sea•md hospitales hima•san pablo
DESCRIPTION
Presentación realizada el jueves, 3 de noviembre de 2011TRANSCRIPT
Doctor’s Center Hospital
Bayamón & Santurce

Médicos invitados:
• Iván del Toro, MD
• Director Médico HIMA•San Pablo Caguas
• Centro de Neurociencias
• Mario Polo, MD - Neuroradiólogo
• Luis Almodóvar, MD - Neurocirujano Oncólogo
• Ulises Nobo, MD - Neurólogo Vascular
• Ignacio Pita, MD
• Neurólogo Especialista en Epilepsia
• Cardiología Intervencional
• Carlos Nieves, MD
• Cardiólogo Invasivo
• Centro de Quemaduras
• Amin Jaskille, MD – Cirujano e Intesivista
• Especialidades Pediátricas y Adolescentes
•Marcos Pérez-Brayfield, MD – Urólogo
•Aurelio Segundo, MD – Cirujano General

Mario Polo, MD Interventional & Diagnostic Neuroradiology
Neurointerventional Surgery Board Certified by the American Board of Radiology

Neurointerventional Surgery at HIMA•San Pablo

Our Neurovascular Team

Bi-Planar Angiography Suite


Subarachnoid Hemorrhage
Clinical Presentation
• Sudden Onset Severe Headache
– “the worst headache of my life”
– Nausea
– Vomiting
– Seizures
– Loss of consciousness
– Neck pain and/or rigidity
– Coma
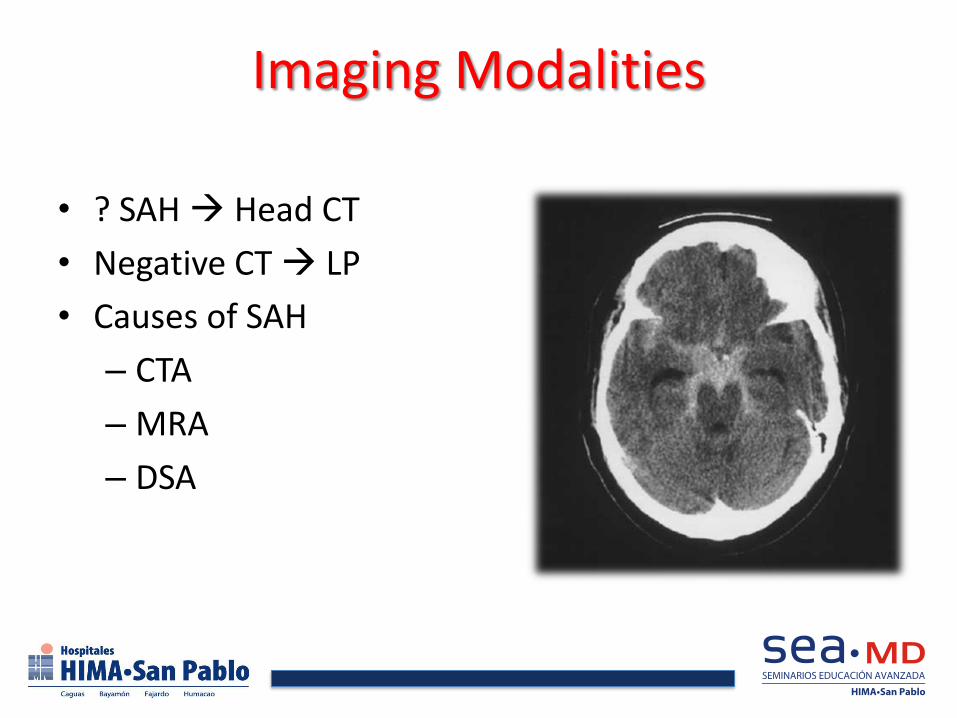
Imaging Modalities
• ? SAH Head CT
• Negative CT LP
• Causes of SAH
– CTA
– MRA
– DSA


Initial Management
• ABC – GCS <8, intubation and sedation – Cardiac monitor: arrythmia – CBC, PT, PTT, CMP, CXR.
• If severe hydrocephalus, no neurosurgeon, may consider lumbar puncture – Gradual, avoid overdrainage.
• CTA with 3-D reconstruction • MRA • Cerebral angiogram: Gold standard.
– In institution with endovascular neurosurgery.
Luis Almodóvar, MD Neurocirujano Oncólogo
Director de Neurología Oncológica
• Neurocirugía Endovascular & Vascular
– Dra. María M. Toledo
• Neurocirugía Pediátrica/Neurocirugía de Espina/
Epilepsia
– Dr. Iván Sosa
• Neurocirugía Oncológica & Cyberknife
– Dr Luis Almodóvar
• Neurocirugía General
– Dr. José Santos Picó
• Neuroradiología Endovascular & Intervencional
– Dr. Mario Polo

History
• The first recognized resection of a primary brain tumor in history was performed by Mr. Rickman Godless in London, England, November 25, 1884
• On February 25, 1886, in San Francisco, California the first documented resection of a primary brain tumor in the United States was performed by Drs. Hirschfelder and Morse
History
• More than 50 years ago the first cases of awake craniotomy for brain tumor resection were done in Montréal, Quebec
• Refinement in surgical techniques and outcomes in last decades due to
– Improved surgical instrumentation
– Development of microsurgical techniques
– Better understanding of the disease process
– Advances in medical therapy
– Use of sereotactic approaches – neuronavigation, etc
Primary Brain Tumors
• Incidence - 14 cases per 100,000 people per year
– 35,000 new cases per year in the US
• Prevalence – 130.8 per 100,000 living (year 2000)
• 48-60% are neuroepithelial tumors
– Mostly glial tumors
• 1.4% of all cancers, 2.4% of cancer-related deaths
Primary Brain Tumors
• Increased tumor incidence in the elderly
– Improved diagnostic procedures (CT/MRI)
– More availability of neurosurgeons
– Evolving strategies to treat the elderly
• Age – median age at onset is 57 years
– Duration of exposure required for malignant transformation
– Genetic alterations leading to clinical disease
– Poorer immune surveillance with advancing age

• Sex
– Gliomas - more common in males
– Meningiomas – female to male ratio is 2:1
– Sellar tumors and cranial / spinal nerve tumors – equal incidence
• Ethnic Variations
– Gliomas – affect Caucasians more than african americans
– Meningiomas – affect Caucasians and african americans equally
Primary Brain Tumors

Survival and Prognostic Factors
• 5-year survival rate in US – 20% (All ages and tumor types)
– Primary malignant brain tumors in children <14 y/o- 72% 5-year survival
• Survival strongly related to age and tumor type
– GBM patients → poorest survival in all age groups
– For any given tumor type – younger do better than older
• Exception – medulloblastoma, poorer prognosis if < 3y/o
• In Europe
– Slightly better 5-year survival for women (20% vs. 17% for men)
• Prognostic factors
– Age
– Histologic type
– Location
– Extent of Resection
Survival and Prognostic Factors
Preoperative Imaging
• MRI – gold standard for detecting brain tumors
• MRS (magnetic Resonance Spectroscopy)
– Measures metabolite levels in a brain “voxel”
– Helps differentiate neoplasm from inflammatory or demyelinating conditions
– Aids in detecting progression of disease

MR Spectroscopy

Preoperative Imaging
• Functional MRI (fMRI)
– Detects small changes in blood volume and T2 signal that occur in eloquent cortex during physiologic activation
– Allows preoperative functional mapping
– Helps tailoring resection in individual patients
• MR Tractography
– Allows visualization of white matter tracts in relationship to a tumor
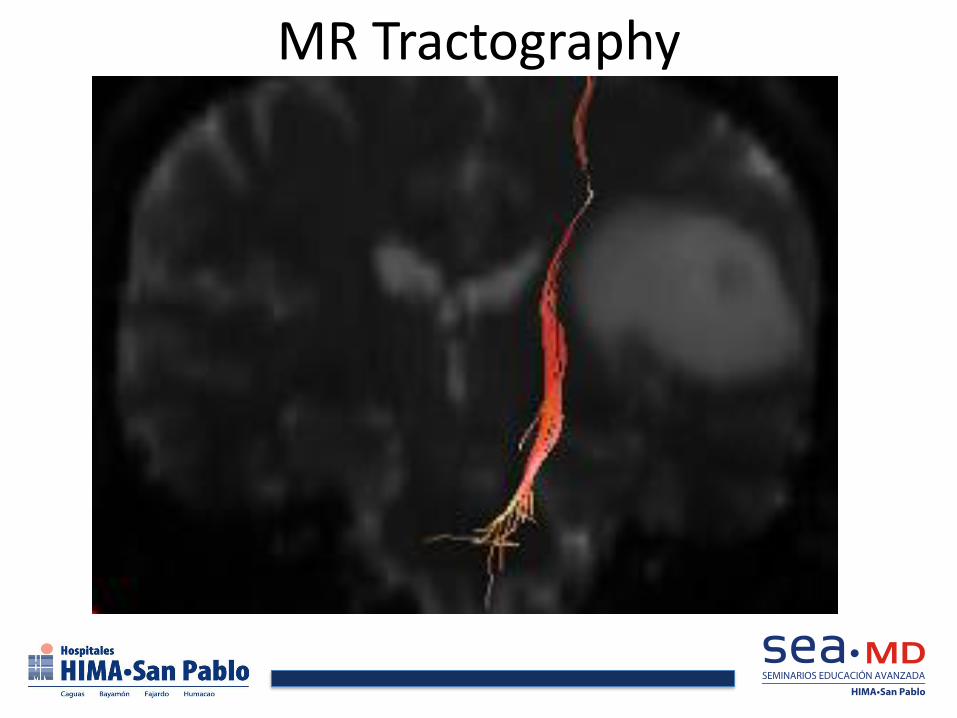
MR Tractography

MR Tractography

Surgical Management
• Goals of surgical management
– Biopsy – to obtain histologic diagnosis
– Cytoreduction – maximize removal of the tumor with optimal preservation of neurological function
– Symptomatic relief
– Optimization of oncologic benefit by minimizing tumor burden to increase effectiveness of adjuvant therapies
Biopsy
• Most often a closed stereotactic procedure
• Can be frame-based or frameless
• Associated with low complication rate – 6% morbidity
– 2% mortality
– 8% failed biopsy due to insufficient tumor
• Limited mostly to a small portion of patients with suspected gliomas – Deep, diffuse, multiple or patient in poor condition
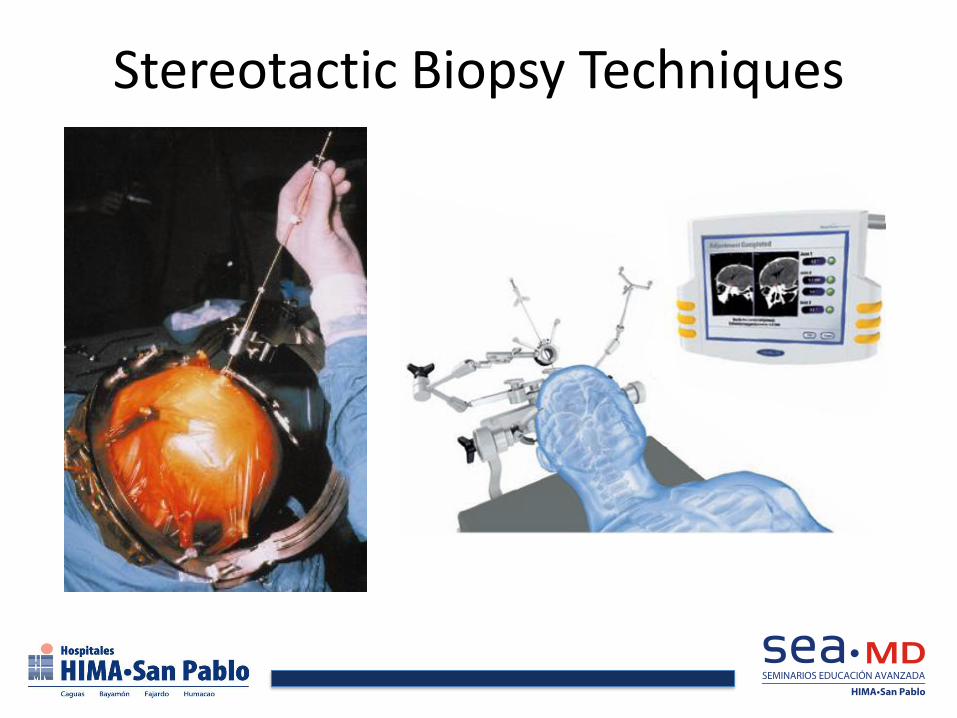
Stereotactic Biopsy Techniques

Biopsy
• Incorrect pathological diagnosis in up to 30%
– Most common misdiagnosis: undergrading a malignant astrocytoma
– Reduced by serial sampling along the radius of a tumor
– Best if examined by experienced neuropathologist

Computer-Assisted Stereotactic Resection
• Allows for precise location of the tumor in three-dimensional space
• Helpful for technically challenging tumor locations
• Minimizes injury and exposure of critical brain areas

Neuronavigation
• Allows a three-dimensional stereotactic correlation between the lesion of interest, neuroimaging studies and the patient’s anatomy
• Components
– Immobilization frame
– Computer system
– Localization device and registration process
– Transmission of real-time data
– Input from specially-acquired neuroimages

Neuronavigation
• Helps the surgeon better plan the surgery and approach to the tumor
• Allows better assessment of the extent of resection intraoperatively
• Aids in the surgeon to localize the tumor even when anatomical landmarks have been displaced by tumor or edema
• Disadvantages – does not take into account brain shift during the
surgery

Neuronavigation
Intraoperative Imaging • Sonography
– Advantages • Generates real-time images
• Easy to use
• Allows for assessment of cyst drainage, tumor resection and allows
• Can be integrated with navigational systems to mathematically calculate brain shift
– Disadvantages • Cannot reliably discern normal from abnormal tissue
• Blood products in surgical cavity may lead to misinterpretation of images
Intraoperative Imaging
• Intraoperative MRI
– Advantages
• Enables imaging of the patient during the resection
• Allows re-registration of the patient’s data to account for the resected tumor
• Eliminates the inaccuracies created by brain shift
• May help detect residual tumor not clearly visible and that may warrant further resection

Intraoperative MRI
Intraoperative MRI
• Disadvantages
– Needs MRI-compatible instrumentation, anesthesia machine and monitoring equipment
– Expensive
– Contrast extravasation due to surgical insult to blood brain barrier may be misinterpreted as tumor
Awake craniotomy
• Goal
– Maximize extent of resection while minimizing neurologic morbidity
• Indications
– Tumors in eloquent cortex
• Motor cortex
• Near speech eloquent areas

Awake craniotomy
Stimulation Mapping Techniques
• Involves stimulation of cortical and subcortical structures to identify functional tissue in and around the tumor
– Minimizes the risk of permanent postoperative deficits
– Only method for identifying descending subcortical motor, sensory and language tracts

Intraoperative Motor Mapping
• Indications:
– Gliomas located within or adjacent to:
• Rolandic cortex
• Supplementary motor area
• Corona radiata
• Internal capsule
• uncinate fasciculus

