schering merck / menopause hormone therapy - focus on ... · 2014/10/07 3 non-hormonal medications...
TRANSCRIPT
2014/10/07
1
1
“FEMININE FOREVER” By Dr. Robert Wilson 1966
Menopause is a “ living decay in which women descended into a vapid cow-like state. Supplemental estrogen would almost magically transform the dull cow into a supple,younger-looking wife and mother. She would not only feel better but also make those around her feel better –especially her partner in bed”
2
The Canadian Population Pyramid The Baby Boom Generation Is Menopausal
Source: Statistics Canada – Annual Demographic Statistics 2005, page 6
MANAGEMENT OF MENOPAUSAL SYMPTOMS
Case Study # 1
• A 48-year-old airline attendant is suffering from severe and disruptive vasomotor symptoms.
• She had her last period 18 months ago. She has had significant problems with sleep disturbance, which are greatly impacting her ability to perform at work where she does many of the trans-Pacific routes.
• She often suffers vaginal dryness and chafing by the end of a long flight.
• She is worried about her ability to remember pills, or not get them mixed up as she regularly crosses the date line.
Menopausal Transition* (lasts average of 5 yr)
Early Late Late
Perimenopause
Variable cycle
length
≥2 skipped cycles &
interval of amenorrhea
Am
eno
rrhea
x 12
mo
s
None
LMP
Premenopausal years
Estrogen Levels Fluctuate Widely During Menopausal Transition
Santoro N, et al. Characterization of reproductive hormonal dynamics in the perimenopause. J Clin Endocrinol Metab 1996;81:1495-501.
Kronenberg F. Hot flashes: epidemiology and physiology. Ann N Y Acad Sci 1990;592:52-86.
Postmenopausal years
Postmenopause (recognized
12 months post-LMP)
Early
Menopause
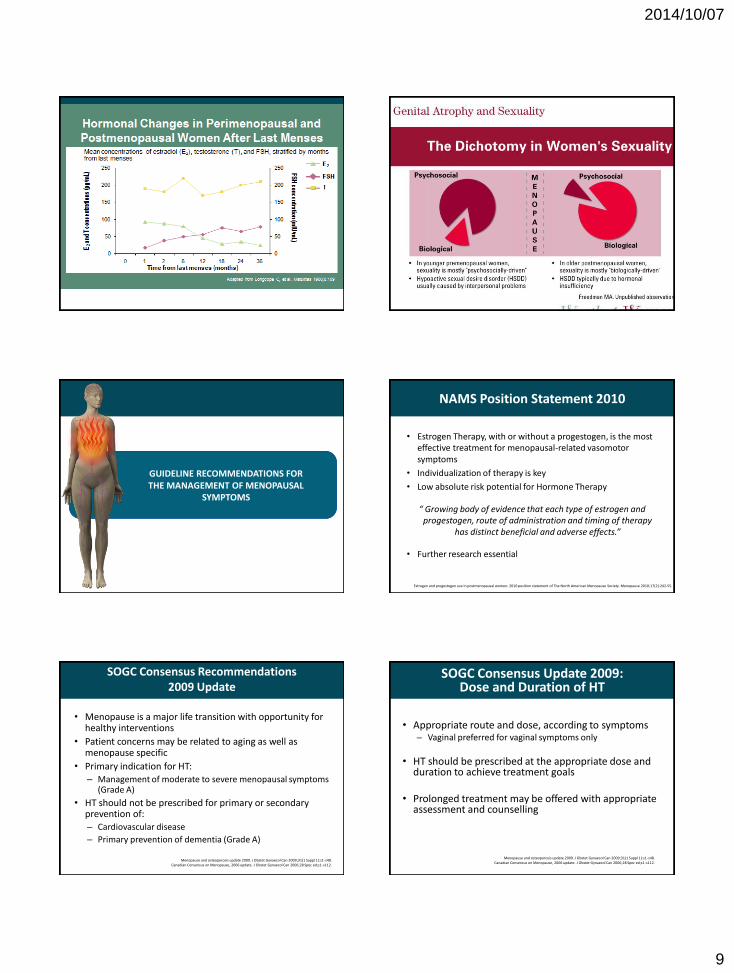
Menopausal Symptom Studies:
% Prevalence in Population Studies
Symptom Pre-menopause Late Perimenopause 2 years Post menopause
Lack of energy 43 43 43
Depression 26 38 32
Aches and joint pain 41 53 57
Insomnia 31 38-39 43
Memory change 31 44 42
Vasomotor 10 42-58 41-48
Vaginal dryness 3 21 32
Bladder control 12 14 26
Sexual dysfunction 42 88
Dry mouth 18 23 29
Dennerstein L, et al. A prospective population-based study of menopausal symptoms. Obstet Gynecol 2000;96:351-8 .
Woods NF, et al. Symptoms during the perimenopause: prevalence, severity, trajectory, and significance in women's lives. Am J Med 2005;118 Suppl 12B;14-24.
Asplund R, et al. Oral dryness, nocturia and the menopause. Maturitas 2005;50(2):86–90.

