radiography.
Classic patterns of thoracic and lumbar spine injuries are shown in Table 75.8.
CLASSIFICATION OF SPINAL CORD INJURIES
COMPLETE INJURYA spinal cord injury is classified as physiologically complete if the patient has no demonstrable motor or sensory function
Table 75.7 Classic Lower Cervical Spine Injury Patterns (C3-C7)
INJURY MECHANISM STABILITY FIGURE COMMENTS
Articularmassfracture
Flexion-rotation
Stable 75.8,A AssociatedwithtransverseprocessandvertebralbodyfracturesUncommon
Burstfracture Axialcompression
Stable 75.8,B CompressivefractureoftheanteriorandposteriorvertebralbodyIntactALLandPLLComplication:spinalcordinjurybecauseofaretropulsedvertebral
bodyfragment(especiallyanteriorcordsyndrome)
Clayshoveler’s(spinousprocess)fracture
Flexion Stable 75.8,B SpinousprocessfracturefromforcefulneckflexionMostcommonlyoccursinthelowercervicallevels,usuallyC7Notassociatedwithneurologicinjury
Extensionteardropfracture
Extension Unstable 75.7,F MostcommonlyoccursatC2SeeTable75.6
Facetdislocation,bilateral
Flexion Unstable 75.8,C Significantanteriordisplacement(>50%)ofthespinewhenbilateralinferiorfacetsdisplaceanteriortothesuperiorfacetsbelow
Atriskforinjuringthedisk,vertebralarteries,andspinalcord
Facetdislocation,unilateral
Flexion-rotation
Stable 75.8,D Usuallycauses25-50%anteriordisplacementofthespineComplication:vertebralarteryinjury(CTangiographyrecommended)
Flexionteardropfracture
Flexionandaxialloading
Unstable 75.8,E Oneofthemostunstablefracturesinthelowercervicalspinebecauseitinvolvesbothcolumns
Fractureandanteriordisplacementoftheanteroinferiorvertebralbody(appearssimilartoanextensionteardropfractureexceptthatitismuchmoreunstable)
Uniquefindingsforflexion(versusextension)teardropfracturesincludesame-levelfracturesanddisplacementofposteriorstructures
RuptureofbothALLandPLLcomplexesUsuallyoccursatC5orC6CanresultfromdivingintoshallowwaterorafootballtacklinginjuryOftenassociatedwithspinalcordinjuryandtetraplegia
Subluxation,anterior Flexion Unstable 75.8,F AnteriorslippingofavertebraoveranotherRupturedPLLsuchthattheanteriorandposteriorvertebrallinesare
disruptedComplication:vertebralarterydissection(CTangiography
recommended)Maybeevidentonlyduringflexionviewsbyconventionalradiography
whentheinterspinousdistancewidensandthevertebralbodysubluxatesanteriorly
Transverseprocessfracture
Lateralflexion Stable 75.8,A Complication:vertebralarteryinjurybecauseittravelswithinthetransverseforamina(CTangiographyrecommended);associatedcervicalradiculopathyandbrachialplexusinjuriesin10%ofcases
Wedgefracture Flexion Stable 75.8,G Compressionfractureofonlytheanterosuperiorvertebralbodyendplate
DisruptionoftheanteriorvertebrallineIntactposteriorvertebralbodyandposteriorvertebralline
ALL,Anteriorlongitudinalligament;CT,computedtomography;PLL,posteriorlongitudinalligament.

