royal national hospital for rheumatic diseases university
TRANSCRIPT
Psoriatic arthritisNeil McHugh
Royal National Hospital for Rheumatic DiseasesUniversity of Bath
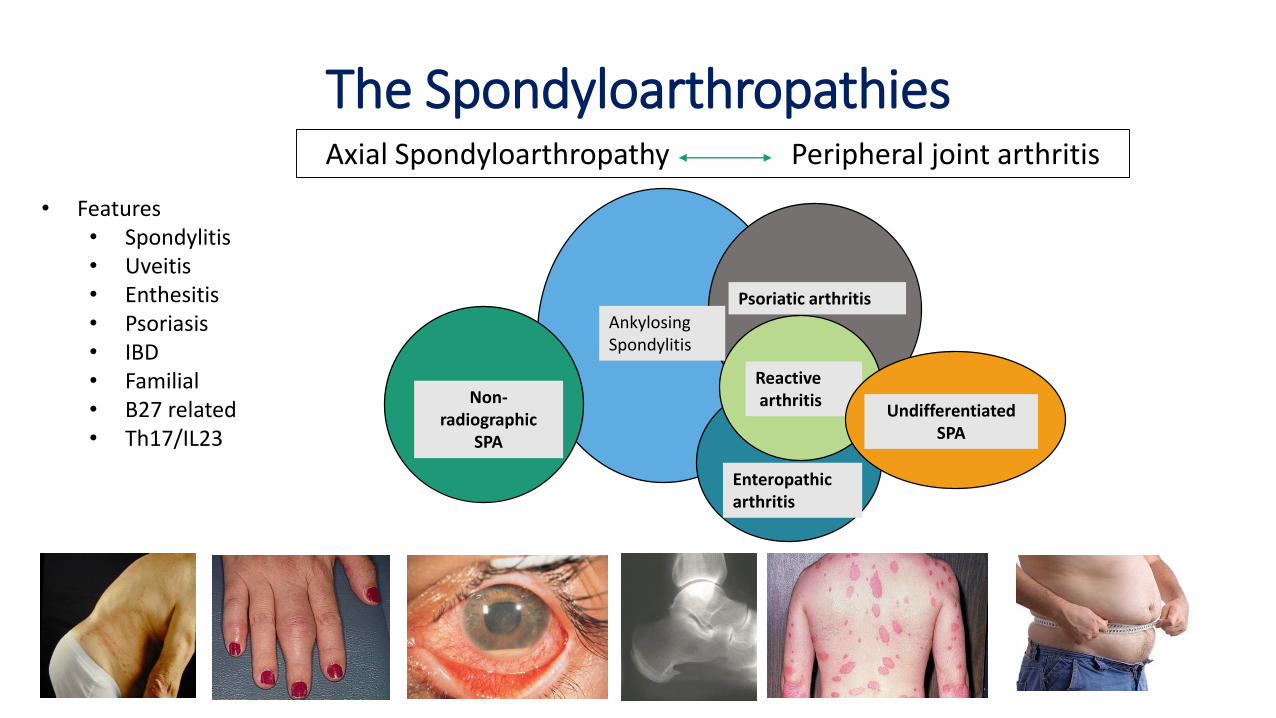
AnkylosingSpondylitis
Psoriatic arthritis
Enteropathicarthritis
Reactivearthritis
• Features• Spondylitis• Uveitis• Enthesitis• Psoriasis• IBD• Familial• B27 related• Th17/IL23
Non-radiographic
SPA
UndifferentiatedSPA
Axial Spondyloarthropathy Peripheral joint arthritis
The Spondyloarthropathies

Topographical association betweennail disease and DIPJ involvement
Psoriasis and ArthritisV WrightAnn Rheum Dis 1956, 15, 348
‘This arthritis was less severe than rheumatoid arthritis, and was characterized by distalinterphalangeal joint involvement, erosion of the terminal phalanges, and a greater incidence of sacro-iliac joint changes.’

Burden of psoriatic arthritis
• Joint damage in 50% within 2 years of disease
• Reduced quality of life similar to rheumatoid arthritis
• Comorbidities – e.g. obesity, cardiovascular disease, uveitis
• One in three unemployed
• High direct health costs (£4832 per patient-year)
Husted Arthritis Rheum 2001
Sokoll J Rheumatol 2001
Lindqvist J Rheumatology 2008
Kane et al Rheumatology 2003

Diagnosis of psoriatic arthritis

Moll and Wright subgroups of psoriatic arthritis
Predominantly DIP Disease
Oligoarthritis
Polyarthritis
Arthritis Mutilans
Spondylitis
Seminar Arthritis Rheum 1973

The CASPAR criteria
To meet the CASPAR criteria a patient must have an inflammatory articular disease (joint, spine or entheseal) and ≥ 3 points from:
1. Current psoriasis 2 points
or Personal history of psoriasis 1 point
or FH of psoriasis 1 point
2. Current psoriatic nail dystrophy 1 point
3. Negative RF 1 point
4. Current or Rheumatologist confirmed dactylitis 1 point
5. Juxta-articular new bone formation 1 point
Taylor et al 2006. Arthritis and Rheum; 54, 2665-2673

