spinal cord trauma
TRANSCRIPT

13/10/15 9:24
Página 1 de 41about:blank
Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e >
Chapter 255. Spine and Spinal Cord TraumaBonny J. Baron; Kevin J. McSherry; James L. Larson Jr.; Thomas M. Scalea
EpidemiologyTrauma to the spinal column can injure the bony elements (vertebral fracture) or the neural elements (spinalcord and nerve root injury), or both. The incidence of vertebral bone fractures is unknown, but there is betteraccounting of traumatic spinal cord injury because of the creation of state and national registries.1 Data fromthese organizations estimate the incidence of traumatic spinal cord injury in the U.S. to be 40 cases per million,with a mean age of 40 years old and a male-to-female predominance of 4 to 1. Spinal injury occurs morefrequently on weekends and holidays and during summer months. The etiology of traumatic spinal cord injuryis estimated to be 42% due to motor vehicle collisions, 27% due to falls, 15% due to acts of violence(primarily gunshot wounds), 8% from sports, and 8% from other mechanisms.
Functional AnatomyThe vertebral column is the central supporting structure for the head and trunk, and provides bony protectionfor the spinal cord. This column consists of 33 vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral (fused toform the sacrum), and 4 coccygeal, which are usually fused.
Axial Vertebrae (C1 and C2)
The axial cervical vertebrae are anatomically and functionally unique. Along with the occiput, these twovertebrae form complex articulations designed for rotary motion. The atlas (C1) consists of a ring formed byanterior and posterior arches and two lateral masses that articulate with the occipital condyles and the vertebralcolumn. The axis (C2) consists of an anterior body—with a superior projection called the dens that articulateswith the inner surface of C1—and a posterior vertebral arch that encircles the spinal cord. The dens isstabilized against the inner surface of the C1 ring by the transverse ligament.
Subaxial Vertebrae
In general, the vertebrae below C2 are fundamentally the same. In accordance with their weightbearingfunction, the vertebrae become larger toward the lower end of the vertebral column. A typical vertebra iscomposed of an anterior body and a posterior vertebral arch (Figure 255-1). The vertebral arch is comprised oftwo pedicles, two laminae, and seven processes (one spinous, two transverse, and four articular). Thesearticulations enable the spine to engage in flexion, extension, lateral flexion, rotation, or circumduction

13/10/15 9:24
Página 2 de 41about:blank
(combination of all movements). The articular processes form synovial joints that act as pivots of the spinalcolumn. The orientation of these articular facet joints changes at different levels of the spine. Differences inorientation of the facet joints account for variations in motion of specific regions of the vertebral column.
Figure 255-1.
Vertebral anatomy. Each vertebra consists of a vertebral body and posterior element. Vertebrae are stabilizedby an anterior longitudinal ligament, posterior ligament, and interspinous ligament.
A series of ligaments serve to maintain alignment of the spinal column. The anterior and posterior longitudinalligaments run along the vertebral bodies. Surrounding the vertebral arch are the ligamentum flavum and thesupraspinous, interspinous, intertransverse, and capsular ligaments. Between adjacent vertebral bodies are theintervertebral disks, consisting of a peripheral annulus fibrosus and a central nucleus pulposus. The annulusfibrosus is composed of fibrocartilage. The nucleus pulposus is a semifluid, gelatinous structure made up of

13/10/15 9:24
Página 3 de 41about:blank
water and cartilage fibers. With advancing age, the proportion of water decreases and fibrocartilage increases.The intervertebral disks act as shock absorbers to distribute axial load. When compressive forces exceed theabsorptive capacity of the disk, the annulus fibrosus ruptures, allowing the nucleus pulposus to protrude intothe vertebral canal. This may result in spinal nerve or spinal cord compression.
Spinal Cord
The spinal cord is a cylindrical structure that begins at the foramen magnum, where it is continuous with themedulla oblongata of the brain. Inferiorly, it terminates in the tapered conus medullaris at the lower border ofthe first lumbar vertebra. The conus medullaris continues at its apex by a prolongation of pia mater, the filumterminale, which extends to the base of the coccyx. The spinal cord gives rise to 31 pairs of spinal nerves: 8cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each spinal nerve emerges through the intervertebralforamen corresponding to the appropriate spinal cord level. During childhood growth, the vertebral columnlengthens more than the spinal cord. As a result of this inequality, the length of the nerve roots within thespinal canal increases progressively from above downward. The lower nerve roots, inferior to the conusmedullaris, form an array of nerves around the filum terminale, called the cauda equina.
Spinal Stability
The assessment of spinal stability is an important factor in the evaluation of the injured spine. Spinal stabilityis defined as the ability of the spine to limit patterns of displacement under physiologic loads so as not todamage or irritate the spinal cord or nerve roots. Spinal stability is mostly due to the strong ligaments thatconnect the vertebral bodies and arches to each other. Although simple in principle, determining spinalstability after an acute injury is particularly difficult. Three operational methods are generally used tojudge stability following an acute injury. The first is that an injury with separation of adjacent vertebral bodiesor arches obviously has enough ligamentous disruption to be unstable. The second method uses radiography toassociate patterns of injury with the potential for instability based on clinical experience. The third methoduses the Denis three-column principle to classify injuries as stable or not.2
The three columns in the Denis system are the anterior, middle, and posterior. The anterior column is formedby the anterior part of the vertebral body, the anterior annulus fibrosus, and the anterior longitudinal ligament.The middle column is formed by the posterior wall of the vertebral body, the posterior annulus fibrosus, andthe posterior longitudinal ligament. The posterior column includes the bony complex of the posterior vertebralarch and the posterior ligamentous complex. The Denis principle is that for an injury to be unstable there mustbe disruption of at least two columns. One important addition to the three-column principle is the degree ofvertebral body compression; vertebral body compressions of >25% for the third to seventh cervicalvertebrae or >50% in the thoracic or lumbar vertebrae from an acute injury are generally consideredunstable.
The ligaments providing stability to the spine can be damaged without associated radiographic abnormalities.Determining stability in cases without associated fracture can be difficult and may require dynamic testing(flexion-extension) or MRI. Determination of stability in such circumstances is better left to the spineconsultant.
Although these concepts are useful for managing the patient, the emergency physician may not have thebenefit of all the imaging necessary nor be able to perform a complete clinical examination due to the patienthaving altered mental status or other serious injuries. Therefore, standard operational principle is that any

13/10/15 9:24
Página 4 de 41about:blank
patient with neurologic deficits or radiographic evidence of injury should be considered to have anunstable injury.
Cervical Spine FracturesThe exposure and mobility of the cervical spine make it particularly vulnerable to injury. Injuries result fromone or a combination of mechanisms: flexion, extension, compression (axial loading), distraction, rotation, andlateral bending. Differences in injury patterns between the upper cervical spine (occiput to C2) and the lower,subaxial cervical spine (C3 to C7) are due to variations in bony anatomy and ligamentous support structures inthe two regions. Harris has created a classification system for describing cervical spine injuries based on thebiomechanical forces responsible for the injury (Table 255-1).3
Table 255-1 Cervical Spine InjuriesFlexionAnterior subluxation (hyperflexion sprain) (stable)*Bilateral interfacetal dislocation (unstable)Simple wedge (compression) fracture (usually stable)Spinous process avulsion (clay-shoveler’s) fracture (stable)Flexion teardrop fracture (unstable)Flexion-rotationUnilateral interfacetal dislocation (stable)Pillar fractureFracture of lateral mass (can be unstable)Vertical compressionJefferson burst fracture of atlas (potentially unstable)Burst (bursting, dispersion, axial-loading) fracture (unstable)HyperextensionHyperextension dislocation (unstable)Avulsion fracture of anterior arch of atlas (stable)Extension teardrop fracture (unstable)Fracture of posterior arch of atlas (stable)Laminar fracture (usually stable)Traumatic spondylolisthesis (hangman’s fracture) (unstable)Lateral flexionUncinate process fracture (usually stable)Injuries caused by diverse or poorly understood mechanismsOccipital condyle fractures (can be unstable)Occipitoatlantal dissociation (highly unstable)Dens fractures (type II and III are unstable)
*Usual occurrence. Overall stability is dependent on integrity of the other ligamentous structures.
13/10/15 9:24
Página 5 de 41about:blank
Specific Cervical Spine Injuries
Occipital Condyle Fractures
Occipital condyle fractures are an unusual type of injury usually associated with high-velocity cervicocranialinjury. These fractures are categorized as type I (comminuted), type II (extension of a linear basilar skullfracture), and type III (avulsion of a fragment). Occipital condyle fractures are rarely visible on plainradiographs and usually require CT imaging for detection. Neurologic impairment is common; usually, lowercranial nerve deficits and/or limb weakness. Patients who develop lower cranial nerve deficits or any patientswith type III occipital condyle fractures should be treated with internal fixation.
Occipitoatlantal Dissociation
In occipitoatlantal dissociation, the skull may be displaced anteriorly or posteriorly, or distracted from thecervical spine. Occipitoatlantal dissociation frequently results in death. Severe occipitoatlantal dissociation iseasily detected on radiographs, but occipitoatlantal subluxation is more difficult to detect. A usefulmeasurement to detect occipitoatlantal subluxation is the basion-dental interval, the distance between thebasion and the superior cortex of the dens. This distance should normally be <8.5 mm on CT scan images, andincreases in this measurement suggest occipitoatlantal subluxation.1 Atlanto-occipital injuries are extremelyunstable.
C1 (Atlas) Fractures
Jefferson Fracture
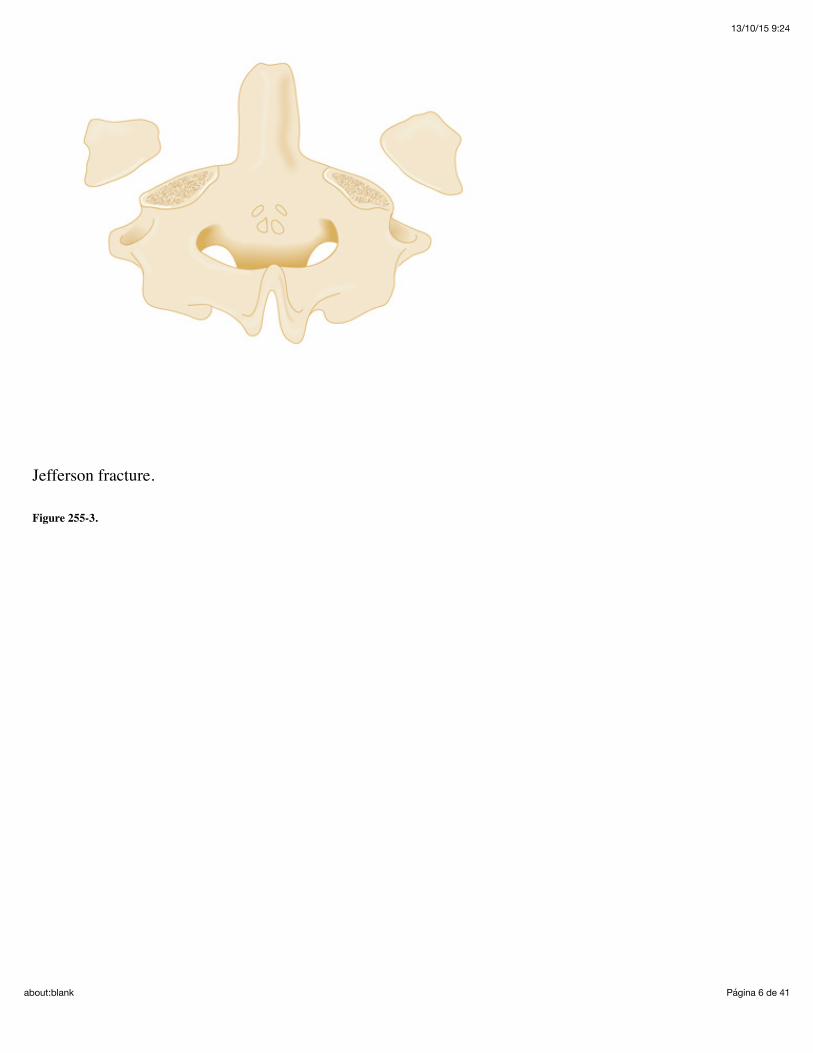
The Jefferson fracture is usually produced when the cervical spine is subjected to an axial load, as would occurfrom a direct blow to the top of the head. The occipital condyles are forced downward and produce a burstfracture by driving the lateral masses of C1 apart (Figure 255-2). The Jefferson fracture produces outwarddisplacement of the lateral masses on the open-mouth odontoid radiograph. A fracture through one lateral masswill cause unilateral displacement on the open-mouth view (Figure 255-3). Spinal instability from theJefferson fracture results from disruption of the transverse ligament and is likely if the lateral masses aresignificantly displaced. If displacement of both lateral masses (measured as offset from the superiorcorner of the C2 vertebral body on each side) is >7 mm when added together, rupture of the transverseligament is likely, and the spine is unstable.
Figure 255-2.
13/10/15 9:24
Página 6 de 41about:blank
Jefferson fracture.
Figure 255-3.

