sensory ataxia
TRANSCRIPT
Approach to sensory ataxia
Susanth MJ
1

Ataxia
• Greek ‘taxis’ = order
• Incoordination without significant weakness
• Impaired balance and/or directional limb movements
and/or dysarthria
• Result from cerebellar, vestibular or sensory disorders
2

Visual impulses from
retinae
Proprioception from ocular
musclesjudge the distance of objects from
the body
LabyrinthsChanges in the velocity of
motion and position of the
body
Proprioceptors of the joints
and muscles esp neck
Reflex, postural, and
volitional movements
Cerebellar &
Brainstem
Structures
Maintenance of Equilibrium

Proprioceptors
• Position of our body or parts of our body
• Force, direction, and range of movement of
the joints (kinesthetic sense)
• Sense of pressure, both painful and
painless
4
Proprioceptive fibers predominantly in
motor nerves
Dorsal root gangliaCell bodies of all the sensory
neurons Posterior (Dorsal) Roots
Posterior
Columns

Somatotopic laminations in the posterior column
5

Posterior column sensations
• Touch-pressure
• Vibration
• Direction of movement and position of
joints
• Stereoesthesia - recognition of surface
texture, shape, numbers, and figures
written on the skin
• Two-point discrimination6
Depend on
patterns of
touch-pressure

Other mediators of proprioception in the spinal cord
• Cells in the more loosely
structured "reticular" part of the
dorsal column nuclei that receive
secondary ascending fibers from
the dorsal horns of the spinal
cord
• Project to brainstem nuclei,
cerebellum, and thalamic nuclei

Clinical Testing of Sensory Ataxia
Proprioception
• Awareness of the position and movements of our limbs, fingers, and
toes
Two modalities comprising proprioception
• Sense of position
• Sense of movement
– Normally, a very slight degree of movement is appreciated in the
digits (as little as 1 degree of an arc)
– Rapid movements are more easily detected than are slow ones
8
Usually lost together
Clinical situations occurs where position is
lost but movement (kinesthesia) is retained
Opposite occurs but is infrequent

Clinical Testing of Sensory Ataxia
Pseudoathetosis
• "piano-playing" movements
• When the patient has his arms
outstretched and eyes closed,
the affected arm will wander
from its original position
9

Clinical Testing of Sensory Ataxia
Romberg sign
• Compares balance as the patient stands with eyes
open and eyes closed
• Only a marked discrepancy in balance with eyes open
and with eyes closed qualifies as a Romberg sign
• Mild degrees of unsteadiness in a nervous or
suggestible patient may be overcome by diverting his
attention10

Clinical Testing of Sensory Ataxia
Romberg sign
• Most certain indication of abnormality is the need to
step to the side or backward to avoid falling
• Positive due to sensory ataxia, vestibulopathy, or
motor disorder
• May be difficult to perform or interpret in a grossly
ataxic patient with a cerebellar disorder
11

Clinical Testing of Sensory Ataxia
Testing of Vibratory Sense
• Composite sensation comprising touch and rapid alterations of
deep-pressure sense
• Only cutaneous structure capable of registering such stimuli of
this frequency is the rapidly adapting pacinian corpuscle
• Conduction of vibratory sense depends on both cutaneous and
deep afferent fibers
– Rarely affected by lesions of single nerves but will be
disturbed in patients with disease of multiple peripheral
nerves, dorsal columns, medial lemniscus, and thalamus12

Clinical Testing of Sensory Ataxia
Testing of Vibratory Sense
• Vibration and position sense are usually lost together
• One of them (most often vibration sense) may be
affected disproportionately
• With advancing age, vibration is the sensation most
commonly diminished, especially at the toes and
ankles
13

Sensory ataxia
Worth considering in any patient with ataxia who
has
• No nystagmus or cerebellar dysarthria.
• Romberg’s sign
• Pseudoathetosis,
• Impaired joint position or vibration sense
14

