respiratory muscle assessment
TRANSCRIPT
BY
Riham Hazem RaafatLecturer Of Pulmonary Medicine, Ain Shams
University

OBJECTIVES:
When should respiratory muscle function be assessed?Clinical signs of respiratory muscle weaknessPathological conditions in which respiratory muscle
weakness can be suspectedPrinciples of assessment of respiratory musclesRespiratory muscle enduranceAssessment Of Respiratory Muscle Function In The ICU

INTRODUCTION
Respiratory muscles generate the pressure differences driving ventilation In advanced stages, respiratory muscle weakness leads to respiratory
pump failure. Inspiratory muscle weakness may partially explain dyspnea and exercise
intolerance. In addition, reduced respiratory muscle force has been shown to be an important predictive factor for poor survival in chronic lung diseases
In advanced stages the functional consequence of respiratory muscle weakness may require mechanical ventilation.
Expiratory muscle weakness leads to problems with speech, and mucus retention due to impaired cough efficacy.

Muscles Of Respiration:1. Diaphragm
2. Accessory Muscles:I. Intercostals (Internal and External)II. ScalenesIII. SternomastoidIV. Pectoralis Major
I. Abdominal muscles: II. Rectus AbdominisIII. Transverse AbdominisIV. External And Internal Obliques

Clinical indications for Respiratory Muscles Strength Assessment:
1. Assessment of neuromuscular disorders (e.g : ALS, MG, MS)2. Evaluations of patients with impaired cough and retained
secretions.3. Evaluation of reduced muscle strength (as in emphysema and
chest wall deformities)4. Unexplained dyspnea .5. Respiratory muscle weakness may compound other diseases:
malnutrition, steroid, drugs, thyroid disorders, heart failure etc.

Clinical signs of respiratory muscle weakness (Clinical Assessment):1. Dyspnoea during normal activities2. Orthopnoea3. Unexplained reduction in vital capacity4. Short sentences during speech5. Paradoxical movement of the abdominal or thoracic
wall6. Problems with cough (and recurrent infections)7. Generalized muscle weakness8. CO2 retention while awake or during sleep, specifically
in the absence of severe airflow obstruction

Principles of assessment of respiratory muscles
In clinical practice respiratory muscle force is indirectly measured through the pressure generated during inspiration or expiration
Respiratory muscle force is generally expressed as kilopascal (kPa) or cm water pressure
The pressure is generated by all the muscles under investigation (inspiratory or expiratory), and is hence not muscle specific nor cause specific.
Respiratory Muscle Testing

Respiratory Muscle Testing
1. Tests of Overall Respiratory Function2. Tests of Respiratory Muscle Strength3. Tests of Respiratory Muscle Endurance4. Imaging Respiratory Muscle Function5. Assessment of Respiratory Muscle Function in
the Intensive Care Unit

I. Tests Of Overall Respiratory Function

1- Spirometry & Lung Volumes:
The most frequently noted abnormality of lung volumes in patients with respiratory muscle weakness is a reduction in vital capacity (SVC & FVC).
Also TLC, RV and FRC might decrease
The VC is limited by weakness of both the inspiratory muscles, and expiratory muscles, inhibiting full inflation and expiration.
In most normal subjects, VC in the supine position is 5–10% less than when upright and a fall of 30% or more is generally associated with severe diaphragmatic weakness.

2- Resistance:
• Airway resistance is normal in uncomplicated respiratory muscle weakness .
3- Maximum Voluntary Ventilation
• The maximum voluntary ventilation was formerly recommended as a more specific test for muscle weakness than volume measurements but, in practice, the proportionate reduction is usually similar to that of VC .

4- Arterial Blood Gases
Arterial blood gases assess the major functional consequence of respiratory muscle weakness.
In chronic muscle weakness Pao2 and the alveolar–arterial O2 difference are usually normal.
In acute muscle weakness, Pao2 may be more markedly reduced, but the picture may be complicated by atelectasis or respiratory infection .

