singapore experience in helping hidden youth with gaming ... · pathological video-gaming among...
TRANSCRIPT

Singapore experience in helping hidden
youth with gaming disorder
Ray Chua
Senior Psychologist
REACH West
National University Hospital, Singapore

Self Introduction
• 30+ years of gaming experience
• 10 years of experience working with gaming
addicts
• Led the counselling and research team at
TOUCH Cyber Wellness
• Leading the Cyber Health and Internet
Programme (CHIP) at REACH West, NUH
• Author of Virtual Realms Real Needs book

Improve mental health of children and
adolescents in schools and at-risk children in the community.
Provide training and support to
School Counsellors , General Practitioners (GP) and Voluntary Welfare Organisations (VWOs) in managing at-risk children and children with mental health conditions
Develop a mental health network for
children and adolescents (including at-risk children) in the community
Introduction to REACH

REACH Network
North - 2007
South - 2009
East - 2010West - 2011
REACHnetwork
REACHnetwork
REACHnetwork
REACHnetwork
GPs
SPEDVWO
GPs
SPEDVWO
GPs
SPEDVWOGPs
SPEDVWO

5
REACH (West) Organization ChartProgram Director
A/Prof John Wong Chee Meng
Team Leader &
Senior Psychologist
Mr Ray Chua
Senior Assistant
Manager
Ms Jia Ning
REACH Doctors
Dr Tian Cheong Sing
Dr Celine Wong
Dr Teng Jia Ying
Child resident
Sr / Psychologists / Psychologist
Associates
Ms Yvonne Heng
Ms Nur Ashikin
Ms Goh Lishan
Ms Nona Ooi
Ms Sarah Lam
Mr Loy Xingqi
Ms Saratri Shanti Widiasri
Sr Occupational Therapist
Ms Stephanie Seow
Medical Social Worker
Ms Grace Ooi
Executive Assistant
Ms Shirley Cassandra Paul

Talk Outline
• Social withdrawal in Singapore
• Case vignette of youth with gaming
disorder and social withdrawal
• Case conceptualization and service
provision for the socially withdrawn
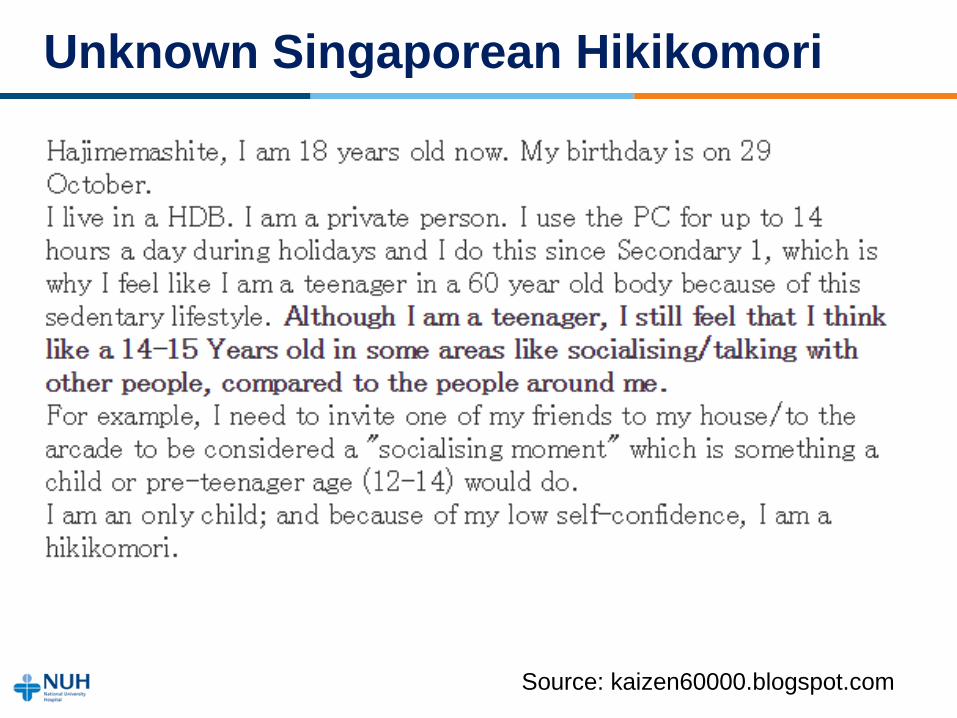
Unknown Singaporean Hikikomori
Source: kaizen60000.blogspot.com

Presentation of social withdrawal in SG
• School refusal
– Legal
• Singapore compulsory education act
– Compulsory primary school education
• Secondary schools have to account to Ministry of
Education for registered students who are not in
education, employment or training (NEET)
– Cultural
• Meritocratic society
• Education as a key driver of social mobility

Presentation of social withdrawal in SG
• Compulsory National Service (NS)
– Legal
• Compulsory for males aged 16.5-40 years under
the Enlistment Act
• NS defaulters are liable for jail term and fine
– Pre-enlistment medical screening
• Declare mental illness/psychiatric condition
• Review by psychiatrist
– Possibility of getting exempted from NS if
there is clinical documentation from
psychiatrist of severe house-boundness due
to psychiatric condition
Presentation of social withdrawal in SG
• Gaming disorder
– Usage location
• Home is the main location for gaming
• Fast broadband internet speeds
– Online purchase and download of games
– Parental concern over excessive time spent
on PC and mobile games

Pathological Video-Gaming among Singaporean Youth
• 2,998 primary and secondary school students
• 8.7% were classified as pathological gamers
• Pathological gamers are more likely to:
– Spend twice as much time playing (averaging 37
hours/week)
– Poorer social competence
– Decreasing time with family and friends in past year
because of games
– Neglecting self-care to play games
Choo, H., Gentile, D., Sim, T., Li, D. D., Khoo, A., & Liau, A.
(2010). Pathological video-gaming among Singaporean youth.

