shraddha ppt
TRANSCRIPT

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 1/35
ooTransfusion ReactionSHRADDHA
BANSAL.C.
M.SC PART II
MICROBIOLOGY
BIOSCIENCE DEPT

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 2/35
CONTENTS:
Blood transfusion Indications of blood transfusion
History
Blood transfusion reaction
Hemolytic blood transfusion reaction Non hemolytic blood transfusion reaction
and its types.
Graft versus host disease
General considerations to prevent blood transfusion reaction. References

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 3/35
BLOOD TRANSFUSION
Blood transfusion is the
infusion of whole blood or a
blood component such asplasma, red blood cells or
platelets into the patients
venous circulation.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 4/35
.INDICATIONS OF BLOOD
TRANSFUSION To increase oxygen carrying capacity of
blood. e.g. Anemia.
To compensate for the blood loss. e.g.
severe hemorrhage, hemolytic
anemia, surgical operations.
To restore blood volume. e.g. Burns, shock.
To promote haemostasis.e.g hemophilia.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 5/35
HISTORY The first historical attempt at blood
transfusion was described by the 17th
century chronicler Stefano Infessura.
Infessura relates that, in 1492, Pope
Innocent VIII sank into a coma, the
blood of three boys was infused into
him at the suggestion of a physician.
T
he boys were ten years old,however, not only did the pope die,
but so did the three children.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 6/35
Many patients had died until
1901,Karl Landsteiner
explained the mechanism
that mixing of blood from two
individuals can lead to blood
clumping or agglutination.
The clumped red cells can
crack and cause toxic
reactions, which can have
fatal consequences.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 7/35
It is the abnormal signs and
symptoms that will occur
during or after transfusion and
effects the patients health.
The severity of the reaction
varies from being relativelymild to more severe which at
times can be fatal.
BLOOD TRANSFUSION
REACTION

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 8/35
TYPES OF BLOOD
TRANSFUSION REACTION There are two types of blood transfusion
reactions:
1. Hemolytic transfusion reaction.
2. Non hemolytic transfusion reaction.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 9/35
HEMOL YTIC TRANSFUSION
REACTIONS
Hemolytic transfusion reactions are themost severe type of reactions that occurswhen the red blood cell were given to thepatient are destroyed by the patient¶s ownimmune system & it can be categorized
into two types:(a) Intravascular transfusion reaction
(b) Extravascular transfusion reaction