2014/10/07
2
Facing a Clinical Dilemma
Depressed1,2
Weight change1
Energy2
Sleep2
Libido1
Thoughts
of death1,2
Worthlessness1,2
Concentration2
Anhedonia1,2
Hot flushes1
Perspiration1
Vaginal dryness1
1.Soares CN, Cohen LS. CNS Spectrums 2001;6:167-74.
2.Joffe H, et al. Psychiatr Clin North Am 2003;26:563-80.
Irritable1,2
DEPRESSION MENOPAUSE
Hypothesis of Thermoregulatory Dysfunction: Core Body Temperature Thresholds
Freedman RR. Hot flashes: behavioral treatments, mechanisms, and relation to sleep. Am J Med 2005;118 Suppl 12B:124-30.
Upper threshold (Upper set point)
Body temperature
Lower threshold (Lower set point)
Thermo-neutral Zone (homeostatic
range)
Body temperature
Shivering Shivering
Sweating Sweating
Core Body Temp
Symptomatic Normal
Why Consider Hormone Therapy?
HT is the most efficacious therapy for VMS
Cochrane database review showed1
– 75% reduction in frequency for any HT
– Significant reduction in hot flash severity
– Combination of E+P slightly more effective than E alone
• Progestin alone has also demonstrated some efficacy2
1. MacLennan AH, et al. Oral oestrogen and combined oestrogen/progestogen therapy versus placebo for hot flushes. Cochrane Database Syst Rev 2004;18(4):CD002978.
2. Canadian Consensus on Menopause, 2006 update. J Obstet Gynaecol Can 2006;28 Spec ed;s1-s112.
9 Newton KM, et al. Treatment of vasomotor symptoms of menopause with black cohosh, multibotanicals, soy, hormone therapy, or placebo: a randomized trial. Ann Intern Med 2006;145(12):869-79. Reproduced with permission.
Multibotanical + soy
Multibotanical
HT * *
8
7
6
5
4
3
2
1
0
Baseline 3 mo 6 mo 12 mo
Vas
om
oto
r Sy
mp
tom
s Pe
r D
ay
* * *
Placebo
Black cohosh
Efficacy of HT vs. Herbals, Soy and Botanicals
Best evidence
Adjusted mean number of vasomotor symptoms per day, by study group
Why bioidenticals?
• Response to 2002 WHI and suspicion of traditional medicine
• Perception of safer alternative – fear of cancer (especially breast cancer) and traditional HT
• Patients still having symptoms
• Wider advertising and broad availability (e.g., Internet)
• Patient comfort with alternative medicines
What is available for women?
Pharmaceutical standardized products • 17β-estradiol – oral and transdermal via patch or gel
• Micronized progesterone in peanut oil
Compounded with prescription by physician
for pharmacist • Customized estrogen mixtures of 80-90% estriol with 10-20%
estradiol (Bi-Est) – 1.25 and 2.5 mg
• Older Tri-Est contained 80% estriol, 10% estradiol and 10% estrone

2014/10/07
3
Non-hormonal Medications for VMS
Gabapentin1 600 mg HS for night sweats
600-2400 mg/d in 3 divided doses
Effective for VMS, no impact on mood
Side effects in 25% of women (headache, dizziness, disorientation)
Clonidine2 Mildly effective at 0.05-0.075 mg bid
12% report reduction of >75%
Most common side effects: dry mouth, constipation, fatigue, restless sleep
SSRI/SNRI2-4 Dosage depends on SSRI/SNRI
Mostly studied in breast cancer survivors
Variable improvements (up to 79% reduction in VMS)
Reduction in severity and frequency
1.Liu JH. Obstet Gynecol. 2006;108(1):4-5. 2.Loibl S, et al. Ann Oncol 2007;18(4):689-93.
3.Carpenter JS, et al. Oncologist 2007;12(1):124-35. 4.Gordon PR, et al. Menopause 2006;13(4):568-75.
Overall Benefits of HT
Demonstrated efficacy:
– ↓ Vasomotor symptoms
– ↓ Urogenital atrophy
– ↓ Somatic pain, arthralgia
– ↓ Risk of osteoporotic fractures
– ↓ Risk of colorectal cancer
– Mood stabilization
Menopause and osteoporosis update 2009. J Obstet Gynaecol Can 2009;31(1 Suppl 1):s1-s48. Canadian Consensus on Menopause, 2006 update. J Obstet Gynaecol Can 2006;28 Spec ed;s1-s112.
Santen RJ, et al. Postmenopausal Hormone therapy: an Endocrine Society position statement. J Clin Endocrinol Metab 2010;95(7 Suppl 1):S1-S66. Estrogen and progestogen use in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause 2010;17(2):242-55.
