shoulder anatomy
DESCRIPTION
Shoulder Anatomy. Shoulder. It is a ball and socket joint that moves in all three planes and has. Most mobile and least stable joint. Shoulder joint motions. Flexion- is raising the arm in the lateral plane from 0-180 degrees. Extension- return to anatomical position. - PowerPoint PPT PresentationTRANSCRIPT

Shoulder Anatomy
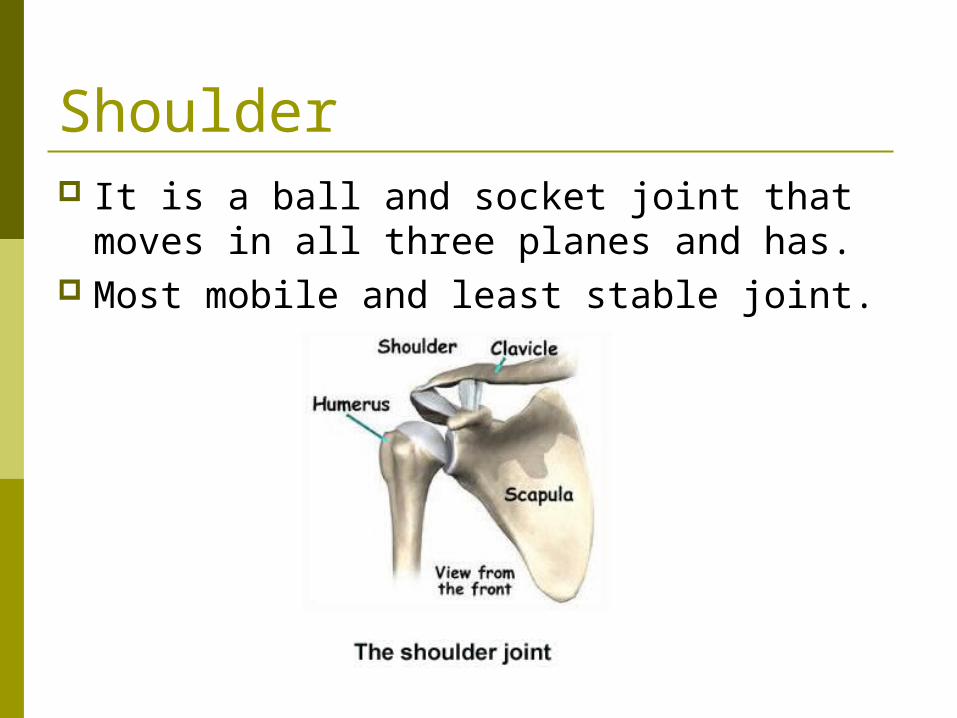
Shoulder It is a ball and socket joint that moves in
all three planes and has. Most mobile and least stable joint.

Shoulder joint motions Flexion- is raising the arm in the lateral
plane from 0-180 degrees. Extension- return to anatomical position. Hyperextension- 0-45 degrees back
through the lateral plane.

Shoulder joint motions Abduction- arm moving in the frontal plane
away from the body, with a 0-180 degrees of motion.
Adduction- arm moving back to midline, with 0-180 degrees of motion.