Psoriatic arthritis
• Skin psoriasis affects 2-3% of normal population often with nail disease
• About 30% of individuals with psoriasis develop a distinct form of inflammatory arthritis called psoriatic arthritis
• Estimated 400,000 in England
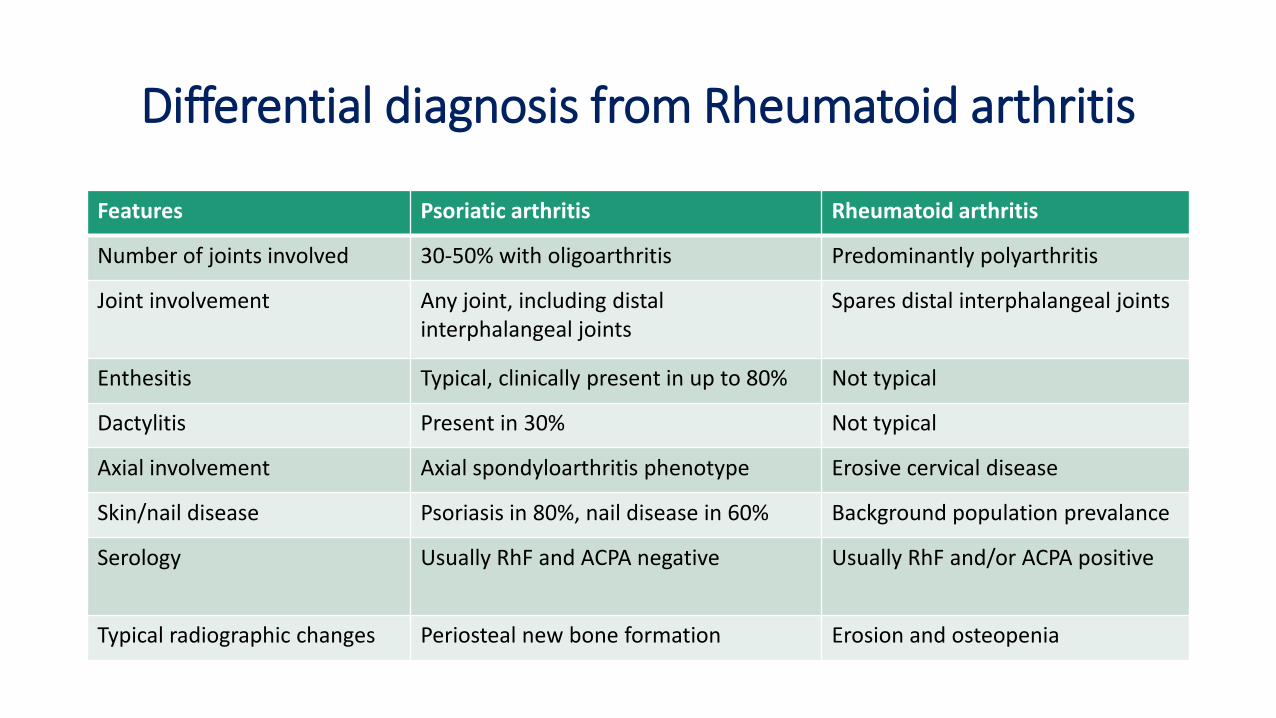
Differential diagnosis from Rheumatoid arthritis
Features Psoriatic arthritis Rheumatoid arthritis
Number of joints involved 30-50% with oligoarthritis Predominantly polyarthritis
Joint involvement Any joint, including distal interphalangeal joints
Spares distal interphalangeal joints
Enthesitis Typical, clinically present in up to 80% Not typical
Dactylitis Present in 30% Not typical
Axial involvement Axial spondyloarthritis phenotype Erosive cervical disease
Skin/nail disease Psoriasis in 80%, nail disease in 60% Background population prevalance
Serology Usually RhF and ACPA negative Usually RhF and/or ACPA positive
Typical radiographic changes Periosteal new bone formation Erosion and osteopenia

Radiographic and MRI features of psoriatic arthritis
McGonagle and Tan Clin Exp Rheum 2015Tillett and McHugh Oxford Textbook PsA 2017

Clinical Practice Research Datalink• Median interval between psoriasis
and PsA 8 years (excluding synchronous
onset 9 years)
• 60% diagnosed within 10 years
RNHRD PsA Database• Median interval between psoriasis
and PsA 7 years (excluding synchronous
onset 13 years)
• 57% diagnosed within 10 years
Time interval from first psoriasis record to first PsA record
comparing CPRD to Bath Psoriatic arthritis cohort
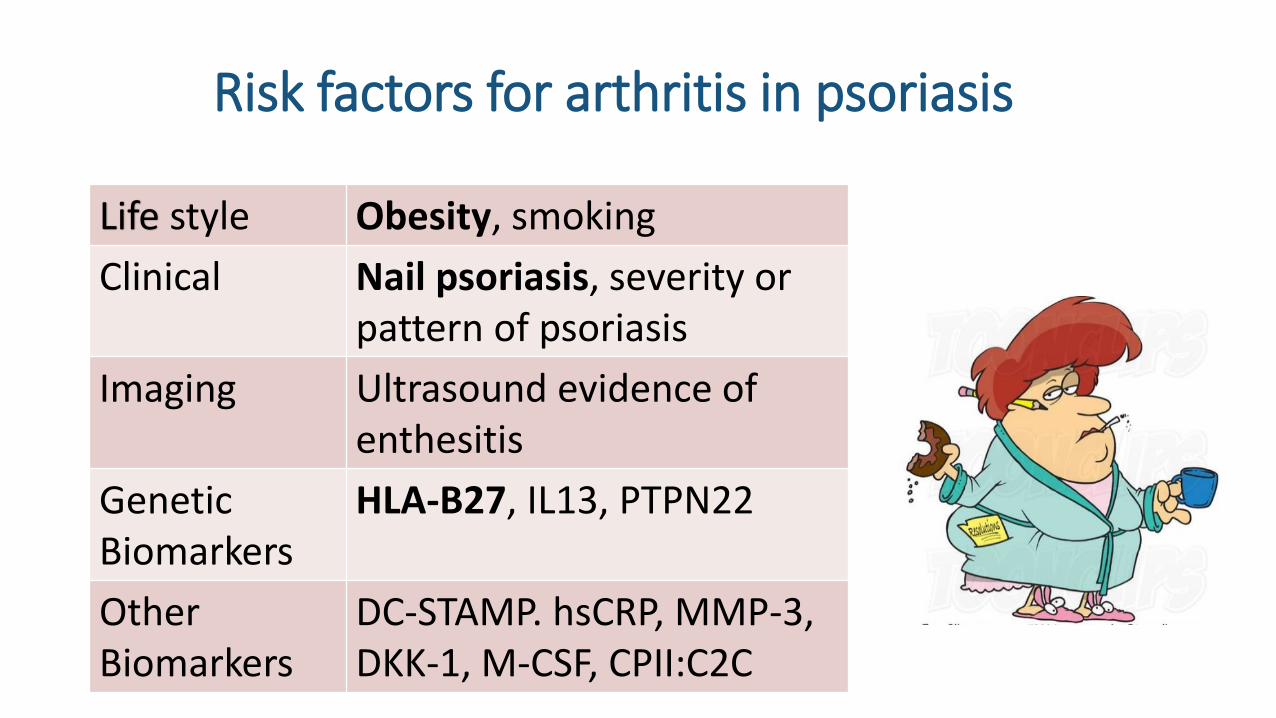
Risk factors for arthritis in psoriasis
Life style Obesity, smoking
Clinical Nail psoriasis, severity or pattern of psoriasis
Imaging Ultrasound evidence of enthesitis
Genetic Biomarkers
HLA-B27, IL13, PTPN22
Other Biomarkers
DC-STAMP. hsCRP, MMP-3, DKK-1, M-CSF, CPII:C2C

