residency manual - vanderbilt university medical center
TRANSCRIPT

1
Pharmacy Postgraduate Year One
Residency Manual 2013 - 2014
Table of Contents
Section I Training Manual Page
1. Purpose and philosophy 2
2. Organization Structure 3
3. Program Goals 4
4. Residency Program Structure 5
5. Benefits 6
6. Verification of Licensure 7
7. Supervision and Work Ethic 7
8. Policy Access 7
9. Required experiences and activities 8-10
10. Tracking Form 11-12
11. Residency Project 13-17
12. Residency Project Worksheet 14
13. Past Residency Project List 16-17
14. Project/Activity Timeline 17
15. Evaluations 19-20
16. Documentation 21
17. Hospital Pharmacy Practice (Staffing) Overview 23-24
18. Self-Assessment Questions 25-26
Section II Schedules / Calendars
1. Evaluation Dates and Residency Council Schedule 27
2. Rotation Schedule (Draft) 28
3. Presentation Calendar 29
4. Orientation Discussion schedule 30-31
5. Orientation Checklist 32-34
6. Orientation Calendar 35
Section III Resident Portfolio
1. Presentations
2. Projects
3. Assignments
4. Evaluations
Section IV On-Call Procedures for 2013 - 14 36-38

2
Pharmacy Practice Residency Program:
Structure
Purpose and Philosophy
Departmental Organization Chart
Program Goals
Program Structure
Benefits
PURPOSE AND PHILOSOPHY
The purpose of this residency is to develop a pharmacist with the skills and abilities
to successfully practice as an acute care pharmacist, adjunct faculty member, and/or
be prepared to pursue and complete PGY2 residency training.
Philosophy
The ASHP accreditation standard provides criteria that every program must meet in
order to receive and maintain accreditation. Although the standard requires
experiences in certain core areas, there is room for concentration in a practice area
and for additional experiences. The mission of our program includes developing a
core skill set in drug information and literature evaluation, pharmacotherapy
evaluation and management, project based research and team functioning,
presentation development and delivery, and direct patient interaction.

3

4
PROGRAM GOALS The residency program will provide each resident with specific learning/practice experiences designed to enable the
resident to expand the scope of his/her practice skills. Outcomes
R1 Manage and improve the medication-use process.
R2 Provide evidence-based, patient-centered medication therapy management with interdisciplinary teams.
R3 Exercise leadership and practice management skills. (Overall Performance and Administration Rotation)
R4 Demonstrate project management skills. (Projects)
R5 Provide medication and practice-related education/training
R6 Utilize medical informatics.
E2 Exercise added leadership and practice management skills.
E6 Provide drug information to health care professionals and/or the public.
E7 Demonstrate additional competencies that contribute to working successfully in the health care environment.
E8 Demonstrate additional competencies that contribute to working successfully in the health care environment (additional)
Patient Care
R2.10 Evaluate patients’ progress and redesign regimens and monitoring plans..
R2.11 Communicate ongoing patient information
R2.12 Document direct patient care activities appropriately.
R2.2 Place practice priority on the delivery of patient-centered care to patients.
R2.3 As appropriate, establish collaborative professional pharmacist-patient relationships.
R2.4 Collect and analyze patient information.
R2.5 When necessary, make and follow up on patient referrals.
R2.6 Design evidence-based therapeutic regimens.
R2.7 Design evidence-based monitoring plans.
R2.8 Recommend or communicate regimens and monitoring plans.
R2.9 Implement regimens and monitoring plans.
Practice Foundation Skills
R1.5 Provide concise, applicable, comprehensive, and timely responses to requests for drug information from patients, health care providers, and the public.
E8.1 Use approaches in all communications that display sensitivity to the cultural and personal characteristics of patients, caregivers, and health care colleagues.
E8.2/7.2 Communicate effectively.
E8.3/7.3 Balance obligations to oneself, relationships, and work in a way that minimizes stress.
E8.4/7.4 Manage time effectively to fulfill practice responsibilities.
R2.1 As appropriate, establish collaborative professional relationships with members of the health care team.
R3.1 Exhibit essential personal skills of a practice leader.
R3.3 Exercise practice leadership.
Practice Management
E1.1 Design, execute, and report results of investigations of pharmacy practice-related issues.
E2.2 Understand the pharmacy procurement process.
E2.6 Understand the process of managing the practice area's human resources.
E6.1* Participate in the organization’s formulary process.
E7.1 Identify a core library, including electronic media, appropriate for a specific practice setting.
E8.5 Make effective use of available software and information systems.
R1.1 Identify opportunities for improvement of the organization’s medication-use system.
R1.2 Design and implement quality improvement changes to the organization’s medication-use system.
R1.3 Prepare and dispense medications following existing standards of practice and the organization’s policies and procedures.
R1.4 Demonstrate ownership of and responsibility for the welfare of the patient by performing all necessary aspects of the medication-use system.
R3.2 Contribute to departmental leadership and management activities.
R4.1 Conduct practice-related investigations using effective project management skills.
R5.1 Provide effective medication and practice-related education, training, or counseling to patients, caregivers, health care professionals, and the public.
R6.1 Use information technology to make decisions and reduce error.