13/10/15 9:24
Página 7 de 41about:blank

13/10/15 9:24
Página 8 de 41about:blank

13/10/15 9:24
Página 9 de 41about:blank
Jefferson fracture CT and radiographs show a Jefferson burst fracture in a 46-year-old man, who sustainedinjuries while body surfing. A. Axial CT images viewed on bone windows show bilateral fractures of both theanterior and posterior arches of C1. B. Lateral radiograph of the cervical spine shows the fracture of theposterior arch of C1, with slight distraction of the posterior fracture fragment. C. Open-mouth view showsslight asymmetry of the dens in relation to the lateral masses of C1, with slight widening of the intervalbetween C1 and the dens. The right lateral mass of C1 is slightly subluxed laterally at the right atlantoaxialjoint.
Transverse Ligament Disruption
The transverse ligament is located anteriorly on the inside of the ring of C1 and runs along the posteriorsurface of the dens. The transverse ligament is crucial to maintaining the stability of the first and secondvertebrae. Pure ligamentous rupture without an associated fracture can occur in older patients from a directblow to the occiput, as would occur in a fall. Without a fracture present, radiographic diagnosis relies onidentifying the atlantodens interval, also known as the predental space, which is the space between theposterior aspect of the anterior arch of C1 and the anterior border of the odontoid. The predental space shouldbe 3 mm or less in adults when measured on a lateral radiograph or 2 mm or less on CT images.2 A predentalspace of >3 mm on a lateral radiograph (2 mm for CT images) implies damage to the transverseligament; >5 mm implies rupture of the transverse ligament.

13/10/15 9:24
Página 10 de 41about:blank
Avulsion Fracture of the Anterior Arch of the Atlas
A hyperextension injury may avulse the inferior pole of the anterior tubercle of C1. This is most readilydetected on the lateral view (Figure 255-4). The presence of perivertebral soft tissue swelling and absence ofcortication distinguish an avulsion fracture from the ununited secondary ossification center of the inferior poleof the tubercle. An isolated avulsion of the anterior tubercle is considered a stable fracture.
Figure 255-4.
Avulsion fracture of the anterior arch of the atlas.
Fracture of the Posterior Arch of the Atlas
Fracture of the posterior arch of the atlas usually results from hyperextension, with the breakage occurringfrom wedging of the posterior arch between the occipital bone and the C2 vertebra. Axial compression mayalso cause such compressive forces, and marked flexion may produce an avulsion-type of injury to theposterior arch. An isolated fracture of the posterior arch of the atlas is considered a stable fracture.
C2 (Axis) Fractures
13/10/15 9:24
Página 11 de 41about:blank
Odontoid Fractures
Fractures of the odontoid usually result from significant external forces that frequently involve other injuries tothe cervical spine and multisystem trauma. Conscious patients will usually describe immediate and severe highcervical pain with muscle spasm aggravated by movement. The pain may radiate to the occiput. Neurologicinjury is present in 18% to 25% of cases with odontoid fractures, ranging from minimal sensory or motor lossto quadriplegia. Odontoid fractures are classified according to the level of injury (Figure 255-5). Type Ifractures are avulsions of the tip. The transverse ligament remains attached to the dens, the fracture is stable,and the injury carries a good prognosis. Type II fractures occur at the junction of the odontoid with the body ofC2 and are the most common type of odontoid fracture (Figure 255-6). Type III odontoid fractures occurthrough the superior portion of C2 at the base of the dens. Both type II and III odontoid fractures areconsidered unstable.
Figure 255-5.
Classification of odontoid fractures.
Figure 255-6.
Type II odontoid fracture. CT scans demonstrate a type II odontoid fracture with posterior ligament complexinjury in a 34-year-old woman involved in a motor vehicle crash. A. Axial CT shows oblique fracture of thedens. B. CT sagittal reformatted image shows the dens fracture with slight anterior angulation.
Traumatic Spondylolisthesis of the Axis (Hangman’s Fracture)
The hangman’s fracture describes a fracture of both pedicles of C2. The resulting instability allows the body ofC2 to displace anteriorly on C3 (Figure 255-7). This fracture is caused by an extension mechanism and hasacquired its colloquial name from its association with judicial hangings, where the noose knot is placed underthe subject’s chin and snaps the head backward as the rope becomes taut at the end of a fall. Suicidal hangingsdo not usually cause the extreme hyperextension seen in judicial hangings and are not associated with thehangman’s fracture. The same fracture is seen in motor vehicle crashes and diving accidents, where suddenhyperextension forces are applied in deceleration. Owing to the large diameter of the spinal canal at the levelof C2, even displacement of C2 on C3 may not cause neurologic injury, and patients may be neurologicallyintact.
Figure 255-7.
Hangman’s fracture.
Lower Cervical Spine (C3 to C7) Fractures
The Denis three-column model of the spine is useful when assessing stability of fractures involving the third toseventh cervical vertebrae. Instability of the anterior column can occur when the anterior 20% of the vertebral

13/10/15 9:24
Página 12 de 41about:blank
body is damaged by compression, such as that seen with a teardrop fracture. Loss of 25% or more of thevertebral body height also is a marker of anterior column instability. Loss of integrity of the posterior wall of avertebral body is a marker for instability in the middle column and is visualized by detecting sagittal planefracture lines through the posterior vertebral body cortex or loss of >25% of posterior vertebral body height.Instability of the posterior column can result from damage to the facet complex, and associated radiographicfindings include fractures through the facet and widening of the pedicles.4
Anterior Subluxation
Anterior subluxation, also known as hyperflexion sprain, produces ligamentous failure in the interspinousand/or posterior longitudinal ligament. An isolated subluxation injury has no associated fractures.Radiographic findings may be absent. Significant ligamentous injury can display anterior soft tissue swelling, a“fanning” or widening of the spinous processes at the level of injury, and posterior widening of theintervertebral space. The cervical disk spaces should have a variation in alignment of <11 degrees betweenadjacent spaces; a variation of more than this may also signal a ligamentous injury. Anterior subluxationinjuries are usually stable, depending on the integrity of the posterior ligaments.
Simple Wedge Fracture
A vertebral wedge fracture is caused by compression between two other vertebral bodies. Normally thesuperior end plate of the vertebral body fractures while the inferior end plate remains intact. The posteriorligaments may be disrupted and increase the distance between the spinous processes. An isolated simplewedge fracture is stable, but the presence of significant posterior ligamentous disruption can make the injuryunstable. A simple wedge fracture is differentiated from a burst fracture by the absence of a vertical fracture ofthe vertebral body.
Flexion Teardrop Fracture
Extreme flexion can produce the flexion teardrop fracture complex. The “teardrop” is the anteroinferior portionof the vertebral body that is separated and displaced from the remaining portion of the vertebral body. There isalso complete disruption of the ligamentous structures at the level of injury. The anterior spinal cord syndromeis associated with this injury presumably because of impingement of the spinal cord on the fracture-inducedhyperkyphosis. This injury is highly unstable.
Spinous Process Avulsion (Clay-Shoveler’s) Fracture
Avulsion off the end of one of the lower cervical spinous processes, classically C7, is known as a clay-shoveler’s fracture. This injury is caused by intense flexion against a contracted posterior erector spinal musclethat fractures the tip of the spinous process. An isolated spinous process avulsion fracture is mechanicallystable.
Unilateral Interfacetal Dislocation
Simultaneous forces of flexion and rotation can produce unilateral facet dislocation, where the articular massand inferior facet on one side of the vertebra is anteriorly dislocated. On a lateral view, the involved vertebralbody will be displaced <50% of its width. On anterior view, there is rotation of the involved vertebra, with the

13/10/15 9:24
Página 13 de 41about:blank
affected spinous process pointing toward the side that is dislocated. This dislocation is mechanically stableunless there is a concomitant fracture either at the base of the inferior articular mass of the dislocated vertebraor at the base of the superior articular mass of the vertebra below.
Bilateral Interfacetal Dislocation
Bilateral interfacetal dislocation occurs when disruption of all ligamentous structures due to hyperflexionallows the articular masses of one vertebra to dislocate superior and anteriorly into the intervertebral foramenof the vertebra below. On radiographs, the vertebral body is dislocated anteriorly at least 50% of its width(Figure 255-8). These injuries are unstable and usually present with neurologic deficits. In partial bilateralinterfacetal dislocation, the inferior articular masses of the dislocated vertebra are “perched” on the superiorarticular processes of the vertebra below. These patients may not have neurologic deficits. The term lockedfacets or perched facets—both of which imply a degree of stability—to describe bilateral interfacetaldislocation is misleading because this injury is unstable regardless of the radiographic appearance.
Figure 255-8.
Bilateral interfacetal dislocation injuries incurred by a 32-year-old man following a head-on collision whileplaying football. A. Lateral radiograph and CT with (B) axial, (C) sagittal, and (D) three-dimensionalreconstruction, show a C3-C4 subluxation with bilateral locked facet joints.
Pillar or Pedicolaminar Fracture
A pillar fracture is an isolated vertical or oblique fracture through the lateral mass composed of the superiorand inferior articular processes. The adjacent lamina and pedicle remains intact. The mechanism that producesa pillar fracture is extension and rotation with impaction of a superior vertebra on the articular surface of itsinferior neighbor. The fractured articular mass is displaced posteriorly and may be visible as a double outlineon the lateral radiograph. Normally, the right and left articular masses are superimposed on one another, andone radiographic outline is seen in the lateral view. When one is displaced, the two outlines are no longersuperimposed and display as a double image. Pillar fractures may or may not be stable, depending on thedegree of ligamentous damage.
Burst Fracture
A direct axial load may cause a burst fracture of the lower cervical vertebra, with fragments displacing in alldirections (Figure 255-9). The spinal cord may be injured if a fragment enters the spinal canal. The lateralradiograph may show fracture of the superior and inferior end plates, and retropulsion of the posterior portionof the vertebral body into the spinal canal. The anterior radiographic view will show a vertical fracture throughthe vertebral body and widening of the interpedicular distance. This injury is unstable.
Figure 255-9.
Burst fracture. A. CT and (B) MRI demonstrate a C7 burst fracture with cord compression in a 19-year-oldman involved in a motorcycle crash.

13/10/15 9:24
Página 14 de 41about:blank
Hyperextension Dislocation
An extreme hyperextension injury involves a complete tear of the anterior longitudinal ligament andintervertebral disk, with disruption of the posterior ligamentous complex. Patients usually present with facialtrauma and a central cord syndrome. On the lateral radiographic view, the vertebrae may be normally alignedbecause the dislocation is reduced by the routine use of cervical immobilization collars, but diffuseprevertebral soft tissue swelling is usually present. Other radiographic signs include anterior disk spacewidening or fracture of the anteroinferior end plate of the vertebral body. These fractures are unstable.
Extension Teardrop Fracture
Hyperextension may cause the anterior longitudinal ligament to avulse a fragment off the anteroinferior cornerof the vertebral body. The height of the avulsed fragment usually exceeds its width. This fracture is morecommon in older patients with osteoporosis. The extension teardrop fracture is unstable in extension.
Laminar Fracture
Isolated laminar fractures are caused by hyperextension and may be associated with spinous process fractures.Laminar fractures are difficult to visualize on plain radiographs and usually require CT for diagnosis.
Uncinate Process Fracture
The lateral superior edges of the vertebral body form bilateral ridges, called the uncinate processes. Theseprocesses are found on the C3 to T1 vertebrae. Extreme lateral flexion may cause a transverse fracture at thebase of the uncinate process. Uncinate process fractures usually present with ipsilateral neurologic deficits, andother cervical spine fractures are common. Isolated uncinate process fractures are usually stable.
Thoracic and Lumbar Spine Fractures
Thoracic Spine (T1 to T10)
The thoracic spine is a rigid segment, with its stiffness enhanced 2.5 times by articulation with the rib cage.Relative to other regions of the vertebral column, a large force is necessary to overcome the intrinsic stabilityof the thoracic spine. Although injury to the thoracic spine is less common than in other regions, the presenceof a thoracic vertebral injury indicates that severe forces were present. The spinal canal in the thoracic regionis narrower than that found in either the cervical or lumbar spine. This narrowing relative to the spinal corddiameter increases the risk of cord injury. When spinal cord injuries occur in the thoracic region, most areneurologically complete. There is an important association between fractures of the thoracic spine andintrathoracic injuries. Patients with blunt chest trauma and mediastinal widening should be evaluated forboth aortic and thoracic spine injuries.
Thoracolumbar Junction (T11 to L2)
The thoracolumbar junction (T11 to L2) is considered a transitional zone between the highly fixed thoracic andrelatively mobile lumbar regions. This distinction is important because the transitional zones sustain the