Shoulder joint motions Internal Rotation-
occur in the transverse plane. This can go to 90 degrees into body
External Rotation- occurs in the transverse plane, 90 degrees out from neutral.
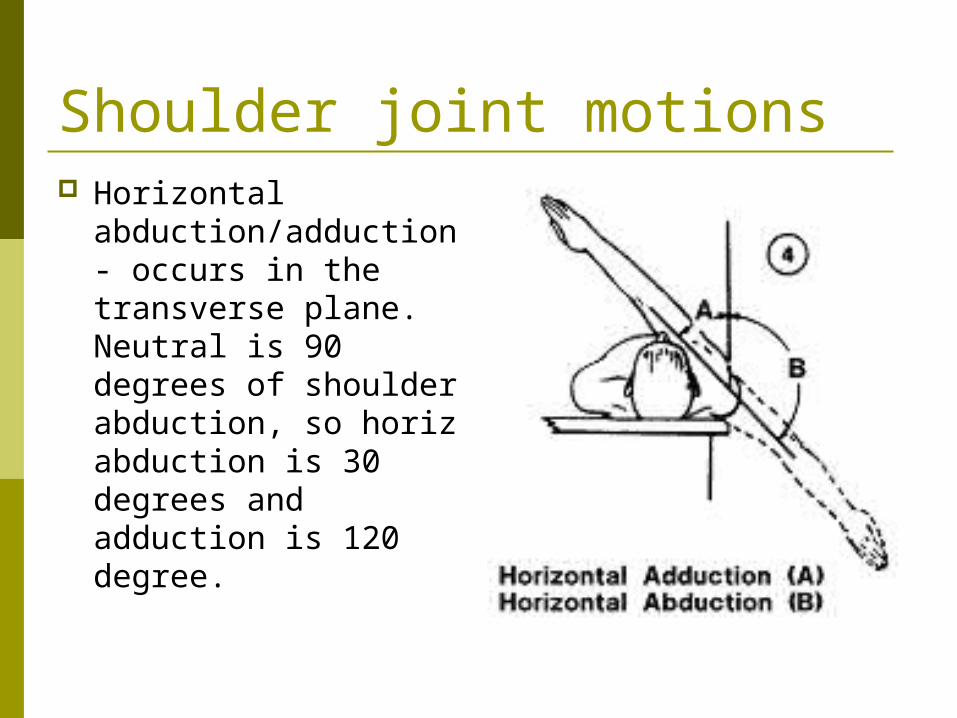
Shoulder joint motions Horizontal
abduction/adduction- occurs in the transverse plane. Neutral is 90 degrees of shoulder abduction, so horiz abduction is 30 degrees and adduction is 120 degree.

Shoulder joint motions Scaption- flexion in
the scapular plane, vs the lateral or frontal plane. 180 degree of motion can occur.

Shoulder Landmarks
ScapulaGlenoid labrum-fibrocartilage ring attached to the rim of the glenoid fossa, which deepens the cavity.

Shoulder Landmarks Humerus-
Head- is the semi round proximal end, articulates with the scapula.
Shaft- body of the humerus is the area between the neck and the epicondyles.
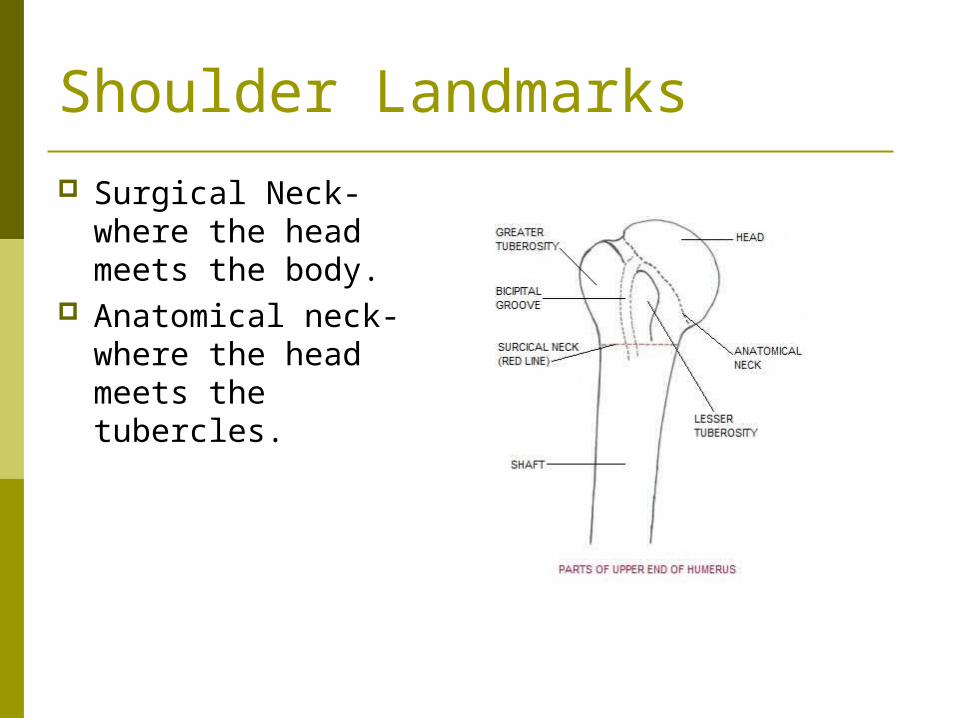
Shoulder Landmarks Surgical Neck- where
the head meets the body.
Anatomical neck- where the head meets the tubercles.

Shoulder Landmarks
Greater Tubercle/Tuberosity- large projection lateral to the head. Supraspinatus, infraspinatus and teres minor attach here.