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 10/35
INTRAVASCULAR
TRANSFUSION REACTION In ITR, haemolysis of red cells takes place within the
circulatory system. This type of reaction is mainly due to
IgM antibodies, mediated by the rapid activation of
complement system and is usually associated with the
transfusion of ABO incompatible blood.
The clinical effects of an ITR are immediate, usually
within minutes after starting the transfusion, thus also
called as ACUTE HAEMOL YTIC TRANSFUSION
REACTIONS (AHTR).
8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 11/35
EXTRAVASCULAR
TRANSFUSION REACTION These reactions are rarely severe and mainly
due to IgG antibodies. These antibodies bring
about the destruction of red cells by the
macrophages in the spleen or liver. The clinical evidence of reaction is some what
slower and in some cases may be delayed upto
two weeks or more after transfusion, thus also
called as DELAYED HEMOL YTIC
TRANSFUSION REACTIONS (DHTR).
8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 12/35
CausesClinical
Manifestation Management
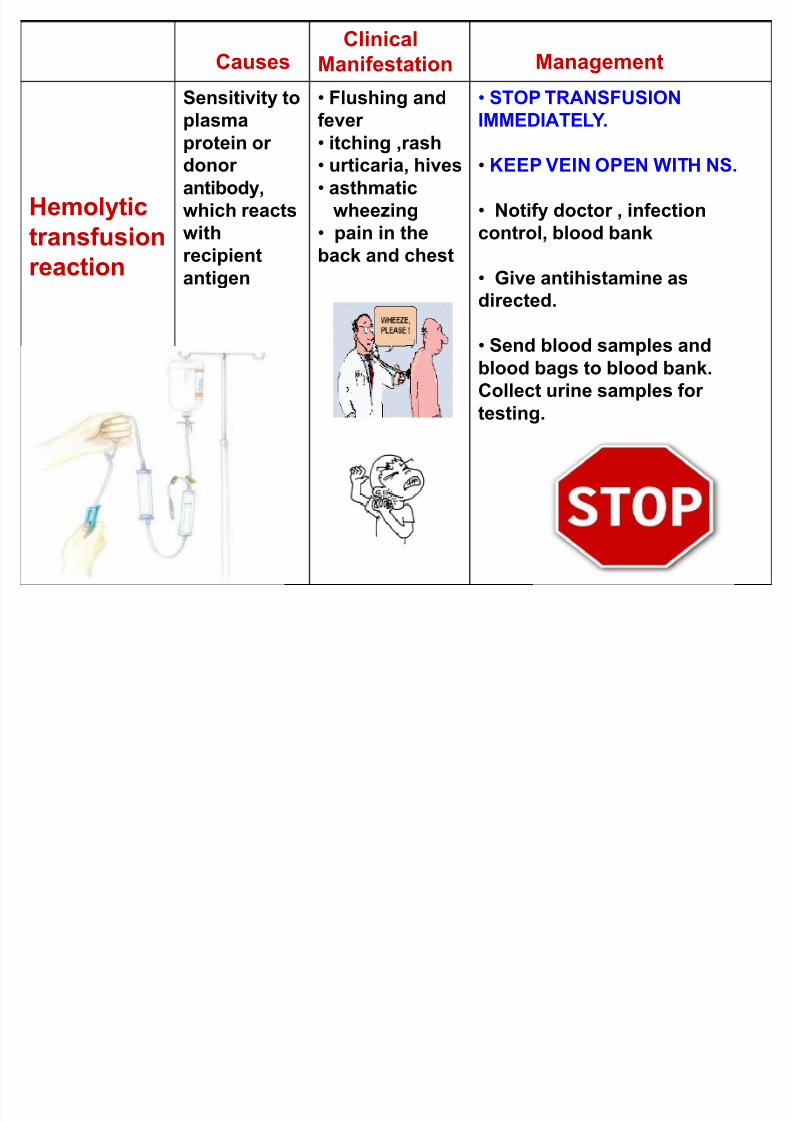
Hemolytic
transfusion
reaction
Sensitivity to
plasma
protein or donor
antibody,
which reacts
with
recipient
antigen
Flushing and
fever
itching ,rash urticaria, hives
asthmatic
wheezing
pain in the
back and chest
STOP TRANSFUSION
IMMEDIATEL Y.
KEEP VEIN OPEN WITH NS.
Notify doctor , infection
control, blood bank
Give antihistamine asdirected.
Send blood samples and
blood bags to blood bank.
Collect urine samples for
testing.
8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 13/35
Laboratory Investigations:
Pink or red discoloration on post-transfusion
plasma indicates the presence of free
haemoglobin due to red cell destruction.
Yellow or brown discoloration of the sampledrawn 6-8 hour after transfusion indicates
increased bilirubin.
Perform direct antiglobulin test (DAT) on the pre-
and post-transfusion sample.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 14/35
Continue:
Rapid test to distinguish hematuria fromhemoglobinuria. The onset of red urine during or
shortly after a blood transfusion may represent
hemoglobinuria (indicating an acute hemolytic
reaction) or hematuria (indicating bleeding in thelower urinary tract).