CHAPTER 75 SpInE TRAUMA AnD SpInAl CORD InjURy
655
Vertebral body
Transverse foramen
Fracture througharticular pillar
Superiorarticular
facet
Transverseprocess fracture
A
C5 spinousprocess fracture
Posterior vertebral line
Anterior vertebral line
C4 burstfracture
C3
C5
B
Both C4 inferior facets “jump”over C5 articular facets
>50% anteriordisplacement
C4 inferiorarticular facet
C5 superiorarticular facet
C5 inferiorarticular facet
C4
C5
C
Single C4 inferior facet “jumps”over C5 articular facet
C4 inferiorarticular facet
C5 superiorarticular facet
C5 inferiorarticular facet
C4
C5
D
C4
C6
Axial loading Posteriordisplacement
Flexion
C5 flexionteardropfracture
Posteriorligamentous
instability
E
Fig. 75.8 A,Superioraxialviewofanarticularpillarfractureandtransverseprocessfracture.B,SagittalviewofaC4burstfractureandC5clayshoveler’s(spinousprocess)fracture.C,SagittalviewofbilateralC4facetdislocation.D,SagittalviewofunilateralC4facetdislocation.E,SagittalviewofaC5teardropfracture. Continued

656
Table 75.8 Classic Thoracic and Lumbar Spine Injury Patterns
INJURY MECHANISM STABILITY FIGURE COMMENTS
Wedgefracture
Flexion Stable,usually
75.8,G MostcommonfractureinthethoracicspineIsolatedanteriorcolumnfractureDisruptionoftheanteriorvertebrallinewithanintactposteriorvertebralline
(classic)MaintainalowthresholdtoobtainspineCTfordifferentiationofawedge
fromaburstfracture(upto22%ofburstfracturesappeartohaveanintactposteriorvertebralline)
Burstfracture
Axialloading Variable 75.8,B FractureoftheanteriorandmiddlecolumnsDisruptionoftheanteriorandposteriorvertebrallines(classic)65%haveassociatedspinalcordinjurybecauseofmiddlecolumn
compromise
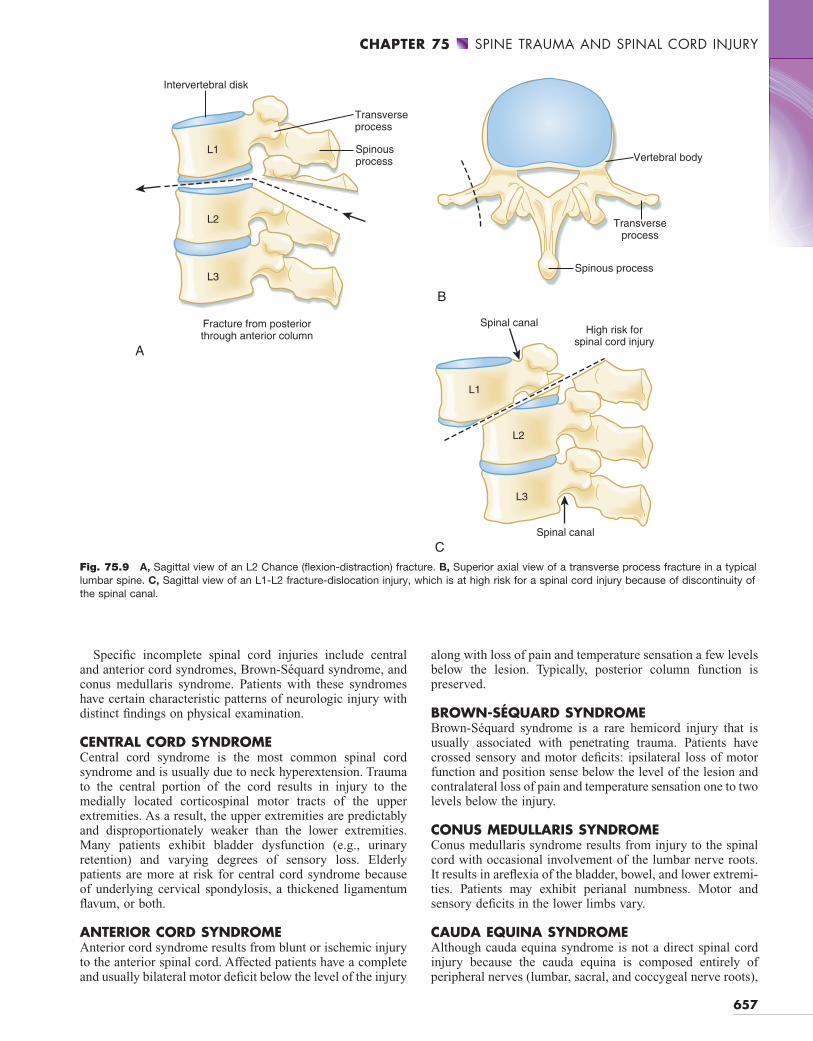
Chancefracture
Flexion-distraction
Unstable 75.9,A Fracturethroughtheanterior,middle,andposteriorcolumns,progressingfromposteriortoanterior
UsuallylocatedattheT12-L2junctionClassicallycausedbyalapbelthyperflexionmechanisminamotorvehicle
collision33-89%associatedwithintraabdominalinjurySpinalcordinjuryisuncommonbecauseofthedistractionmechanism
Transverseprocessfracture
Stable 75.9,B MostcommonfractureinthelumbarspineClassicallyhasaverticalfractureorientationAhorizontaltransverseprocessfractureorientationsuggestsadistraction
injury(Chancefracture)Morethan50%oftransverseprocessfracturesaremissedbyconventional
radiographyanddetectedonspineCTClinicallyinsignificant,butariskfactorforotherinjurypatterns50%associatedwithanintraabdominalinjury30%associatedwithapelvicfracture(especiallyanL5transverseprocess
fracture)L2transverseprocessfractureisassociatedwithrenalarterythrombosis
Fracture-dislocation
Compressionordistraction
Unstable 75.9,C SignificantspinalmisalignmentandvertebralcolumndiscontinuityFracturethroughtheanterior,middle,andposteriorcolumnsExtremelyhighincidenceofspinalcordinjury
CT,Computedtomography.