5
STRUCTURE
Orientation (required) Core Rotations (required) Transitional Elective Rotations
(choose 6) Hospital Orientation Residency/RLS Computer Training Hospital Practice
Administration General Internal Medicine Critical Care (pick two) Surgical ICU Trauma ICU Medical ICU Pediatric ICU Nutrition
Hospital Pharmacy Practice Projects ASHP Midyear
Solid Organ Transplant Bone Marrow Transplant General Pediatrics Hematology/Oncology Nutrition Infectious Disease Critical Care Medicine Trauma Burn Surgical Geriatrics Coumadin Clinic HIV/AIDS Cardiology ICU Pediatrics NICU Pediatrics Informatics
Longitudinal (required)
Drug Information P&T MUE Journal Club Case Conference Hospital Pharmacy Practice Staffing (operational and clinical) Residency Project Seminars Therapeutic Exchange CE 60min Residency Project 15-30min Criteria Based Skill Assessments (CBAs)

6
BENEFITS
Educational leave Full access to Biomedical Library
Books directly related to the residency (RD approval required) Lab coats are the responsibility of the resident, but
can be purchased through the hospital
15 days paid vacation & sick leave (Flex PTO) Select holidays
Travel & relocation expense directly related (moving company, rental, fuel, hotel) to the move –
up to $1500
Financial support and professional leave for the University of Tennessee
Annual Residency Program, the ASHP MYCM and the Annual Southeastern Residency Conference in Athens, GA
Life insurance Discounts at local merchants
Professional liability insurance supplied by the Medical Center
Limited financial support for presentations at Vanderbilt and outside the campus ( RD approval required) – depends on the
residents activities at the meeting (officer, presentation, etc.)
Health care coverage plan options All ACPE approved continuing education provided by the
Department of Pharmaceutical Services
Payment of Tennessee Board of Pharmacy license fee in June – license fee and professional tax.
We do not pay NABPLEX fees or for reciprocation of license to TN. We will pay for transfer of NABPLEX scores.
Immunizations and other health related costs required by the Medical Center
Photocopying directly related to residency House staff & hospital orientation programs
Office space & computer workstation Competitive stipend
Employee Assistance Program Employee Wellness Program
Concierge Service Membership in professional organizations is the
responsibility of the resident
Purchase of software, books, or other materials must be directly related to the achievement of residency objectives, and must be approved beforehand by the Residency Director.
Explanation of Time Off: Residents (Exempt Status) o Fifteen vacation days are accrued over the course of the year. Ten (10) vacation days are available for
use and must be taken during the year. Each resident must sign up for and take no less than one week of
vacation time prior to January 15 of the residency year. (Residency Director may approve alterations in
certain situations). In general, a maximum of five (5) of the 15 days accrued may be paid out to each
resident at the completion of the residency (these may be used during the year for extraneous
circumstances if deemed appropriate by the Residency Director). Vacation may not be taken during
ASHP Midyear Meeting or SERC meeting days, or scheduled holidays/weekends in the staffing
component of the residency. Vacation requested for June is discouraged and will be reviewed on a case
by case basis by the Residency Director. Residents may not be absent more than 5 days from any
rotation experience (professional leave/personal/vacation) unless approved by the Residency Director.
o Requests for vacation days should be submitted to the Residency Director via electronic mail at least 4
weeks in advance for priority consideration. Requests made after the 4 week cut-off will be handled on a
case-by-case basis in order to ensure appropriate staffing. All requests will receive a response within 2
business days. If for some reason the Residency Director is not available, the responsibility for reviewed
vacation requests will be delegated to the Residency Coordinator.
o 12 Sick Days are accrued over the course of the year. Refer to the hospital/department policy for details.
o Seven (7) Holidays (July 4th
, Labor Day, Thanksgiving Day, Christmas Eve, Christmas Day, New
Year’s Day, Memorial Day) and 3 personal days are accrued over the course of the residency year.
These must be taken. If required to work a holiday, the holiday is to be taken on an alternate day within
30 days of accrual. Residents will agree with rotation preceptor if the resident is to work the actual
holiday or take an alternate day as the holiday. If the resident is scheduled on the pharmacy staffing
schedule for a holiday, that shift prevails. The department also recognizes the day after Thanksgiving
and New Year’s Eve in the department staffing rotation and these are handled and scheduled per
department policy.