Cortical Language Localization
• Traditional cortical speech areas
– Broca’s area – posterior portion of inferior frontal cortex
– Wernicke’s area – perisylvian temporoparietal cortex
• Cortical language localization is variable in each individual
– Does not follow a reproducible pattern in the population
• Standard dominant temporal lobe resections > permanent post-op speech deficits

Surgical Preparation and Technique
• Patient placed in appropriate position for exposure
• Extremities and pressure points padded
• Core temperature kept within 1°C of normal with heating blanket
• General anesthesia induced/maintained – Propofol or alfentanil drip used for sedation
– Foley placed, IV antibiotics given
• Area shaved, cleaned, incision marked and local anesthesia infiltrated – May define tumor borders with neuronavigation

• Surgical Access
– Incision opened and flap raised
– Wide craniotomy done to expose tumor and surrounding brain
• Ensures availability of enough cortical sites for testing
– Dura infiltrated with xylocaine/marcaine
• Dura is pain sensitive
• Minimize discomfort while patient is awake
– Tumor located with ultrasound or navigation
Surgical Preparation and Technique
Identification of Motor Cortex and Subcortical Pathways
• Identify the motor cortex – Use bipolar electrode (5mm separation) for 2-3 secs.
– Stimulation parameters: • 2 to 16 mA, 60Hz biphasic square-wave pulse, 1.25 msec pulse
– Use EMG recordings and visual observation of movement to increase sensitivity and reduce stimulation • Not necessary to go beyond 16 mA
– Have ice-cold Ringer’s lactate to irrigate if focal seizure
– Identify lower motor cortex (face/hand movements)
– Place strip electrode along falx to evoke leg movements • Safe – lack of bridging veins at leg motor cortex

• Identify subcortical tracts – Similar stimulation parameters
– Very important due to • Possible presence of functional motor, sensory or
language eloquent tissue within or surrounding the macroscopically obvious tumor
• Presence of functional tissue in infiltrated brain
• Do post-resection stimulation – The patient will likely recover from post-op deficits
if stimulation reveals intact tracts
Identification of Motor Cortex and Subcortical Pathways

Identification of Language Sites
• Keep the patient awake
• Stimulate with bipolar electrode with electrocorticography in progress
– If after-discharge potentials seen on monitor decrease until no after-discharge seen
• Ask the patient to count from 1 to 50 while stimulating near inferior motor strip
– Complete speech arrest signifies location of Broca’s area

Identification of Language Sites
• Present the patient with object-naming slides
– Patient asked to name objects during stimulation
– All sites essential for naming are marked
– Sites checked three times
• Distance of resection to language site is the most important factor predicting post-op deficits
– Ideal distance from language site is 1 cm or more
Prognostic Significance of Surgery
• Low grade gliomas
– Controversial but evidence favors a positive effect in outcome after extensive resection
• High grade gliomas
– Statistically significant impact on survival (survival advantage) seen if ≥ 98% of tumor removed
Brain Metastases
• More than 100,000 new cases of brain metastases each year in the US
– 30-60% originate from a lung primary
• Non-small cell lung cancer (80%)
• Small-cell lung cancer
• 33% of non-small cell lung cancer present with brain mets
– 14-20% originate from a breast primary

Brain Metastases
• Indications for resection – Single metastatic lesions – improved survival
compared to whole-brain radiotherapy (WBRT) alone, to establish a diagnosis • 8-9 months with resection +WBRT vs. 3-4 months for
WBRT alone
– Multiple lesions – palliative for relief of mass effect of dominant lesions • Consider extent of systemic disease, tolerability for
surgery and comorbidities
• Can result in survival outcomes similar to single mets

Approaches By Tumor Location

Trans-Sphenoidal • Indications
– Tumors in the sellar/pituitary region – Microadenomas
– Macroadenomas
– Meningiomas
– Craniopharyngiomas
– Rathke’s cleft cyst
– Metastasis
– Etc…
• Contraindications
– Aberrant carotid artery
– Extensive suprasellar extension
Trans-sphenoidal
• Preop work-up
– Pituitary hormonal panel – Prolactin
– Growth hormone
– ACTH
– TSH
– Cortisol
– IGF-1
– FSH, LH
– Evaluation by endocrinologist
– Ophthalmologic evaluation for visual field testing

Trans-Sphenoidal

Trans-sphenoidal

Transcranial Approaches

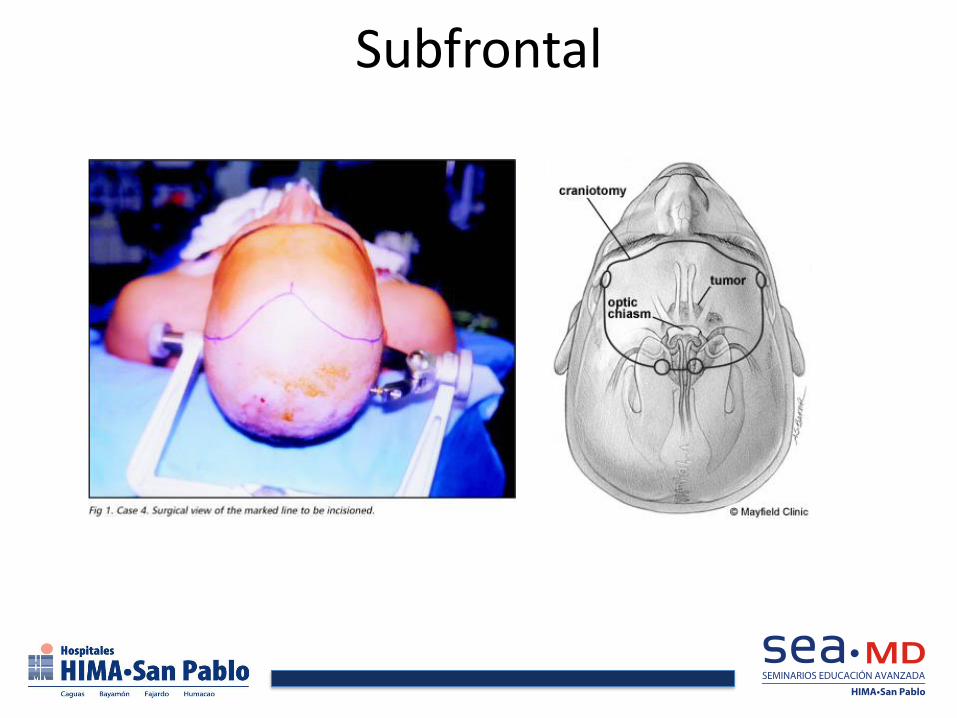
Subfrontal
• Indications
– Tumors in the anterior cranial base
– Midline tumors in the suprachiasmatic / suprasellar region with significant suprasellar extension
• Common lesions in this location • Olfactory groove or planum sphenoidale meningiomas
• Large pituitary tumors
• craniopharyngiomas
Subfrontal
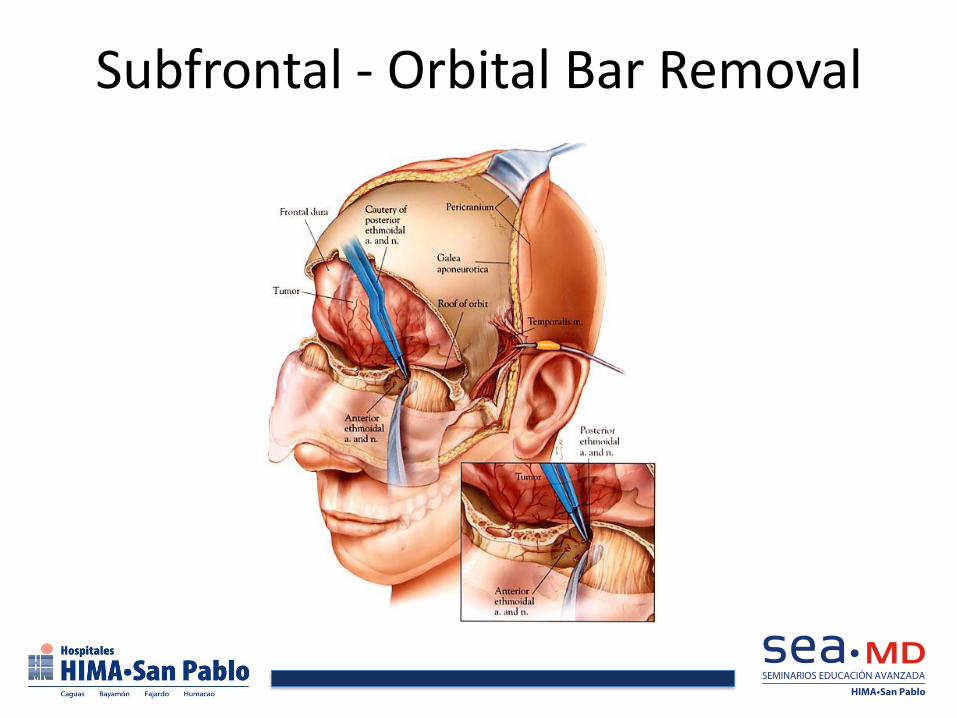
Subfrontal - Orbital Bar Removal

Subfrontal

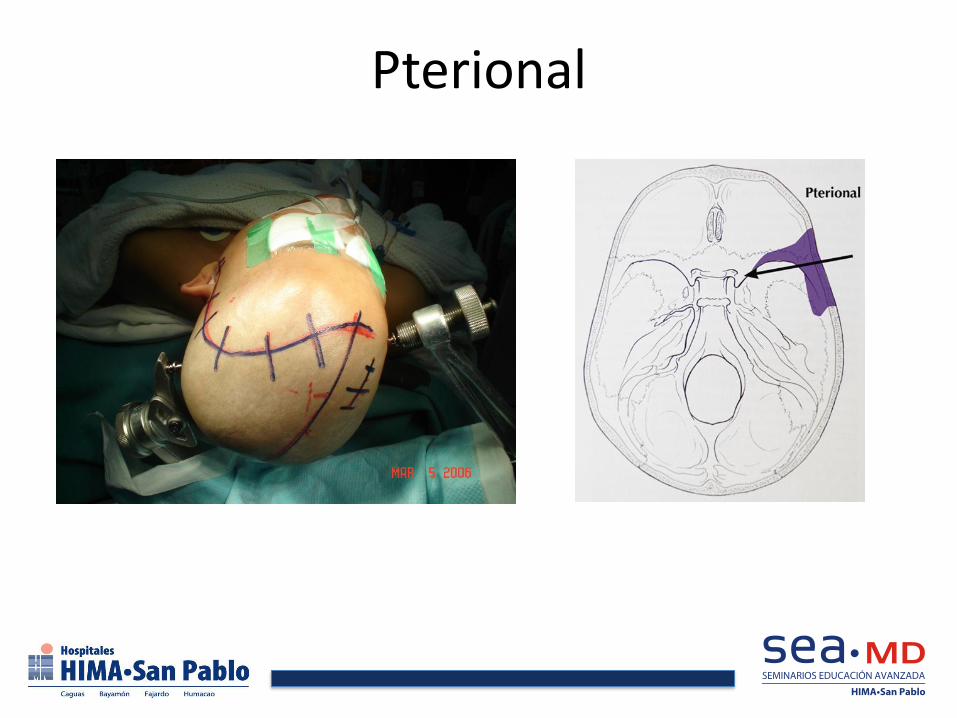
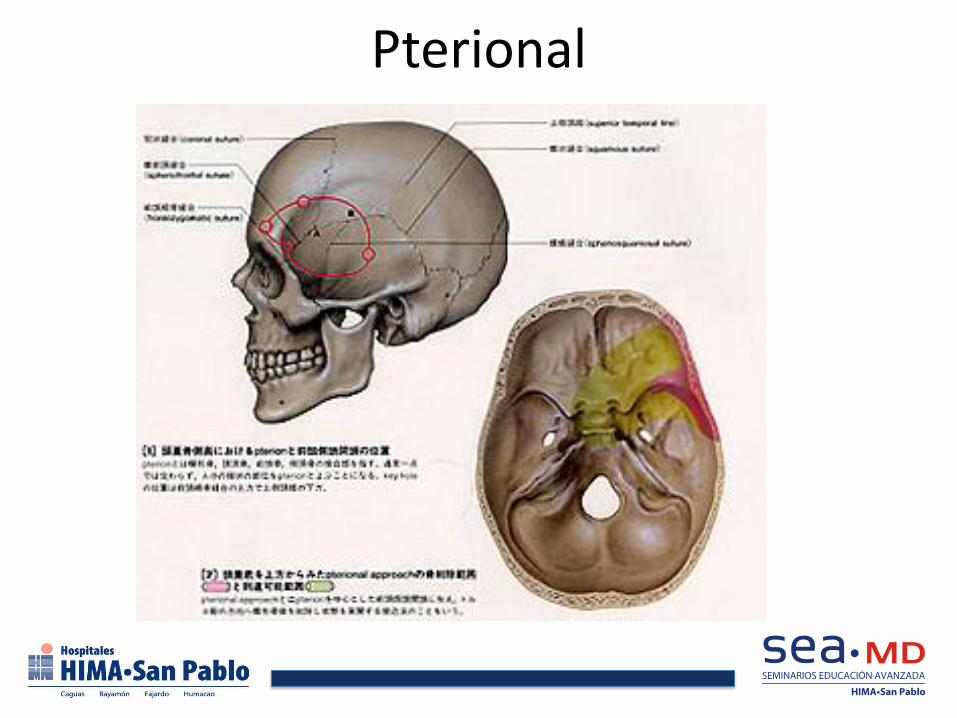
Pterional
• Based on the pterion
• Indications
– Tumors in the sphenoid ridge
– Midline tumors near the carotid artery or optic nerves
– Frontotemporal tumors
• Very versatile approach
– Can be modified or extended to allow access to a large portion of the cranial base
Pterional
Pterional