With mild weakness, Paco2 is usually less than normal , implying alveolar hyperventilation.
In the absence of primary pulmonary disease, daytime hypercapnia is unlikely unless respiratory muscle strength is reduced to 40% of predicted and VC is reduced to 50% of predicted.
In patients with Duchenne muscular dystrophy, hypercapnia has been shown to predict shorter survival .

II- Tests Of Respiratory Muscle Strength

Volitional tests of respiratory include:
a- Mouth Pressures (Maximal Static Inspiratory and Expiratory Pressure).
b- Sniff Test
c- SNIP Test (Sniff pressure at nose measured )
d- Cough Tests
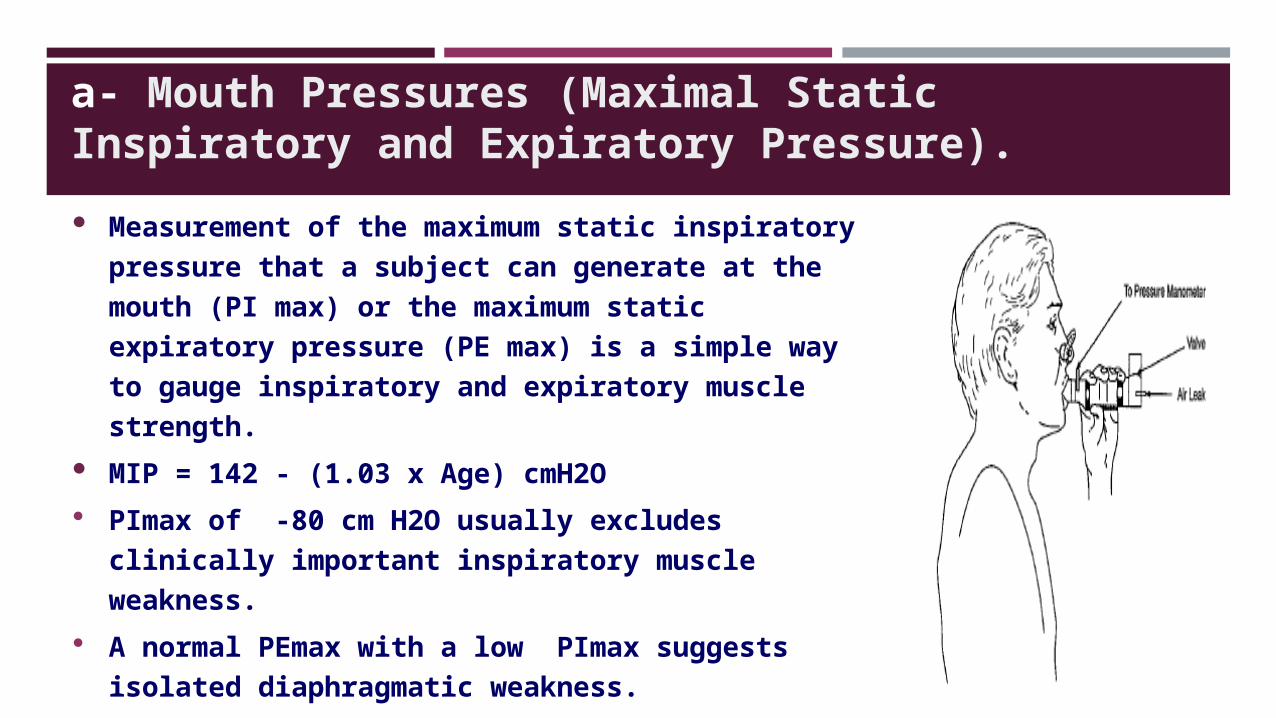
a- Mouth Pressures (Maximal Static Inspiratory and Expiratory Pressure). Measurement of the maximum static
inspiratory pressure that a subject can generate at the mouth (PI max) or the maximum static expiratory pressure (PE max) is a simple way to gauge inspiratory and expiratory muscle strength.
MIP = 142 - (1.03 x Age) cmH2O PImax of -80 cm H2O usually excludes clinically
