respiratory tubes
TRANSCRIPT

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 1/26
1
CENTRAL PHILIPPINE UNIVERSITY NURSING REVIEW CENTERIn Collaboration with
A1 PASSERS TRAINING, RESEARCH, REVIEW AND DEVELOPMENT COMPANY
ATTY.SALEX E.ALIBOGHA, RN, MAN, LLB (BAR)
MAINTAINING THE FUNCTION OF TUBES AND DRAINSA. TRACHEOSTOMY TUBE
1. Overviewa. Tracheotomy is a surgical procedure that creates an opening in trachea to establish a patent
airway.b. A tracheostomy is an opening (stoma) that is surgically createdc. A variety of tubes can be inserted into a tracheostomy , depending on whether it is temporary or
permanent, on length of anticipated use, on whether mechanical ventilation will be used , andon need to be able to speak while in place (see figure 28-1)
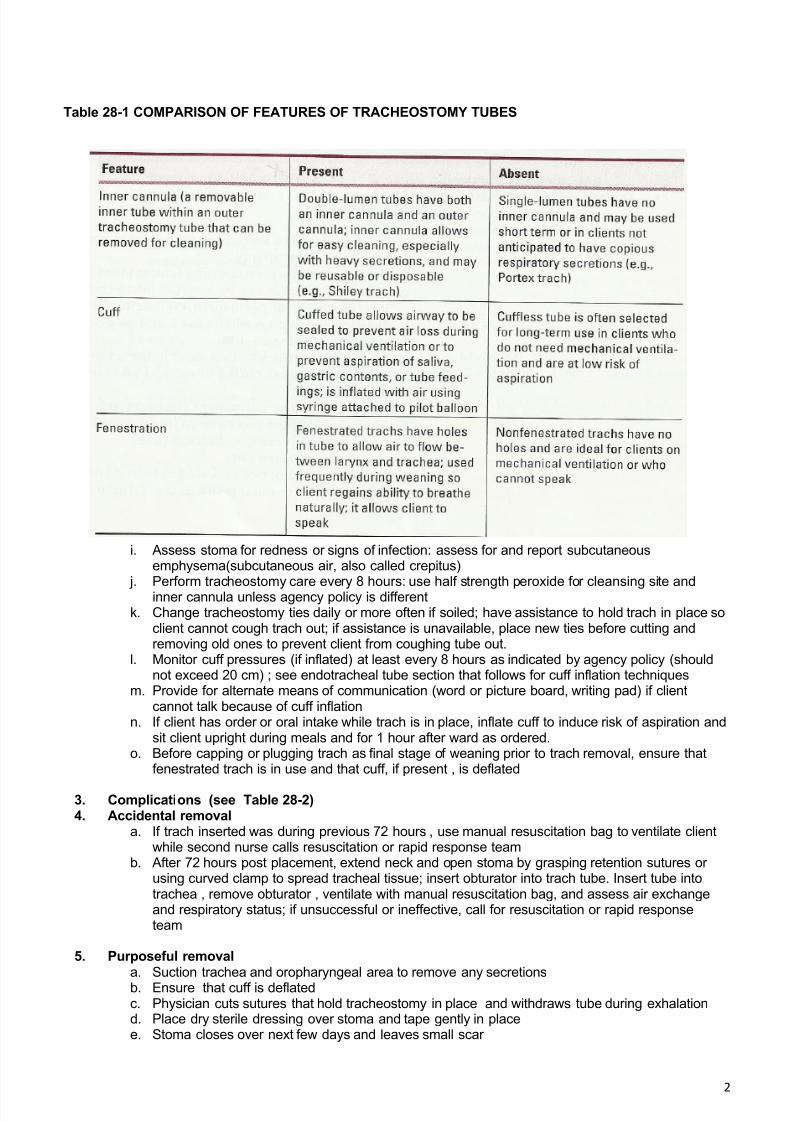
d. Variations in tubes include double lumen or single lumen (inner cannula or no inner cannula),cuffed or cuffles, and fenestrated or nonfenestrated (see table 28-1)
e. Clients who have permanent tracheostomies often use metal trach tubes, which are cuffles andhave an inner cannula; can be used long term with regular cleaning (example : Jackson tube)
2. Therapeutic management
a. Maintain head of bed elevated at least 30 degreesb. Ensure that a manual resuscitation (Ambu) bag is at bedside at all times
FIGURE 28-1
c. Keep spare tracheostomy set of same size, Obturator , and clamps at bedside for use if trach isaccidentally removed
d. Ensure that air and oxygen flowing into airway is humidified: notify respiratory therapy if waterbottle attached to oxygen flowmeter runs low
e. Encourage coughing and deep breathing to reduce risk of atelectasis and pneumonia
f. Perform respiratory assessments , including breath sounds, at regular intervals minimally every4 hours
g. Monitor and document trend of oxygen saturation and/or arterial blood gas results
h. Suction client as indicated by results of assessment (cough , noisy respirations or adventitiousbreath sounds are indicators of need to suction): hyperoxygenate client before and after, suctionfor no more than 10 seconds at one time; assess nature of secretions (purulent secretionsindicate infection)
8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 2/26
2
Table 28-1 COMPARISON OF FEATURES OF TRACHEOSTOMY TUBES
i. Assess stoma for redness or signs of infection: assess for and report subcutaneous
emphysema(subcutaneous air, also called crepitus) j. Perform tracheostomy care every 8 hours: use half strength peroxide for cleansing site and
inner cannula unless agency policy is differentk. Change tracheostomy ties daily or more often if soiled; have assistance to hold trach in place so
client cannot cough trach out; if assistance is unavailable, place new ties before cutting andremoving old ones to prevent client from coughing tube out.
l. Monitor cuff pressures (if inflated) at least every 8 hours as indicated by agency policy (shouldnot exceed 20 cm) ; see endotracheal tube section that follows for cuff inflation techniques
m. Provide for alternate means of communication (word or picture board, writing pad) if clientcannot talk because of cuff inflation
n. If client has order or oral intake while trach is in place, inflate cuff to induce risk of aspiration andsit client upright during meals and for 1 hour after ward as ordered.
o. Before capping or plugging trach as final stage of weaning prior to trach removal, ensure thatfenestrated trach is in use and that cuff, if present , is deflated
3. Complications (see Table 28-2)4. Accidental removal
a. If trach inserted was during previous 72 hours , use manual resuscitation bag to ventilate clientwhile second nurse calls resuscitation or rapid response team
b. After 72 hours post placement, extend neck and open stoma by grasping retention sutures orusing curved clamp to spread tracheal tissue; insert obturator into trach tube. Insert tube intotrachea , remove obturator , ventilate with manual resuscitation bag, and assess air exchangeand respiratory status; if unsuccessful or ineffective, call for resuscitation or rapid responseteam
5. Purposeful removala. Suction trachea and oropharyngeal area to remove any secretionsb. Ensure that cuff is deflatedc. Physician cuts sutures that hold tracheostomy in place and withdraws tube during exhalationd. Place dry sterile dressing over stoma and tape gently in placee. Stoma closes over next few days and leaves small scar