Shoulder Landmarks
Lesser Tubercle/Tuberosity- smaller projection on the anterior surface, subscapularis attaches here.

Shoulder Landmarks
Deltoid tuberosity- lateral side, near the midpoint, deltoid attaches here.

Shoulder Landmarks
Bicipital Groove- groove between the tubercles containing the long head of the biceps tendon.

Impingement Syndrome A condition that occurs when the space between
the humeral head and the acromion above becomes narrowed.
The three things that can get pinched are the:joint capsule, tendons of rotator cuff, and bursa.
Impingement Syndrome Impingement can create either bursitis, or
tendonitis depending on what structure is being squeezed.
Overhead athletes are more likely to have problems with this injury.
1/3 of shoulder problems are due to impingement.

Impingement Syndrome Signs and Sx
Pain and tender GH joint
Pain and weak active abd in mid range
Limited internal rotation + Hawkins Test Tender subacromial
area possibly into the deltoid
Treatment Correct technique Strengthen inferior
muscles Strengthen weak
rotator cuff muscles
Impingement Syndrome Special Tests
Hawkins Test Neer’s Impingement Cross over Test

Impingement Syndrome Stretches-
3 way door stretch Posterior shoulder Internal Rotation with
Exercises Internal Rotation External Rotation Adduction
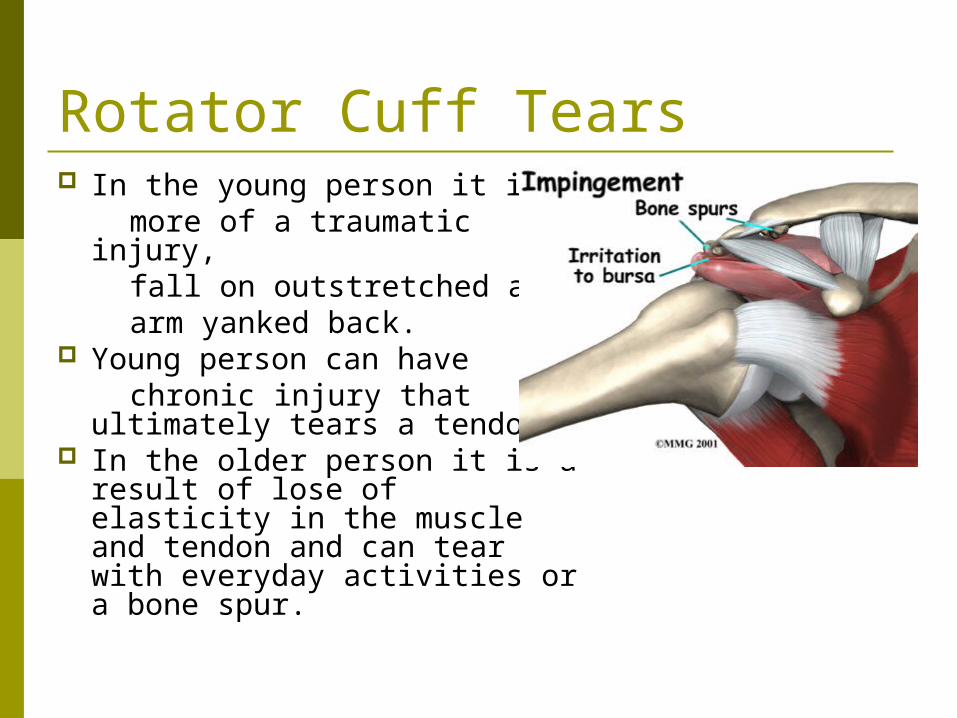
Rotator Cuff Tears In the young person it is more of a traumatic injury, fall on outstretched arm, arm yanked back. Young person can have chronic injury that ultimately
tears a tendon. In the older person it is a
result of lose of elasticity in the muscle and tendon and can tear with everyday activities or a bone spur.
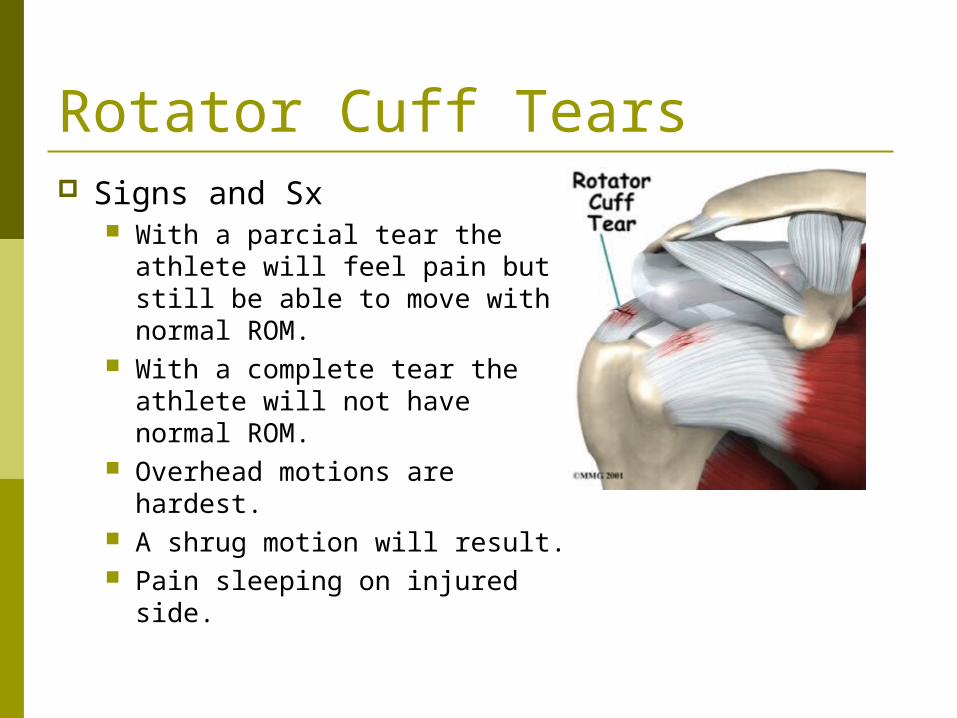
Rotator Cuff Tears Signs and Sx
With a parcial tear the athlete will feel pain but still be able to move with normal ROM.
With a complete tear the athlete will not have normal ROM.
Overhead motions are hardest. A shrug motion will result. Pain sleeping on injured side.

