ataxia panel plus - blueprintgenetics.com · spinocerebellar ataxia 6 (sca6; mim #183086) is...
TRANSCRIPT
1 / 7
Blueprint Genetics Oy, Haartmaninkatu 8, Biomedicum Helsinki, 00290 Helsinki, FinlandVAT number: FI22307900, CLIA ID Number: 99D2092375, CAP Number: 9257331
1 / 7
Ataxia Panel PlusFAMILY EXTENSION SERVICE
REFERRING HEALTHCARE PROFESSIONAL
NAME<referriing professional name>
HOSPITAL<hospital name>
PATIENT
DOB GENDERFemale
AGE35
SAMPLE COLLECTION DATE
NAME<patient name>
PRIMARY SAMPLE TYPE DNA
ORDER ID
CUSTOMER SAMPLE ID
SUMMARY OF RESULTS
TEST RESULTS
Patient is heterozygous for CACNA1A c.2816dup, p.(Ser940Glnfs*128), which is pathogenic.
Del/Dup (CNV) analysis did not detect any known disease-causing copy number variation or novel or raredeletion/duplication that was considered deleterious.
VARIANT TABLE: GENETIC ALTERATIONS
GENECACNA1A
POS19:13409633
TRANSCRIPTNM_001127221.1
NOMENCLATUREc.2816dup, p.(Ser940Glnfs*128)
CONSEQUENCEframeshift_variant
GENOTYPEHET
CLASSIFICATIONPathogenic
ID gnomAD AC/AN2/185606
POLYPHENN/A
SIFTN/A
MUTTASTERN/A
OMIM
PHENOTYPEEpileptic encephalopathy early infantile 42,Episodic ataxia,Migraine familial hemiplegic,Spinocerebellar ataxia 6
INHERITANCEAD
COMMENT-
SEQUENCING PERFORMANCE METRICS
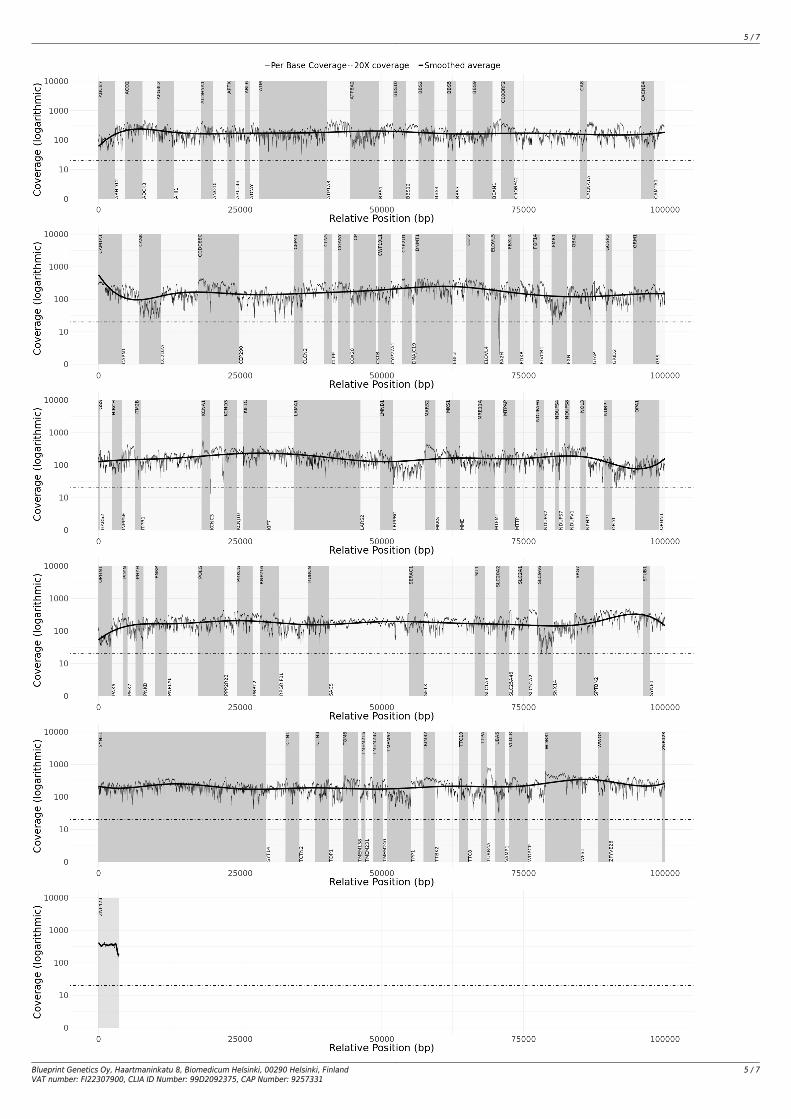
PANEL GENES EXONS / REGIONS BASES BASES > 20X MEDIAN COVERAGE PERCENT > 20XAtaxia Panel 157 2559 503595 503378 184 99.96
TARGET REGION AND GENE LIST
