responsible pain management highlighting new regulations of indiana’s medical licensing board and...
TRANSCRIPT

Responsible Pain Management
Highlighting New Regulations of Indiana’s Medical Licensing Boardand Best Practices for Patient Care
Your Name Here

Goals and Objectives
1. Identify trends and consequences of the current opioid epidemic
a) Increased Use
b) Paucity of data supporting COT
c) Data demonstrating perils of COT
2. Review new Indiana laws for opioid prescribing
3. Outline “pearls” for office implementation of best practices and compliance monitoring

Trends and Consequences

We Treat, but Do We Help?
• Aggressive use of opioids and interventional technologies between 1997 and 2005 resulted in ~ 65 % increase in expenditures without evidence of improvement in self-assessed health status and pain.
• Many outcomes were worse
JAMA. 2008; 299(6):656-664

• Pew Health Group
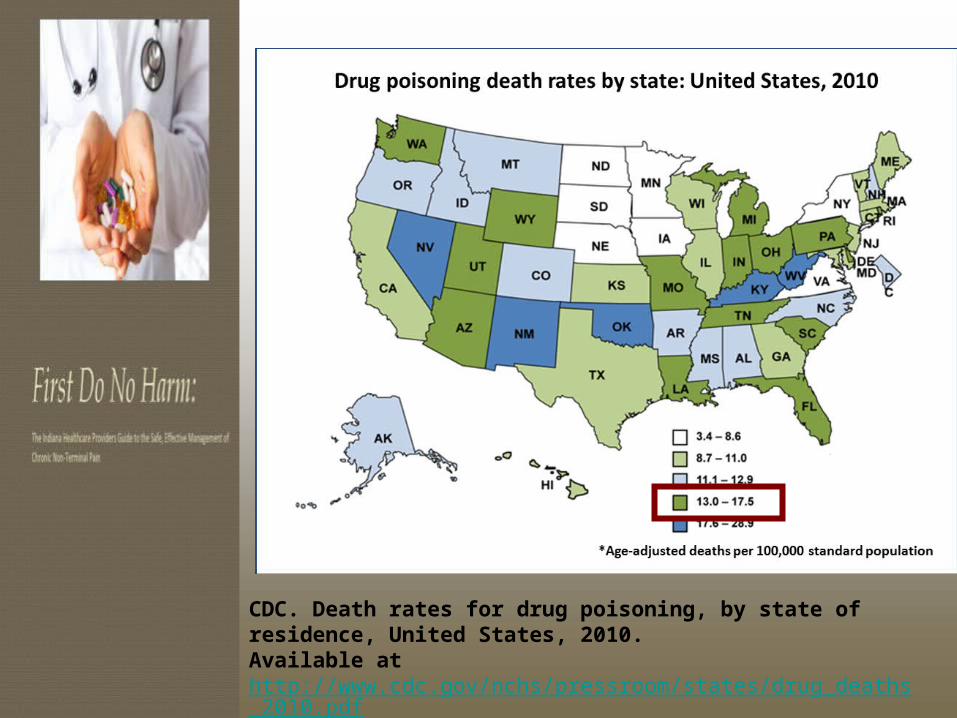
CDC. Death rates for drug poisoning, by state of residence, United States, 2010. Available at http://www.cdc.gov/nchs/pressroom/states/drug_deaths_2010.pdf

7
Drug Overdose Death Rates Versus Motor Vehicle Accidents
NCHS Data Brief, December, 2011, updated with 2009 and 2010 mortality data
Years 1980-2010

Percent Change in Ten Leading Causes of Injury Death* Indiana,
2000–2010
*Age-adjusted rates Source: WISQARS

Unintentional Poisoning Death Rates, Age-Specific, Indiana,
2005 – 2010
Source: Centers for Disease Control and Prevention, WISQARS Database
* Rates based on 20 or fewer deaths may be unstable. Use with caution.