Rotator Cuff Tears Special Tests
Active Abduction-look for hiking shoulder Drop Arm sign- athlete abduct above head
then lowers slow, look for loss of muscle control.
Supraspinatus muscle test- looking for weakness
Empty Can Test- supraspinatus/subscap motion MRI is final diagnostic tool

Biceps Tendonitis Discomfort in the front
of the shoulder. Can be caused by
impingement. Special Tests-
Speed’s Test Yergeson’s Test

Traumatic Shoulder Injuries Shoulder Dislocation Glenoid Labrum Injuries Multidirectional Instabilites Acromioclavicular Separation Brachial Plexus Injury Fractures

Anterior Shoulder Dislocation A humerus can
dislocate Anteroinferiorly-front
and down (most common)
Inferiorly – down Posteriorly -back
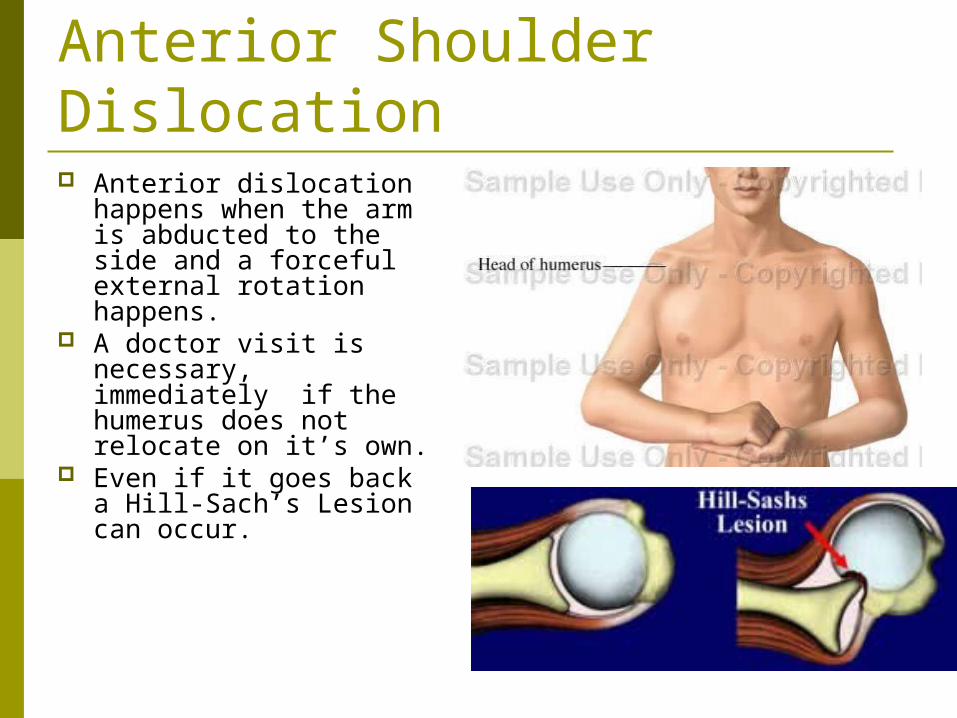
Anterior Shoulder Dislocation Anterior dislocation
happens when the arm is abducted to the side and a forceful external rotation happens.
A doctor visit is necessary, immediately if the humerus does not relocate on it’s own.
Even if it goes back a Hill-Sach’s Lesion can occur.