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 3/26
3
B. Endotracheal tube (see figure 28-2)1. Overview
a. An artificial that maintains airway patency and allows for client to receive mechanical ventilation ;intended for short term use, up to 10 to 14 days
b. Consists of a long tube with a universal adapter and proximal end for attachment to oxygen sourceor ventilator , inflatable cuff at distal end, and pilot balloon at proximal end for cuff inflation
2. Routes of insertiona. Orotracheal insertion route allows for use of larger tube, rapidly restores airway,, and reduces
respiratory effort; disadvantages include discomfort to client, possible displacement through tonguemovement and occlusion from biting on tube; oral airway may need to be used
b. Nasotracheal route allow for use of smaller tube, prevents dislodgement with bleeding disorders,epitaxis, or nasal obstruction
3. Therapeutic managementa. To check placement after insertion, ventilate with manual resuscitation bag, assess that both left and
right sides of chest rise and fall, and auscultate for bilateral breath sounds; if only right sided chestmovement and breath sounds are present , tube needs to be pulled back slightly from placement inright mainstem bronchus
b. Auscultate over epigastric area to ensure esophageal intubation did not occur, if it did, ventilationsounds will be louder over stomach than chest and
TABLE 28-2 COMPLICATIONS OF TRACHEOSTOMY
COMPLICATION PREVENTION AND THERAPEUTIC MANAGEMENT
Short termTube Displacement
Secure tube properlyKeep spare tube of same size at bedsideDo not allow client to pull at tubePrevent traction on tube during care and avoid excessive tube movement
Tube obstruction Humidify oxygenSuction as needed and note if secretions are becoming thick and viscousEncourage client to cough and deep breatheKeep inner cannula clean by doing trach care regularly as scheduled
Assess client for respiratory difficulty and/ or newly increased peakpressure on mechanical ventilatorPrepare for rapid tube replacement in the event of obstruction caused bycuff prolapsed over distal end of tube
Long termTracheomalacia(tracheal dilation anderosion caused by highcuff pressures)
Note whether trach tube has low pressure cuff for preventionMonitor air volumes needed to keep cuff inflated and cuff pressures as perpolicy, identify and report increases
Assess for air leaks around cuff or lost tidal volume if mechanicalventilation is being used
Assess for aspiration of bits of food or fluids if client is allowed oral intakeMonitor for a report onset of bleeding caused by pressureProgress client to use of uncuffed tube at earliest opportunity
Tracheoesophagealfistula (abnormalconnection betweenposterior wall of tracheaand esophagus fromhigh cuff pressure)
Similar to tracheomalacia above. Assess for coughing or respiratory distress while taking food or fluids Administer supplemental oxygen by mask to treat hypoxemiaPrepare client for possible insertion of gastric or jejunostomy tube forfeedings if pressure of nasogastric tube in esophagus was contributingfactor
Tracheal stenosis(tracheal lumennarrowing from scarformation secondary tocuff irritation)
Prevent by avoiding high cuff pressures and avoiding traction or pulling ontubeObserve for respiratory difficulty, increased coughing, inability to managesecretions, or difficulty in speaking after cuff deflation or trach tube removalPrepare client for surgical dilation of trachea for definitive treatment asneeded
Tracheal- innominateartery fistula (erosion oflateral wall of tracheainto artery caused bypressure from distal endof tube)
Prevent by keeping tube in midline position and avoiding on tube from anycause
Assess for pulsation of trach tube with each client heartbeat and notifyphysician immediately if it occursNote fresh bleeding at or through stoma and report immediatelyPhysician may remove trach tube immediately and apply direct pressure toblood vessel at stoma sitePrepare client for immediate life saving surgical repair

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 4/26
4
Abdomen wil l rise and fal l with venti lat ions; tube is remo ved immediately if i t occurs
c. A carbon dioxide (CO2) analyzer is frequently use to check proper placement in the tracheausing advanced cardiac life support (ACLS) protocols
d. Confirm placement by portable chest x-ray; distal tip of tube should be 1 to 2 cm above carina(point of bifurcation of right and left mainstem bronchi)
e. Note position of tube by noting centimetre marking at lip line and then tape tube in place or useother securing device; monitor placement at least every 8 hours
f. Ensure manual resuscitation bag is kept at bedside at all timesg. Perform respiratory assessments every 4 hours and as needed; suction client as indicated by
results of assessment as with tracheostomyh. Inflate cuff using minimal occluding volume technique by injecting air into pilot ballom just until
no air leakage sounds can be heard during inspiration with stethoscope placed over trachea
i. Inflate cuff using minimal leak technique by injecting air into pilot balloon until sealed and thendeflating slightly so that no harsh sounds can be heard at peak of inspiration
j. Insert oral airway if orotracheal route is used to prevent client from biting tube or displacingtube with tongue movement
k. Reposition orotracheal tube from one side of mouth to other daily with assistance of one otherperson; assess oral cavity for ulceration or necrosis
l. Provide oral care every 2 hours to prevent drying and cracking of lips and mucous membranesm. Provide the alternative means of communication (word or picture board, writing pad)
4. Removala. Suction endotracheal tube well , then suction oropharyngeal areab. Elevate head of bed to semi –Fowler’s or high-Fowler’s position as toleratedc. Cuff is deflated and client is asked to inhale; at peak inspiration. Tube is removed
d. Encourage client to cough and deep breathe to clear any residual secretions in pharyngeal areae. Apply oxygen as orderedf. Monitor client closely for first 30 minutes after extubation and continue to monitor frequently
thereafter; notify physician if respiratory rate or effort show steady increase , oxygen saturationdecreases, or respiratory distress occurs
g. Teach client that sore throat and hoarse voice are common; monitor status and reporthoarseness that doesn’t improve over time, which may indicate damage to vocal cords
II. CLOSED CHEST DRAINAGE SYSTEMS
A. Overview1. A chest tube is use to drain air (pneumothorax), blood (hemathorax), or large amounts of fluid
(pleural effusion) from pleural cavity2. Restores negative pressure to intrapleural space
B. Design1. Most systems in use today have 3 chambers: collection, water seal, and suction (figure 28-3)2. Collection chamber lies under point attachment between tube and system and consists of marked
columns (generally three) that indicate amount of drainage collected3. Water seal chamber is filled to 2-cm marking during system setup; water allows air to escape
system but not to reenter; water moves up and down in tube in this chamber with inhalation andexhalation to indicate patency