Contraindications to HT Non-contraindications to HT
• Unexplained/undiagnosed vaginal
bleeding prior to investigation • Known or suspected
breast carcinoma • Acute liver disease • Active thromboembolic disease • Acute cardiovascular disease • Recent stroke • Pregnancy
• Smoking
• Diabetes
• Hypertension
• Migraine
Who Can Take Hormone Therapy Risk/Benefit Analysis from
Hormone Therapy Trials
Clinical Event HERS (E&P)1 WHI (E&P)2 WHI (E Alone) 3
CHD 0.99 1.29* 0.91
Stroke 1.23 1.41* 1.39*
PE 2.79 2.13* 1.34
Breast CA 1.30 1.26* 0.77
Colon CA 0.69 0.63* 1.08
Hip Fracture 1.10 0.66* 0.61*
Death 1.08 0.98 1.01
Global Index ---- 1.15 1.01
* Statistically significant
1. Hulley S, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA 1998;280(7):605-13. 2. Rossouw JE, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women's Health Initiative randomized
controlled trial. JAMA 2002;288(3):321-33. 3. Anderson GL, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial.
JAMA 2004;291(14):1701-12.
Case Study # 2
• A 36-year-old teacher with premature menopause with complaints of hot flashes and night sweats that are interfering with her sleep and work.
• She previously underwent a total hysterectomy with bilateral oophorectomy for the treatment of severe pelvic inflammatory disease and tubal abscesses.
• After 6 months of oral estrogen, continued VMS, fatigue, decreased energy and libido.
Premature Menopause
• Medically a distinct group
• ↑ risk of negative effects on cardiovascular system, bone, cognition, mood & sexuality
Santen RJ, et al. Postmenopausal hormone therapy: an Endocrine Society scientific statement. J Clin Endocrinol Metab 2010;95(7 Suppl 1):S1-S66. Estrogen and progestogen use in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause 2010;17(2):242-55.

2014/10/07
4
Biological Potency Oral Contraception vs. Hormone Therapy
Estr
oge
n P
ote
ncy
Hormone Therapy
The biological potency of oral contraceptives is 3 to 5 times that of Hormone Therapy
Mashchak CA, et al. Comparison of pharmacodynamic properties of various estrogen formulations. Am J Obstet Gynecol 1982;144(5):511-8.
Hormonal Contraception
Reproductive Age
Risks of Premature Menopause
• Risk of overall mortality and CVD increase with earlier age of onset of premature menopause1
• Guidelines recommend HT to restore natural estrogen levels until at least the average age of natural menopause (~51 years)2,3
1. Shuster LT, et al. Premature menopause or early menopause: long-term health
consequences. Maturitas 2010;65(2):161-6. 2. Menopause and osteoporosis update 2009. J Obstet Gynaecol Can 2009;31(1 Suppl
1):s1-s48. Canadian Consensus on Menopause, 2006 update. J Obstet Gynaecol Can 2006;28 Spec ed;s1-s112.
3. Estrogen and progestogen use in postmenopausal women: 2010 position
statement of The North American Menopause Society. Menopause
2010;17(2):242-55.
0.01 0.1 1 10 100
Impact of Age on CV Risk from HT Data from Multiple RCTs
Younger Women < 60 Older Women > 60
Salpeter SR, et al. Brief report: coronary heart disease events associated with hormone therapy in younger and older women. A meta-analysis. J Gen Intern
Med 2006;21(4):363–6.
TOTAL (95% Cl) 0.68 (0.48, 0.96)
Favours HT Favours control
TOTAL (95% Cl) 1.03 (0.91, 1.16)
Favours HT Favours control
0.001 0.01 0.1 1 10 100
WHI Re-analysis: Effect of Estrogen Alone on Major Outcomes for Women <60 Years vs 70-79 Years
*Expressed as absolute rates per 10,000 women annualized over the average follow-up period of 10.7 years
50-59 Years 70-79 Years
Acute MI -12 +16
Death -13 +19
Adverse events (Global index of chronic diseases)
-18 +48
Differences in Outcomes in Women Who Received CEE*
LaCroix AZ, et al. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy: a randomized controlled trial. JAMA.2011;305(13):1305-14.
Atherosclerosis timeline: A unifying hypothesis
Image from Pepine CJ. Am J Cardiol 1998;82(suppl 10A):23S
Foam
cells
Fatty
streak
Intermediate
lesion Atheroma Rupture
Fibrous
plaque
Thrombosis,
haematoma Growth mainly by lipid accumulation
Estrogen worsens Estrogen
prevents
Endothelial dysfunction
Case Study # 3
• 54 years old, BMI 32, postmenopausal (2 years since her last menstrual period).
• Family history of stroke (Dad) and DVT (Mom).
• She is experiencing disruptive menopause symptoms including night sweats, hot flashes and severe moodiness. These were initially self-managed with herbal remedies, but her symptoms are now having a more severe impact on her life (e.g., increase work absences, frequently upset and irritable).
• She is worried about the risk of VTE associated with hormone therapy and feels it is too risky for her.
.

2014/10/07
5
Risk Factors for VTE
• Increasing age
• Obesity body mass index over 30
• Previous VTE
• Post-thrombotic syndrome
• Varicose veins with phlebitis
Venous thromboembolism and hormone replacement therapy [Green-top guideline no 19]. 3rd ed. London: Royal College of Obstetricians and Gynaecologists; 2011.
• First degree family history of VTE
• Immobility for more than 3 days
• Surgical procedures
• Other disorders
Duration of HT Use and VTE
• Year 1 4.01 RR
• Year 2 1.97 RR
• Year 3 1.74 RR
• Year 4 1.70 RR
• Year 5 2.90 RR
• Year 6 1.04 RR
Women’s Health Initiative Investigators. Estrogen plus progestin and the risk of venous thrombosis. JAMA 2004;292(13):1573-80.