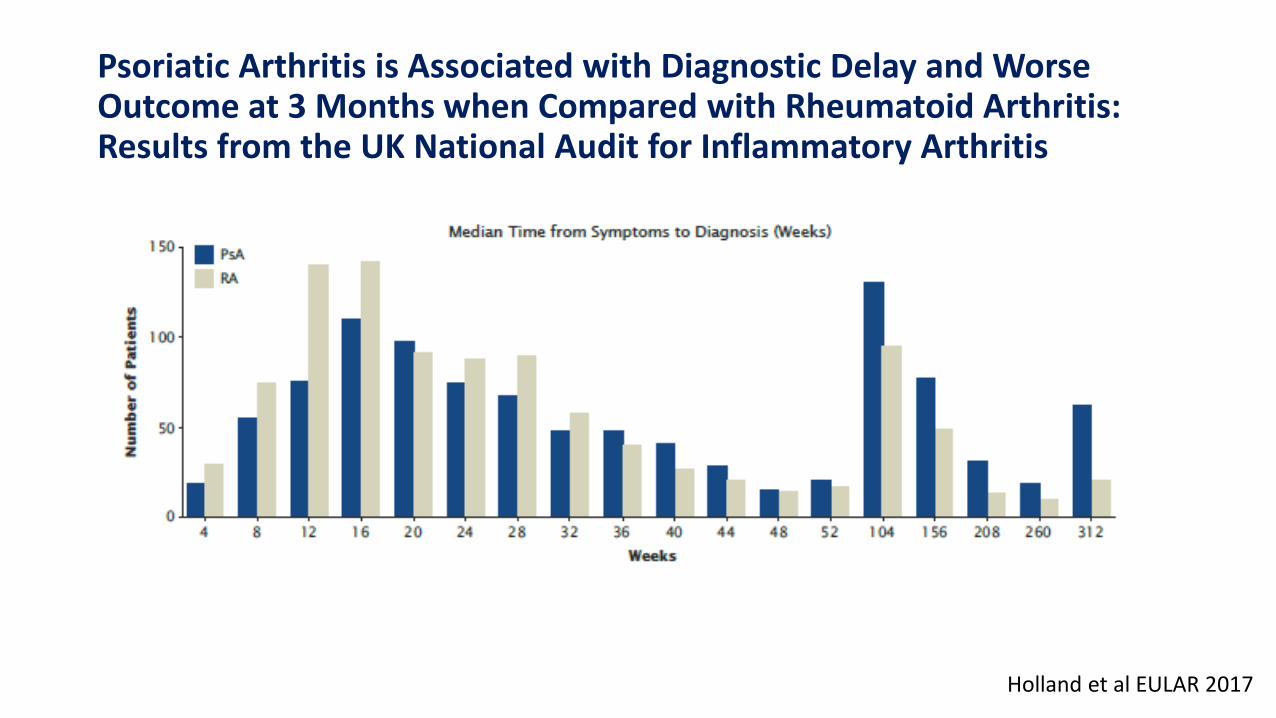
Psoriatic Arthritis is Associated with Diagnostic Delay and Worse Outcome at 3 Months when Compared with Rheumatoid Arthritis: Results from the UK National Audit for Inflammatory Arthritis
Median time to diagnosis in weeks
Holland et al EULAR 2017
PsA (n=1016) RA (n=1016)
Symptoms to GP presentation 8.9 6.6
GP presentation to referral 5.4 4
GP presentation to diagnosis 12.1 9.7
Symptoms to diagnosis 28.6 21.6
Adjusted for age, sex, ethnicity and deprivation index; P<0.02 for all between-group comparisons
Psoriatic Arthritis is Associated with Diagnostic Delay and Worse Outcome at 3 Months when Compared with Rheumatoid Arthritis: Results from the UK National Audit for Inflammatory Arthritis
Holland et al EULAR 2017

How important is detection of early psoriatic arthritis?
• Recent meta-analysis suggest between 10-15 % prevalence of undiagnosed PsA in dermatology clinics1
• Delay in diagnosis may be associated with poor outcome
• Most studies are retrospective and have selection and recall bias
• NICE recommends annual screening for patients in primary care on treatment for psoriasis
• At least 40% people with psoriasis not on treatment or not attending healthcare2
1 Vilani et al JAAD 20152 Lebwohl AJCD 2015