The Blueprint Genetics Ataxia Panel (version 3, Mar 01, 2018) Plus Analysis includes sequence analysis and copy number variation analysis of the following genes:ABCB7, ABHD12, ACO2, ADCK3, AFG3L2*, AHI1, ALDH5A1, ANO10, APTX, ARL13B, ARL6, ATCAY, ATM, ATP1A3, ATP8A2, BBS1, BBS10, BBS12, BBS2, BBS4, BBS5,BBS7, BBS9, BEAN1, C10ORF2, C5ORF42, CA8, CACNA1A, CACNB4, CAMTA1, CAPN1, CASK, CC2D2A, CCDC88C, CEP290*, CEP41, CLCN2, CLN5, CLPP, COASY,COX20, CP*, CSTB, CWF19L1, CYP27A1, CYP2U1, DNAJC19, DNMT1, EBF3, EEF2, ELOVL4, ELOVL5, FA2H, FBXL4, FDXR, FGF14, FLVCR1, FMR1, FXN*, GBA2, GFAP,GOSR2*, GRID2, GRM1, GSS, HARS2, HIBCH, INPP5E, ITM2B, ITPR1, KCNA1, KCNC3, KCND3, KCNJ10, KIF1C*, KIF7, LAMA1, LARS2, LMNB1, LRPPRC, MARS2, MKKS,MKS1, MME, MRE11A, MTFMT, MTPAP, MTTP, NDUFAF6, NDUFS2, NDUFS4, NDUFS7, NDUFS8, NDUFV1, NOL3, NPHP1, NUBPL, OFD1, OPA1, OPHN1, PAX6, PDYN,PEX7, PHYH, PNKD, PNKP, PNPLA6, POLG, PPP2R2B, PRKCG, PRRT2, RNF216*, RPGRIP1L, RUBCN, SACS, SERAC1, SETX, SIL1, SLC1A3, SLC20A2, SLC25A46, SLC2A1,SLC52A2, SLC9A6, SNX14, SPG7, SPTBN2, STUB1, SYNE1, SYT14*, TCTN1, TCTN2, TCTN3, TDP1, TGM6, TMEM138, TMEM216, TMEM231, TMEM237, TMEM240,TMEM67, TPP1, TRIM32, TTBK2, TTC19, TTC8, TTPA, TUBB4A*, UBA5*, VAMP1, VLDLR, WDPCP, WDR81, WFS1, WWOX, ZFYVE26 and ZNF423. This panel targetsprotein coding exons, exon-intron boundaries (± 20 bps) and selected non-coding, deep intronic variants (listed in Appendix 5). This panel should be used to detectsingle nucleotide variants and small insertions and deletions (INDELs) up to 220 bps and copy number variations defined as single exon or larger deletions andduplications. This panel should not be used for the detection of repeat expansion disorders or diseases caused by mitochondrial DNA (mtDNA) mutations. The testdoes not recognize balanced translocations or complex inversions, and it may not detect low-level mosaicism.