M, 16 year old Chinese Male
“Future seems like a fog”
Presentation
• Unusually quiet, perfectionistic personality
• Took a long time to respond to questions, often saying “I
don’t know how to say”
• Extreme dislike in learning Chinese, good results in
other subjects
• School late-coming started in Secondary 1 after
schoolmate commented that he was too quiet and weird
• Said he had no friends, felt lonely during recess
• Started to be absent from school and stopped going to
school completely from June 2017
• Stayed in his room, played games through the night,
slept during the day
• Little communication at home with family members

Service Provision
• Referred to REACH and diagnosed with gaming disorder
• Referred for psychotherapy and his parents referred to
community agency for family therapy
• Therapy sessions at home ended after 3 sessions in Aug
2017 as M felt that it was pointless to continue therapy
• Referred to Enhanced Step-Up programme with YMCA
Project Bridge. Youth worker was to explore alternative
education or vocational training options with M. Only
attended one session with youth worker.

Challenges
• Lack of motivation to engage in psychotherapy
• M’s father not keen for M to see the psychiatrist
• Parents blaming school for not protecting M from school
bullies
• M’s difficulties in self-expression
• M’s parents expecting M to verbalize his difficulties to them

Guiding him through the fog
• School teachers did a home visit in March 2018 to bring
him test papers and chinese new year goodies. M told
teacher that he was keen to seek help through medication.
• Expressed that he would like to do better but he does not
know how and does not feel like it.
• Dr appointment made for him in 3 weeks time. Did not
attend as he was crying at home before appointment.
• Appointment postponed to Apr 2018. M was diagnosed as
having mixed anxiety and depressive symptoms and
prescribed medication.
• Referred to see REACH to resume psychotherapy.

Guiding him through the fog
• Saw M for 7 sessions of psychotherapy in 2018
• Felt that he was unmotivated, unproductive and has
serious problem with procrastination
• Goal for therapy was to find motivation in life
• Employed cognitive behavioural approach in therapy
• Sharing of case formulation to help him understand his
difficulties
– How his anxiety and perfectionistic personality traits led to
avoidance of important tasks and instead engaging in
procrastination activities like gaming
• Engaged in exposure therapy to address anxiety
• Taught M adaptive coping strategies in preparation for
return to school

Case formulation
Predisposing
Factors
Precipitating
Factors
Perpetuating
Factors
Protective
Factors
Shy
temperament
Perfectionistic
personality
traits
Poor verbal
expression
abilities
Bullying and
ostracization in
secondary
school
Use of
avoidance
Low motivation
during periods
of low mood
Black and white
thinking
High self-
expectations
Negative belief
that help from
family means
that he is
incapable
Supportive
school
Supportive
parents and
friends

Seeing light beyond the fog
• Returned to school in Jan 2019
• REACH wrote a memo to school recommending for him to
be dropped from Express to Normal stream to reduce
academic stress. He will take his GCE N levels exams this
year.
• Motivated and engaged at the beginning and wanted to
take two subjects at Express level
• Recurrence of late-coming and absenteeism from school
towards middle of the year
• Told psychiatrist that the reason was that he was lazy
• Doctor felt that it is likely to be avoidance due to increasing
pressure to perform academically. Medication dosage was
increased.
Case reflections
• Continued outreach from school and extended
family was instrumental
• Working with the socially withdrawn takes time
• Case conceptualization is key in helping them
understand their difficulties and in planning for
interventions
Case Conceptualization
• Consider biological, psychological and social
(and spiritual) factors
• Avoid bias of conceptualizing through the lens of
your profession or training

Biological factors
• Physical health problems
– eg, diabetes, eczema
• Mental health disorders
– Psychotic disorders (eg, schizophrenia)
– Anxiety disorders (eg, social anxiety)
– Mood disorders (eg, depression)
– Development disorders (eg, autism)
– Personality disorders (eg, paranoid, schizoid)
– Stress related disorders (eg, PTSD)
Psychological factors
• Early childhood experiences or adverse
childhood events
• Self esteem/image
• Personality
• Procrastination
• Social competence

Social factors
• Societal and family expectations
• Family dynamics
• Parenting styles
• Relationships
• School issues

Service Provision - Outreach
• Be familiar with the typical activities of the
socially withdrawn
– Gaming
– Social media
– Drama shows
– Anime/manga

Service Provision - Outreach
• Physical outreach
– Build rapport through their interests
– Playing games with them
• Virtual outreach
– Gaming worlds, guilds/clans
– Social media
– Online forums

Service Provision - Interventions
• Biological factors
– Medical treatment
– Medication
• Psychological factors
– Psychotherapy
– Case management
• Social factors
– Parenting training
– Family therapy
– School interventions

Summary
• There are the socially withdrawn in every society
but they may present to services under various
forms
• Complex biological, psychological, and social
factors might underlie the social withdrawal
• Services for the socially withdrawn should
ideally assess clients using the biological,
psychological and social framework in order to
provide them with appropriate interventions