sle round
TRANSCRIPT

Prof.Dr. Prof.Dr. Mirvat El-ToukhyMirvat El-Toukhy

Definition and Epidemiology:
Systemic Lupus Erythematosus is a multi system connective tissue disease characterized by wide spread organ involvement and numerous auto-antibodies.
The disease onset occur between 25-45 years.
SLE occurs more frequently in women with a female to male ratio of 9 – 1.
Women are more prone to SLE during the child bearing period.


Etiology: SLE is an autoimmune disease of un known
etiology & of multifactorial theories, it is due to the interaction of:
1- Genetic factors: The susceptibility of SLE depends on multiple genes that increase the relative risk for disease as HLA-DR2 & DR3.
2- Environmental factors:
- Exposure to UV B light.
- Sex hormones.
- Dietary factors: High caloric diet, high intake of unsaturated fat.
- Infectious agents: Retrovirus & bacterial lipo- polysaccharides.
- Drugs: Hydralazine, Procainamide, Isoniazid, Depenicillamine, Interfron-alfa and antiepileptic.

3- Immune abnormalities:
- Defective supressor T lymphocyte. - Increased CD4 T helper cells. - B lymphocyte activation. - Over production of auto-antibodies and immune
complex. - Defect in apoptosis.
* The over production of auto-antibodies contribute to: A. Direct damage: Antibody mediated
thrombocytopenia, lymphopenia and hemolytic anaemia by anti-platelets, anti-lymphocyte and anti-RBCS.
B. Indirect damage: by antigen-antibody complex (DNA- anti DNA antibody complex) as in lupus nephritis.


1- Activation of self-reactive B cells — the source of autoantibodies — as they encounter with self-antigen in the presence of T-cell help.
2- Activated B cells then undergo somatic hypermutation and clonal selection — forming both effector and memory B cells. Effector B cells release IgG autoantibodies into the circulation, where they form immune complexes in the presence of antigens. 3- Excess immune complexes accumulate in the small vessels of organs where they become pathogenic causing local activation of the complement system and/or binding of Fc receptors, which leads to the degranulation of mast cells and the infiltration of neutrophils and macrophages thus inducing inflammation.
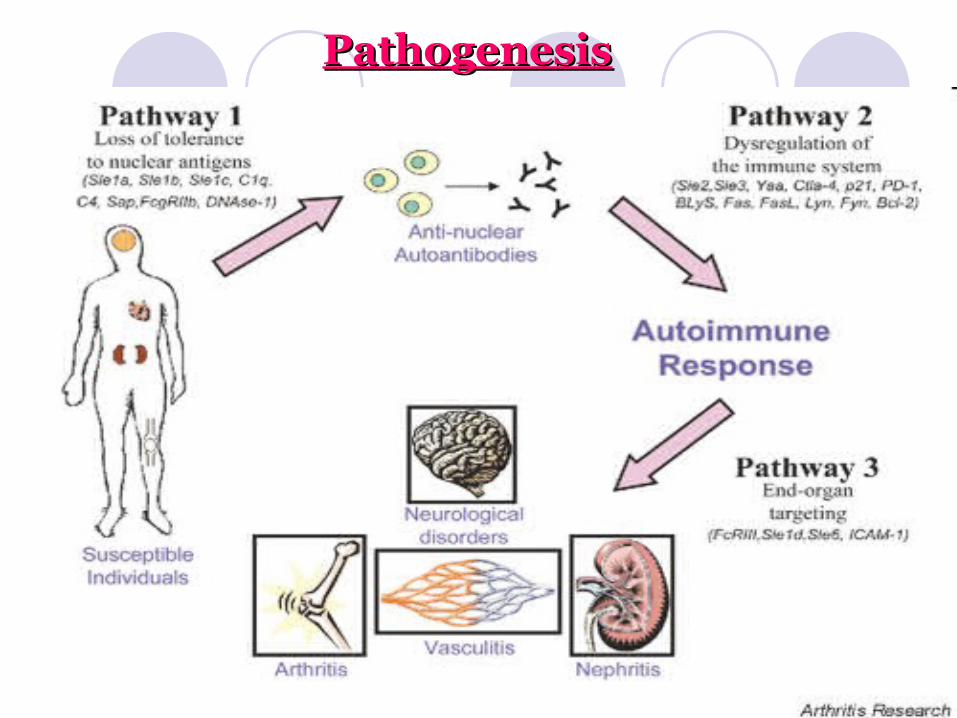
PathogenesisPathogenesis

Clinical features: I. General: 1- Low grade fever, if high….. 2- generalized fatigue. 3- Weight loss. II. Musculoskeletal manifestation: 1- Arthralgia ( > 90 %), symetric nonerosive arthritis
of PIP, MCPs, Wrists and Knees. 2- Myalgia, myositis is uncommon. 3- Osteoporosis is frequent due to prolonged steroid
therapy. 4- Avascular necrosis of the hip occurs in 5-10% of
patients under steroid therapy. 5- Chronic inflammatory arthritis and tenosynovitis
leads to non erosive deformities ( Jaccouds arthropathy).