2 / 7
Blueprint Genetics Oy, Haartmaninkatu 8, Biomedicum Helsinki, 00290 Helsinki, FinlandVAT number: FI22307900, CLIA ID Number: 99D2092375, CAP Number: 9257331
2 / 7
*Some, or all, of the gene is duplicated in the genome. Read more: https://blueprintgenetics.com/pseudogene/The sensitivity to detect variants may be limited in genes marked with an asterisk (*).
Family Extension Service includes free familial mutation testing of five first degree relatives within 12 months of the original index patient report date for likely pathogenic and pathogenic variants.
3 / 7
Blueprint Genetics Oy, Haartmaninkatu 8, Biomedicum Helsinki, 00290 Helsinki, FinlandVAT number: FI22307900, CLIA ID Number: 99D2092375, CAP Number: 9257331
3 / 7
STATEMENT
CLINICAL HISTORY
Patient is a 35-year-old female with paroxysmal cerebellar ataxia. The family history of the disease is positive.
CLINICAL REPORT
Sequence analysis using the Blueprint Genetics (BpG) Ataxia Panel Plus identified a heterozygous frameshift variant c.2816dup, p.(Ser940Glnfs*128) in CACNA1A.There are 2 individuals heterozygous for this variant in the Genome Aggregation Database (gnomAD, n>120,000 exomes and >15,000 genomes). No homozygotes were observed. Database curators have made every effort to exclude individuals with severe pediatric diseases from these cohorts. The variant duplicates 1 bp and generates a frameshift leading to a premature stop codon at position 128 in a new reading frame. It is predicted to cause loss of normal protein function either through protein truncation (1067 out of 2261 aa) or nonsense-mediated mRNA decay. The variant has been identified in a family with eight affected family members with episodic ataxia type 2 (PMID: 11370629). The variant segregated with the disease in three generations.Voltage-dependent calcium channels mediate the entry of calcium ions into excitable cells and are also involved in a variety of calcium-dependent processes, including muscle contraction, hormone or neurotransmitter release, and gene expression. Calcium channels are multisubunit complexes composed of alpha-1, beta, alpha-2/delta, and gamma subunits. The channel activity is directed by the pore-forming alpha-1 subunit, whereas, the others act as auxiliary subunits regulating this activity. The distinctive properties of the calcium channel types are related primarily to the expression of a variety of alpha-1 isoforms, alpha-1A, B, C, D, E, and S. The CACNA1A (MIM *601011) gene on chromosome 19p13.13 encodes the alpha-1A subunit, which is predominantly expressed in neuronal tissue. Mutations in this gene are associated with autosomal dominant neurologic disorders. Familial hemiplegic migraine (FMH; MIM #141500) is a rare variety of migraine with aura characterized by the presence of a motor weakness during the aura (MIM #157300). Severe attacks may occur in FHM with prolonged hemiplegia, confusion, coma, fever and seizures. The clinical spectrum also includes permanent cerebellar signs (nystagmus, ataxia, dysarthria) and less frequently various types of seizures and intellectual deficit. The prevalence of FMH is 1/10,000 (ORPHA569). Episodic ataxia (EA) is a genetically heterogeneous neurologic condition characterized by spells of incoordination and imbalance, often associated with progressive ataxia. Episodic ataxia 2 (EA2; MIM #108500; GeneReviews NBK1501), caused by CACNA1A mutations is the most common form of EA. Its prevalence has been estimated at lower than 1/100,000. About 50% of individuals with EA2 have migraine headaches. Onset is typically in childhood or early adolescence (age range 2-32 years). Spinocerebellar ataxia 6 (SCA6; MIM #183086) is characterized by adult-onset, slowly progressive cerebellar ataxia, dysarthria, and nystagmus. The most common mutation is an expanded CAG(n) repeat in exon 47 of the CACNA1A gene. Normal alleles contain 4 to 18 repeats, whereas pathogenic alleles contain 19 to 33 repeats.Early infantile epileptic encephalopathy-42 (EIEE42; MIM #617106) can also be caused by CACNA1A mutations as targeted sequencing in an unsolved cohort of individuals with a diverse range of epileptic encephalopathies revealed 4/531 patients with pathogenic missense mutations in CACNA1A (PMID 27476654). All of them, including one patient from earlier cohort, had early onset seizures (beginning during the first day in 5 individuals) and typically included focal, tonic and tonic-clonic seizures and occasional myoclonic seizures accompanied with moderate to severe intellectual disability. Missense mutations were clustered in the transmembrane domains of the protein. In