10
Other Adverse Outcomes
SAMHSA NSDUH, DAWN, TEDS data sets
Coalition Against Insurance Fraud. Prescription for Peril. http://www.insurancefraud.org/downloads/drugDiversion.pdf 2007.
emergency department visits

Date of download: 1/6/2013
Copyright © 2012 American Medical Association. All rights reserved.
Neonatal Abstinence Syndrome and Associated Health Care Expenditures: United
States, 2000-2009
JAMA. 2012;307(18):1934-1940. doi:10.1001/jama.2012.3951
NAS indicates neonatal abstinence syndrome. Error bars indicate 95% CI. P for trend < .001 over the study period. The unweighted sample sizes for rates of NAS and for all other US hospital births are 2920 and 784 191 in 2000; 3761 and 890 582 in 2003; 5200 and 1 000 203 in 2006; and 9674 and 1 113 123 in 2009; respectively.
Figure Legend:
2009 NAS vs. OtherLOS 16.4 d vs. 3.3dCosts $53,400 vs. $9,500

Youth and Controlled Substances

Percentage of College Students Reporting Rx Misuse in the Past
Six Months in Indiana, 2013
Rx Drug Prevalence
Adderall 10.1%
Vicodin 3.6%
Xanax 3.5%
Codeine 2.7%
Ritalin 1.7%Lortab 1.5%
Percocet 0.9%
Oxycontin 1.3%
Morphine 0.4%
Methadone 0.2%
Steroids 0.1%
Key:OpioidStimulantCNS DepressantOther
Source: Indiana College Substance Use Survey, 2013. Indiana Prevention Resource Center.

National Survey on Drug Use and Health 2011.
Narcotic Sources
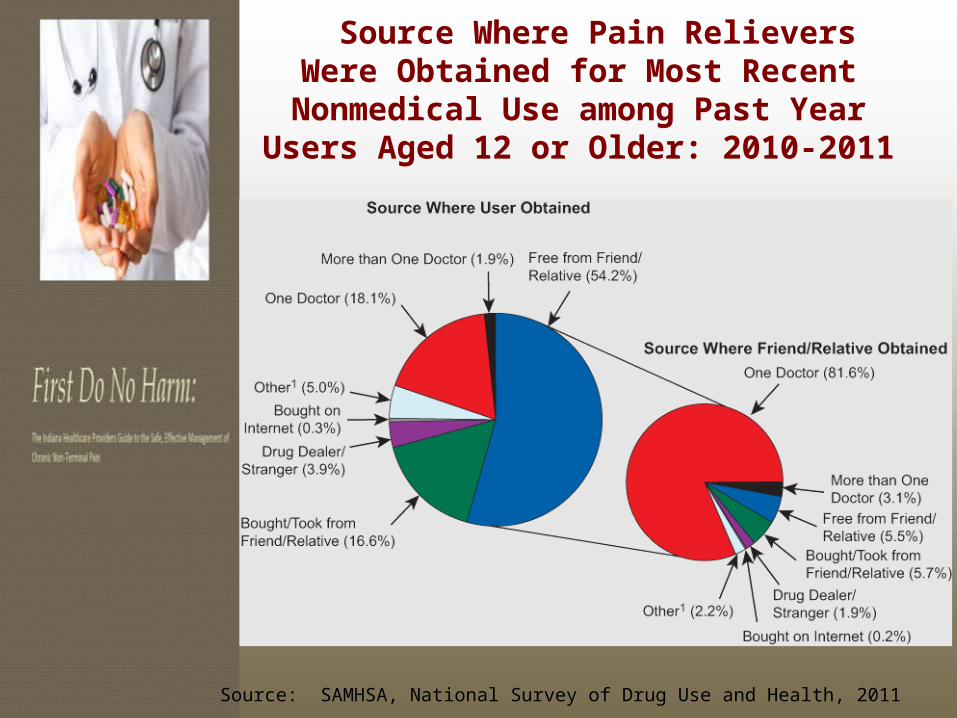
Source Where Pain Relievers Were Obtained for Most Recent Nonmedical
Use among Past Year Users Aged 12 or Older: 2010-2011
Source: SAMHSA, National Survey of Drug Use and Health, 2011

Cost of Opioid Prescriptions in US
• 2006 estimated total cost nonmedical
use of prescription opioids was $53.4 billion
• $42 billion (79%) was attributable to lost productivity
• $8.2 billion (15 %) to criminal justice costs• $2.2 billion (4%) to drug abuse treatment• $944 million to medical complications (2%)
• CDC’s estimate for 2009 is $ 72 billion
Clin J Pain 2011;27:194–202

Primary Care Monitoring of Long-Term Opioid Therapy among Veterans with
Chronic Pain
Pain Medicine 2011;12:740-746

Opioid Prescribing Rules

The NEW Medical Licensing Rules
The MLB rules take effect on December 15, 2013 and apply to:
Any patient taking >60 opioid pills per month for ≥ 3 months
Any patient taking a morphine equivalent dose (MED) of >15 mg for ≥ 3 months