Assessment of psoriatic arthritis
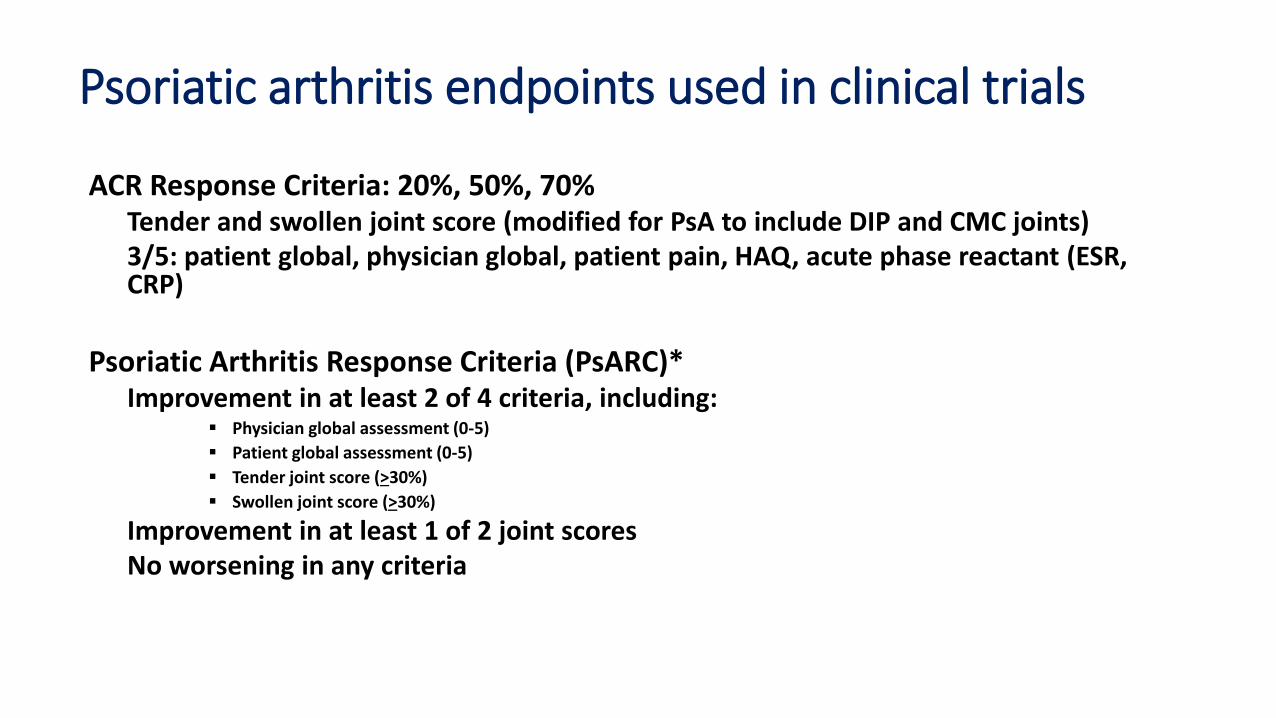
Psoriatic arthritis endpoints used in clinical trials
ACR Response Criteria: 20%, 50%, 70%Tender and swollen joint score (modified for PsA to include DIP and CMC joints)3/5: patient global, physician global, patient pain, HAQ, acute phase reactant (ESR, CRP)
Psoriatic Arthritis Response Criteria (PsARC)*Improvement in at least 2 of 4 criteria, including:
Physician global assessment (0-5)
Patient global assessment (0-5)
Tender joint score (>30%)
Swollen joint score (>30%)
Improvement in at least 1 of 2 joint scoresNo worsening in any criteria
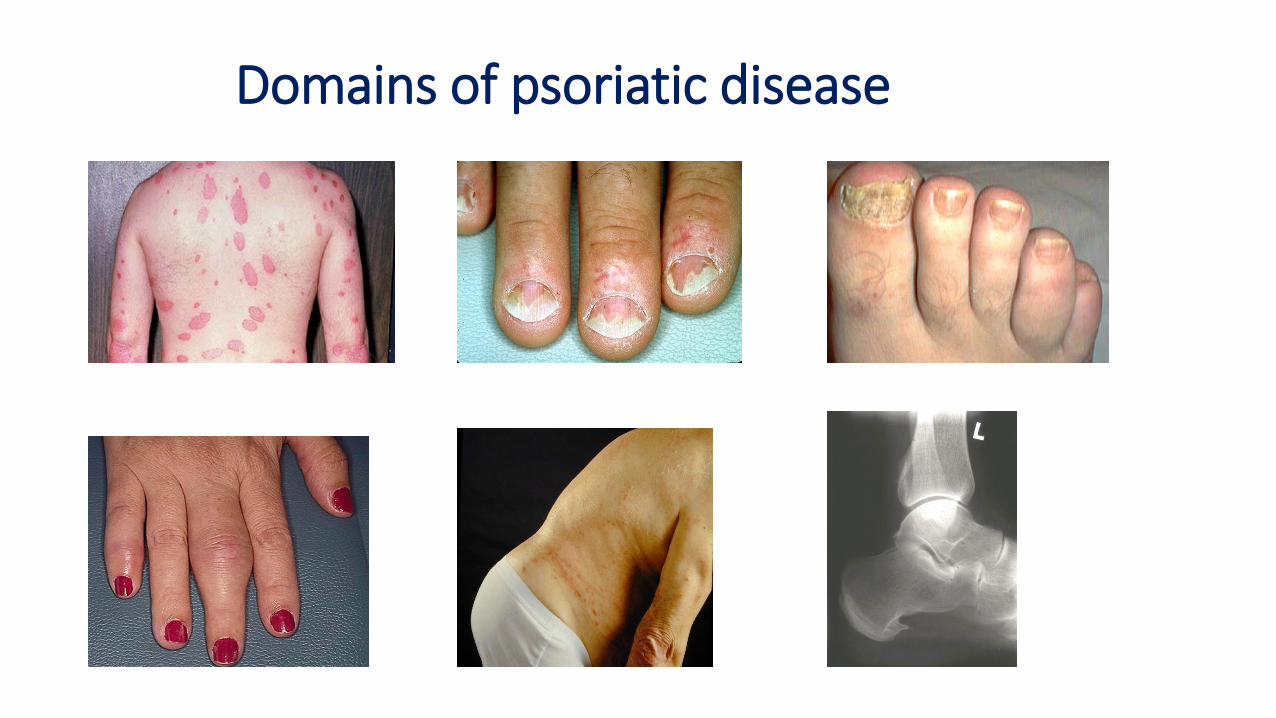
Domains of psoriatic disease

CPDAI (composite psoriatic disease activity index)None (0) Mild (1) Moderate (2) Severe (3)
Peripheral
Arthritis
≤ 4 joints; normal
function (HAQ <0.5)
≤ 4 joints but function
impaired; or > 4 joints,
normal function
> 4 joints and function
impaired
Skin Disease PASI ≤ 10 and DLQI
≤ 10
PASI ≤ 10 but DLQI >10;
or PASI > 10 but DLQI ≤
10
PASI > 10 and DLQI > 10
Enthesitis ≤ 3 sites; normal
function (HAQ <0.5)
≤ 3 sites but function
impaired; or >3 sites but
normal function
>3 sites and function
impaired
Dactylitis ≤ 3 digits; normal
function (HAQ <0.5)
≤ 3 digits but function
impaired; or >3 digits but
normal function
>3 digits and has function
impaired
Spinal Disease BASDAI <4; normal
function (ASQol < 6)
BASDAI >4 but normal
function; BASDAI <4 but
function impaired
BASDAI >4 and function
impaired

ACTIVITY
DamageImpact of
Disease
Disease
Severity*
Reversible
Irreversible
*Total effect of disease on organ function
Musculoskeletal
Psychosocial
Cardiovascular
Patient reported outcomes
HAQ
ASQOL
DLQI
SF36
EQ5D
WPAI
ACR 20
PsARC
PASI 75
CPDAI
PASDAS
AMDF
DAPSA
Sharp score
Mortality
66/68 joint
score
BASDAI
PASI score
NAPSI
Enthesitis score