Pterional

Interhemispheric
Interhemispheric Approach
• Indications
– Midline hemispheric tumors
– Intraventricular tumors, including third ventricular tumors
• Common tumors resected by this approach
– Colloid cysts
– Intraventricular meningiomas
– Central neurocytomas
– Hypothalamic hamartomas
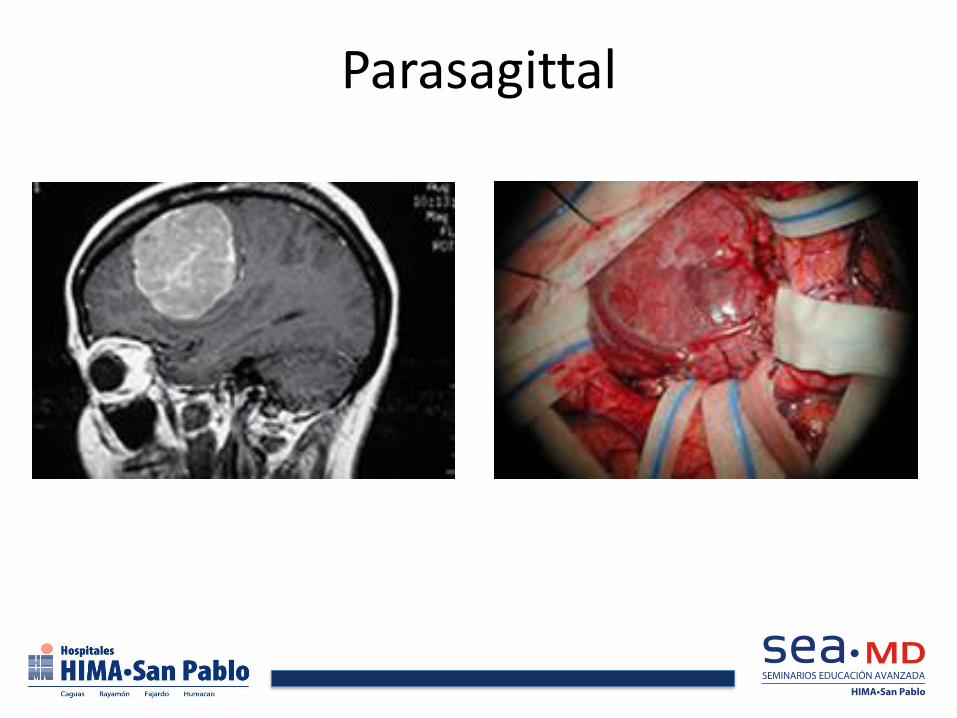
Parasagittal

Retromastoid
• Indications
– Tumors in the cerebellopontine angle and lateral aspect of the cerebellum
• Common tumors treated by this approach
– Acoustic schwannomas
– Meningiomas
– Epidermoid tumors
– Metastasis
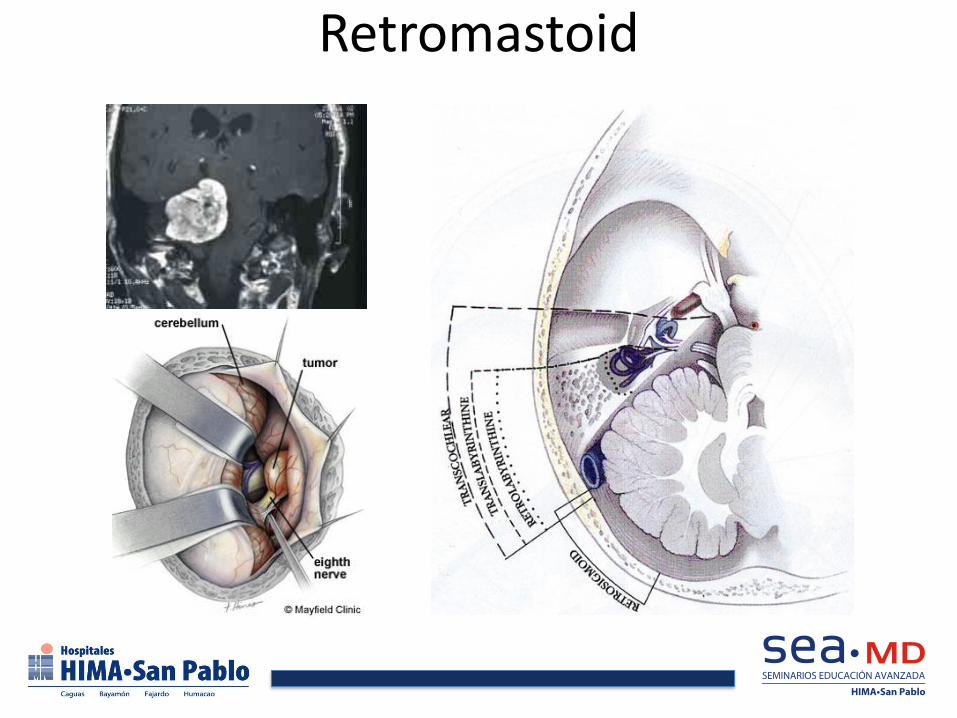
Retromastoid
Suboccipital • Indications
– Posterior fossa tumors of the midline or cerebellar hemispheric tumors
– Tumors of the fourth ventricle
• Tumors commonly treated by this approach • Pilocytic astrocytomas
• Medulloblastomas
• Ependymomas
• Hemangioblastomas
• meningiomas
• metastasis

Suboccipital
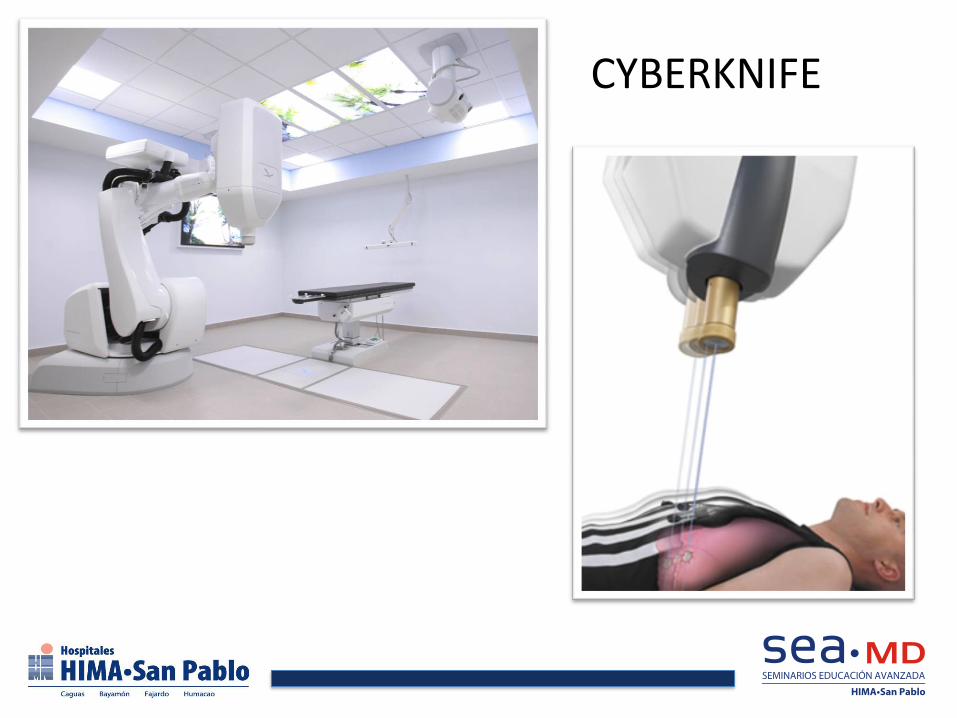
CYBERKNIFE
DR. ULISES NOBO Stroke Unit Director
Board Certified Psychiatry & Neurology Board Certified Neurology & Vascular Neurology

STROKE CENTER WHY?
3RD CAUSE OF DEATH 1ST CAUSE OF DISABILITY IN ADULTS
OVER 65 BILLION DOLLARS IN COSTS
IT CAN BE PREVENTED
IT CAN BE TREATED
PUERTO RICO IS IN DESPERATE NEED FOR THIS KIND OF RESOURCES

1 IN 3 ADULTS
HAS SOME FORM OF
CARDIOV.DISEASE
EVERY 26 SECONDS
SOMEBODY SUFFERS A
HEART ATTACK
EVERY 40 SECONDS
SOMEBODY SUFFERS A
STROKE
MOST OF THESE EVENTS CAN BE PREVENTED !

TIME IS BRAIN QUANTIFIED
NEURONS
LOST
SYNAPSES
LOST
MYELINATED
FIBERS LOST
ACCELERATED
AGING
PER
STROKE
1.2
BILLION
8.3
TRILLION
7140 KM 36 YEARS
PER
HOUR
120
MILLION
830 BILLION 714 KM 3.6 YEARS
PER
MINUTE
1.9
MILLION
14 BILLION 12 KM 3.1 WEEK
PER
SECOND
32, 000 230
MILLION
200 METERS 8.7 HOURS
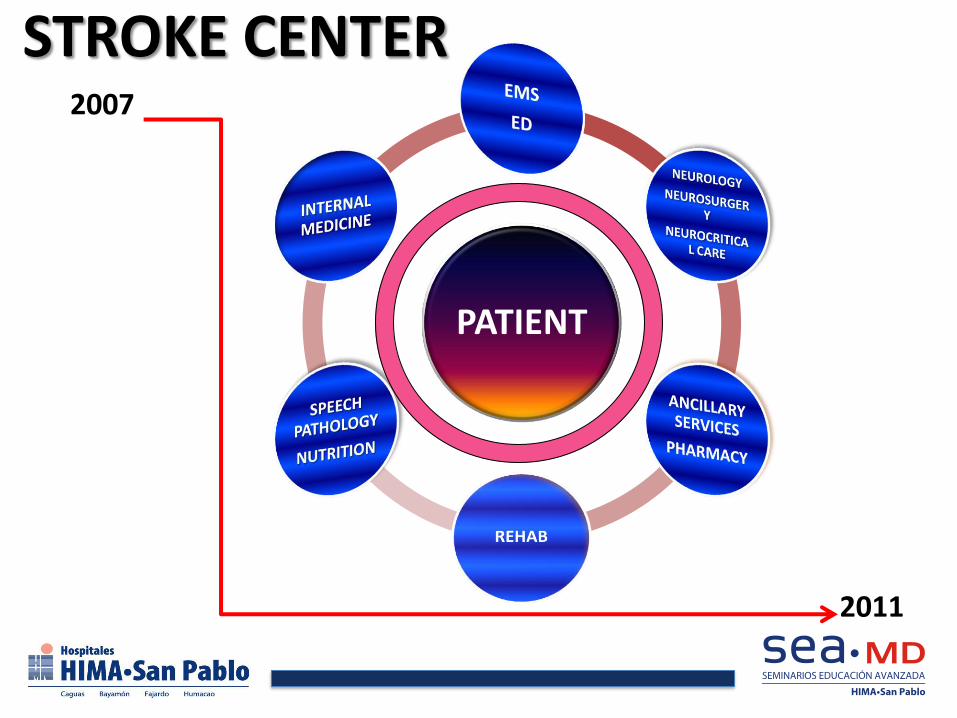
STROKE CENTER
PATIENT
2007
2011

NEUROLOGY
STROKE CENTER
MS CENTER
EPILEPSY UNIT
NEUROSURGERY
VASCULAR & ENDOVASCULAR NEUROSURGERY
NEUROSURGERY& ONCOLOGY
BACK NEUROSURGERY &
PEDIATRICS
NEURO-INTENSIVE UNIT
Dra. Yadira Dacosta
Dr. Ulises Nobo Dr. Abiezer Rodriguez
Dr. Ignacio Pita Dr. Horacio Dauvon
Dra. Marimerce Toledo
Dr. Luis Almodovar
Dr. Ivan Sosa
Dra. Gloria Rodriguez Dra. Rosangela Fernandez

NINDS 1 – 2
0 1 2 3 4 5 6 7 8 9 HS
A S K
ATLANTIS
ECASS 1
ECASS 2
MAST - E
MAST - I
LARGE TRIALS OF IV TPA AND STREPTOKINASE
ECASS-III
PROACT-II
MULTI-MERCI
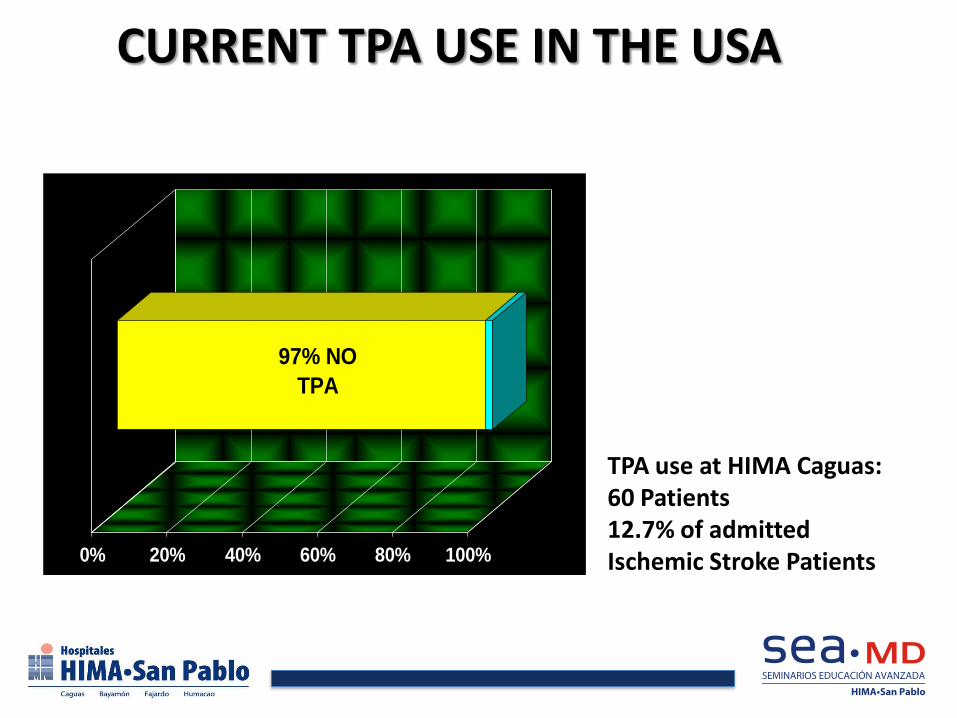
CURRENT TPA USE IN THE USA
97% NO
TPA
0% 20% 40% 60% 80% 100%
TPA use at HIMA Caguas: 60 Patients 12.7% of admitted Ischemic Stroke Patients
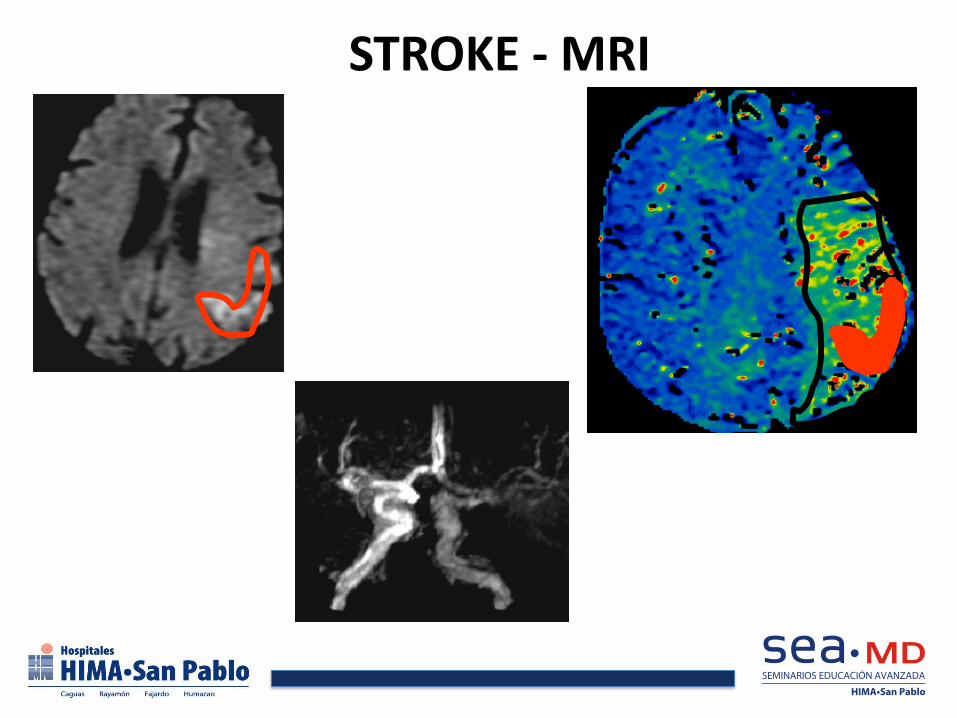
STROKE - MRI
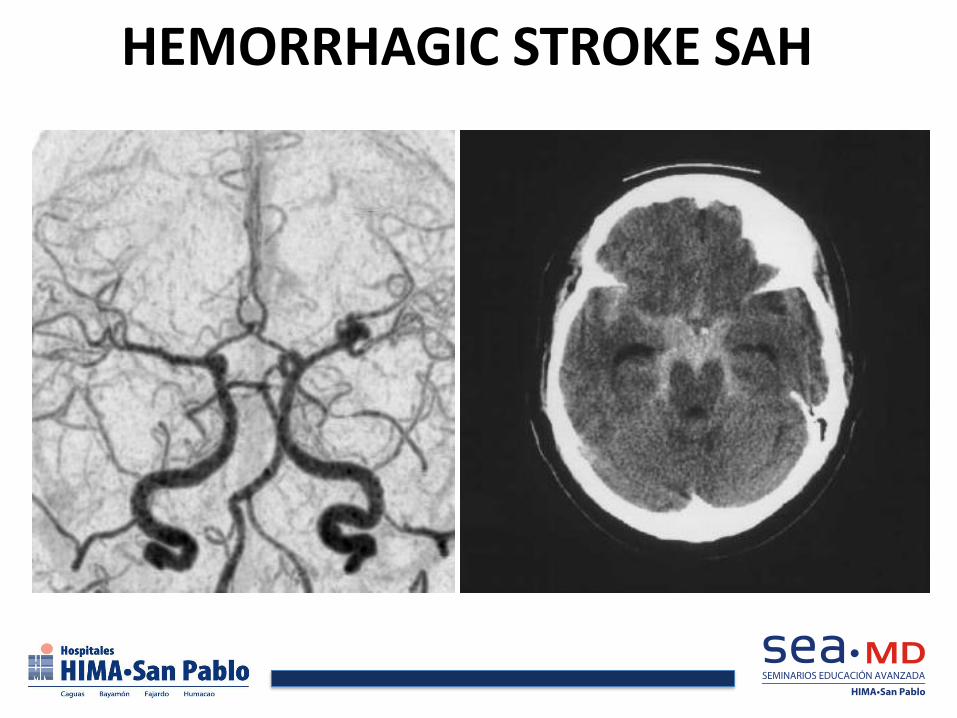
HEMORRHAGIC STROKE SAH