13/10/15 9:24
Página 15 de 41about:blank
greatest amount of stress during motion and are most vulnerable to injury. In addition to this change in boneanatomy, the thoracolumbar junction serves as the level of transition from the end of the spinal cord (about L1)to the nerve roots of the cauda equina. Relative to the thoracic spine, the width of the spinal canal in thethoracolumbar region is greater. Therefore, despite a large number of vertebral injuries at the thoracolumbarjunction, most do not have neurologic deficits, or, if present, they are partial or incomplete.
Lumbar Spine (L3 to L5)
Relative to the thoracic and thoracolumbar regions, the lower lumbar spine is more mobile. Because of thewidth of the spinal canal in the lumbar region and the ending of the spinal cord at the L1 level, isolatedfractures of the lower lumbar spine rarely injure the spinal cord or result in neurologic injury. When neurologicinjuries occur, they are usually complete cauda equina lesions or isolated nerve root deficits.
Specific Thoracic and Lumbar Spine Fractures
Fractures of the thoracolumbar spine can be divided into minor and major injuries (Table 255-2). Minorinjuries are those that are localized to part of a column and do not cause instability. These fractures often resultfrom direct blunt trauma to the posterior elements of the spine. Often, these injuries are found when CT is usedto evaluate for potential intra-abdominal injury.
Table 255-2 Thoracic and Lumbar Spine FracturesMinor Injuries Major Injuries
Transverse process fracture Compression (wedge) fracturesSpinous process fracture Burst fracturesPars interarticularis fractures Flexion-distraction (“seat-belt”) injuries
Fracture-dislocation (translation) injuries
Compression fractures result from axial loading and flexion, with subsequent failure of the anterior column(Figure 255-10). The middle column remains intact. These injuries are usually stable unless they produce>50% decrease in vertebral body height. Compression fractures are unlikely to be directly responsible forneurologic damage.
Figure 255-10.
Wedge compression fracture. Wedge compression fractures are often caused by axial unloading with failure ofthe anterior column. A. Schematic of a compression fracture. B. Lateral reconstruction CT scan demonstratesthe anterior wedging. C. Axial CT scan demonstrates the anterior wedging and vertebral body fracture. Notethe lack of retropulsion of elements into the spinal canal.
Burst fractures occur following failure of the vertebral body under axial load (Figure 255-11). In contrast tocompression fractures, both the anterior and middle columns fail. There is retropulsion of bone and diskfragments into the canal that may cause spinal cord compression. Burst fractures are considered unstable.
Figure 255-11.

13/10/15 9:24
Página 16 de 41about:blank
Burst fracture. Burst fractures are also caused by axial loading. Both anterior and middle columns have failed.A. Schematic of the forces transmitted. B. Lateral reconstruction CT scan demonstrates failure of both theanterior and middle columns. C. Axial CT scan demonstrates the burst vertebral body. Note the retropulsion ofelements into the spinal canal.
Flexion-distraction injuries are commonly seen following seat belt–type injuries, particularly those in whichlap belts alone are used (Figure 255-12). The seat belt serves as the axis of rotation during distraction, andthere is failure of both the posterior and middle columns. The intact anterior column prevents subluxation.Typical radiographic findings reveal increased height of the posterior vertebral body, fracture of the posteriorwall of the vertebral body, and posterior opening of the disk space. Flexion-distraction injuries are consideredunstable. A variant of flexion-distraction injuries is the Chance fracture, a fracture complex that presents withminor anterior vertebral compression and significant distraction of the middle and posterior ligamentousstructures; usually including the interspinous ligament, ligamentum flavum, facet capsule, posterior annulus,and thoracodorsal fascia. These injuries are often misdiagnosed as an anterior compression fracture, butwhether or not a fracture is present, all three supporting columns are distracted, and this injury is unstable. Thepresence of an anterior compression fracture in the thoracolumbar transition zone (T11 to L2) in a restrainedyoung patient following a motor vehicle collision should suggest the possibility of a Chance fracture.
Figure 255-12.
Flexion-distraction injuries. Flexion-distraction injuries involve rotation of forces. This results in failure ofboth the posterior and middle columns. A. Schematic of the forces transmitted. B. Lateral view of plain filmdemonstrating a flexion distraction injury. C. Lateral CT reconstruction confirming the pattern, alsodemonstrating posterior opening of the disk space. D. Axial CT scan shows loss of the middle column withfracture through the lateral elements.
Fracture-dislocations are the most damaging of injuries (Figure 255-13). Compression, flexion, distraction,rotation, or shearing forces lead to failure of all three columns. The end result is subluxation or dislocationwith a grossly unstable spine (Figure 255-14).
Figure 255-13.
Fracture-dislocation injuries. Fracture dislocations are the most damaging of injuries leading to failure of allthree columns. A. Schematic demonstration of these injuries. B. Lateral CT reconstruction demonstrates lossof all three columns. C. Axial CT scan demonstrates the dislocation and displacement of the vertebral body.
Figure 255-14.
Fracture-dislocation injury CT with (A) axial, (B) sagittal, and (C) three-dimensional reconstructions shows aT10-T11 fracture-dislocation in a 37-year-old man who sustained a 20-ft fall.
Sacrum and Coccyx Fractures

13/10/15 9:24
Página 17 de 41about:blank
The sacrum supports the lumbar vertebral column and transmits loads from the trunk to the pelvic girdle andinto the lower limbs. The upper border articulates with the fifth lumbar vertebra, and the inferior borderarticulates with the coccyx. Laterally, the sacrum articulates with the iliac bones to form the sacroiliac joints.The vertebral foramina together form the sacral canal that contains the nerve roots of the lumbar, sacral, andcoccygeal spinal nerves and the filum terminale. The coccyx, which articulates with the sacrum, consists offour vertebrae fused together. Except for the first vertebra, the remaining coccygeal vertebrae consist of bodiesonly.
Injuries of the sacral spine and nerve roots are very unusual. When they occur, they are frequently associatedwith fractures of the pelvis. There are multiple different classification schemes of sacral fractures that help topredict neurologic deficits and establish treatment protocols. In general, transverse fractures through the bodyare most significant in that they cause injury to part or all of the cauda equina. Longitudinal fractures maycause radiculopathy. Sacral fractures that involve the central sacral canal can produce bowel or bladderdysfunction.5
Coccygeal injuries are usually associated with a direct fall onto the buttocks. Patients typically describe intensepain with sitting and straining. Diagnosis of a coccyx fracture is made on rectal examination by eliciting painwith motion of the coccyx. Imaging is not needed to diagnose coccygeal fractures. Treatment is symptomaticwith analgesics and use of a rubber doughnut pillow.
Mechanism of InjuryMotor vehicle crashes are the principal cause of injury to the spinal cord in developed countries. Otheretiologies, in descending order of frequency, include falls, gunshot wounds, and injuries secondary to sports orrecreational activities. Obvious neurologic deficits identify an unstable injury and the need for emergenttreatment. In the absence of deficits, the mechanism of injury with an understanding of the forces involved canguide management.
Blunt Injury
Motor Vehicle-Related Injuries
Motor vehicle crashes usually produce acceleration-deceleration injuries. The cervical spine is the mostsusceptible to injury by this mechanism, but the thoracic and lumbar regions are also at risk. The majority ofpatients seen in the ED for spine trauma following a motor vehicle crash are involved in low-impact crasheswith primarily soft tissue injuries. Patients usually describe pain in the posterior neck and back. High-speed,high-energy crashes are more likely to result in structural damage to the spine. Lap-only seat belts areassociated with thoracolumbar injuries.
Pedestrians struck by vehicles and motorcyclists are at considerable risk for multiple skeletal injuries,including spinal injuries.
Falls
Falls from a height produce axial loading forces and are associated with fractures of the lower extremities,pelvis, and spine. The most common site of spinal injury from a fall is the thoracolumbar junction. These

13/10/15 9:24
Página 18 de 41about:blank
fractures can he highly unstable with significant distraction (Figure 255-13).
Sports Injuries
The specific spinal injury from a sport is more related to the mechanism, the force involved, and the point ofapplication of the force, rather than to the specific sport. The majority of injuries are self-limiting soft tissueinjuries. Sports-related injuries can also damage the intervertebral disk and produce disk herniation ordegeneration. Injuries to bone can range from minimal avulsion-type fractures to compressions or fracturedislocations. Most bone injuries are not associated with neurologic sequelae. When neurologic impairmentoccurs, it is usually secondary to direct axial forces. Catastrophic spinal injuries have been associated withcontact sports (e.g., football, rugby, lacrosse, and ice hockey) and sports with the potential for falls andcollision with solid objects (e.g., gymnastics and diving) (Figure 255-14).6
Penetrating Injury
Most penetrating spinal cord lesions are caused by gunshot wounds. These wounds may be localized to thespine or may involve transperitoneal trajectories. The spinal cord may be injured by direct contact with thebullet, by bone fragments, or from concussive forces.7 Most gunshot wounds result in stable vertebral injuries,although associated spinal cord lesions are often complete. Stabbing injuries to the spinal cord are much lesscommon. These may be inflicted by a variety of implements, including knives, axes, ice picks, screwdrivers,and glass fragments. The majority of stab wounds that injure the spinal cord produce incomplete Brown-Séquard lesions in the thoracic section. Among incomplete spinal cord injuries, the prognosis for patients withstab injuries to the spine and incomplete paralysis is significantly better than for patients with gunshot woundsto the spine and a similar extent of paralysis.
Spinal Cord InjuriesDamage to the spinal cord is the result of two types of injury. First is the direct mechanical injury fromtraumatic impact. This insult sets into motion a series of vascular and chemical processes that lead tosecondary injury. The initial phase is characterized by hemorrhage into the cord and formation of edema at theinjured site and surrounding region. Local spinal cord blood flow is diminished owing to vasospasm andthrombosis of the small arterioles within the grey and white matter. Extension of edema may furthercompromise blood flow and increase ischemia. A secondary tissue degeneration phase begins within hours ofinjury. This is associated with the release of membrane-destabilizing enzymes, mediators of inflammation, anddisturbance of electrophysiologic coupling by disruption of calcium channel pathways. Lipid peroxidation andhydrolysis appear to play a major role in this secondary phase of spinal cord injury.
Spinal Cord Lesions
The severity of spinal cord injury determines the prognosis for recovery of function, so it is important todistinguish between complete and incomplete spinal cord injuries. Complete lesions have a minimal chance offunctional motor recovery. Patients with incomplete lesions are expected to have at least some degree ofrecovery. The American Spinal Injury Association defines a complete neurologic lesion as the absence ofsensory and motor function below the level of injury. This includes loss of function to the level of thelowest sacral segment. In contrast, a lesion is incomplete if sensory, motor, or both functions are partially

13/10/15 9:24
Página 19 de 41about:blank
present below the neurologic level of injury. This may consist only of sacral sensation at the analmucocutaneous junction or voluntary contraction of the external anal sphincter upon digital examination. Thedifferentiation between complete and incomplete spinal cord damage may be complicated by the presence ofspinal shock. Patients in spinal shock lose all reflex activities below the area of injury, and lesions cannotbe deemed complete until spinal shock has resolved.
There are four distinct incomplete spinal cord syndromes identified by predictable physical examinationfindings (Table 255-3).
Table 255-3 Incomplete Spinal Cord SyndromesSyndrome Etiology Symptoms Prognosis*
Anteriorcord
Direct anteriorcord compression
Complete paralysis below the lesion with loss of pain andtemperature sensation
PoorFlexion of cervicalspine
Preservation of proprioception and vibratory functionThrombosis ofanterior spinalartery
Centralcord
Hyperextensioninjuries
Quadriparesis—greater in the upper extremities than the lowerextremities. Some loss of pain and temperature sensation, alsogreater in the upper extremities
GoodDisruption ofblood flow to thespinal cordCervical spinalstenosis
Brown-Séquard
Transversehemisection of thespinal cord Ipsilateral spastic paresis, loss of proprioception and vibratory
sensation, and contralateral loss of pain and temperature sensation GoodUnilateral cordcompression
Caudaequina
Peripheral nerveinjury
Variable motor and sensory loss in the lower extremities, sciatica,bowel/bladder dysfunction, and “saddle anesthesia” Good
*Outcome improves when the effects of secondary injury are prevented or reversed.
A large number of descending and ascending tracts have been identified in the spinal cord. The three mostimportant of these in terms of neuroanatomic localization of cord lesions are the corticospinal tracts,spinothalamic tracts, and dorsal (posterior) columns.
The corticospinal tract is a descending motor pathway. Its fibers originate from the cerebral cortex throughthe internal capsule and the middle of the crus cerebri. The tract then breaks up into bundles in the pons andfinally collects into a discrete bundle, forming the pyramid of the medulla. In the lower medulla,approximately 90% of the fibers cross (decussate) to the side opposite that of their origin and descend throughthe spinal cord as the lateral corticospinal tract. These fibers synapse on lower motor neurons in the spinalcord. The 10% of corticospinal fibers that do not decussate in the medulla descend in the anterior funiculus ofthe cervical and upper thoracic cord levels as the ventral corticospinal tract. Damage to the corticospinal tract