Anterior Shoulder Dislocation Rehabilitation is very
important to this injury.
Reinjury will likely happen if a first time injury happens before the age of 20.
Surgery may be necessary if repeated dislocation occurs.

Special Test-Dislocation Apprehension test
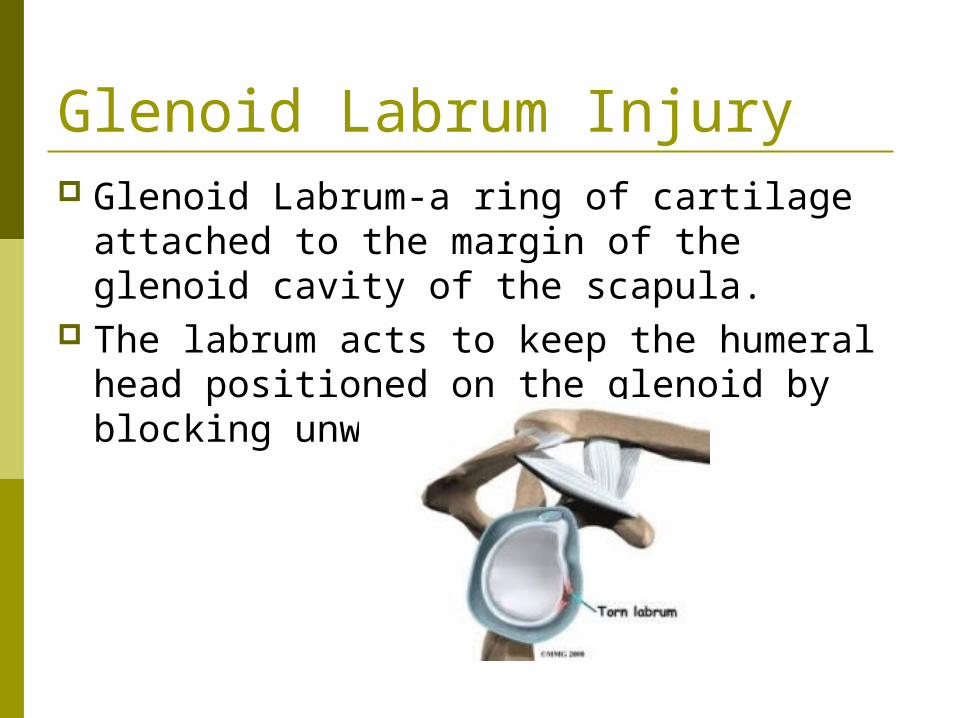
Glenoid Labrum Injury Glenoid Labrum-a ring of cartilage
attached to the margin of the glenoid cavity of the scapula.
The labrum acts to keep the humeral head positioned on the glenoid by blocking unwanted movement.
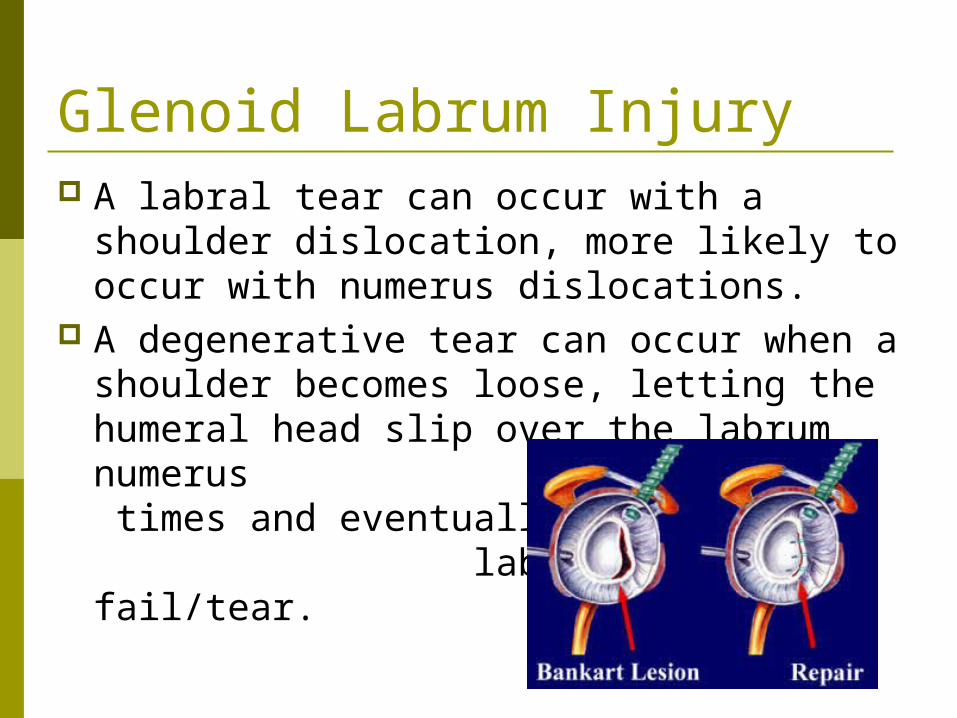
Glenoid Labrum Injury A labral tear can occur with a shoulder
dislocation, more likely to occur with numerus dislocations.
A degenerative tear can occur when a shoulder becomes loose, letting the humeral head slip over the labrum numerus times and eventually the labrum will fail/tear.
Glenoid Labrum Injury Signs and Sx
Pain with catching and popping
Possible weakness Possible limited ROM
Special Tests Clunk Test Cross Over Test
Treatment Rotator Cuff
strengthening Surgery