important inspiratory muscle weakness. A normal PEmax with a low PImax suggests
isolated diaphragmatic weakness.
b- Sniff Test
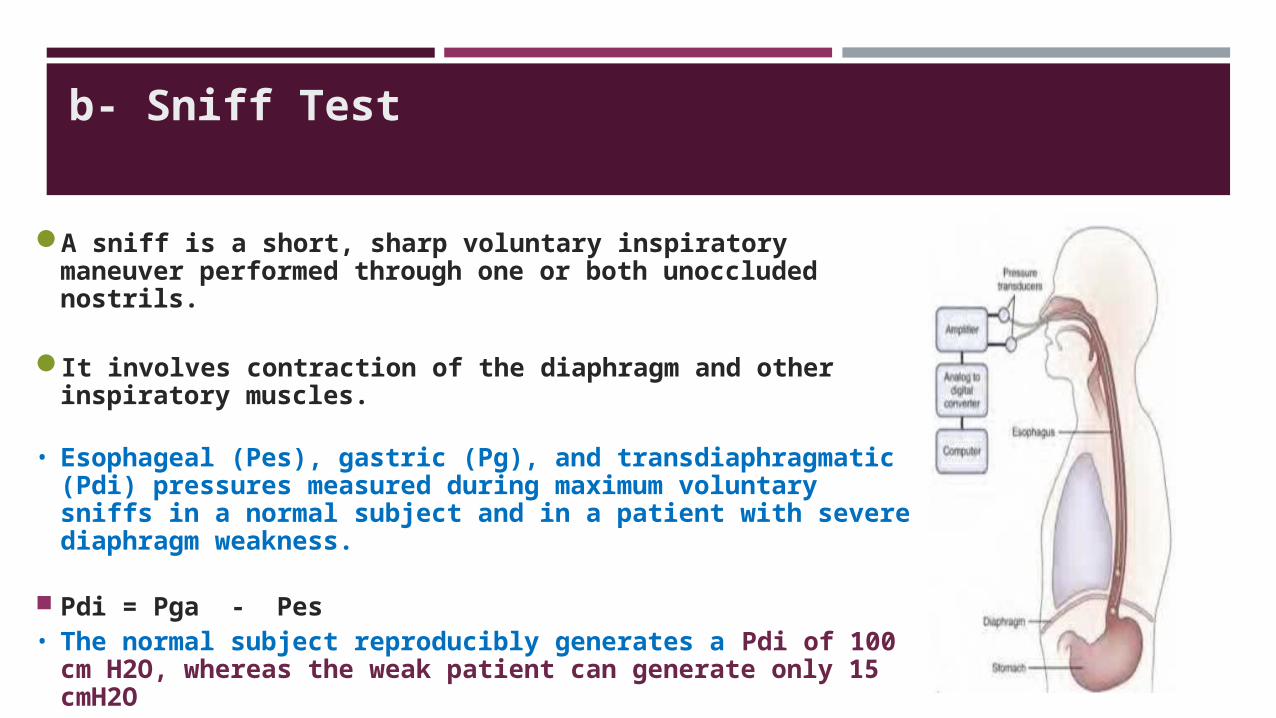
A sniff is a short, sharp voluntary inspiratory maneuver performed through one or both unoccluded nostrils.
It involves contraction of the diaphragm and other inspiratory muscles.
• Esophageal (Pes), gastric (Pg), and transdiaphragmatic (Pdi) pressures measured during maximum voluntary sniffs in a normal subject and in a patient with severe diaphragm weakness.
Pdi = Pga - Pes• The normal subject reproducibly generates a Pdi of 100
cm H2O, whereas the weak patient can generate only 15 cmH2O

C- Sniff nasal inspiratory pressure (SNIP)
Simple bedside test
Normal valve established (men > 70 cm H2O. women > 60 cm H2O)
D- Cough Tests
The main expiratory muscles and the abdominal muscles are used in cough.
• PE max and cough esophageal pressures comparable
• The mean maximal Pga, co was 230 cm H2O for men and 166 cm H2O for women.

