severly elevated blood pressure : dr peter andre soltau
TRANSCRIPT

SEVERE ELEVATED HIGH BLOOD
PRESSURE AND “NOTHING ELSE”
CLINICALLY, DO THEY NEED ADMISSION ?
Dr. Peter Andre SoltauPGY 4.5 DM Emergency Medicine
UWI MONA


Case 1■ 55 year old male patient presents to the triage department, after
he presented to the ophthalmology clinic for cataract surgery to the left eye. He was found to have an elevated blood pressure and was therefore referred to A&E for further management with a diagnosis of hypertensive urgency vs emergency. The patient is a known hypertensive diabetic maintained on Nifedipine 30mg bd, Enalapril 20mg bd and Metformin 500mg tid. He reports no SOB, leg swelling or chest pain. He does however admit to waking from 5am to come to the hospital for St. Thomas and did not take his medications
■ His Vitals at triage : T 95.7 P102 RR18b/min BP 190/115 U/A –prot+ , leu+, blood+
■ What is his triage designation?■ How would you manage this patient?


Case 2■ 78 year old female patient presents to the triage department for management of
her high blood pressure. She presented to the local health clinic two weeks prior for her routine follow up and was told her blood pressure was very high 180/110. She notes she had been having headaches at that time and was told by the doctor it was due to her blood pressure. She was given a referral to the hospital, however she decided to use home remedy “garlic” and watch the pressure.
■ Today she went to a health fair held at her church and the blood pressure was noted to be 210/160. She decided to present because her headache is persistent and the BP just wont go down. The patient is a known hypertensive maintained on Amlodipine 10mg od and Enalapril 20mg bd. She reports forgetting where she puts her medications at times but claims good compliance. She reports dizziness but no SOB, leg swelling, chest pain or limb weakness.
■ Vitals at triage : T 96.2 P82 RR24b/min BP 240/150 U/A - NAD
■ How would you manage this patient?


What is Severe Elevated High Blood Pressure ?
■Severely elevated blood pressure is commonly defined as a systolic blood pressure greater than or equal to 180 mm Hg or diastolic blood pressure greater than or equal to 110 mm Hg *
■JNC 7 classified Stage 2 hypertension as systolic blood pressure greater than or equal to 160 mm Hg or diastolic blood pressure greater than or equal to 100 mm Hg* Severely increased blood pressure in the emergency department.
Shayne PH, Pitts SR. Ann Emerg Med 2003 Apr;41(4):513-29.

What is a Hypertensive Emergency ?■ 1) Is there acute end-organ dysfunction and/or damage?
■ 2) Is the dysfunction attributable to the elevated blood pressure (or will the elevated BP likely to make the dysfunction worse)?
■ 3) Is altering the BP necessary to improve the organ dysfunction?

Types Of Hypertensive Emergencies■Microvascular disorders:
characterized by small vessel dysregulation, with endothelial damage and local inflammation (e.g. encephalopathy, pre-eclampsia/eclampsia)
■“Macro” vascular disorders: (i.e. CHF, aortic dissection, stroke, subarachnoid hemorrhage)

