satheesh krishna sabarish narayanasamy wael shabana c.ymcdn.com/sites/ · pdf filesatheesh...
TRANSCRIPT

Satheesh Krishna Sabarish Narayanasamy Wael Shabana Adnan Sheikh
Department of Medical Imaging, The Ottawa Hospital.

Nothing to disclose

Common and unusual presentations and manifestations of testicular torsion
Identify common, uncommon and unusual causes of testicular ischemia and differentiate them from torsion of the testis

• 9 year old male with 6
hour history of right
scrotal pain.
• Ultrasound (US) shows
subtle reduction of
vascularity to right testis
compared to left.
• Intraoperatively, torsion
was confirmed, testis was
viable and orchidopexy
was done.
Right
Left

• Presence of vascularity does not always exclude torsion
• Vascularity in both testes should always be compared for subtle differences

• US demonstrates
complete absence of
flow and
heterogeneous
testicular echo texture.
Features are
suggestive of testicular
necrosis secondary to
torsion.
• Swirl sign (arrow)
reflects twisting of the
spermatic cord

Early diagnosis is crucial as likelihood of testicular salvage depends on time interval between onset and surgery

22 year old male with 4 hour history of left scrotal pain. Pain
completely relieved en route to hospital. Ultrasound shows subtle
increased vascularity to left testis compared to right. Epididymis
was normal (inset). Findings were confirmed intraoperatively.
Left Right

Classical history with subtle hyperemia should raise concern of possible torsion followed by spontaneous detorsion.
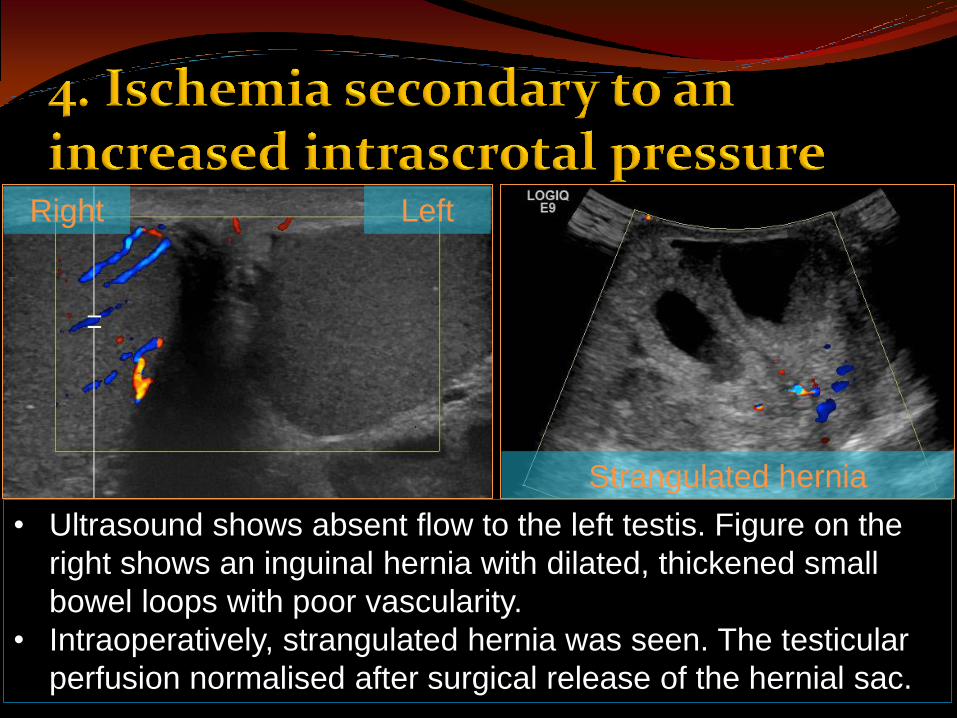
• Ultrasound shows absent flow to the left testis. Figure on the
right shows an inguinal hernia with dilated, thickened small
bowel loops with poor vascularity.
• Intraoperatively, strangulated hernia was seen. The testicular
perfusion normalised after surgical release of the hernial sac.
Strangulated hernia
Right Left

• Ultrasound demonstrates a tense hydrocele on the right with
no demonstrable internal vascularity in right testes.
• Testicular flow normalised after drainage of hydrocele.
Tense hydrocele
Right Post surgery Absent vascularity

• Increased intrascrotal pressure can cause secondary testicular ischemia.
• Urgent correction of the primary cause is necessary to preserve testicular viability.

• Decreased flow
with high
resistance in a
chronically
atrophic testis
from prior
orchitis.
• Contralateral
testis showing
normal flow.
• Testicular
hypoperfusion
may be chronic.
Right
Left
Right

Left Left
• 45 year old male with left scrotal discomfort/pain.
• History of vasectomy 4 months prior. Ultrasound shows diffuse
hypoechogenicity and segmental absence of flow in the upper
two-thirds of the testicular parenchyma.
• Testicular ischemia was secondary to gonadal artery injury
from the prior vasectomy surgery.

• 65 year old male with a 4-day history of testicular pain.
• Ultrasound shows complete absence of flow within the testis.
However, the epididymis was bulky and hyperemic (orange arrow).
Surrounding septated hydrocele was also noted (yellow arrow).
• Intraoperatively, there was no evidence of torsion!!
• Inflamed, red epididymis was seen with infected hydrocele fluid.
• Testicular ischemia was sequel to epididymitis. Postulated
mechanism is venous thrombosis.

• Testicular torsion usually results in absent flow in both the testes and epididymis.
• Absent testicular flow with preserved or increased flow in epididymis should suggest other etiologies.

• 23 year old male with history
of trauma with severe pain.
• Absence of flow in lower
portion of testis with
geographic well demarcated
hypoechogenicity (arrow).

Geographic hypoechogenicity reaching the capsule with absence of flow is diagnostic of testicular rupture in the setting of trauma.

• 18 year old was kicked in testicle.
• US shows no fracture or hematoma.
• Diffusely heterogenous echotexture of
the testes with absent color flow.
• Swirling of cord was noted (not shown)
and a diagnosis of torsion was made.

Torsion of spermatic cord can be secondary to testicular trauma.

There is apparent reduced
flow in the left testis
compared to the right. This
can potentially mimic
ischemia/torsion of the left.
However, apparent reduced
flow in left testes is due to
increased vascularity on the
right. Patient had right sided
epididymo-orchitis with pain
and swelling on the right side.
Hence it is important to know
which testis is symptomatic.
Right Left
Right

Hyperperfusion in the contralateral testis can potentially mimic torsion due to apparent appearance of reduced flow in the other testis. Clinical history is of paramount importance.

A variety of causes (acute, subacute and chronic) may result in testicular ischemia manifesting as decreased colour flow on Doppler ultrasound.
Depending on the cause of ischemia, they may be potentially emergent conditions requiring urgent management or chronic incidental findings managed conservatively.
Familiarity with various causes and features of testicular ischemia is essential to help guide management.

Satheesh Krishna Jeyaraj
Fellow in Abdominal Imaging,
The Ottawa Hospital,
501, Smyth Road,
Ottawa,
K1H 8L6
Email: [email protected]