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 5/26
5
4. Suction control chamber allows use of suction to provide negative pressure to chest; negativepressure aids in reinflating lung more quickly by removing air, blood, pus, or effusion; somesystems use “dry “suction, controlled by adjusting suction knob appropriate level, both types areconnected to low wall suction with a connecting tube.
C. Therapeutic management
1. Maintain occlusive dressing at chest tube insertion site; dressing is secured with large strips ofwide tape or Elastoplast; dressing may be reinforced as needed but not changed.
2. Secure all chest tube and suction tubing connections with tape3. Keep collection apparatus below chest level to allow gravity to promote chest drainage; keep
tubing straight to prevent dependent loops of obstructions4. Milk chest tube to maintain patency only if ordered ; milking chest tube can cause tissue drainage5. Chest tube is not to be clamped when client is mobile and is never clamped without a physician
order; keep a clamp at bedside for use or surgeon if needed and as noted by agency policy andprocedure
6. Monitor chest tube drainage at 1 to 4 hour intervals; report and document bright red blood,sudden increase in drainage, or consistent drainage greater than 100mL/hour (physician mayalso specify volume to report)
7. Maintain 2-cm water level in water seal chamber; low water volume creates higher suction thanmay be desired, contributing to pleural tissue damage
8. Assess for fluctuation in water seal chamber , which indicates tube is patent; lack of fluctuation
may indicate tube obstruction, loop or kink (requires correction) or may indicate full lungreexpansion (indicating tube is ready for removal);
9. Assess for bubbling in water seal chambera. Continuous bubbling indicates an air leak in systems and needs to be corrected; if leak
is not found, notify surgeon of problemb. Intermittent bubbling with inspiration indicates drainage of air (pneumothorax) from
pleural space and proper function of chest tube; continue with usual monitoring10. Assess suction control chamber for correct amount of suction by either dial (dry suction system) or
water level (fluid system) ; add sterile water if level is low (excessive will suction can causemore rapid evaporation); remove excessive water by aspiring from rubber seal in chamber
11. Suction control chamber in system that uses water should have gentle. Continuous bubbling assign of proper function ; vigorous bubbling will evaporate water but not increase suction, and
lack of continuous bubbling will not harm client but will not provide suction that assist in clearingpneumothorax or hemathorax
12. Assess respiratory status breath sounds oxygen saturation, and comfort level of 4 hours or asindicated; assess that dressing in intact and check for an report subcutaneous emphysema
13. Change client position every 4 hours and encourage coughing and deep breathing14. Anticipate that client may have frequent (up to daily) portable chest x-rays to monitor lung
reexpansion15. Keep occlusive dressing materials and sterile water at bedside for emergency use (petrolatum
gauze, dry sterile gauze, wide adhesive tape).
8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 6/26
6
16. If drainage system becomes damaged or broken, insert chest tube into sterile water to re-establishunderwater seal and replace with new system
17. If chest tube is accidentally pulled out of chest, pinch skin together, apply occlusive dressing usingmaterials noted above, and notify surgeon immediately
18. Chest tube removala. Indicated when fluctuation stops in water seal chamber, chest x-ray shows full lung
expansion, and client has returned to normal or baseline respiratory statusb. Obtain suture removal set, petrolatum gauze, dry sterile gauze or Telfa gauze, and wide
adhesive tape, premedicate client with oral medication 30 minutes prior to removal ifimpossible
c. Instruct client to take deep breath, hold breath (valsalva) or exhale according to surgeonpreference just prior to tube removal
d. Open and prepare dressing materials just prior to removal of tube by physician; assistwith application of dressing, and obtained follow up chest, x-ray if ordered
e. Assess respiratory status post removal
D. Heimlich valve1. Used instead of chest tube for selected ambulatory clients who have pneumothorax or to treat
tension pneumothorax2. Valve allows air to escape from chest cavity during exhalation but closes during inhalation to
prevent air from reentering pleural cavity
III. RENAL AND URINARY TUBESA. Nephrostomy or ureteral tube
1. Position tube carefully (no kinks or compression) to maintain patency ; do not clamp tube2. Monitor and record urine output carefully; report output of less than 30 mL/hr or no drainage for 15
minutes or more3. Never irrigate tube unless there is a specific order allowing it4. Irrigate with a maximum of 5ml volume and use strict surgical aseptic technique5. Report and document immediately if irrigation fails to restore patency of tube
B. Indwelling urinary catheter1. Insert using sterile technique; measure and record initial outflow amount and characteristics of
urine2. Properly position drainage bag below level of bladder and secure catheter to thigh to prevent
traction of tube balloon against urethra and bladder neck3. Measure and record outputs accurately4. Provide routine catheter care using soap and warm water; follow standards precaution5. Wash front to back for females ; in males retract forekin if present, and return to original position
after cleansing6. Explain procedure to client just prior to removal; empty and record drainage, deflate balloon, and
withdraw catheter while client exhales to reduce discomfort
IV. NASOGASTRIC TUBED
A. OVERVIEW1. Inserted via naris to stomach for decompression of stomach and occasionally for enteral feeding 2. Commonly used tube in Salem sump, double lumen tube with air vent that allows for continuous
(rather than intermittent) suction for gastric decompression 3. Much less commonly used tube is Levin tube, single lumen tube that requires use of intermittent
suction (lack air vent causes tube collapse if continuous suction is used)B. Insertion procedure
1. Sit client upright (High Fowler’s position) 2. Place distal end of tube at tip of nose and measure to earlobe and then to xiploid process to
determine distance for tube insertion; apply tape to tube to indicate point at which to top insertion
3. Lubricate distal 2 to 3 inches tubewith lidocaine gel or water- soluble gel according to policy (notpretrolatum / oil-based lubricant, which could cause pneumonia if tube enters trachea)
4. Ask client to tilt head downward to close epiglottis and allow tube to enter esophagus 5. Insert tube into naris and advance upward and backward until resistance is met at back of nose;
rotate catheter gently and advance into nasopharynx 6. Ask client to take sips of water if able while tube advance into nasopharynx 7. Stop tube insertion and pull back on tube if client coughs or chokes during procedure; when client
respiratory status returns to normal, continue insertion 8. Stop advancing tube one tape reaches naris; check placement as outlined below