13/10/15 9:24
Página 20 de 41about:blank
neurons (upper motor neurons) in the spinal cord results in ipsilateral clinical findings such as muscleweakness, spasticity, increased deep tendon reflexes, and a Babinski’s sign.
The two major ascending pathways that transmit sensory information are the spinothalamic tracts and thedorsal columns. The first neurons of both of these afferent systems begin as sensory receptors situated in theskin and stretch receptors of muscles. Their cell bodies are located in the dorsal root ganglia of the spinalnerves. The spinothalamic tract transmits pain and temperature sensation. As the axons of the first neuronsenter the spinal cord, most ascend one or two levels before entering the dorsal grey matter of the spinal cord,where they synapse with the second neuron of the spinothalamic tract. The second neuron immediately crossesthe midline in the anterior commissure of the spinal cord and ascends in the anterolateral funiculus as thelateral spinothalamic tract. When the spinothalamic tract is damaged in the spinal cord, the patientexperiences loss of pain and temperature sensation in the contralateral half of the body. The (pain andtemperature) sensory loss begins one or two segments below the level of the damage.
The dorsal columns transmit vibration and proprioceptive information. Neurons enter the spinal cord proximalto pain and temperature neurons. They differ from pain and temperature neurons in that they do notimmediately synapse in the spinal cord. Instead, these axons enter the ipsilateral dorsal column and do notsynapse until they reach the gracile or cuneate nuclei of the medulla. From these nuclei, fibers cross themidline and ascend in the medial lemniscus to the thalamus. Injury to one side of the dorsal columns will resultin ipsilateral loss of vibration and position sense. The sensory loss begins at the level of the lesion. Light touchis transmitted through both the spinothalamic tracts and the dorsal columns. Therefore, light touch is notcompletely lost unless there is damage to both the spinothalamic tracts and the dorsal columns.
Each spinal nerve is named for its adjacent vertebral body. In the cervical region, there is an additional pair ofspinal nerve roots compared to the number of vertebral bodies. The first seven spinal nerves are named for thefirst seven cervical vertebrae, each exiting through the intervertebral foramen above its corresponding vertebralbody. The spinal nerve exiting below C7, however, is referred to as the C8 spinal nerve, although no eighthcervical vertebra exists. All subsequent nerve roots, beginning with T1, exit below the vertebral body forwhich they are named.
During fetal development, the downward growth of the vertebral column is greater than that of the spinal cord.Because the adult spinal cord ends as the conus medullaris at the level of the lower border of the first lumbarvertebra, the lumbar and sacral nerve roots must continue inferiorly below the termination of the spinal cord toexit from their respective intervertebral foramina. These nerve roots form the cauda equina. A potentialconsequence of this arrangement is that injury to a single lower vertebra can involve multiple nerve roots inthe cauda equina. For example, an injury at the L3 vertebra can involve the L3 nerve root as well as the lowernerve roots that are progressing to a level caudal to the L3 vertebra.
Anterior Cord Syndrome
The anterior cord syndrome results from damage to the corticospinal and spinothalamic pathways, withpreservation of posterior column function. This is manifested by loss of motor function and pain andtemperature sensation distal to the lesion. Only vibration, position, and crude touch are preserved. Thissyndrome may occur following direct injury to the anterior spinal cord. Flexion of the cervical spine mayresult in cord contusion or bone injury with secondary cord injury. Alternatively, thrombosis of the anteriorspinal artery can cause ischemic injury to the anterior cord. Anterior cord injury can also be produced by anextrinsic mass that is amenable to surgical decompression. The overall prognosis for recovery of function

13/10/15 9:24
Página 21 de 41about:blank
historically has been poor and remains so today.6
Central Cord Syndrome
The central cord syndrome is usually seen in older patients with preexisting cervical spondylosis who sustain ahyperextension injury. As named, this injury preferentially involves the central portion of the cord more thanthe peripheral. The centrally located fibers of the corticospinal and spinothalamic tracts are affected. Theneural tracts providing function to the upper extremities are most medial in position compared with thethoracic, lower extremity, and sacral fibers that have a more lateral distribution. Clinically, patients with acentral cord syndrome present with decreased strength and, to a lesser degree, decreased pain andtemperature sensation, more in the upper than the lower extremities. Spastic paraparesis or spasticquadriparesis can also be seen. The majority will have bowel and bladder control, although this may beimpaired in the more severe cases. Prognosis for recovery of function is good; however, most patients do notregain fine motor use of their upper extremities.
Brown-SéQuard Syndrome
The Brown-Séquard syndrome results from hemisection of the cord. It is manifested by ipsilateral loss ofmotor function, proprioception, and vibratory sensation, and contralateral loss of pain and temperaturesensation. The most common cause of this syndrome is penetrating injury. It can also be caused by lateral cordcompression secondary to disk protrusion, hematomas, bone injury, or tumors. Of all of the incomplete cordlesions, Brown-Séquard syndrome has the best prognosis for recovery.
Cauda Equina Syndrome
The cauda equina is composed entirely of lumbar, sacral, and coccygeal nerve roots. An injury in this regionproduces a peripheral nerve injury rather than a direct injury to the spinal cord. Symptoms may includevariable motor and sensory loss in the lower extremities, sciatica, bowel and bladder dysfunction, and“saddle anesthesia” (loss of pain sensation over the perineum). Because peripheral nerves possess theability to regenerate, the prognosis for recovery is better than that for spinal cord lesions.
Neurogenic ShockInjury to the spinal cord at the level of the cervical or thoracic vertebrae causes peripheral sympatheticdenervation. The loss of sympathetic arterial tone results in decreased systemic vascular resistance and bloodpressure. Loss of sympathetic innervation to the heart (T1 through T4 cord levels) leaves the parasympatheticcardiac innervation via the vagus nerve unopposed, resulting in bradycardia, or an absence of reflextachycardia. In general, patients with neurogenic shock are warm, peripherally vasodilated, andhypotensive with a relative bradycardia. Patients tend to tolerate hypotension relatively well, as peripheraloxygen delivery is presumably normal. Bradycardia is characteristic but not universal. Loss of sympathetictone and subsequent inability to redirect blood from the periphery to the core may cause excessive heat lossand hypothermia.8
The diagnosis of neurogenic shock should be one of exclusion. Certain clues—such as bradycardia and warm,dry skin—may be evident, but hypotension in the trauma patient can never be presumed to be caused by

13/10/15 9:24
Página 22 de 41about:blank
neurogenic shock until other possible sources of hypotension have been excluded.9 A large percentage ofpatients will have significant concomitant injuries, with blood loss as the cause of their hypotension.9,10 Asearch for hemorrhage should be conducted before hypotension can be attributed solely to neurogenic shock.
Treatment of Neurogenic Shock
Loss of sympathetic innervation during neurogenic shock results in blood pooling in the distal circulation.Infusion of IV crystalloid will correct this relative hypovolemia. Adequate fluid resuscitation should beundertaken, with the aim of keeping the mean arterial blood pressure at 85 to 90 mm Hg for the first 7 daysafter acute spine injury.11 Though a bit arbitrary, it has been determined by collective clinical experience thatthis level of pressure provides adequate perfusion and minimizes the effects of secondary cord injury.12 Theaggressive use of fluids in neurogenic shock should be performed with careful monitoring, as there is danger ofexcessive fluid replacement, with resultant heart failure and pulmonary edema.13 The placement of apulmonary artery catheter and its resultant pressure measurements can be of tremendous benefit in helping toprevent excess fluid administration. If IV fluids are not adequate to maintain organ perfusion, positiveinotropic pressor agents may be beneficial adjuncts to improve cardiac output and raise perfusionpressure.14 Optimal combinations and doses of these agents are variable and should be titrated to the patient’shemodynamic response.
Bradycardia, when present, usually occurs within the first few hours or days after spinal cord injury because ofa predominance of vagal tone to the heart. In cases of hemodynamically significant bradycardia, atropine maybe needed. In rare instances, patients will have an atrioventricular conduction block, with significantbradycardia requiring a pacemaker.
Spinal ShockThe syndrome neurogenic shock must be differentiated from spinal shock; the two terms have very differentmeanings and are not interchangeable. Spinal shock refers to the temporary loss or depression of spinalreflex activity that occurs below a complete or incomplete spinal cord injury. The lower the spinal cordinjury, the more likely that all distal reflexes will be absent.15 Loss of neurologic function that occurs withspinal shock can cause an incomplete spinal cord injury to mimic a complete cord injury. Therefore, cordlesions cannot be deemed complete until spinal shock has resolved. The bulbocavernosus reflex is among thefirst to return as spinal shock resolves. The duration of spinal shock is variable; it generally persists for days toweeks.
General Approach to Patients with Spinal Injury
Prehospital Care
The prehospital treatment of patients with spinal injury involves recognition of patients at risk, appropriateimmobilization, and triage to an appropriate facility (see Chapter 1, Emergency Medical Services, and Chapter2, Prehospital Equipment and Adjuncts). A basic EMS principle is that patients who have complaints of neckor back pain or who have tenderness on prehospital assessment should be presumed to have a spine injury until
13/10/15 9:24
Página 23 de 41about:blank
proven otherwise. In addition, patients with significant injury above the clavicles are also presumed to havecervical spine injury, regardless of related complaints. Also, patients with neurologic complaints should bepresumed to have a spinal cord injury. Sometimes this is obvious, as in a patient with flaccid paraplegia. Moreoften, symptoms are much more subtle (numbness or tingling in an extremity). Transport to an appropriatefacility is important, as the outcome of treatment of these injuries is somewhat time related. Therefore, initialtriage to a center that is capable of rapid diagnostics and therapeutics is important to optimize outcomefollowing spinal injury.
Field assessment can be difficult. Patients may have a concomitant head injury that makes them unable todescribe their injuries and hence does not allow for neurologic assessment. Other injuries may precludeaccurate neurologic assessment. The mechanism of injury is an important criterion on which prehospitalproviders can rely. High-speed or rollover vehicular crashes, falls from a substantial height (injuries to thethoracolumbar junction), and diving and surfing accidents typically produce cervical spine injuries. A patient atrisk by mechanism of injury may also be presumed to have a spinal cord injury. Although this may result in asubstantial rate of overtriage, this is acceptable because the consequences of undertriage can be devastating.
Prehospital care for spinal injuries involves immobilization of the entire spine at the scene, withimmobilization maintained during transport. The cervical spine can be immobilized with a rigid cervical collarsupplemented with external rigid objects placed bilaterally (e.g., sandbags or solid foam blocks) and with tapeor self-adhesive straps applied across the forehead to hold the head to the backboard. The thoracic and lumbarspine can be immobilized using a long backboard, and patients are usually “papoosed” onto the board tomaintain spinal alignment during transport. As described, efforts should be made to transport patients withsymptomatic spinal injuries to the regional spine center to avoid delays engendered by initial transport to adifferent site that may result in delays to definitive care.
ED Stabilization
ED evaluation of the patient with potential spinal injury should not differ substantially from that of any patientwith multiple injuries. Consideration should be given to immediate airway control in patients with cervicalspine injuries, no matter how apparently stable at the time of presentation. The higher the level of spinal injury,the more compelling the indication for early airway intervention. The roots of the phrenic nerve, which supplythe diaphragm, emerge at the third, fourth, and fifth cervical vertebral levels. Thus, any patient with aninjury at C5 or above should have his or her airway secured via endotracheal intubation. It may beprudent to intubate patients with cervical cord lesions even below this level. Significant spinal cord edema mayprogress rostrally to involve the roots of the phrenic nerve. Many patients can initially support ventilatoryfunction utilizing intercostal muscles or abdominal breathing, but they eventually tire and subsequentlydevelop respiratory failure.
If possible, the neurologic assessment should be performed before patients are intubated and sedated. Spinalimmobilization should be maintained while securing the airway. This is usually accomplished usingorotracheal intubation with in-line cervical stabilization (without distraction force) and cricoid pressure.Injudicious motion of an unstable cervical spine fracture can worsen or produce spinal cord injury.
Hypotension is initially treated with IV crystalloid. Because hypotension in patients with spinal cord injuriesmay be due to neurogenic shock, blood loss, cardiac injury, or a combination, it should never be assumed thata patient with hypotension and bradycardia is suffering from isolated neurogenic shock. Vital signs cannot berelied upon to differentiate among these causes; patients in hemorrhagic shock with intraperitoneal bleedingmay have a vagal response and not be able to mount a tachycardic response. Blood loss should be presumed
13/10/15 9:24
Página 24 de 41about:blank
to be the cause of hypotension until proven otherwise. More than 90% of hypotensive patients withpenetrating spinal cord injury have blood loss to at least partly explain their hypotension.9,10
Patients with spinal injury can have associated intrathoracic, retroperitoneal, intraperitoneal, or pelvichemorrhage. A chest radiograph will usually identify significant blood loss within the thorax. Retroperitonealbleeding may occur with concomitant pelvic fractures or may be secondary to lumbar arterial bleeding fromspine fractures, especially in patients with substantial falls from a height. Retroperitoneal bleeding should besuspected in patients without evidence of intra-abdominal blood loss who develop abdominal distention ortenderness.16 Retroperitoneal hemorrhage is usually found on CT scanning. Intraperitoneal hemorrhage isusually associated with solid organ damage and may be detected by sonographic or CT imaging. Pelvichemorrhage can be more difficult to diagnose and treat; angiography may be necessary for both diagnosis andtreatment of active bleeding.
Neurologic Examination
Once patients are stabilized and other life-threatening injuries have been excluded or treated, a detailedneurologic assessment should be performed. Details of history include whether the patient has had a loss ofconsciousness or other neurologic symptoms at the scene. A patient who was asymptomatic in the field andexperiences subsequent neurologic deterioration in the ED requires emergent assessment. The presence ofurinary or fecal incontinence or priapism identifies a patient at high risk for spinal cord injury.
Physical examination should delineate the level of spinal cord injury (Figure 255-15). An appropriatelydetailed initial neurologic examination is important to allow for comparison later should a patient deteriorate.The presence or absence of neck or back tenderness should be noted. Motor function for muscle groups shouldbe tested (Table 255-4). The level of sensory loss should be determined (Figure 255-16). Proprioception orvibratory function should be investigated to examine posterior column function. Deep tendon reflexes shouldbe tested. Anogenital reflexes should also be tested because “sacral sparing” with preservation of thereflexes denotes an incomplete spinal cord level, even if the patient has complete sensory and motor loss.To test the bulbocavernosus reflex, the penis is squeezed to determine whether the anal sphinctersimultaneously contracts. Rectal tone can be assessed at the same time. The cremasteric reflex is tested byrunning a pin or a blunt instrument up the medial aspect of the thigh. If the scrotum rises, there is some spinalcord integrity. The area around the anus should be tested with a pin. An “anal wink reflex” (contraction of theanal musculature) indicates at least some sacral sparing. Conversely, priapism implies a complete spinal cordinjury.
Figure 255-15.
Spinal cord level. The spinal cord level of injury can be delineated by physical examination, including adetailed neurologic examination.
Table 255-4 Motor Grading SystemGrade Movement0 No active contraction1 Trace visible or palpable contraction2 Movement with gravity eliminated
13/10/15 9:24
Página 25 de 41about:blank
3 Movement against gravity4 Movement against gravity plus resistance5 Normal power
Figure 255-16.
Dermatomes for sensory examination.
Diagnostic Imaging
Patients with suspected spine or spinal cord injury should have diagnostic imaging; the challenge is identifyingthe appropriate patient and selecting the appropriate imaging modality. It is not practical nor prudent to imagethe spine in every patient who presents to the ED after sustaining trauma. Therefore, clinical guidelines havebeen developed to assist the physician’s judgment in deciding whom to image. In addition, the differentimaging modalities have their own particular value in detecting injuries to the bone, ligamentous structures,and spinal cord.
Cervical Spine Imaging
Patients with head or neck trauma who are not fully alert (Glasgow Coma Scale score of <15) should undergoimaging of their cervical spine. The frequency of cervical spine injury in association with blunt head trauma isapproximately 2% to 5%, but frequency increases to almost 9% in patients with significant head injury, definedas a Glasgow Coma Scale score of <10 in one study.17
The utility of imaging of the cervical spine in patients who are alert, oriented, and have no neck or back painor tenderness is negligible. Two clinical decision rules have been defined, which target low-risk traumapatients, to avoid unnecessary radiography. These rules are intended for alert, stable adult trauma patients whohave no neurologic deficits. The National Emergency X-Radiography Utilization Study (NEXUS) groupdetermined that cervical spine imaging would be unnecessary in patients who demonstrate five clinical criteria(Table 255-5).18 In the original study, the NEXUS criteria were 99.6% sensitive for detecting clinicallysignificant cervical spine injuries, but only 12.9% specific.
Table 255-5 National Emergency X-Radiography Utilization Study Criteria: Cervical Spine ImagingUnnecessary in Patients Meeting These Five CriteriaAbsence of midline cervical tendernessNormal level of alertness and consciousnessNo evidence of intoxicationAbsence of focal neurologic deficitAbsence of painful distracting injury
The Canadian Cervical Spine Rule for Radiography was developed for alert, stable trauma patients to reducepractice variation and inefficiency in the ED use of cervical spine radiography.19 The Canadian Rule consistsof three questions or assessments; if the answer to any one of the three is “no,” then imaging is performed