7
LICENSURE VERIFICATION
Pharmacy licensure in Tennessee is a requirement for pharmacy practice residents at VUMC. The residency
program director will confirm that each resident has taken the NABPLEX and the Tennessee pharmacy law
exam, or will take the Tennessee law exam upon transfer of NABPLEX scores from another state, or already
had a valid Tennessee pharmacy license. Upon notification of successful completion of the NABPLEX and/or
law exam the resident will provide documentation of licensure to the residency program director. The resident
will provide the department the licensure certificate for display during the resident’s year at VUMC. Licensure
must be obtained no later than July 31 of the residency year.
SUPERVISION AND WORK ETHIC
The resident is expected to achieve the objectives of the Residency Program related to both administrative and
professional practice skills. The resident reports to and is supervised by the rotation preceptor and the residency
director. During staffing, the resident is under the supervision of the pharmacist in charge.
Hours of practice vary according to the requirements set forth by the preceptor and director. The resident is
expected to be present in body, mind, and spirit at all assigned activities of the service they are currently a part
of, including medical staff rounding, education classes, and administrative activities. It is not uncommon for the
resident to be assigned duties that require work overnight or that may continue during days away from the
hospital. Although these assignments will be frequent, they will not be beyond the expectations of other
pharmacy professionals’ duties. An eight hour day is a minimum requirement for physical presence on site
during assigned work days.
The work of the Department is the resident’s most important commitment. Working outside the residency
program (moonlighting) is strongly discouraged, particularly at the beginning of the residency. Should posted
time be available inside the Department, the resident will be paid at a competitive staff pharmacist rate. To work
overtime, the resident must be trained in the area. Extra work moonlighting and overtime work must be
approved by the Residency Director, and hours worked will be reported on a monthly basis by each resident.
The ACGME duty hour requirements are to be followed at all times.
Additional Policies Applicable to Pharmacy Residents Should
be reviewed at the following websites:
Vanderbilt Human Resources WebSite: http://hr.vanderbilt.edu/
VUMC Website: http://vumcpolicies.mc.vanderbilt.edu
VUH Pharmacy Residency Policy: http://vumcpolicies.mc.vanderbilt.edu/E-
MANUAL/Hpolicy.nsf/AllDocs/A09FD26D92F6770886257289005AB35F

8
Pharmacy Practice Residency:
Activities/Requirements
Residency Experience Synopses
Tracking Form for requirement completion
Residency Project Requirement Overview and Timeline
Residency Project Description Worksheet
Completed Residency Project List (1999-2013)
Suggested Timeline for Requirements Completion

