segmental colitis caused by idiopathic myointimal...
TRANSCRIPT
1130-0108/2016/108/12/821-826Revista española de enfeRmedades digestivas© Copyright 2016. sepd y © ARÁN EDICIONES, S.L.
Rev esp enfeRm dig2016, Vol. 108, N.º 12, pp. 821-826
CASE REPORTS
ABSTRACT
Diseases causing colonic ischemia may be mistaken with other causes of segmental colitis such as inflammatory bowel disease, especially in young patients. The authors present the case of a 47-year-old male with severe proctosigmoiditis. Assessment exclud-ed infectious causes, thrombophilia and systemic vasculitis. The initial histological specimen was suggestive of inflammatory bowel disease and therapy was initiated with intravenous steroids and, at day 5, infliximab, with no response. The patient was proposed for surgery. Pathological examination of the surgical specimen revealed an idiopathic myointimal hyperplasia of mesenteric veins, a rare entity exhibiting necrotizing phlebitis with rapid progression to seg-mental necrosis in the rectosigmoid colon. In this paper the authors discuss the differential diagnosis of proctosigmoiditis in young ages and the approach to this exceptionally rare ischemic entity.
Key words: Ischemic colitis. Idiopathic myointimal hyperplasia of mesenteric veins.
INTRODUCTION
Diseases causing colonic ischemia may have simi-lar presentation symptoms to other causes of segmental colitis such as inflammatory bowel disease, especially in young patients. Idiopathic myointimal hyperplasia of mesenteric veins (IMHMV) is a rare condition causing segmental colonic ischemia that should be considered in the differential diagnosis of severe colonic inflammato-ry bowel disease refractory to intensive medical treat-ment. Preoperative diagnosis of IMHMV could be diffi-cult as intimal thickening venules are in the submucosa and deeper layers. Even when a full-thickness biopsy is performed the diagnosis may be inconclusive. Standard treatment is surgical resection and there are no reports of postoperative disease recurrence. The following case illustrates this rare clinical condition in a young adult male patient.
CASE REPORT
A 47-year-old Caucasian male patient was admitted to our medical department on February 2012 with bloody diarrhea (more than 20 stools per day), lower abdominal cramping pain, proctalgia and malaise.
The patient reported a previous 9 month history of hypogastric cramp-like pain, 4-5 small volume stools, without blood, mucus or pus, as well as a compelling urge to defecate and fecal incontinence. One month before, the patient had been assessed on the emergency department of another hospital due to clinical deterioration with anal pain, persistent urge to defecate, tenesmus and straining at stool. There, he had undergone a colonoscopy with biopsy and a pelvic CT scan. The colonoscopy showed edema of the rectal mucosa and sigmoid colon. The biopsies did not reveal any significant alterations. The pelvic CT scan identified parietal thickening of the rectum. At that time, the patient was treated with an antispasmodic. No improve-ment was observed.
Patient’s personal and family histories were irrelevant and epidemiological context was unremarkable. He had not been undergoing any other course of medication and denied known allergies, smoking, alcohol and history of injected or inhaled drug use.
Upon physical examination, he was afebrile with lower abdominal tenderness with no signs of peritoneal irritation.
Routine blood analysis revealed normal hemoglobin (13.8 g/dL), no leukocytosis nor neutrophilia with a slight-ly raised level of C-reactive protein (6.3 mg/dL; normal level: < 5 mg/dL). Infectious causes were excluded.