children with CACNA1A mutations, eye movement disorder was found to be a presenting feature in conjunction with developmental delay, cerebellar atrophy, FHM, ataxia and seizures (PMID: 26814174).Currently, 198 disease-causing variants in CACNA1A are reported in the Human Gene Mutation Database (HGMD Professional 2018.2). This includes missense variants (50.0%), nonsense variants (14.1%), splice variants (6.1%), small deletions (12.6%), small insertions (5.6%), gross deletions (8.6%), complex rearrangements (0.5%) and repeat variations (2.5%). These variants are mainly implicated in ataxia phenotypes, and most of these in episodic ataxia (122 disease-causing variants reported in HGMD).Nine distinct disease-causing variants have been reported in patients with epilepsy in HGMD: missense variants have been reported in association with epilepsy of infancy with migrating focal seizures (n=1), idiopathic epilepsy (n=2) and epileptic encephalopathy (n=3). In addition, one nonsense variant has been reported in a patient with idiopathic epilepsy, one small deletion has been reported in a patient with epileptic encephalopathy and one large deletion has been reported in a patient with epilepsy and mental retardation.Mutation nomenclature is based on GenBank accession NM_001127221.1 (CACNA1A) with nucleotide one being the first nucleotide of the translation initiation codon ATG.
CONCLUSION
Considering the current literature and the well-established role of CACNA1A c.2816dup, p.(Ser940Glnfs*128) as a disease-causing variant, we classify it as pathogenic. Genetic counseling and family member testing are recommended. Disease caused by CACNA1A variants is inherited in an autosomal dominant manner, and thus each child of an affected individual has a 50% chance of inheriting the variant. BpG offers targeted variant testing for the family if requested.
CONFIRMATION
CACNA1A c.2816dup, p.(Ser940Glnfs*128) has been confirmed with bi-directional Sanger sequencing.
STEP DATE
Order date Aug 08, 2018
Sample received Aug 30, 2018
4 / 7
Blueprint Genetics Oy, Haartmaninkatu 8, Biomedicum Helsinki, 00290 Helsinki, FinlandVAT number: FI22307900, CLIA ID Number: 99D2092375, CAP Number: 9257331
4 / 7
STEP DATE
Reported Sep 26, 2018
On Sep 26, 2018 the statement has been prepared by our geneticists and physicians, who have together evaluated the sequencing results:
Kirsi Alakurtti, Ph.D., CLG
Geneticist
Juha Koskenvuo, MD, Ph.D.
Lab Director, Chief Medical Officer
5 / 7
Blueprint Genetics Oy, Haartmaninkatu 8, Biomedicum Helsinki, 00290 Helsinki, FinlandVAT number: FI22307900, CLIA ID Number: 99D2092375, CAP Number: 9257331
5 / 7
6 / 7
Blueprint Genetics Oy, Haartmaninkatu 8, Biomedicum Helsinki, 00290 Helsinki, FinlandVAT number: FI22307900, CLIA ID Number: 99D2092375, CAP Number: 9257331
6 / 7
APPENDIX 5: SUMMARY OF THE TEST
PLUS ANALYSIS
Laboratory process: Total genomic DNA was extracted from the biological sample using a spin column method. DNA quality and quantity were assessed usingelectrophoretic methods. After assessment of DNA quality, qualified genomic DNA sample was randomly fragmented using non-contact, isothermal sonochemistryprocessing and purified with SPRI beads. DNA fragments were then end-repaired and sequencing adapters were ligated to both ends of the resulting fragments.Prepared DNA-Adapter libraries were size-selected with SPRI beads to ensure optimal template size and then amplified by ligation-mediated PCR (LM-PCR). Theamplified sequencing library was purified using SPRI beads and a hybridization-capture method was applied for enrichment of whole exome and select non-codingregions (xGen Exome Research Panel with custom-designed capture probes, IDT). The enriched sequencing library was amplified by LM-PCR and purified using SPRIbeads. The quality of the completed sequencing library was controlled by ensuring the correct template size and quantity and to eliminate the presence of leftoverprimer-dimers. Each captured library passing quality control was sequenced using the Illumina sequencing system with paired-end sequencing (150 by 150 bases).Sequencing-derived raw image files were processed using a base-calling software (Illumina) and the sequence data was transformed into FASTQ format.Bioinformatics and quality control: The bioinformatics analysis began with quality control of raw sequence reads. Clean sequence reads of each sample weremapped to the human reference genome (GRCh37/hg19). Burrows-Wheeler Aligner (BWA-MEM) software was used for read alignment. Duplicate read marking, localrealignment around indels, base quality score recalibration and