9
RESIDENCY EXPERIENCE ACTIVITIES
Out-of-State Conferences:
ASHP Midyear: Usually occurs the first week of December. Residents should start registration process for this meeting in
August.
Southeastern Residency Conference:
This is usually in April or May in Athens, Georgia. Registration begins in January/February and Abstract submission deadline is
usually around February 10. Residents are responsible for meeting these registration deadlines. Residents are to confirm these
deadlines and register in early January. Information for this conference can be found at:
http://www.rx.uga.edu/main/home/ce/programs-and-seminars/serc.asp#dates
Hospital Pharmacy Practice:
The residents will practice in a guided hospital practice scheduled every fourth weekend, selected holidays and one evening per week.
The resident will gain experience in the IV room, Central dispensing area, Narcotic Room procedures, and responsibilities of the
pharmacist in charge as well assist with clinical consults and dashboard monitoring.
Journal Club:
This is a longitudinal activity. Residents will sign up to formally present two current pharmacotherapy related studies during the
residency year. This will include a self-evaluation and a formal evaluation. Resident attendance is required at all sessions. The primary
goal of journal club is to exercise skills in critical thinking and literature evaluation.
Case Conference:
This is a longitudinal activity. Residents will sign up to formally present two case presentations during the residency year. The cases
presented should revolve around pharmacotherapy topics and include primary literature and be a case in which the resident was
directly involved. This will include a self-evaluation and a formal evaluation. PowerPoint is used for this presentation. Resident
attendance is required at all sessions.
Seminars:
Two formal presentations by each resident will be conducted during the residency year:
One of these will be a Therapeutic Exchange slot. This presentation should be a pharmacotherapy topic that includes
some controversy and/or is a hot topic in pharmacotherapy. This is a 60 minute CE presentation. This is not just a
review of a disease state. Primary literature is to be used as a guiding force to put this presentation together. This is to be
prepared and presented with MS Power Point. This will include a self-evaluation and a formal evaluation. Presentation
objectives and Title are to be submitted by July 15th to Gayle Lane. Self-assessment questions (~5 questions for the
audience) will are due by August 1st to Gayle Lane.
The second formal presentation will be a 10-15 minute presentation of the resident’s residency project. This includes
several practice sessions then the formal presentation with feedback/evaluation from preceptors and residents during
practice and attendees at SERC.
These presentations will be presented to the pharmacy department and other guests. Resident attendance is required at all sessions.
Pharmacy and Therapeutics Committee:
Each resident will attend one P&T committee meeting and related subcommittees during the residency year. A drug monograph will
be written and presented during this experience. This will be assigned by the P&T Pharmacist. Drug monographs require review and
presentation of primary literature. A 10 minute power point presentation will be prepared that focuses on the drug’s place in therapy,
with a literature supported comparison and analysis of efficacy, safety and cost of the drug and its competitors. An opinion should be
outlined with recommendation for formulary status. This will be presented to the P&T Committee. As new agents are constantly be
approved by the FDA, monographs will be assigned as they come to the attention of the P&T Committee. A resident will have
approximately 30 days to prepare the monograph once assigned.
Newsletter/Fast Facts:
Each resident will make two (2) Fast Facts contributions to the newsletter.
Research Project:
Each resident will conduct a research project over the course of the residency year. This project will include idea development,
literature review, study design, IRB submission, data collection, data analysis, data interpretation, oral presentation and a written
manuscript. The written manuscript is to include identification of an appropriate journal for potential submission and the following of
the instruction to authors for that journal. The manuscript must be written and submitted in final form prior to completion of
residency. The manuscript must be reviewed by the project mentor(s) and approved by the residency director.
10
MUE: Each resident will complete one medication use evaluation during the residency year. These are assigned in the first or second quarter
of the year and depending on the scope of the MUE chosen may be conducted individually or in pairs. Findings are to be summarized
in a 10 minute power point presentation with recommendations of the most appropriate course of action based on the findings to the
P&T Committee and/or appropriate committee.
Recruitment:
Residents will assist in the resident recruitment and candidate selection process.
Therapeutic Exchange:
This is a weekly conference held at noon on Thursdays by the pharmacy department for pharmacists and technicians to obtain
continuing education hours. Attendance by residents is strongly encouraged throughout the year.
Block Rotations:
There are 10 block rotation periods during the PGY1 residency year. Each block rotation period is approximately 4 weeks in duration.
A minimum of 7 of the seven rotation periods must be completed in clinical patient care rotations. All residents must complete the
following four required rotations: administration, internal medicine, two critical care rotations in either surgical or trauma intensive
care. Nutrition can be used for one critical care requirement if desired by the resident. During block rotations, residents will fulfill
many of the clinical core requirements of the residency as well as develop interest areas through selected rotations. Rotation
requirements may vary based on preceptor. Criteria based assessments should be reviewed at the outset of each rotation by resident
and preceptor to assure completion of all requirements by the end of the residency year.
Medical Center Educational Programs:
Noon conferences, departmental grand rounds, and other educational conferences are offered throughout VUMC. These are posted in
the Vanderbilt publications. Residents are encouraged to attend various conferences related to specific rotations.