C4 anterior subluxationwith disrupted anterior and posterior
vertebral lines
Posteriorligamentious
instability
Posterior vertebral line
C4
C5
Anterior vertebral line
F
Posterior vertebral line
Anterior vertebral line
G
C5 wedge fracturewith disruption of anterior vertebral line
C5
C4
Flexion
F,SagittalviewofC4anteriorsubluxation.G,SagittalviewofaC5wedgefracture.Fig. 75.8, cont’d
CHAPTER 75 SpInE TRAUMA AnD SpInAl CORD InjURy
657
Fig. 75.9 A,SagittalviewofanL2Chance(flexion-distraction)fracture.B,Superioraxialviewofatransverseprocessfractureinatypicallumbarspine.C,SagittalviewofanL1-L2fracture-dislocationinjury,whichisathighriskforaspinalcordinjurybecauseofdiscontinuityofthespinalcanal.
Intervertebral disk
Transverseprocess
Spinousprocess
Fracture from posteriorthrough anterior column
L1
L2
L3
A
Vertebral body
Transverseprocess
Spinous process
B
Spinal canalHigh risk for
spinal cord injury
Spinal canal
L1
L2
L3
C
along with loss of pain and temperature sensation a few levels below the lesion. Typically, posterior column function is preserved.
BROWN-SÉQUARD SYNDROMEBrown-Séquard syndrome is a rare hemicord injury that is usually associated with penetrating trauma. Patients have crossed sensory and motor deficits: ipsilateral loss of motor function and position sense below the level of the lesion and contralateral loss of pain and temperature sensation one to two levels below the injury.
CONUS MEDULLARIS SYNDROMEConus medullaris syndrome results from injury to the spinal cord with occasional involvement of the lumbar nerve roots. It results in areflexia of the bladder, bowel, and lower extremi-ties. Patients may exhibit perianal numbness. Motor and sensory deficits in the lower limbs vary.
CAUDA EQUINA SYNDROMEAlthough cauda equina syndrome is not a direct spinal cord injury because the cauda equina is composed entirely of peripheral nerves (lumbar, sacral, and coccygeal nerve roots),
Specific incomplete spinal cord injuries include central and anterior cord syndromes, Brown-Séquard syndrome, and conus medullaris syndrome. Patients with these syndromes have certain characteristic patterns of neurologic injury with distinct findings on physical examination.
CENTRAL CORD SYNDROMECentral cord syndrome is the most common spinal cord syndrome and is usually due to neck hyperextension. Trauma to the central portion of the cord results in injury to the medially located corticospinal motor tracts of the upper extremities. As a result, the upper extremities are predictably and disproportionately weaker than the lower extremities. Many patients exhibit bladder dysfunction (e.g., urinary retention) and varying degrees of sensory loss. Elderly patients are more at risk for central cord syndrome because of underlying cervical spondylosis, a thickened ligamentum flavum, or both.
ANTERIOR CORD SYNDROMEAnterior cord syndrome results from blunt or ischemic injury to the anterior spinal cord. Affected patients have a complete and usually bilateral motor deficit below the level of the injury

SECTION VIII TRAUMATIC DISORDERS
658
Fig. 75.10 In-line cervical spine immobilization during endotracheal intubation.Standingtothepatient’sside,theassistantusesbothhandstostabilizethenecktopreventhyperextension.
it still requires emergency neurosurgical intervention. Clinical findings include asymmetric sensory loss, weakness of the lower extremities, urinary retention or incontinence, decreased rectal tone, and saddle anesthesia.
TREATMENT
Prehospital and ED management should include protection of the spine and spinal cord until injuries can be identified or excluded. A rigid backboard should typically be removed promptly from beneath cooperative patients because a calm person can maintain spinal column neutrality. Extended use of a rigid backboard is associated with complications such as back pain, respiratory impairment, aspiration, and decubitus ulcers.