SAVES LIVES
AHA
STROKE MEASURES


Ignacio Pita, MD Director del Centro de Epilepsia
Neurólogo Especialista en Epilepsia

CENTRO DE EPILEPSIA

93
Epilepsy
• Epilepsy is a disorder of brain function characterized by the occurrence of periodic or unpredictable seizures1
• Epilepsy and seizures affect 2.5 million Americans of all ages2
• 315,000 children ≤14 years have epilepsy
• 600,000 persons ≥65 years have epilepsy
• Approximately 181,000 new cases of epilepsy and seizures occur each year2
• In 1995, it was estimated that epilepsy cost the nation approximately $12.5 billion annually2
1. Mattson. Neurology. 1998;51(suppl 4):S15-S20. 2. Epilepsy Foundation. Epilepsy and seizure statistics. Available at: http://www.epilepsyfoundation.org/answerplace/statistics.cfm.

94
pregabalin
95
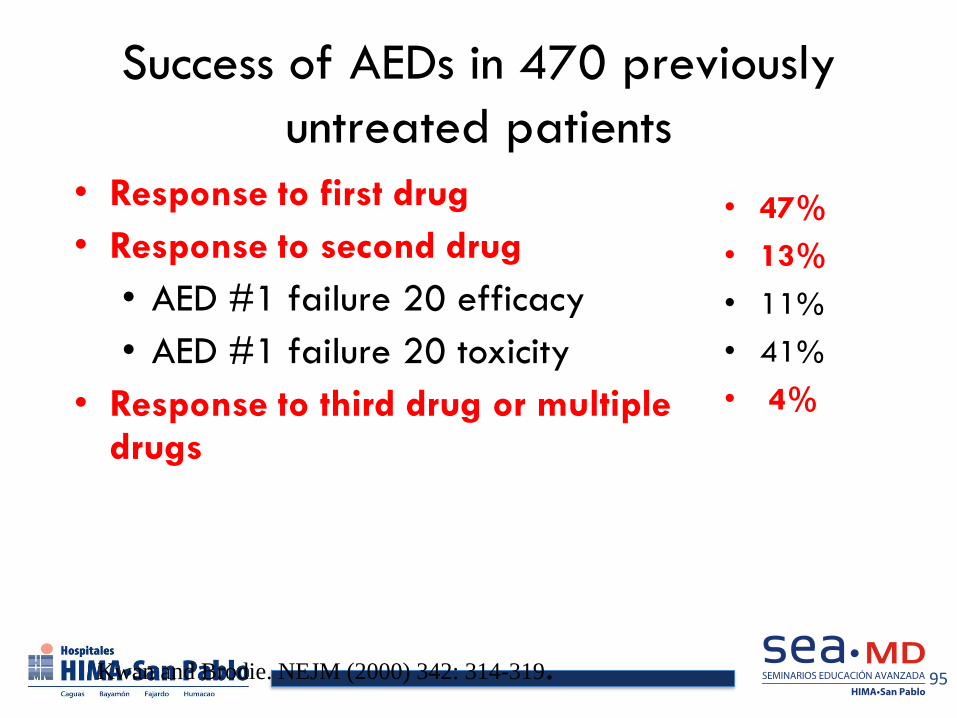
Success of AEDs in 470 previously
untreated patients
• Response to first drug
• Response to second drug
• AED #1 failure 20 efficacy
• AED #1 failure 20 toxicity
• Response to third drug or multiple drugs
• 47%
• 13%
• 11%
• 41%
• 4%
Kwan and Brodie. NEJM (2000) 342: 314-319.

96

97
Intractable Epilepsy
• Early Referral for EEG – Video monitoring
– Diagnostic evaluation – Intractable versus Pseudointractable epilepsy
– Pre-surgical Evaluation
• Seizure semiology
• Interictal EEG
• Ictal EEG localization
• Further testing
98
Seizure Surgery Depends on
Congruence of Test Findings
• EEG-Video monitoring-ictal and interictal
• MRI
• Positron Emission Tomography
• Neuropsychological Testing
• WADA Test (Localize memory / language)
• Ictal Spect
• Magnetic Resonance Spectroscopy
• fMRI
• MEG

Comprehensive Epilepsy Program
• Epilepsy Monitoring Unit
• Epileptologist
• Epilepsy Neurosurgeon
• Endovascular Neurosurgeon
• Neuropsychologist
• Specialized Nurses and EEG Technicians

VIDEO/EEG
• Simultaneous recording of clinical and electrographic findings in patients with history or suspected epilepsy

Epilepsy Monitorin Unit
• Diagnostic procedure.
• In hospital procedure
• Duration: 3-7 days

Epilepsy Monitoring Unit
• Facilities:
– Six (6) private bedroom
– 360 degree camera with infrared light for
nocturnal recording
– Continuous monitoring by trained EEG tech
and nurses
Indications
• Diagnosis – epileptic versus non-epileptic events
• Classification – Characterize the epileptic event
• Intractable epilepsy
• Localization of the ictal focus for presurgical evaluation

Advantages
• By confirming the diagnosis, classifying the epilepsy type and indentifying the ictal focus a well developed treatment plan can be established to better utilize health care services and improve quality of life

Insurance Coverage
• 450 patients evaluated • Current waiting list 2-3 weeks • Insurance with contract
– SSS – SSS OPTIMO – MEDICARE – MCS – MCS CLASSICARE – HUMANA – HUMANA REFORMA
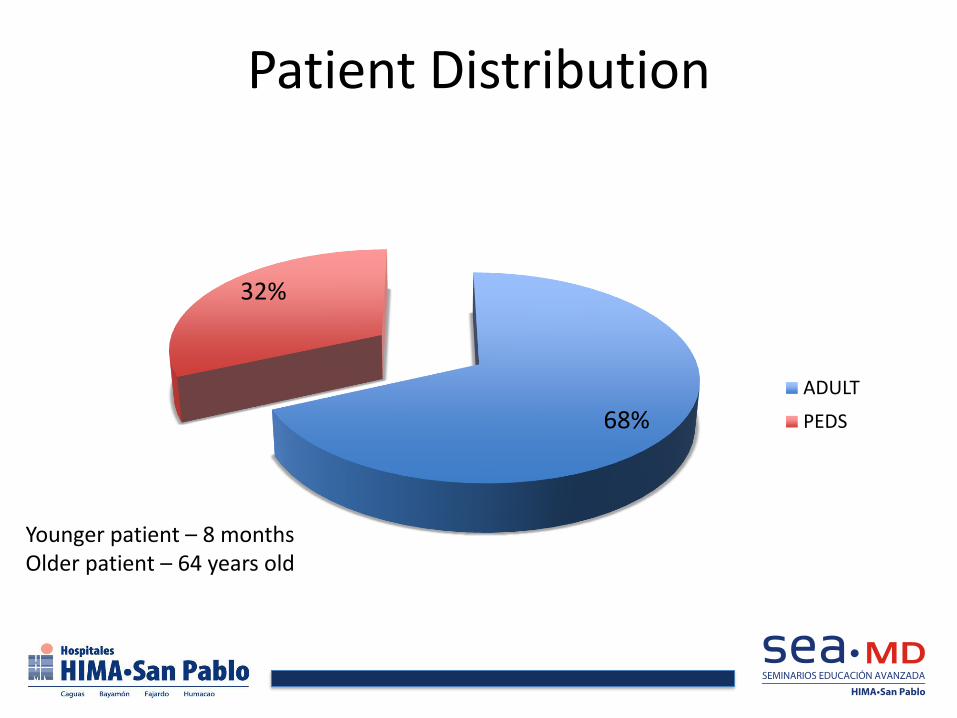
Patient Distribution
68%
32%
ADULT
PEDS
Younger patient – 8 months Older patient – 64 years old
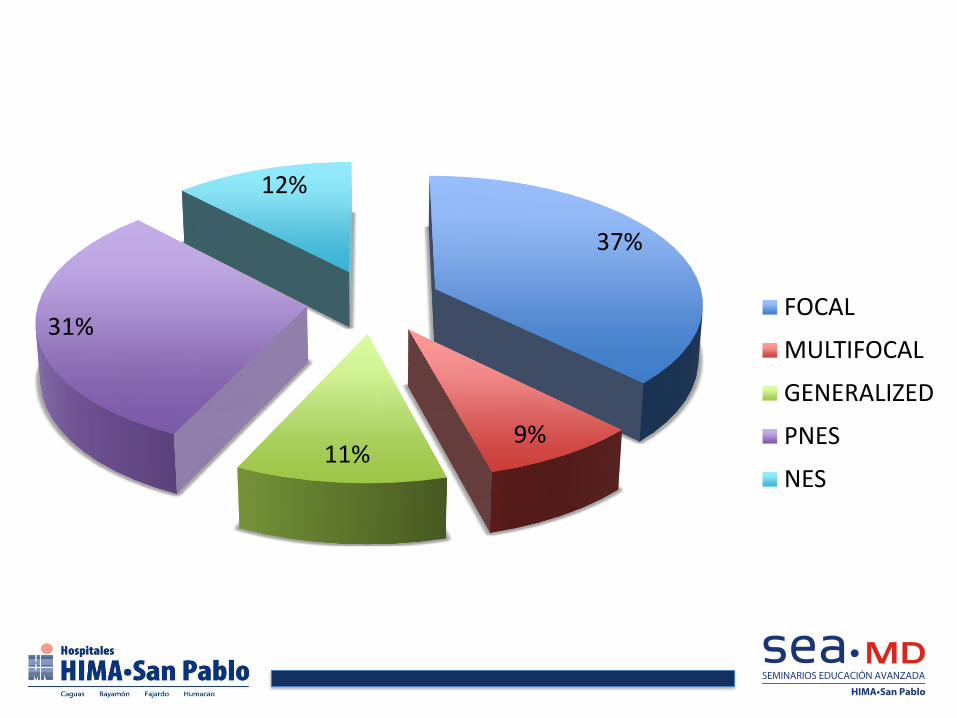
37%
9% 11%
31%
12%
FOCAL
MULTIFOCAL
GENERALIZED
PNES
NES
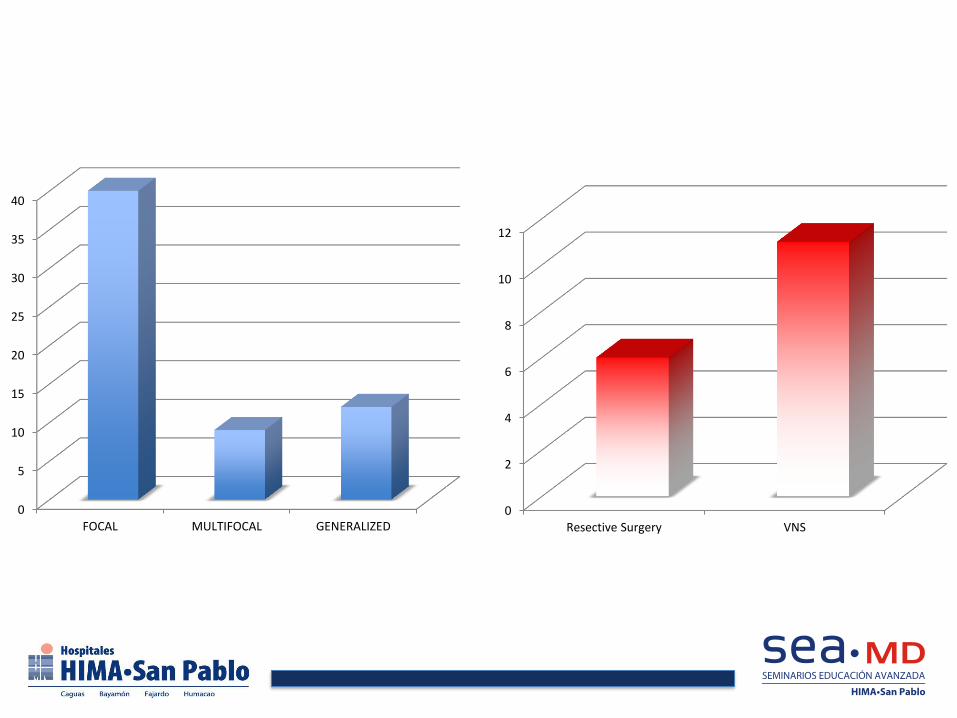
0
5
10
15
20
25
30
35
40
FOCAL MULTIFOCAL GENERALIZED 0
2
4
6
8
10
12
Resective Surgery VNS
109
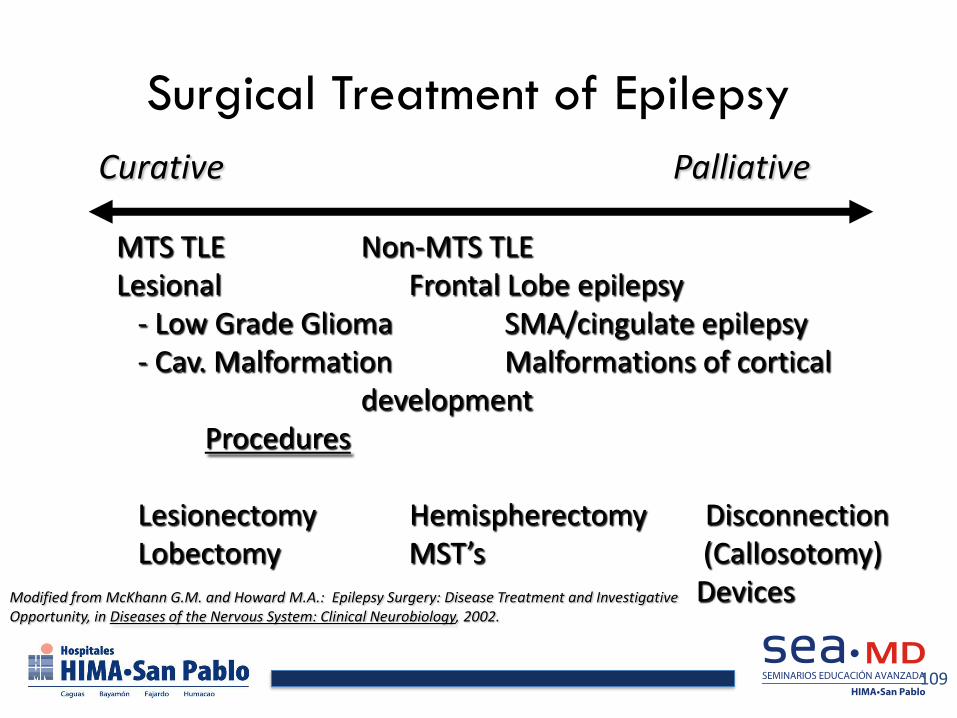
Surgical Treatment of Epilepsy
Modified from McKhann G.M. and Howard M.A.: Epilepsy Surgery: Disease Treatment and Investigative Opportunity, in Diseases of the Nervous System: Clinical Neurobiology, 2002.
Curative Palliative MTS TLE Non-MTS TLE Lesional Frontal Lobe epilepsy - Low Grade Glioma SMA/cingulate epilepsy - Cav. Malformation Malformations of cortical development Procedures Lesionectomy Hemispherectomy Disconnection Lobectomy MST’s (Callosotomy) Devices
110
Seizure Surgery Outcome
• Mayo
– MTS MRI with concordant interictal/ictal EEG had 90% SZ-Free rate
– MTS MRI with EEG discordant had 60% SZ-free rates
– Neocortical Lesional had 50-70% SZ-free rate
– Neocortical non-lesional had 20-30% SZ-free rate with additional 25% having SZ reduction of at least 80%
111
Practice Parameter: Temporal Lobe and Localized Neocortical
Resections for Epilepsy
• Level A evidence for temporal lobectomy in
pharmacoresistant patients
• Insufficient evidence to make recommendations
for extratemporal resections
Neurology 2003: 60:538-547