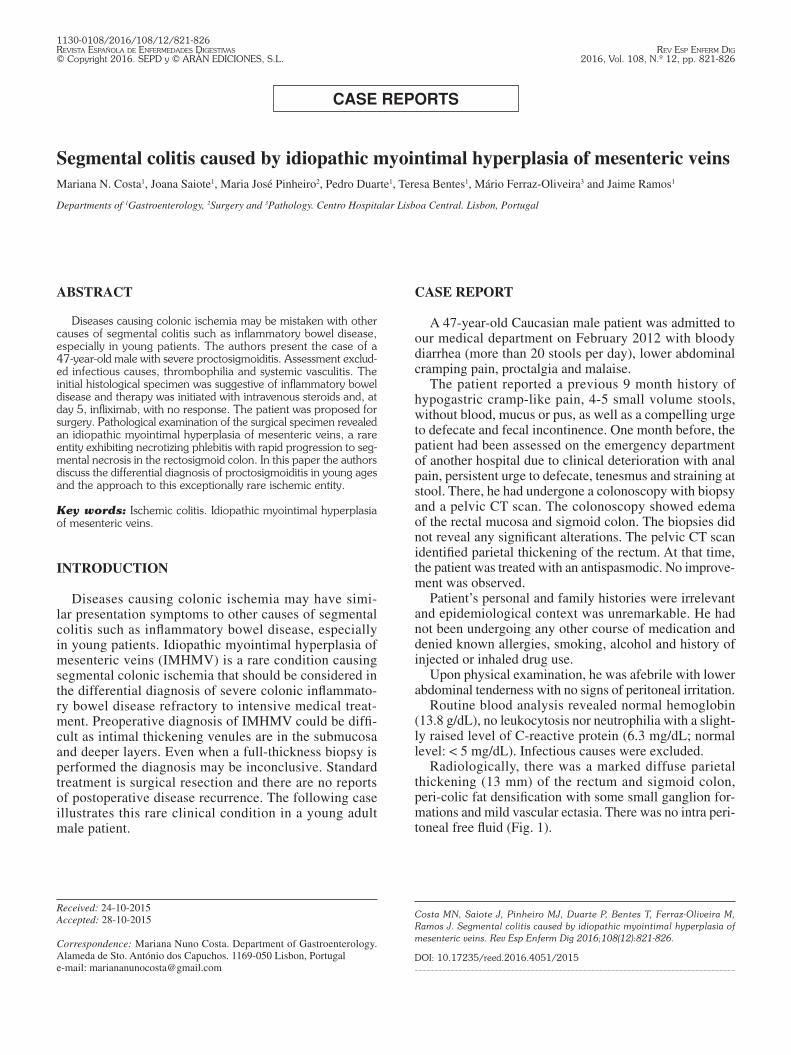
Radiologically, there was a marked diffuse parietal thickening (13 mm) of the rectum and sigmoid colon, peri-colic fat densification with some small ganglion for-mations and mild vascular ectasia. There was no intra peri-toneal free fluid (Fig. 1).
Received: 24-10-2015Accepted: 28-10-2015
Correspondence: Mariana Nuno Costa. Department of Gastroenterology. Alameda de Sto. António dos Capuchos. 1169-050 Lisbon, Portugale-mail: [email protected]
Costa MN, Saiote J, Pinheiro MJ, Duarte P, Bentes T, Ferraz-Oliveira M, Ramos J. Segmental colitis caused by idiopathic myointimal hyperplasia of mesenteric veins. Rev Esp Enferm Dig 2016;108(12):821-826.
DOI: 10.17235/reed.2016.4051/2015
Segmental colitis caused by idiopathic myointimal hyperplasia of mesenteric veinsMariana N. Costa1, Joana Saiote1, Maria José Pinheiro2, Pedro Duarte1, Teresa Bentes1, Mário Ferraz-Oliveira3 and Jaime Ramos1
Departments of 1Gastroenterology, 2Surgery and 3Pathology. Centro Hospitalar Lisboa Central. Lisbon, Portugal
822 M. N. COSTA ET AL. Rev esp enfeRm Dig
Rev esp enfeRm Dig 2016;108(12):821-826
The rectosigmoidoscopy showed diffuse edema of the rectal mucosa with sudden transition to a circumferential and continuous mucosal ulceration and luminal stenosis of the sigmoid colon. Histologic examination showed mucosal edema and vascular congestion without signifi-cant glandular lesions, with mild inflammatory infiltration and fragments of base of ulcer without pericriptitis, crypt abscesses or granulomas.
Intravenous methylprednisolone (40 mg daily) was initi-ated. There was no improvement in the clinical course after 5 days of intravenous steroids, so treatment with intrave-nous 400 mg infliximab (5 mg/kg) was started.