IN-LINE IMMOBILIZATION OF THE CERVICAL SPINEDuring the initial resuscitation phase of trauma victims, patients with a potential cervical spine injury may require endotracheal intubation before a definitive diagnosis can be made. By preventing neck hyperextension during direct laryngoscopy, in-line cervical spine immobilization during intubation maintains cervical spine neutrality (Fig. 75.10).
NEUROGENIC SHOCKNeurogenic shock results from a sympathectomy-induced reduction in blood pressure, heart rate, cardiac contractility, and cardiac output. Overly vigorous fluid resuscitation can be hazardous because of compromised cardiac output. Judicious use of vasopressors such as phenylephrine hydrochloride, dopamine, and norepinephrine is often indicated. Significant bradycardia should be treated hemodynamically with atropine.
Systolic blood pressure lower than 80 mm Hg is rarely due to neurogenic shock alone, and other causes of shock, primar-ily from hemorrhage, must be excluded. It should never be assumed that hypotension is due to spinal shock until hemor-rhage is excluded.
CORTICOSTEROID THERAPY FOR SPINAL CORD INJURYThough controversial, treatment of blunt spinal cord injury with high-dose methylprednisolone is common. This
RED FLAGS (PITFALLS)
Failure to identifyoccult injuries inhypoestheticareas.Forexample, in a patient with a midthoracic sensory leveldeficit, occult intraabdominal injuries may be hiddenbecausetheabdomenmaybeinsensate.
Failure to consider a spinal cord injury in a patient withnormal radiographic and computed tomographic (CT)findings.
FailuretorepeatplainfilmsorobtainCTimagingwhenplainfilmradiographsofthecervical,thoracic,orlumbarspineareinadequate.
Failuretoexcludeothercausesofhypotensioninatraumapatient before assuming that it is neurogenic shock. Asearchforoccultbloodlossshouldfirstbedone.
Failuretoconsideradistractinginjury,particularlyfractures,as a reason for a patient’s ability to localize neck andbackpain.
therapeutic recommendation is based on the findings of the National Acute Spinal Cord Injury Study (NASCIS), which demonstrated improved neurologic function in patients receiv-ing high-dose corticosteroids within 8 hours of injury. Improved neurologic function, however, was defined as a modest gain in motor scores but not functional improvement. In NASCIS, a loading dose of 30 mg/kg of methylpredniso-lone administered over a 15-minute period was followed by an infusion of 5.4 mg/kg/hr and continued for 24 hours (in patients treated within 3 hours of injury) or 48 hours (in patients treated 3 to 8 hours after injury).20,21 No benefit was found when steroids were administered more than 8 hours after injury.
Steroid therapy is not indicated for penetrating injuries and has not been adequately studied in children younger than 13 years or in patients with cauda equina or spinal root injury.
Finally, systemic corticosteroid therapy is not benign. Com-plications of steroid therapy include gastrointestinal hemor-rhage and wound infection in patients treated with corticos teroid infusions for 24 hours and higher rates of severe sepsis and severe pneumonia in those treated for 48 hours. The use of steroids for blunt traumatic spinal cord injury is far from the standard of care.22 More research is needed to verify or refute this controversial therapy.
SURGICAL MANAGEMENT OF SPINAL CORD INJURYTimely reduction of the displaced spinal column plus decom-pression of the spinal cord has been associated with recovery from otherwise devastating spinal cord injuries.23 The optimal timing of surgery following a spinal injury remains controversial. Some argue for immediate surgery, whereas others advocate delayed surgery because of the initial post-traumatic swelling. The sole absolute indication for immedi-ate surgery is progressively worsening neurologic status in patients with spinal fracture-dislocations who initially have incomplete or absent neurologic deficits.24

CHAPTER 75 SpInE TRAUMA AnD SpInAl CORD InjURy
659
PRIORITY ACTIONS
Providepaincontrol.Maintainfullspinalprecautionsuntilthespinecanbecleared
radiographicallyorclinically.If intubating a trauma patient, an assistant should provide
in-line cervical spine immobilization until the cervicalspinecanbeassessedmoredefinitivelyatalatertime.
Performacarefulinitialneurologicexamination,especiallyinpatients who are about to undergo sedation or neuro-muscularblockade.