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 7/26
7
9. Tape tube in place 10. Place tube to low continuous (Salem sump)or intermittent (Levin) suction for gastric
decompression 11. Do not begin enteral feedings by nasogastric tube unless placement confirmed by chest x-ray
C. Therapeutic management
1. Assess placementa. Chest x-ray is most reliable method of assessing tube placement b. Aspirate gastric contents using piston syringe and apply to strip of ph test paper (color
indicating ph of 4 or less is consistent with gastric placement and ph of 6 or greaterindicates intestinal placement); note that enteral feedings could alter ph and make thismethod less reliable
c. Insert 5 to 10 ml air into tube while listening over epigastric area with stethoscope for“whooshing” or popping sound as air enters stomach; this method is less reliable than x-ray or gastric ph measurement
2. Assess residual prior to and regularly during enteral feedings3. Irrigate tube with 30 to 50 ml water or saline as ordered to check tube patency instill fluid using
piston syringe and aspirate contents back ; repeat if tube is difficult to irrigate or sluggish;
document fluid instilled and aspirated back on intake and output record 4. Assess naris for ulceration from pressure when changing tape daily ; provide nose care by
removing any crusted areas with moist swabs 5. Provide mouth care every 2 hours ; presence of tube in nose leads to mouth breathing and
dryness 6. Tube removal
a. Check order and apply gloves b. Remove tape securing tube to nose c. Ask client to hold breath d. Withdraw tube smoothly over 3-6 seconds while coiling tube around hand for control e. Provide comfort care and document procedure
VI. COMBINED ESOPHAGEAL AND GASTRIC TUBES A. OVERVIEW
1. Exert pressure against or provide tamponade to bleeding esophageal varices2. Contraindicated if client has history of esophageal surgery or has ulceration or necrosis of
esophageal area 3. Airway management is an ongoing priority concern 4. Sengstaken-Blakemore tube- has three lumens; one gastric lumen provides low intermittent gastric
suction while round gastric balloon apply pressure against bleeding blood vessels a. Gastric balloon, if inflated first, and then esophageal balloon is inflated (25 to 45mmHg
pressure) if gastric balloon is insufficient to stop bleeding b. Traction is needed to maintain position of inflated balloons c. Check placement of tube by x-ray of chest and upper abdomen
d. Prepare to insert nasogastric tube in apposite naris to suction secretions thataccumulate above esophageal balloon in esophagopharyngeal area to preventaspiration
5. Minnesota tube is similar to Sengstaken Blakemore tube but has additional (fourth) lumen to drainsecretions from esophagopharyngeal area, eliminating need for separate tube placement in thisarea
B. Therapeutic management1. Position client upright for insertion 2. Check all balloons clamp lumens to avoid air leaks 3. Double clamp lumens to avoid air leaks 4. Keep head or bed raised after insertions 5. Obtain x-ray to verify placement
6. Release esophageal balloon pressure intermittently per agency policy to prevent isophageal injuryfrom ulceration or necrosis
7. Keep scissors at bedside to cut tube to rapidly deflate balloons if respiratory distress occurs 8. Monitor for complications
a. Continued bleeding: steady or increased body drainage from gastric suction port b. Esophageal rupture: upper abdominal and back pain , hypotension, tachycardia; report
immediately : this is medical emergency

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 8/26

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 9/26
9
3. Leads to decreased oxygen consumption, muscle tension, metabolism , and vital signs (heart rate,respiratory rate, and blood pressure)
4. Should be done for minimum of 10 minutes5. Assists client to assume correct posture, such as sitting with feet flat on floor (body parts
supported, joints slightly flexed, and arms and legs uncrossed)
Position clients properly before engaging in progressive relaxation. The body must be fully supported to prevent risk of fall or other injury.
6. Tense and release muscles is specific sequence (more than one sequence available)a. Right first, left first, then both firstsb. Both firsts and both armsc. Toes, then ankles, then kneesd. Buttocks and groine. Stomach and lower backf. Chest and upper back, then shouldersg. Forehead , then jaw
C. IMAGERY
1. Uses power of imagination to assist with physical, psychological and spiritual healing2. Often involves visualization but can also utilize other senses to create desired image3. When imagery is assisted, it is called guided imagery4. Consists of creating one or more of several types of images
a. Healing a specific body part or increasing energy in bodily area (body mind)b. Destroying microorganisms or increasing local circulation (correct biologic)c. Being is a healed state (end state)d. Experiencing sense of unity, light , power, or spirituality (generalized healing)e. Connecting with higher levels consciousness (transpersonal)
D. MEDITATION1. Produces combined state of deep peace and rest along with mental alertness
2. May or may not be associated with religious practice or prayer3. Includes relaxation and focused attention; may focus on object (concentrative meditation) or remain open
to all stimuli (mindfulness meditation)4. General guidelines
a. Choose specific time (early morning or evening, at least 2 hours after meal and comfortable,distraction-free environment)
b. Keep spine straight and body relaxed: may sit cross-legged on floor or be upright in straightbacked chair
c. Close eyes and place palms on thighsd. Use deep breathing or relaxation exercises; focus on either breathing or selected mental image;
let distracting thoughts drift out of mind without focusing on theme. Perform daily for 10 to 20 minutes at a time
E. MUSIC THERAPY 1. Often used in preoperative holding and cardiac units , birthing and counselling rooms, rehabilitation units,
and for sleep induction2. Use to alter ordinary level of consciousness , change mental focus, or change perception of time3. Type of music chosen (classical, romantic , impressionistic, New Age, and others) depends on client
preferences ad goals of therapy4. Choose music without words to enhance relaxation5. Encourage clients to record preferred musical selections6. Typical use is for approximately 20 minutes7. Encourage client to let body respond to music spontaneously (such as relax muscles, lie down, hum or
clap)
F. HUMOR AND LAUGHER1. Helps client to establish relationships by decreasing social distances and placing people at ease2. Helps to relieve anxiety or tension3. Assists in relieving aggression or anger4. Helps to facilitate learning if carefully planned5. Laugher raises heart and respiratory rates and increases oxygen exchange and muscular tension6. A relaxation phase follows laugher. which reverses these changes7. Humor can stimulate endorphin production, which reduces pain8. Has healing properties because it fosters positive emotion

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 10/26
10
G. CLINICAL AROMATHERAPY1. Consists of controlled use of essential oils to achieve measureable outcomes2. Use to improve mood and reduce stress, edema, acne, bruising and allergies3. Uses essential oil from plants that are inhaled, added to bath water, massaged into body, or applied as
cold or warm compresses; over 300 oils currently in use
4. Oils vary in quality and are unregulated; caution client to use carefully5. Teach a client to use only as directed ; some oils; such as wintergreen and camphor, are toxic if inhaled
a. Before using topical application of oil, test skin for allergies with a small amount of diluted oilb. Dilute essentials oils properly before applying to skinc. Do not use near eyes or internallyd. Store in dark covered bottles and keep away from light and heate. Consult health care provider before using essential oils if pregnant; some are reported to bring
on menstruation while others are reportedly useful in pregnancy and delivery
Essential oils are chemicals. As such, they can be toxic. Use them cautiously after consulting with primaryhealth care provider.
H. NURSE‟S ROLE 1. Asses client use alternative therapies , such as those discussed in this section and other alternative
therapies , such as acupuncture , massage therapy, or hyposis provided by other practitioners2. Communicate openly with client to build trust3. Educate client about how to evaluate data sources , such as internet or infomercials4. Do not provide advice regarding use of alternative therapy regimens; instead, communicate data to
primary care provider, who will collaborate with client
II. PRINCIPLES OF USING HERBS AS DIETARY SUPPLEMENTSA. General use
1. Not intended for acute illness episodes or long term therapy2. Appropriate as adjunct to conventional Western therapies
3. Therapeutic effectiveness is slower than prescription medications; may take as long as severalweeks, depending on the herb
4. Many herbs are available in multiple forms, including teas, extracts, tinctures, and capsules ortablets containing powdered or freeze dried forms of the herb
5. Most herbs are multipurpose, used, for example, as skin wash, gargle, compress, lotion and eyebath
6. They are not intended to replace healthy lifestyle7. Safe use in pregnancy and lactation is either contraindicated or unknown and may dry up breast
milk during lactation ; ginger may be an exception8. Although they may be effective in children, herbs should be avoided in acute, sudden-onset illness9. Many herbs interact with other herbs, food and prescription medications
B. Government regulation
1. The Dietary Supplemental Health and Education Act (DSHEA) of 1994 defines herbs as dietarysupplements
2. Because they are not defined as medicines , herbs cannot be promoted with therapeutic claims butonly with information about how they affect structure and function of human body
3. The Food and Drug Administration (FDA) does not regulate use of the herbs in the United Statesbut approves certain herbs for their action on the body (how they affect structure and function);does not monitor herbs for quality, composition or preparation
4. Formulations vary in their potency and recommended dosage, with frequent lack of consensus ondosing
C. Safety, labelling, and purity1. Container levels must carry a disclaimer stating the FDA does not evaluate the product for treating
, curing or preventing disease
2. Labels should contain specific direction for dosing and use3. Only the standardized extract, when available, should be use4. Not all herbs have empirical support for their safety and efficacy5. Much of the research and standardization originates in Europe, where use of herbs popular,
particularly in Germany6. Many herbs contain toxic substances (e.g. , arnica, belladonna, hemlock, lily of the valley, and
sassafras)7. Health care providers should report all adverse effects of herbs to the FDA