Multidirectional Instabilities Typically an anatomical problem. Multiple dislocations will make it worse. Exercise may help with the problem, surgery
sometimes, but not always Weight bearing exercise are helpful. Like what?

Acromicavicular Separation Also known as an AC sprain. Occurs due to fall on outstretched arm or tip of
shoulder. May be due to blow to tip of shoulder

AC separation Signs and Sx
deformity Pain in vicinity of AC
Special Test Shear Test Sulcus Sign
Treatment Three grades –the
grade determines treatment
Grade one is exercise and ice
Grade two immobilize 3 weeks and then exercise
Grade three immobilize 5 weeks and then exerccise

Muscles of the Shoulder Joint Deltoid is superficial muscle. All three
parts of it attach to the deltoid tuberosity. Axillary Nerve
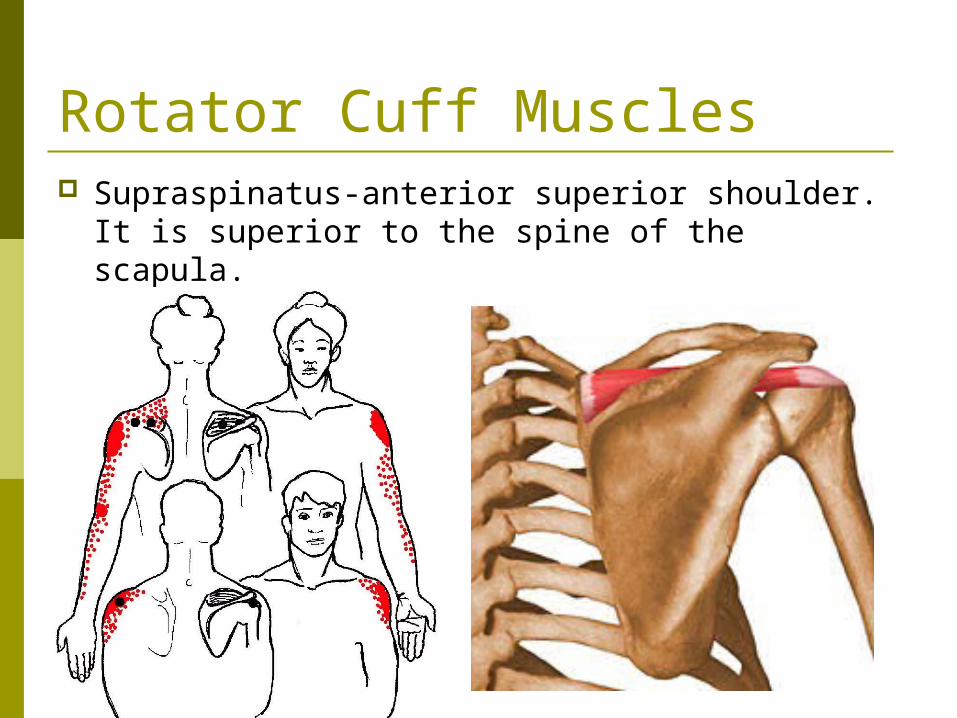
Rotator Cuff Muscles Supraspinatus-anterior superior shoulder. It is
superior to the spine of the scapula. abduction

