serum biomarkers: promising tool for predicting … · 2/26/2015 · serum biomarkers: promising...
TRANSCRIPT

Lab in Statistical Design and Analysis
Final Lab Report
Serum Biomarkers: Promising Tool for Predicting Survival and
Tumor Response in Malignant Mesothelioma
Abstract
Introduction
Malignant Mesothelioma (MM) is an aggressive form of cancer with median survival less than 1
year. The number of MM cases has risen steadily over the past two decades. Radiologic
assessment of the tumor response for MM is difficult, therefore researchers are trying to
identify an alternative approach to monitor tumor response. In this study, we are interested in
using serum biomarkers (CA125, SMRP, MPF and CYFRA) as a tool to monitor tumor response
and predict survival outcome.
Methods
Data from patients diagnosed with MM between 2005 and 2010 at the University Health
Network were collected retrospectively from chart review. Baseline biomarkers values and
other covariates were used in survival analysis. Tumor response between pre and post
treatment, showing progression, stable and response were compared to corresponding changes
in the biomarkers values.
Results
Seventy-three patients (median age: 64 years old (range: 29-83)) were included in the overall survival
analysis with median follow-up time of 1.1 years (range: 0.05 – 3.5). Forty-four patients were
deceased and 29 still alive. The median survival was 1.5 years. Multi-variate analysis indicated
that the biomarker CYFRA (p=0.0005), baseline platelet (p=0.0012) and surgery (p=0.0004) were
predictive of survival. Associations were identified for biomarker CYFRA (p=0.037) and SMPR
(p=0.04) with the tumor response for patients treated with chemotherapy. No association was
observed for biomarker MPF and CA125.
Conclusion
Baseline CYFRA, platelet and surgery are potential predictors for survival outcome. Percentage
change or difference in SMRP or CYFRA pre and post treatment are potential useful markers of
tumor response. A prospective study with larger sample is recommended to validate the
findings in this study.
Table of Content
Abstract ----------------------------------------------------------------------------------------------------------------------------- 2
Table of Content ------------------------------------------------------------------------------------------------------------------ 3
Introduction ----------------------------------------------------------------------------------------------------------------------- 4
Materials and Methods --------------------------------------------------------------------------------------------------------- 5
1. Study Design/Population --------------------------------------------------------------------------------------------- 5
1.1 Study participants ------------------------------------------------------------------------------------------------ 5
1.2 Variable ------------------------------------------------------------------------------------------------------------- 6
2. Outcome ------------------------------------------------------------------------------------------------------------------ 7
3. Statistical Analysis ------------------------------------------------------------------------------------------------------ 7
3.1 Overall Survival --------------------------------------------------------------------------------------------------- 7
3.2 Association between the difference or percentage change in the pre and post values of the
biomarkers CA125, CYFRA, SMRP and MPF and the tumor response in each type of treatment ------ 8
4. Software ------------------------------------------------------------------------------------------------------------------ 8
Results ------------------------------------------------------------------------------------------------------------------------------- 9
5.1 Overall Survival ------------------------------------------------------------------------------------------------------ 9
5.2 Association between the difference or percentage change in the pre and post values of the
biomarkers CA125, CYFRA, SMRP and MPF and the response in each type of treatment ----------------- 13
Discussion ------------------------------------------------------------------------------------------------------------------------- 17
Conclusion ------------------------------------------------------------------------------------------------------------------------- 19
Reference-------------------------------------------------------------------------------------------------------------------------- 20
Appendices ------------------------------------------------------------------------------------------------------------------------ 21
A. Tables --------------------------------------------------------------------------------------------------------------------- 21
B. Figures -------------------------------------------------------------------------------------------------------------------- 23
SAS codes -------------------------------------------------------------------------------------------------------------------------- 48
4 | P a g e
Introduction
Asbestos, a silicate mineral which is resistant to fire and heat, is often used as electrical
insulation for hotplate wiring and in building insulation. It has been mined and exported from
Canada for centuries. Although asbestos has lucrative commercial qualities, it is carcinogenic.
Since 1960, industrial exposure to asbestos has led to a dramatic rise in the number of cases of
malignant mesothelioma (MM). MM is a rare form of cancer that affects the thin membrane of
the mesothelium (lining of lung, heart and abdomen). Malignant mesothelioma is highly
aggressive with median survival less than 1 year. Symptoms may not appear 20-50 years after
exposure. In Canada, the rate of diagnosed mesothelioma cases has risen steadily over the
past two decades, from 153 cases in 1984 to 344 cases in 20036.
Malignant mesothelioma does not usually grow spherically, rather as an increased
thickening of the pleural rind. Therefore, it is difficult to monitor the response to treatment for
MM patients. Non-invasive biomarker, which is defined as a characteristic that can be
objectively measured and evaluated as an indicator of normal and disease processes or
pharmacological responses5, have been widely used to predict, detect and monitor cancer
disease. Several immunohistochemical markers have been identified as a useful tool to monitor
the response. In this study, we are interested in using serum biomarkers as a tool to monitor
the response to treatment and predict survival outcome.
The four candidate serum biomarkers examined in this study are i) Cancer Antigen 125
(CA125), ii) Soluable mesothelin-related peptide (SMRP), iii) soluble cytokeratin 19 fragment
(CYFRA) and iv) megakaryocyte potentiating factor (MPF). These biomarkers are proteins found

5 | P a g e
on the surface of the cancerous cells. Previous studies have indicated that increased levels of
these biomarkers have a positive correlation with the metastases, tumor progression and
invasion. The two main objectives of this study are to examine the relationship between the
biomarkers and overall survival, as well as how the changes in values of the biomarkers related
to response to treatment (i.e. progression, response or stable).
As workplace exposure to asbestos continues in Canada, primarily in the mining and
construction sectors, it is important to identify non-invasive biological tools which can be used
to monitor or detect the disease so patient’s quality of life and life expectancy can be extended.
It will have positive impact on patients’ health as well as the economy, as billions of dollars will
be saved in treatment and compensation.
Materials and Methods
1. Study Design/Population
1.1 Study participants
This is a single institute retrospective chart-review study, which 117 UHN (University Health
Network) patients diagnosed with MM between 2005 and 2010 were included in the study.
Patients’ information was collected from clinical records, radiotherapy, surgical, pathology and
pharmacy records and recorded in MS Access database. No a priori calculation on sample size
was done and all available patients satisfied the above criteria were included.
In order to qualify for the survival analysis, a patient must have baseline biomarker values
obtained within 3 months of diagnosis and follow up data. For the analysis on response to
treatment, patients must have a pair of measurements pre and post treatment. Biomarker
6 | P a g e
values and CT scan results must be obtained both pre and post treatment. The pre-treatment
biomarker values must be within 1 month of the pre-treatment CT scan, same criteria apply for
the post-treatment.
1.2 Variable
The main variables of interest are the four biomarkers CA125, SMRP, CYFRA and MPF. Those
values were captured as continuous variables. For survival analysis, follow-up time
(continuous) was calculated from date of diagnosis to the last follow up date for alive patients,
and date of death for deceased patients. Covariates were examined in both uni-variate and
multi-variate survival analyses. Categorical covariates were sex (M/F), stage (1-4), thorax
involved (Y/N), histological subtype (epitheliod/biphasic), surgery (Y/N), ECOG (0/0+),
chemotherapy (Y/N), white cell count (≤8.3/>8.3), haemoglobin (≤140/>140), platelet count
(≤400/>400), chest pain (Y/N), weight loss (Y/N), smoking status (current/former/never).
Continuous covariate was age at diagnosis (calculated from date of diagnosis and date of birth).
For the analysis on response to treatment, radiological stage of the response was assessed
using the modified Response Evaluation Criteria In Solid Tumors (mRECIST), which measure
pleural tumor thickness perpendicular to the chest wall at three separate levels. CT scan was
obtained pre and post treatment, the change in tumor was classified as response (>30%
decrease in size), stable or progression (>20% increase in size). Difference and percentage
change were calculated from pre and post measurements of the four biomarkers. Difference
was calculated from subtracting the pre from the post measurement. Percentage change was
calculated from subtracting the pre from the post measurement then divided by the pre
treatment measurement. Missing data could not be imputed, they were treated as missing.
7 | P a g e
2. Outcome
There are two outcomes of interest i) Overall survival analysis ii) the association between the
difference or percentage change in the pre and post values of the biomarkers CA125, CYFRA,
SMRP and MPF and the tumor response in each type of treatment (chemotherapy, best
supportive care (BSC) and radiation). The difference and percentage change were used
because these are the two clinical standards that the clinicians were interested in to examine
the changes. Also clinicians were trying to mimic the analyses that were done in an earlier
study7.
3. Statistical Analysis
3.1 Overall Survival
Kaplan-Meier (non-parametric) and Cox proportional hazard (semi-parametric) were used for
the analyses. A patient had an event if the patient deceased. The follow-up time and the
covariates used in the analysis were provided in section 1.1. Uni-variate analyses on the 18
covariates were performed. Purposeful selection of covariates was used to select covariates for
the multi-variate model. Variables which were significant in the uni-variate model were
included in the multi-variate model. The variables that were significant in the new model
remained in the model and the ones that were not significant were removed. The remaining
variables (which were not significant in the uni-variate analysis) were added one by one to
decide the final model. The Cox proportional hazard assumption was tested by introducing
interaction between the covariate and the log of follow-up time. If the p-value of the
interaction term is not significant, the Cox proportional hazard assumption is not violated.
Interactions between the covariates in the final multi-variate model were examined. The