Sensory ataxia Vs Cerebellar Ataxia
• Sensory ataxia is often mistaken for cerebellar ataxia,
leading to diagnostic errors and delays
• Cerebellar ataxia is more common and easier to
identify with certainty
• ‘Sensory ataxia-plus’ syndromes may have a
component of cerebellar ataxia
15
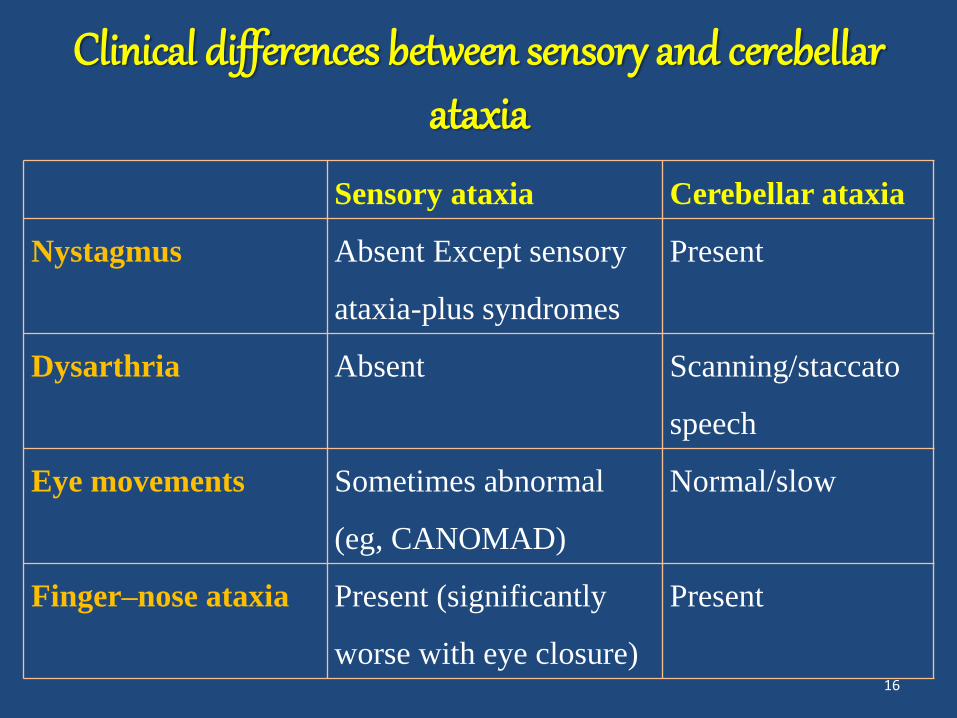
Clinical differences between sensory and cerebellarataxia
Sensory ataxia Cerebellar ataxia
Nystagmus Absent Except sensory
ataxia-plus syndromes
Present
Dysarthria Absent Scanning/staccato
speech
Eye movements Sometimes abnormal
(eg, CANOMAD)
Normal/slow
Finger–nose ataxia Present (significantly
worse with eye closure)
Present
16

Clinical differences between sensory and cerebellarataxia
Sensory ataxia Cerebellar ataxia
Heel–shin ataxia Present (significantly
worse with eye
closure)
Present
Deep tendon reflexes Absent/present Normal/pendular
Joint position sense Impaired Normal
Pseudoathetosis Usually present Absent
Exteroceptive
sensation
Reduced Normal
17

Clinical differences between sensory and cerebellarataxia
Sensory ataxia Cerebellar ataxia
Romberg’s sign Positive Classically negative
Gait High stepping
(stamping)/unsteady
Broad-based,
staggering
18

Proposed criteria for diagnosing clinically probable sensory ataxia
1. Ataxia confirmed by clinical examination:
– Finger–nose incoordination and/ or heel–toe ataxia
and/or broad-based ataxic gait
2. Two or more of:
a) Romberg’s sign or ataxia significantly worse with
eyes closed, or history of ‘wash basin sign’3
b) Pseudoathetosis and/or impaired joint position and/or
vibration sense/s.
c) Absence of nystagmus and/or cerebellar dysarthria.19

DDs Of Sensory Ataxia
• Pathology is most likely in the
proprioceptive system
• Anywhere in the pathway from the
peripheral sensory nerves, dorsal root
ganglia, sensory nerve roots, dorsal
column of spinal cord, medial
lemnisci of the brainstem and parietal
cortices
• Dorsal root ganglia is often the
major site of pathology
20