If a spinal fracture is suspected or detected, evaluate forassociatedinjuries:• For the cervical spine, examine for associated head
andfacialinjuries.• For the thoracic spine, examine for rib fractures and
pulmonary, cardiac, diaphragmatic, and mediastinalinjuries.
• Forthelumbarspine,examineforintraabdominalinju-ries,pelvicfractures,andcalcanealfractures.
• Forallspinallevels,examineforspinalcordinjury.Obtainurgentspineimagingifafractureorspinalcordinjury
issuspected.Obtainemergencymagneticresonanceimagingofthespine
ifaspinalcordinjuryissuspected.Consideradministeringcorticosteroidsifanadultpatienthas
sustained blunt spinal trauma and exhibits neurologicdeficitswithin8hoursofinjury.
Prolongedimmobilizationonarigidbackboardisuncomfort-able for the patient and places the patient at risk foraspirationandearlypressuresores.Aim to remove thebackboardassoonaspossibleandideallywithin2hoursof patient arrival. A standard hospital gurney providesadequatethoracicandlumbarstability.
Performserialneurologicexaminationsonpatientswithsus-pectedorknownspinal injuriestodocumentneurologicimprovement or deterioration. Neurologic deteriorationinvolving the cervical and upper thoracic levels mayrequire empiric endotracheal intubation for impendingrespiratoryfailure.
Once a spinal injury is detected, carefully reexamine theentirecervical, thoracic,and lumbarspine.Obtainplainfilmsorcomputedtomographyscansofany levelswithpainortendernessbecauseofthehighriskforasecondspinalinjury.
Whenperforming“clinicalclearance”ofapatient’scervicalspineorobtainingflexion-extensioncervicalspineplainfilms,donotpassivelyrangetheneckforthepatient.Thismay cause an iatrogenic spinal injury. Pain with activemovementwillprevent thepatient fromoverrangingtheneck.
TIPS AND TRICKS
In a series of patients with traumatic central cord syndrome, those who underwent early surgery (<24 hours after injury) and had an underlying disk herniation or fracture-dislocation exhibited significantly greater overall motor improvement than did those who underwent late surgery (>24 hours after injury).25 Unfortunately, early decompressive surgery does not uniformly improve outcome following spinal cord injury.
FOLLOW-UP, NEXT STEPS IN CARE, AND PATIENT EDUCATION
Most patients with traumatic spinal fractures are admitted to the hospital because they fulfill at least one of four admission criteria: (1) intractable pain, (2) fracture involvement of more than one column, (3) a functionally unstable fracture pattern, and (4) the presence or potential for development of a spinal cord injury.
Patients who can be discharged home include those with normal neurologic function and (1) an isolated, stable poste-rior column fracture (spinous process, transverse process) in the cervical, thoracic, or lumbar spine or (2) a stable wedge fracture in the thoracic or lumbar spine.
Patients with confirmed or suspected spinal cord injury should be scheduled for early consultation with a neurosur-geon or orthopedist. This may require transfer of the patient to a spine specialty center.
The level of the spinal cord injury, associated neurologic deficits, and other traumatic injuries will determine whether the patient should be admitted to the intensive care unit, neu-rosurgical observation unit, or general ward. Circular beds, rotating frames, and serial inflation devices are used to protect the patient from pressure sores.
Discharged patients without a fracture or spinal cord injury require only conservative management. Discharged patients with a stable spinal fracture require only conservative man-agement with or without an immobilization device, such as a cervical collar or thoracolumbar sacral orthosis back brace. Soft collars and back braces are not recommended because they predispose patients to stiffness of the neck and back, respectively.
Discharged patients with persistent neck pain who are still at risk for an unstable ligamentous injury should wear a semi-rigid cervical collar (e.g., Philadelphia or Miami J collar) for 7 to 10 days until adequate flexion-extension plain films can be obtained. Discharge instructions should include informa-tion about the warning signs of spinal cord injury.
DOCUMENTATION
Documentneckandbacktenderness,alongwiththeneuro-logicexamination,inalltraumapatients.
Inspinalcordinjurypatients,marktheinitiallevelofsensorydeficittomonitorprogressionofthepatient’sneurologicstatus.
Forpatientswithneurologicdeficits,performanddocumentthebulbocavernosusreflexandsacral-sparingexamina-tiontoassessforspinalshock.

SECTION VIII TRAUMATIC DISORDERS
660
3. Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-Spine Rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med 2003;349: 2510-8.
REFERENCES
References can be found on Expert Consult @ www.expertconsult.com.