Do we have the correct outcome measures for psoriatic arthritis?
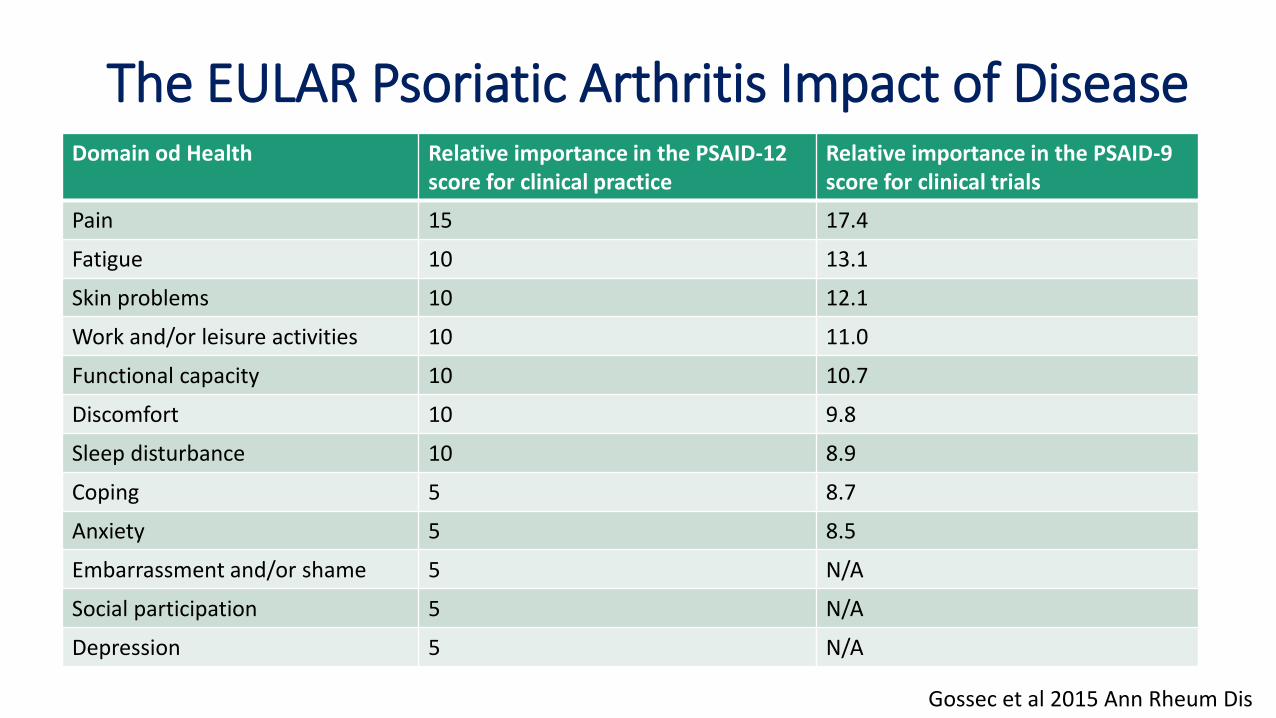
The EULAR Psoriatic Arthritis Impact of DiseaseDomain od Health Relative importance in the PSAID-12
score for clinical practiceRelative importance in the PSAID-9score for clinical trials
Pain 15 17.4
Fatigue 10 13.1
Skin problems 10 12.1
Work and/or leisure activities 10 11.0
Functional capacity 10 10.7
Discomfort 10 9.8
Sleep disturbance 10 8.9
Coping 5 8.7
Anxiety 5 8.5
Embarrassment and/or shame 5 N/A
Social participation 5 N/A
Depression 5 N/A
Gossec et al 2015 Ann Rheum Dis

Ann Rheum Dis 2017
Revised 2016 OMERACT core set domains for psoriatic arthritis
International patient and physician consensus on a psoriatic arthritis core outcome set for clinical trials
Ana-Maria Orbai, Maarten de Wit, Philip Mease, Judy A Shea, Laure Gossec, Ying Ying Leung, William Tillett, MusaabElmamoun, Kristina Callis Duffin, Willemina Campbell, Robin Christensen, Laura Coates, Emma Dures, Lihi Eder, Oliver FitzGerald, Dafna Gladman, Niti Goel, Suzanne Dolwick Grieb, Sarah Hewlett, Pil Hoejgaard, Umut Kalyoncu, Chris Lindsay, Neil McHugh, Bev Shea, Ingrid Steinkoenig, Vibeke Strand, Alexis Ogdie
Treatment and guidelines

secukinumab,ustekinumab,
apremilast
2015
Authorisations for therapies with alternative MoAs
brodalumab,tofacitinib,
guselkumab,clazakizumab,ixekizumab,
ABT-122
2016 and The Future
More targets and more options
etanercept
The first biological
therapy: TNFi4
2000 2005
infliximab,adalimumab
2009
golimumab
2014
More TNFi
certolizumabpegol
1990s
RA csDMARDs1
Methotrexate,sulfasalazine etc
c.1960s
PsA described as a clinical
entity
Early treatments: NSAIDs,
corticosteroids
Advancing treatments for psoriatic arthritis
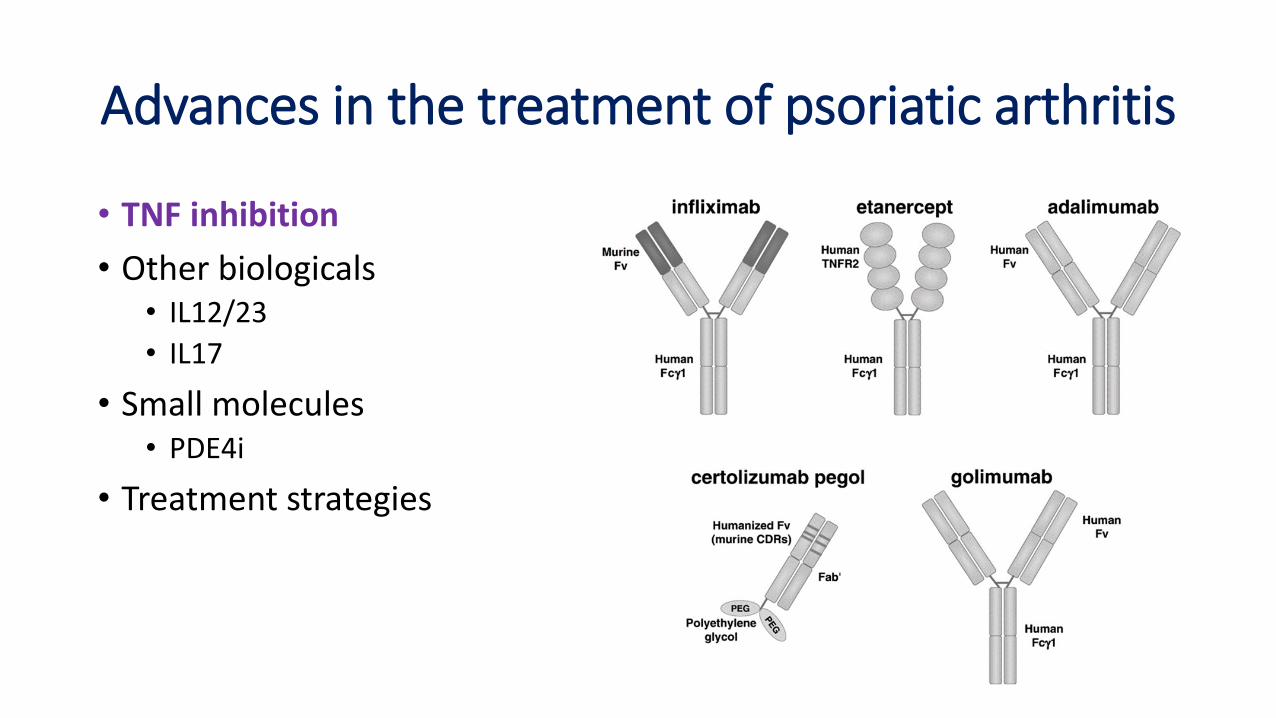
Advances in the treatment of psoriatic arthritis
• TNF inhibition
• Other biologicals• IL12/23
• IL17
• Small molecules• PDE4i
• Treatment strategies

Efficacy of traditional DMARDs vs anti-TNF
LFN: . Peter Kaltwasser, et al., ; CSA: Salvarani et al; SSZ: Salvarani et al; MTX: Kinsgley et al.