8 | P a g e
martingale residuals and deviance residuals were used to access the goodness of fit of the final
model.
3.2 Association between the difference or percentage change in the pre and
post values of the biomarkers CA125, CYFRA, SMRP and MPF and the tumor
response in each type of treatment
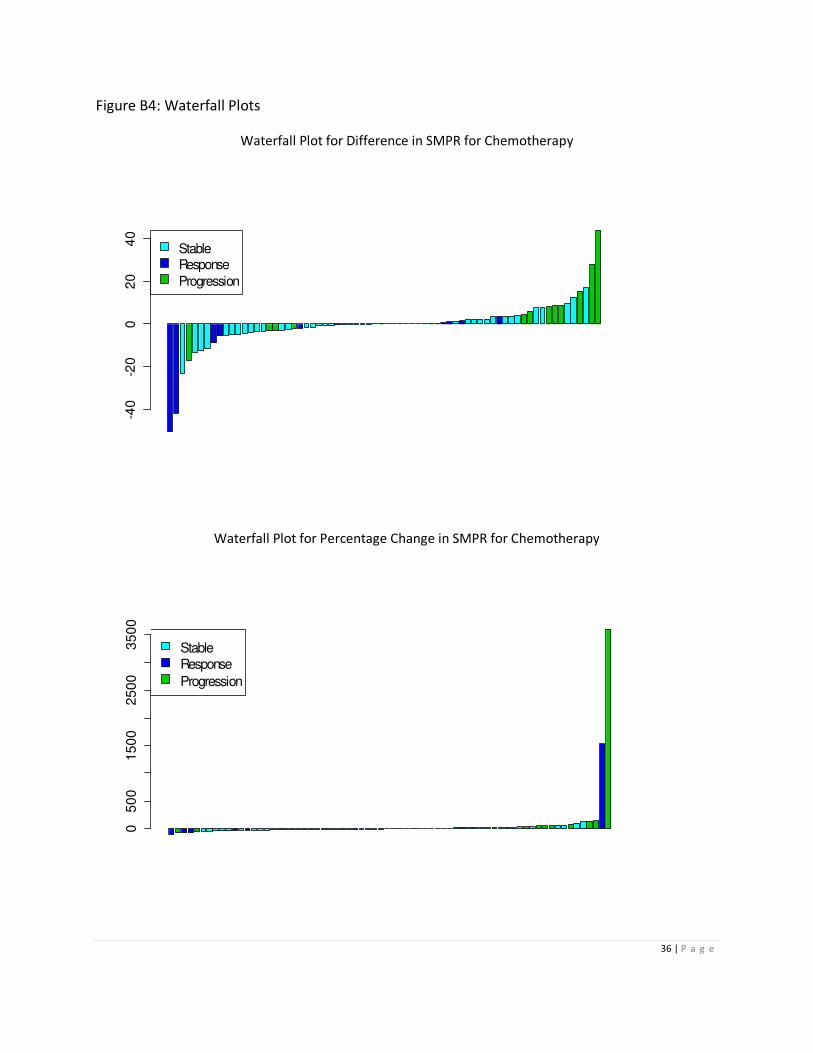
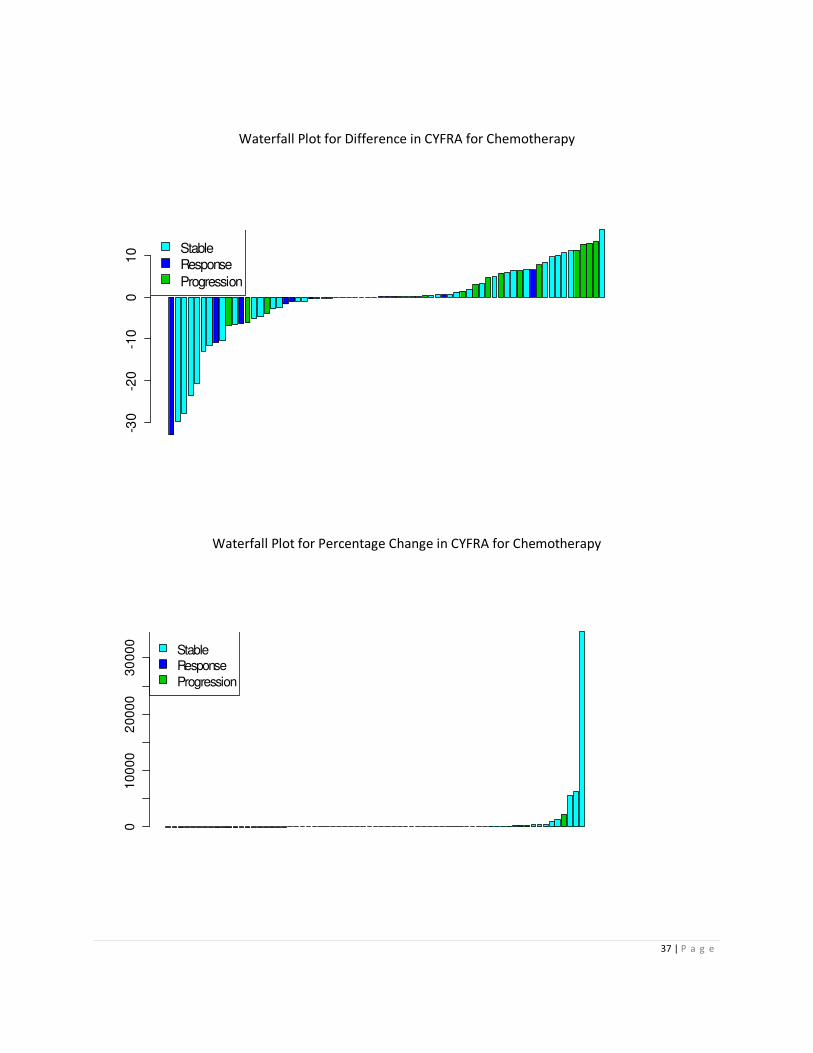
Box plots and waterfall plots were created to explore the difference and percentage change in
the biomarkers in each treatment group. Krustal-Wallis non-parametric test was used to
compare the difference or percentage change in the pre and post values of the biomarkers and
the response to treatment (progression, stable and response) in the chemotherapy group.
Wilcoxin-Mann-Whitney non-parametric test was used for the treatment group Best-
Supportive-Care because there were only two response types (progression and stable). There
were only a few patients in the radiation group, no analysis was carried out. Recognizing there
are other methodologies such as ANCOVA that can be used for the analysis, based on the
constraint to mimic analyses done in a previous study mentioned above, the described
methodologies were chosen. Correlation between the four biomarkers was evaluated using
spearman’s rank correlation coefficient.
4. Software
The SAS procedures: proc means, proc univariate, proc freq, proc npar1way, proc lifetest and
proc tphreg were used to carry out the statistical analysis. All analyses were performed using
SAS v9.1 for windows and all reported p-values were 2-sided. P-value < 0.05 was considered
significant. Reported p-values will not be adjusted for multiple testing; results should be
interpreted with caution.
9 | P a g e
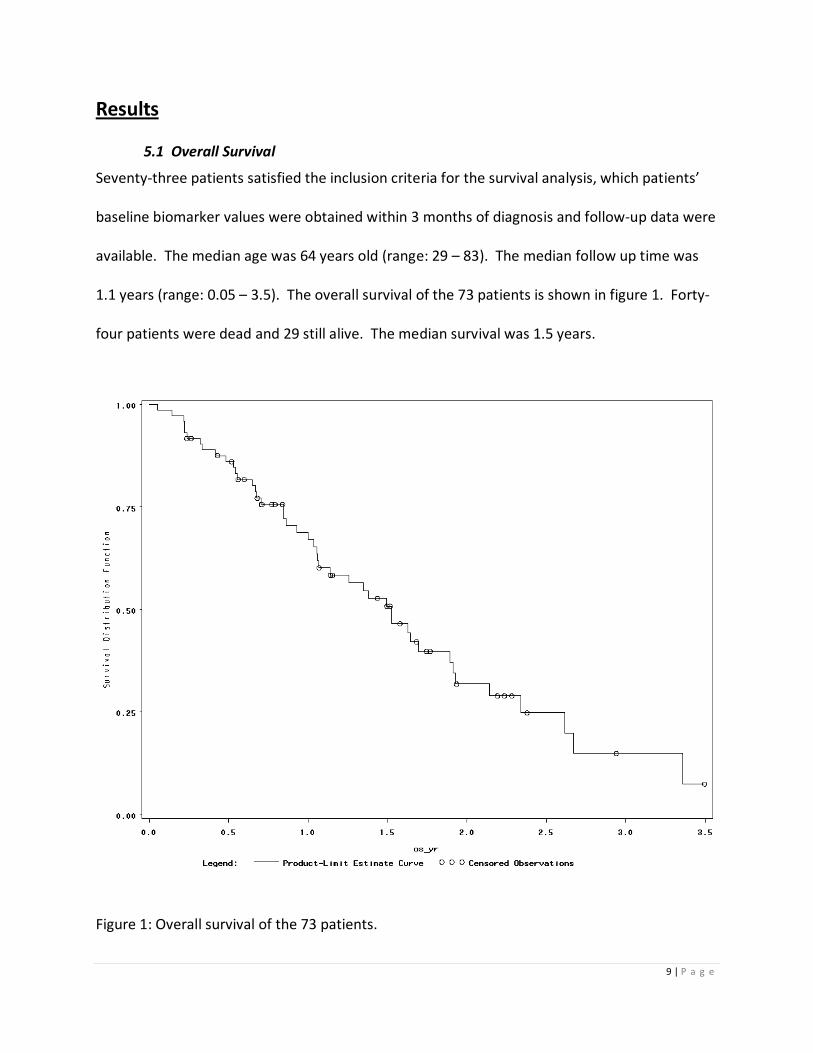
Results
5.1 Overall Survival
Seventy-three patients satisfied the inclusion criteria for the survival analysis, which patients’
baseline biomarker values were obtained within 3 months of diagnosis and follow-up data were
available. The median age was 64 years old (range: 29 – 83). The median follow up time was
1.1 years (range: 0.05 – 3.5). The overall survival of the 73 patients is shown in figure 1. Forty-
four patients were dead and 29 still alive. The median survival was 1.5 years.
Figure 1: Overall survival of the 73 patients.
10 | P a g e
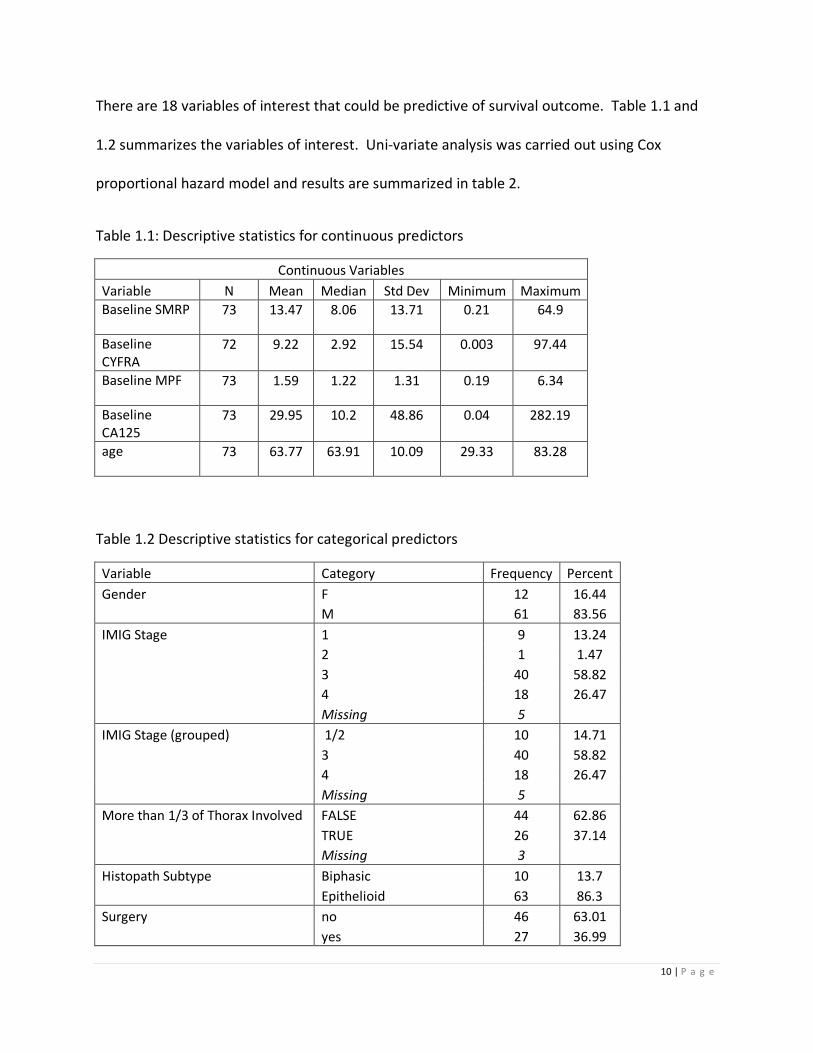
There are 18 variables of interest that could be predictive of survival outcome. Table 1.1 and
1.2 summarizes the variables of interest. Uni-variate analysis was carried out using Cox
proportional hazard model and results are summarized in table 2.
Table 1.1: Descriptive statistics for continuous predictors
Continuous Variables
Variable N Mean Median Std Dev Minimum Maximum
Baseline SMRP 73 13.47 8.06 13.71 0.21 64.9
Baseline
CYFRA
72 9.22 2.92 15.54 0.003 97.44
Baseline MPF 73 1.59 1.22 1.31 0.19 6.34
Baseline
CA125
73 29.95 10.2 48.86 0.04 282.19
age 73 63.77 63.91 10.09 29.33 83.28
Table 1.2 Descriptive statistics for categorical predictors
Variable Category Frequency Percent
Gender F 12 16.44
M 61 83.56
IMIG Stage 1 9 13.24
2 1 1.47
3 40 58.82
4 18 26.47
Missing 5
IMIG Stage (grouped) 1/2 10 14.71
3 40 58.82
4 18 26.47
Missing 5
More than 1/3 of Thorax Involved FALSE 44 62.86
TRUE 26 37.14
Missing 3
Histopath Subtype Biphasic 10 13.7
Epithelioid 63 86.3
Surgery no 46 63.01
yes 27 36.99

11 | P a g e
Chest Pain No 22 42.31
Yes 30 57.69
Missing 21
Weight Loss No 25 40.32
Yes 37 59.68
Missing 11
ECOG 0 37 50.68
1 27 36.99
2 5 6.85
3 4 5.48
ECOG (grouped) 0 37 50.68
1/2/3 36 49.32
Smoking Status Current 9 13.43
Former (>1 yr) 3 4.48
Former (>1 yr) Pack
years- 1 1.49
Never 32 47.76
former (>1 yr) 22 32.84
Missing 6
Smoking Status (grouped) never 32 47.76
former 26 38.81
current 9 13.43
Missing 6
Chemotherapy Yes 47 64.38
no 26 35.62
White Cell Count ≤ 8.3 37 60.66
> 8.3 24 39.34
Missing 12
Platelet ≤ 400 41 66.13
> 400 21 33.87
Missing 11
Haemoglobin ≤ 140 41 66.13
> 140 21 33.87
Missing 11
12 | P a g e
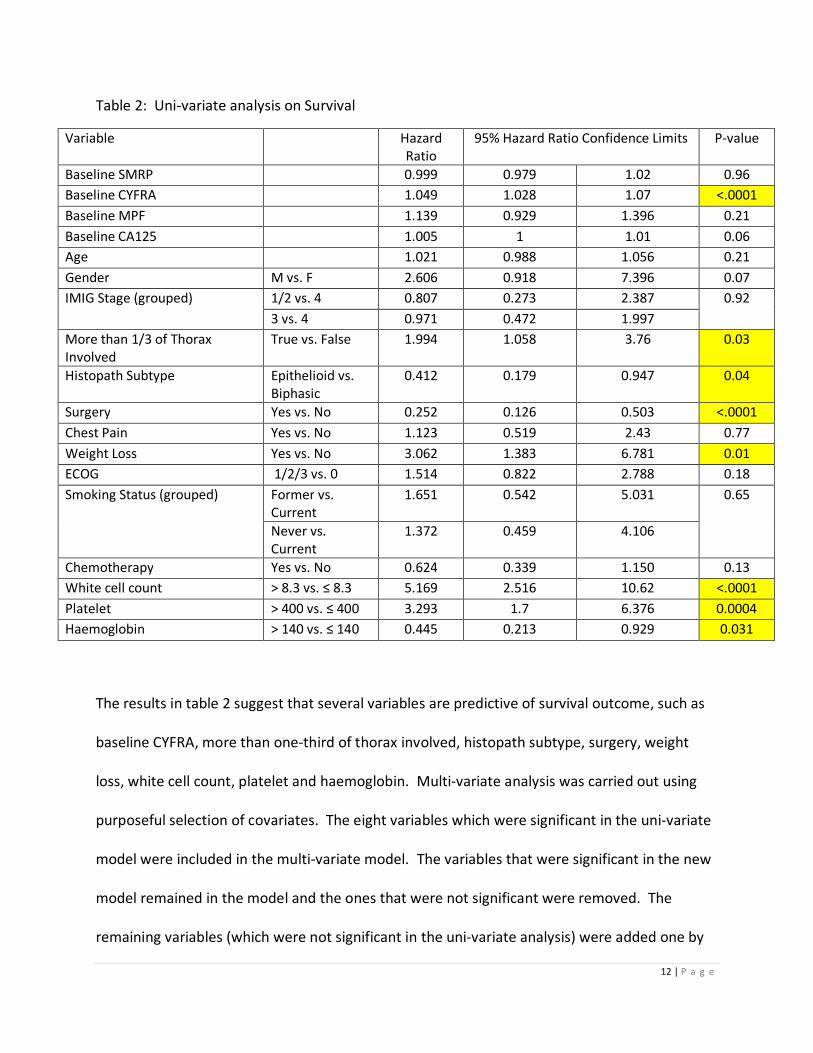
Table 2: Uni-variate analysis on Survival
Variable Hazard
Ratio
95% Hazard Ratio Confidence Limits P-value
Baseline SMRP 0.999 0.979 1.02 0.96
Baseline CYFRA 1.049 1.028 1.07 <.0001
Baseline MPF 1.139 0.929 1.396 0.21
Baseline CA125 1.005 1 1.01 0.06
Age 1.021 0.988 1.056 0.21
Gender M vs. F 2.606 0.918 7.396 0.07
IMIG Stage (grouped) 1/2 vs. 4 0.807 0.273 2.387 0.92
3 vs. 4 0.971 0.472 1.997
More than 1/3 of Thorax
Involved
True vs. False 1.994 1.058 3.76 0.03
Histopath Subtype Epithelioid vs.
Biphasic
0.412 0.179 0.947 0.04
Surgery Yes vs. No 0.252 0.126 0.503 <.0001
Chest Pain Yes vs. No 1.123 0.519 2.43 0.77
Weight Loss Yes vs. No 3.062 1.383 6.781 0.01
ECOG 1/2/3 vs. 0 1.514 0.822 2.788 0.18
Smoking Status (grouped) Former vs.
Current
1.651 0.542 5.031 0.65
Never vs.
Current
1.372 0.459 4.106
Chemotherapy Yes vs. No 0.624 0.339 1.150 0.13
White cell count > 8.3 vs. ≤ 8.3 5.169 2.516 10.62 <.0001
Platelet > 400 vs. ≤ 400 3.293 1.7 6.376 0.0004
Haemoglobin > 140 vs. ≤ 140 0.445 0.213 0.929 0.031
The results in table 2 suggest that several variables are predictive of survival outcome, such as
baseline CYFRA, more than one-third of thorax involved, histopath subtype, surgery, weight
loss, white cell count, platelet and haemoglobin. Multi-variate analysis was carried out using
purposeful selection of covariates. The eight variables which were significant in the uni-variate
model were included in the multi-variate model. The variables that were significant in the new
model remained in the model and the ones that were not significant were removed. The
remaining variables (which were not significant in the uni-variate analysis) were added one by