DDs Of Sensory Ataxia
21
Secondary To Peripheral Neuropathies
Paresthesia, tingling, Pseudocramp
Symmetrical distal sensory loss
Areflexia or hyporeflexia
Weakness, if present, symmetrical
When the neuropathy is primarily
demyelinating rather than axonal,
paresthesia is an early feature

DDs Of Sensory Ataxia
22
Acute
Miller Fisher syndrome
Sensory variant of GBS
Semisynthetic penicillins
Subacute Lyme disease
Neurosarcoidosis
Chronic
CIDP
Paraproteinaemia
Diabetes mellitus
Coeliac disease
Vitamin E deficiency
Secondary To Peripheral Neuropathies

Miller Fisher syndrome
• Characterised by ophthalmoplegia, ataxia and
areflexia
• May be either antecedent infection (mainly
Campylobacter jejuni and Haemophilus influenzae)
and/or underlying autoimmune or neoplastic disorder
• Serum anti-GQ1b IgG antibody titre is elevated in
over 80% of cases
23

Sensory variant of Guillain–Barré syndrome
• Rare
• Solely involves the large sensory fibres
• Sensory ataxia, impaired joint position and vibration
sense and areflexia, but usually normal strength
• Serum antibodies to GD1b and GQ1b gangliosides
may be positive
24

MFS and Sensory GBS
NCS
• Both may show demyelinating polyradiculoneuropathy
• MFS may often have either normal or show small
SNAPs
CSF
• Normal cell count but raised protein
25

CIDP
• Typically presents with monophasic, relapsing or
progressive symmetrical sensory and motor neuropathy
• Evolving over 8 weeks
• Paraesthesia, proximal weakness without wasting,
areflexia and loss of vibration and/or joint position sense
• NCS may show either conduction slowed to the
demyelinating range or partial conduction block
26

Sensory Ataxic form of CIDP
• Uncommon
• Manifests as prominent numbness in the extremities,
ataxia, areflexia and impaired vibration and/or joint
position sense
• Weakness may be mild or absent
27

Sensory Ataxic form of CIDP
• NCS show motor abnormalities typical of CIDP
• Nerve biopsy shows demyelination and remyelination
• Management is along lines similar to typical CIDP
• Often responds to corticosteroids and/or intravenous
immunoglobulins
28

It is worthwhile measuring antiganglioside antibodies in
all patients with otherwise idiopathic sensory ataxic
neuropathies, as intravenous immunoglobulin
treatment is often effective
29

Paraproteinaemic neuropathy
• Late onset slowly progressive, demyelinating neuropathy
• Distal and symmetrical, mainly sensory neuropathy.
• Monoclonal IgM antibodies against myelin-associated
glycoprotein
• Predominant impairment of joint position and vibration
sense
• May have tremor but little weakness.
30

Paraproteinaemic neuropathy
• NCS usually show symmetrical and predominantly distal
demyelination with disproportionately prolonged distal
motor latencies
• History of diabetes mellitus and alcohol excess (both
common causes of neuropathy) do not preclude the
possibility of coexisting pathology
• Serum immunoelectrophoresis and immunofixation are,
therefore, important investigations in the diagnostic
workup of ataxic neuropathy
31

Waldenström’s macroglobulinaemia
• Lymphoplasmacytoid malignancy producing IgM paraprotein
• Can present with sensory ataxia if the IgM paraprotein shows
antimyelin-associated glycoprotein activity
CANOMAD
• Chronic Ataxic Neuropathy, Ophthalmoplegia, Monoclonal
IgM protein, Cold Agglutinins and AntiDisialosyl antibodies
• Associated with anti-GQ1b and antidisialosyl antibodies
32
Paraproteinaemic neuropathy

Diabetic neuropathy
• Commonly presents with distal symmetrical polyneuropathy
• Small fibres are usually affected first, giving pain, burning,
impaired spinothalamic sensations and autonomic dysfunction.
• Large fibre sensation is affected later- develop paraesthesia
and gait imbalance.
• Often impaired vibration, joint position and pressure
sensations and loss of ankle reflex
• In advanced stage, there may be sensory ataxia
33

Coeliac ataxia
• Chronic inflammatory enteropathy
• Associated with sensitivity to ingested gluten.
• Neurological complications occur in 6–10%
– Ataxia and peripheral neuropathy are the common
presentations
– Ataxia may be cerebellar or sensory
34