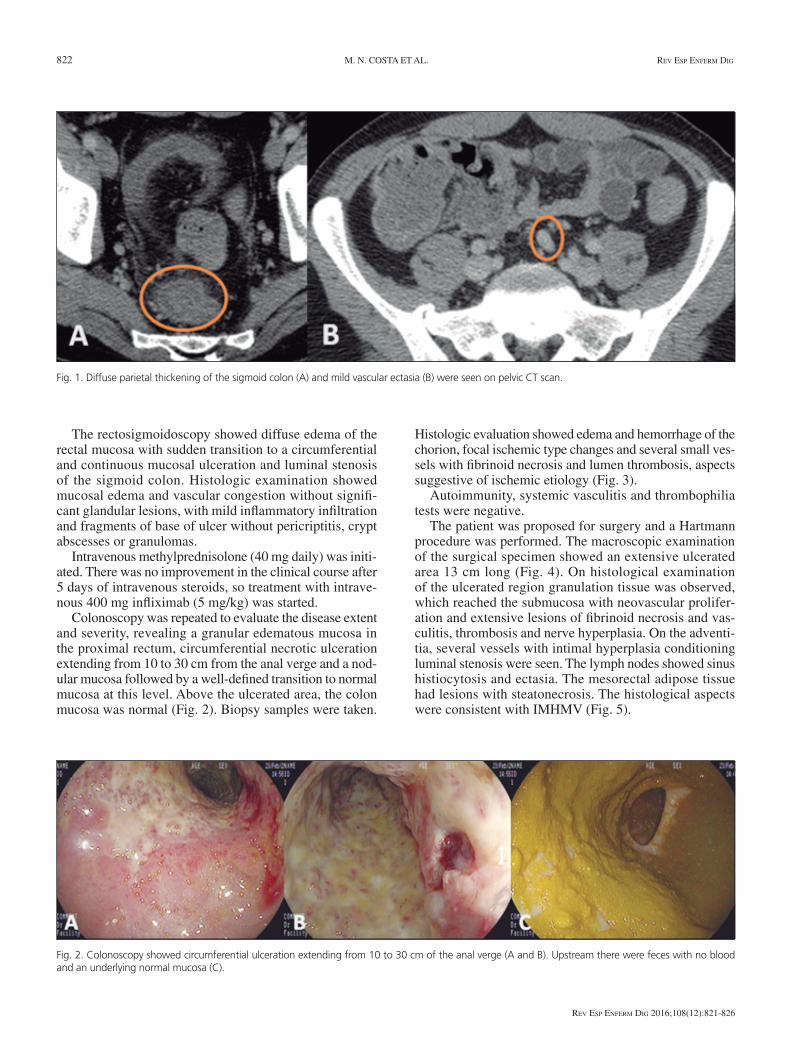
Colonoscopy was repeated to evaluate the disease extent and severity, revealing a granular edematous mucosa in the proximal rectum, circumferential necrotic ulceration extending from 10 to 30 cm from the anal verge and a nod-ular mucosa followed by a well-defined transition to normal mucosa at this level. Above the ulcerated area, the colon mucosa was normal (Fig. 2). Biopsy samples were taken.
Histologic evaluation showed edema and hemorrhage of the chorion, focal ischemic type changes and several small ves-sels with fibrinoid necrosis and lumen thrombosis, aspects suggestive of ischemic etiology (Fig. 3).
Autoimmunity, systemic vasculitis and thrombophilia tests were negative.
The patient was proposed for surgery and a Hartmann procedure was performed. The macroscopic examination of the surgical specimen showed an extensive ulcerated area 13 cm long (Fig. 4). On histological examination of the ulcerated region granulation tissue was observed, which reached the submucosa with neovascular prolifer-ation and extensive lesions of fibrinoid necrosis and vas-culitis, thrombosis and nerve hyperplasia. On the adventi-tia, several vessels with intimal hyperplasia conditioning luminal stenosis were seen. The lymph nodes showed sinus histiocytosis and ectasia. The mesorectal adipose tissue had lesions with steatonecrosis. The histological aspects were consistent with IMHMV (Fig. 5).
Fig. 1. Diffuse parietal thickening of the sigmoid colon (A) and mild vascular ectasia (B) were seen on pelvic CT scan.
Fig. 2. Colonoscopy showed circumferential ulceration extending from 10 to 30 cm of the anal verge (A and B). Upstream there were feces with no blood and an underlying normal mucosa (C).