11
RESIDENCY EVALUATION TRACKING FORM
RESIDENT: _________________
(Indicate date of completion in box)
SUMMATIVE EVLAUATIONS
Rotation Period Rotation 1 Rotation 2 Rotation 3 Rotation 4 Rotation 5 Rotation 6 Rotation 7
Preceptor’s Evaluation
Resident Self-Assessment
Preceptor/Rotation Eval
LONGITUDINAL EVALUATIONS
Hospital Practice Quarter 1 Quarter 2 Quarter 3 Quarter 4
Preceptor’s Evaluation
Resident Self-Assessment
Preceptor/Rotation Eval.
Residency Project
Preceptor’s Evaluation
Resident Self-Assessment
Preceptor/Rotation Eval
Training Plan Progress
Residency Council Report
Resident Training Plan Self Assess
PRESENTATIONS
Case Presentations #1 #2
Preceptor’s Evaluation
Resident Self-Assessment
Formal Presentations #1 #2
Therapeutic Exchange/Seminar SERC
Therapeutic Exchange/Seminar Self-Assessment
JOURNAL CLUB/DRUG INFORMATION
Journal Club #1 #2
Preceptor’s Evaluation
Resident Self-Assessment
DI Questions #1 #2 #3 #4 #5 #6
DI Researched Question Eval
Resident Self-Assessment ***Turn in to corresponding preceptor during rotation
12
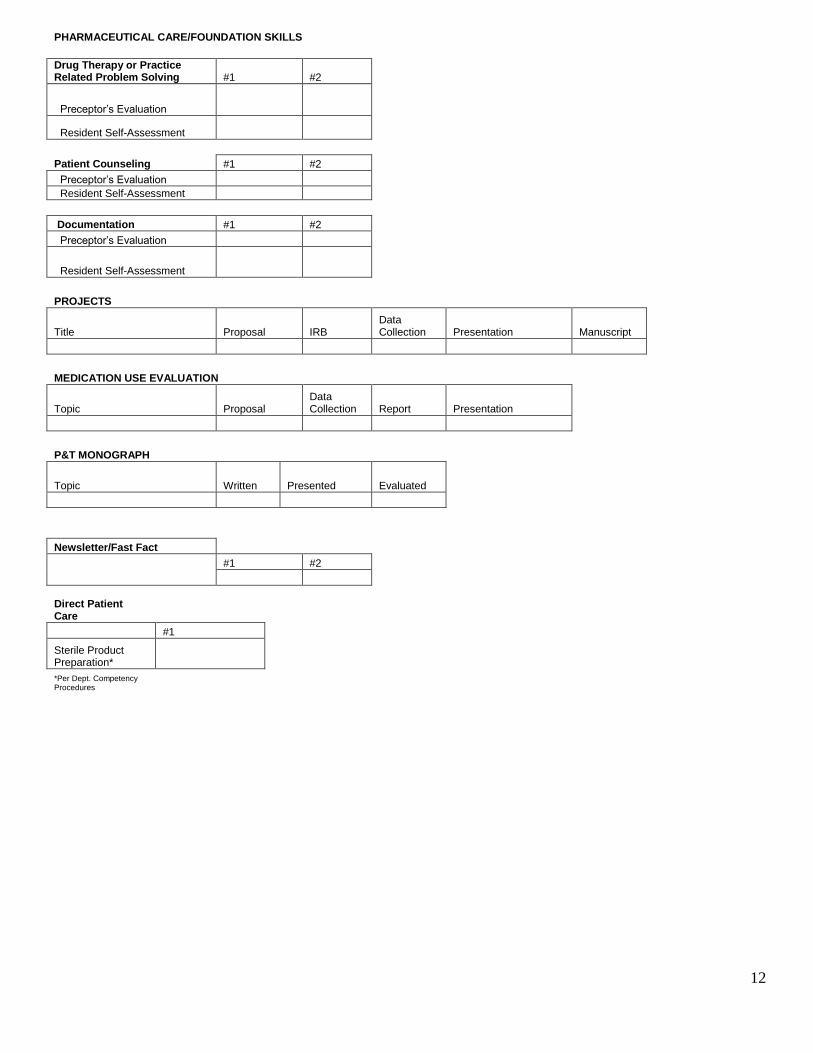
PHARMACEUTICAL CARE/FOUNDATION SKILLS
Drug Therapy or Practice Related Problem Solving #1 #2
Preceptor’s Evaluation
Resident Self-Assessment
Patient Counseling #1 #2
Preceptor’s Evaluation
Resident Self-Assessment
Documentation #1 #2
Preceptor’s Evaluation
Resident Self-Assessment
PROJECTS
Title Proposal IRB Data Collection Presentation Manuscript
MEDICATION USE EVALUATION
Topic Proposal Data Collection Report Presentation
P&T MONOGRAPH
Topic Written Presented Evaluated
Newsletter/Fast Fact
#1 #2
Direct Patient Care
#1
Sterile Product Preparation*
*Per Dept. Competency Procedures