The NEW Medical Licensing Rules
Patients that are exempt from monitoring under these rules include those who are:
Terminally ill Involved with palliative care service Managed in a hospice program Registered nursing home resident We encourage safety monitoring
practices for all patients

Physician Shall Do:
Perform detailed history and physical
Review records from previous healthcare providers
Have the patient complete objective pain assessment tool
Assess mental health status

Physician Shall Do:
Tailor a diagnosis and treatment plan with functional goals
When appropriate – use non-opioid options
Counsel women on Neonatal abstinence syndrome

Treatment Agreement The physician and patient shall
review and sign a “Treatment Agreement” which shall include the following:
Goals of treatment Consent to toxicology screening Permission to conduct random pill
counts Information on pain meds
prescribed by other physicians

Physician Shall Do:
Have face to face visits with patient every 4 months
Conduct an initial INSPECT query on patient and then annually thereafter (the initial requirement goes into effect December 2013 but the annual requirement is extended to November 1, 2014).

Physician Shall Do: Perform drug screens annually
(this provision is not required until January 2015)
If the patient’s opioid dose reaches a morphine equiv of 60 milligrams/day, face to face review of the treatment plan is required.
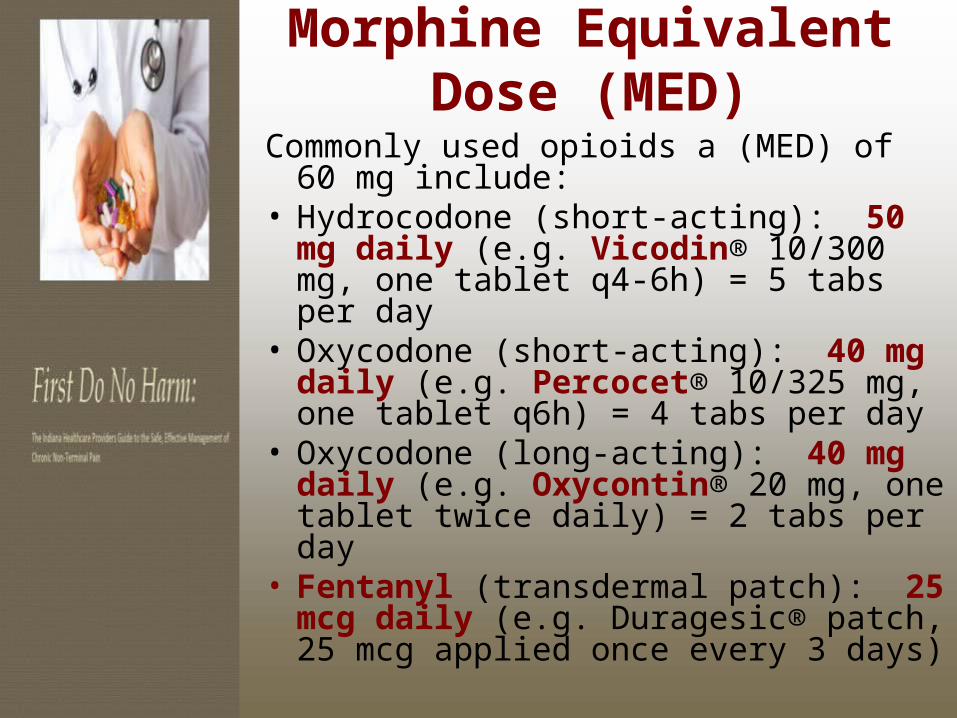
Morphine Equivalent Dose (MED)
Commonly used opioids a (MED) of 60 mg include:
• Hydrocodone (short-acting): 50 mg daily (e.g. Vicodin® 10/300 mg, one tablet q4-6h) = 5 tabs per day
• Oxycodone (short-acting): 40 mg daily (e.g. Percocet® 10/325 mg, one tablet q6h) = 4 tabs per day
• Oxycodone (long-acting): 40 mg daily (e.g. Oxycontin® 20 mg, one tablet twice daily) = 2 tabs per day
• Fentanyl (transdermal patch): 25 mcg daily (e.g. Duragesic® patch, 25 mcg applied once every 3 days)

“First Do No Harm”Indiana’s Safe
Prescribing Recommendations

Healthcare Provider Working Group
Goal was to have geographic, professional and specialty diversity represented.
Formed a “working group” with folks that were already working with this issue in the private sector as well as in academics.
Met a number of times with all day work meetings to discuss issues.
All recommendations have been vetted through this group.