112
Vagus Nerve Stimulation
Reprinted with permission.

FURTHER DEVELOPMENT

114
115
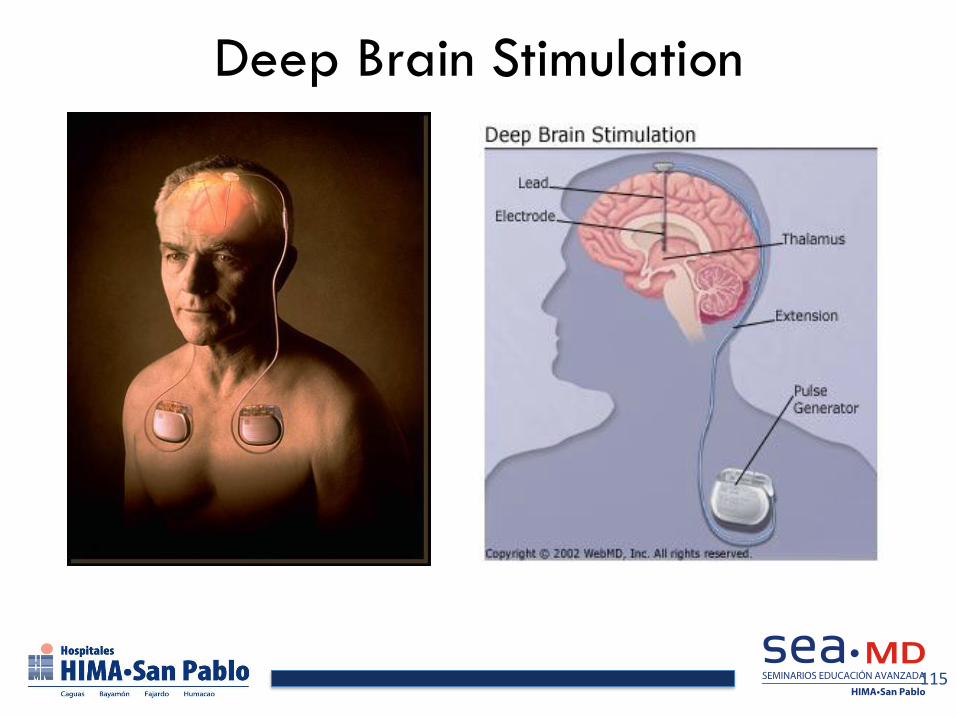
Deep Brain Stimulation

116
Responsive Neurostimulation

Carlos Nieves, M.D.,F.A.C.C. Director de Cardiología HIMA•San Pablo Bayamón
Cardiólogo Intervencional
Overview of Cardio Vascular Services at HIMA San Pablo Hospital
• General and Non-Invasive Cardiology
• Invasive and Interventional Cardiology
• Cardiovascular Surgery
• Vascular Surgery
• Endovascular Interventions
• Electrophysiology

Non Invasive Cardiology
• 20 Clinical Cardiologists
• Telemetry monitoring beds
• ICU
• Transthoracic Echocardiography
• Transesophageal Echocardiography (24)
• Myocardial Perfusion Imaging /Exercise and Pharmacologic Stress Testing and MUGA
• CTA of Coronaries

Interventional Cardiologists
• Rene Perez Rios, M.D., Director CCL
• Humberto Quintana Irazola, M.D.
• Steven Rivas Marquez, M.D.
• Carlos M. Nieves La Cruz, M.D.
Invasive and Interventional Cardiology 2010
• Right Heart Catheterization (183)
• Coronary Angiography, Lt. Heart Cath (2,298)
• PCI: Coronary Stenting : DES > BMS (1,073) Laser Coronary Atherectomy
• Aspiration Thrombectomy
• IABP: Intraortic Balloon Pump
• IVUS: Intravascular Ulrasound for intermediate lesions and complex coronary interventions.
Electrophysiology
• Single and Dual Chamber Permanent Pacemakers (121)
• ICD Implantable Cardioverter Defibrillator (56)
• Bi-Ventricular Pacing for patients with CHF and LBBB or wide QRS (29)
• Implantable prolonged monitoring device
• Electrophysiologists: Daniel Arzola M.D.
• Near future: Ablation (SVT, WPW, Afib, VT)
• EPS
Cardiovascular Surgery (2010)
• Coronary Bypass Surgery (366)
• Aortic Valve Replacement (28)
• Mitral Valve Replacement and repair (3)
• Thoracic Aortic Aneurysm/Dissection Graft Repair
• Carotid Endarterectomy
• Peripherovascular Surgery (162)
• Thoracic Surgery (39)

Vascular Surgery/Endovascular Interventions (2010)
• Peripherovascular Surgery (162)
• Aorto -Fem and Fem-Pop Bypass
• Carotid Endarterectomy
• Aortic Aneurysm and Aortic Dissection repair
• PTA, Stenting and Laser Atherectomy (48)
• Carotid Stenting
• EVAR: Endovascular Aortic Repair (14)
• Renal artery stenting
• IVC Filter

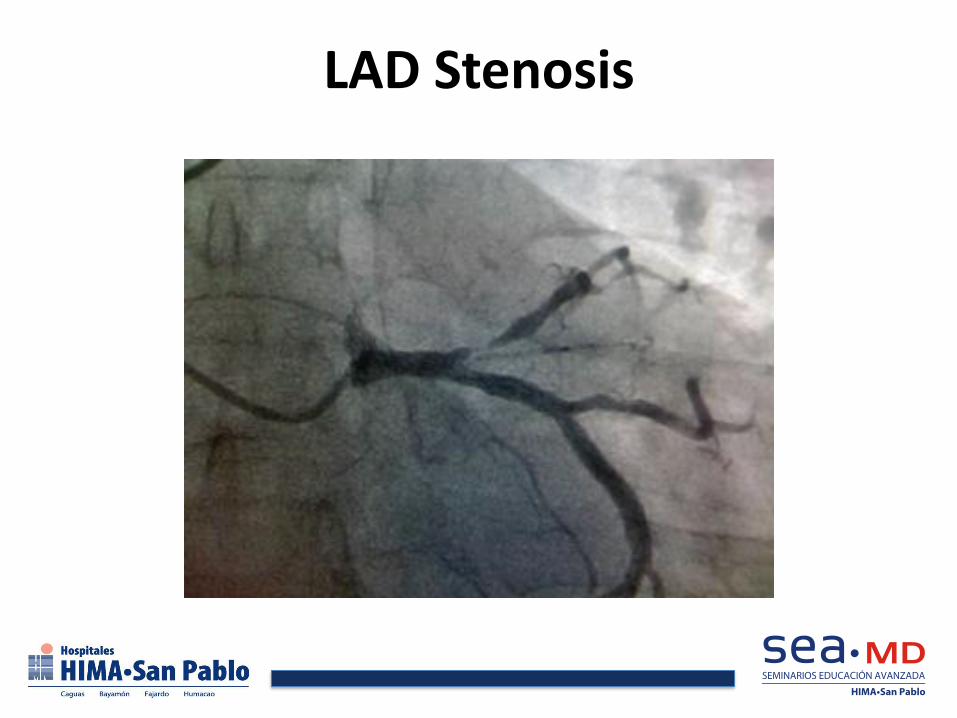
LAD Stenosis
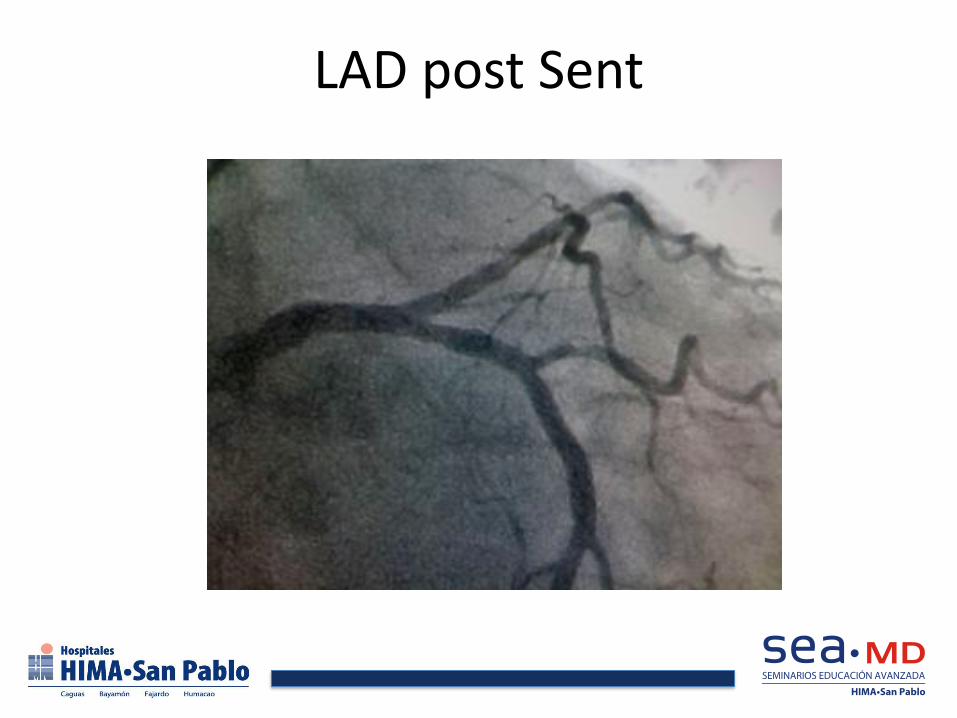
LAD post Sent