III- Electro-physiologic Techniques for the Assessment of Respiratory Muscle Function
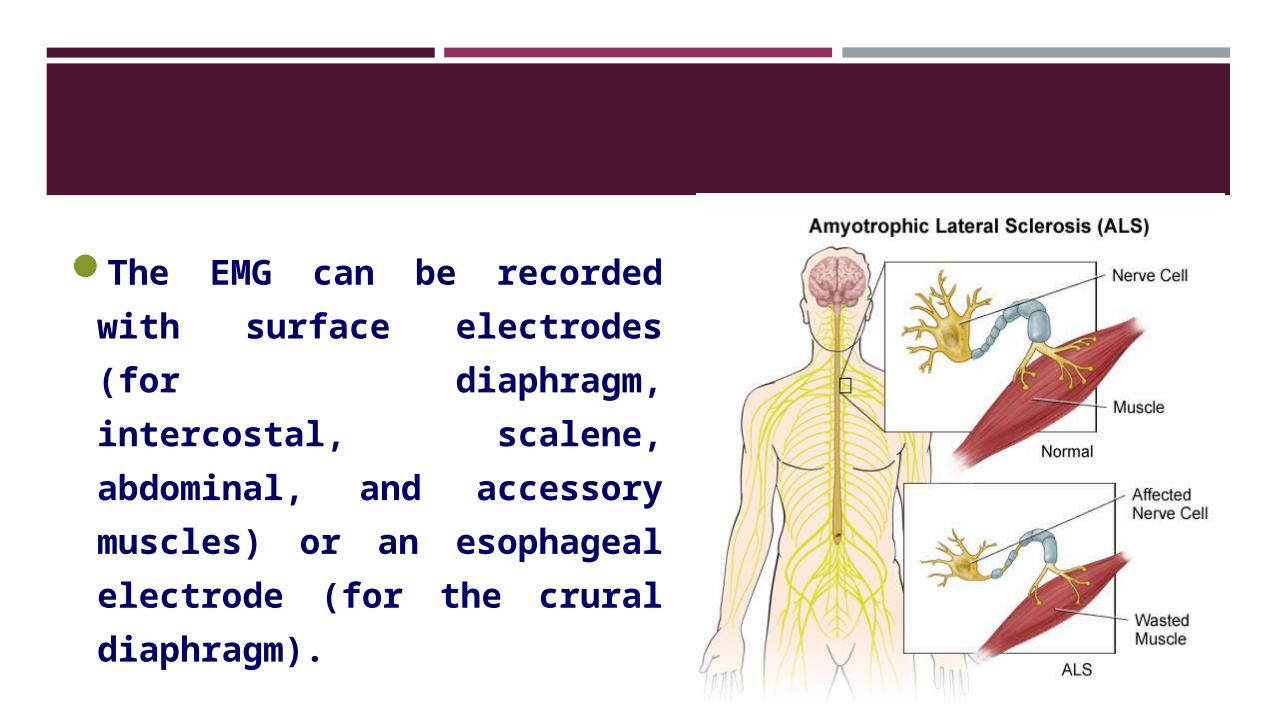
The EMG can be recorded with surface electrodes (for diaphragm, intercostal, scalene, abdominal, and accessory muscles) or an esophageal electrode (for the crural diaphragm).
VI- Imaging Respiratory Muscle Function

Imaging Respiratory Muscle Function
1. Transmission Radiography
2. Ultrasound
3. Volumetric Imaging
4. Nuclear Medicine