III. Skin manifestation: Associated in 80% of cases
1- Malar rash (butter fly) over the cheek and nasal bridge: Occur in 70 % of cases, causing fixed flat or raised erythema exacerbated by UV rays.
2- Discoid rash: Erythematous raised patches with follicular plugging, adherent keratotic scaling and atrophic scaring.
3- Patchy alopecia: In > 50% of cases, can be permanent. 4- Oral or nasopharyngeal ulcer: Usually painless. 5- Raynauds phenomenon: In 20 % of cases, may precede
other manifestations. 6- Photosensitivity: Skin rash that resulted from unusual
reaction to sun light. 7- Telangectasia, livido reticularis and palmer & planer
rashes.



IV. Cardiovascular manifestation:
Occur in 30-50% of cases. 1- Pericarditis that may be associated with
pericardial effusion. 2- Myocarditis causing arrythmia and
heart failure. 3- Myocardial infarction , occur with
vasculitis or coronary emboli. 4- Libman-sacks endocarditis (sterile
endocarditis).

V. Pulmonary manifestation: Involved in 2/3 of cases.
1- Recurrent dry pleurisy and pleural effusions.
2- Lupus pneumonitis, pulmonary fibrosis and hypertension.
3- Restrictive lung defect with progressive dyspnea( shrinking lung syndrome).

VI. Renal manifestation:
Occur in 50% of patients, often Occur in 50% of patients, often asymptomatic and may result in:asymptomatic and may result in: 1- 1- ProteinuriaProteinuria is the most common is the most common findings and may produce nephrotic findings and may produce nephrotic syndrome.syndrome. 2- 2- HematuriaHematuria, usually microscopic., usually microscopic. 3- 3- HypertensionHypertension in about 20% of in about 20% of patients.patients. 4- Acute or chronic 4- Acute or chronic renal failurerenal failure..

VII. Ophthalmic manifestation:
1- Conjunctivitis & optic neuritis.
2- Retinal vasculitis: cytoid bodies appear as hard exudates.
3- 2ry Sjogren syndrome.

VIII. Gastrointestinal manifestation: 1- Abdominal pain: due to perisplenitis or mesenteric
vasculitis. 2- GIT ulceration but rare.
IX. Central nervous system manifestation: Occur in up to 30 % of patients. 1- Diffuse manifestations: ( Antineuronal Ab. &
Antiribosomal P protein Ab. Found in serum). * Organic brain syndrome: (cognetive dysfunction,
dementia, altered consciousness). * Psychosis, Depression and aseptic meningitis. 2- Focal manifestations: ( with Antiphospholipid Ab.) * Stroke, transverse myelitis and movement
disorders ( chorea).
3- Seizures: Generalized or focal. 4- Lupus headache. 5-Neuropathies: Peripheral n., Cranial n.,
mononeuritis multiplex and Guillian-Barre syndrome.
X. Blood disorders: Due to antibodies mediated destruction of peripheral
blood cells. 1- Hemolytic anemia in 10% of patients. 2- Thrombocytopenia and purpura. 3- Leucopenia and lymphopenia. 4- Splenomegaly and lymphadenopathy. 5- Circulating anticoagulants: Lupus anticoagulant
presenting with thrombosis, abortion and purpura (Antiphospholipid syndrome).

Diagnosis:# The commonest clinical presentation in SLE patients
are arthralgia, malaise, fever, wieght loss and skin rash.
# The diagnosis of SLE should be suspected in any female below 40 years of age having non erosive arthritis associated with un explained multisystem involvement.
Systemic Lupus International Collaboration Clinic (SLICC) Revision of American Collage of Rheumatology ( ACR) classification criteria for SLE classify the patient as having SLE if:
I. The patient has biopsy-proven lupus nephritis with ANA or anti-dsDNA. or
II. The patient satisfied four of the criteria, including at least one clinical and one immunologic criterion.

Clinical Criteria: 1- Acute or subacute cutaneous lupus. 2- Chronic cutaneous lupus. 3- Oral/ nasal ulcers. 4- Non scaring alopecia. 5- Inflammatory synovitis with physician-observed
swelling of two or more joints or tender joints with morning stiffness.
6- Serositis. 7- Renal: 24 hr. urine protein representing at least 500
mg or red blood cell casts. 8- Neurologic: Seizure, Psychosis, mononeuritis
multiplex, myelitis, peripheral or cranial neuropathy, cerebritis( acute confusional state).
9- Hemolytic anemia. 10- Leucopenia ( < 4000/mm3) at least once. Or Lymphopenia ( < 1000/mm3) at least once. 11-Thrombocytopenia ( < 100,000/mm3) at least once.

Immunologic Criteria:
1- ANA above laboratory reference range. 2- Anti-dsDNA above laboratory range ( except ELISA:
twice above laboratory reference range). 3- Anti-Sm ab. 4- Antiphospholipid antibody: - Lupus anticoagulant. - False-positive test for syphilis. - Anticardiolipin- at least twice normal or
medium-high titre. - Anti-ß 2 glycoprotein 1. 5- Low complement -Low C3 -Low C4 -Low CH50 6- Direct Coombs test in absence of hemolytic anemia.