IVUS
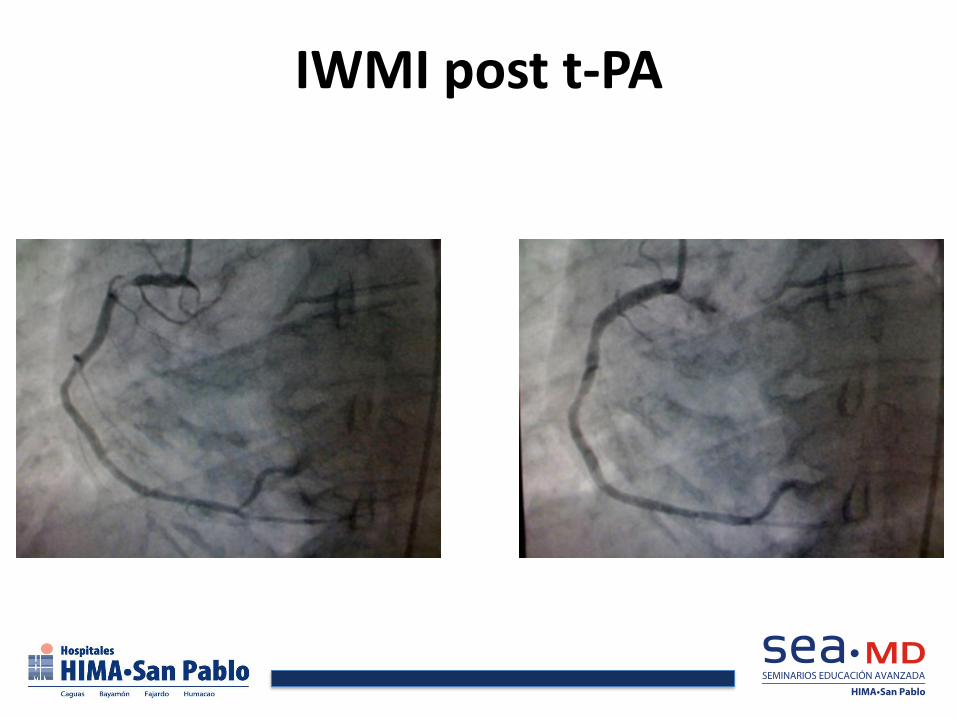
IWMI post t-PA

IWMI RCA Occlusion

AWMI Occluded LAD

LAD Guidewire

Post PTCA

LAD Post PTCA
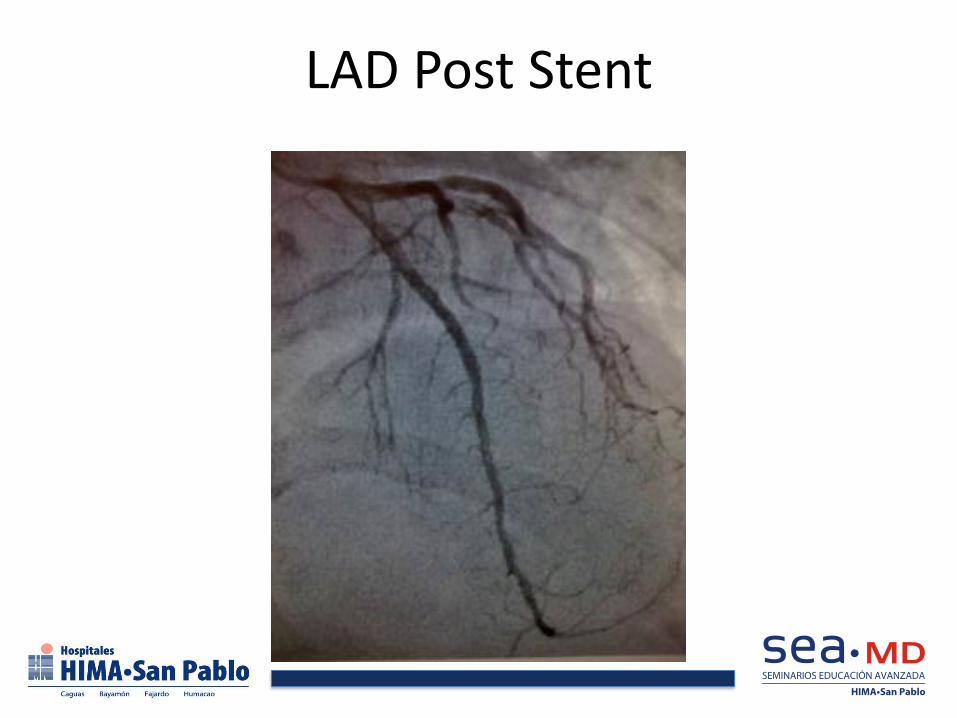
LAD Post Stent

STEMI Interventions
• Pre-Hospital 12 Lead ECG • Primary Percutaneous Coronary Intervention • Door to Balloon < 90 min • Fibrinolysis → Pharmaco-Invasive Strategy • CCL On call team → 24 hour coverage • Radial acces for Pharmacoinvasive Strategy and PPCI • Thrombus Aspiration • Bivalirudin +/- GP-IIBIIIA inhibitors • Stenting • IABP

Cardiovascular Solutions at HIMA•San Pablo Hospital
• HIMA San Pablo provides a wide variety of therapeutic options for patients with complex and advanced cardiovascular disease.
• A multi-disciplinary team is involved in the cardiovascular care of the patient often with the collaboration of multiple cardiovascular and other specialists.

Amín Jaskille Mujica, MD Director Centro
Cirujano e Intensivista

Manejo Inicial
• 100% oxígeno humidificado
• Entubar?
• Acceso intravenoso
– Adultos: 500mL/hr
– Niños > 5 años: 250 mL/hr
– Niños < 5 años: no se recomienda suero
ABA. Advanced Burn Life
Support Providers
Manual. Chicago, IL. 2005
Manejo Inicial
• Remover agente
– Ropa
– Joyería
• Agua directo al área
– Nunca hielo
Evaluación Secundaria
• Historial
– Fuego: ropa, gasolina, explosión, adentro vs
afuera
– Escaldadura: qué líquido, temperatura, abuso?
– Química: agente, duración, explosión
– Eléctrica: Voltaje, caída?, pérdida de
conocimiento

Evaluación Secundaria
• Resto del historial y físico
• Severidad de la quemadura
–Profundidad
–Extensión
Laboratorios - pruebas iniciales
• H/H, electrolitos, U/A
• ABG
• Carboxyhemoglobin
• Glucosa (niños < 12)
• CXR
• EKG

Profudidad
• Primer Grado
– Sol
– Epidermis
– Roja y dolorosa
– No se usa para %TBSA


Profundidad
• Segundo Grado
– Epidermis y parte
de dermis
– Ampollas
– Dolorosa
• Tercer Grado
– “Full Thickness”
– Dermis y
epidermis
– Cuero
– “No duele”



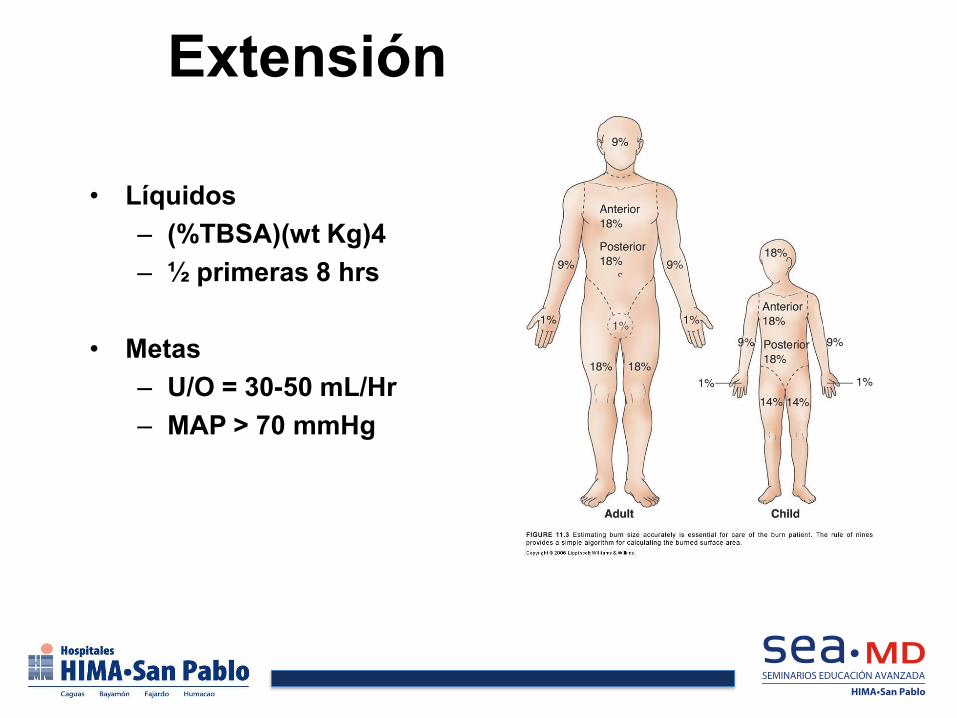
Extensión
• Líquidos
– (%TBSA)(wt Kg)4
– ½ primeras 8 hrs
• Metas
– U/O = 30-50 mL/Hr
– MAP > 70 mmHg
Referido a Centro Quemaduras
• Parciales (segundo grado) de > 10% TBSA
• Cara, manos, pies, genitalia, perineo o articulaciones
• Tercer grado
• Eléctricas
• Químicas
• Inhalación
• Comorbilidades
• Trauma asociado
• No se sienten cómodos

Transporte
• Sábana seca
• Transportación
– Tierra
– Helicóptero: 30-150 millas o condición en rápido deterioro
Centro de Quemaduras
• Director
– Cirujano – Intensivista
• Sala de emergencia
– Estabilización inicial
• Sala de operaciones
– 24/7
• Intensivo

Centro de Quemaduras
• Rehabilitación
– Adultos
– Niños
– Intensivo


Consideraciones Especiales
• Constricción por escara de
tercer grado
– Extremidades
– Pecho
– Cuello

CASOS

Quemadura Química


































Marcos Pérez-Brayfield, MD Urólogo
Board Certified by the American Board of Urology




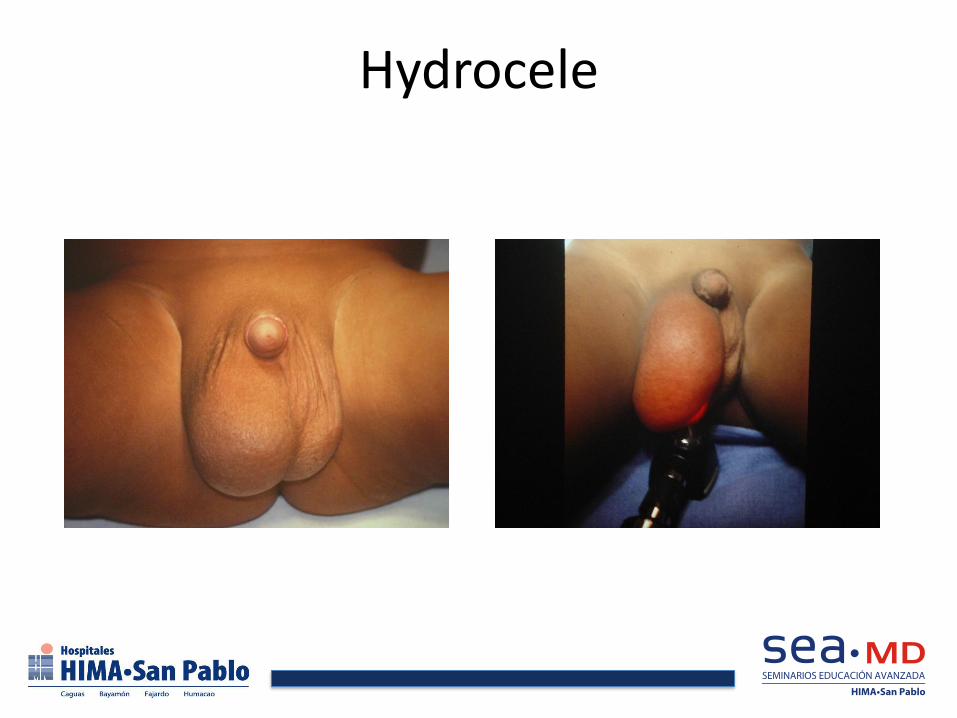
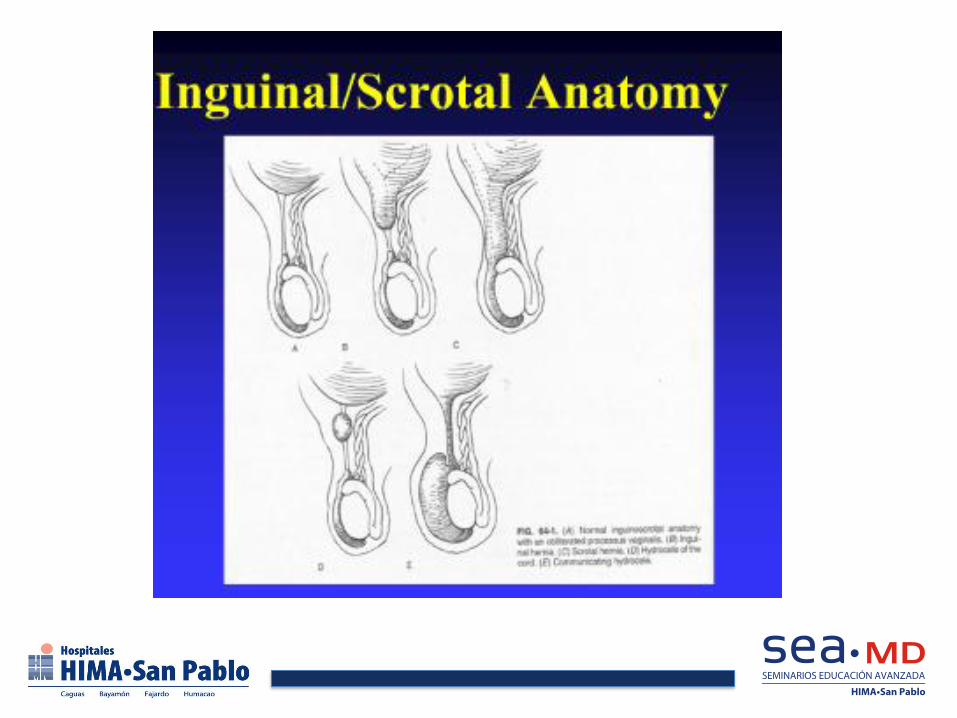
Hydrocele