Recommendations1. Do your own evaluation.
• Perform a detailed history/physical exam and obtain appropriate tests, as indicated.
• Obtain and review records from previous caregivers
• Ask your patient to complete a Brief Pain Inventory (BPI) survey to document and better understand their specific pain concerns.
• Establish a working diagnosis and a treatment plan

Evaluation
Ask your patient to
complete a pain
assessment survey
like the:
Brief Pain Inventory

Risk Stratification – 2 Main Areas to Address
Mental Health Assessment Risk for substance abuse The use of chronic opioids
in “high risk” individuals is strongly discouraged

Mental Health Assessment Tools
Chronic pain may be caused,
influenced or modulated by …
Depression (PHQ-2,PHQ-4 PHQ-9)
Post Traumatic Stress Disorder
Anxiety/Panic Disorder (GAD-7)

Substance Abuse Assessment Tools
Ask patients about any past or current
history of substance abuse (alcohol, Rx meds, or illicits) prior to initiating treatment for chronic pain with opioids
ORT – Opioid Risk Tool SOAPP – Screener/Opioid
Assessment for Patients in Pain (starting opioids)
COMM – Common Opioid Misuse Measure (pts already using opioids)
These survey tools will be available at:
www.bitterpill.in.gov

Opioid Risk Tool (ORT)
Webster & Webster. Pain Med. 2005;6:432.
Mark each box that applies: Female Male
1. Family history of substance abuse
Alcohol 1 3
Illegal drugs 2 3
Prescription drugs 4 4
2. Personal history of substance abuse
Alcohol 3 3
Illegal drugs 4 4
Prescription drugs 5 5
3. Age (mark box if between 16-45 years) 1 1
4. History of preadolescent sexual abuse 3 0
5. Psychological disease
ADO, OCD, bipolar, schizophrenia 2 2
Depression 1 1
Scoring totals:

Keep in Mind …
The use of chronic opioids in high risk patients is discouraged unless the underlying issues are appropriately addressed.Specialty consultation may be appropriate.

Recommendations3. Set functional goals with your
patients that include achievable targets for pain management. • It is unrealistic for patients to expect
complete resolution of their chronic pain.
• Work together towards improving pain control and achieving specific functional goals, as both are key outcomes.
• Functional goals might include increasing physical activity level, resuming a job/hobby or improving the quality of sleep.

Functional Goals and Managing Pain
Working together with your patient determine:
Specific Achievable Functional Goals
Assess progress at each visitReframe expectations: A realistic “Pain Score” target isn’t zero!

Recommendations
4. Utilize evidence based treatments, including non-opioid options initially, where possible. Consider non-pharmacologic
therapies, in addition to the various medications available.
Utilize first-line pharmacologic options before prescribing opioids.

Recommendations
4. Utilize evidence based treatments, including non-opioid options initially, where possible. Use the lowest dose of medication
required to reduce pain and improve functioning.
Don’t begin a treatment that you are not prepared to stop.



Evidence Based Treatment
AVOID opioids in patients with: Chronic headache Chronic low back pain Chronic pelvic pain Fibromyalgia Functional bowel disorders (IBS)
Use non-opioid pharmacologic agents and other treatment modalities for pain
management in these situations.

Prescribing Opioids Start with the lowest dose
possible. After reasonable titration, consider
discontinuing opioids if pain does not improve and or functional goals are not met.
Don’t begin a treatment that you are not prepared to stop!
Always have an EXIT strategy!

Recommendations5. Discuss the potential risks and
benefits of opioid treatment for chronic pain, as well as expectations related to prescription requests and proper medication use. Together, review and sign a “Treatment
Agreement”, which includes the details of this discussion for all patients that are prescribed controlled substances (opioids, benzodiazepines, stimulants) on an ongoing basis.
Refer to the sample “Opioid Consent Form and Treatment Agreement” included in the Tool Box.

Prescribing Opiates: Informed Consent
Discuss the risks and benefits of opioid treatment (including common adverse effects).
Counsel women of child-bearing age about the potential for fetal opioid dependence and neonatal abstinence syndrome (NAS).