variant calling were performed using GATK algorithms (Sentieon). The panel content was sliced fromhigh-quality exome sequencing data acquired as presented above. The sequencing depth and coverage for the tested sample was calculated based on thealignments. The sequencing run included in-process reference sample(s) for quality control, which passed our thresholds for sensitivity and specificity. The patient'ssample was subjected to thorough quality control measures as well, after which raw sequence reads were transformed into variants by a proprietary bioinformaticspipeline. Copy number variations (CNVs), defined as single exon or larger deletions or duplications (Del/Dups), were detected from the sequence analysis data usinga proprietary bioinformatics pipeline, which processes aligned sequence reads. The difference between observed and expected sequencing depth at the targetedgenomic regions was calculated and regions were divided into segments with variable DNA copy number. The expected sequencing depth was obtained by usingother samples processed in the same sequence analysis as a guiding reference. The sequence data was adjusted to account for the effects of varying guanine andcytosine content.Interpretation: Our variant classification follows the Blueprint Genetics Variant Classification Schemes modified from the ACMG guideline 2015. Minormodifications were made to increase reproducibility of the variant classification and improve the clinical validity of the report. Likely benign and benign variantswere not reported. The pathogenicity potential of the identified variants were assessed by considering the predicted consequence, the biochemical properties of thecodon change, the degree of evolutionary conservation as well as the number of reference population databases and mutation databases such as, but not limited,to the 1000 Genomes Project, gnomAD, ClinVar and HGMD. For missense variants, in silico variant prediction tools such as SIFT, PolyPhen, MutationTaster were usedto assist with variant classification. In addition, the clinical relevance of any identified CNVs was evaluated by reviewing the relevant literature and databases suchas 1000 Genomes Project, Database of Genomic Variants, ExAC, DECIPHER. The clinical evaluation team assessed the pathogenicity of the identified variants byevaluating the information in the patient referral, reviewing the relevant literature and manually inspecting the sequencing data if needed. Reporting was carriedout using HGNC-approved gene nomenclature and mutation nomenclature following the HGVS guidelines.Confirmation: Pathogenic and likely pathogenic variants that established a molecular diagnosis were confirmed with bi-directional Sanger sequencing unless all ofthe following criteria were fulfilled: 1) the variant quality score (QS) was above the internal threshold for a true positive call, 2) an unambiguous manual curation ofthe variant region using IGV was concordant with the variant call and 3) previous Sanger confirmation of the same variant has been performed at least three timesin our laboratory. Reported variants of uncertain significance were confirmed with bi-directional Sanger sequencing only if the QS was below our internally definedscore for a true positive call. CNVs (Dels/Dups) were confirmed using a quantitative-PCR assay if they covered less than 10 target exons or were not confirmed atleast three times previously at our laboratory.Analytic validation: This laboratory-developed test has been independently validated by Blueprint Genetics. The sensitivity of this panel is expected to be in thesame range as the validated whole exome sequencing laboratory assay used to generate the panel data (sensitivity for SNVs 99.65%, indels 1-50 bps 99.07%, one-exon deletion 92.3% and two exons CNV 100%, and specificity >99.9% for most variant types). A normal result does not rule out the diagnosis of a genetic disordersince some DNA abnormalities may be undetectable by the applied technology. Test results should always be interpreted in the context of clinical findings, familyhistory, and other relevant data. Inaccurate, or incomplete information may lead to misinterpretation of the results.Regulation and accreditations: This test has not been cleared or approved by the FDA. This analysis has been performed in a CLIA-certified laboratory(#99D2092375), accredited by the College of American Pathologists (CAP #9257331) and by FINAS Finnish Accreditation Service, (laboratory no. T292),accreditation requirement SFS-EN ISO 15189:2013. All the tests are under the scope of the ISO 15189 accreditation.