13/10/15 9:24
Página 26 de 41about:blank
(Table 255-6). In the original study, the Canadian Cervical Spine Rule had 100% sensitivity and 42.5%specificity for identifying patients with “clinically important” cervical spine injuries, suggesting that thisclinical rule could significantly reduce the use of imaging ordered for alert, stable trauma patients.
Table 255-6 Canadian Cervical Spine Rule for Radiography: Cervical Spine Imaging Unnecessary in PatientsMeeting These Three Criteria
Question or Assessment Definitions
There are no high-risk factorsthat mandate radiography.
High-risk factors include:Age 65 years or olderA dangerous mechanism of injury (fall from a height of >3 ft; an axial loadinginjury; high-speed motor vehicle crash, rollover, or ejection; motorizedrecreational vehicle or bicycle collision)The presence of paresthesias in the extremities
There are low-risk factors thatallow a safe assessment ofrange of motion.
Low-risk factors include:Simple rear-end motor vehicle crashesPatient able to sit up in the EDPatient ambulatory at any timeDelayed onset of neck painAbsence of midline cervical tenderness
The patient is able to activelyrotate his/her neck. Can rotate 45 degrees to the left and to the right
These two decision tools were developed for slightly different purposes and had a different outcome definition,so it is not appropriate to conclude that one rule is diagnostically better than the other.20,21 In experiencedhands, either rule is useful for its intended purpose.21
The NEXUS and Canadian Cervical Spine rules were designed to identify “low-risk” patients (e.g., with a riskof <0.5% or <5 per 1000 for cervical spine injury) who do not require imaging. Other decision rules have beendeveloped to identify “high-risk” patients (e.g., with a risk >5% or > 50 per 1000 for cervical spine injury)who should undergo early advanced imaging (Table 255-7).22,23
Table 255-7 Patients at High Risk for Cervical Spine Injury
Injury mechanism
High speed (>35 mph or 56 kph combined impact) motor vehicle crashMotor vehicle crash with death of an occupantPedestrian stuck by moving vehicleFall from height >10 ft or 3 m
Primary clinical assessmentSignificant or serious closed head injury*Neurologic symptoms or signs referable to the cervical spinePelvic or multiple extremity injuries
Additional information Intracranial hemorrhage seen on CT
*The definition of significant or serious head injury is subjective, but may include intracranial hemorrhage,parenchymal contusion, skull fracture, or persistent altered level of consciousness or unconsciousness.

13/10/15 9:24
Página 27 de 41about:blank
Cervical Spine Plain Radiography
Standard radiography for the identification of bony cervical injury includes three views of the cervical spine:lateral, anteroposterior, and odontoid. These views allow for imaging of the entire cervical spine. It isimportant that all seven cervical vertebrae be imaged, including the junction between the seventh cervical andthe first thoracic vertebrae. A single lateral cervical spine film will identify approximately 90% of injuries tobone and ligaments.24 The lateral view should be inspected for proper alignment (Figure 255-17). Theanterior vertebral body line, posterior vertebral body line, and spinolaminar line should all be smooth anduninterrupted. The loss of normal cervical lordosis is indicative of muscle spasm and may indicate spinalinjury. The soft tissues should be examined for the presence or absence of prevertebral swelling. Prevertebralswelling is generally secondary to a hematoma and is consistent with spinal column injury. The prevertebralspace anterior to C3 should be <5 mm. The predental space should be <3 mm in an adult. The open-mouthodontoid view will identify many of the remaining abnormalities. Cervical spine immobilization should bemaintained during imaging. If the initial lateral view is normal and the patient is neurologically intact, theanteroposterior and open-mouth views can be delayed until other injuries are adequately stabilized. If optimalradiographs are obtained, the combination of lateral, anteroposterior, and odontoid views is generally adequateto identify, or at least raise the suspicion of, most clinically important cervical spine injuries.
Figure 255-17.
Lateral cervical spine alignment. Vertebral alignment of the lateral cervical spine: (1) anterior vertebral bodyline, (2) posterior vertebral body line, (3) spinolaminar line, and (4) spinous processes line.
Cervical radiography has limitations. Plain films are poor for imaging C1 and C2. In addition, visualization ofthe entire cervical spine via plain films is often problematic. Patients’ body habitus may not allow visualizationof all seven vertebral bodies. An alternative is a swimmer’s view, which is aimed through the axilla in anattempt to image the lower cervical spine. Oblique views (45 degrees) can also be obtained. These views havethe added advantage of showing the neural foramina, visualizing the pedicles, and identifying the laminae.
Cervical Spine CT
High-speed, high-resolution multidetector CT scan has greatly enhanced the ability to image the cervical spine.CT is more sensitive and specific than plain radiography for evaluating the cervical spine in traumapatients, and can be performed in a more expeditious fashion.25–30CT can be used to visualize the entirecervical spine and is particularly useful at the craniocervical and cervicothoracic regions, where plain films areoften limited.
The current trend in most trauma centers is to use CT as the initial imaging modality to evaluate thecervical spine, and CT scanning is the imaging modality of choice for suspected cervical spine fractures.
Evaluation for Cervical Ligamentous Injury
Plain films, and even CT imaging of the cervical spine, may not identify patients with pure ligamentousinjuries. In these patients, the ligaments are disrupted, but the spine spontaneously reduces to a normalposition. The resulting instability risks subsequent neurologic injury if the spine moves.

13/10/15 9:24
Página 28 de 41about:blank
Flexion-extension radiographic views can be used to assess spinal column stability. They should only be donein a fully awake, unsedated, cooperative patient who has pain or tenderness with normal plain radiographicimages. With direct physician observation, the seated patient carefully and slowly flexes and extends his or herneck, with motion limited by increasing pain or the appearance of any neurologic symptom. Radiographs areobtained in the flexed and extended positions with a step-off of 3.7 mm or an angulation of >11 degreesdenoting cervical spine instability.31 The role of flexion and extension views following an acute injury islimited because it is possible to have normal flexion-extension films with ligamentous disruption, as muscletone can splint the bones in a stable configuration. Most patients in this latter category note pain improvementwith analgesics after a few days.
Reliable patients with persistent pain but normal imaging studies, including flexion/extension radiographs if soobtained, can be discharged in a hard collar with outpatient follow-up in 3 to 5 days. Most patients’ symptomswill resolve over a few days. A patient with persistent pain will require additional imaging. Unreliable patientswith persistent pain and normal plain radiographic or CT images should be considered for an MRI study,although this is rarely indicated as part of the initial investigation.
Thoracic and Lumbar Spine Imaging
Many of the same principles used for cervical spine imaging can be applied to thoracic and lumbar imaging(Table 255-8).32 The determination of a spinal column injury at one level should prompt imaging of theremainder of the spine; approximately 10% of patients with a spine fracture in one segment will have asecond fracture at another.
Table 255-8 Indications for Thoracic and Lumbar Imaging after Trauma
Mechanism
GunshotHigh energyMotor vehicle crash with rollover or ejectionFall >10 ft or 3 mPedestrian hit by car
Physical examinationMidline back painMidline focal tendernessEvidence of spinal cord or nerve root deficit
Associated injuries
Cervical fractureRib fracturesAortic injuriesHollow viscus injuries
Patients should be moved off the hard backboard and maintained in a flat, supine position on the gurneymattress. Skin breakdown and pressure sores can develop very quickly, particularly in obese patients, fromlaying on a hard surface, and the standard hospital mattress provides adequate spinal support. Patientsshould be carefully moved with maintenance of spinal immobilization during transfers from bed to stretcher. Itmay be helpful to place patients on a scoop stretcher or back on a backboard for the transportation phases oftheir care. The thoracic spine has inherent stability from the rib cage, and few fractures in these patients will beunstable.