Does triage BP correlate with outpatient HTN?
■For patients who present at triage with a high BP, an elevated second measurement 60 to 80 minutes later correlates highly with actual outpatient hypertension, and does not correlate with the patient’s anxiety and/or pain
Moderate-to-severe blood pressure elevation at ED entry: hypertension or normotension?Dieterle T, Schuurmans MM, Strobel W, Battegay EJ, Martina B Am J Emerg Med. 2005 Jul;23(4):474-9.
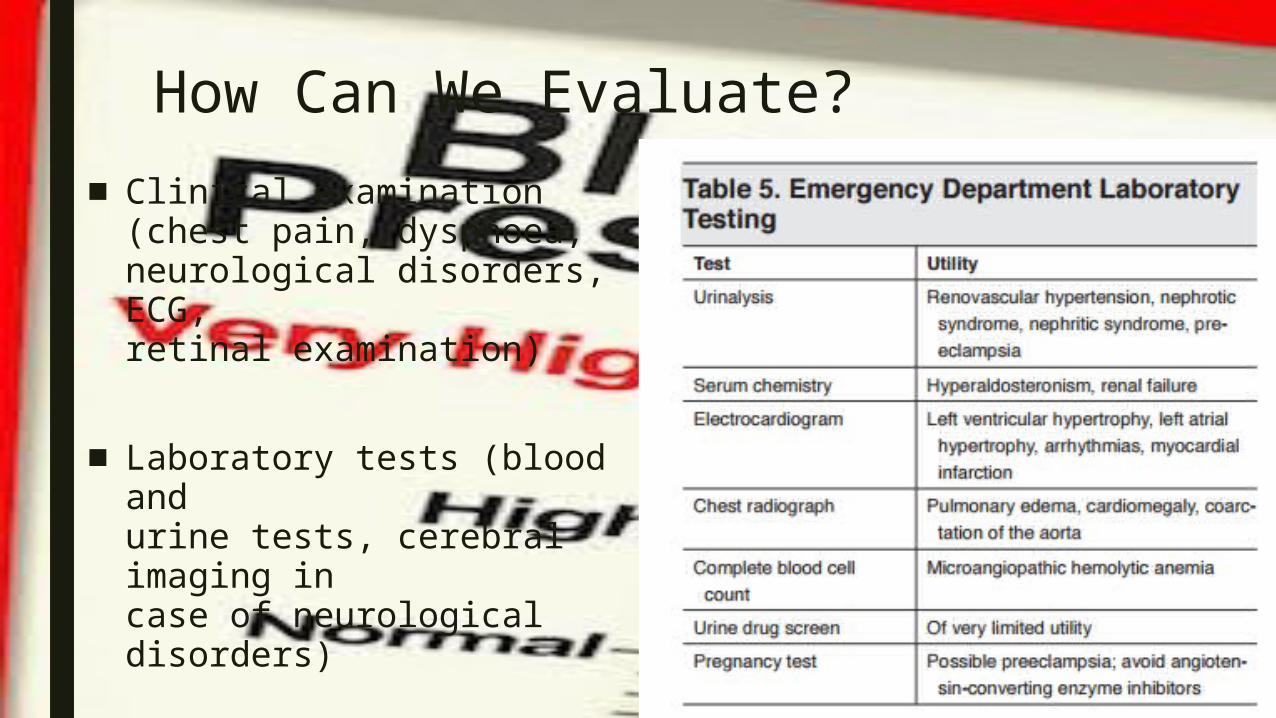
How Can We Evaluate?■Clinical examination
(chest pain, dyspnoea, neurological disorders, ECG,
retinal examination)
■Laboratory tests (blood and urine tests, cerebral imaging in case of neurological disorders)

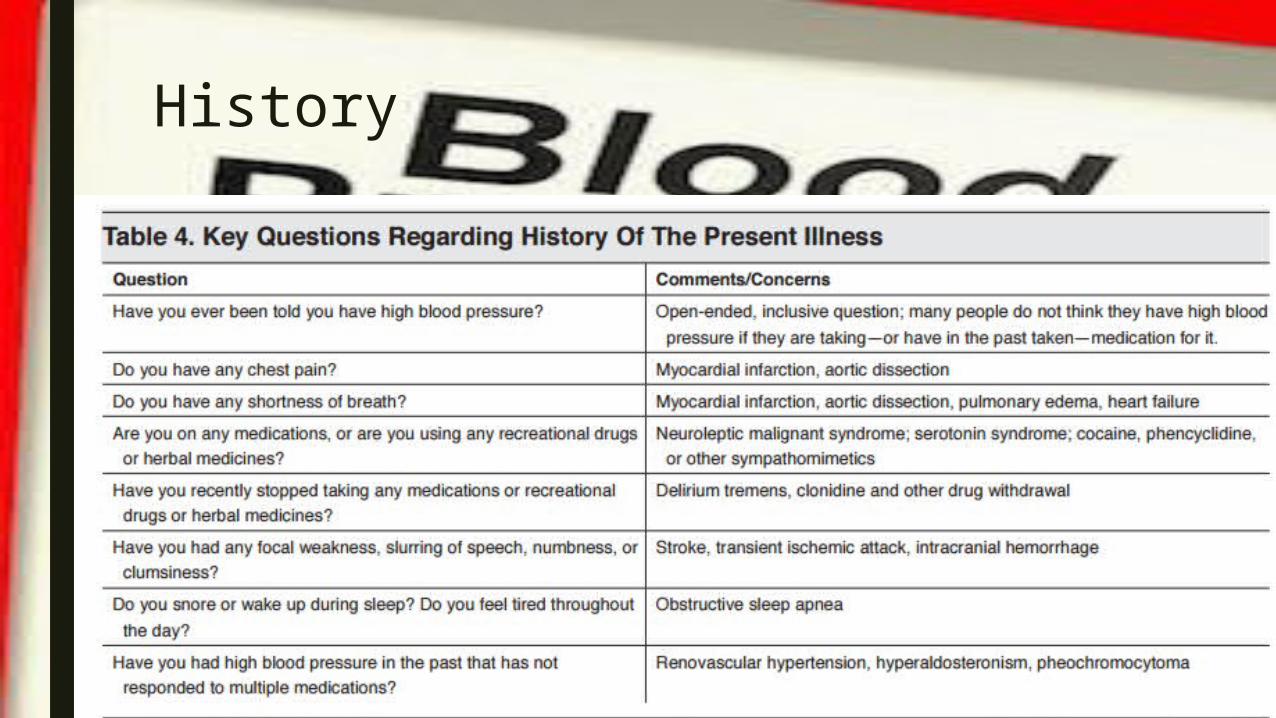
History1) Does the patient have a history of hypertension?2) Are they compliant with their medications? Any medication changes?3) Do they have a recent trigger (high salt diet, alcohol use, NSAID use, steroids, cold meds)4) Are they pregnant or are they postpartum?5) When was the last time they had their BP checked (and is this chronic hypertension that does not require acute management)?