NON-CODING VARIANTS COVERED BY THE PANEL:
NM_000051.3(ATM):c.-174A>GNM_000051.3(ATM):c.-31+595G>ANM_000051.3(ATM):c.-30-1G>TNM_000051.3(ATM):c.1236-404C>TNM_000051.3(ATM):c.2639-384A>GNM_000051.3(ATM):c.2839-579_2839-576delAAGTNM_000051.3(ATM):c.3403-12T>ANM_000051.3(ATM):c.3994-159A>GNM_000051.3(ATM):c.5763-1050A>GNM_024649.4(BBS1):c.951+58C>TNM_024649.4(BBS1):c.1110+329C>TNM_033028.4(BBS4):c.77-216delANM_152384.2(BBS5):c.619-27T>GNM_001127221.1(CACNA1A):c.5404-13G>ANM_025114.3(CEP290):c.6012-12T>ANM_025114.3(CEP290):c.2991+1655A>GNM_000178.2(GSS):c.-9+5G>ANM_002241.4(KCNJ10):c.-1+1G>TNM_000253.2(MTTP):c.619-5_619-2delTTTA

7 / 7
Blueprint Genetics Oy, Haartmaninkatu 8, Biomedicum Helsinki, 00290 Helsinki, FinlandVAT number: FI22307900, CLIA ID Number: 99D2092375, CAP Number: 9257331
7 / 7
NM_000253.2(MTTP):c.1237-28A>GNM_152416.3(NDUFAF6):c.298-768T>CNM_024407.4(NDUFS7):c.17-1167C>GNM_025152.2(NUBPL):c.815-27T>CNM_003611.2(OFD1):c.935+706A>GNM_003611.2(OFD1):c.1130-22_1130-19delAATTNM_130837.2(OPA1):c.610+360G>ANM_130837.2(OPA1):c.610+364G>ANM_130837.2(OPA1):c.2179-40G>CNM_000280.4(PAX6):c.*125537G>TNM_000280.4(PAX6):c.524-41T>GNM_000280.4(PAX6):c.-52+1G>ANM_000280.4(PAX6):c.-128-1G>TNM_000280.4(PAX6):c.-129+2T>ANM_000288.3(PEX7):c.-45C>TNM_007254.3(PNKP):c.1387-33_1386+49delCCTCCTCCCCTGACCCCNM_022464.4(SIL1):c.1030-18G>ANM_006516.2(SLC2A1):c.680-11G>ANM_182961.3(SYNE1):c.15918-12A>GNM_001077416.2(TMEM231):c.824-11T>CNM_000391.3(TPP1):c.887-18A>GNM_006005.3(WFS1):c.-43G>T
GLOSSARY OF USED ABBREVIATIONS:
AD = autosomal dominantAR = autosomal recessiveCNV = Copy Number Variation e.g. one exon or multiexon deletion or duplicationgnomAD = genome Aggregation Database (reference population database; >138,600 individuals)gnomAD AC/AN = allele count/allele number in the genome Aggregation Database (gnomAD)HEM = hemizygousHET = heterozygousHOM = homozygousID = rsID in dbSNPMutationTaster = in silico prediction tools used to evaluate the significance of identified amino acid changes. Nomenclature = HGVS nomenclature for a variant in the nucleotide and the predicted effect of a variant in the protein level OMIM = Online Mendelian Inheritance in Man®PolyPhen = in silico prediction tool used to evaluate the significance of amino acid changes.POS = genomic position of the variant in the format of chromosome:positionSIFT = in silico prediction tool used to evaluate the significance of amino acid changes.