13/10/15 9:24
Página 29 de 41about:blank
Plain radiographs of the thoracic and lumbar spine may be obtained as the initial imaging of these spinallevels, but improvements in CT technology has rendered the role for plain films in thoracic or lumbar injurymore limited. Anterior and lateral films are generally obtained and examined for abnormality. Patients withpoint tenderness and normal plain radiographs are a clinical dilemma; CT imaging can be useful in this subset,although the yield for detecting fractures is low.
As with the cervical spine, CT has assumed a much more important role in the imaging of thoracic and lumbarinjuries. Newer-generation multidetector CT scanning is rapid and allows for complete three-dimensionalimaging of bone structures. CT scanning is indicated in almost all patients with proven bony spinal injury,subluxations, neurologic deficits (but no apparent abnormalities on plain films), severe neck or back pain (withnormal plain films), and when the thoracic and lumbar spine should be examined to define the anatomy of afracture and the extent of impingement on the spinal canal. Rather than obtaining separate plain radiographs ordedicated CT images, the thoracic and abdominal CT scans obtained to evaluate the multiple trauma patientcan be reformatted and used to reconstruct images of the thoracic and lumbar spine.33,34 CT can reveal theanatomy of an osseous injury, grade the extent of spinal canal impingement by bone fragments, and assess thestability of an injury.
MRI is not as sensitive as CT for detecting or delineating bone injuries, but is superb at defining neural,muscular, and soft tissue injury.35,36 MRI is the diagnostic test of choice for describing the anatomy ofnerve injury. Entities such as herniated disks or spinal cord contusions can also be delineated on MRI.Although many of the neural or soft tissue injuries may require only supportive therapy, some require acutesurgical intervention, and early identification helps plan therapy for all. MRI is indicated in patients withneurologic findings with no clear explanation after plain films and CT scanning. CT myelography is analternative when MRI is unavailable and immediate diagnosis of a spinal cord or other neurologic lesion isrequired. If the patient is neurologically stable and MRI is unavailable, delayed MRI or transfer to a tertiarycare facility may be appropriate.
Treatment of Spinal InjuriesThe goals of treatment are to prevent secondary injury, alleviate cord compression, and establish spinalstability. Spinal immobilization should be maintained and movement kept to a minimum.
After initial patient stabilization, if a neurologic deficit is present or the patient has an unstable spinal column,subspecialty consultation should be requested emergently. The consultant, be it a neurosurgeon or orthopedicsurgeon, should have the opportunity to perform an appropriate neurologic examination early in the patient’scourse. Patients with progressive neurologic deterioration may require urgent surgical intervention.
Corticosteroids
High-dose methylprednisolone remains a controversial treatment in acute blunt spinal cord injury. In1990, the National Acute Spinal Cord Injury Study (NASCIS) group published the results of a series of multi-institutional studies to evaluate the efficacy of methylprednisolone in spinal trauma.37 The articles reportedthat methylprednisolone infusion resulted in improvement of both motor and sensory function inpatients with complete and incomplete neurologic lesions. This positive outcome was dependent upondosage of steroids and time of administration (Table 255-9).

13/10/15 9:24
Página 30 de 41about:blank
Table 255-9 The National Acute Spinal Cord Injury Study Protocol
IndicationsBlunt traumaNeurologic deficit referable to the spinal cordTreatment can be started within 8 h of injury
TreatmentMethylprednisolone, 30 milligrams/kg bolus, is administered IV over 15 minFollowed by a 45-min pauseMethylprednisolone, 5.4 milligrams/kg/h, is then infused for 23 h
This protocol was evaluated only in patients with blunt spinal cord injury; penetrating injuries were excludedfrom the study. Massive steroid therapy has not been found to be effective in penetrating spinal cordinjury, and in fact, may impair recovery of neurologic function.38
The major neuroprotective mechanism by which high-dose methylprednisolone is believed to work is itsinhibition of free radical–induced lipid peroxidation. Other proposed beneficial actions include its ability toincrease levels of spinal cord blood flow, increase extracellular calcium, and prevent loss of potassium frominjured cord tissue. Methylprednisolone is advocated in preference to other steroids because it crosses cellmembranes more rapidly and completely.
The results of the NASCIS clinical trials have been criticized as not providing sufficient clinical evidence tosupport the use of steroids in acute spinal cord injury. Reassessment and meta-analysis by other authors havequestioned the validity of the NASCIS trials and the effectiveness of high-dose steroid therapy in thesepatients.39,40 The current guidelines of the American Association of Neurological Surgeons, published in2002, state that there is insufficient evidence to support the use of methylprednisolone as a treatment standardor guideline, and that “methylprednisolone for either 24 or 48 hours is recommended as an option in thetreatment of patients with acute spinal cord injuries that should be undertaken only with the knowledge that theevidence suggesting harmful side effects is more consistent than any suggestion of clinical benefit.”41Potential complications associated with prolonged, high-dose steroids, such as pneumonia, sepsis, woundinfection, thromboembolism, GI bleeding, and delayed healing are frequently cited concerns.
Penetrating Injury
There are additional considerations in evaluating and treating penetrating spinal trauma (Figure 255-18).Optimal treatment of these injuries has been the subject of debate. One concern is that of infectiouscomplications related to the presence of foreign bodies and contamination associated with transperitoneal andtransintestinal trajectories of gunshot wounds to the spine. In gunshot wounds with a transabdominaltrajectory, prophylactic broad-spectrum IV antibiotics are indicated and should be given in the ED. Surgicaldebridement with laminectomy has not proven effective in reducing the incidence of infectious complications,as most are managed nonoperatively.
Figure 255-18.
Algorithm for gunshot injury to spine. *Consider bullet removal in thoracolumbar region.
As with blunt trauma, there is general agreement that progressive neurologic deficits warrant surgical
13/10/15 9:24
Página 31 de 41about:blank
decompression. The indication for removal of bullet and bone fragments in those patients with nonprogressiveneurologic deficits is less clear. Wound location may determine the need for surgical intervention. Bulletremoval does not significantly improve the neurologic status of patients with stable cervical and thoracic spinalcord lesions. In contrast, bullet removal from the thoracolumbar region (T11 to L2) may significantly improvemotor recovery in both complete and incomplete injuries.42 Most gunshot wounds to the spine are stable andrequire only symptomatic treatment with a supportive orthosis and analgesics.
Patients who present with stab wounds to the spinal region with no neurologic deficits should receiveantibiotics and local wound care. CT may be performed to evaluate for a retained foreign body. If no metallicforeign bodies are present, neurologic deficits are best evaluated with MRI. Progressive neurologic deficits aregenerally treated surgically.
Stab wounds to the cervical spine may directly penetrate the spinal cord neural elements, produce spinalinfarction, or rarely cause a spinal epidural hematoma, as well as potentially injure other structures in the neck(see Chapter 257, Trauma to the Neck). Vertebral instability is generally not an issue, and delayed deficits arerare following a cervical spine stab wound. When they do occur, they are usually related to retained fragmentof blade within the spinal canal.
Nonoperative Spinal Stabilization
The goal of stabilization is to reduce deformities and then restrict motion and maintain alignment. In thecervical spine, it is important to determine the adequacy of cervical bone reduction. Subluxations are generallyreduced using Gardner-Wells tongs, which are placed into the soft tissue of the temples under local anesthesia.
Spinal orthoses are used to immobilize well-reduced cervical fractures. The cervical spine is the region mosteffectively stabilized by external splinting devices because there is less soft tissue separating the brace fromthe spine at this level. In addition, some braces can be solidly secured by fixation points at the cranium and thethoracic cage. Cervical orthoses consist of cervical and cervicothoracic types. Cervical collars fit around theneck and contour to the mandible and occiput. They restrict flexion and extension in the middle and lowercervical spine. Lateral bending and rotational movements, however, are poorly controlled. Examples ofcervical orthoses include the hard collar, the Philadelphia collar, and the Miami J collar (see Chapter 2,Prehospital Equipment and Adjuncts). Cervicothoracic braces provide additional support, with the “goldstandard” being the halo cervical immobilizer, which provides the most rigid stabilization. Consisting of a haloring pinned to the skull, a vest, and upright posts, it can be used for traction and reduction of unstablefractures, as well as immobilization.
Immobilization of the upper thoracic spine by orthoses is difficult, but, fortunately, an intact rib cage andsternum provide relative stability. Although brace immobilization is not always necessary in the treatment ofthese fractures, braces can provide additional comfort. Thoracic corsets provide minimal control of motion andare appropriate only for minor injuries. Jewett and Taylor-Knight braces provide intermediate control of spinalmotion. Maximum limitation of motion is provided by the Risser jacket and the body cast.
The thoracolumbar junction and lower lumbar regions are also difficult to immobilize externally. Splints arelimited by lack of an adequate caudal fixation point. The functions of most thoracolumbosacral orthoses arethe following: to create an awareness and remind the patient to restrict movements, to support the abdomenand relieve some of the load on the lumbosacral spine, to provide some restriction of motion of the upperlumbar and thoracolumbar spine by three-point fixation, and to reduce lumbar lordosis in order to provide astraighter, more comfortable lower back.

13/10/15 9:24
Página 32 de 41about:blank
Complications of external immobilization devices include pain, pressure, muscle weakness and disuse atrophy,venous compromise, psychological dependence, ineffective stabilization, and pin-site complications (halovest).
Operative Management of Spine Injuries
The indication for operative stabilization is somewhat controversial and varies from institution to institution.Those favoring an aggressive approach stress the importance of early mobilization of the multiply injuredpatient, as it helps decrease pulmonary problems, skin breakdown, deep venous thrombosis, and pulmonaryembolus. Rigid fixation may also decrease time in hospital as well as long-term pain and deformities. Thoseadvocating a nonoperative approach point out the possibility of worsening neurologic performance byoperative manipulation. In addition, the long-term results with operative intervention may not be substantiallybetter than with nonoperative therapy.
All would agree that progressive neurologic deterioration is an indication for urgent surgery. In addition,spinal instability should most often be managed operatively, even in the case of a complete spinal cord level,as this helps prevent long-term deformity.
Pediatric Spine and Spinal Cord InjuriesSpinal injuries occur less frequently in children than in adults. However, when children sustain these injuries,they are often devastating and result in debilitating long-term neurologic disability. Diagnosis of pediatricinjury can be challenging as young children are frequently unable to communicate their disabilities or describepain, and they may not readily cooperate with physical examination or diagnostic evaluation. Unique anatomicfeatures of the pediatric spine predispose children to different patterns of injury than adults. In addition,imaging may not readily reveal radiographically occult injuries or may identify normal pediatric variants thatare difficult to interpret. Any child with a significant mechanism of injury or history suggestive of spinal cordinjury requires a thorough, systematic evaluation.
Motor vehicle crashes, sports-related injuries (e.g., football, diving, soccer, rugby, ice hockey), falls fromheights, and child abuse are the most common causes of spinal injury in children.43–45 Penetrating traumaand gunshot wounds are rare in young children but increase in prevalence throughout adolescence.
Developmental Features of the Pediatric Spine
In children <10 years of age, spinal injury occurs mainly in the upper cervical vertebrae and is associated witha high risk of neurologic sequelae (Table 255-10). Beyond 10 years of age, the fulcrum of cervical spinemovement approaches that of the adult patient, and the majority of injuries in older children occur in the lowercervical spine, similar to adults. Multilevel spinal injuries occur more frequently in children, withapproximately 16% occurring at noncontiguous levels.43–45 This association stresses the importance ofcomplete examination of the entire vertebral column.
Table 255-10 Developmental Features Associated with Pediatric Cervical Spine InjuryChildren <10 y of age: injury mainly in upper cervical vertebraeLigamentous laxity and hypermobility
13/10/15 9:24
Página 33 de 41about:blank
Incomplete ossification of cartilaginous elementsHorizontal orientation of shallow facet jointsPoorly developed, weak cervical musculatureLarge head to body ratioChildren >10 y of age: majority of injuries in lower cervical spine
Clinical Features
As in adults, assessment and restoration of airway, breathing, and circulation occurs while maintaining neutralcervical spine immobilization. A brief neurologic evaluation should be done as part of the primary survey.
If the history or mechanism of injury suggests spinal cord injury, it is important that spinal immobilization bemaintained until a complete assessment, including appropriate imaging studies, is accomplished. A modifiedlong board for spinal immobilization may be required to accommodate the relatively large occiput of smallchildren to prevent inadvertent flexion of the cervical spine. The risk of maintaining immobilization in anuncooperative child, who may require sedation, must be balanced with that of secondary injury to a childallowed to move freely with an unstable spinal injury. Clinical criteria may be applied by experiencedclinicians to cooperative patients with low-risk injuries to help determine the need for continued cervical spineimmobilization, but limited data exist to fully utilize the NEXUS or Canadian Cervical Spine Rule forRadiography criteria with confidence in the pediatric population. Removal of helmets and shoulder pads toobtain radiographs must be conducted cautiously while maintaining in-line immobilization and gentle spinalcord traction.
Given the difficulties of adequately evaluating an injured child, a high index of suspicion must be maintainedfor all those at risk for spinal injuries. In addition, there is a high incidence of concomitant injuries in childrenwith spine injuries, including head (25% to 50%), extremity (30%), and thorax (21%).46–48 A thoroughsecondary survey is necessary to avoid missed injuries.
Specific Spine Injuries in Pediatric Patients
Occipitoatlantal dislocation is a rare occurrence following motor vehicle crashes and falls, with young childrenat particular risk. This injury commonly causes cardiorespiratory arrest and anoxic brain damage.Occipitoatlantal dislocation is usually fatal, and most survivors suffer severe neurologic damage. Axialcompression resulting in a Jefferson burst fracture of C1 is rare in children. Typically, these fractures are seenin teenagers following motor vehicle crashes and diving accidents.
Odontoid fractures are among the most common cervical spine injuries in children.49 These fractures must notbe confused with the normal anatomic variations in the odontoid due to synchondrosis between the body of theaxis and the odontoid, which may be seen in children up to 7 years of age. Fractures of the body and neuralarch of the axis (C2) are less common than fractures of the odontoid process and the atlas. The usualmechanism involves hyperextension, resulting in a hangman’s fracture with bilateral fracture of the parsinterarticularis of the axis, horizontal tearing of the C2-C3 disk, and anterior subluxation of C2 on C3.Neurologic damage occurs if the fracture extends to the vertebral foramina with injury to the vertebral artery. Itis considered an unstable fracture.
Injuries to the mid- and lower cervical spine more closely follow the adult-type pattern and account for 14% of