Review and Sign a Treatment Agreement
Consider including the following information in your treatment agreement:Long term benefit of treatment with opioids has not been establishedOne prescriber, one pharmacyNo sharing or selling medsKeep medications safe; lost or stolen Rx will not be replacedRenewals are contingent on scheduled appointments

Review and Sign a Treatment Agreement
Consider including the following information in your treatment agreement:There is potential for addiction, and abstinence syndrome if the medication is stopped abruptlyPrescription Drug Monitoring (INSPECT) will be reviewed regularlyParticipation in Urine Drug Monitoring, as directed

Review and Sign a Treatment Agreement
Consider including the following information in your treatment agreement:Failure to follow policies or lack of functional benefit with the treatment will result in discontinuation of the opioid trial (taper)No phone refills

Recommendations6. Avoid prescribing for patients
without periodic scheduled visits. It’s the Law. Evaluate patient progress and
compliance with their treatment plan regularly and set clear expectations along the way (e.g. attending PT, counseling or other treatment options).
Follow-up visits should occur at least once every 3-4 months.
More frequent visits would be appropriate.

Recommendations
7. Remember the 5 A’s when managing your chronic pain patients with opioids:
Activities of Daily Living Analgesia Affect (screen for mental
illness & substance use) Adverse effects Aberrant drug use behaviors

Recommendations8. INSPECT: Indiana’s
prescription drug monitoring program, helps us all. Use INSPECT regularly for both new and
established patients. It tracks all controlled substance prescriptions filled by patients state-wide and some neighboring states.
You can register with the state at www.in.gov/inspect
INSPECT reports should be run at least once every 3-6 months; or more often as desired or appropriate.

INSPECT: Indiana Scheduled Prescription Electronic Collection & Tracking
COLLECTSControlled substances dispensed to Indiana residents from: Retail pharmacies Hospital Outpatient pharmacies Mail Order pharmacies Non-resident pharmacies Physician dispensing out of office that is more than a 72-hour
supply
DOES NOT COLLECT Any substance that is not controlled Pseudoephedrine Morphine/Methadone (that is less than 72-hour supply) VA facility dispensing - will be included by 2014 Any substance dispensed that is less than a 72-hour supply Any substance that is administered directly to a patient
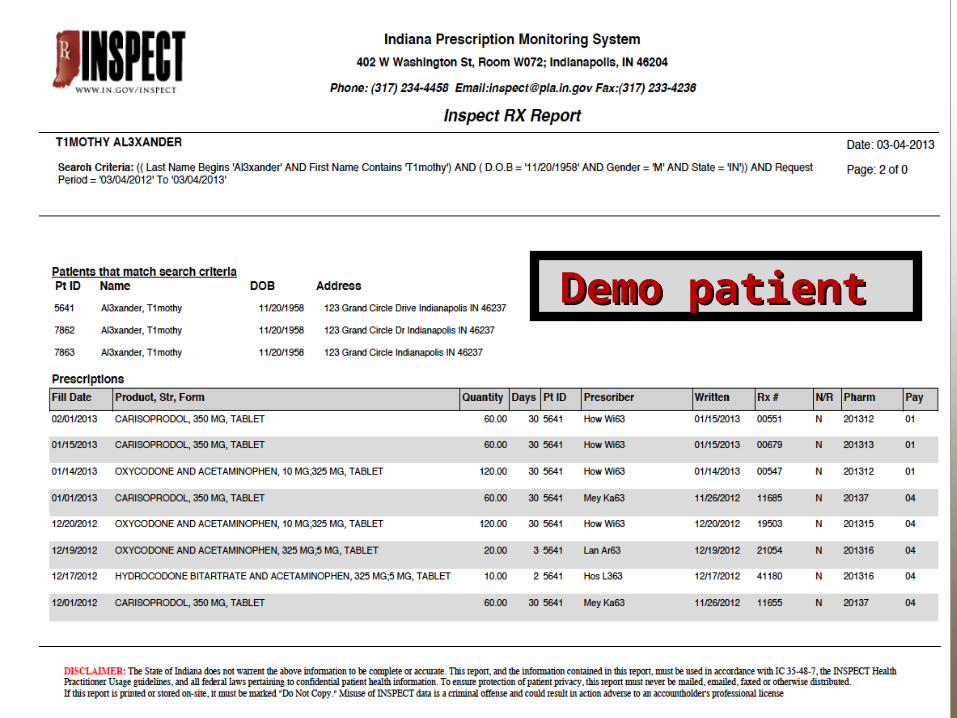
Demo patient Demo patient

Recommendations
9. Urine drug monitoring (UDM) protects you and your patients. UDM is a useful objective tool that complements your other risk assessments.Discussion with patients regarding the need for UDM should legitimately be based on their SAFETY

Urine Drug Monitoring (UDM)
UDM has evolved to become a standard of care when prescribing opioids for patients with chronic pain. It will assist in:
Detecting illicit substances
Monitoring patient adherence to prescribed medications

Urine Drug Monitoring
UDM should be performed at the initiation of an opioid trial and at least annually.
Test frequency may vary depending on the level of identified risk or prescriber concern.