Intravaginal Torsion



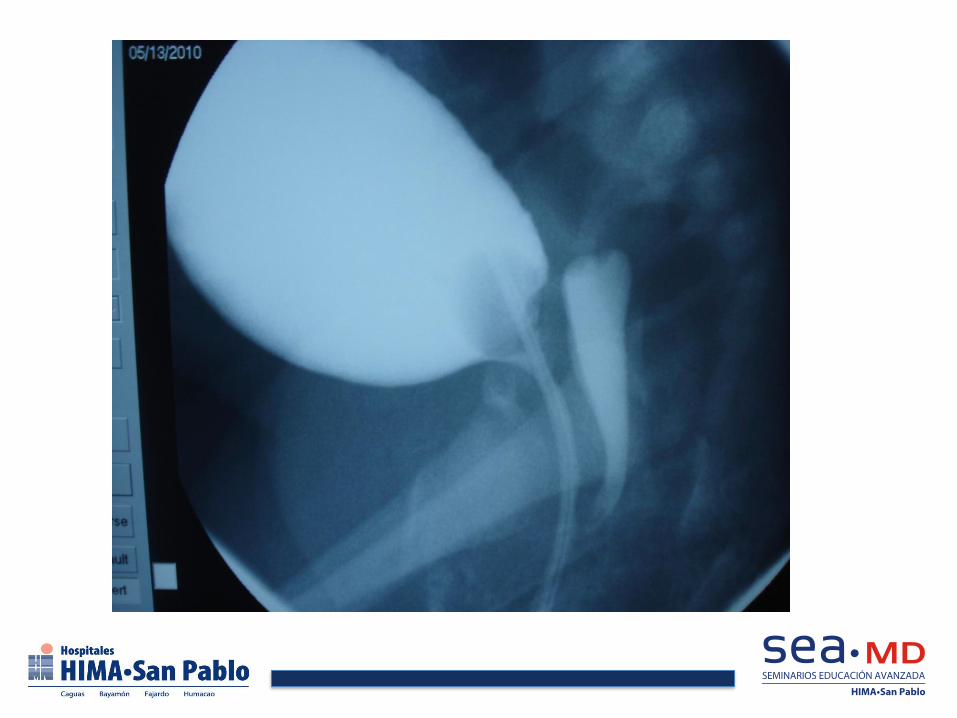



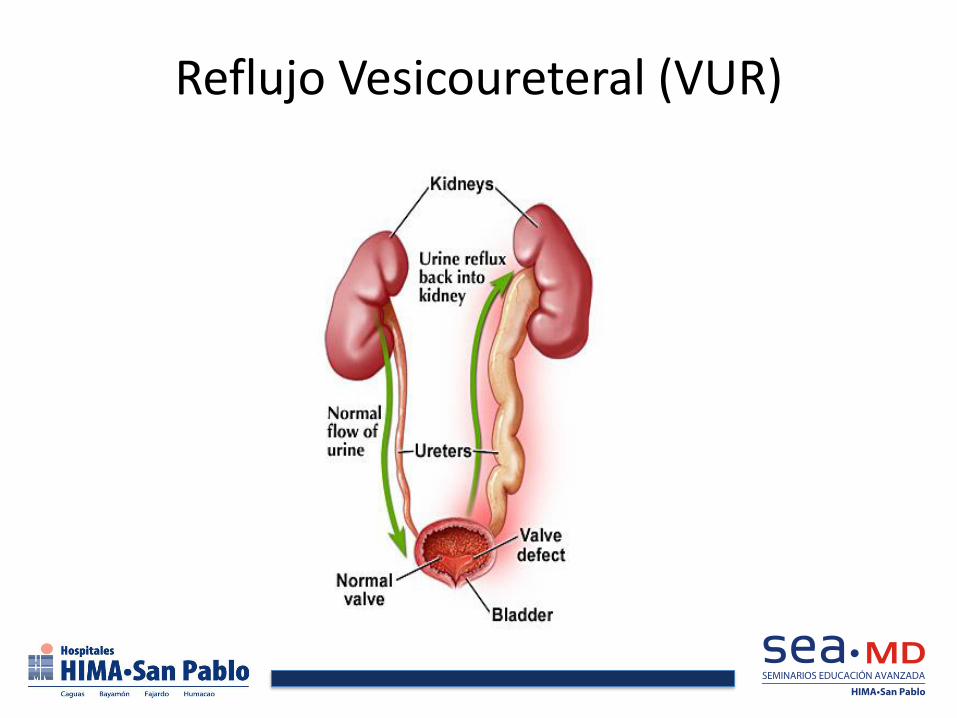
Reflujo Vesicoureteral (VUR)
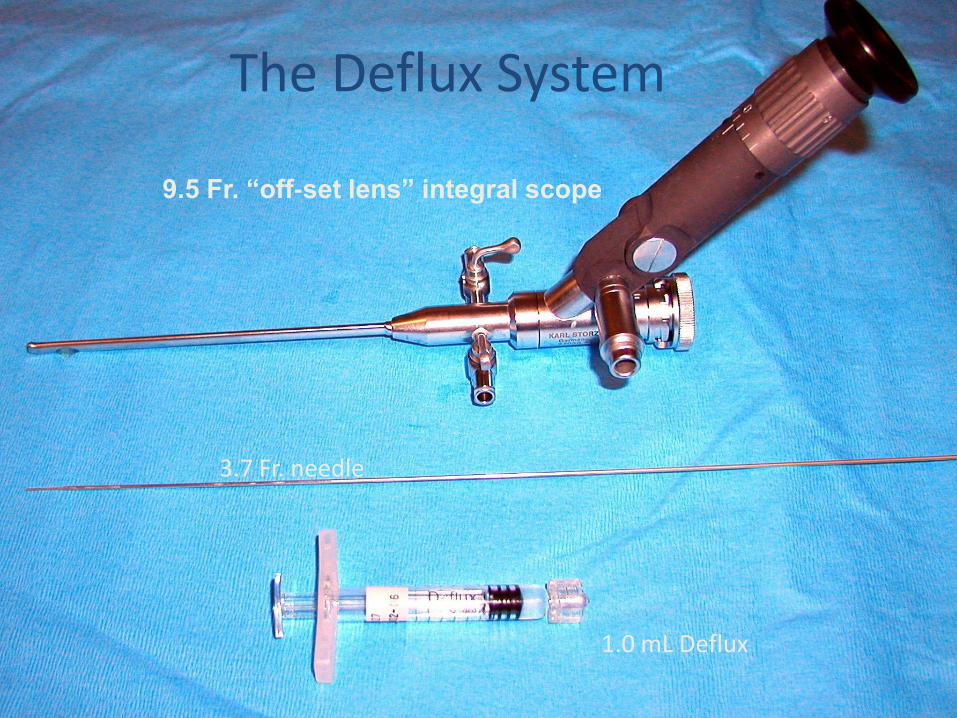
9.5 Fr. “off-set lens” integral scope
1.0 mL Deflux
3.7 Fr. needle
The Deflux System
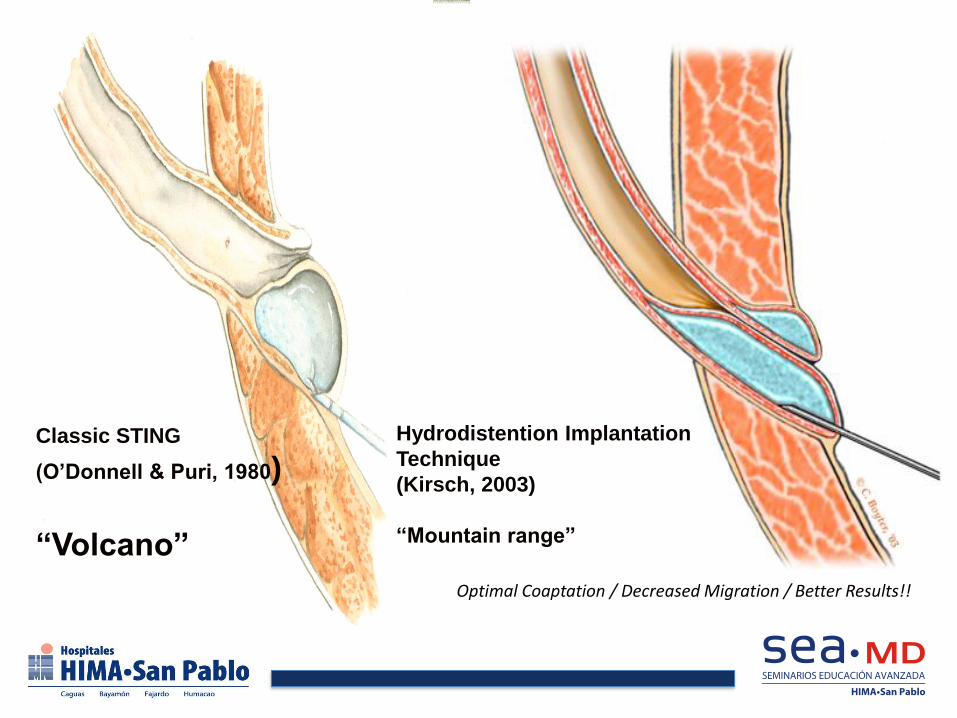
Classic STING
(O’Donnell & Puri, 1980)
“Volcano”
Hydrodistention Implantation
Technique
(Kirsch, 2003)
“Mountain range”
Optimal Coaptation / Decreased Migration / Better Results!!
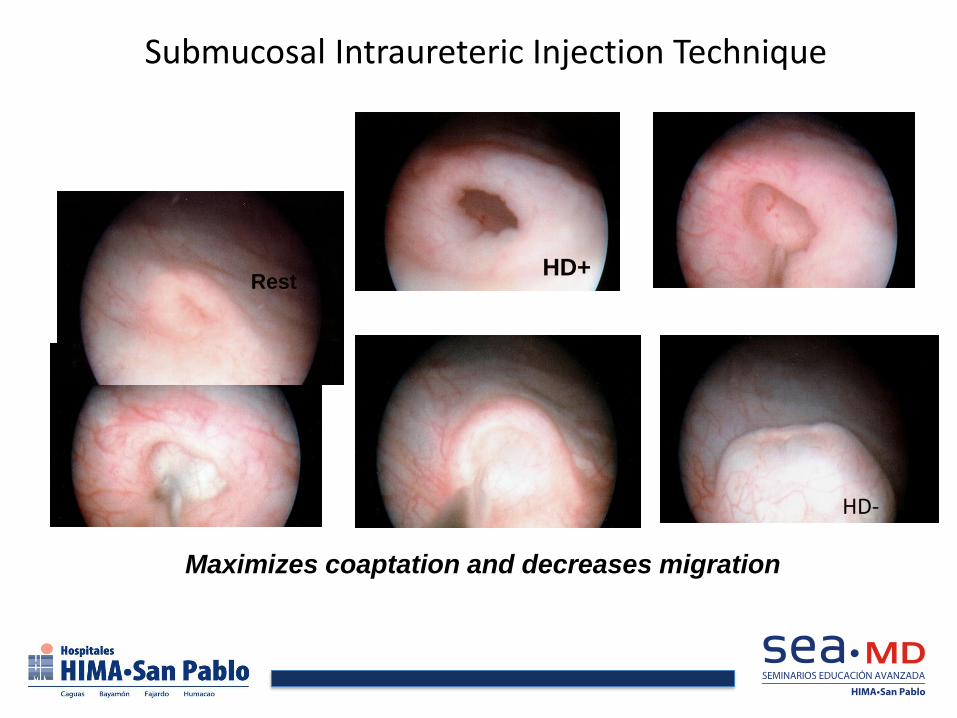
Submucosal Intraureteric Injection Technique
HD+
HD-
Maximizes coaptation and decreases migration
Rest


Undescended Testis

Undescended Testis

Laparoscopy for UDT
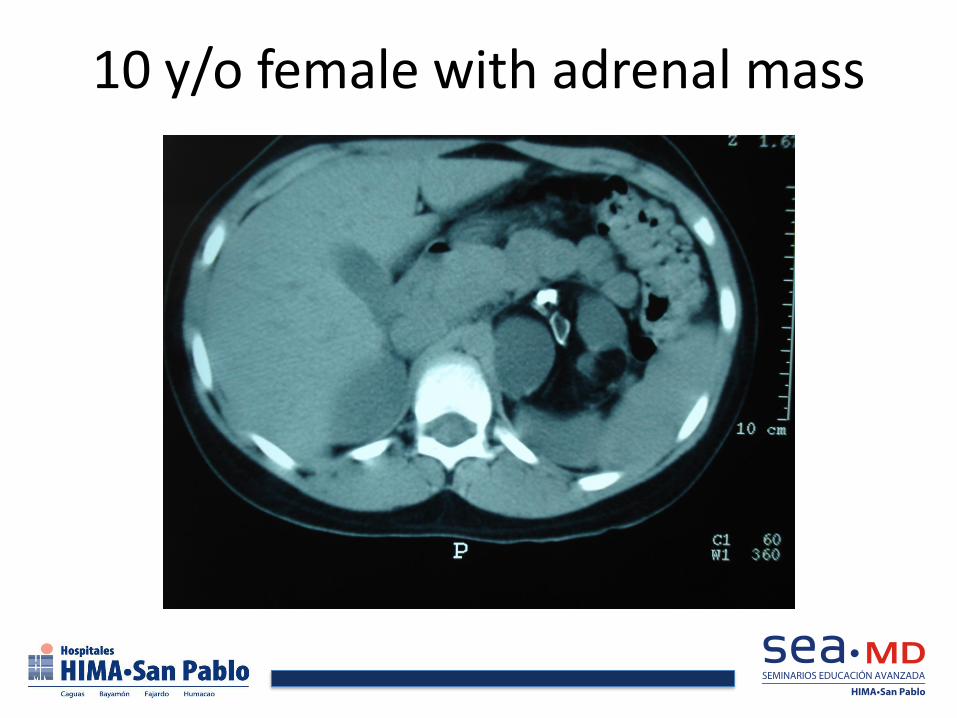
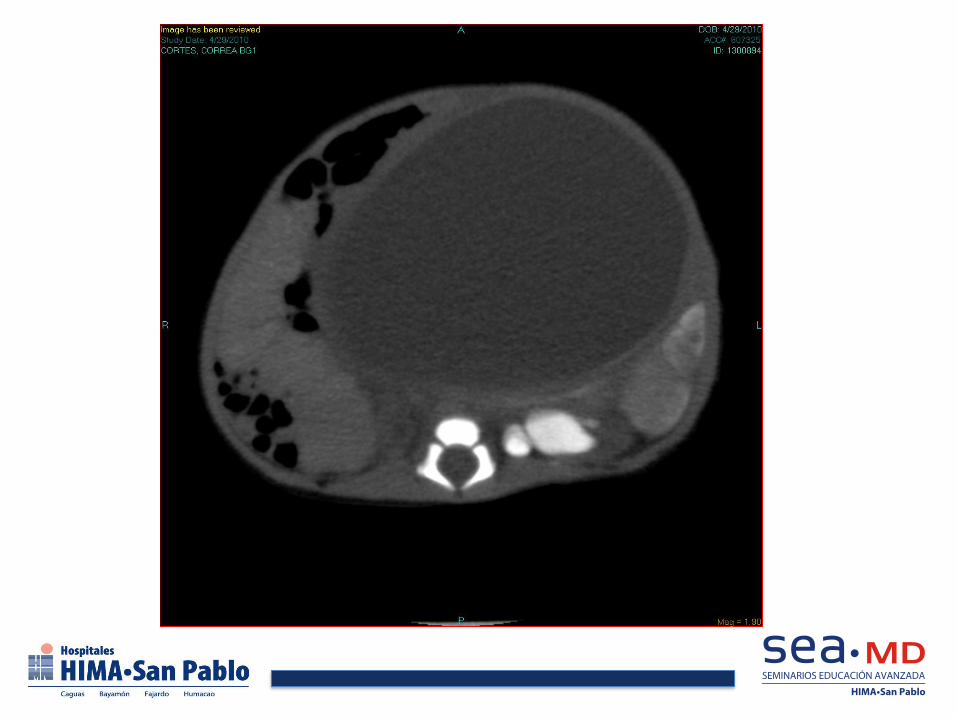
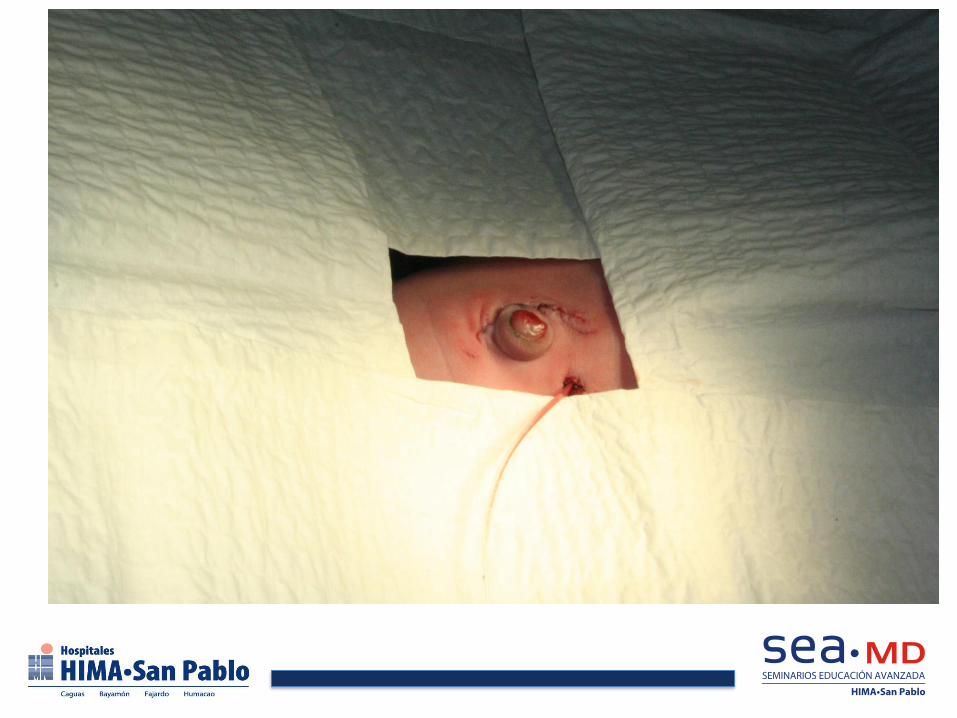
10 y/o female with adrenal mass
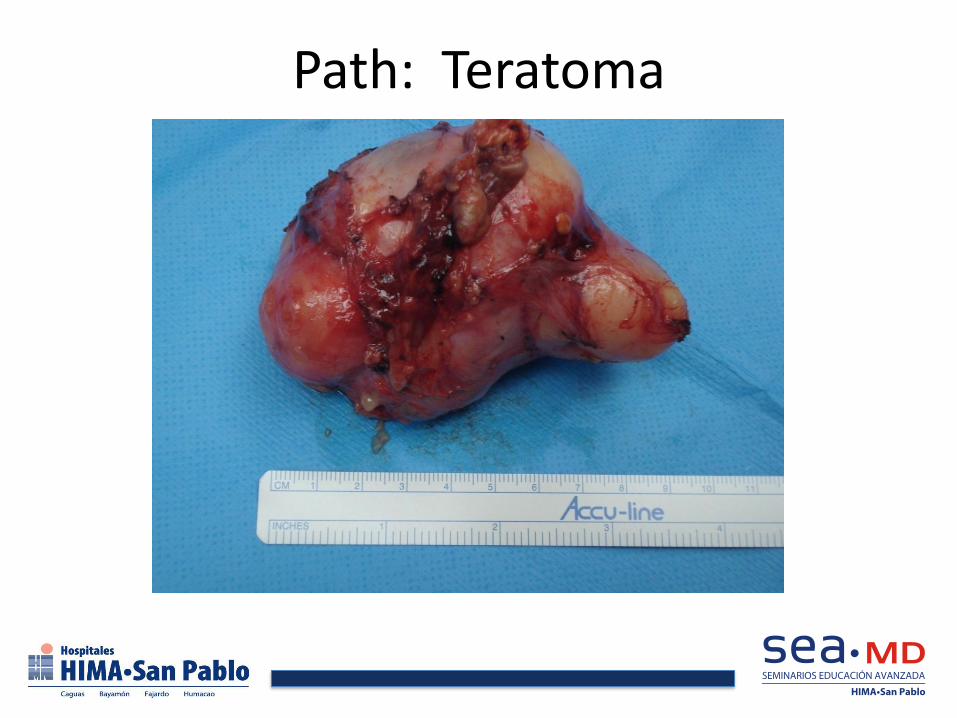
Path: Teratoma