MANAGEMENT OF MENOPAUSAL SYMPTOMS:
FOCUS ON TRANSDERMAL ESTROGENS
Why Transdermal? Why Now?
• Needs assessment revealed gaps in practitioner knowledge
• Extensive information on oral hormone therapy; only delivery system looked at in WHI
• Since then – information has continued to evolve over past 10 years
• New science on transdermal delivery system
• There is a difference
Metabolism and Activity of Estrogen
E1 and E2 Oral Gut
E1, E2 & E3 Transdermal
Vaginal
Converted in GI Tract
E2 E1
Excretion of conjugates in urine & feces
Bloodstream Conjugated in Liver
E2 E1
E3
Bloodstream
Target Organs
E2 E1
Bloodstream
Bloodstream
Case Study # 4
• 49 year-old P-0 woman whose last menstrual period was 3 months ago.
• Her mother is a breast cancer survivor.
• History of DVT from 20 years ago
• She presents reporting difficulty sleeping because of hot flushes. She feels that this is interfering with her ability to function. She also reports that she has no energy.
• She currently smokes (1/2 pack per day).
• She has dense breasts on mammogram.
30

2014/10/07
6
Transdermal Estrogens: Impact on Cardiovascular Risk Factors
• Estrogen and Thromboembolism Risk (ESTHER) study1 – Lower risk of VTE compared with oral E2
• Markers of inflammation unaffected2
• Triglycerides decreased3
• Less effect on SHBG and TBG2
• Less favourable for HDL and LDL changes4 - CEE alone and CEE + MPA have a favourable effect on HDL-C
• Decreased CV risk in patients with metabolic syndrome5-7
1. Canonico M, et al. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER study.
Circulation 2007;115(7):840-5.
2. Shifren JL, et al. A comparison of the short-term effects of oral conjugated equine estrogens versus transdermal estradiol on C-reactive protein, other serum markers of inflammation, and other
hepatic proteins in naturally menopausal women. J Clin Endocrinol Metab 2008;93(5):1702-10.
3. Sanada M, et al. Substitution of transdermal estradiol during oral estrogen-progestin therapy in postmenopausal women: effects on hypertriglyceridemia. Menopause 2004;11(3):331-6.
4. Walsh BW, et al. Effects of postmenopausal estrogen replacement on the concentrations and metabolism of plasma lipoproteins. N Engl J Med 1991;325(17):1196-1204.
5. Modena MG, et al. Effects of hormone replacement therapy on C-reactive protein levels in healthy postmenopausal women: comparison between oral and transdermal administration of estrogen. Am J Med 2002;113(4):331-4.
6. Lewandowski KC. Effects of hormone replacement therapy type and route of administration on plasma matrix metalloproteinases and their tissue inhibitors in postmenopausal women. J Clin
Endo 2006;91(8):3123-30.
7. Chu MC. Metabolic syndrome in postmenopausal women: the influence of oral or transdermal estradiol on inflammation and coagulation markers. Am J Ob Gyn 2008;199(5):526.e1-e7.
SHBG = sex hormone-binding globulin; TBG = thyroxine-binding globulin.
Risk of VTE with Oral vs. Transdermal Estrogen: The ESTHER Study
Ad
just
ed
Od
ds
Rat
io (
95
% C
I)
Scarabin PY, et al. Differential association of oral and transdermal oestrogen-replacement therapy with venous thromboembolism risk. Lancet 2003;362(9382):428-32.
OR = 4.0 (1.9-8.3)
Some Postmenopausal Women are at Higher Risk of VTE
<0.05 25.5 Prothrombotic
mutation + oral E
NS 1.0 Transdermal E
<0.0001 3.2 Oral E
<0.0001 4.8 Prothrombin
mutation
<0.0001 3.4 Factor V Leiden
P-value Risk (odds ratio)
Oral, but not transdermal, estrogen increased VTE risk in
postmenopausal women with prothrombotic mutations
Straczek et al. Circulation 2005;112:3495-3500.
Postmenopausal HT and Risk of VTE: Results of the E3n Trial
1.0
Multivariate-adjusted hazard ratio* (95% CI)
1.5 2.0 0.5
Never use (n=181)
Past use (n=66)
Current use of oral estrogens (n=81)
Current use of transdermal estrogens (n=174)
1 [reference]
Age-adjusted HR Multivariate-adjusted HR*
1 [reference]
1.0 (0.7 -1.3)
1.5 (0.9 -2.3)
1.1 (0.7 -1.6)
1.1 (0.8 -1.5)
1.7 (1.1 -2.8)
1.1 (0.8 -1.8)
2.5
Canonico M, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol 2010;30(2):340-5.
Hazard ratios of idiopathic VTE in relation to both estrogens by route of administration and concomitant progestogens
*Adjusted for age, body-mass index, parity, educational level and time-period.