Coeliac ataxia
Clinicians should request serum antigliadin antibodies
in patients presenting with sporadic idiopathic ataxia
35

Mitochondrial neuropathy
SANDO
Sensory Ataxic Neuropathy, Dysarthria and
Ophthalmoparesis
• Rare Triad due to mutations in polymerase gamma
(POLG) or TWINKLE genes
• As the clinical features include dysarthria, this leads
to confusion with cerebellar pathology
36

DDs Of Sensory Ataxia
37
Subacute
HIV, HTLV-1, HCV
Small cell lung cancer
Pyridoxine intoxication
Chemotherapeutic agents
Thalidomide
Organophosphate exposure
Colonic carcinoma
Neuroendocrine tumour
Breast and ovarian cancer
Chronic Sjögren’s syndrome
Chronic active hepatitis
Due to Dorsal Root
Ganglionopathies

Dorsal Root Ganglionopathy
• Frequently associated with paraneoplastic disorders,
dysimmune conditions like Sjögren’s syndrome or
toxic exposure to drugs, such as chemotherapeutic
agents and pyridoxine
• Leads to degeneration of peripheral axons and central
sensory projections in the dorsal columns
• Unique pattern of non-length dependent sensory
nerve degeneration 38

Dorsal Root Ganglionopathy
• Asymmetric, patchy neuropathic symptoms of pain, burning,
paraesthesia and sensory loss, with predilection for upper
limbs
• Early sensory ataxia, areflexia, markedly impaired
proprioception, pseudoathetosis, but relatively preserved
muscle strength
NCS
• Often marked involvement of the sensory fibres, with reduced
or absent SNAPs in a non-length-dependent fashion
39

Paraneoplastic dorsal root ganglionopathy
• Subacute and rapidly progressive sensory ataxia, pain and
paraesthesia
• Most commonly associated with small cell lung cancer
• Other malignancies
– Colonic carcinoma
– Hodgkin’s lymphoma
– Neuroendocrine tumours
– Breast and ovarian carcinoma
40
Paraneoplastic dorsal root ganglionopathy
• Associated with anti onconeural antibodies
• May develop before the cancer becomes clinically
overt
• Can antedate the cancer diagnosis by 0.5–62 months
41

Paraneoplastic dorsal root ganglionopathy
Antionconeural Antibodies
• anti-Hu (antineuronal nuclear autoantibodies type 1)
– Most commonly associated antibody
– Sensitivity of 82% and specificity of 99%
Other antibodies
• antiamphyphysin
• anticollapsin response mediator protein-5 (CRMP-5)42

Immune mediated dorsal root ganglionopathy
Sjogren’s syndrome
• Lymphocytic infiltration in the dorsal root ganglion
• Present with dry eyes and dry mouth
• Lip biopsy can show destruction of small salivary
glands and inflammatory infiltrates
• Ganglionopathy almost always predates the diagnosis
of Sjögren’s syndrome
43

Sjogren’s syndrome
• Sensory symptoms of numbness, tingling, burning pain
and dysaesthesia
• Often asymmetric at onset
• Predominantly involve the upper limbs
• With progression, the symptoms and signs become
symmetrical and generalised
• Negative ANA/ENA (antinuclear antibody/extractable
nuclear antigen) (Anti-SSA (Ro))/SSB (La) antibodies)
does not exclude the diagnosis.44

Medication-induced dorsal root ganglionopathy
Pyridoxine overuse
• Pure sensory neuropathy with features of large fibre
involvement
• Rarely cause sensory dorsal root ganglionopathy
• Doses as little as 200 mgs per day may be the cause
45

Medication-induced dorsal root ganglionopathy
Anticancer drugs, particularly platinum compounds
like cisplatin
• Severity of neuropathy usually correlates with the
cumulative drug dose
• Coasting
– Sensory deficits may progress for several months
after stopping treatment
46

Infection-associated dorsal root ganglionopathy
HIV
• Most common infection associated with sensory
ataxia
• Typically presents acutely or subacutely.
• Peripheral neuropathy commonly associated
47