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 11/26
11
D. Nurses „role and client education 1. Obtain a complete history and physical before starting any therapy with herbs 2. Herbs are not effective for or to be used for acute illness or episodes 3. Herbs take longer to work than do prescription medications, usually weeks4. Report use of all herbs to health care provider 5. Explain that client should start with one herb at a time, at lower than recommended doses, and
closely monitor response 6. Teach client to know particular use, dosing and safe administration of each herb and take only as
directed 7. Herbs may cause allergic reactions and adverse effects; if one occurs , discontinue herb and
report symptoms to health care provider 8. Become familiar with all herb-herb, herb-drug, and herb-food interactions 9. Client should purchase herbs from a reputable source and be aware of where and how the herb
was processed, and should purchase standardized form herbs if possible 10. Terms such as natural or all natural do not equate with safety or efficacy of herb 11. Become familiar with various names by which particular herbs are identified 12. Client should avoid use of herbs in pregnancy, lactation, and in children 13. Client should accurately assess advertising claims ; few definitive clinical trials have demonstrated
safety and efficacy of these agents14. Nurses should continue to read new evidence that emerges from research in this field, such as
studies founded by National Center for Complementary and Alternative Medicine 15. Nurses should refrain from recommending or endorsing any particular product or agent
III. SPECIFIC HERBAL SUPPLEMENTSA. Bilberry ( Vaccinium myrtillus, European blueberry, huckleberry, whortleberry)
1. Descriptiona. Relative of blueberry and cranberry; shrub with small, sweet, black berriesb. Active ingredients : anthocyanoside (antioxidant bioflavonoid), pectin (soluble fiber)c. Stabilizes collagen activityd. Prevents production and release of compounds that promote inflammation such as histamine
and prostaglandinse. Relaxes smooth muscle in vasculaturef. Inhibits platelet aggregationg. Reduces permeability and strengthens capillary wall membrane
2. Usesa. Most commonly used for treatment of simple diarrheab. Prevention and treatment of eye disorders: diabetic retinopathy, night blindness, macular
degeneration, glaucoma, cataractsc. Diabetes mellitusd. Antioxidante. Possible treatment of varicose veins, haemorrhoids
3. Precautions
a. May increase coagulation timeb. May interfere with iron absorption when taken internallyc. Use cautiously with acetylsalicylic acid (aspirin), anticoagulants , vitamin E, fish oils,
feverfew, garlic, ginger, ginkgod. Contraindicated in pregnancy and lactatione. Avoid long term large doses: doses over 1.5 grams/kg/day may be fatal, and doses over 480
mg/day may be dangerousB. Black cohosh (Cimicifuga racemosa, black snakeroot, rattleweed, rattleroot, squawroot, cimifuga)
1. Descriptiona. Active ingredients : triperpenoid glycosides, isoflavenones, aglycones b. Binds to estrogen receptors c. Inhibits luteinizing hormone
d. Apparent estrogen-like activity2. Uses
a. Primarily used for treatment of premenstrual syndrome (PMS), and post menopausal symptoms b. Promotes labor of pregnancy c. Decreases blood pressure d. Use to treat snake bites e. Recommended uses by herbalists: dysmenorrhea, rheumatism,antispasmodic, astringent,
diuretic, expectorant, sedative

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 12/26
12
3. Precautions a. Contraindicated use with antihypertensives or hormone replacement therapy b. May cause bradycardia , hypotension, joint pain c. Contraindicated in lactation d. Use in pregnancy only when birth is imminent to promote labor e. Adverse side effects include nausea. dizziness , decreased pulse rate, and increased
perspiration C. Echinacea (Echinacea purpurea , snake root, purple or American cone flower, Sampson root, blackSampson, hedgehog, survey root)
1. Descriptiona. Member of daisy family , with 9 speciesb. Active ingredients: polysaccharides, alkylamides, flavonoids, caffeic acid derivatives
(echinocosides), essential oils and otherc. Available in capsule, tablet, candle, glycerite, hydroalcoholic extract, fresh-pressed juice,
lollipop, lozenge, tea and tincture formsd. Activates T lymphocytes and intensifies phagocytosis of macrophagese. Stimulates tumor necrosis factor, interferon, and interleukinf. Nonspecific stimulation of immune system
g. Stabilizes hyaluronic acid (a component of connective tissue) to protect cells and connectivetissue from microorganism invasion and attack from free radicals
h. Inhibits lipoxygenase to reduce inflammation2. Uses
a. Most common : prevention or reduction of symptoms of cold or influenzaRecall that enchinacea is an ingredient in some sore throat drops. This will aid in remembering that it is
most effective if used early for colds and sore throatsb. Boosts immune system and increases body resistance to infection, particularly upper respiratory
and urinary infectionc. Use to treat herpes simplex and Candida infectiond. Topically : improves wound healing , provide antioxidant protection from ultraviolet A and B light
rays
3. Precautionsa. Not to be used in presence of autoimmune disease (e.g., HIV/AIDS), collagen disease, multiple
sclerosis , tuberculosis) severe illness , or allergy to sunflower or daisy familyb. Not to be used with immunosuppressant (e.g., corticosteroids or cyclosporine)c. Prolonged use (longer than 8 weeks) may cause hepatotoxicity and suppression of immune
systemsd. Not to be used with other hepatotoxicants (e.g. , anabolic steroids , amiodarone, methotrexate,
ketoconazole)e. May influence fertility by spermatozoa enzyme interferencef. Many tinctures contain large amounts of alcoholg. Contraindicated in alcoholism, children, pregnancy, and lactationh. Adverse effects: allergic reaction and anaphylaxis
D. Feverfew (Tanacetum parthenium, bachelor‟s button, febrifuge plant, feather few feather foil)1. Description
a. Short, bushy perennial; member of daisy family; has yellow flowers and yellow-green leavesresembling chamomile
b. Active ingredients; sesquiterpene lactones , especially parthenolide, essential oilsc. Suppresses secretion of granules in platelets and neuthrophils to inhibit platelet aggregationd. May suppress production of prostaglandins (thromboxane, leukotriene)e. Inhibits release of serotonin
2. Usesa. Principle use: prevention of recurrent migraine headaches , treatment of arthritisb. Relief of menstrual painc. Astma
d. Dermatitis , psoriasise. Antipyretic (promotes diaphoresis)
3. Precautionsa. Long term studies not doneb. Contraindicated in pregnancy, lactation, and under age 2c. Cross allergy to ragweedd. Adverse effects; allergic reaction , lip and tongue swelling, mouth ulcers and loss of taste from
chewing leaves, abdominal colic, palpitations increased menstrual flow