HORMONE THERAPY AND RECURRENCE OF VENOUS THROMBOEMBOLISM
• 1,023 postmenopausal women with a comfirmed first VTE were followed for risk of recurrence and impact of HRT
• Recurrent VTE occurred in 77 women
• Transdermal estrogens H.R. 1.0
• Oral estrogens H.R. 6.4
• Progestogen use was not significant
35
Oral and Transdermal Estrogen: Risk of Stroke
1.0
Adjusted HR* (95% CI)
1.5 2.0 0.5
None (n=14,496)
Transdermal route (n=103)
Low dose ≤50 mg (n=76)
Oral route (n=618)
0.92 (0.74-1.14)
Crude HR Adjusted HR*
0.95 (0.75-1.20)
2.5
*Adjusted for age, body-mass index, smoking status, alcohol misuse, diabetes, hyperlipidemia, hypertension, atrial fibrillation, CVD, transient ischemic attack, aspirin or other NSAID use, and history of hysterectomy or oophorectomy. † Lose dose: ≤0.625 mg CEE or ≤2 mg estradiol; high dose: >0.625 mg CEE or >2 mg estradiol. Mean age of cases and controls at index date was 70 years.
High dose >50 mg (n=27)
Low dose† (n=515)
High dose † (n=103)
1.00 [reference] 1.00 [reference]
0.78 (0.61-1.00) 0.81 (0.62-1.05)
1.87 (1.17-2.98) 1.89 (1.15-3.11)
1.20 (1.09-1.33) 1.28 (1.15-1.42)
1.16 (1.04-1.29) 1.25 (1.12-1.40)
1.51 (1.20-1.90) 1.48 (1.16-1.90)
3.0
Renoux C, et al. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ 2010;340:C2519.

2014/10/07
7
1. Jensen J, et al. Cigarette smoking, serum estrogens, and bone loss during hormone-replacement therapy early after menopause. N Engl J Med 1985;313(16):973-5.
2. Lobo RA, et al. Pharmacokinetics of oral 17 beta-estradiol. J Reprod Med 1992;37(1):77-84.
Estrogen Therapy: Smoking Impacts Selection of Route of Administration
Smoking
– Free E2 levels may be lower in smokers ( liver metabolism; sex-hormone-binding globulin)1,2
– Increased dose of oral E may be required
– Transdermal E may be beneficial
ERT = estrogen replacement therapy; E2 = estradiol; E = estrogen
MANAGEMENT OF MENOPAUSAL SYMPTOMS:
FOCUS ON THE PROGESTOGENS
Available Progestogens
• Micronized progesterone (natural)
– Prometrium®
– Chemically identical to endogenous progesterone
– Only natural agent approved by Health Canada & U.S. FDA for oral use
• Synthetic progestins
– C-21 class (e.g., medroxyprogesterone acetate) • e.g., Megestrol®, Provera®
– 19-nortestosterone class (e.g., norethindrone acetate) • e.g., Micronor®, Norlutate®
Progestogen Indications
• Primary menopause-related indication is endometrial protection from unopposed ET
• Not necessary with standard doses of vaginal ET (including vaginal ring)
• Progestogen not generally indicated with ET post-hysterectomy
Estrogen and progestogen use in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause 2010;17(2):242-55.
Micronized Progesterone Metabolism
• Metabolized primarily by the liver
• Metabolites act at non-sex-steroid receptor sites
• Beneficial effects of metabolites – Sedation effect with higher doses of oral progesterone
– Has anti- aldosterone properties
• May reduce bloating, breast tenderness and edema
• Adverse effects of metabolites – May cause nausea and dizziness
– Contraindicated in patients with peanut allergy
Case Study # 5
• 52 years old, 2 years postmenopausal. Currently experiencing severe VMS, sleep deprivation, decreased libido and sexual response, and dyspareunia.
• Has experimented with black cohosh with no success. Trials of clonidine and venlafaxine also resulted in a poor response.
• Patient is interested in trying HT but does not wish to experience BTB and has family hx of breast cancer
• She currently smokes 1/2 pack per day.

2014/10/07
8
14
12
10
8
6
4
2
0
Rel
ativ
e R
isk
10 years oophx
Menopause <49
Exercise
Alcohol
5 years post HRT
1 year post HRT
1st child >age 30
HRT>5 years
Young menarche
Obesity
2 affected relatives
Risk Factors for Breast Cancer Breast Cancer Risk and Progestogen Selection
1.0
Adjusted relative risk* (95% CI)
1.5 2.0 0.5
Estrogen alone (n=20,347)
Estrogen + progesterone (n=40,537)
Estrogen + dydrogesterone (n=31,045)
Estrogen + other progestogens (n=104,243)
1.29 (1.02-1.65)
1.00 (0.83 -1.22)
1.16 (0.94-1.43)
1.69 (1.50 -1.91)
2.5
Relative risk of invasive breast cancer by type of HT and duration of exposure, compared with HT never-use
N=80,377 postmenopausal women, mean age 52.4 years. At start of HT, 31.9% of participants were aged 40-45 years; 25.7% were 45-50 years, 20.4% were 50-55 years, 13.8% were 55-60 years, and 8.2% were 60-65 years. *Adjusted for time since menopause, age at menarche, parity and age at first full-term pregnancy, breastfeeding, age at menopause, type of menopause, personal history of benign breast disease, family history of breast cancer in first-degree relatives, family history of breast cancer in other relatives, BMI, previous mammography. Further stratified on year of birth.