Infection-associated dorsal root ganglionopathy
Other infections causing sensory ataxia
• Hepatitis C
• Measles
• Epstein–Barr
• Varicella zoster
• Human T-cell lymphotropic virus type I
48

Chronic idiopathic ataxic neuropathy
• No identifiable cause
• Indolent, slowly progressive, dorsal root
ganglionopathy
• Normal strength with areflexia
• CSF, EMG and motor NCS are often normal, but
sensory potentials are absent
• Often refractory to treatment
49

DDs Of Sensory Ataxia
50
Chronic
Chronic immune sensory
polyradiculopathy
Due to sensory nerve
root involvement
Severe sensory loss with preserved
sensory nerve action potentials

Chronic immune sensory polyradiculopathy
• Preferential involvement of the large myelinated
sensory nerve roots proximal to the dorsal root
ganglion.
• Presents with ataxia and limb paraesthesia.
• On examination sensory ataxia, areflexia, impaired
joint position and vibration sense but normal strength
51
Chronic immune sensory polyradiculopathy
• NCS normal, but somatosensory-evoked potentials are
abnormal, suggesting sensory root involvement
• MRI Lumbar spine may show enlarged and enhancing
nerve roots
• CSF may show raised protein
• Sensory rootlet biopsies may show demyelination similar
to CIDP
• May respond to immunomodulation52

DDs Of Sensory Ataxia
53
Due to posterior spinal
column involvement
Paresthesias in the form of tingling and
pins-and-needles sensations or girdle- and
band-like sensations
Loss of vibratory and position sense
occurs below the level of the lesion
May simulate a parietal "cortical"
lesion, but differs in that vibratory sense
is also lost in spinal cord syndromes

DDs Of Sensory Ataxia
54
Chronic
Vitamin B12 deficiency
Copper deficiency
Tabes dorsalis
HIV, HCV
Cervical myelopathy
Due to posterior spinal
column involvement

Vitamin B12 deficiency
• Classical malabsorption disease uncommon
nowadays
• More likely occurs with
– Nitrous oxide exposure—anaesthesia and dental
staff or recreational abusers
– Gastric or ileal resections with bacterial
overgrowth in blind loops, anastomoses or
diverticula55

Vitamin B12 deficiency
• Present with limb paraesthesia, subacute gait disorder
with sensory ataxia and/or spasticity
• Examination shows signs of dorsal column impairment,
including loss of proprioception and vibration as well as
the combination of sensory ataxia and spastic paraparesis.
• Length-dependent peripheral neuropathy often coexists
– May manifest as depressed lower limb reflexes with
stocking sensory loss56

Vitamin B12 deficiency
• MR scan of spine may show increased T2 signal,
most commonly in the dorsal cervical and thoracic
cord
• May have normal or borderline B12 level
• Helpful tests to confirm the diagnosis
– Increased serum levels of homocysteine and
methylmalonic acid
57
Copper deficiency
• Under-recognised cause of neurological and
haematological abnormalities
Risk factors for copper deficiency
• Previous upper gastrointestinal surgery
• Zinc overload from zinc supplementation or ingestion
of denture cream
– Competes with copper for absorption
58

Copper deficiency
• Clinical picture is often clinically and radiologically
indistinguishable from vitamin B12 deficiency
• Anaemia (microcytic, macrocytic, or normocytic), leucopenia
and, rarely, thrombocytopenia. Plasma copper, caeruloplasmin
levels and urinary copper levels are all reduced
• Neurological syndrome is incapacitating and frequently
irreversible, especially if treatment is delayed
– Early diagnosis and treatment with copper supplementation
is therefore essential
59

HIV infection
• Can cause vacuolar myelopathy
• Causes symptoms in about 10% of patients with
AIDS, although half show pathological evidence at
autopsy.
• Often occurs in the late stages of HIV infection
• Commonly parallels the development of AIDS
dementia complex
60

HIV infection
• Slowly progressive painless spastic paraparesis,
sensory ataxia and sphincter dysfunction
• MR scan of the spine usually normal although there
may be non-specific tract hyperintensities
61
Tabes dorsalis
• In late-stage or tertiary neurosyphilis
• Degeneration of the dorsal columns of the spinal cord and
sensory nerve roots
• Lancinating or lightning-like pains, progressive sensory
ataxia, proprioceptive loss and positive Romberg’s sign
• Also by diabetes mellitus, vitamin B12 deficiency, and
other diseases that involve the posterior roots or dorsal
root ganglia62
Hepatitis C infection
• May cause transverse myelopathy
• Sensory ataxia may be its only manifestation
63