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 13/26
13
e. Sudden withdrawal may cause post feverfew syndrome (muscle aches, pain and stiffness):taper off to discontinue
f. Other proven (conventional ) remedies for relief of migraine should be use first; do not use feverfew while taking prescription drugs for headache
g. May interfere with blood clotting mechanism ; not to be used with anticoagulants such asaspirin, warfarin (Coumadin ), bilberry, garlic, ginger, ginkgo
h. Feverfew is known to cause rebound headachesE. Garlic (allium sativum, stinking root or rose, nectar of the goals, camphor of the poor , poor man‟streacle, rustic treacle)
1. Descriptiona. Empirical support for effectiveness and use; most widely researched herbb. Active ingredients (23 constituents ): allicin (odourless, sulphur containing amino acid), ajoenec. Should be crushed or bruised to effectively convert various enzymes, protein, lipids, amino
acids, and other ingredients to allicind. Allicin and ajoene not found in dried garlic but may be present if dried at low temperatures or
taken in enteric coated tabletse. Inhibits platelet aggregationf. Well documented research shows that it reduces and inhibits metabolism of cholesterol
g. Increases bile acid secretion2. Uses
a. Principle uses: reduces cholesterol (decreases triglycerides and low density lipoproteins;increases high-density lipoproteins; increases high density lipoproteins) and lowers mildhypertension
b. Reduces risk o strokec. Antibacterial, antiviral, antifungald. Anticancer propertiese. Lay use: antihelmintic, antispasmodic, diuretic, carminative (relieves flatulence ), digestant ,
expectorant, topical antibiotic
3. Precautions
a. Avoid large amounts of garlic with ASA (aspirin) , anticoagulants such as warfarin (Coumadin) ,and other herbs that affect coagulation( bilberry, fever-few , ginger , ginkgo
b. May potentiate diabetes drugsc. Adverse effect: contact dermatitis, vertigo, garlic breath or scent, hypothyroidism, GI irritation,
nausea and vomiting with large dosesd. Enteric coated tablets containing powdered form may reduce bad breath but are not as potent
as raw garlice. Contraindicated in pregnancy. GI (peptic ulcer and GERD) and bleeding disordersf. Chronic use may lower haemoglobin levelsg. When used to decreased cholesterol levels, plan should be monitored by the health care
providerF. Ginger (Zingiber officinal , Jamaica ginger, Cochin ginger, black ginger, race ginger)
1. Descriptiona. Green purple flower resembling the orchidb. Active ingredient : sesquiterpenes, aromatic ketones (gingerols), and volatile oilsc. Inhibits thromboxane production to enhance effects of anticopagulationd. Inhibits leukotriences and prostaglandins to produce anti inflammatory and analgesic effect
2. Usagea. Principle use:antiemetric; improves appetiteb. Diuretic , digestion aid ; alleviates dyspepsiac. Anti inflammatory in treatment of rheumatoid arthritis and osteoarthritisd. Relieves muscle paine. May reduce motion sickness and relieve vertigo
3. Precautions
a. Adverse effect: headache, anxiety insomnia, elevated blood pressure, tachycardia, asthmaattack, postmenopausal bleeding
b. Contraindicated and postoperative nausea in clients with increased risk of bleedingc. Not to be used concomitantly with bilberry, feverfew, garlic, ginkgo, or other anticoagulants
such as ASA (aspirin) or warfarin (coumadin)d. Severe overdose: possible CNS depression and cardiac arrhythmiase. Excess of 6 grams/day results in gastric irritation and ulcer formationf. Conflicting data related to safe use during pregnancy (relatively safe according to FDA);
contraindicated in treatment of hyperemesis gravidarum

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 14/26
14
G. Ginkgo (Ginkgo biloba, GBE 761, GBE, GBX, Tebonin, Tebofortan, Ginkogink)1. Description
a. Active ingredients: flavones glycosides , flavonoids, terpene lactones (such as ginkgolides andbilobalide)
b. Ginkgo biloba extract referred to as GBE c. Flavonoids act as antioxidants by destroying lipid layer of cell membrane
d. Flavone glycosides produce mild platelet aggregation e. Ginkgolides antagonize platelet activating factor to decrease coagulation f. Bilobalide increases cerebral circulation to improve tissue perfusion and increase memory g. Protects brain from effects of hypoxia
2. Uses a. Cerebrovascular insufficiency and symptomatic relief of organic brain dysfunction to improve
short term memory loss b. Peripheral vascular disease (e.g. , Raunaud’s disease, intermittent claudication), varicosities c. Senile macular degeneration d. Treatment of age related mental decline such as short term memory loss and poor
concentration e. Treatment of depression related cognitive disorders
f. Treatment of depression in older adults , particularly depression related to chroniccerebrovascular deficiency that does not respond to standard drug therapy
g. Tinnitus 3. Precautions
a. Effects may not be apparent for 4-8 weeks b. Not to be used concomitantly with bilberry, feverfew, garlic, ginger, or other anticoagulants ,
such as ASA (aspirin) or warfarin (coumadin) c. Avoid use of unprocessed ginkgo leaves that contain allergens related to urushiol, the chemical
responsible for the itch in poison ivy d. Crude, dried leaf or tea may not contain sufficient active ingredient to be effective e. Large doses may cause restlessness, headaches, nausea, vomiting, diarrhea, dizziness , or
palpitations
f. Edible solid form sold in Orientals shops should be kept out of reach of children because seedsmay cause seizures
g. Avoid use in pregnancy, lactation, and children
H. Ginseng , Korean (Panax ginseng, American ginseng, Panaschinseng)1. Description
a. Active ingredients : titerpenoid saponin glycosides (ginsenosides panaxosides) b. Possible effect on pituitary gland with action similar to corticosteroidsc. Improves serum glucose , glycosylated haemoglobin (HbA1c) and aminoterminalpropeptide
concentrations d. Hypertensive effect with low doses, hypotensive effect with higher doses
2. Uses
a. Most common: counteracts effects of physical and mental fatigue and improves stamina andconcentration in healthy individuals
b. Used to treat chronic hepatotoxicity related to alcohol and drug ingestion c. Improves body ability to resists stress and disease; increases vitalityd. Regulates blood pressure e. Improves psychomotor performance (attention, auditory reaction time); may reduce mood
swings f. Regulates blood glucose levels in type 2 diabetes g. Aphrodisiac
3. Precautions a. Most side effects reported are related to excessive or inappropriate use b. Avoid concomitant use with stimulants, such as coffee, tea, cola
c. May potentiate MAOI actions d. Adverse effects : insomnia, palpitations , pruritus , nervousness , euphoria
I. Ginseng , Siberian (Eleutherococcus senticosus, five fingers, tartar root, Western Ginseng , sengand sang, Asian ginseng. Jintsam)
1. Descriptiona. Active ingredients : eutherosides b. Pharmacologic actions not well understood c. Elevates lymphocyte count (T cells), boosts immune system