Muscles of the Shoulder Joint Pectoralis Major-
Clavicular portion-most effective during flexion from 0-90
Sternal portion- most effective in extension 180-120 degrees of shoulder extension
Both of them adduct, internally rotate and horizontally adduct the shoulder.
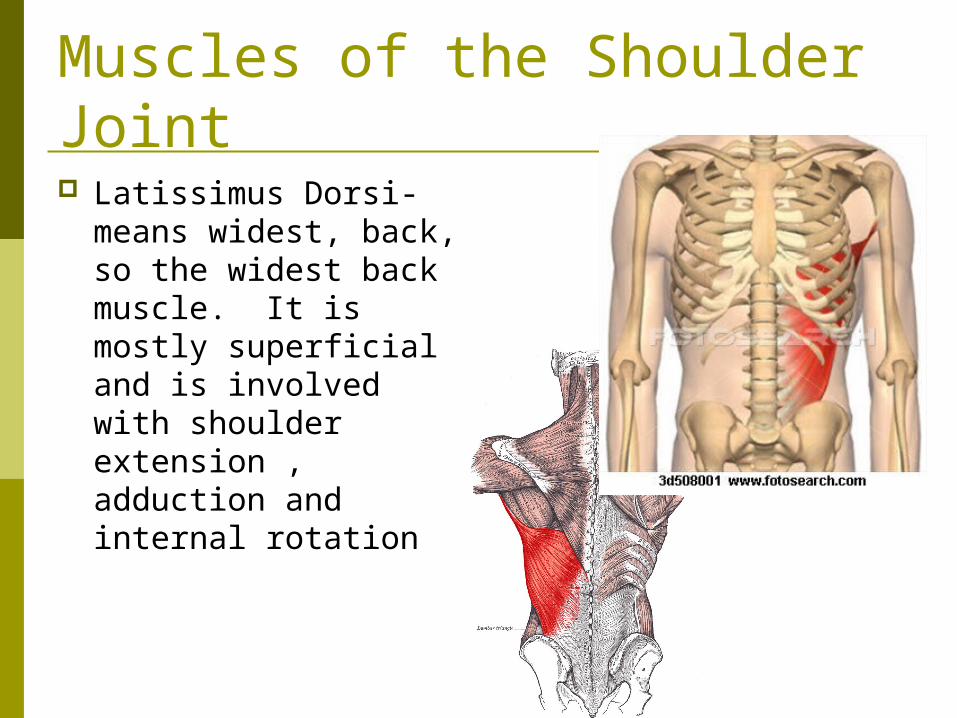
Muscles of the Shoulder Joint Latissimus Dorsi-
means widest, back, so the widest back muscle. It is mostly superficial and is involved with shoulder extension , adduction and internal rotation
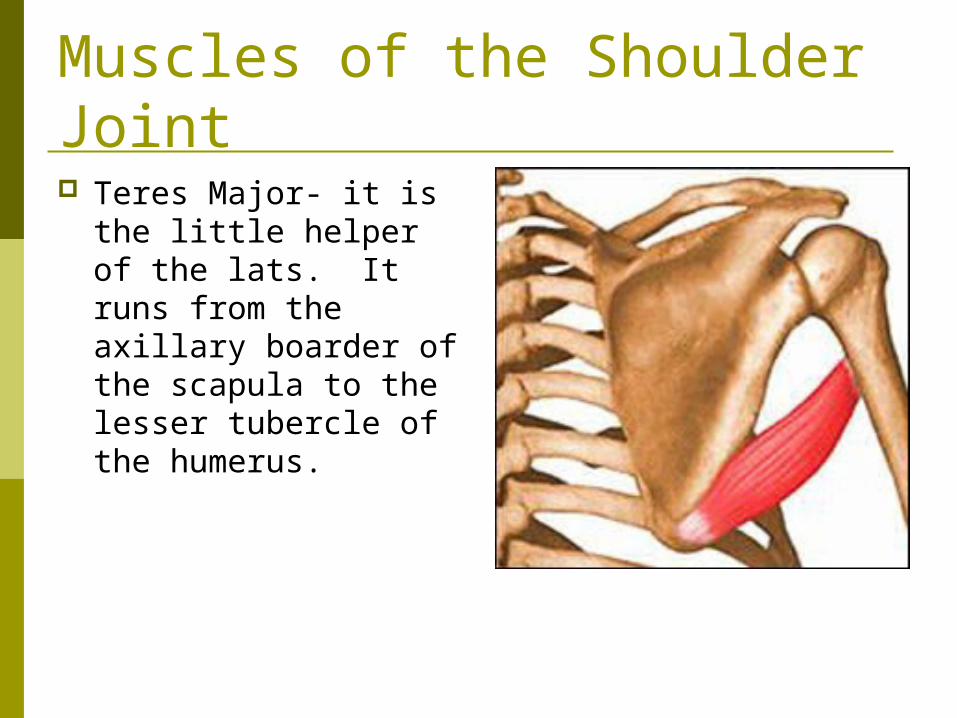
Muscles of the Shoulder Joint Teres Major- it is the
little helper of the lats. It runs from the axillary boarder of the scapula to the lesser tubercle of the humerus.

