specific learning objectives at the end of this lecture a student will be able to – 1.describe the...
TRANSCRIPT

Lipid Transport and Storage
Dr.S.Chakravarty ,MD

Specific Learning Objectives • At the end of this lecture a student will be able to –
1. Describe the composition of various lipoproteins and list the key Apo proteins
2. Describe the various pathways of lipoprotein metabolism in detail
3. List the enzymes and receptors involved in lipoprotein metabolism and their deficiency states
4. Classify Lipoproteinemias and describe the clinical features of various lipoproteinemias
5. Describe the pathogenesis of atherosclerosis
6. List the drugs used to treat hyperlipoproteinemias and its mechanism of action

What are lipoproteins?
• Transport of lipids from various tissues for storage and utilization – water soluble.
• Lipoproteins - large mostly spherical complexes
• Hydrophobic core – TGs and cholesterol esters
• Hydrophilic surface – phospholipids, unesterified Cholesterol and Apoproteins.

Structure of Lipoprotein
Harper 28th

Apolipoproteins1) Provide structure to lipoproteins
2) Enzyme co-factors – – C2 for lipoprotein lipase– A1 for Lecithin cholesterol acyl transferase
3) Ligands for receptors – – Apo B100 and APO E – LDL receptor– Apo A1 – Srb1 and ABCA 1 receptor
4) Enzyme inhibitors: – C1 – cholesterol ester transfer protein.

SEPARATION OF LIPOPROTEINS
CHYLOMICRON
VLDL
HDL
LDL
IDL
FFA
CHYLOMICRON
VLDL
HDL
LDL
IDL
FFA-Alb
-ve
+ve
Electrophoresis
DENSITY

Separation based on ultracentrifugation /density:

Key Apoproteins to identify various lipoproteins
• APO A1 – HDL• APO B48 – Chylomicrons• APO -B100 – VLDL, IDL, LDL• APO C and E – present in all particles(with
exceptions ) predominantly donated by HDL to other molecules

Types of lipoproteins:Chylomicrons :
– derived from intestinal absorption of TGs and other lipids
– Exogenous triglycerides – Highest triglyceride content – Major APO protein – APO-B48
VLDL :– Derived from liver and helps in transport of TGs to
peripheral tissues.– Endogenous triglycerides– Major APO protein – APO-B100

LDL :– Derived from catabolism of VLDL– APO proteins same as VLDL– Highest cholesterol content– Formation of modified / oxidized LDL - Atherosclerosis
HDL:– Reverse cholesterol transport– Extracts cholesterol from the tissues and brings it to liver– Provides Apoproteins to VLDL and Chylomicrons for maturation– Major APO protein – APO A-1

CHOLESTEROL DIGESTION
• CHOLESTEROL CHOLESTEROL ESTER
NON –POLAR POLAR

Cholesterol
+ Cholesterol esters
Bile, Pancreatic esterase
Cholesterol + FA
CE+TG+PL
Reesterification by ACAT(acyl cholesterol acyl transferase)
G I tract
lntestinal cells
CE + TG + PL +
APO B 48
Chylomicrion
Lymph & Thoracic duct
Hydrolysis , emulsification & absorption
CHOLESTEROL DIGESTION

Cholesterol absorption
Glucose
Kaplan USMLE step 1

Structure of Lipoprotein
Harper

Chylomicrons
TG, CE
TG, CE
TG, CE
+
Harper

VLDL,IDL AND LDL
TG, C
TG, C
TG, C
TG,C
+
Harper

CHYLOMICRONS AND VLDL
SIMILARITIES DIFFERENCES
Apo B , C & E Apo B 48 VS Apo B 100
Huge CARRIES – CE in Chylomicrons VS mainly C in VLDL
Both carry TG SYNTHESIS - Intestine vs Liver
Lymph vs Blood

LPL – lipoprotein lipase • Activated by Insulin
• Requires cofactor apo C-II protein
• Present in endothelium of capillaries – mainly in heart, adipose tissue and skeletal muscle
• LPL of heart has low Km compared to adipose tissue.
• Heparin LPL is released from tissues Clears Lipemia