2016, Vol. 108, N.º 12 SEGMENTAL COLITIS CAUSED BY IDIOPATHIC MYOINTIMAL HYPERPLASIA OF MESENTERIC VEINS 823
Rev esp enfeRm Dig 2016;108(12):821-826
DISCUSSION
A significant diagnostic challenge is raised by seg-mental colitis because of its broad differential diagnosis. Many diseases such as diverticulitis, radiation colitis, mucosal prolapsed/solitary ulcer syndrome, infectious diseases, colon carcinoma, inflammatory bowel disease and colonic ischemia may present a segmental colonic involvement.
Colonic ischemia may result from various etiologies but it can be broadly classified as non-occlusive and occlusive. Venous occlusion is an uncommon cause of ischemic bow-el disease, and the majority of such cases are caused by venous thrombosis (1,2). Non-thrombotic occlusion of the mesenteric veins is rare and has previously been described in vasculitis associated with systemic lupus erythemato-sus, Behçet’s disease, enterocolic lymphocytic phlebitis and IMHMV (3,4).
Colonic ischemia is more common in the elderly but younger patients may also be affected. In these patients, segmental ischemic colitis is a rare differential diagnosis of inflammatory bowel disease (5) and it results of a hypoxic tissue injury with secondary necrosis and inflammation (6). It may present a spectrum of severity ranging from mild, transient mucosal erosion to fibrous scarring with stricture formation or even transmural infarction (7).
IMHMV is a rare entity exhibiting necrotizing phle-bitis with rapid progression to segmental necrosis in the rectosigmoid colon. The precise incidence of IMHMV is unknown, as only 21 cases have been reported in the lit-erature to date (Table I). This disease is known to occur predominantly in young, healthy men, with a sudden onset of crampy abdominal pain accompanying repeated epi-sodes of diarrhea and bloody stools (4,8). The pathophys-iologic mechanism seems to be an abnormal arteriovenous shunting with elevated venous pressure and consecutive congestion and ischemia of the involved bowel segment
Fig. 3. Histologic examination showed hemorrhage of the chorion, focal ischemic type changes and several small vessels with fibrinoid necrosis and lumen thrombosis.
Fig. 4. Resected colon with a 13 cm long ulcerated area.
Fig. 5. Histologic evaluation showed myointimal hyperplasia of the veins (thin arrows); arteries were unaffected (large arrows).

824 M. N. COSTA ET AL. Rev esp enfeRm Dig
Rev esp enfeRm Dig 2016;108(12):821-826
Table I. Reported cases of IMHMV to date
Age/Gender Presenting symptoms Site Clinical diagnosis Surgical indication Time to surgery Reference
1 30/M Abdominal pain/hematochezia
Sigmoid Stricture Bowel obstruction 1 mo (4)
2 38/M Abdominal pain/hematochezia/diarrhea/constipation
Sigmoid Ulcerative colitis Toxic megacolon 2 mo (4)
3 25/M Abdominal pain/hematochezia/diarrhea/constipation
Rectosigmoid Ulcerative colitis Perforation > 6 mo (4)
4 67/M Abdominal pain/diarrhea/constipation
Sigmoid Crohn’s disease Bleeding, severe pain 3 mo (4)
5 58/M Abdominal pain/hematochezia/diarrhea
Sigmoid IBD ischemia Bleeding > 1 y (3)
6 22/M Hematochezia/diarrhea Rectosigmoid Ulcerative colitis Bleeding NA (10)
7 38/M Abdominal pain/hematochezia/constipation
Rectosigmoid IBD Perforation 5 mo (8)
8 54/F Abdominal pain/hematochezia/diarrhea
Sigmoid IBD Severe pain 15 mo (11)
9 32/F Abdominal pain/hematochezia/diarrhea
Sigmoid Primarypneumatosisintestinalis
Severe pain andbleeding
3 mo (12)
10 60/M Abdominal pain/hematochezia/diarrhea
Rectosigmoid Ulcerative colitis Pain and bleeding 1 mo (13)