13 | P a g e
one to decide the final model. Table 3 presents the results for the multi-variate model. For
every unit increases in baseline CYFRA, the risk for event of death increases by 4%. The group
with platelet > 400 has 3 times the risk to experience of outcome of death whereas the group
with surgery has lower risk compare to the group without surgery. Interactions of the variables
in table 3 were examined and results are provided in Appendix A1. The proportional hazard
assumption was tested by introducing interaction between the covariate and the log of follow-
up time, results provided in Appendix A2. The goodness of fit of the model was examined using
martingale residuals and deviance residuals. The results are provided in Appendix B1 and B2.
The goodness of fit indicated this multi-variate model was suitable.
Table 3: Multi-variate analysis on Survival
Variable Hazard
Ratio
95% Hazard Ratio Confidence Limits P-value
Baseline CYFRA 1.04 1.02 1.07 0.0005
Platelet > 400 vs. ≤ 400 3.29 1.6 6.8 0.0012
Surgery Yes vs. No 0.22 0.1 0.5 0.0004
5.2 Association between the difference or percentage change in the pre and post
values of the biomarkers CA125, CYFRA, SMRP and MPF and the response in each
type of treatment
There were 104 patients satisfied the inclusion criteria and were included in this analysis. All of
these patients have a pair of pre and post treatment blood measurement and CT scan. Also the
blood measurements were obtained within 1 month from the CT scan. The analysis was carried
out separately for each of the treatment group (i.e. chemotherapy, best supportive care and
radiation). Table 4 summarizes the number of patients included in the analysis for each of the
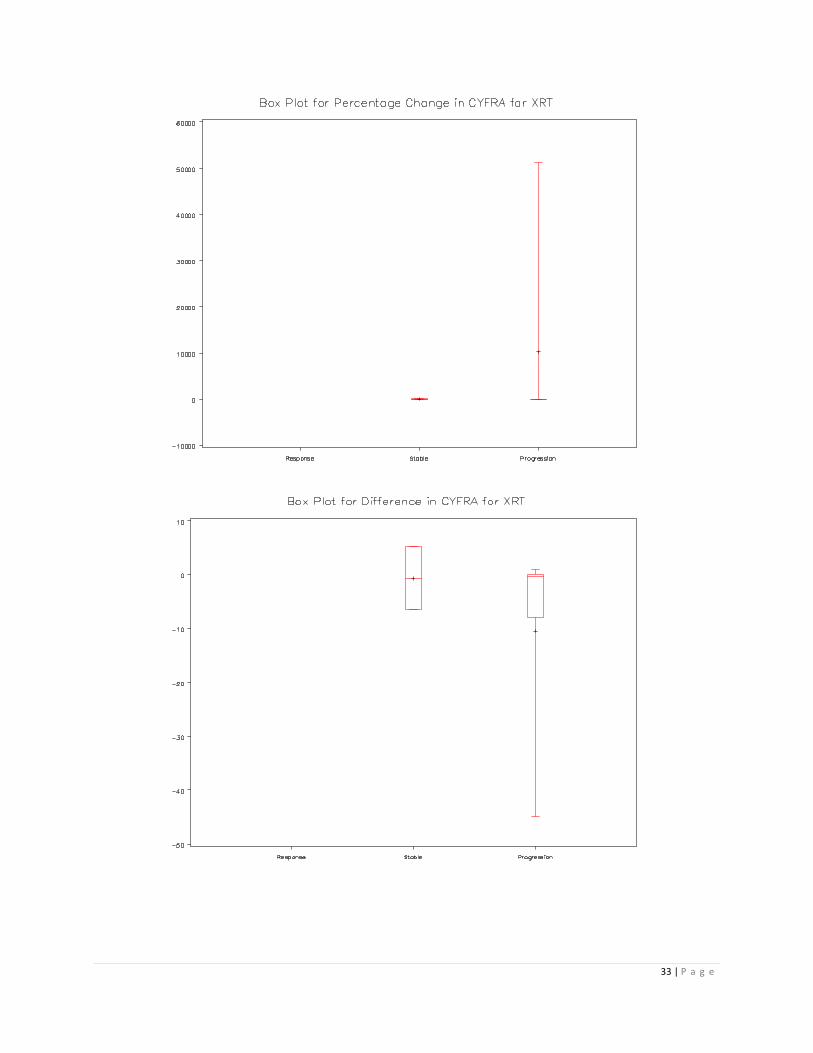
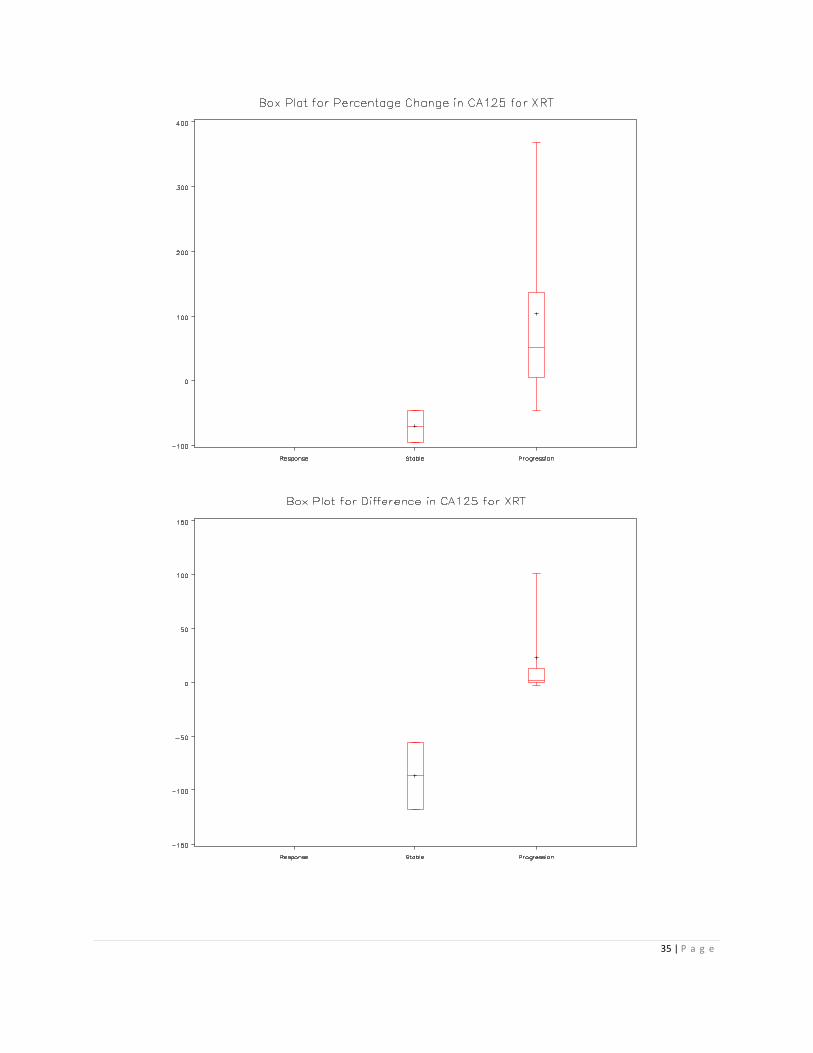
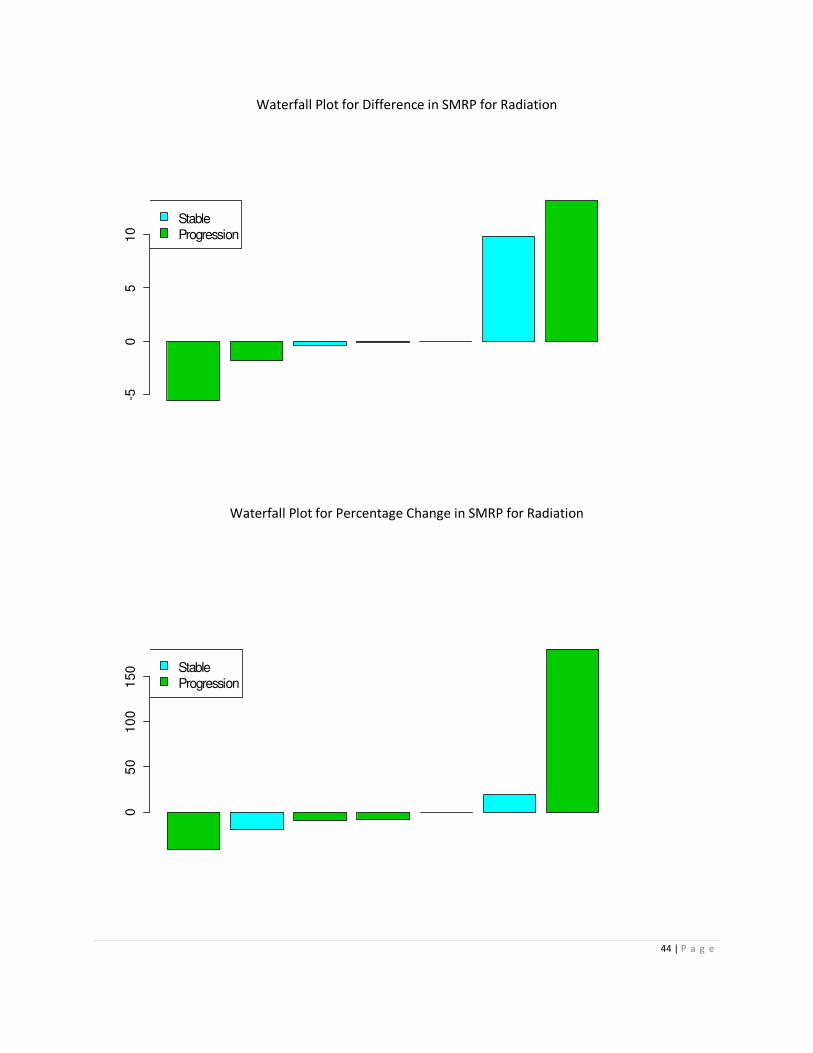
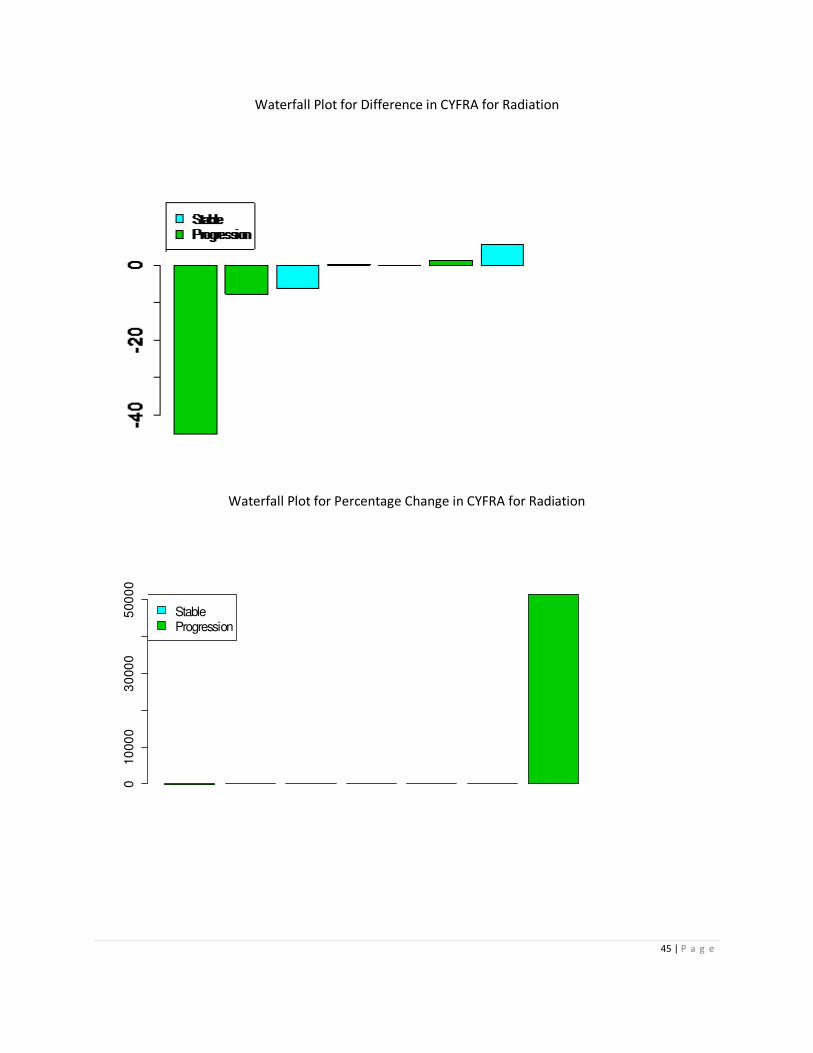
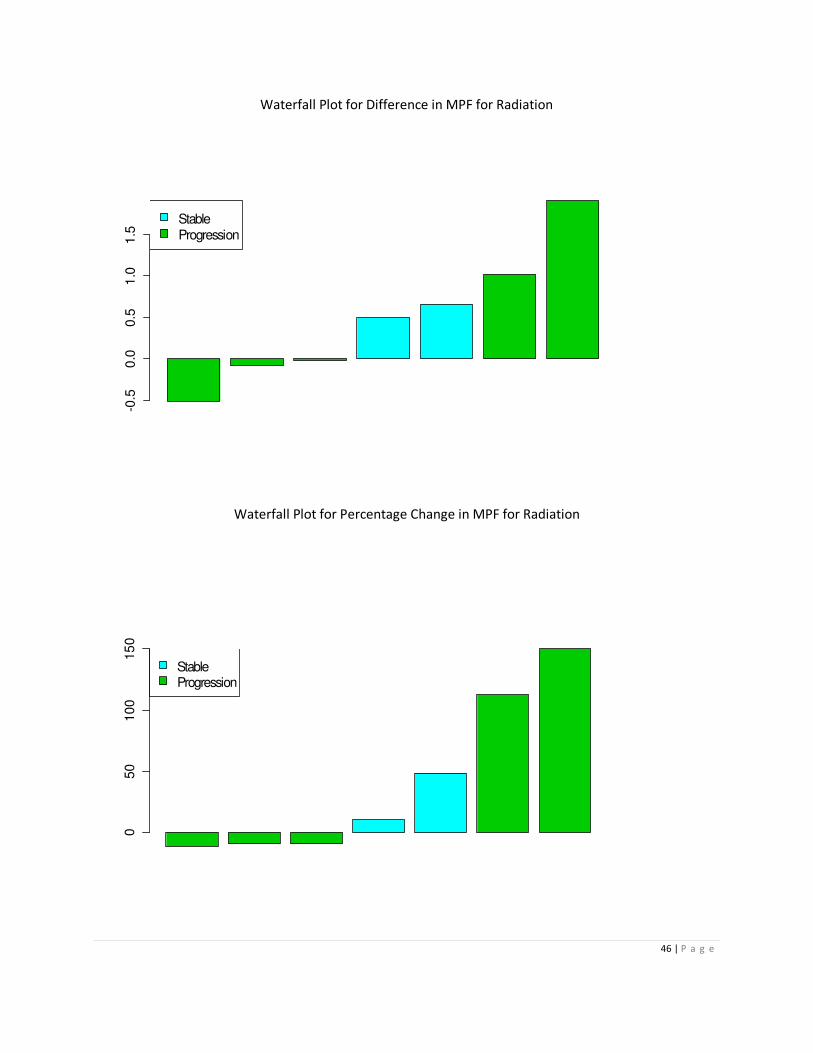
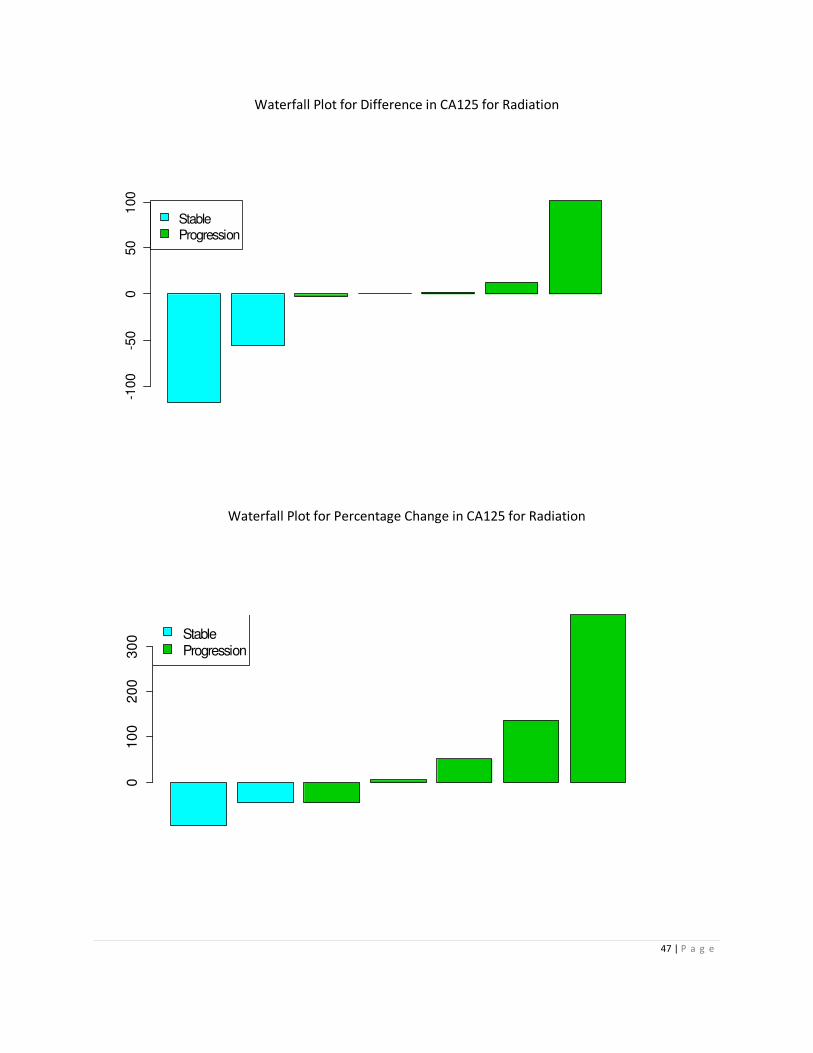
treatment group. There were only 7 patients in the radiation group, therefore analysis was
deemed unsuitable and only exploratory work such as box plots and waterfall plots were
14 | P a g e
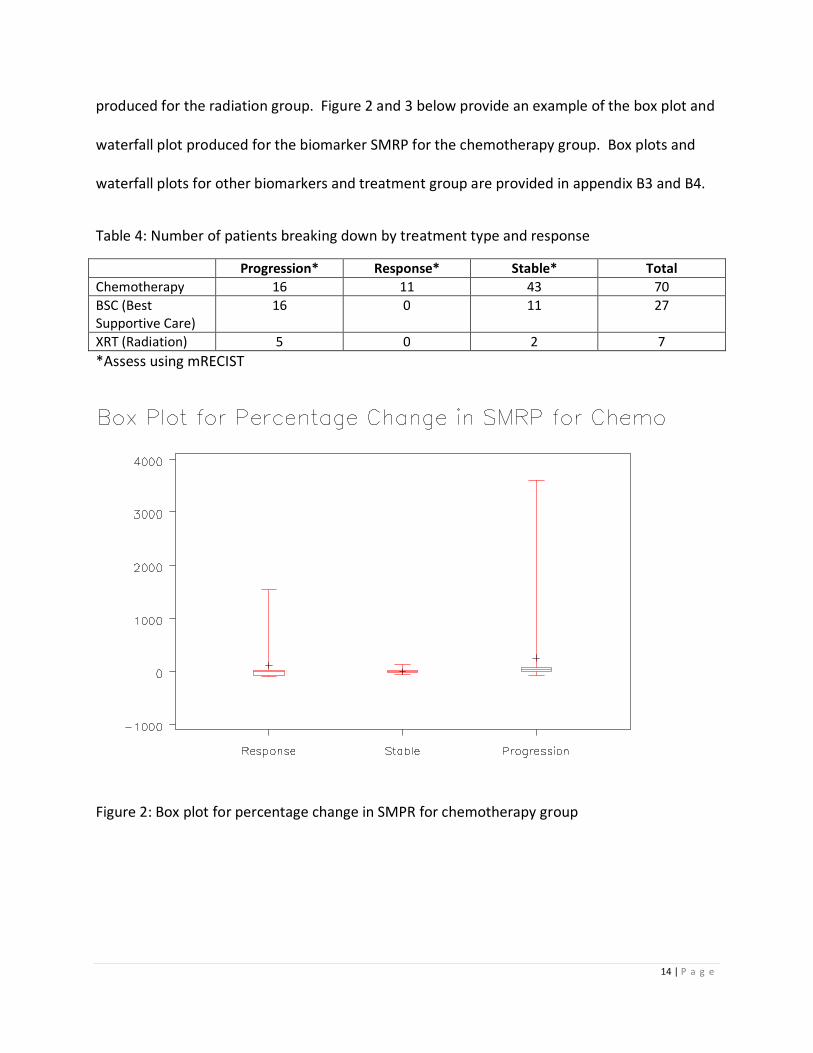
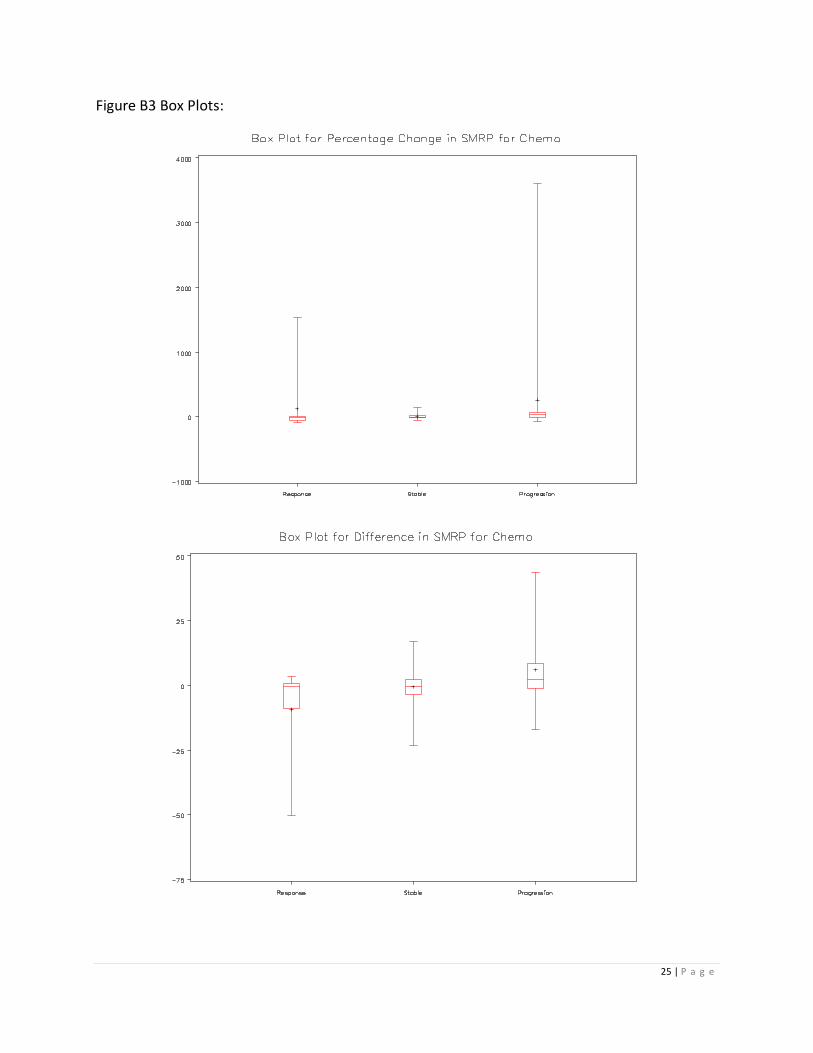
produced for the radiation group. Figure 2 and 3 below provide an example of the box plot and
waterfall plot produced for the biomarker SMRP for the chemotherapy group. Box plots and
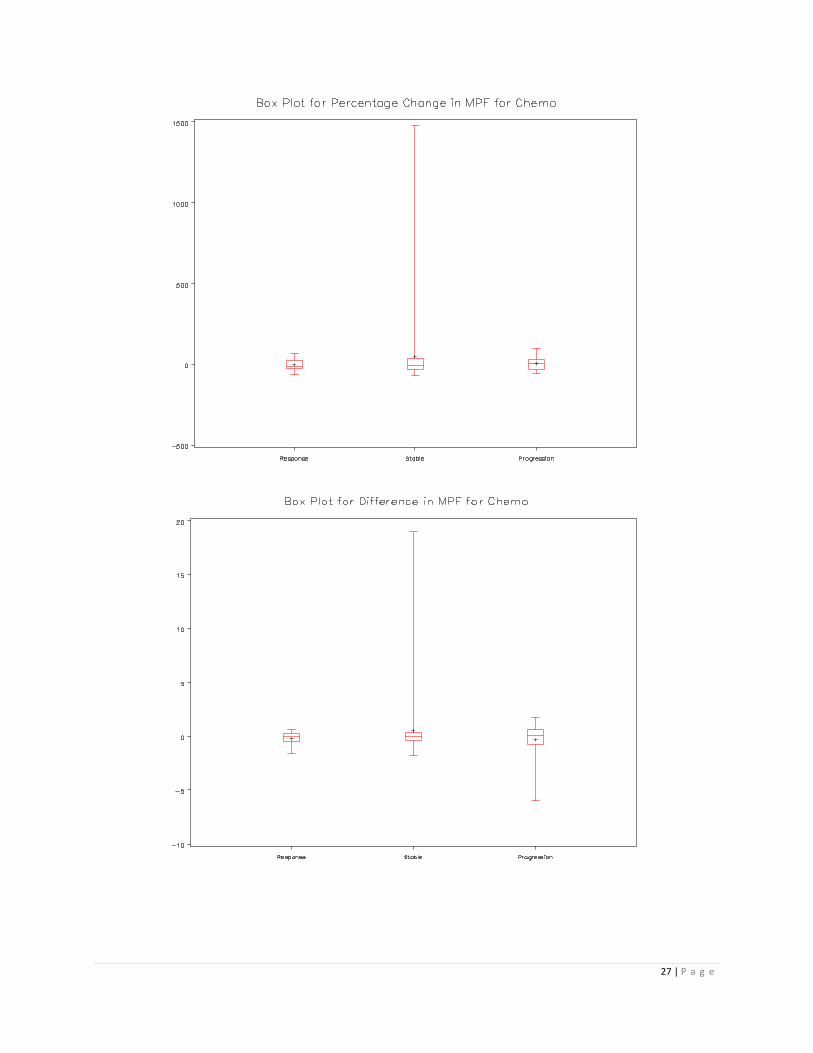
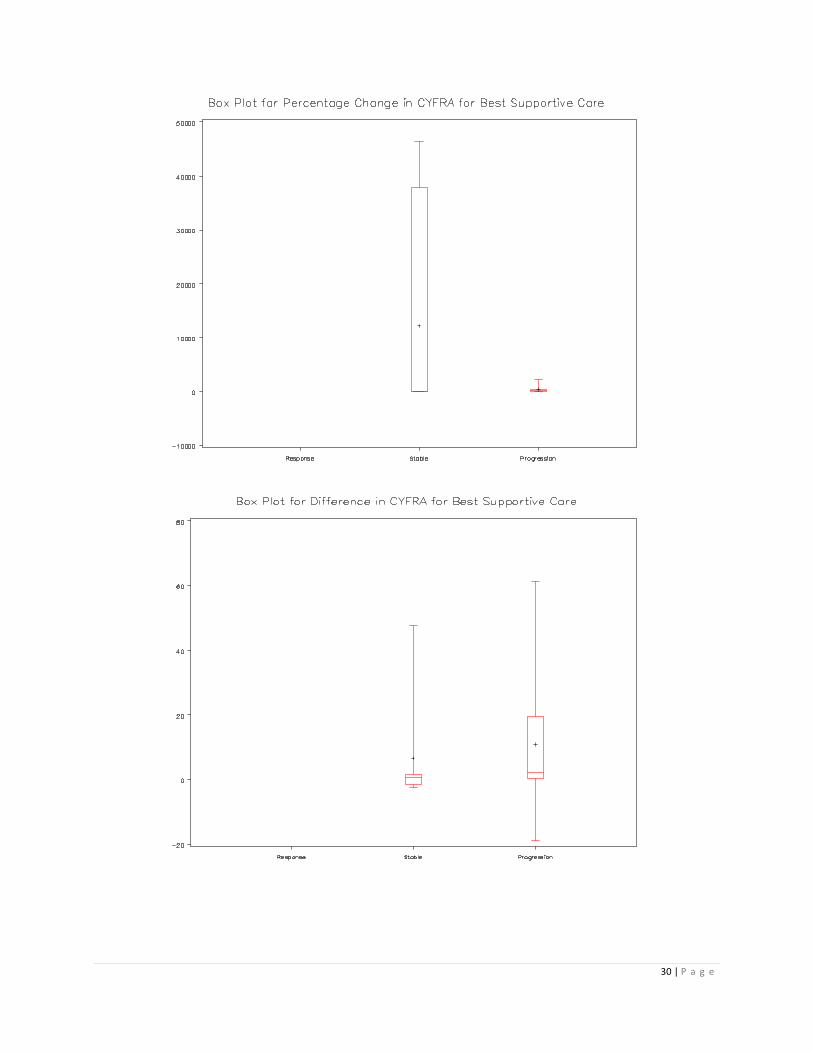
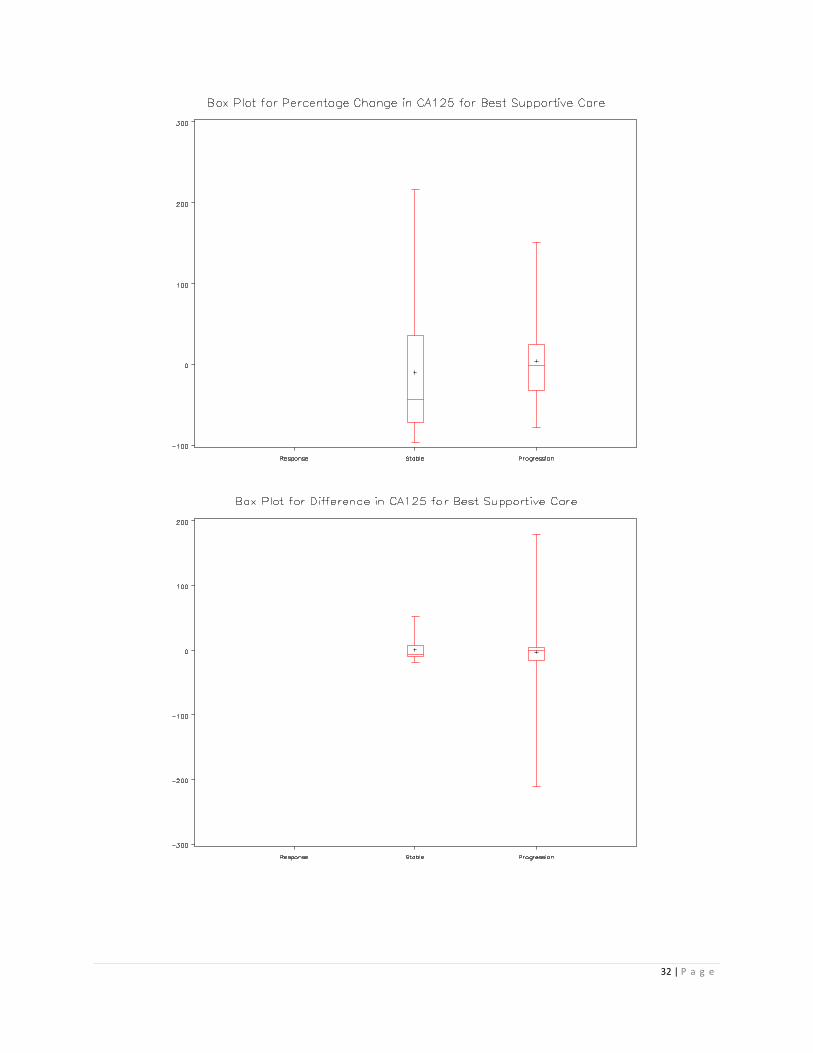
waterfall plots for other biomarkers and treatment group are provided in appendix B3 and B4.
Table 4: Number of patients breaking down by treatment type and response
N=104 Progression* Response* Stable* Total
Chemotherapy 16 11 43 70
BSC (Best
Supportive Care)
16 0 11 27
XRT (Radiation) 5 0 2 7
*Assess using mRECIST
Figure 2: Box plot for percentage change in SMPR for chemotherapy group