Compressive and demyelinating disorders
Cervical myelopathy
• Painful stiff neck, upper limb paraesthesia and gait and
balance disturbance
Other compressive pathologies (eg, meningioma)
• Cause sensory ataxia if there is predominant involvement
of the posterior columns
• Spastic weakness in limbs, impaired joint position and
vibration sense as well as a positive romberg sign64

Compressive and demyelinating disorders
Multiple sclerosis
• Can cause sensory ataxia if demyelination involves
the central sensory pathways
65

DDs Of Sensory Ataxia
66
Due to Thalamus lesions• Involvement of the VPL and
VPM nuclei of the thalamus
• Usually because of a vascular
lesion, less often because of a
tumor
• Position sense is affected more
frequently than any other
sensory function

DDs Of Sensory Ataxia
67
Due to Parietal lesions•Loss of proprioceptive sensation,
or to lack of spatial orientation
•Due to the destruction of the
parietopontine fibres destined for
the cerebellum
•Can occur without any sensory
loss

Inherited causes of sensory ataxia
Complete absence of SNAPs in someone with no positive
sensory symptoms strongly suggests a genetic cause
• Friedreich’s ataxia
• Ataxia with vitamin E deficiency
• Abetalipoproteinaemia
• Spinocerebellar ataxia with neuropathy
• Mitochondrial neuropathies
68

Role Of Neurophysiology
• Slowing and reduced amplitude of SNAP
– Lesions of nerve or sensory ganglion
• Severe sensory loss with preserved sensory nerve action
potentials indicates a radiculopathy
• Suggest the pathological process, Axonal Versus
Demyelination.
• Neurophysiology can and should be repeated if the
clinical syndrome progresses or alters 69

Role Of Neurophysiology
Dorsal root ganglionopathy
• SNAPs may be more affected in the upper than the lower
limbs
• Non-length-dependent axonal degeneration helps to
distinguish DRG from the more common dying-back axonal
neuropathies
Sensory root involvement, as in chronic immune sensory
polyradiculopathy
• Normal nerve conduction, but often abnormal somatosensory-
evoked potentials70

To Detect And Diagnose Sensory Ataxias
• Initial differentiation relies heavily on a careful and
targeted clinical examination
• Subsequently detecting correct cause of sensory
ataxia by adopting a logical anatomical approach
• Requires neurophysiology
– into anatomical (nerve, dorsal root ganglion, etc.)
and pathological (demyelinating vs axonal) subsets
71

Other investigationsAetiology Ancillary investigations
Miller Fisher syndrome Anti-GQ1b antibodies, CSF, NCS
Sensory variant of GBS Anti-ganglioside antibodies, CSF, NCS
Lyme disease Lyme serology
Neurosarcoidosis CSF, NCS, ACE, chest X ray, HPE
CIDP NCS, CSF
Paraproteinaemia Electrophoresis, anti-MAG
Diabetes mellitus Plasma glucose.
Coeliac disease Anti-tTG antibodies
Vitamin E deficiency Serum vitamin E level 72

Other investigations
Aetiology Ancillary investigations
HIV, HTLV-1, HCV Serology
Paraneoplastic Anti-Hu, CRMP-5, Relevant imaging
Pyridoxine intoxication History of exposure; pyridoxine levels
Chemotherapeutic
agents
History of exposure
Sjögren’s syndrome ENA (Anti-SSA/SSB) Abs, Lip biopsy
Chronic active hepatitis RF, ANA, ASMA, hepatitis serology
73

Other investigations
Aetiology Ancillary investigations
CISP NCS, SSEP, CSF, MRI
Vitamin B12 deficiency Serum B12, Schilling’s test
Copper deficiency Serum copper and ceruloplasmin level.
Tabes dorsalis Syphilis serology
Cervical myelopathy Neuroimaging
74

75

Thank you
76

Clinical Approach To Ataxia
• First step is to distinguish cerebellar, sensory and
vestibular ataxia
77