INSULIN
+
POLAR +
Kaplan USMLE step 1 Lecture Notes
Summary of Chylomicrons and VLDL

Cell
mem
bran
e
LDL
HDL
CE
TG, C
Apo A LCAT = esterification of cholesterol to CE
Once esterified Cholesterol is trapped inside as it becomes Non-Polar
cc
C
c = OH group of cholesterol Apo A
LCAT

Fate of Cholesterol
Kaplan USMLE step 1 Lecture Notes
LDL receptor defectType II a Hypercholesterolemia or Familial Hypercholesterolemia
No cholesterol can come insideMore endogenous synthesis !!
Loss of receptors

HDL

Ox-LDL (B-100 donates an electron )Scavenger Receptor
SR -A NOT DOWNREGULATED
BY CHOLESTEROL
FREE RADICALS
LDL
HDL , LDL AND ATHEROGENESIS Kaplan USMLE step 1 Lecture Notes
SR –B1
Smooth Muscle Proliferation
-ve Vitamin E( role in preventingatherosclerosis DOUBTFUL)
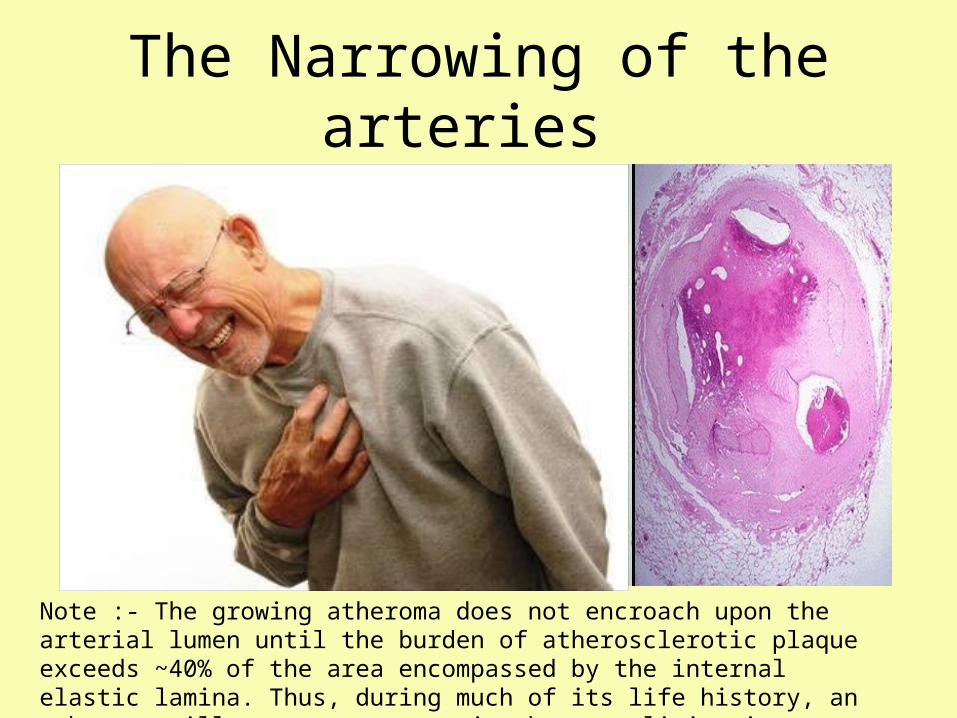
The Narrowing of the arteries
Note :- The growing atheroma does not encroach upon the arterial lumen until the burden of atherosclerotic plaque exceeds ~40% of the area encompassed by the internal elastic lamina. Thus, during much of its life history, an atheroma will not cause stenosis that can limit tissue perfusion.