Urine Drug Monitoring
Immunoassay (IA)
Quick, inexpensive, point of care
Identifies classes of drugs (e.g. Opioids, THC)
Can have false positives (e.g. NSAIDS + THC)
Can have false negative (e.g. low dose Vicodin®)
Will need confirmatory test if results are not consistent
Gas ChromatographyMass spectrometry
(GCMS) The definitive confirmatory test
Specific for medication and/or the metabolite(s)
More expensive ($60-$500)
Send out to lab (~2d for results)
Actionable intelligence

Urine Drug Monitoring Data in a Practice Setting
Fort Wayne Medical Education Program; Reporting Period: January – December 2012

10. Reassessment is Required when ≥ 60 MED
• Face-to-face review to reassess your patient if pain is poorly controlled or there is lack of functional improvement
• Formulate/document a revised assessment and treatment plan
• Discuss the increased risk for adverse outcomes with higher opioid doses if that is what you plan to do

60
Overdose Risk Based on Dose, Group Health, 1997-2005
Dunn et al, Opioid prescriptions for chronic pain and overdose. Ann Int Med 2010;152:85-92.

Additional Options … Opioid adjustments may include: a
slow wean, modified dose (up/down) or rotation to another formulation
Collaboration with a mental health professional, as needed.
Referral to a pain management specialist for evaluation/treatment.
Referral to an addiction specialist for evaluation when a substance use disorder is suspected.

Co-Morbid Risks with Opioids …
Patient mortality risk is more pronounced for patients that have any of the following active co-morbid issues:Benzodiazepine use Illicit substance use/abuseAlcohol overuse/abuseUntreated mental health issues (e.g. depression, hx of suicide attempt)Chronic respiratory problems
(e.g. Asthma, COPD, OSA, CHF)
Pearls for High-Risk Patients
• ALWAYS refer for Chemical Dependency Evaluation &
Treatment
• Non-judgmental ∙ Empathetic care
• Do not abandon your patient

Putting it All Together

Challenges to Adoption of Opiate Guidelines
Lack of Time Lack of knowledge Patient expectations Decreased patient satisfaction Strained physician-patient
relationship Beliefs that opioids are safe Physician belief that this change is
not necessary

Healthcare Provider Toolbox:
www.bitterpill.in.gov
A comprehensive “Clinical Resource” to assist
you in managing your patients with chronic pain
A starting point for you and your staff

Toolkit - Format
Not a dissertation; “designed for the busy doc”
Designed to be easy to read Provides links to resources/tools Provides templates for various
surveys & forms Links to websites with more in-depth
information for you and your patients Talking points for difficult
conversations

A number of topics to choose from to
assist you in coming into
compliance with recommendations
and rules

Key StatTo engage
OverviewHas a bit more depth than the recommendations and includes links to forms, additional info, etc
Specific RecommendationsJust the facts ma’am
Includes “Talking Points”
• Conversation starters with patients
• In the margins will be testimonials and other useful info
Includes resources for implementation:
Screening tools
Templates
FAQs
Drug Information
Primer on Urine Drug Monitoring
Resources

Develop Policy & Optimize Workflow
Educate office staff Protocol for new patients Protocol for existing patients Refill policy Lost scripts Missed visits Drug Monitoring Ceiling for opioids? Benzo policy
Educate patients
Letter Policy Framed around safety to
them, their family and their community
Changing the Paradigm Need to begin educating public about
the new rules and recommendations for physicians and the impact on healthcare delivery.
Focus is on functionality as well as pain control.
Resetting expectations of the public – they will need to be more actively engaged in their treatment.
Op ed pieces throughout the next year Posters for exam rooms and other
public areas


Summary

Summary Preserve patient safety first and
foremost. Screen for mental health problems
and substance abuse, using available survey tools to supplement your history.
Set Functional Goals and expect your patient to play an active role in their treatment plan. Not just pills!
Monitor compliance using objective tools; INSPECT and UDM are valuable resources. Please use them!