15 | P a g e
05
00
15
00
25
00
35
00
StableResponse
Progression
Figure 3: Waterfall plot for percentage change in SMPR for chemotherapy group
As one can observed in figure 2 and 3, there are some outliers for the percentage change and
the difference. Those outliers have been verified with the clinician to ensure data accuracy.
Non-parametric test such as Krustal-Wallis and Wilcoxin-Mann-Whitney were employed for the
analysis which utilizes the rank, transformation was not applied to data. Descriptive statistics of
the difference and percentage change of the four biomarkers are presented in table 5 for the
chemotherapy group and table 6 for the best supportive care group. The descriptive statistics
for the radiation group is provided in appendix A3.
16 | P a g e
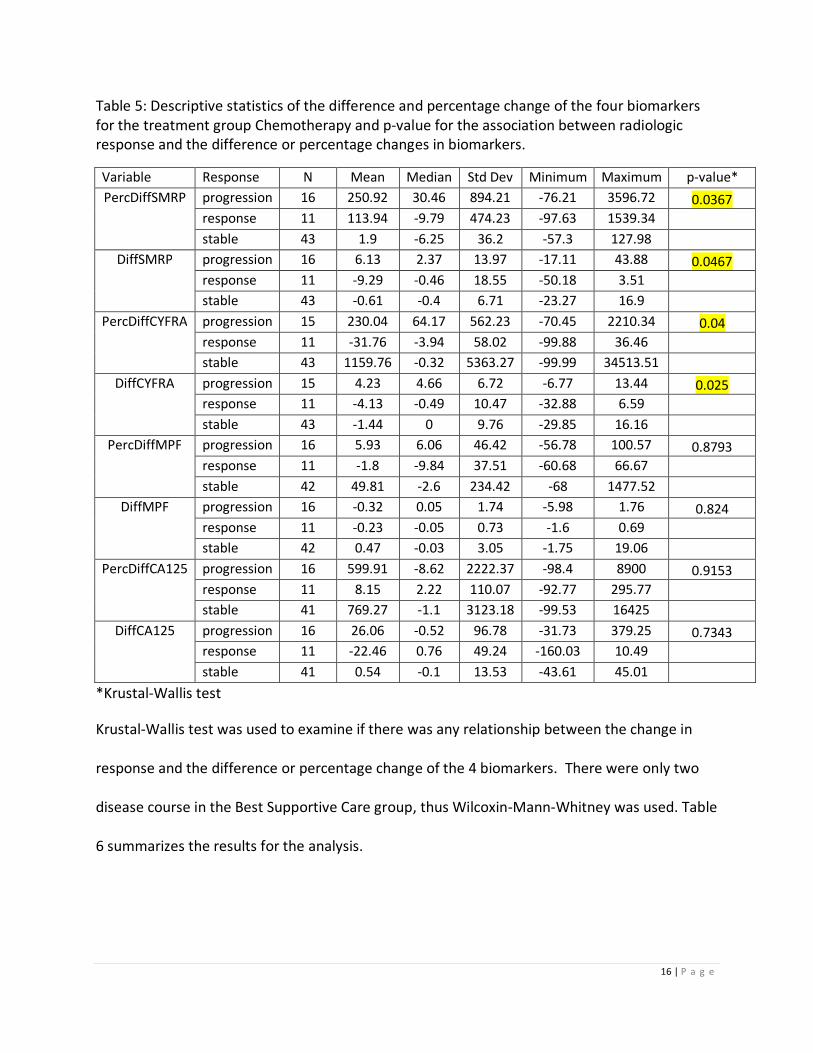
Table 5: Descriptive statistics of the difference and percentage change of the four biomarkers
for the treatment group Chemotherapy and p-value for the association between radiologic
response and the difference or percentage changes in biomarkers.
Variable Response N Mean Median Std Dev Minimum Maximum p-value*
PercDiffSMRP progression 16 250.92 30.46 894.21 -76.21 3596.72 0.0367
response 11 113.94 -9.79 474.23 -97.63 1539.34
stable 43 1.9 -6.25 36.2 -57.3 127.98
DiffSMRP progression 16 6.13 2.37 13.97 -17.11 43.88 0.0467
response 11 -9.29 -0.46 18.55 -50.18 3.51
stable 43 -0.61 -0.4 6.71 -23.27 16.9
PercDiffCYFRA progression 15 230.04 64.17 562.23 -70.45 2210.34 0.04
response 11 -31.76 -3.94 58.02 -99.88 36.46
stable 43 1159.76 -0.32 5363.27 -99.99 34513.51
DiffCYFRA progression 15 4.23 4.66 6.72 -6.77 13.44 0.025
response 11 -4.13 -0.49 10.47 -32.88 6.59
stable 43 -1.44 0 9.76 -29.85 16.16
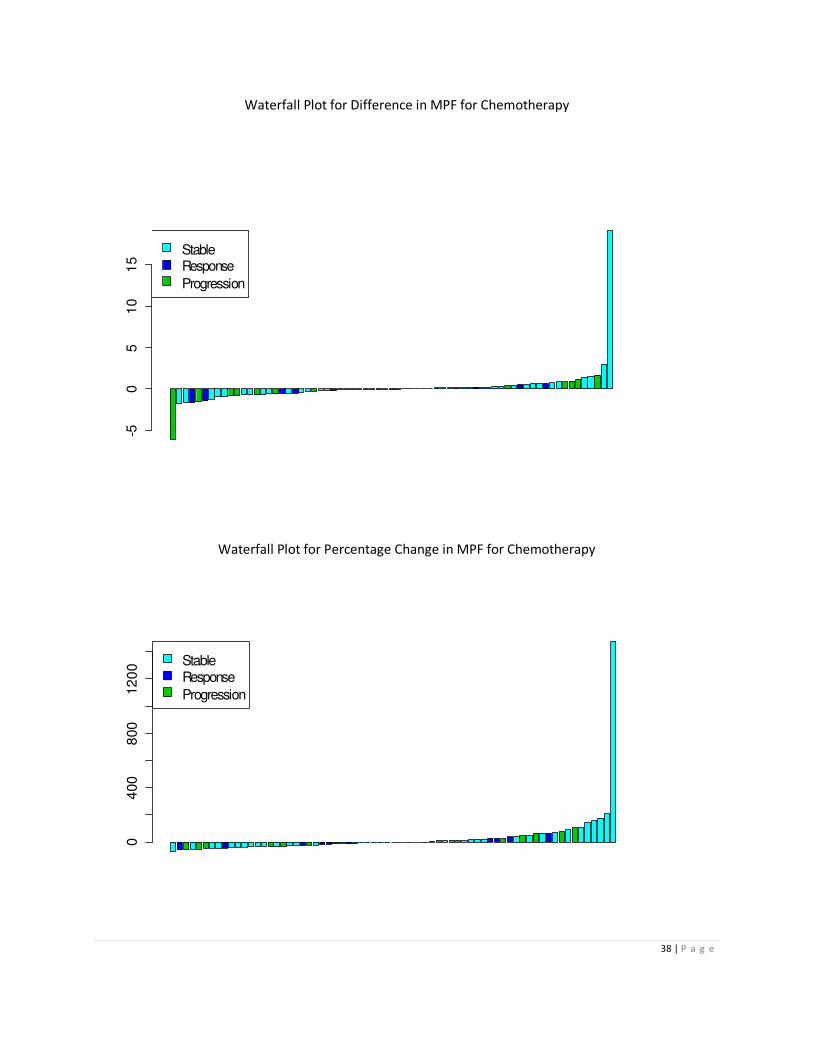
PercDiffMPF progression 16 5.93 6.06 46.42 -56.78 100.57 0.8793
response 11 -1.8 -9.84 37.51 -60.68 66.67
stable 42 49.81 -2.6 234.42 -68 1477.52
DiffMPF progression 16 -0.32 0.05 1.74 -5.98 1.76 0.824
response 11 -0.23 -0.05 0.73 -1.6 0.69
stable 42 0.47 -0.03 3.05 -1.75 19.06
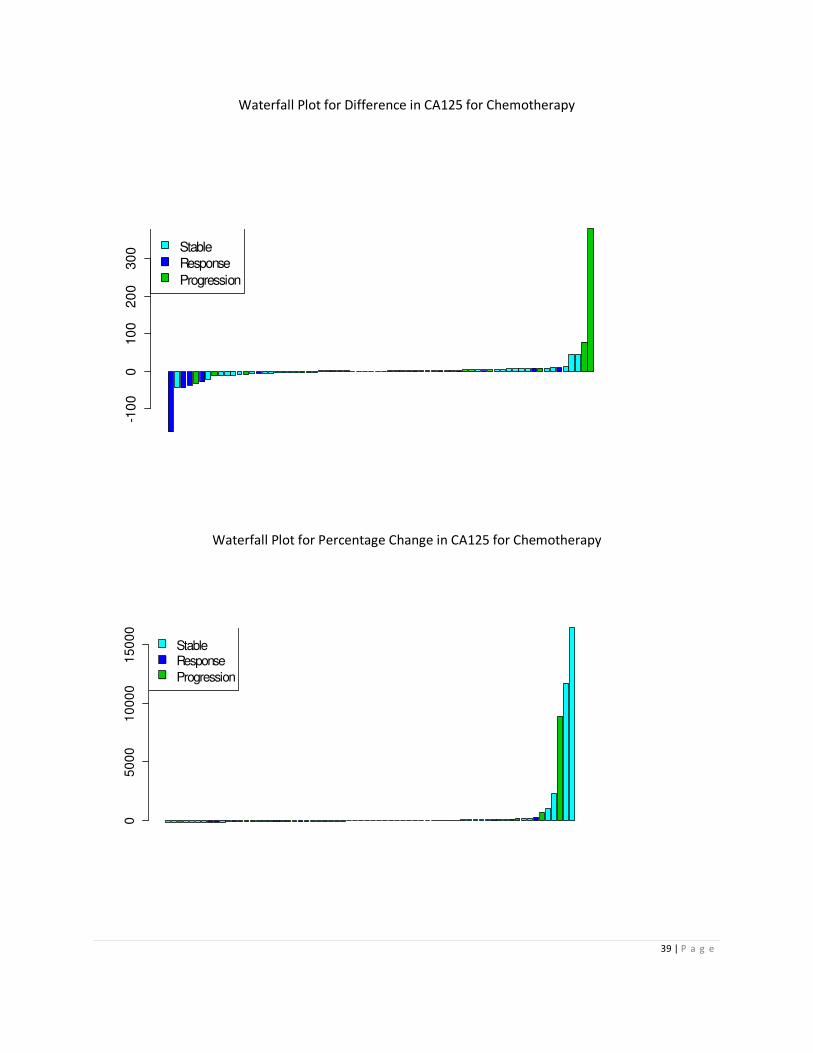
PercDiffCA125 progression 16 599.91 -8.62 2222.37 -98.4 8900 0.9153
response 11 8.15 2.22 110.07 -92.77 295.77
stable 41 769.27 -1.1 3123.18 -99.53 16425
DiffCA125 progression 16 26.06 -0.52 96.78 -31.73 379.25 0.7343
response 11 -22.46 0.76 49.24 -160.03 10.49
stable 41 0.54 -0.1 13.53 -43.61 45.01
*Krustal-Wallis test
Krustal-Wallis test was used to examine if there was any relationship between the change in
response and the difference or percentage change of the 4 biomarkers. There were only two
disease course in the Best Supportive Care group, thus Wilcoxin-Mann-Whitney was used. Table
6 summarizes the results for the analysis.