Hypolipoproteinemias • Abetalipoproteinemia :- No chylomicrons , VLDL, LDL
– Rare ; blood acyl glycerols low; intestine and liver accumulate acylglycerols ;Intestinal malabsorption .
– Fat malabsorption, spinocerebellar ataxia, pigmented retinopathy– Early death avoidable by administration of large doses of fat-soluble
vitamin E.
• Familial alpha –lipoprotein deficiency – Tangier’s disease(ABCA1 transporter deficiency)– Fish-eye disease (partial LCAT deficiency)– Apo A-I deficiency
• LOW or NEAR Absence of HDL Tendency toward hypertriacylglycerolemia as a result of absence of apo C-II.Low LDL

Fredrickson classification of hyperlipoproteinemiasHyperlipo-proteinemia Synonyms Defect Increased
lipoprotein Main symptoms TreatmentSerum appearance
Estimated prevalence
Type I
a Buerger-Gruetz syndrome, or Familial hyperchylomicronemia
Decreased lipoprotein lipase (LPL) Chylomic
rons
(= Increased
TG)
Abdominal pain (from pancreatitis), lipemia retinalis, eruptive skin xanthomas, hepatosplenomegaly
Diet control Creamy top layer 1 in 1,000,000
b
Familial apoprotein CII deficiency
Altered ApoC2
Type IIa Familial hypercholesterolemia LDL receptor
deficiencyLDL Xanthelasma, arcus
senilis, tendon xanthomas
Bile acid sequestrants, statins, niacin
Clear 1 in 500 for heterozygotes
b Familial combined hyperlipidemia
Decreased LDL receptor and increased ApoB
LDL and VLDL
Statins, niacin, fibrate Clear 1 in 100
Type III Familial dysbetalipoproteinemia
Defect in Apo E 2 synthesis IDL
Tubo-Eruptive Xanthomas & Palmar Xanthomas
Fibrate, statins Turbid 1 in 10,000
Type IV Familial hypertriglyceridemiaIncreased VLDL production and Decreased elimination
VLDLCan cause pancreatitis at high triglyceride levels
Fibrate, niacin, statins Turbid 1 in 100
Type VIncreased VLDL production and Decreased LPL
VLDL and Chylomicrons
Niacin, fibrateCreamy top layer & turbid bottom

Type
DEFICIENCY iNHERITANCE LIPID elevated in Blood
Lipoprotein elevated in Blood
Comments
I Familial lipoprotein lipase (rare )Apo C-II (rare )
Autosomal recessive
TG CHYLOMICRONS (after a high carb diet )
VLDL
Red orange eruptive xanthomasFatty liverAcute pancreatitis Abdominal pain after fatty meal
IIa LDL receptor defect! AUTOSOMAL DOMINANT
CHOLSETSROL LDL High risk of atherosclerosis and CADHomozygous condition , death usually by <20 yearsXanthomas of the Achilles tendonTuberous Xanthomas on elbowsXanthelasmasCorneal Arcus
USMLE FAVOURITES!!

Tuberous Xanthomas
Corneal Arcus Xanthelasma


Lp(a) excess
Normally Plasminogen activated to Plasmin Plasmin binds Fibrin Fibrin is lysed.
• Lp(a) has Structural homology with Plasminogen
• Lp(a) excess Binds to fibrin Inactivates Plasminogen activation Fibrin is not lysed
• Normal levels <15mg/dl• >30mg/dl = increased risk of Coronary artery disease

Acquired Lipoproteinemias
• Diabetes Mellitus • Nephrotic Syndrome• Hypothyroidism• Obstructive Jaundice• Metabolic syndrome

Metabolic Syndrome
ANY THREE OUT OF :-
Drugs used in Hyperlipoproteinemia• Statins - HMG-CoA reductase inhibitors
• Bile acid sequestrants- Basic ion exchange resin
• Fibrates – (+) Lipoprotein lipase • Nicotinic acid (-) TGs in liver and (+) LPL

Drugs
• Orlistat – (-) pancreatic lipase• Ezetimibe – (-) cholesterol and bile salt from
gut.

• A lipoprotein synthesized in liver , containing high concentration of TG and mainly cleared from circulation by adipose tissue and muscle ?
A. CHYLOMICRONSB. HDLC. IDLD. LDLE. VLDL

• Which of the following lipoproteins increase in Familial hypercholesterolemia Type 1 .
A. Chylomicrons B. LDLC. VLDLD. Total cholesterolE. IDL

Thank you