respiratory failure 31/08/2011 vivian ho. contents definition types pathogenesis effects blood gases...
TRANSCRIPT

Respiratory failure
31/08/2011
Vivian Ho

Contents• Definition• Types• Pathogenesis• Effects• Blood gases• Management

Definition• Failure to maintain gas exchange• Numbers…
pO2 < 60 mmHg pCO2 > 50mmHg
Types• Acute / acute on chronic / chronic
• Type 1 vs Type 2
• Causes

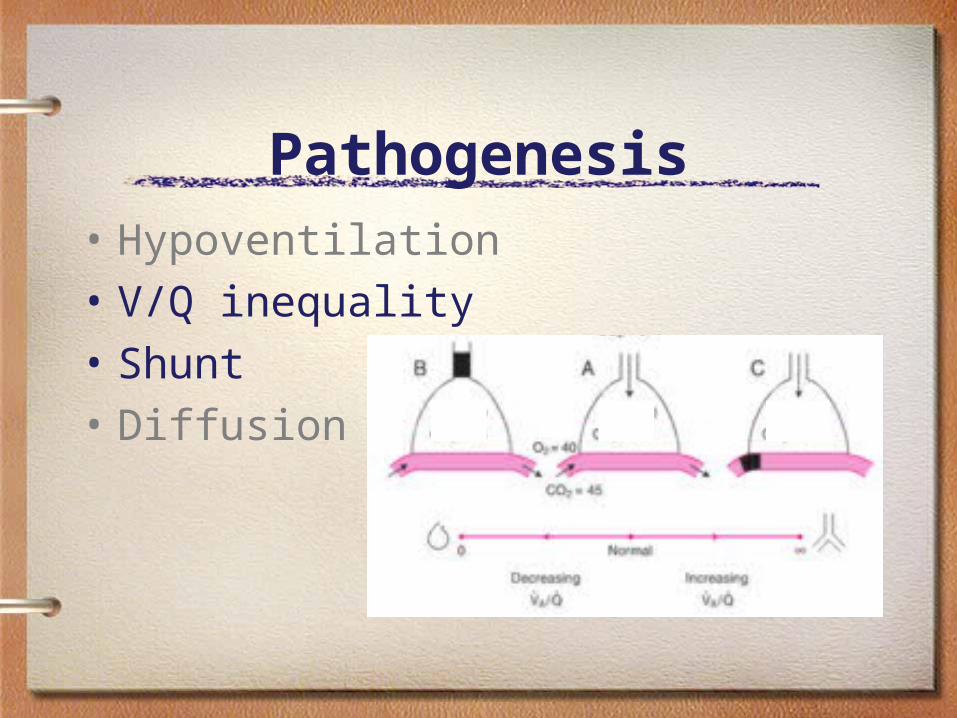
Pathogenesis• Hypoventilation • V/Q inequality• Shunt• Diffusion impairment

Pathogenesis• Hypoventilation • V/Q inequality• Shunt• Diffusion impairment
Pathogenesis• Hypoventilation • V/Q inequality• Shunt• Diffusion impairment

PaO2
40
0.25 0.75 Time (s)
Pathogenesis• Hypoventilation • V/Q inequality• Shunt• Diffusion impairment