17 | P a g e
Table 6: Descriptive statistics of the difference and percentage change of the four biomarkers
for the treatment group Best Supportive Care and p-value for the association between
radiologic response and the difference or percentage changes in biomarkers.
Variable Response N Mean Median Std Dev Minimum Maximum p-value*
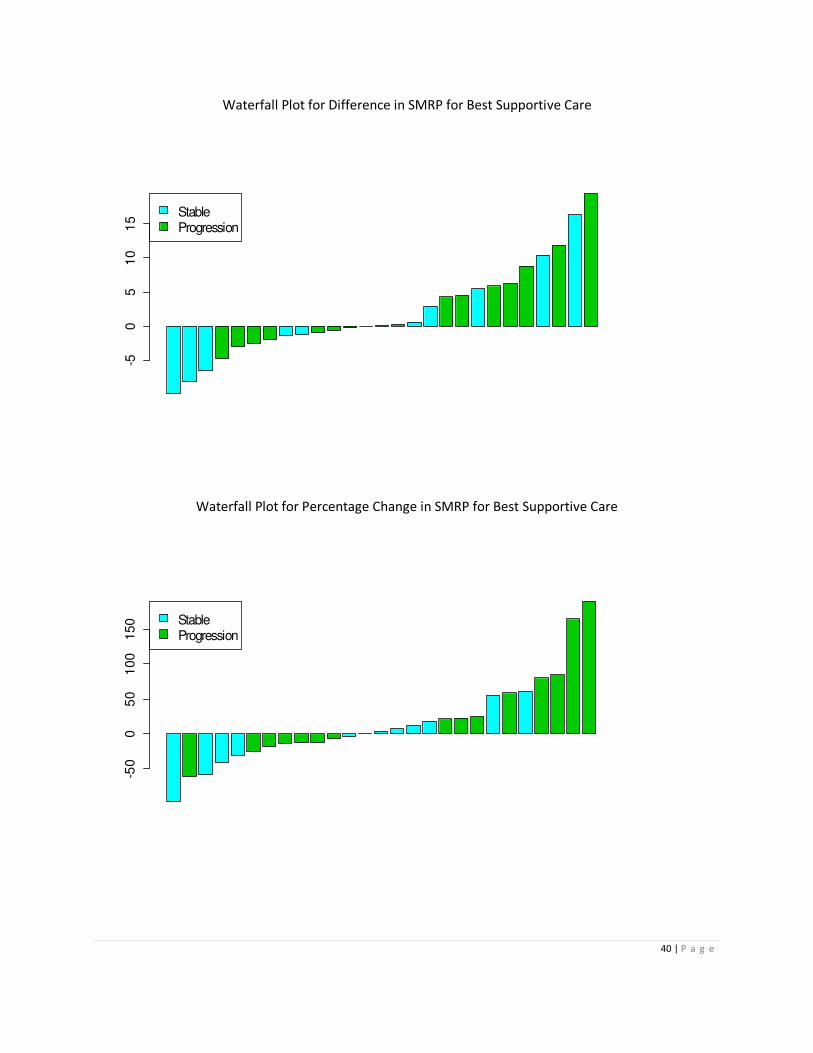
PercDiffSMRP progression 16 31.4 10.7 68.72 -59.88 189.17 0.2669
stable 11 -6.49 3.79 46.79 -95.41 60.48
DiffSMRP progression 16 2.97 0.16 6.37 -4.7 19.4 0.5053
stable 11 0.83 0.1 7.87 -9.8 16.42
PercDiffCYFRA progression 16 408.39 142.73 653.54 -92.24 2263.64 0.8243
stable 11 12206 46.15 19796.9 -82.58 46400
DiffCYFRA progression 16 10.86 1.97 21.71 -18.78 61.23 0.1748
stable 11 6.55 0.76 15.86 -2.6 47.72
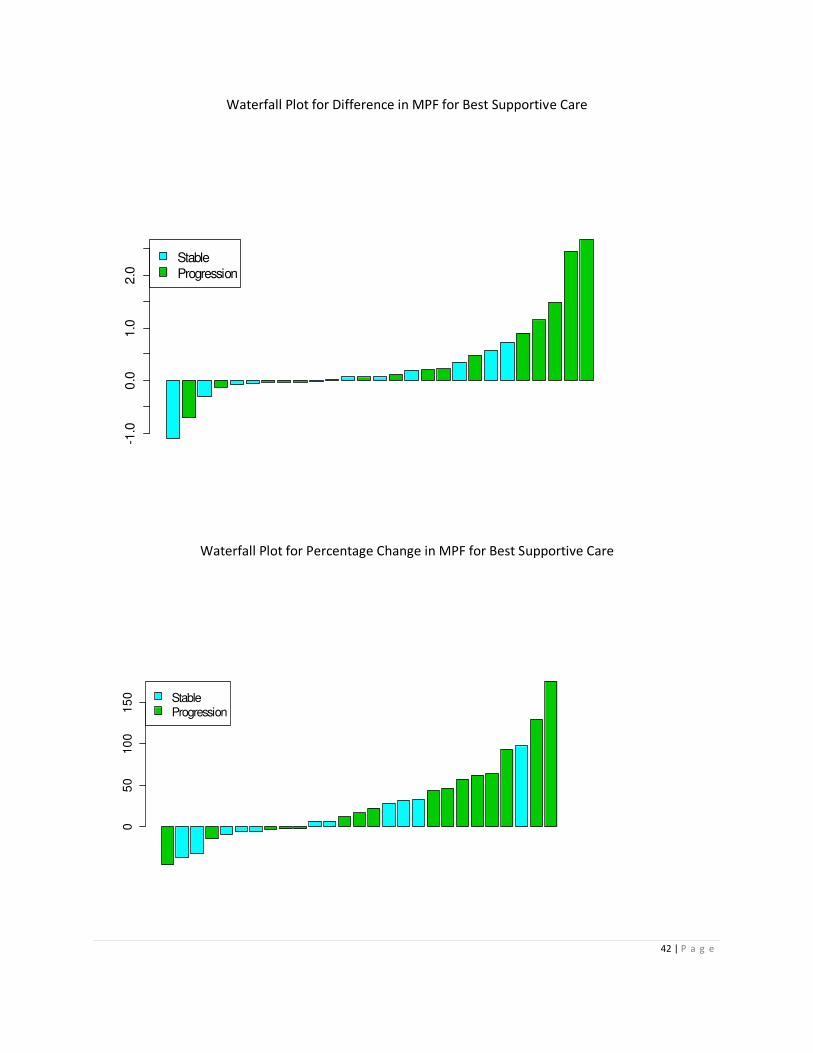
PercDiffMPF progression 16 41.01 33.17 56.89 -46.05 176.26 0.1201
stable 11 9.98 6.14 37.28 -36.82 97.3
DiffMPF progression 16 0.55 0.16 0.95 -0.7 2.67 0.2361
stable 11 0.04 0.06 0.48 -1.09 0.72
PercDiffCA125 progression 16 4.28 -1.45 54.92 -77.56 151.41 0.2083
stable 11 -9.62 -42.99 90.07 -96.08 217.43
DiffCA125 progression 16 -2.87 -0.18 74.98 -210.71 178.85 0.7113
stable 11 0.48 -6.74 19.31 -19.6 52.5
* Wilcoxon-Mann-Whitney
Spearman correlation was used to examine any relationship between the biomarkers.
Correlation was identified between SMPR and MPF in both chemotherapy (pre-treatment:
corr= 0.46, p-value: < 0.0001; post-treatment: corr=0.53, p-value: 0.0047) and Best Supportive
Care (pre-treatment: corr= 0.45, p-value: < 0.0001; post-treatment: corr=0.62, p-value: 0.0006).
Discussion
Previous large-scale radiologic screening studies with plain chest X-ray and CT scanning have
proved ineffective for detecting early stage MM among asbestos-exposed individuals.1 Future
prospects hinge on the identification and validation of effective biomarkers for the non-invasive
detection of MM, hoping to identify patients at an earlier, more treatable stage as well as
prolonging the survival of this deadly disease. In this study, four serum biomarkers were