13/10/15 9:24
Página 34 de 41about:blank
vertebral fractures in children.44,45 Facet disruption without associated fractures may occur in childrenbecause of ligamentous laxity. Cervicothoracic junction injury is rarely reported in children <10 years of age.
Pure ligamentous injuries may result in delayed instability, even when initial radiographs appear normal.Children present with persistent neck pain, stiffness, or muscle spasm. Prevertebral swelling, loss of lordosis,widening of interspinous distances and the occasional dimple fracture of a vertebral body are clues to thediagnosis.
Thoracolumbar fractures, though rare in children, can have devastating consequences. These injuries arefrequently overlooked during the pediatric trauma assessment. Significant morbidity and long-term neurologicsequelae have been reported following thoracolumbar injuries. These fractures most commonly result fromhigh-impact or rapid deceleration, falls from heights, vehicular crashes, and contact sports. Mechanism ofinjury is generally hyperflexion of the lower thoracic or upper lumbar vertebrae with subsequent posteriorligamentous disruption. Diagnosis may be delayed or missed because of a lack of clinical signs. Long-termstructural or functional impairment may go unrecognized until later in childhood or adulthood.50
Associated Injuries
Spinal cord injury without radiologic abnormality, or SCIWORA, refers to the lack of evidence of vertebralfracture or malalignment on plain radiographs and CT in a patient with spinal cord injury. It is more commonin younger children and occurs most frequently with cervical spine injuries. SCIWORA has been reported inup to 55% of thoracolumbar injuries in the pediatric population.51 Despite the lack of findings on radiographyor CT, MRI has shown significant pathology in many of these patients.
Two theories have been described to explain SCIWORA: (1) developmental characteristics of the immaturespine allow for transient excessive movement during trauma, with subsequent cord distraction or compression;and (2) cord ischemia occurs due to direct vessel injury or hypoperfusion.
Delayed onset of neurologic damage is usually apparent within 48 hours. Numbness, paresthesias, or“shock-like” sensations in the extremities are suggestive of SCIWORA, and should be expeditiouslyevaluated for evidence of spinal cord injury. MRI is indicated to differentiate cord edema from hemorrhageas well as to assess ligamentous injury.52,53
Transient quadriparesis (referred to as “Stinger”) is seen relatively frequently in children, most often in youngboys after sports injuries. Clinically, there are paresthesias or weakness of the extremities, lasting from secondsto minutes, with complete recovery within 48 hours. No radiologic abnormalities are found. However,radiologic evidence of congenital spinal stenosis, acquired stenosis, cervical instability, or congenitalabnormalities such as Klippel-Feil syndrome are found with some degree of frequency. The etiology is thoughtto be concussion of the spinal cord.53,54
“Shaken-baby syndrome” or child abuse should be suspected when there is a discrepancy between thehistory and degree of physical injury, a delay in seeking treatment, history of repeated injuries, or wheninformants appear inconsistent with their report of injury. Spinal injuries typically associated with“shaken-baby syndrome” include flexion-extension type injuries, particularly at the cervicothoracic orthoracolumbar junction. Compression fractures may also be seen. Skull fractures with intracranial hemorrhage,rib and long bone fractures, blunt abdominal trauma, and retinal hemorrhages are all associated with child

13/10/15 9:24
Página 35 de 41about:blank
abuse.55,56 The presence of such injuries should prompt a thorough search for additional spinal injuries.
Acquired torticollis, spasm of the sternocleidomastoid muscle or “wry neck,” occurs far more frequently thancervical spine injuries. It should be treated conservatively with mild analgesics; low-dose benzodiazepines canbe given. The contracted sternocleidomastoid muscle is on the side opposite the direction of head rotation.
Congenital Anomalies
There is increased risk of cervical spine injury associated with various congenital anomalies. These includeaplasia or hypoplasia of the odontoid and “os odontoideum,” block vertebrae, Klippel-Feil syndrome, Downsyndrome, skeletal dysplasias (e.g., Morquio syndrome and diastrophic dwarfism), and juvenile chronicarthritis. “Os odontoideum” refers to an oval or round ossicle with a smooth cortical border located in theposition of the odontoid process. It is thought to arise from the nonunion of an unrecognized odontoid fracture.Atlantoaxial instability is reported to occur in 10% to 20% of children with Down syndrome but issymptomatic in only about 3%.
Imaging Studies
Patients at risk for spinal injury, who cannot have their cervical spines “cleared” clinically, requireradiographic evaluation. Plain radiographs of the cervical spine are often the initial imaging modality. A lateralcervical spine radiograph visualizing all seven cervical vertebrae from the occiput to the cervicothoracicjunction and an anterior view should be obtained initially. If possible, an open-mouth odontoid view shouldalso be obtained, but in small children, this may be technically difficult.
In multiple trauma patients or patients with abnormal or inadequate plain films, a CT scan should beperformed. CT is particularly useful to visualize those portions of the cervical spine that are commonlymissed and frequently injured in children, such as the occipitoatlantal and cervicothoracic junctions.Limited CT can be used in conjunction with plain radiographs to reduce radiation exposure. CT may detectinjuries not readily apparent on plain radiographs. Thin cut sections (2 to 3 mm) with sagittal and coronalthree-dimensional reconstruction are recommended and should be tailored to the plain radiographic findings.CT provides detailed anatomic information and allows assessment of impingement of the thecal sac and spinalcord from extradural sources such as retropulsed bony fragments or hematoma.
Because children are more likely than adults to suffer ligamentous injury, CT scanning in children <8 years ofage may have limited utility.47,51 MRI best assesses spinal cord, disk, and ligamentous disruption. MRIcan also detect soft tissue injury and hematoma not visualized by other imaging modalities. Thecondition of the spinal cord on MRI is predictive of neurologic outcome. Spinal cord transection and majorhemorrhage are associated with poor outcome and significant neurologic sequelae. Minor hemorrhage oredema is associated with moderate-to-good recovery. The absence of an abnormal signal is associated with fullrecovery.
Choice of imaging modalities should be individualized for each patient. One should carefully consider whichdiagnostic studies are needed to adequately evaluate all injuries that may be present. At the same time,attempts should be made to avoid unnecessary studies that may predispose the patient to long-term, deleteriouseffects associated with excessive radiation.
Pediatric Normal Variants

13/10/15 9:24
Página 36 de 41about:blank
A number of normal variants may be present in pediatric cervical spine films that can make interpretationespecially difficult. Variations in alignment may appear as vertebral displacements, variations in curvature mayresemble muscle spasm or ligamentous injury, and the appearance of growth centers may be confused withfractures (Table 255-11).
Table 255-11 Normal Variants of the Pediatric Cervical SpineAbsence of normal cervical lordosis in 14% of normal children.“Pseudospread” of the atlas on the axis up to age 7 y old.Anterior wedging of the vertebral bodies of up to 3 mm.Over-riding of the anterior arch of C1 above the odontoid in up to 20% of children.Lack of uniform angulation of the interspaces with flexion.Pseudosubluxation:The anterior and posterior spinal lines, joining the anterior and posterior borders of the cervical spine,respectively, are useful in children >7 y of age. Pseudosubluxation of C2 on C3 or C3 on C4 is a normalvariant that can cause disruption of these lines. The spinous processes should form a straight line on anteriorview; any offset suggests unilateral facet dislocation.Persistence of synchondrosis at the base of the odontoid, the apical odontoid epiphysis, and incompleteossification of the posterior arch of C1 and secondary ossification centers of the spinous processes mayresemble bony fractures in children.
Consultation
Emergency physicians should work closely with trauma surgeons to expedite the evaluation and treatment ofany child with spinal trauma. Neurosurgical/orthopedic consultation should be obtained promptly for any childwith an obvious neurologic deficit, altered mental status, or documented radiographic evidence of vertebralfracture, dislocation, spinal cord damage, or associated bone injuries.
Disposition and Follow-Up
Children with documented spinal injury, neurologic deficits, or history of a high-risk mechanism of injuryshould be admitted to a pediatric intensive care unit. If specialty expertise is unavailable, patients withsignificant injuries should be stabilized and transferred to a regional trauma center.
Injury Prevention
Improper positioning of seat restraints and location of children within motor vehicles can result in significantinjury.57 All child restraint seat manufacturers provide information about the proper installation and use of thisequipment, and many local police departments can assist in their proper installation. Parents should beinstructed to maintain safety in their own home environment. Childproof gates on stairways, door locks, andwindow guards should be installed. Helmets and appropriate padding should be used for all sports-relatedrecreational activities.
Athletic coaches should understand the need for protective equipment appropriate for the child’s physicalhabitus as well as the degree of physical contact between participants. There is significant variability in heightsand weights between similarly aged children, and this can lead to a substantial mismatch between participants
13/10/15 9:24
Página 37 de 41about:blank
in a given athletic activity. Trained personnel with knowledge of proper spinal immobilization techniquesshould be on site at sporting events involving physical contact.
References1. National Spinal Cord Injury Statistical Center, Spinal Cord Injury: Facts & Figures at a Glance 2009.Available at:https://www.nscisc.uab.edu/public_content/pdf/Facts%20and%20Figures%20at%20a%20Glance%202010.pdf.Accessed December 7, 2009. 2. Denis F: The three column spine and its significance in the classification of acute thoracolumbar spinalinjuries. Spine 8: 817, 1983. [PubMed: 6670016] 3. Harris J: Spine, including soft tissues of the pharynx and neck, in Harris J, Harris W (eds): The Radiology ofEmergency Medicine, 4th ed. Philadelphia, Lippincott Williams & Wilkins, 2000, p. 137. 4. Stauffer ES, MacMillan M: Fractures and dislocations of the cervical spine, in Rockwood CA, Green DP(eds): Rockwood and Green’s Fractures in Adults, 5th ed. Philadelphia, Lippincott Williams & Wilkins, 2000. 5. Denis F, Davis S, Comfort T: Sacral fractures: an important problem. Retrospective analysis of 236 cases.Clin Orthop 227: 67, 1988. [PubMed: 3338224] 6. Tall RL, De Vault W: Spinal injury in sport: epidemiologic considerations. Clin Sports Med 12: 441, 1993. [PubMed: 8364984] 7. Kihtir T, Ivatury RR, Simon R, Stahl WM: Management of transperitoneal gunshot wounds of the spine. JTrauma 31: 1579, 1991. [PubMed: 1749025] 8. Gilson GJ, Miller AC, Clevenger FW, Curet LB: Acute spinal cord injury and neurogenic shock inpregnancy. Obstet Gynecol Surv 50: 556, 1995. [PubMed: 7566833] 9. Zipnick RI, Scalea TM, Trooskin SZ, et al: Hemodynamic responses to penetrating spinal cord injuries. JTrauma 35: 578, 1993. [PubMed: 8411282] 10. Soderstrom CA, McArdle DQ, Ducker TB, Militello PR: The diagnosis of intraabdominal injury inpatients with cervical cord trauma. J Trauma 23: 1061, 1983. [PubMed: 6655752] 11. [No authors listed]: Blood pressure management after acute spinal cord injury. Neurosurgery 50: 558,2002. 12. Amar AP, Levy ML: Pathogenesis and pharmacological strategies for mitigating secondary damage inacute spinal cord injury. Neurosurgery 44: 1027, 1999. [PubMed: 10232536] 13. Wilson RH, Whiteside MC, Moorehead RJ: Problems in diagnosis and management of hypovolaemia inspinal injury. Br J Clin Pract 47: 224, 1993. [PubMed: 8260349] 14. Ball PA: Critical care of spinal cord injury. Spine 26: S27, 2002. 15. Atkinson PP, Atkinson JLD: Spinal shock. Mayo Clin Proc 71: 384, 1996. [PubMed: 8637263] 16. Woodring JH, Lee C, Jenkins K: Spinal fractures in blunt chest trauma. J Trauma 28: 789, 1988. [PubMed: 3385822] 17. Bayless P, Ray VG: Incidence of cervical spine injuries in association with blunt head trauma. Am J EmergMed 7: 139, 1989. [PubMed: 2920074] 18. Hoffman JR, Mower WR, Wolfson AB, et al: Validity of a set of clinical criteria to rule out injury to thecervical spine in patients with blunt trauma. N Engl J Med 343: 94, 2000. [PubMed: 10891516] 19. MacDonald RL, Schwartz ML, Mirich D, et al: The Canadian C-spine rule for radiography in alert andstable trauma patients. JAMA 286: 1841, 2001. 20. Stiell IG, Clement CM, McKnight RD, et al: The Canadian C-spine rule versus the NEXUS low-riskcriteria in patients with trauma. N Engl J Med 349: 2510, 2003. [PubMed: 14695411] 21. Yealy DM, Auble TE: Choosing between clinical prediction rules. N Engl J Med 349: 2553, 2003. [PubMed: 14695417]