Fournier A, et al. Unequal risks for breast cancer associated with different hormone replacement therapies: results from the E3N cohort study. Breast Cancer Res Treat 2008;107(1):103-11.
CEE = conjugated equine estrogen; MP = micronized progesterone; MPA = medroxyprogesterone acetate. P <0.001 for all active treatment groups. *P <0.004 for CEE, CEE + MP cyclic.
mg/
dL
CEE* CEE CEE CEE + MP* + MPA + MPA cyclic cyclic continuous Placebo
PEPI: Effects of HT on HDL–C in Post-Menopausal Women
Average Changes in HDL – Baseline to 36 Months
The Writing Group for the PEPI Trial. Effects of Estrogen or Estrogen/ Progestin Regimens on Heart Disease Risk Factors in Postmenopausal Women: The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA 1995;273(3):199-208.
Improved Sleep Efficiency
as a Benefit of HT
Fragmented sleep
A source of:
• daytime fatigue
• loss of concentration
• psychomotor performance
• mood changes
“Better sleep”
Often reported by
women as one of
the most important
benefits of HT
Investigators’ Evaluation of
Sleep Efficiency: Micronized
Progesterone vs. Hypnotics
• Micronized progesterone can produce an effect
similar to that of hypnotics with respect to sleep
efficiency improvement without: – modifying normal sleep architecture
– inducing daytime sleepiness
Montplaisir J, et al: Menopause 2001; 8(1):10-6.
• Sexual health is important to quality of life at any age
• Majority of women age 50+ sustain sexual interest and ability into old age
• Sexuality of the older woman is an important medical concern1
1. Lamont JH. WMJ 1998;97(8):18.
Sexual Health
2014/10/07
9
GUIDELINE RECOMMENDATIONS FOR THE MANAGEMENT OF MENOPAUSAL
SYMPTOMS
NAMS Position Statement 2010
• Estrogen Therapy, with or without a progestogen, is the most effective treatment for menopausal-related vasomotor symptoms
• Individualization of therapy is key
• Low absolute risk potential for Hormone Therapy
“ Growing body of evidence that each type of estrogen and progestogen, route of administration and timing of therapy
has distinct beneficial and adverse effects.”
• Further research essential
Estrogen and progestogen use in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause 2010;17(2):242-55.
SOGC Consensus Recommendations 2009 Update
• Menopause is a major life transition with opportunity for healthy interventions
• Patient concerns may be related to aging as well as menopause specific
• Primary indication for HT: – Management of moderate to severe menopausal symptoms
(Grade A)
• HT should not be prescribed for primary or secondary prevention of: – Cardiovascular disease
– Primary prevention of dementia (Grade A)
Menopause and osteoporosis update 2009. J Obstet Gynaecol Can 2009;31(1 Suppl 1):s1-s48. Canadian Consensus on Menopause, 2006 update. J Obstet Gynaecol Can 2006;28 Spec ed;s1-s112.
SOGC Consensus Update 2009: Dose and Duration of HT
• Appropriate route and dose, according to symptoms – Vaginal preferred for vaginal symptoms only
• HT should be prescribed at the appropriate dose and duration to achieve treatment goals
• Prolonged treatment may be offered with appropriate assessment and counselling
Menopause and osteoporosis update 2009. J Obstet Gynaecol Can 2009;31(1 Suppl 1):s1-s48. Canadian Consensus on Menopause, 2006 update. J Obstet Gynaecol Can 2006;28 Spec ed;s1-s112.
2014/10/07
10
Endocrine Society Scientific Statement on HT
• Overall mortality: Menopausal HT (MHT) was associated with a 40% reduction in mortality in trials in which participants had a mean age below 60 yr or were within 10 yr of menopause onset.
• Standard-dose oral MHT may increase stroke risk by about 1/3 in generally healthy postmenopausal women.
• Transdermal estrogen does not increase venothrombotic episode risk.
• Micronized progesterone in combination with estrogen does not increase breast cancer risk if given for 5 years or less.
Santen RJ, et al. 2010, Postmenopausal hormone therapy: an Endocrine Society
Scientific Statement. J Clin Endocrinol Metab 2010;95(7 Suppl 1):S1-S66.
The Medical Letter Position BHT
“There is no acceptable evidence that “bioidentical” (custom-compounded)
hormones are safe or effective.
Patients should be discouraged
from taking them.”
May 2010
Bioidentical hormones. Med Lett Drugs Ther 2010;52(1339):43-4.
Summary
• Primary purpose for prescribing HT remains symptomatic relief
• Transdermal estrogens are considered part of the armamentarium of HT
– May offer certain benefits in specific clinical scenarios
• Micronized progesterone may also offer benefits in bleeding patterns and reduced risk of breast cancer compared to MPA
• Evidence-based recommendations for management of menopausal symptoms can help guide optimal treatment decisions
SOGC Trusted Resources
• sogc.org
• menopauseandu.ca
• endometriosisinfo.ca
• sexualityandu.ca
• hpvinfo.ca
A 53-year-old patient continues to complain of low libido. She has had a simple hysterectomy for fibroids in the past, and her menopausal symptoms are now well controlled using a daily dose 1 mgm of micronized estradiol p.o. You have taken a sexual history and provided appropriate counseling. Which of the following would you consider, if any?