Rotator Cuff Muscles Infraspinatus-
posterior inferior shoulder
Inferior to the spine of the scapula
External rotation

Rotator Cuff Muscles
Teres Minor- posterior shoulder Adduction

Rotator Cuff Muscles Subscapularis-anterior
shoulder Internal rotation
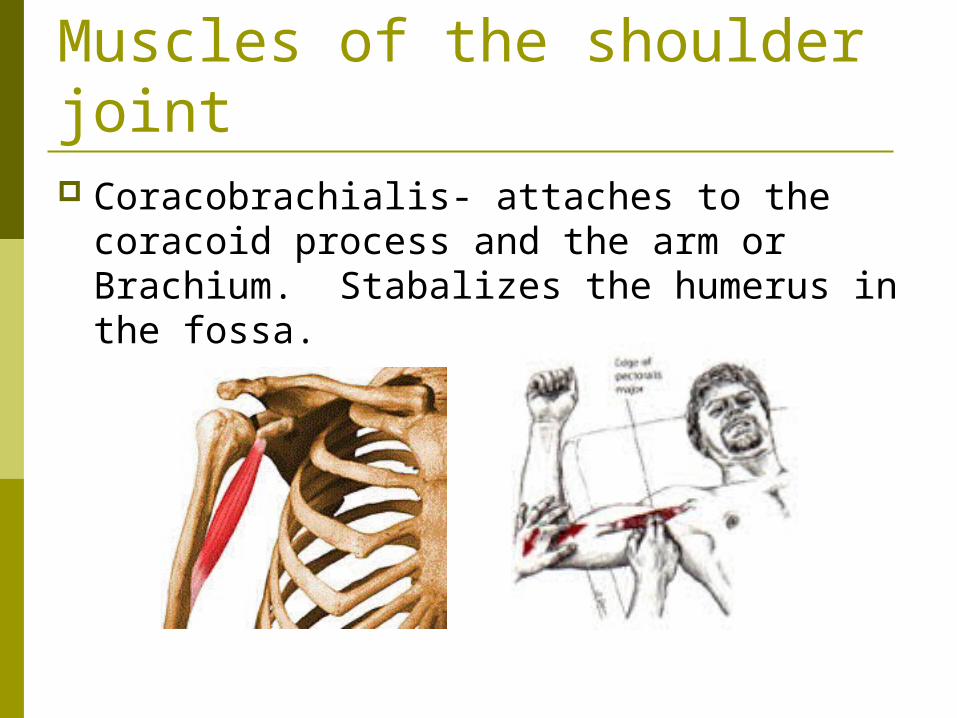
Muscles of the shoulder joint Coracobrachialis- attaches to the coracoid
process and the arm or Brachium. Stabalizes the humerus in the fossa.

Muscles of the Shoulder Joint The four rotator cuff
muscles cover the humeral head and hold the head against the glenoid fossa.
Rotator Cuff Muscles Know these muscles if you remember
nothing else. Infraspinatus Supraspinatus Subscapularis Teres Minor