13/10/15 9:24
Página 38 de 41about:blank
22. Blackmore CC, Emerson SS, Mann FA, Koepsell TD: Determination of fracture risk to optimize use ofcervical spine imaging in trauma patients: a clinical prediction rule. Radiology 211: 759, 1999. 23. Hanson JA, Blackmore CC, Mann FA, Wilson AJ: Cervical spine injury: a clinical decision rule canidentify high risk patients to for helical CT screening. AJR Am J Roentgenol 174: 713, 2000. 24. MacDonald RL, Schwartz ML, Mirich D, et al: Diagnosis of cervical spine injury in motor vehicle crashvictims: How many x-rays are enough? J Trauma 30: 392, 1990. 25. Blackmore CC, Mann FA, Wilson AJ: Helical CT in the primary trauma evaluation of the cervical spine:an evidence-based approach. Skeletal Radiol 29: 632, 2000. [PubMed: 11201032] 26. Brohi K, Healy M, Fotheringham T, et al: Helical computed tomographic scanning for the evaluation of thecervical spine in the unconscious, intubated trauma patient. JTrauma 58: 897, 2005. [PubMed: 15920399] 27. Mathen R, Inaba K, Munera F, et al: Prospective evaluation of multislice computed tomography versusplain radiographic cervical spine clearance in trauma patients. J Trauma 62: 1427, 2007. [PubMed: 17563660]28. Holmes JF, Akkinepalli R: Computed tomography versus plain radiography to screen for cervical spineinjury: a meta-analysis. J Trauma 58: 902, 2005. [PubMed: 15920400] 29. Brown CV, Antevil JL, Sise MJ, et al: Spiral computed tomography for the diagnosis of cervical, thoracic,and lumbar spine fractures: its time has come. J Trauma 58: 890, 2005. [PubMed: 15920398] 30. Daffner RH: Cervical radiography for trauma patients: a time effective technique? AJR Am J Roentgenol175: 1309, 2000. [PubMed: 11044030] 31. Panjabi MM, White AA: Basic biomechanics of the spine. Neurosurgery 7: 76, 1980. 32. Singh R, McD Taylor D, D’Souza D, et al: Injuries significantly associated with thoracic spine fractures: acase-control study. Emerg Med Australas 21: 419, 2009. [PubMed: 19694786] 33. Inaba K, Munera F, McKenney M, et al: Visceral torso computed tomography for clearance of thethoracolumbar spine in trauma: a review of the literature. J Trauma 60: 915, 2006. [PubMed: 16612322] 34. Howes MC, Pearce AP: State of play: clearing the thoracolumbar spine in blunt trauma victims. EmergMed Australas 18: 471, 2006. [PubMed: 17083636] 35. Holmes JF, Mirvis SE, Panacek EA, et al: Variability in computed tomography and magnetic resonanceimaging in patients with cervical spine injuries. J Trauma 53: 524, 2002. [PubMed: 12352491] 36. Horn EM, Lekovic GP, Feiz-Erfan I, et al: Cervical magnetic resonance imaging abnormalities notpredictive of cervical spine instability in traumatically injured patients. J Neurosurg Spine 1: 39, 2004. [PubMed: 15291018] 37. Bracken MB, Shepard MJ, Collins WF, et al: A randomized, controlled trial of methylprednisolone ornaloxone in the treatment of acute spinal cord injury: Results of the second national acute spinal cord injurystudy. N Engl J Med 322: 1405, 1990. [PubMed: 2278545] 38. Prendergast MR, Saxe JM, Ledgerwood AM, et al: Massive steroids do not reduce the zone of injury afterpenetrating spinal cord injury. J Trauma 37: 576, 1994. 39. Nesathurai S: Steroids and spinal cord injury: revisiting the NASCIS 2 and NASCIS 3 trials. J Trauma 45:1088, 1998. [PubMed: 9867054] 40. Short DJ, El Masry WS, Jones PW: High-dose methylprednisolone in the management of acute spinal cordinjury - a systematic review from a clinical perspective. Spinal Cord 38: 273, 2000. [PubMed: 10822400] 41. Hadley MN, Walters BC, Grabb PA, et al: Guidelines for the management of acute cervical spine andspinal cord injuries. Clin Neurosurg 49: 407, 2002. [PubMed: 12506565] 42. Waters RL, Adkins RH: The effects of removal of bullet fragments retained in the spinal canal. Acollaborative study by the National Spinal Cord Injury Model Systems. Spine 16: 934, 1991. [PubMed:1948380] 43. d’Amato C: Pediatric spinal trauma: injuries in very young children. Clin Orthop Relat Res 432: 34, 2005. [PubMed: 15738801] 44. Brown RL, Brunn MA, Garcia VF: Cervical spine injuries in children: a review of 103 patients treatedconsecutively at a level 1 pediatric trauma center. J Pediatr Surg 36: 1107, 2001. [PubMed: 11479837]
13/10/15 9:24
Página 39 de 41about:blank
45. Viccellio P, Simon H, Pressman BD, et al: A prospective multicenter study of cervical spine injury inchildren. Pediatrics 108: E20, 2001. 46. Sharma OP, Oswanski MF, Yazdi JS, et al: Assessment for additional spinal trauma in patients withcervical spine injury. Am Surg 73: 70, 2007. 47. Macciocchi S, Seel RT, Thompson N, et al: Spinal cord injury and co-occurring traumatic brain injury:assessment and incidence. Arch Phys Med Rehabil 89: 1350, 2008. 48. Dormans JP: Evaluation of children with suspected cervical spine injury. J Bone Joint SurgAm 84: 124,2002. [PubMed: 11792790] 49. Roche C, Carty H: Spinal trauma in children. Pediatr Radiol 31: 677, 2001. [PubMed: 11685436] 50. Santiago R, Guenther E, Carroll K, Junkins EP: The clinical presentation of pediatric thoracolumbarfractures. J Trauma 60: 187, 2006. [PubMed: 16456454] 51. Dickman CA, Zabramski JM, Hadley MN, et al: Pediatric spinal cord injury without radiographicabnormalities: report of 26 cases and review of the literature. J Spinal Disord 4: 295, 1991. 52. Sledge JB, Allred D, Hyman J: MRI in evaluating injuries to the pediatric thoracolumbar spine. J PediatrOrthop 21: 288, 2001. [PubMed: 11371807] 53. Perks DH: Transient spinal cord injuries in the young athlete. J Trauma Nurs 12: 127, 2005. [PubMed:16602338] 54. Vaccaro AR, Klein GR, Ciccoti M et al: Return to play for the athlete with cervical spine injuries resultingin stinger and transient quadriplegia/paresis. Spine J 2: 351, 2002. [PubMed: 14589466] 55. Wirtz SJ, Trent RB: Passive surveillance of shaken baby syndrome using hospital inpatient data. Am J PrevMed 34: 134, 2008. 56. Trenchs V, Curcoy AI, Navarro R, Pou J: Subdural hematomas and physical abuse in the first two years oflife. Pediatr Neurosurg 43: 352, 2007. [PubMed: 17785998] 57. Achildi O, Betz RR, Grewal H: Lapbelt injuries and the seatbelt syndrome in pediatric spinal cord injury. JSpinal Cord Med 30: 521, 2007.
Useful Web Resources
Eastern Association for the Surgery of Trauma—http://www.east.orgNational Spinal Cord Injury Association—http://www.spinalcord.orgNational Institute of Neurological Disorders and Stroke—http://www.ninds.nih.gov/disorders/sci/sci.htmNational Spinal Cord Injury Statistical Center—https://www.nscisc.uab.edu
McGraw Hill
Copyright © McGraw-Hill Global Education Holdings, LLC.All rights reserved.Your IP address is 207.249.33.173
Silverchair
Vertebral anatomy. Each vertebra consists of a vertebral body and posterior element. Vertebrae are stabilizedby an anterior longitudinal ligament, posterior ligament, and interspinous ligament.
Jefferson fracture.
Jefferson fracture CT and radiographs show a Jefferson burst fracture in a 46-year-old man, who sustained

13/10/15 9:24
Página 40 de 41about:blank
injuries while body surfing. A. Axial CT images viewed on bone windows show bilateral fractures of both theanterior and posterior arches of C1. B. Lateral radiograph of the cervical spine shows the fracture of theposterior arch of C1, with slight distraction of the posterior fracture fragment. C. Open-mouth view showsslight asymmetry of the dens in relation to the lateral masses of C1, with slight widening of the intervalbetween C1 and the dens. The right lateral mass of C1 is slightly subluxed laterally at the right atlantoaxialjoint.
Avulsion fracture of the anterior arch of the atlas.
Classification of odontoid fractures.
Type II odontoid fracture. CT scans demonstrate a type II odontoid fracture with posterior ligament complexinjury in a 34-year-old woman involved in a motor vehicle crash. A. Axial CT shows oblique fracture of thedens. B. CT sagittal reformatted image shows the dens fracture with slight anterior angulation.
Hangman’s fracture.
Bilateral interfacetal dislocation injuries incurred by a 32-year-old man following a head-on collision whileplaying football. A. Lateral radiograph and CT with (B) axial, (C) sagittal, and (D) three-dimensionalreconstruction, show a C3-C4 subluxation with bilateral locked facet joints.
Burst fracture. A. CT and (B) MRI demonstrate a C7 burst fracture with cord compression in a 19-year-oldman involved in a motorcycle crash.
Wedge compression fracture. Wedge compression fractures are often caused by axial unloading with failure ofthe anterior column. A. Schematic of a compression fracture. B. Lateral reconstruction CT scan demonstratesthe anterior wedging. C. Axial CT scan demonstrates the anterior wedging and vertebral body fracture. Notethe lack of retropulsion of elements into the spinal canal.
Burst fracture. Burst fractures are also caused by axial loading. Both anterior and middle columns have failed.A. Schematic of the forces transmitted. B. Lateral reconstruction CT scan demonstrates failure of both theanterior and middle columns. C. Axial CT scan demonstrates the burst vertebral body. Note the retropulsion ofelements into the spinal canal.
Flexion-distraction injuries. Flexion-distraction injuries involve rotation of forces. This results in failure ofboth the posterior and middle columns. A. Schematic of the forces transmitted. B. Lateral view of plain filmdemonstrating a flexion distraction injury. C. Lateral CT reconstruction confirming the pattern, alsodemonstrating posterior opening of the disk space. D. Axial CT scan shows loss of the middle column withfracture through the lateral elements.
Fracture-dislocation injuries. Fracture dislocations are the most damaging of injuries leading to failure of allthree columns. A. Schematic demonstration of these injuries. B. Lateral CT reconstruction demonstrates lossof all three columns. C. Axial CT scan demonstrates the dislocation and displacement of the vertebral body.
Fracture-dislocation injury CT with (A) axial, (B) sagittal, and (C) three-dimensional reconstructions shows aT10-T11 fracture-dislocation in a 37-year-old man who sustained a 20-ft fall.
Spinal cord level. The spinal cord level of injury can be delineated by physical examination, including adetailed neurologic examination.

13/10/15 9:24
Página 41 de 41about:blank
Dermatomes for sensory examination.
Lateral cervical spine alignment. Vertebral alignment of the lateral cervical spine: (1) anterior vertebral bodyline, (2) posterior vertebral body line, (3) spinolaminar line, and (4) spinous processes line.
Algorithm for gunshot injury to spine. *Consider bullet removal in thoracolumbar region.