1- TRANSMISSION RADIOLOGY

2- ULTRASOUND

3- VOLUMETRIC IMAGING
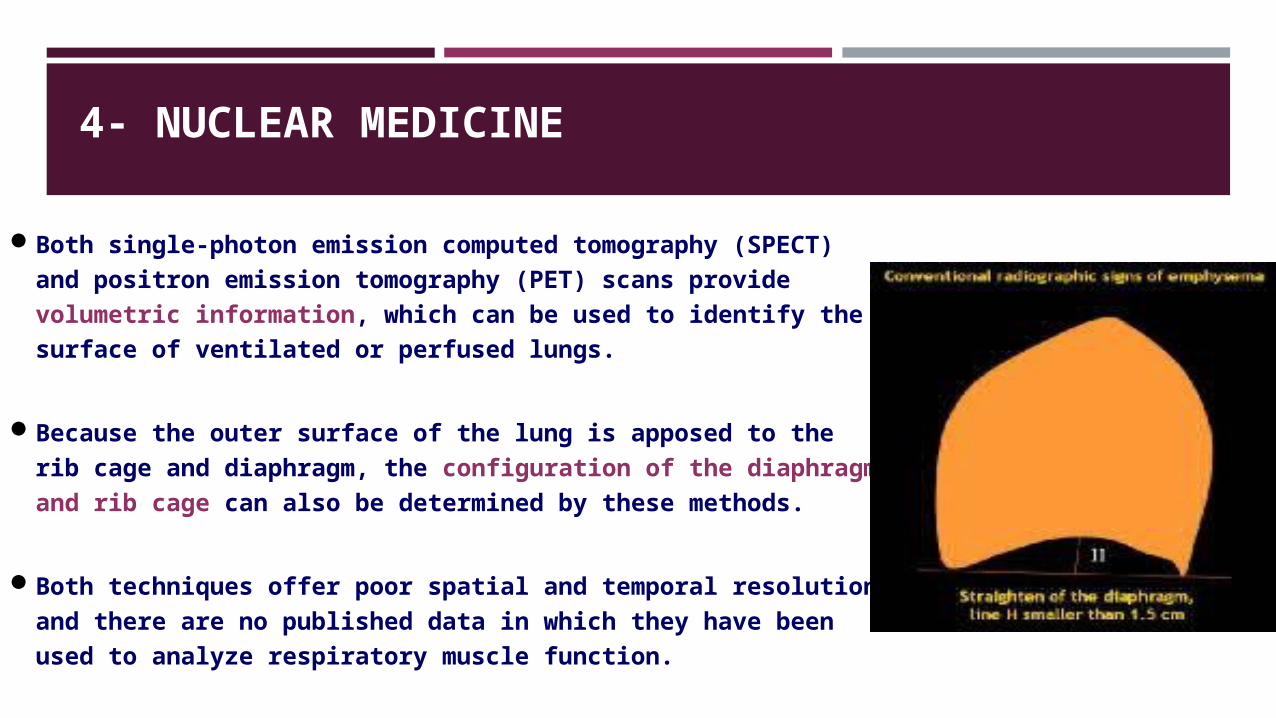
Volumetric computed tomography scans and magnetic resonance imaging can determine the configuration of the thoracic cavity. Both methods can be used to determine the detailed shape of the diaphragm , the rib cage, and ribs in normal and emphysematous subjects.
Volumetric imaging has limited research application.
4- NUCLEAR MEDICINE
Both single-photon emission computed tomography (SPECT) and positron emission tomography (PET) scans provide volumetric information, which can be used to identify the surface of ventilated or perfused lungs.
Because the outer surface of the lung is apposed to the rib cage and diaphragm, the configuration of the diaphragm and rib cage can also be determined by these methods.
Both techniques offer poor spatial and temporal resolution and there are no published data in which they have been used to analyze respiratory muscle function.