NEFRECTOMIA TRANSPERITONEAL POSICIÓN PACIENTE / TROCAR

DAVINCI CIRUGíA ROBÓTICA

Cirugía Robótica













Aurelio Segundo, M.D., F.A.C.S. Cirujano Pediátrico

Pediatric Neck Masses “Lumps and Bumps”

Thyroglossal Duct Cyst
Infectious/ Inflammatory
Neoplasms
Pediatric Neck Mass
Congenital Acquired
Branchial cleft cyst
Cystic hygroma
Dermoid cyst

Neck Masses
• Midline Neck Masses – Thyroid nodules – Cervical Lymphadenopathy – Thyroglossal Duct cyst – Thymus gland anomalies – Plunging ranula
• Lateral Neck Masses – Branchial cleft anomalies – Laryngoceles – Dermoid and Teratoid Cysts
– Sternocleidomastoid Pseudotumor of Infancy



Pearls: Hypertrophic Pyloric Stenosis
• Non-bilious projectile vomiting; 3-8 weeks
• Most common: first born males
• Hypokalemic, Hypochloremic metabolic alkalosis with paradoxical aciduria.
• Not a surgical emergency- fix electrolytes with NS boluses, D5 0.5 NS maintenance. Add K+ once baby is urinating.
• OR when Chloride > 98; HCO3 <26
• Treatment: pyloromyotomy; babies often vomit postop- just keep feeding!




Intussusception
• Most common cause of intestinal obstruction in children 6 months to 3 years.
• Ileum usually intussuscepts into cecum.
• Severe crampy abdominal pain with lethargic intervals. Currant jelly stool usually not present.
• Diagnosed with US or contrast enema
• Treated with contrast enema >80% of time. air pressure to 120 mmHg, barium to 100 cm H2O
– 10% recurrence, often within hours
• Lead points (meckels, polyp) more common in older children.
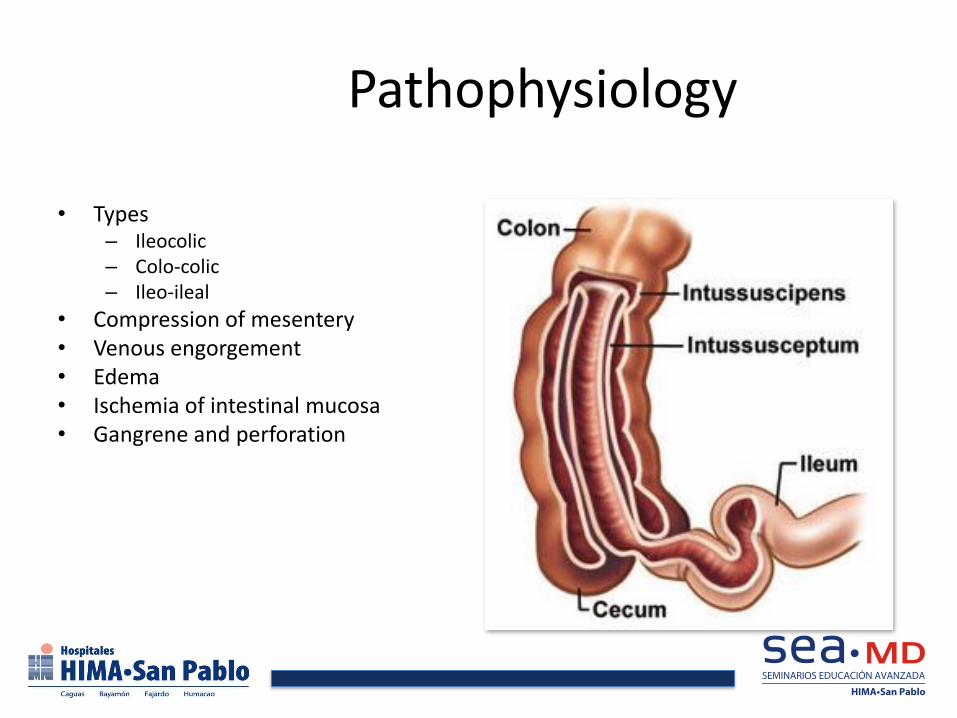
Pathophysiology
• Types – Ileocolic – Colo-colic – Ileo-ileal
• Compression of mesentery • Venous engorgement • Edema • Ischemia of intestinal mucosa • Gangrene and perforation







“Neonatal
bilious emesis is a surgical emergency until proven otherwise”

MALROTATION
• Must consider in every infant with bilious emesis
• Many subtle variations of malrotation/ nonfixation
• 30% present within first week of life
• 50% within first month
• Midgut volvulus with necrosis disastrous
• Can lead to SBS, intestinal tx, death

Malrotation

Abdominal Pain • Perhaps the most common reason for urgent consultation with a surgeon is
the child with acute abdominal pain.
• Most episodes of abdominal pain are self-limited and short-lived.
• While viral illness, UTI, intussusception, Meckel’s, pneumonia, pancreatitis, and a variety of other conditions can lead to abdominal pain, persistent acute abdominal pain in the childhood years must raise consideration of appendicitis.
• Missed appendicitis is a major source of liability claims against pediatricians and family physicians.

Incidence Most common cause of acute surgical
abdomen in children
Lifetime risk:
8.67% for boys
6.7% for girls
Peak Incidence between 12 and 18 years
Rare under the age of 5
Genetic predisposition, especially in children with appendicitis before age 6

Classic Description
Anorexia, then vague periumbilical pain
Pain migrates to Right Lower Quadrant
Nausea and Vomiting follow pain
Diarrhea may occur
Fever, if present, is low grade
Appendix commonly ruptures 24-48 hours after onset of symptoms
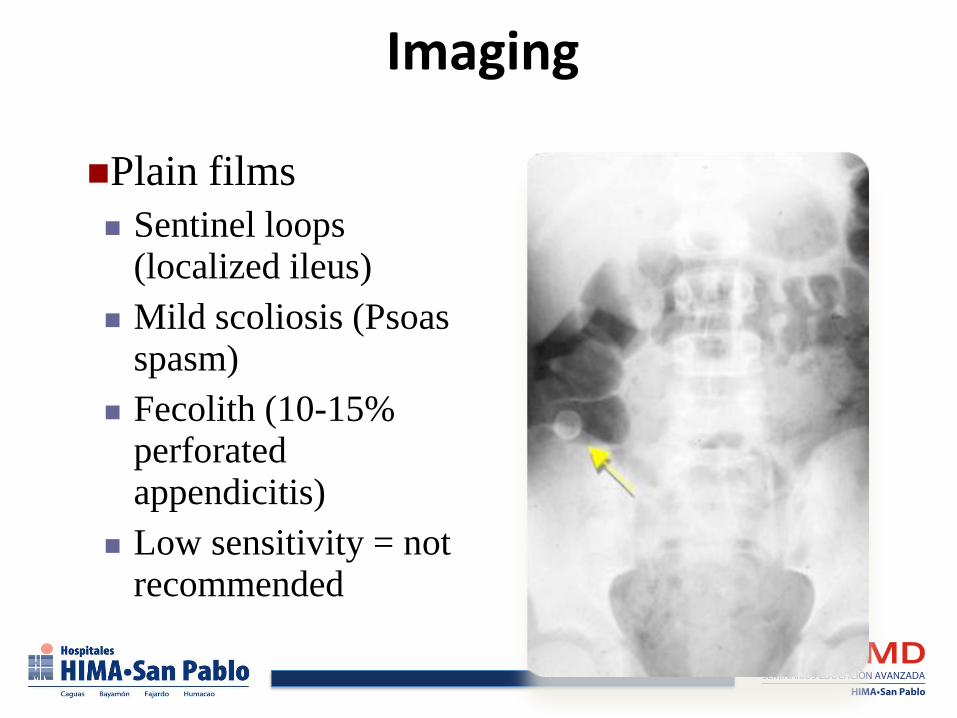
Imaging
Plain films
Sentinel loops (localized ileus)
Mild scoliosis (Psoas spasm)
Fecolith (10-15% perforated appendicitis)
Low sensitivity = not recommended

Imaging
Ultrasound
Specificity 90%, Sensitivity 50-92%
Normal appendix must be seen to exclude appendicitis
Positive criteria
Noncompressible tubular structure 6mm or greater
Complex mass in RLQ
Fecolith
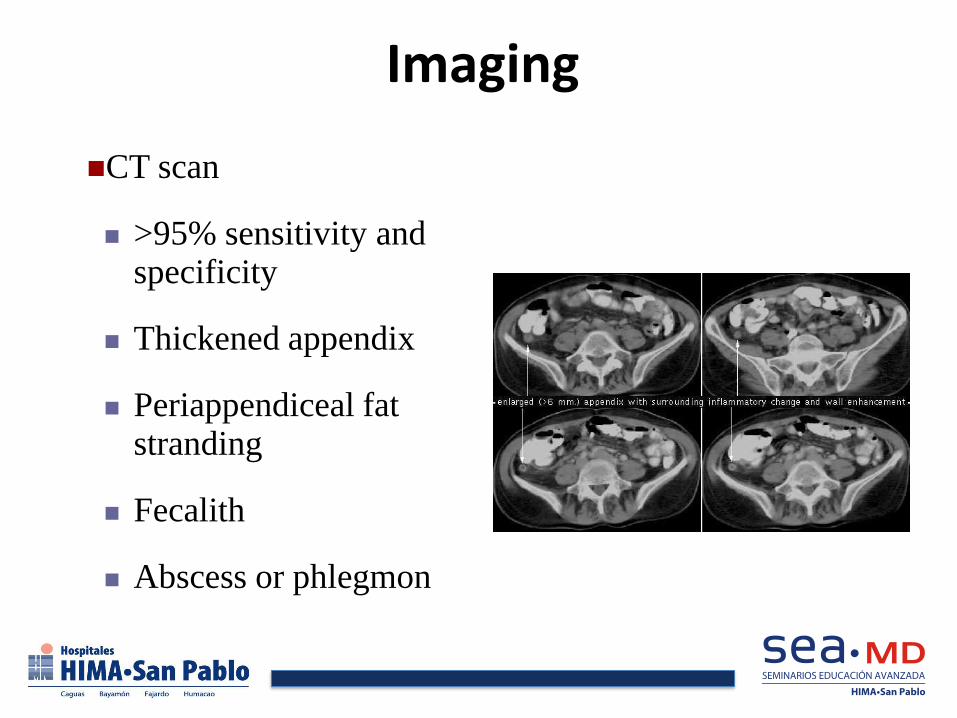
Imaging
CT scan
>95% sensitivity and specificity
Thickened appendix
Periappendiceal fat stranding
Fecalith
Abscess or phlegmon


CT scans
Highly accurate, but are they necessary?
More expensive than ultrasound
May require contrast administration
Exposure to ionizing radiation
One CT equivalent to 100 plain abdominal films
Single CT scan carries average 1/1000 lifetime mortality risk from radiation-induced malignancy
Imaging has not changed negative appendectomy rate
Treatment
Intravenous fluids
Antibiotics
Appendectomy
Non-operative therapy may be considered for those with perforated appendicitis
Children who fail to improve in 24-72 hours will need appendectomy
High failure rate if significant bandemia in differential
Treatment
Immediate vs. Delayed Appendectomy
No need to operate in middle of night with hemodynamically stable child with appendicitis
No change in perforation rate or complications
Findings seem to be more indicative of initial presentation



Definitions
• Hernia
• A general term referring to a protrusion of a tissue
through the wall of the cavity in which it is
normally contained
• Incarceration
• the contents of the hernia cannot be returned to the
cavity from which they came
• Strangulation
• The blood supply to the herniated tissue is
disrupted causing ischemia and tissue death


INCARCERATED INGUINAL HERNIA
• Most common in first year of life
• 30% of infant hernias present with incarceration most manually reducible
• Dx by physical examination alone