Anti-TNF treatments: ACR responses at 12/14 weeks
Trial n ACR20% ACR50% ACR70%
Rx P Rx P Rx P
Adalimumab 315 58 14 36 4 20 1
Certolizumab 409 58 24 36 11 25 3
Etanercept 205 59 15 38 4 11 0
Golimumab 405 52 8 32 3.5 18 0.9
Infliximab 200 58 11 36 3 15 1
• Effective for all domains of disease and slow structural damage
• Risk of infection (e.g. mycobacterium)
• Risk of malignancy and safety in pregnancy and heart failure?
Adapted from Mease Rheum Dis Clin N Am 2015
Predictors of response to anti-TNF
• Positive predictors• Male gender
• High CRP
• Younger age
• Concomitant methotrexate
• Negative predictors• Smoking
• Obesity
• High HAQ-DI

Effectiveness of switching anti-TNF-registry data
• South Swedish Arthritis Treatment Group Register
• ACR20 response at 12 weeks falls to 47% for first time switches and and to 22% for second time switches
• Median drug survival time 64 months for first time switches and 14 months for second-time switches
• Higher HAQ predicted premature drug withdrawal
• Results suggest that other therapeutic options should be considered after 2nd course of anti-TNF
Kristensen et al J Rheum 2016:43:81-87

Advances in the treatment of psoriatic arthritis
• TNF inhibition
• Other biologicals• IL12/23
• IL17
• Small molecules• PDE4i
• Treatment strategies

IL-12 and IL-23 cytokines
Teng et al Nature Med 2015:21:719
• TNF inhibition
• Other biologicals• IL12/23
• IL17
• Small molecules• PDE4i
• Treatment strategies
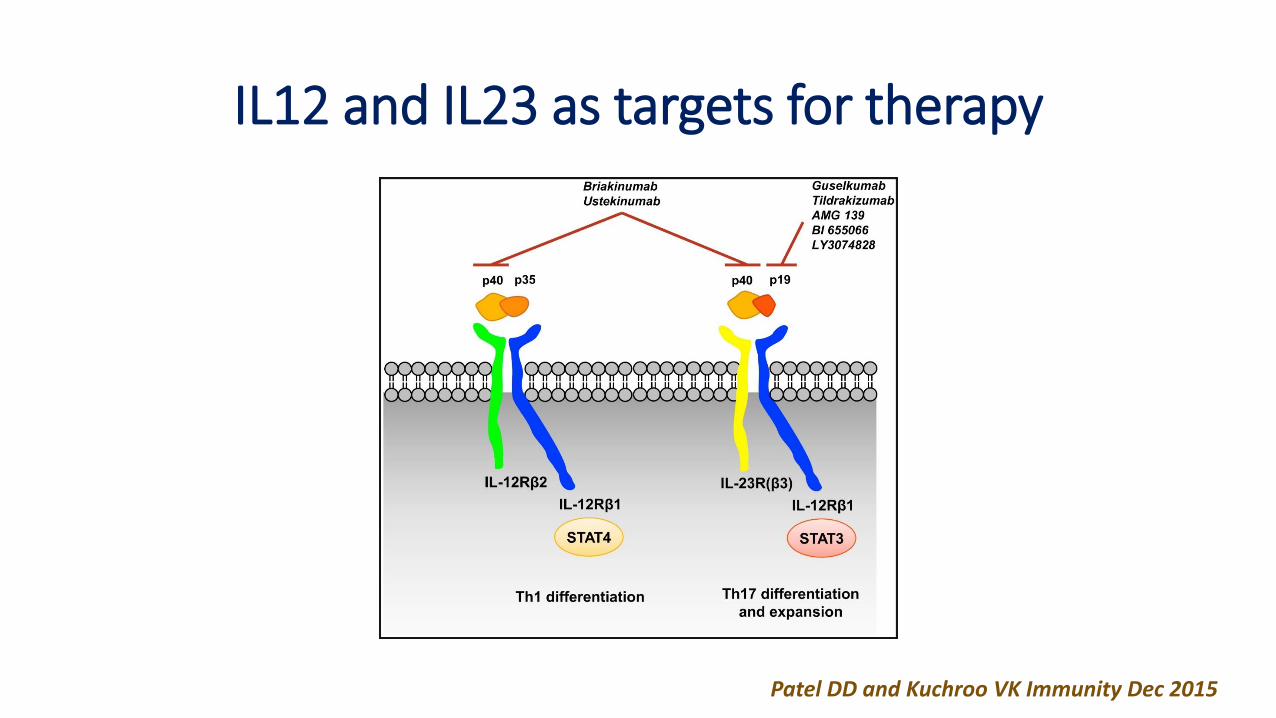
Patel DD and Kuchroo VK Immunity Dec 2015
IL12 and IL23 as targets for therapy