Effects

Blood gases 1pH 7.47pCO2 33pO2 47Na 144 K 3.7HCO3 24BE 0.5FiO2 55%
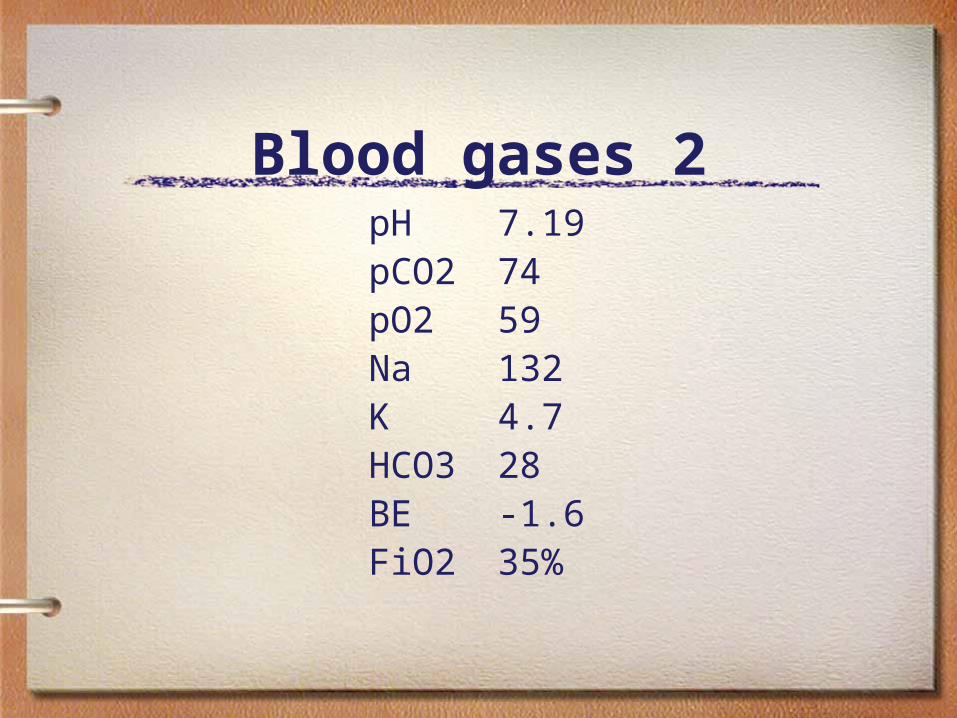
Blood gases 2pH 7.19pCO2 74pO2 59Na 132 K 4.7HCO3 28BE -1.6FiO2 35%
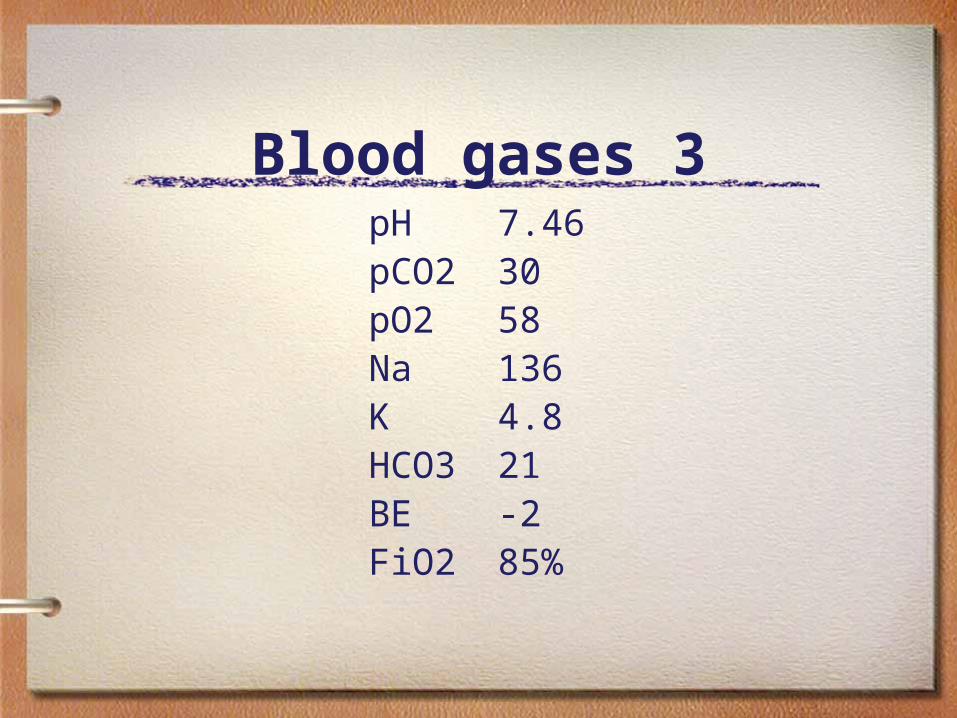
Blood gases 3pH 7.46pCO2 30pO2 58Na 136 K 4.8HCO3 21BE -2FiO2 85%
Management• Treat cause
• Oxygen
• Ventilatory support
To tube or not to tube
Ventilatory support
NIV• What is it?• How does it work?• When does it work? • What does the evidence suggest?

NIV• Indications
– Hypercapnic respiratory failure– COPD with resp acidosis pH 7.25-7.35 – Cardiogenic pulmonary oedema– Pneumonia in the immunosuppressed– Weaning from the ventilator in
hypercapnic COPD patients
NIV• Contraindications
– Airway – Facial abn– Respiratory Arrest– Severe hypoxaemia– Untreated pneumothorax– Haemodynamic instability– Agitation– GI bleed / ileus/ surg

Cochrane• NIV vs Medical therapy alone
– Lower mortality NNT 8
– Prevent intubation NNT 5
– Length of stay – Improved pH/paCO2/RR within 1h of
tx
NIV• Compared with intubation..
– Hosp acq pneumonia– Complications
Mechanical Ventilation• Indications for intubation
– Airway– Ventilation – Improve Oxygenation– Decrease work of breathing– Stabilise chest wall in severe injury

Summary• Resp failure is the inability to
maintain adequate gas exchange• Type 1: hypoxaemic• Type 2: hypercapnic + hypoxaemic• NIV should be considered in
– patients with hypercapnic resp failure – cardiogenic pulmonary oedema – pneumonia in immunosuppressed