18 | P a g e
examined, SMRP, CYFRA, CA125 and MPF, and their relationship with survival outcome and
radiological stage of the response. These 4 biomarkers have been identified by various studies
as potential candidates predictive of the tumor response. Seventy-three patients were
included in the survival analysis and the results in table 2 and 3 suggested that CYFRA is
predictive of survival outcome in both uni-variate and multi-variate analysis. This finding is
consistent with the study conducted by Bonfrer et al, which amongst the 52 MM patients that
were examined, CYFRA levels were highly correlated with survival analysis2.
In the analysis of association between the 4 serum biomarkers and the radiological stage of
response, an increase in the SMRP and CYFRA level seems to associate with the progression of
MM. The results coincide with earlier finding published by Robinson et al2 and Grigoriu et al3.
Both of the study findings concluded that increasing serum levels of SMRP and CYFRA were
associated with disease progression, whereas stable or decreasing values suggested response
to treatment. In addition, percentage change is a better measure than difference in pre and
post biomarkers value because the change in size of a tumor is best presented by percentage
change8.
Correlation was identified between SMRP and MPF, however the results have indicated that
SMRP is predictive of MM whereas MPF is not. This contradicts with the finding of the study
conducted by Tomasetti et al5, which showed both SMRP and MPF had equivalent diagnostic
performance.
There are several limitations to the study such as the usage of mRECIST as the assessing tool
for the radiologic response, the sample size and the retrospective nature of the study. mRECIST
is identified to be suitable because of its ability to measure the pleural tumor thickness