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 15/35
Prevention
ASSESSMENT Before transfusion ask the patient about
past reaction. If patient has history of
reaction, alert health care provider , have
emergency drugs available, and remain atbed side for the first 30min.
The time between the suspicion of
transfusion reaction, investigation and
treatment should be as short as possible.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 16/35
NON HEMOL YTIC
TRANSFUSION REACTION These are mild type of transfusion reactions and can be
categorized as:
- Febrile non hemolytic transfusion reaction
- Urticarial (allergic) transfusion reaction.- Anaphylatic transfusion reaction.
- Circulatory overload.
- Non cardiogenic pulmonary edema.
- Graft versus host disease.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 17/35
Febrile non haemolytic
transfusion reaction These reactions are the most common and
account for over 90% of transfusion reaction.
These are benign, self limiting reaction due to
the presence of antibodies to WBC or plateletsantigens and are usually seen in multi
transfused patients.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 18/35
Causes Clinical
Manifestations
Management
Febrile non
haemolytic
transfusion
reaction
hypersensitivity to
donor white blood
cells , platelets, or plasma protein
-sudden chills
and fever
-anxietyheadache
Malaise
STOP TRANSFUSION
IMMEDIATEL Y
KEEP VEIN
OPEN WITH NS
Notify doctor ,
infection control, blood
bank
give antipyretics asdirected.
check temperature
every 1/2hrs.or as
indicated
send blood samples
and blood bags toblood bank. Collect
urine samples for
testing.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 19/35
Prevention
- ASSESSMENT
Give antipyretic before
transfusion as directed.
Leukocyte ± poor blood
products may be
recommended for futuretransfusion.
8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 20/35
Urticarial (Allergic) transfusion
reaction
This type of reaction may be due to the patients
performed, regains reacting with transfused
allergens or due to soluble substances in donor
plasma.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 21/35
Causes Clinical
Mainifestations
Management
Urticarial
(allergic)
transfusionreaction
Transfusion of
blood or bloodcomponents
contaminated
with bacteria.
rapid onset of
chillsHigh fever
Vomiting ,
diarrhea
Marked
hypotension
STOP TRANSFUSION
IMMEDIATEL Y
KEEP VEIN OPEN
WITH NS.
give antipyretics as
directed.
check temperature every
1/2hrs.or as indicated obtain cultures of
patients blood
return blood bags &
blood set to blood bank.
treat septicemia as
directed ( IV fluids.Antibiotics...
Give antihistamine.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 22/35
Prevention
Do not permit blood to stand
at room temperature longer
than necessary warm
temperatures promotebacterial growth.
Inspect blood for gas
bubbles, clotting or abnormalcolor.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 23/35
Anaphylactic transfusion
reaction
This is a severe, life threatening reaction which
occur in rare patients who are IgA deficient and
have developed anti-IgA antibodies.
The reaction developed quickly within minutes of starting the transfusion.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 24/35
Causes Clinical
Mainifestations
Management
Anaphylactic
Transfusion
reaction
Fluid
administrated at arate or volume
greater than the
circulatory
system can
accommodate
increased bloodin pulmonary
vessels.
rise in venous
pressure gastrointestinal
upset
Cough
STOP TRANSFUSION
IMMEDIATEL Y
KEEP VEIN OPEN
WITH NS
place patient upright
with feet in dependent
position. administer prescribed
diuretic, oxygen,
epinephrine.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 25/35
Prevention
Any patient with anti IgA who
had an anaphylactic reaction
should be given:
Plasma free products e.g.
deglycerolized RBCs.
Plasma containing products
from IgA deficient donor only.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 26/35
Non cardiogenic pulmonary edema
It is rare but potentially fatal transfusion reaction. It is caused by donor¶s leucoagglutinins which
reacts with recipients leucocytes and produceaggregates.
These leucocytes aggregates are trapped in thepulmonary circulation causing endothelialdamage by oxidative, physical and other means.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 27/35
Clinical
Manifestations
Management Prevention
Non
cardiogenic
pulmonary
edema
acute respiratory
distress
Fever and chillsX-rays shows
pulmonary edema
No other sign of
heart failure
STOP
TRANSFUSION
IMMEDIATEL Y
KEEP VEIN OPEN
WITH NS
- give steroids every
6 hrs for 48 hrs.
-Give respiratorysupport.
Use washed red
blood cell in futuretransfusion.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 28/35
Causes Clinical
Manifestations
Management
Circulatory
overload
Fluid
administrated at ahigh rate or
volume greater
than the
circulatory system
can accommodate
Increased blood inpulmonary vessels
rise in venous
pressureCough
breathless
STOP TRANSFUSION
IMMEDIATEL Y
KEEP VEIN OPEN
WITH NS
Notify doctor ,
infection control, blood
bank place patient upright
with feet in dependent
position.
administer prescribed
diuretic, oxygen.
8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 29/35
Prevention
Concentrated blood products
should be given whenever
positive.
Transfuse at a rate within the
circulatory reserve of the patient.
Monitor central venous pressureof patient with heart disease.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 30/35
Graft versus host disease
GVHD is a rare complication following transfusion but hasbeen reported in variety of conditions in which the
immune system is depressed.
They are the result of antibodiesin the recipient¶s plasma directed
against antigens on the
donor¶s erythrocytes.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 31/35
Causes Clinical
Manifestations
Management
Graft
versus host
disease
donorslymphocytes
engrafting in the
recipient &
reacting against
host antigen.
-Fever, rash,
diarrhoea
-Liver dysfunction
-Bonemarrow
suppression
leukocyte free blood or
irradiated bloodcomponents.

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 32/35
GENERAL
CONSIDERATIONSTO PREVENT
BLOODTRANSFUSION
REACTION

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 33/35
LABPRATORY ST AFF
DONORS
BEFORE receiving blood
DURINGInstruct the client
Remain with the patient-15min
V/S ± every hour until 1hr after
transfusionBlood components are infused
within standard time limits ( 4 hours)
AFTER
Healthy donors
Blood screening for infectious
diseases.Blood compatibility ± RH
Proper storage
Antibody screening
Doctor order Consent
Patient assessment
Preparation-IV cannula
Equipment - Multi-lead tubing
Premedicate the PT.30min-T AB.
before transfusion - IV
AFTER receiving bloodCheck blood
Patient identityPatient assessment ± bed side
Close observation to the pt.
Proper dispose of IV tubing/bag
Documentation

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 34/35
Continue«.
Compatibility Test:
MAJOR MINORPatient¶s serum Patient¶s cell
+ +
Donor¶s cell Donor¶s serum

8/2/2019 Shraddha Ppt
http://slidepdf.com/reader/full/shraddha-ppt 35/35
REFERENCES