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 15/26
15
2. Usesa. Enhances physical and mental performance under stress b. Improves athletic performance c. Increases oxygen metabolism , work capacity, and exhaustion time in a variety of illness (e.g. ,
atherosclerosis, diabetes, chronic bronchitis ) d. Stimulates WBC production in clients undergoing antineoplastic therapy
3. Precautionsa. Adverse reactions: hypertension, tachycardia, insomnia and irritability b. Contraindicated in pregnancy , lactation, premenopausal women, hypertension, CNS stimulants
, or with antipsychotic medications J. Hawthorn (Crataegus oxyacantha , Mayblossom, Maybush, whitehorn, Ll 132)
1. Descriptiona. Small to medium tree of several species ; leaves , flowers , berries (fruit) are used in
standardized extracts b. Active ingredients : flavonoids , primarily procyanidins and proanthocyanidins c. Acts as antioxidant that decreases damage by free radicals to cardiovascular system by
increasing levels of vitamin C intracellularly d. Increase coronary and myocardial circulation
e. Decreases peripheral vascular resistance to decrease blood pressure f. Increases strength of myocardial contraction (positive inotropic effect) and decreases heart rate
(negative chronotropic effect) g. Angiotensin 1 to angiotensin II, a potent vasoconstrictor
2. Usesa. Treatment of mild hypertension b. Treatment of athero and arteriosclerosis c. Treatment (prevention) of chronic angina: not intended for acute angina d. Treatment of early congestive heart failure
3. Precautions a. Contraindicated with concomitant use of prescription antihypertensives or nitrates b. Supervision of health care provider necessary for those with existing cardiac disease
c. May interfere with digoxin pharmacodynamics and monitoring d. Adverse effects: nausea, fatigue, perspiration and cutaneous eruption of the hands, increased
CNS depression and sedation e. Contraindicated in pregnancy and lactation
K. Milk thistle (Silbyum marianum, Mary thistle, Marian thistle, Lady‟s thistle, Holy thistle silymarin ,the “liver herb”)
1. Descriptiona. Tall plant, prickly leaves, milky sap, member of daisy family b. Active ingredients ; silymarin and its component silybinin to act as hepatoprolectant c. Promotes glutathione production, a powerful endogenous antioxidant
d. Binds to hepatocyte membrane and blocks uptake of toxins into liver cells e. Stimulates nucleolar polymerase. A activity to promote new liver cell growth f. Stimulates regeneration of liver by stimulating protein synthesis g. Inhibits action of leukotriene by Kupffer cells h. Binds to site on liver cell membrane, blocking availability for attack from phalloidine, the toxin in
death cap mushroom i. Stabilizes liver cell membrane by decreasing turnover rate of phospholipids
Note that the words milk and thistle both contain the letters/ and i, which may help you to associate this herbwith the liver
2. Usesa. Reduces hepatotoxicity related to psychoactive drugs such as phenothiazines
b. Adjunct therapy in liver inflammation related to cirrhosis, hepatitis, and fatty infiltrate related toalcohol or other toxins
c. Treatment of overdose of death cap mushroom 3. Precautions
a. Insoluble in water, not to be taken in a tea form b. Avoid alcohol based extract in decompensated cirrhosis c. Cross allergy to ragweed d. Adverse effects: loose stools, diarrhea in high doses e. Contraindicated in pregnancy and lactation

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 16/26
16
f. Close monitoring by health care provider in presence of active liver disease L. Saw palmetto (Serenoa repens, sabal, American dwarf palm free, LSESR)
1. Descriptiona. Shrublike palm tree with reddish brown to black berriesb. Active ingredients: saturated and unsaturated fatty acids and sterols from berries (liposterolic
acid)
c. Reduces action 5-alpha reductase enzyme that converts testosterone to dehydrotestosterone(DHT) in aging (effects similar to finasteride [Proscar]with fever side effects)
d. No effect on prostatic specific antigene. May reverse testicular and mammary gland atrophyf. May increase sperm production and increase sexual vigor
2. Usesa. Demonstrated effects through research: symptomatic treatment of benign prostatic hyperplasia
(BPH)b. Helps initiate urine stream; decreases urinary frequency, residual volumes nocturia, and dysuria;
unclear whether actual prostatic size is reducec. Lay uses: treatment of asthma, bronchitis, and gynecomastia
3. Precautions
a. Long term use with approximately 6 weeks for initial effectsb. Insoluble in water; not to be taken in tea formc. Adverse effects: nausea ; abdominal pain, hypertension, headache , diarrhea with large dosesd. May interfere with iron absorptione. Supervision by health care provider necessary for diagnosed BPHf. Should not be used by pregnant or lactating women
M. St. John‟s wort (Hypericum perforatum, amber, goat weed, touch-and –heal, Johnswort witch‟sherb, Klamath weed, chassediable, devil‟s scourge)
1. Descriptiona. Yellow perennial flower with red pigmented leaves containing small black dots b. Active ingredient: hypericin from red pigmented leaves, pseudohypericin and flavonoids,
tannin and others
c. Inhibits reuptake of serotonin; actions not well determined or understoodd. Low monoamine oxidase inhibitor (MAOI) e. Effects comparable to imipramine (Tofranil) f. Produces fewer side effects than prescription antidepressants
2. Usesa. Treatment of mild to moderate depression b. Not intended for treatment of suicidal ideation, psychotic behavior, or severe depression c. Possible antibacterial , antiviral, wound healing properties
3. Precautions a. Not to be used concurrently with prescription antidepressants , especially selective
serotonin reuptake inhibitors (SSRI) or MAOLS or food containing tyramine (such as agedcheese, smoked meats, liver, figs, dried or cured fish, yeast, beer, Chianti wine).
b. Not to be use concurrently with opioids, amphetamines, or OTC cola and flu preparations c. May inhibit absorption of iron d. Adverse effects (may continue for 4 to 4 weeks): GI distress, emotional vulnerability,
fatigue, pruritus, weight gain, headaches, dizziness, restlessness e. May cause photosensitivity: avoid sun exposure , especially if fair skinned f. May decrease digoxin levels g. Contraindicated in pregnancy, lactation, and children
N. Valerian root ( valerian officinalis, wild valerian, garden heliotrope, setwall, capon‟s tail, all-heal,Amantilla, Baldrian wurzel, benedictal)
1. Description a. Tall perennial with hallow stem, leaves , and white or red flowers
b. Active ingredients : valepotriates and susquiterpine derivatives, valeric acid, valeranone,and other
c. Binds weakly to gammaaminobutyric acid (GABA) receptor sites to decrease CNS activity,causing sedation with decreased side effects
d. Action similar to benzodiazepines but non-addicting and produces no morning hangover 2. Uses
a. Sedative , reduction of anxiety b. Treatment of insomia’