SUGGESTED READINGS1. Bracken MB, Shepard MJ, Holford TR, et al. Administration of
methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-604.
2. Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. N Engl J Med 2000;343:94-9.

CHAPTER 75 SpInE TRAUMA AnD SpInAl CORD InjURy
660.e1
REFERENCES1. Berkowitz M. Assessing the socioeconomic impact of improved treatment of head
and spinal cord injuries. J Emerg Med 1993;11:63-57.2. Reid DC, Henderson R, Saboe L, et al. Etiology and clinical course of missed
spine fractures. J Trauma 1987;27:980-6.3. Nunez Jr DB, Zuluaga A, Fuentes-Bernardo DA, et al. Cervical spine trauma:
how much more do we learn by routinely using helical CT? Radiographics 1996;16:1307-18.
4. Woodring JH, Lee C. Limitations of cervical radiography in the evaluation of acute cervical trauma. J Trauma 1993;34:32-9.
5. Hauser CJ, Visvikis G, Hinrichs C, et al. Prospective validation of computed tomographic screening of the thoracolumbar spine in trauma. J Trauma 2003; 55:228-34.
6. Lucey BC, Stuhlfaut JW, Hochberg AR, et al. Evaluation of blunt abdominal trauma using PACS-based 2D and 3D MDCT reformations of the lumbar spine and pelvis. AJR Am J Roentgenol 2005;185:1435-40.
7. Patten RM, Gunberg SR, Brandenburger DK. Frequency and importance of transverse process fractures in the lumbar vertebrae at helical abdominal CT in patients with trauma. Radiology 2000;215:831-4.
8. Tyroch AH, McGuire EL, McLean SF, et al. The association between Chance fractures and intra-abdominal injuries revisited: a multicenter review. Am Surg 2005;71:434-8.
9. Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. N Engl J Med 2000;343:94-9.
10. Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-Spine Rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med 2003;349: 2510-8.
11. Mahadevan SV, Navarro M. The evaluation and clearance of the cervical spine in adult trauma patients: clinical concepts, controversies, and advances. Trauma Rep 2004;5:1-12.
12. Velmahos GC, Theodorou D, Tatevossian R, et al. Radiographic cervical spine evaluation in the alert asymptomatic blunt trauma victim: much ado about nothing? J Trauma Injury 1994;40:768-74.
13. Blackmore CC, Ramsey SD, Mann FA, et al. Cervical spine screening with CT in trauma patients: a cost-effective analysis. Radiology 1999;212:117-25.
14. Brenner DJ, Hall EJ. Computed tomography—an increasing source of radiation exposure. N Engl J Med 2007;357:2277-84.
15. Mettler Jr FA, Huda W, Yoshizumi TT, et al. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 2008;248:254-63.
16. Lowery DW, Wald MM, Browne BJ, et al. Epidemiology of cervical spine injury victims. Ann Emerg Med 2001;38:12.
17. Deyo RA, Rainville J, Kent DL. What can the history and physical examination tell us about low back pain? JAMA 1992;268:760-5.
18. Ballock RT, Mackersie R, Abitbol JJ, et al. Can burst fractures be predicted from plain radiographs? J Bone Joint Surg Br 1992;74:147-50.
19. Goldberg W, Mueller C, Panacek E, et al. Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med 2001;38:17-21.
20. Bracken MB, Holford TR. Effects of timing of methylprednisolone or naloxone administration on recovery of segmental and long-tract neurological function in NASCIS 2. J Neurosurg 1993;79:500-7.
21. Bracken MB, Shepard MJ, Holford TR, et al. Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. Results of the Third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 1997;277:1597-604.
22. Spencer MT, Bazarian JJ. Evidence-based emergency medicine/systematic review abstract. Are corticosteroids effective in traumatic spinal cord injury? Ann Emerg Med 2003;41:410-3.
23. Brunette DD, Rockswold GL. Neurologic recovery following rapid spinal realignment for complete cervical spinal cord injury. J Trauma 1987;27:445-7.
24. Lindsey RW, Pneumaticos SG, Gugala ZG. Management techniques in spinal injuries. In: Browner BD, Jupiter JB, Levine AM, et al, editors. Skeletal trauma: basic science, management, and reconstruction. 3rd ed. Philadelphia: Saunders; 2003. pp. 746-7.
25. Guest J, Eleraky MA, Apostolides PJ, et al. Traumatic central cord syndrome: results of surgical management. J Neurosurg 2002;97:25-32.