V- Assessment Of Respiratory Muscle Function In The ICU

Assessment Of Respiratory Muscle Function In The ICU
1. Breathing Pattern
2. Lung Volumes
3. Pressure Measurements
4. Prediction of Weaning
1.Breathing Pattern Abnormalities of the pattern of breathing are common in ICU patients,
especially in those with respiratory muscle dysfunction.Tachypnea is a sensitive marker of deteriorating clinical status, but is
not specific. Paradoxical motion of the rib cage and abdomen occurs with elevated
respiratory load, but is not diagnostic of respiratory muscle fatigue.
2.Lung VolumesFew studies have been conducted in critically ill patients examining
the usefulness of lung volume measurements.

3. Pressure Measurements 1. Measurements of maximum inspiratory pressure have poor reproducibility in critically ill patients and are of limited use for decision making in the ICU.
2. Airway occlusion pressure (P0.1) is easy to measure in patients receiving assisted ventilation, and high values signal increased respiratory motor output.
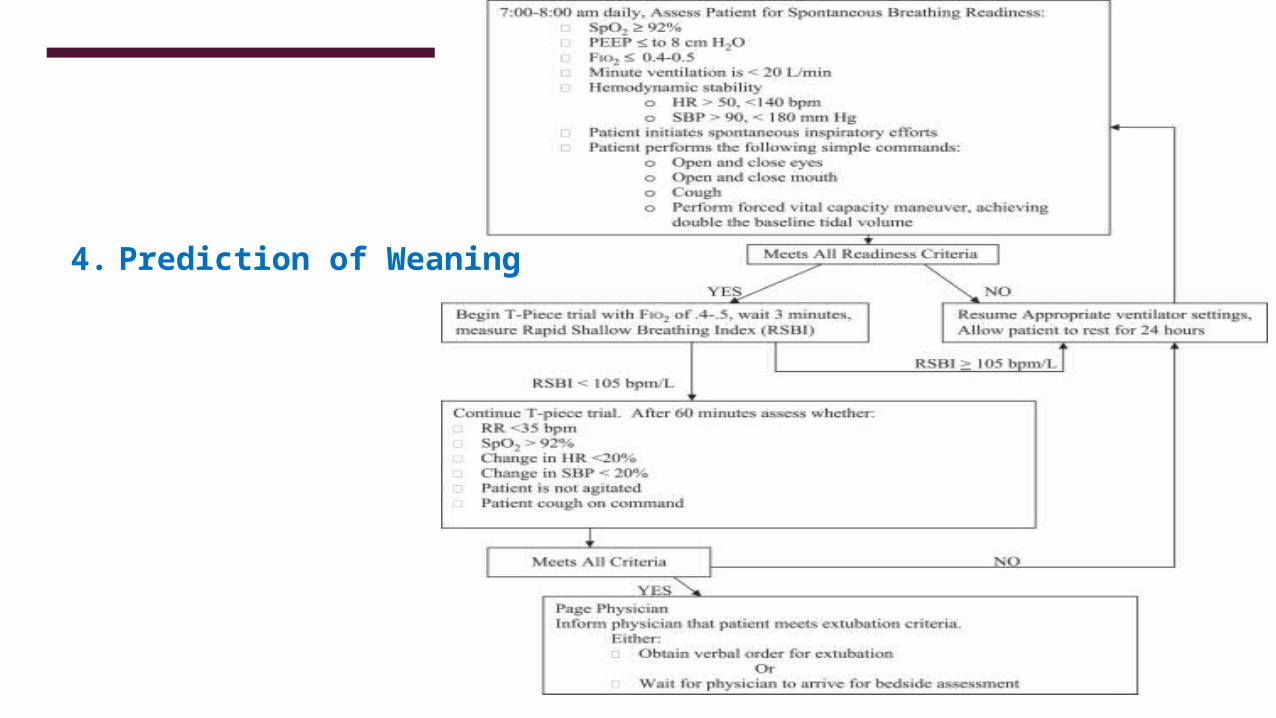
4. Prediction of Weaning

Thank You