Indications for Ustekinumab
• Recommended by NICE as a possible treatment, alone or with methotrexate, for adults with active psoriatic arthritis, if TNFicontraindicated or failed one or more TNFis
• 90 mg dose at same cost as 45 mg dose for patients > 100 kg
• Stopped after 24 weeks if not working
• Ideal patient• High psoriasis burden
• TNFi refractory, especially primary non-responder
• TNF adverse events ( e.g. lupus-like reaction) or contraindications (recurrent infections?)
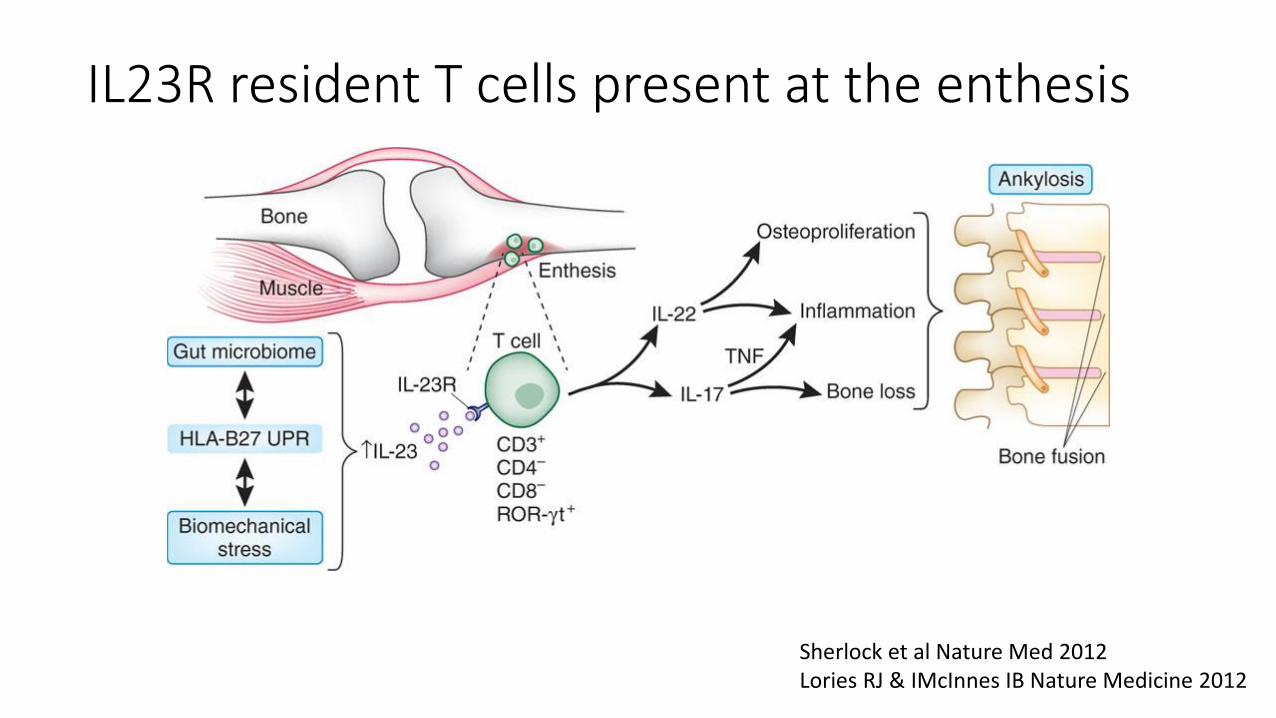
Sherlock et al Nature Med 2012Lories RJ & IMcInnes IB Nature Medicine 2012
IL23R resident T cells present at the enthesis
Advances in the treatment of psoriatic arthritis
• TNF inhibition
• Other biologicals• IL12/23
• IL17
• Small molecules• PDE4i
• Treatment strategies

IL-17 as a target for treatment in psoriatic arthritis
• Interleukin-17A producing cells increased in circulation, joints and skin plaques of patients with PsA
• Synovium of PsA enriched with IL-17 producing CD4+ effector memory T cells, CD4-CD8+ T cells and functionally active IL-17RA
Patel DD et al ARD 2013, Raychaudhuri SP et al Mol Cell Biochem 2012, Menon et al Arthritis Rheum 2014

Patel DD and Kuchroo VK Immunity Dec 2015
IL-17 isoforms as targets for treatment

Busa S & Kavanaugh A Expert Opin. Drug Saf 2015
Apremilast: Mechanism of action
• TNF inhibition
• Other biologicals• IL12/23
• IL17
• Small molecules• PDE4i
• Treatment strategies
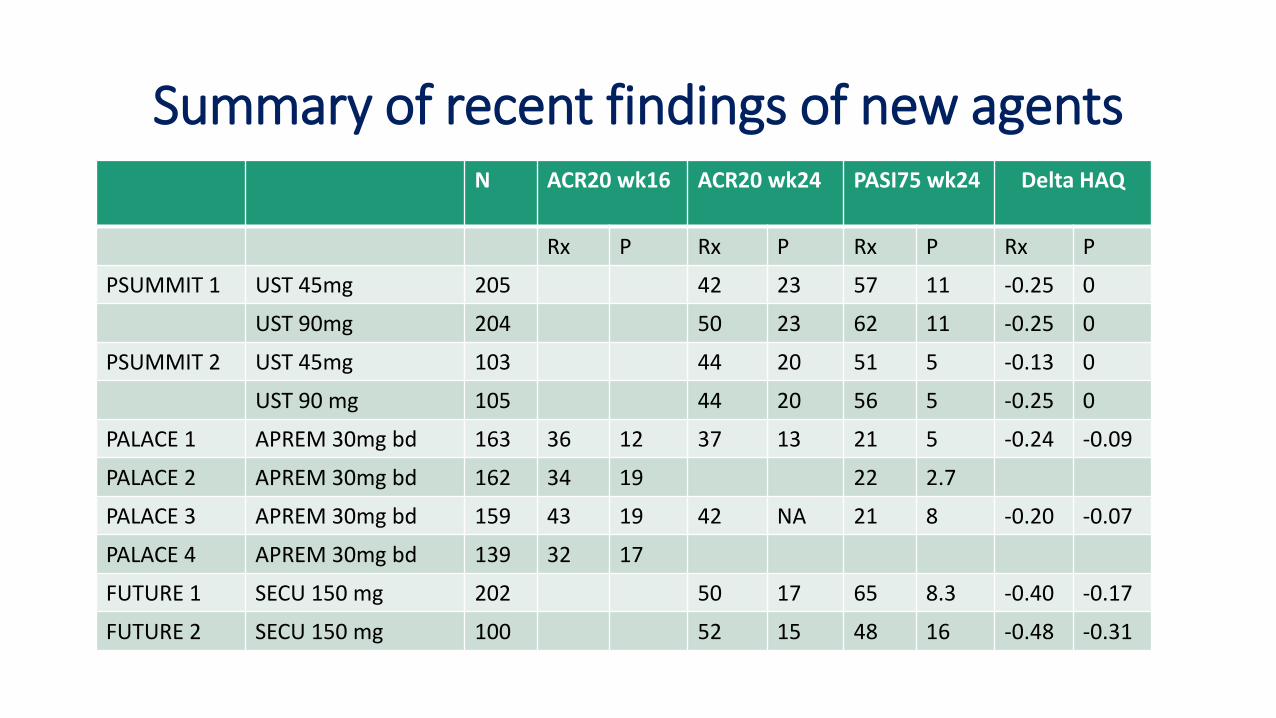
Summary of recent findings of new agentsN ACR20 wk16 ACR20 wk24 PASI75 wk24 Delta HAQ
Rx P Rx P Rx P Rx P
PSUMMIT 1 UST 45mg 205 42 23 57 11 -0.25 0
UST 90mg 204 50 23 62 11 -0.25 0
PSUMMIT 2 UST 45mg 103 44 20 51 5 -0.13 0
UST 90 mg 105 44 20 56 5 -0.25 0
PALACE 1 APREM 30mg bd 163 36 12 37 13 21 5 -0.24 -0.09
PALACE 2 APREM 30mg bd 162 34 19 22 2.7
PALACE 3 APREM 30mg bd 159 43 19 42 NA 21 8 -0.20 -0.07
PALACE 4 APREM 30mg bd 139 32 17
FUTURE 1 SECU 150 mg 202 50 17 65 8.3 -0.40 -0.17
FUTURE 2 SECU 150 mg 100 52 15 48 16 -0.48 -0.31
Advances in the treatment of psoriatic arthritis
• TNF inhibition
• Other biologicals• IL12/23
• IL17
• Small molecules• PDE4i
• Treatment strategies
• Minimal disease activity (MDA) achieved in tight control arm if 5 of the following criteria are met:
• Tender joint count (0-68): ≤1• Swollen joint count (0-66): ≤1• Patient global activity VAS (0-100): ≤20• Patient pain VAS (0-100): ≤15• HAQ-DI (0-3): ≤0.5• Tender entheseal points (0-13): ≤1• PASI (0-72): ≤1 or BSA(0-100): ≤3%
Lancet. 2015 December 19; 386(10012): 2489–2498.
A treat-to-target strategy has effectiveness in PsAand current guidelines support this approach
• In TICOPA, a tight control strategy leads to better outcomes (although greater incidence of AEs) with more patients at MDA and potential associated cost effectiveness in the long-term.
• 2016 GRAPPA recommendations• An ultimate goal of therapy is to achieve the lowest possible level of disease
activity in all domains…
• The treat-to-target approach has also become the first recommendation in 2016 EULAR guidelines
Coates L. C, et al. Lancet. 2015;386:2489─98Coates L. C, et al. Arthritis Rheum. 2016 May;68(5):1060-71 Gossec L, et al. Ann Rheum Dis. 2016 Mar;75(3):499-510.