11 75/F Abdominal pain/hematochezia/diarrhea
Rectum Inflammatorymass
Severe pain andbleeding
NA (14)
12 62/M Abdominal pain/hematochezia/diarrhea
Whole colon Ulcerative colitis Bleeding 18 mo (15)
13 62/M Hematochezia/diarrhea Rectosigmoid Infectious colitis Severe pain 4 wk (16)
14 81/M Abdominal pain/ascitis/weight loss
Terminal ileum NA NA 6 mo (17)
15 62/M Abdominal pain/hematochezia/diarrhea
Whole colon, rectum spared
Ulcerative colitis Symptoms refractor to medical management
10 mo (15)
16 59/M Abdominal pain/constipation/incontinence
Rectosigmoid Colitis Symptoms refractor to medical management
1 mo (15)
17 62/F Abdominal pain/hematochezia/diarrhea
Rectosigmoid Idiopathicmyointimalhyperplasia
Pain and lack ofhealing
2 mo (18)
18 76/M Diarrhea/abdominal pain/weight loss
RS IBD, ischemia Severe pain 12 mo (19)
19 58/M Abdominal pain/hematochezia/diarrhea
Descendent colon, rectosigmoid
IBD, ischemia Symptoms refractor to medical management
NA (20)
20 62/F Abdominal pain/diarrhea Terminal ileum Ileitis Small bowel perforation
NA (21)
21 62/M Diarrhea Left-sided colon Ischemia Acute abdomen NA (22)
22 47/M Diarrhea/abdominal pain Rectosigmoid IBD, ischemia Symptoms refractor to medical management
9 mo Present case
M: Male; F: Female; mo: Months; IBD: Inflammatory bowel disease.

2016, Vol. 108, N.º 12 SEGMENTAL COLITIS CAUSED BY IDIOPATHIC MYOINTIMAL HYPERPLASIA OF MESENTERIC VEINS 825
Rev esp enfeRm Dig 2016;108(12):821-826
(3). IMHMV diagnosis can be based on clinical manifes-tations causing acute, progressive ulcers in the rectosig-moid colon and pathohistologic findings on the resected specimen. A biopsy is generally not helpful for diagnostic purposes since specimens that include concentric intimal thickening venules in the submucosa and deeper layers are often not obtained (9). Pathohistologic examination of a resected specimen reveals a striking pattern of scattered circumferential intimal thickening of vessels, with or with-out lymphocyte infiltration around venules and complete obliteration of venules from the submucosa to subserosa (4). Regarding treatment, complete resection of the necrot-ic segments is recommended. The postoperative clinical prognosis is generally good, with no recurrence (4).
Our patient is a typical case of this extremely rare con-dition. The results of the initial biopsy revealed nonspecific changes in the intestinal mucosa. As with other cases of IMHMV, medical therapies were ineffective. Given that subsequent biopsies suggested a possible ischemic etiolo-gy, our patient underwent a surgical resection. The histo-logical examination of the resected specimen established the diagnosis of IMHMV. Overall, this case presents an entity that is difficult to diagnose since both the endoscopic and biopsy appearance are nonspecific and only the surgi-cal specimen provides the diagnosis.
REFERENCES
1. Grendell JH, Ockner RK. Mesenteric venous thrombosis. Gastroen-terology 1982;82:358-72.
2. Hunter GC, Guernsey JM. Mesenteric ischemia. Med Clin North Am 1988;72:1091-115.
3. Abu-Alfa AK, Ayer U, West AB. Mucosal biopsy findings and venous abnormalities in idiopathic myointimal hyperplasia of the mesenteric veins. Am J Surg Pathol 1996;20:1271-8. DOI: 10.1097/00000478-199610000-00014
4. Genta RM, Haggitt RC. Idiopathic myointimal hyperplasia of mesen-teric veins. Gastroenterology 1991;101:533-9.
5. Brandt LJ, Boley SJ. AGA technical review on intestinal ischemia. American Gastrointestinal Association. Gastroenterology 2000; 118:954-68.