1. Obtain serum levels of total , free and bio-available testosterone2.
2. Obtain levels of SHBG
3. Start transdermal testosterone therapy
4. Change from oral to trans-dermal estrogen therapy
5. Start oral androgen therapy
6. Maintain status
7. All of the above
Question # 1
Which one of the following regimens would be considered “bio-identical’?
1. Transdermal estradiol and oral micronized progesterone
2. Combination estradiol norethindrone acetate patch
3. Transdermal estradiol patch and levonorgestrol IUD
4. Oral ethinyl estradiol and drospirenone
5. All of the above
Question # 2
2014/10/07
11
Micronized progesterone is advised/approved for the following indications:
1. Primary endometrial protection in menopausal women on estrogen
2. Primary endometrial protection in women using vaginal estrogen
3. Primary treatment for sleep disorders in menopause
4. Primary treatment for irregular bleeding in menopause
Question # 3 Question # 4
• All of the following are absolute contraindications to HT except:
– Acute liver disease
– Active thromboembolic disease
– Smoking
– Breast cancer
Transdermal estrogens do all the following except:
1. Improve HDL cholesterol
2. Increase the markers of inflammation such as C reactive protein
3. Decrease triglycerides
4. Have a demonstrable lower VTE risk compared to oral estrogens
Question # 5
Which technique should NOT be used to reduce the dose of
transdermal estrogen?
1. Reduce the surface area of gel application
2. Reduce the number of pumps of gel
3. Cut the reservoir patch
4. Cut the matrix patch
5. Use a lower dose patch
Question # 6
Which of the following is INCORRECT regarding micronized
progesterone?
1. Micronization prevents progesterone breakdown in the GI tract
2. Cannot be given to individuals with a peanut allergy
3. Is not metabolized by the liver
4. May exhibit somnolence as a side effect
5. Can be used in conjunction with estrogen patches
Question # 7
For women who have not had a hysterectomy, a progestin is
recommended when using local (vaginal) estrogen.
1. True
2. False
Question # 8

2014/10/07
12
The treatment of menopausal symptoms should not be started
until a woman stops menstruating or has a documented FSH
>26 micromoles/litre
1. True
2. False
Question # 9
Oral HT increases the risk of thrombotic events in:
a. Obese patients
b. In patients with a family history of DVT
c. In long-term users of HT
d. In new users of HT
e. In surgical patients
1. ALL OF THE ABOVE
2. NONE OF ABOVE
3. A AND C
4. B AND D
5. A,B,C AND D
Question # 10
The progestin addition to estrogen in HT:
1. Does not affect hot flash frequency
2. Does not affect incidence of breast cancer
3. Protects against endometrial cancer
4. Affects the incidence of DVT
5. Provides contraception
Question # 11
Current indications for HT in 2011 state that HT:
1. Can only be prescribed for 5 years
2. Is a good therapy for symptomatic patients with osteoporosis
3. Improves mood for perimenopausal patients
4. Improves memory in menopausal patients
5. Prevents myocardial infarctions
Question # 12
HT is associated with a reduction in mortality if initiated in
women under 60 years old or within 10 years of menopause
onset.
1. True
2. False
Question # 13
The risk of VTE increases with the duration of HT.
1. True
2. False
Question # 14

2014/10/07
13
There is some good evidence confirming that black cohosh, red
clover and/or evening primrose oil decrease the amount of hot
flashes in menopausal women compared to placebo.
1. True
2. False
Question # 15 Question # 16
A 51-year-old woman has transdermal estradiol gel and an oral progestin for
her menopausal symptoms. She is using 2 pumps (2.5 g) / day but tells you
that she has not had much improvement. Your next most appropriate step
is to:
1. Measure serum levels of estradiol
2. Review with her how and where she is applying gel
3. Increase to three pumps/day
4. Add a local vaginal estrogen
5. Add a low dose SNRI
3. Increase to three pumps/day
2. Review with her how and where she is applying gel
A 45-year-old woman has had an early spontaneous menopause.
She has chosen EPT to manage disruptive symptoms. She is
particularly bothered by sleep disruption, which is compromising
her day time function. Which of the following will you
recommend?
1. Combination transdermal EP patch
2. Combination oral estradiol and norethindrone acetate
3. Transdermal estradiol gel and medroxyprogesterone acetate po
4. Estradiol patch and micronized progesterone
5. All of the above
Question # 17
76
Nurses’ Health Study: Major Coronary Heart Disease
Conjugated estrogen
Person years Multi-variate RR 95% CI
Never 313,661 1.0
0.3 mg 19,964 0.58 0.37-0.92
0.625 mg 116,150 0.54 0.44-0.67
1.25 mg 39,026 0.70 0.51-0.97
Grodstein F, et al. A prospective observational study of postmenopausal hormone therapy and primary prevention of cardiovascular disease. Ann Intern Med 2000;133(12):933-41.