2016 EULAR guidelines for psoriatic arthritis: management of peripheral joint disease
Gossec et al Nat Rev Rheum 2016

2016 EULAR guidelines for psoriatic arthritis: management of predominant entheseal disease
Gossec et al Nat Rev Rheum 2016

2016 EULAR guidelines for psoriatic arthritis: management of predominant axial disease
Gossec et al Nat Rev Rheum 2016
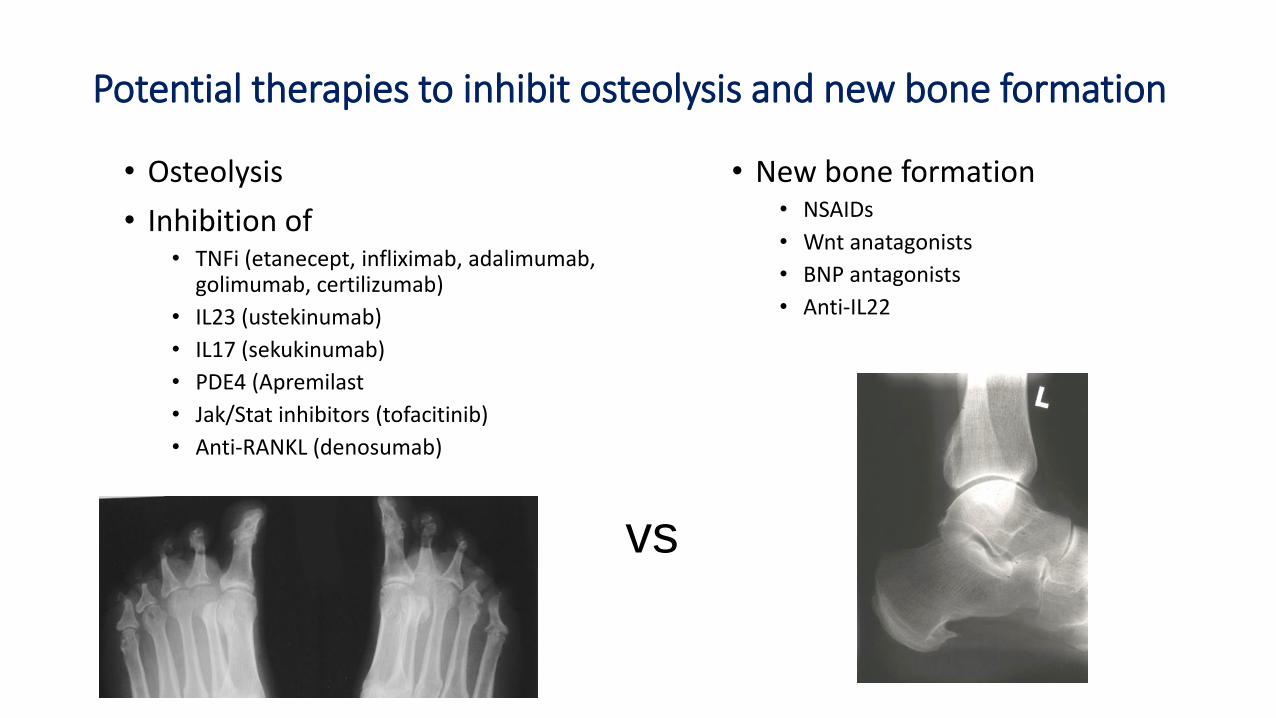
• Osteolysis
• Inhibition of• TNFi (etanecept, infliximab, adalimumab,
golimumab, certilizumab)
• IL23 (ustekinumab)
• IL17 (sekukinumab)
• PDE4 (Apremilast
• Jak/Stat inhibitors (tofacitinib)
• Anti-RANKL (denosumab)
• New bone formation• NSAIDs
• Wnt anatagonists
• BNP antagonists
• Anti-IL22
Potential therapies to inhibit osteolysis and new bone formation
vs

Key messages
• Psoriatic arthritis is not uncommon but is frequently undiagnosed
• In addition to skin psoriasis other important risk factors are obesity, nail disease and HLA-B27
• Significant comorbidities include obesity, uveitis, Crohn’s, and cardiovascular disease
• Newer treatments (e.g. anti-TNF, anti-IL23, anti-IL17) are more effective than traditional DMARDS ( e.g. methotrexate) and small molecule inhibitors are becoming available
• Psoriatic arthritis is not a benign disease