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 17/26

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 18/26
18
5. Side/ adverse effects a. Nausea, vomiting,anorexia, constipation, diarrhea b. Headache, stomatitis, edema, rash, mucositis, generalized pain, bone pain c. Supraventicular dysrhythmias, tachycardia d. Renal or hepatic dysfunction, dyspnea, seizures, porphyria e. Report neutrophil count of 20,000/mm3 to physician
f. Adult respiratory distress syndrome (ARDS), pleural effusiong. Myocardial infarction (MI), gastrointestinal (GI) hemorrhage, thrombus formation
6. Nursing considerations for sargramostim (Leukine) a. Assess CBC and platelet count before administration and 2 times per week
during medication administration b. Assess renal and hepatic function c. Assess for excessive myeloid blasts in bone marrow d. Do not administer during pregnancy; use cautiously during lactatione. Dilute with normal saline and store in the refrigerator; administer only one dose
per vial
Table 46-1 COMMON IMMUNOSTIMULANT MEDICATIONS
Generic / Trade Names ActionsSargramostim (Leukine) Increases the production of granulocytes and macrophages before
and after bone marrow transplantation, so labelled as a GM-CSF
Epoetin alfa (Epogen) Increases the RBC count in clients with chronic renal failure, canceror human immunodeficiency virus; is actually a haematological, notan immunological, colony stimulating factor, but is used in client whohave immunodeficiency
Filgrastim (Neupogen)Pegfilgrastim (Neulasta)
Increase neutrophil (granulocyte ) production in cancer clients toprevent infection, so labelled as a G-CSF
7. Nursing considerations for epoetin alfa (Epogen) a. Assess blood pressure (BP) prior to administration and regularly during therapy;
hypertension may occur if hematocrit level rises rapidly b. Epoethin alfa should be used cautiously during lactation c. The client should eat food rich in iron and possibly take an iron supplement to
increase effectiveness of therapy on RBC formation d. Assess Homan’s sign periodically to detect thrombus development with
increased RBC counts e. Administer cautiously with lactation f. Do not shake solution after it has been reconstituted g. Assess Hct to determine if it has been risen 4 points in 2 weeks; a rapid elevation
of 4 points may lead to hypertension and seizures 8. Nursing considerations for filgrastim (Neupogen)
a. Assess results of CBC, differential , and platelet count before administration and
2 times per week during therapy b. Do not administer 24 hours before or after chemotherapy c. Assess for hypersensitivity to E. Coli products d. Filgrastim is pregnancy category C; use cautiously with lactation e. Administer only one dose per vial, and discard after 24 hours; store medication in
the refrigerator f. Reconstitute in dextrose 5% , and avoid shaking the bottle to prevent damage to
the protein g. Avoid exposure to infection because clients lowered white cell count indicates
increased risk of infection 9. Client education for sargromostim (Leukine)
a. Avoid exposure to infection and be aware of signs and symptoms of infection
b. Report difficulty breathing and fever c. CBC and platelet count must be done periodically d. Address body image with client because of alopecia
10. Client education for epoetin alfa (Epogen) a. Administration of medication at home with home dialysis; action, side effects, and
nursing implications associated with epoetin alfa administration b. Signs and symptoms of clot formation c. Self monitor BP d. Eat and diet high in iron and take iron supplement it ordered

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 19/26

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 20/26

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 21/26

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 22/26

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 23/26
23
G. Biological response modifies (BRMs)
1. Group of substances that can elicit, modify , and restore biological response between an individualand a tumor cell
2. Examples a. Monoclonal antibodies, (produced by a specific group of identical cells) may be used to
treat tumors because of their specific targeting effect b. Colony stimulating factors, (a group of proteins that stimulate growth of either RBCs or
WBCs) prevent or help reduce a clients adverse response to disease; these types ofBRMs are used in a variety of hemotologic and immunologic diseases
IV. COMMON TESTS AND PROCEDURES OF THE IMMUNE SYSTEM
A. Skin Testing1. A small quantity of allergen is introduced into skin by scratching or intradermal (ID) injection 2. A scratch test is used to test many antigens at a single time; it is of lower sensitivity than injection,
but many allergens can be tested at once and result can be obtained in 30 minutes 3. ID injection is more accurate but leads to higher incidence of systemic reactions
4. Patch test evaluates contact allergens by applying allergen directly to skin and covering with adressing
5. Antihistamines that could impair immune response should be discontinued 72 hours prior to skintesting
6. Immediate positive reaction usually occurs within 10 to 30 minutes and consists of wheal formationand erythema formation greater than 3 millimeters of a positive control (histamine)
7. Minor itching at site can be relieved by cool compresses, topical steroids , and topical oralantihistamines
B. Radioallergosorbent test (RAST)1. Reveals elevated levels of IgE associated with atopy (allergic reactions stemming from hereditary
disposition)
2. Allergen is usually planted on a surface such as paper disk 3. Client blood is then applied to surface and incubated 4. Antibodies specific to an allergen bind to allergen, but others wash away, and level of IgE can be
measured 5. More sensitive than skin testing but also more time consuming and expensive
C. Pulmonary functions tests to diagnose asthma
D. Blood assays reveal increased circulating IgE in presence of allergic disease
E. Eosinophilia may be present with allergic disease
V. HYPERSENSITIVITY REACTIONS
A. Hypersensitivity is an abnormal exaggerated immune response to a specific response to a specificresponse
B. The Gell and Coombs Classification of Hypersensitivity Reactions categorizes a reactionaccording to type, class, and immunity
Table 67-2 GELL AND COOMBS CLASSIFICATION
Type Class Immunity
I Immediate hypersensitivity Humoral
II Cytotoxic Humoral II Immune complex related Humoral
IV Cell -mediated
C. Type I: anaphylactoid reactions1. Involves an immediate response; however, potential response can be cumulative; for example,
initial and sensitizing dose may not elicit a strong response, but subsequent contacts, even isnot long term in nature, may cause a stronger response

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 24/26

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 25/26

8/12/2019 Respiratory Tubes
http://slidepdf.com/reader/full/respiratory-tubes 26/26