Bleeding Patterns on Continuous - Combined HRT: MPA vs. MP
Study Incidence of Bleeding During First 6 - 12 Months of HT
CEE+MPA (2.5 mg)1
CEE+MPA (5 mg)1
Transdermal E2 (50 mg/d) + MP* (100 mg, 25 d/month)
% of cycles
38 27 162 53
% of patients
59 47 292 203
1. Archer DF, et al. Bleeding patterns in postmenopausal women taking continuous combined or sequential regimens of conjugated estrogens with medroxyprogesterone acetate. Menopause Study Group. Obst Gynecol 1994;83(5 Pt 1):686-92.
2. Gillet JY, et al. Induction of amenorrhea during hormone replacement therapy: optimal micronized progesterone dose. A multicenter study. Maturitas 1994;19(2):103-115. 3. Foidart JM, et al. Impact of percutaneous oestradiol gels in postmenopausal hormone replacement therapy on clinical symptoms and endometrium. Br J Obstet Gynecol 1997;104:305-310.
*MP is associated with a lower incidence of bleeding

2014/10/07
14
MPA , 10 mg/d (n=19)
Nomogestrol acetate, 5 mg/d
(n=22)
Dydrogesterone, 10 mg/d (n=19)
MP, 200 mg/d (n=19)
Number of cycles evaluated
224 262 226 225
Duration of regular progestogen-related bleeding, median (range)
3.9 (2.8-5.1) 4.2 (3.1-5.3) 4.0 (2.6-5.4) 4.4 (2.9-5.9)
Irregular bleeding (% of cycles)
8.4% 5.7% 7.5% 12%*
Spotting (% of cycles) 9.8% 6.8% 8.8% 16%**
Amenorrhea (% of cycles)
9.8% 5.7% 8.4% 7.5%
All patients received transdermal 17b-estradiol, 50 µg/day. *P<0.05 vs. nomogestrol acetate. **P<0.05 vs. nomogestrol acetate and dydrogesterone; P=0.051 vs. MPA.
Di Carlo C, et al. Bleeding patterns during continuous estradiol with different sequential progestogens therapy. Menopause 2005;12(5):520-5.
12 d/mo x 12 mo
Comparison of Bleeding Patterns With Cyclic Progestogens
Postmenopausal HT and Risk of VTE: Results of the E3n Trial (cont’d)
1.0
Multivariate-adjusted hazard ratio* (95% CI)
1.5 2.0 0.5
No progestogens use (n=26)
Current use of micronized progesterone (n=47)
Current use of norpregnane derivatives (n=69)
Current use of nortestosterone derivatives (n=22)
---
Age-adjusted HR Multivariate-adjusted HR*
---
0.9 (0.6 -1.4)
1.4 (0.8 -2.5)
1.0 (0.7 -1.5)
0.9 (0.6 -1.5)
1.4 (0.7 -2.4)
1.1 (0.7 -1.8)
2.5
Canonico M, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol 2010;30(2):340-
5.
Hazard ratios of idiopathic VTE in relation to both estrogens by route of administration and concomitant progestogens
*Adjusted for age, body-mass index, parity, educational level and time-period.
Progestogens
• Any substance that has progestational activity
• Includes “natural” and “bioidentical” progesterone and synthetic progestins
• Progestins are synthetic progestogens with biologic activity to progesterone
• Oral progesterone is broken down in GI tract and therefore is inactive
• Progestins were developed which are not broken down in the GI tract; derived from progesterone or testosterone (19-nortestosterone) precursors
• Once micronization was discovered, progesterone could be given orally
Progestogen Selection
Two different classes of progestogens are used in HT:
1. 17-hydroxyprogesterone (norpregnane) derivatives (including medroxyprogesterone acetate [MPA], megestrol, and progesterone)
2. 19-nortestosterone derivatives (norethindrone and norethindrone acetate)
Menopause and osteoporosis update 2009. J Obstet Gynaecol Can 2009;31(1 Suppl 1):s1-s48. Canadian Consensus on Menopause, 2006 update. J Obstet Gynaecol Can 2006;28 Spec ed;s1-s112.
WHI Re-analysis: Effect of Estrogen Alone on Major Outcomes for Women <60 Years Old
Event % difference in RR to Placebo (95% CI)
# of events/10,000 women/yr of CEE alone
therapy
Coronary heart disease -37 (0.36-1.09) -11
Stroke -11 (-.47-1.69) -2
Venous thromboembolism +37 (0.70-2.68) +4
Breast Cancer -18 (0.65-1.04) -8
Fractures -30 (0.59-0.83) -56
New-onset diabetes -12 (0.77-1.01) -14
Total mortality -29 (0.46-1.11) -11
Hodis H, Mack WJ. Postmenopausal hormone therapy in clinical perspective. Menopause 2007;14(5):944-57.
WHI Re-analysis: Effect of Conjugated Equine Estrogen Alone on Stroke
LaCroix AZ, et al. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy: a randomized controlled trial. JAMA. 2011;305(13):1305-14.