History■CNS: Headache, nausea, vomiting, confusion, visual
changes, neurologic localizing symptoms■Cardiac: chest pain, shortness of breath, ankle
swelling, orthopnea, PND■Renal: polyuria, nocturia, hematuria■Secondary causes should be searched in patients who
are younger (<30), and have very high BP (renal artery stenosis). Also think about Cushing syndrome, hyperaldosteronism, pheochromocytoma, etc.
History

What diagnostic tests should we do for patients with asymptomatic hypertension?
■Karras et al show a 6– 7% rate of clinically meaningful findings:Bloods : BMP 2%, CBC 2%Urine analysis: 4%ECG 2%
■Consider screening tests on select patients (poor follow up and you think that the result of the test will affect disposition (ie admission)
Karras DJ, et al: Utility of routine testing for patients with asymptomatic severe blood pressure elevation in the emergency department. Ann Emerg Med 2008; 51:231

What diagnostic tests should we do for patients with asymptomatic hypertension?
■In JNC 7, routine laboratory testing, including an ECG for left ventricular hypertrophy or ischemia, chest radiograph (CXR) for cardiomegaly or pulmonary edema, serum creatinine level for renal dysfunction, and urinalysis for proteinuria, is recommended before initiating therapy
■ACEP 2013 guidelines suggest no workup is needed

ACEP 2013■“ Currently, there is very little evidence to guide
the practitioner about which patients to test who present to the ED with asymptomatic elevated blood pressure. No current study measured adverse outcomes on the basis of the decision to test patients with asymptomatic elevated blood pressure. Of the available evidence, ED screening for creatinine level may identify a small group of patients with renal dysfunction in the setting of asymptomatic markedly elevated blood pressure. However, it is unclear how this frequency compares with that of patients who present with normal or near-normal blood pressures. No other diagnostic screening tests appear to be useful”

Treating Asymptomatic Hypertension
Should we treat patients with asymptomatic hypertension in the ED?
■ Although there is a paucity of evidence for treatment of hypertension in the ED affecting short term outcome, reducing BP will reduce risk of morbidity and mortality over the longer term
■ How low and how fast should you go?■ Do not drop BP rapidly, as it alters cerebral perfusion and puts
patients at risk for organ underperfusion (i.e. ischemic stroke), especially if their blood pressure elevation has been chronic
Should we treat patients with asymptomatic hypertension in the ED?■ The ACEP Clinical Policy states there is no need to immediately
reduce an asymptomatic patient with high blood pressure■ They can instead be referred back to their family physician for
BP management
■ The Canadian Emergency Medicine Cardiac Research and Education Group (EMREG) guidelines advise ED physicians to consider beginning antihypertensive therapy for patients with BP of >180/110, and to initiate treatment if BP > 200/130
■ These recommendations are based on limited evidence

Is there a target BP for asymptomatic HTN?
■ There are no guidelines for the exact target BP that needs to be achieved before discharge.
■ 2015: Study in Academic Emergency Medicine suggests that prescription of anti-hypertensives in the ED may be safe and effective, at least in the short-term, for patients with asymptomatic hypertension

Which drug is best for treatment of asymptomatic hypertension?
■ Most patients can be started on a thiazide, an ACE-inhibitor or ARB, or a calcium-channel blocker (CCB) according to the JNC 8 -Exceptions:
■ 1. For patients with coronary artery disease, a B-blocker is first line■ 2. For black patients, cardiac risk reduction is best achieved with a
thiazide or a CCB■ ** Contraindications for each agent.
ACEi or ARBs are contraindicated in patients at risk for hyperkalemiaDo not use thiazides in patients with gout, and avoid B-blockers in patients with COPD or asthma. **

Follow up for patients with asymptomatic hypertension
■Although there is a paucity of evidence, most clinicians recommend follow up within 7 days, or more urgently for patients with severe hypertension or comorbidities
■CHEP guidelines are more liberal; they advise BP be rechecked within 1 month
■However, patients started on an ACE or an ARB should follow up sooner, and have their electrolytes checked within 1 week.

Discharge Education & Instructions
■Have a conversation with the patient■Assure the patient that their BP won’t cause them
any harm■Educate the patient that the damage from BP
happens over months to years to decades- not hours to days
■Make sure that the patient understands that rapid BP correction can harm them
■Give good return precautions (chest pain, neuro sxs, etc.)
■Give written discharge instructions regarding follow-up

Questions ?