19 | P a g e
perpendicular to the chest wall. However this method has not been widely adopted and no
validation studies have been published to confirm the utility of this approach. MM is a rare
disease, recruiting a sufficient sample size is always difficult. Although many studies have
examined the predictive ability of the biomarkers, all of them are retrospective studies. At
present, there is no validation of these biomarkers in prospective trials. This is possibly related
to the latency of this disease, usually 20-50 years after the exposure to asbestos. Therefore, it
is difficult to prove the sensitivity and specificity of these biomarkers for adaption to the clinic.
Conclusion
Serum biomarker CYFRA is potentially a promising marker predictive of survival outcome and
tumor response in patients with MM. Biomarker SMRP is consistent with other literatures in its
association with response to treatment. A prospective study with larger sample is
recommended to validate the findings in this study and an alternative tool to assess the
response to treatment such as naked eye would confirm the suitability of mRECIST.
Identification of serum biomarkers that can be used clinically will not only benefit patients, but
would also save billions of dollars in compensation and treatment on patients with MM.
20 | P a g e
Reference
1Pass H and Carbone M. Current Status of Screening for Malignant Pleural Mesothelioma.
Semin Thorac Cardiovasc Surg 21:97-104. 2009
2Bonfrer JM, Schouwink JH, Korse CM, et al: 21-1 and TPA as markers in MM. Anticancer Res
17:2971-2973, 1997
3Robinson BW, Creaney J, Lake R, et al. Mesothelin-family proteins and diagnosis of
mesothelioma. Lancet 362:1612-1616, 2003
4 Grigoriu BD, Chahine B, Scherpereel A. Kinetics of soluble mesothelin in patients with
malignant pleural mesothelioma during treatment. Am J Respir Crit Care Med 179(10):950-954,
2009
5 Tomasetti M, Santarelli L et al. Biomarkers for Early Detection of Malignant Mesothelioma:
Diagnostic and Therapeutic Application. Cancers 2010, 2, 523-548. 2010
6 Canadian Medical Association or its licensors. Canadian cancer statistics at a glance:
mesothelioma. CMAJ 677-678. 2008
7 Wheatley-Price P, Xu W, Liu G et al. Soluble mesothelin-related peptide and osteopontin as
markers of response in malignant mesothelioma. Journal of Clinical Oncology V28:3316-3322,
2010
8 De Cupis A, Pirani P, Favoni R. Establishment and preliminary characterization of human
malignant mesothelioma cell lines. Monaldi Arch Chest Dis 53:188-192, 1998

21 | P a g e
Appendices
A. Tables
The interactions below were not significant, thus the interaction terms were removed and the
final model was presented in table 3.
Table A1: Multi-variate model on overall survival including the interactive terms
Parameter Estimate SE P-value
PLATELET 1.076 0.458 0.0189
Surgery -1.431 0.494 0.0038
CYFRA_result_1 0.038 0.021 0.0664
CYFRA_result*PLATELET 0.010 0.026 0.7058
CYFRA_result*Surgery -0.005 0.042 0.9114
The interaction terms with log of time were added in the model to verify the proportional
hazard assumption. None of the interaction term was significant, thus they were removed and
the final model was presented in table 3.
Table A2:Multi-variate model on overall survival including the interaction terms with logT
Parameter Estimate SE P-value
PLATELET 1.25 2.41 0.6021
Surgery -8.12 5.22 0.1195
CYFRA_result_1 -0.12 0.04 0.6963
LogT*PLATELET -0.05 0.42 0.9014
LogT*Surgery 1.10 0.94 0.1892
LogT*CYFRA_result_1 0.01 0.01 0.2079
22 | P a g e
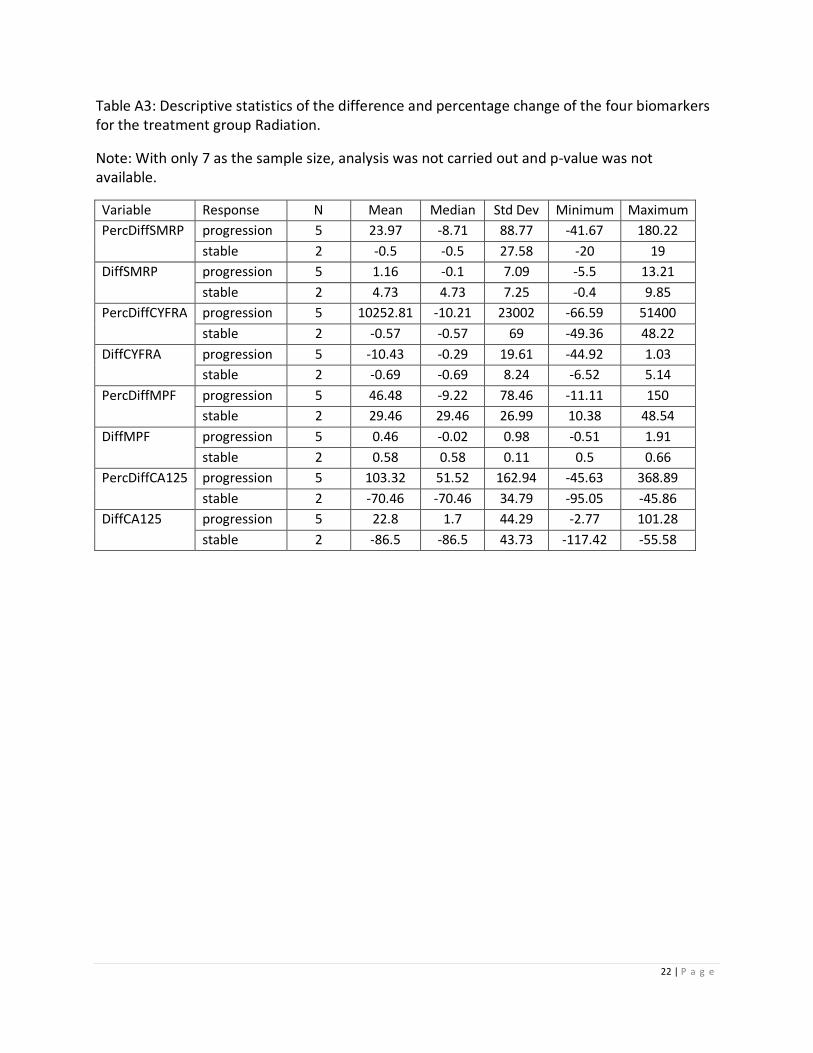
Table A3: Descriptive statistics of the difference and percentage change of the four biomarkers
for the treatment group Radiation.
Note: With only 7 as the sample size, analysis was not carried out and p-value was not
available.
Variable Response N Mean Median Std Dev Minimum Maximum
PercDiffSMRP progression 5 23.97 -8.71 88.77 -41.67 180.22
stable 2 -0.5 -0.5 27.58 -20 19
DiffSMRP progression 5 1.16 -0.1 7.09 -5.5 13.21
stable 2 4.73 4.73 7.25 -0.4 9.85
PercDiffCYFRA progression 5 10252.81 -10.21 23002 -66.59 51400
stable 2 -0.57 -0.57 69 -49.36 48.22
DiffCYFRA progression 5 -10.43 -0.29 19.61 -44.92 1.03
stable 2 -0.69 -0.69 8.24 -6.52 5.14
PercDiffMPF progression 5 46.48 -9.22 78.46 -11.11 150
stable 2 29.46 29.46 26.99 10.38 48.54
DiffMPF progression 5 0.46 -0.02 0.98 -0.51 1.91
stable 2 0.58 0.58 0.11 0.5 0.66
PercDiffCA125 progression 5 103.32 51.52 162.94 -45.63 368.89
stable 2 -70.46 -70.46 34.79 -95.05 -45.86
DiffCA125 progression 5 22.8 1.7 44.29 -2.77 101.28
stable 2 -86.5 -86.5 43.73 -117.42 -55.58

23 | P a g e
B. Figures
The deviance plot and martingale plots were used to assess the goodness-of-fit. Based on the
figures, deviance and martingale residual were bounded between [-1,1], the multi-variate
model was a good fit to the data.
Devi ance Resi dual
-2
-1
0
1
2
3
Li near Predi ct or
-2 -1 0 1 2 3 4 5 6
Figure B1: Deviance Plot

24 | P a g e
Mart i ngal e Resi dual
-3
-2
-1
0
1
Li near Predi ct or
-2 -1 0 1 2 3 4 5 6
Figure B2: Martingale residual
25 | P a g e
Figure B3 Box Plots:

26 | P a g e
27 | P a g e

28 | P a g e

29 | P a g e
30 | P a g e

31 | P a g e
32 | P a g e
33 | P a g e

34 | P a g e
35 | P a g e
36 | P a g e
Figure B4: Waterfall Plots
Waterfall Plot for Difference in SMPR for Chemotherapy -4
0-2
00
20
40
StableResponse
Progression
Waterfall Plot for Percentage Change in SMPR for Chemotherapy
05
00
15
00
25
00
35
00
StableResponse
Progression
37 | P a g e
Waterfall Plot for Difference in CYFRA for Chemotherapy -3
0-2
0-1
00
10 Stable
Response
Progression
Waterfall Plot for Percentage Change in CYFRA for Chemotherapy
01
00
00
20
00
03
00
00
StableResponse
Progression
38 | P a g e
Waterfall Plot for Difference in MPF for Chemotherapy
-5
05
10
15
StableResponse
Progression
Waterfall Plot for Percentage Change in MPF for Chemotherapy
04
00
800
12
00 Stable
Response
Progression
39 | P a g e
Waterfall Plot for Difference in CA125 for Chemotherapy
-1
00
010
02
00
30
0 Stable
Response
Progression
Waterfall Plot for Percentage Change in CA125 for Chemotherapy
05
00
01
00
00
15
00
0
StableResponse
Progression
40 | P a g e
Waterfall Plot for Difference in SMRP for Best Supportive Care
-50
51
01
5
StableProgression
Waterfall Plot for Percentage Change in SMRP for Best Supportive Care
-50
05
01
00
150 Stable
Progression

41 | P a g e
Waterfall Plot for Difference in CYFRA for Best Supportive Care
020
40
60
StableProgression
Waterfall Plot for Percentage Change in CYFRA for Best Supportive Care
010
00
03
00
00
StableProgression
42 | P a g e
Waterfall Plot for Difference in MPF for Best Supportive Care
-1
.00
.01
.02
.0
Stable
Progression
Waterfall Plot for Percentage Change in MPF for Best Supportive Care
05
010
01
50 Stable
Progression

43 | P a g e
Waterfall Plot for Difference in CA125 for Best Supportive Care
-20
0-1
00
01
00
StableProgression
Waterfall Plot for Percentage Change in Ca125 for Best Supportive Care
-50
05
01
00
20
0
StableProgression
44 | P a g e
Waterfall Plot for Difference in SMRP for Radiation
-50
510
StableProgression
Waterfall Plot for Percentage Change in SMRP for Radiation
05
010
01
50 Stable
Progression
45 | P a g e
Waterfall Plot for Difference in CYFRA for Radiation
Waterfall Plot for Percentage Change in CYFRA for Radiation
010
00
03
000
05
00
00
StableProgression
46 | P a g e
Waterfall Plot for Difference in MPF for Radiation
-0.5
0.0
0.5
1.0
1.5
StableProgression
Waterfall Plot for Percentage Change in MPF for Radiation
050
100
15
0
StableProgression
47 | P a g e
Waterfall Plot for Difference in CA125 for Radiation
-100
-50
050
100
StableProgression
Waterfall Plot for Percentage Change in CA125 for Radiation
01
00
20
03
00 Stable
Progression