6. Feuerstadt P, Brandt LJ. Colon ischemia: Recent insights and advances. Curr Gastroenterol Rep 2010;12:383-90. DOI: 10.1007/s11894-010-0127-y
7. Hwang S-S, Chung W-C, Lee K-M, et al. Ischemic colitis due to obstruction of mesenteric and splenic veins: A case report. World J Gastroenterol 2008;14:2272-6. DOI: 10.3748/wjg.14.2272
8. Kao PC, Vecchio JA, Hyman NH, et al. Idiopathic myointimal hyperplasia of mesenteric veins: A rare mimic of idiopathic inflam-matory bowel disease. J Clin Gastroenterol 2005;39:704-8. DOI: 10.1097/00004836-200509000-00011
9. Mizoshita T, Tanida S, Joh T. A case of punched-out ulcer occurring in the rectosigmoid colon with sudden onset of bloody stools. Gastroen-terology 2011;141:e9-10. DOI: 10.1053/j.gastro.2010.05.092
10. Savoie LM, Abrams A V. Refractory proctosigmoiditis caused by myo-intimal hyperplasia of mesenteric veins: Report of a case. Dis Colon Rectum 1999;42:1093-6. DOI: 10.1007/BF02236711
11. Lavu K, Minocha A. Mesenteric inflammatory veno-occlusive disor-der: A rare entity mimicking inflammatory bowel disorder. Gastro-enterology 2003;125:236-9. DOI: 10.1016/S0016-5085(03)00663-2
12. García-Castellanos R, López R, De Vega VM, et al. Idiopathic myo-intimal hyperplasia of mesenteric veins and pneumatosis intestinalis: A previously unreported association. J Crohns Colitis 2011;5:239-44. DOI: 10.1016/j.crohns.2010.12.003
13. Chiang C-K, Lee C-L, Huang C-S, et al. A rare cause of ischemic proc-tosigmoiditis: Idiopathic myointimal hyperplasia of mesenteric veins. Endoscopy 2012;44(Suppl2):E54-5. DOI: 10.1055/s-0031-1291529
14. Feo L, Cheeyandira A, Schaffzin DM. Idiopathic myointimal hyperpla-sia of mesenteric veins in the elderly. Int J Colorectal Dis 2013;28:433-4. DOI: 10.1007/s00384-012-1480-0
15. Korenblit J, Burkart A, Frankel R, et al. Refractory pancolitis: A novel presentation of idiopathic myointimal hyperplasia of mesenteric veins. Gastroenterol Hepatol 2012;8:696-700.
16. 1Thomas BS. Myointimal hyperplasia of the mesenteric veins mimick-ing infectious colitis. Int J Colorectal Dis 2013;28:727. DOI: 10.1007/s00384-012-1522-7
17. Lanitis S, Kontovounisios C, Karaliotas C. An extremely rare small bowel lesion associated with refractory ascites. Idiopathic myointimal hyperplasia of mesenteric veins of the small bowel associated with appendiceal mucocoele and pseudomyxoma peritonei. Gastroenterol-ogy 2012;142:e5-7. DOI: 10.1053/j.gastro.2011.11.052
18. Wangensteen KJ, Fogt F, Kann BR, et al. Idiopathic myointimal hyper-plasia of the mesenteric veins diagnosed preoperatively. J Clin Gas-troenterol 2015;49:491-4. DOI: 10.1097/MCG.0000000000000290
19. Sahara K, Yamada R, Fujiwara T, et al. Idiopathic myointimal hyperplasia of mesenteric veins: Rare case of ischemic colitis mimicking inflammato-ry bowel disease. Dig Endosc 2015;27:767-70. DOI: 10.1111/den.12470.
20. Abbott S, Hewett P, Cooper J, et al. Idiopathic myointimal hyperplasia of the mesenteric veins: A rare differential to be considered in idiopathic colitis. ANZ J Surg 2015 Jul 3. [E-pub ahead of print] DOI: 10.1111/ans.13210.
21. Laskaratos F-M, Hamilton M, Novelli M, et al. A rare cause of abdomi-nal pain, diarrhoea and GI bleeding. Gut 2015;64:214. DOI: 10.1136/gutjnl-2014-308319
22. Zijlstra M, Tjhie-Wensing JW, Van Dijk M, et al. Idiopathic myointi-mal hyperplasia of mesenteric veins: An unusual cause of diarrhoea. Ned Tijdschr Geneeskd 2014;158:A7752.