SLE has to be differentiated from drug induced lupus by:
1- History of drug intake; isoniazide. 2- Present with arthralgia, skin rash, serositis. 3- Positive ANA (Ab. Against histone of the nucleus). 4- Older age group. 5- Renal involvement. 6- Anti-dsDNA antibodies are negative. 7- Gradual improvement after withdrwal of offending
drug.
SLE has to be differentiated from RA by: 1- General illness is out of proportion to joint lesion. 2- Erosion, deformities and ankylosis rarely occur. 3- Wide spread systemic involvement ( polyserositis).

Laboratory investigation:
I.Blood cytology: 1- Elevated ESR. 2- Normal CRP but increased in infection and
vasculitis. 3- Mild or moderate anemia. 4- Moderate leucopenia ( 2000-3000/mm3). 5- Moderate or sever thrombocytopenia
( platelets< 100,000/ mm3). II. Serum protein: 1- Low serum albumin, with persistant
proteinuria as in nephrotic syndrome. 2- Hypergammaglobulinemia. 3- Serum creatinine & urea.

III. Immunology: 1- Low serum complement Disease activity. v. low C3 & C4 Active lupus nephritis. 2- LE cell. 3- ANA in 95%. 4- +ve RF in 33%. 5- Prolonged prothrombin time predispose
to arterial and venous thrombosis especially in pregnancy fetal loss is common.
6- Antithyroid antibody. 7- Anti clotting factors. 8- Anti Sm antibodies, specific for SLE. 9- Anti-Ro and Anti-La antibodies seen in SLE and
Sjogren syndrome.IV. Urine for:
Proteins, blood and casts for renal disease.

Preventive measure
* Regular evaluation: Assess lupus activity. Routine chemistry, blood count &
urine analysis. Control of blood pressure. Control of hyperlipidemia. * Photoprotection: Avoid intense sun exposure. Sun screens. * Infection control: Suspect infection in all febrile lupus
patients. Antibiotic prophylaxis for dental &
genitourinary procedures. Influenza & pneumococcal
immunisation. * Pregnancy issues: Birth control with v. active lupus &
with cytotoxic drugs. High risk obestetric care is required

Management: A) Mild disease:
- NSAIDS: In patient with musculoskeletal manifestation and mild systemic features.
- Antimalarials, Hydroxychloroquine (200-400mg/ day) used in patients not responding with NSAIDS or with skin lesions & fatigue.
- Low dose corticosteroids ( 5-10 mg/ day) in patients with serositis or mild thrombocytopenia.
B) Moderate& severe disease:
- Corticosteroids: 40-80 mg/day prednisolone orally. Pulse therapy with methylprednisolone ( 1gm iv on 3 successive days).

- Immunosupressive drugs: Used for patients with
severe nephritis & active cerebritis.
1- Azathioprine: 2mg/kg orally daily.
2- Cyclophosphamide: 1-3mg/kg orally daily or 0.5-1gm/m2 body surface area iv monthly for patients with life-threatening dis. ( severe nephritis & severe neuropsychiatric manifestations).
3- Cyclosporine and mycophenolate mofetil: ( in severe nephritis).
4- Plasmapharesis: In patients with serious steroid resistant exacerbations.

Recent therapy: 1- B cell depletion therapy: anti-CD20 monoclonal
antibody rituximab. 2-Autologous haematopoietic stem cell transplant:
Immunoablation followed by autologous haematopoietic stem cell transplant (HSCT) has been explored in patients with severe systemic lupus who are unresponsive to conventional therapies or suffer intolerable side-effects.
3- Biological therapies: anti-tumour necrosis factor-α therapies: TNF-α participates in the immune dysregulation evident in SLE by increasing production of other proinflammatory cytokines such as IL-1, IL-6 and IL-8, and furthermore may be altered by circulating immune complexes.
4- Co-stimulatory molecules:
Inhibition of several different pathways in lupus pathogenesis have been explored. Targeted immunosuppression of CD40 ligand/CD40.
5- IL-1 receptor antagonist (Anakinra).
6- Anti-IL-10 monoclonal antibody: IL-10 induces B cell differentiation.
7- Anti-B lymphocyte stimulator (BLys): is member of TNF protein family; anti-BLys modulates B cell immune responses by reduction of apoptosis & interference with B cell development and differentiation.

SLE & Pregnancy

• Pregnancy is not contraindicated in patients with SLE in remission( at least 6 months) with good renal function.
• Fertility rate is normal, but there is a high spontaneous miscarriage rate (30%) especially if antiphospholipid antibodies are present, venous and arterial thrombosis recurrent fetal loss.
• Prematurity & stillbirth may occur in the first or second trimesters in patients with severe disease.
• The use of intrauterine device is not recommended because of the possibility of fulminant uterine infection.

Prognosis Episodic course is characterized with
exacerbations and complete remission which may last for long time.
The 5 years survival is > 90%.
The worst prognosis is with severe renal & neurological diseases.
Infection is an important cause of morbidity.
Disease flare are common during pregnancy with increased incidence of maternal& fetal complications.