48 | P a g e
SAS codes
libname m 'C:\Desktop\Geof Project';
/*Data preparation for overall survival*/
/*obtain the date of diagnosis and vital status*/
proc sort data = m.diagnosis out = dia (keep=study_no Date_of_Diagnosis); by study_no; run;
proc sort data = m.vital out = death (keep=study_no Date_of_Death If_Alive_date_last_seen);
by study_no; run;
data surv_date; merge dia death; by study_no; run;
/*calculate follow up day and assign censor info*/
data surv_date; set surv_date;
if not missing(Date_of_Death) then do;
os_cen =1;
os_day = (Date_of_Death - Date_of_Diagnosis) + 1;
end;
else if not missing(If_Alive_date_last_seen) then do;
os_cen = 0;
os_day = (If_Alive_date_last_seen - Date_of_Diagnosis) + 1;
end;
run;
*check how many patients with both pre/post and their vital;
PROC SORT DATA = m.ct_response (where=(prognosis = 'TRUE')) out=prognosis ; BY STUDY_NO
blood_1_date; RUN;
DATA PROGNOSIS; MERGE PROGNOSIS (IN=A) SURV_DATE(IN=B); BY STUDY_NO; IF A; RUN;
/*obtain baseline covariates*/
proc sort data = prognosis; by study_no; run;
proc sort data = m.pt_info out = pt_info; by study_no; run;
data prognosis; merge prognosis(in=a) pt_info(in=b); by study_no; if a; run;
/*calculate age of diagnosis*/
data prognosis; set prognosis;
age = (Date_of_Diagnosis - DOB)/365.25; run;
/*stage*/
proc sort data = m.stage out = stage; by study_no; run;
49 | P a g e
data prognosis; merge prognosis (in=a) stage (in=b); by study_no; if a; run;
/*histopath subtype*/
proc sort data = m.diagnosis out = diagnosis(keep=study_no Histopath_subtype); by study_no;
run;
data prognosis; merge prognosis (in=a) diagnosis (in=b); by study_no; if a; run;
/*surgery*/
proc sort data = m.surg out = surg(rename=(pid=study_no)); by pid; run;
data prognosis; merge prognosis (in=a) surg (in=b); by study_no; if a; run;
/*symptom*/
proc sort data = m.baseline_symptom out = baseline_symptom; by study_no; run;
data prognosis; merge prognosis (in=a) baseline_symptom (in=b); by study_no; if a; run;
/*chemo*/
proc sort data = m.chemo out = chemo (keep=study_no) nodupkey; by study_no; run;
data chemo; set chemo;
chemo = 'Yes'; run;
data prognosis; merge prognosis (in=a) chemo (in=b); by study_no; if a; run;
/*Platelet, Hemoglobin, White cell count*/
proc sort data = m.baseline_bloodtests out = baseline_bloodtests(keep=study_no WCC
Haemoglobin Platelet); by study_no; run;
data prognosis; merge prognosis (in=a) baseline_bloodtests (in=b); by study_no; if a; run;
/*grouping*/
proc format;
value ecog 0 = '0' 1 = '1/2/3';
value imig 1 = '1/2' 2 = '2' 3='3';
value smoke 0 = 'never' 1 = 'former' 2 = 'current';
run;
data prognosis; set prognosis;
if ecog = 0 then ecog_new = 0;
else if ecog > 0 then ecog_new = 1;
format ecog_new ecog.;
if imig_stage in (1,2) then imig_stage_new = 1;
else imig_stage_new = imig_stage;
format imig_stage_new imig.;
if Smoking_Status in ('Former (>1 yr)' 'Former (>1 yr) Pack years-' 'former (>1 yr)') then
smoking_status_new = 1;
else if smoking_status = 'Never' then smoking_status_new = 0;
else if smoking_status = 'Current' then smoking_status_new = 2;
50 | P a g e
format smoking_status_new smoke.;
run;
data m.prognosis; set prognosis; run;
/*Descriptive Statistics*/
ODS CSV FILE='C:\Desktop\TEMP.CSV';
proc freq data = prognosis;
table os_cen gender IMIG_Stage IMIG_Stage_new morethanonethird Histopath_subtype
Surgery Chest_Pain Weight_Loss ECOG ECOG_new Smoking_Status Smoking_Status_new
chemo WCC PLATELET HAEMOGLOBIN; run;
proc means data = prognosis n mean median std min max maxdec =2;
var os_day SMRP_result_1 CYFRA_result_1 MPF_result_1 CA125_result_1 age ; run;
proc corr data = prognosis spearman;
var SMRP_result_1 CYFRA_result_1 MPF_result_1 CA125_result_1; run;
ods csv close;
/*Survival*/
ODS CSV FILE='C:\Desktop\TEMP1.CSV';
data km; set m.prognosis;
os_yr = os_day/365.25;run;
proc lifetest data = km plots=(s);
time os_yr*os_cen(0);
run;
*continuous variables;
%macro os(var);
proc phreg data = prognosis;
model os_day*os_cen(0) = &var/risklimits; run;
%mend;
*categorical variables;
%macro os_cat(var, refvar);
proc tphreg data = prognosis;
class &var/REF=first;
model os_day*os_cen(0) = &var/risklimits; run;
%mend;
51 | P a g e
%os(SMRP_result_1);
%os(CYFRA_result_1);
%os(MPF_result_1);
%os(CA125_result_1);
%os(age);
%os_cat(gender);
%os_cat(IMIG_Stage_new);
%os_cat(morethanonethird);
%os_cat(Histopath_subtype);
%os_cat(Surgery);
%os_cat(Chest_Pain);
%os_cat(Weight_Loss);
%os_cat(ECOG_new);
%os_cat(Smoking_Status_new);
%os_cat(chemo);
%os_cat(WCC);
%os_cat(PLATELET);
%os_cat(HAEMOGLOBIN);
ods csv close;
ODS CSV FILE='C:\ Desktop\TEMP2.CSV';
*Multi-variate model;
proc tphreg data = prognosis;
class PLATELET Surgery /REF=first;
model os_day*os_cen(0) = PLATELET Surgery CYFRA_result_1/risklimits; run;
*interaction;
proc tphreg data = prognosis;
class PLATELET Surgery /REF=first;
model os_day*os_cen(0) = PLATELET Surgery CYFRA_result_1 Platelet*CYFRA_result_1
Surgery*CYFRA_result_1/risklimits; run;
*Goodness-of-fit – martingale and deviance plot;
PROC TPHREG DATA=PROGNOSIS NOPRINT;
class PLATELET Surgery/REF=first;
MODEL os_day*os_cen(0)= PLATELET Surgery CYFRA_result_1/RL ;
OUTPUT OUT=RESOUT XBETA=XB RESMART=MART RESDEV=DEV;
RUN;
SYMBOL COLOR=BLUE VALUE=DOT HEIGHT=1.0;
PROC GPLOT DATA=RESOUT;
52 | P a g e
PLOT MART*XB;
RUN;
PROC GPLOT DATA=RESOUT;
PLOT DEV*XB;
RUN; QUIT;
ods csv close;
/*Analysis on tumor response and change in biomarker value*/
*number of patients;
proc sql;
select count (distinct Study_no) from m.pt_info; quit;
*data checking;
data ct_response; set m.ct_response;
if Study_no = 116 and blood_1_date = '01MAY2010'd then blood_1_date = '01MAY2007'd;
*switch the two records;
if Study_no = 85 and blood_1_date = '06APR2010'd and blood_2_date = '10FEB2010'd then do;
blood_1_date = '10FEB2010'd;
SMRP_result_1 = 1.5;
CYFRA_result_1 = 10.76;
MPF_result_1 = 1.15;
CA125_result_1 = 2.9;
blood_2_date = '06APR2010'd;
SMRP_result_2 = 1.3;
CYFRA_result_2 = 0.36;
MPF_result_2 = 1.18;
CA125_result_2 = 8.56;
end;
run;
data ct_response; set ct_response;
if Study_no = 5 and blood_1_date = . and blood_2_date = '13NOV2009'd then tracking =
'FALSE'; run;
Data ct_response;
Set ct_response (rename =(
Study_no = PID
blood_1_date = Test1
blood_2_date = Test2
Overall_Response_of_CT = Response
SMRP_result_1 = PreSMRP

53 | P a g e
SMRP_result_2 = PostSMRP
CYFRA_result_1 = PreCYFRA
CYFRA_result_2 = PostCYFRA
MPF_result_1 = PreMPF
MPF_result_2 = PostMPF
CA125_result_1 = PreCA125
CA125_result_2 = PostCA125));
where tracking = 'TRUE';
RUN;
/*calculate difference or percentage change*/
Data ct_response_tracking; Set ct_response (drop=POST_CYFRA_NEW PRE_CYFRA_NEW);
Length response_new $20;
if response in ('Complete Response' 'Partial Response') then response_new = 'response';
else if response = 'Progressive Disease' then response_new = 'progression';
else if response = 'Stable Disease' then response_new = 'stable';
if (PreSMRP ne . and PostSMRP ne .) then do; DiffSMRP = PostSMRP - PreSMRP; PercDiffSMRP =
100*(PostSMRP - PreSMRP)/PreSMRP; end;
if (PreCYFRA ne . and PostCYFRA ne .) then do; DiffCYFRA = PostCYFRA - PreCYFRA;
PercDiffCYFRA = 100*(PostCYFRA - PreCYFRA)/PreCYFRA; end;
if (PreMPF ne . and PostMPF ne .) then do; DiffMPF = PostMPF - PreMPF; PercDiffMPF =
100*(PostMPF - PreMPF)/PreMPF; end;
if (PreCA125 ne . and PostCA125 ne .) then do; DiffCA125 = PostCA125 - PreCA125;
PercDiffCA125 = 100*(PostCA125 - PreCA125)/PreCA125; end;
Run;
/*108 RECORD WHERE TRACKING IS TRUE*/
*NOW UPDATE WHETHER IS CHEM/SURGERY OR BEST SUPPORTIVE CARE
*use the file that Sinead generate for the different category;
PROC SORT DATA = ct_response_tracking; BY PID TEST1 TEST2; RUN;
PROC SORT DATA = M.TX_RECEIVED OUT = TX_RECEIVED; BY PID TEST1 TEST2; RUN;
DATA M.ct_response_tracking; MERGE ct_response_tracking TX_RECEIVED; BY PID TEST1
TEST2; RUN;
proc corr data = M.ct_response_tracking spearman;
54 | P a g e
where chemo = 'Yes';
var preSMRP preCYFRA preMPF preCA125; run;
proc corr data = M.ct_response_tracking spearman;
where bsc = 'Yes';
var preSMRP preCYFRA preMPF preCA125; run;
proc corr data = M.ct_response_tracking spearman;
where chemo = 'Yes';
var postSMRP postCYFRA postMPF postCA125; run;
proc corr data = M.ct_response_tracking spearman;
where bsc = 'Yes';
var postSMRP postCYFRA postMPF postCA125; run;
*descritpive statistics;
proc freq data = m.ct_response_tracking;
table (chemo bsc xrt)*response_new; run;
*boxplot;
proc format;
value resp 1 = 'Response' 2 = 'Stable' 3 = 'Progression'; run;
data boxplotdata; set m.ct_response_tracking;
if response_new = 'progression' then response_new_num = 3;
if response_new = 'stable' then response_new_num = 2;
if response_new = 'response' then response_new_num = 1;
format response_new_num resp.;
run;
proc sort data = boxplotdata; by response_new_num; run;
goptions reset = all ftext=simplex;
options pageno=1 center;
options orientation=portrait nodate nonumber;
ods rtf file = 'C:\ Desktop\graph.rtf';
ods graphics on;
%macro plot_box(title_name,categ,var1);
axis1 label=("");
axis2 label=("") order=(1 to 3 by 1) ;
title "Box Plot for &title_name";
proc boxplot data= boxplotdata;

55 | P a g e
where &categ = 'Yes';
plot &var1*response_new_num/vaxis = axis1 haxis=axis2;
run;
%mend;
%plot_box(Percentage Change in SMRP for Chemo, chemo, PercDiffSMRP);
%plot_box(Difference in SMRP for Chemo, chemo, DiffSMRP);
%plot_box(Percentage Change in CYFRA for Chemo, chemo, PercDiffCYFRA);
%plot_box(Difference in CYFRA for Chemo, chemo, DiffCYFRA);
%plot_box(Percentage Change in MPF for Chemo, chemo, PercDiffMPF);
%plot_box(Difference in MPF for Chemo, chemo, DiffMPF);
%plot_box(Percentage Change in CA125 for Chemo, chemo, PercDiffCA125);
%plot_box(Difference in CA125 for Chemo, chemo, DiffCA125);
%plot_box(Percentage Change in SMRP for Best Supportive Care, BSC, PercDiffSMRP);
%plot_box(Difference in SMRP for Best Supportive Care, BSC, DiffSMRP);
%plot_box(Percentage Change in CYFRA for Best Supportive Care, BSC, PercDiffCYFRA);
%plot_box(Difference in CYFRA for Best Supportive Care, BSC, DiffCYFRA);
%plot_box(Percentage Change in MPF for Best Supportive Care, BSC, PercDiffMPF);
%plot_box(Difference in MPF for Best Supportive Care, BSC, DiffMPF);
%plot_box(Percentage Change in CA125 for Best Supportive Care, BSC, PercDiffCA125);
%plot_box(Difference in CA125 for Best Supportive Care, BSC, DiffCA125);
%plot_box(Percentage Change in SMRP for XRT, XRT, PercDiffXRT);
%plot_box(Difference in SMRP for XRT, XRT, DiffXRT);
%plot_box(Percentage Change in CYFRA for XRT, XRT, PercDiffCYFRA);
%plot_box(Difference in CYFRA for XRT, XRT, DiffCYFRA);
%plot_box(Percentage Change in MPF for XRT, XRT, PercDiffMPF);
%plot_box(Difference in MPF for XRT, XRT, DiffMPF);
%plot_box(Percentage Change in CA125 for XRT, XRT, PercDiffCA125);
%plot_box(Difference in CA125 for XRT, XRT, DiffCA125);
ods graphics off;
ods rtf close;
*Krustal-Wallis or Mann-Whiteney;
ODS CSV FILE='C:\Desktop\TEMP3.CSV';
Proc Npar1way data = m.ct_response_tracking Wilcoxon;
Class response_new;
Var PercDiffSMRP DiffSMRP PercDiffCYFRA DiffCYFRA PercDiffMPF DiffMPF PercDiffCA125
DiffCA125;
Where Chemo = "Yes";
Run;

56 | P a g e
Proc Npar1way data = m.ct_response_tracking Wilcoxon;
Class response_new;
Var PercDiffSMRP DiffSMRP PercDiffCYFRA DiffCYFRA PercDiffMPF DiffMPF PercDiffCA125
DiffCA125;
Where BSC = "Yes";
Run;
Proc Npar1way data = m.ct_response_tracking Wilcoxon;
Class response_new;
Var PercDiffSMRP DiffSMRP PercDiffCYFRA DiffCYFRA PercDiffMPF DiffMPF PercDiffCA125
DiffCA125;
Where XRT = "Yes";
Run;
ods csv close;
*descriptive statistics;
ODS CSV FILE='C:\Desktop\TEMP4.CSV';
proc means data = m.ct_response_tracking n mean median std min max maxdec = 2;
Class response_new;
Var PercDiffSMRP DiffSMRP PercDiffCYFRA DiffCYFRA PercDiffMPF DiffMPF PercDiffCA125
DiffCA125;
Where Chemo = "Yes";
run;
proc means data = m.ct_response_tracking n mean median std min max maxdec = 2;
Class response_new;
Var PercDiffSMRP DiffSMRP PercDiffCYFRA DiffCYFRA PercDiffMPF DiffMPF PercDiffCA125
DiffCA125;
Where BSC = "Yes";
run;
proc means data = m.ct_response_tracking n mean median std min max maxdec = 2;
Class response_new;
Var PercDiffSMRP DiffSMRP PercDiffCYFRA DiffCYFRA PercDiffMPF DiffMPF PercDiffCA125
DiffCA125;
Where XRT = "Yes";
run;
ods csv close;

57 | P a g e
R Code was used to generate waterfall plots. A sample of the code used to generate the graphs
for the chemotherapy group and biomarker SMRP is shown below. Codes for Best Supportive
Care and Radiation are very similar and thus they are not provided here.
#Chemo
x<- read.csv("C:\\Documents and Settings\\XPMUser\\Desktop\\clean.csv", sep=',', dec='.',
na.strings='')
x$Response2 <- as.numeric(x$Response)+2
x2<-x[x$Chemo=='Yes',]
x2<-x2[order(x2$DiffSMRP),]
plot(x2$DiffSMRP, col=x2$Response, type='h', lwd=5, ylim=c(-100,4000), xlab='', ylab='',
cex.axis=1.5, cex.lab=1.5)
abline(h=0)
temp<-cbind(x2$DiffSMRP,x2$Response)
barplot(x2$DiffSMRP, col=as.numeric(x2$Response)+2)
legend("topleft", legend=c("Stable","Response","Progression"), col=c(5,4,3), fill=c(5,4,3))
x2<-x2[order(x2$PercDiffSMRP),]
plot(x2$PercDiffSMRP, col=x2$Response, type='h', lwd=5, ylim=c(-100,4000), xlab='', ylab='',
cex.axis=1.5, cex.lab=1.5)
abline(h=0)
temp<-cbind(x2$PercDiffSMRP,x2$Response)
barplot(x2$PercDiffSMRP, col=as.numeric(x2$Response)+2)
legend("topleft", legend=c("Stable","Response","Progression"), col=c(5,4,3), fill=c(5,4,3))