13
RESIDENCY PROJECT
A project, administered by the resident and mentored by a primary preceptor, is
required of all residents. The project is to be of benefit to the individual, the
Department, and to the institution. There is to be a significant amount of literature
review, project design, data gathering, statistical evaluation, writing, and reporting
done by the resident. The end product is a presentation at the Southeastern
Residency Conference and a written manuscript suitable for publication in the
pharmacy refereed journal, written in according to the Instructions for Authors of
the American Journal of Health-System Pharmacists or selected journal
requirements. Residency project ideas will be submitted by the Department to the
residents early in the year. Deadlines are set for initial submission of project plans.
Projects must be evaluated for feasibility and approved by the residency director /
research committee before performing the project. One preceptor will be selected
for each project who will act to facilitate the project, mentor the resident, and who
shares responsibility for meeting deadlines, submission of applications for research
(IRB, etc.), presentations and manuscript development and submission. The project
plan submitted should be binding to the resident and to the preceptor(s) involved.
Project designs will be reviewed by the research committee. The committee will
serve as a consultant and advisor for the residency project.
Project Deadline Schedule:
Preceptor ideas due July 10
Project topic/title selected August 23
Study Protocol and data collection form complete October 4
IRB submission completed November 8
Project data collection complete March 5
Data analysis complete April 1
First manuscript draft May 30
Final revisions completed June 16

14
Residency Project Description Worksheet
2013-14
_________________________________________________________________
Resident: Project Advisor:
Date of Initiation: Date of Completion:
Responsible Investigators:
Department(s) Involved:
Key Personnel to Obtain Approval From:
Question to be Answered:
Expected Outcomes of the Study:
Rationale for the Study:
Defining Measurements:
Data that will be Collected:
Databases to Study or Create:
Data Analysis:
Description of Results:
Benefit to the Resident:
Benefit to the Department:
Likelihood of Publication:
Commitments: _________________ ____________________ __________
Resident Preceptor Other

15
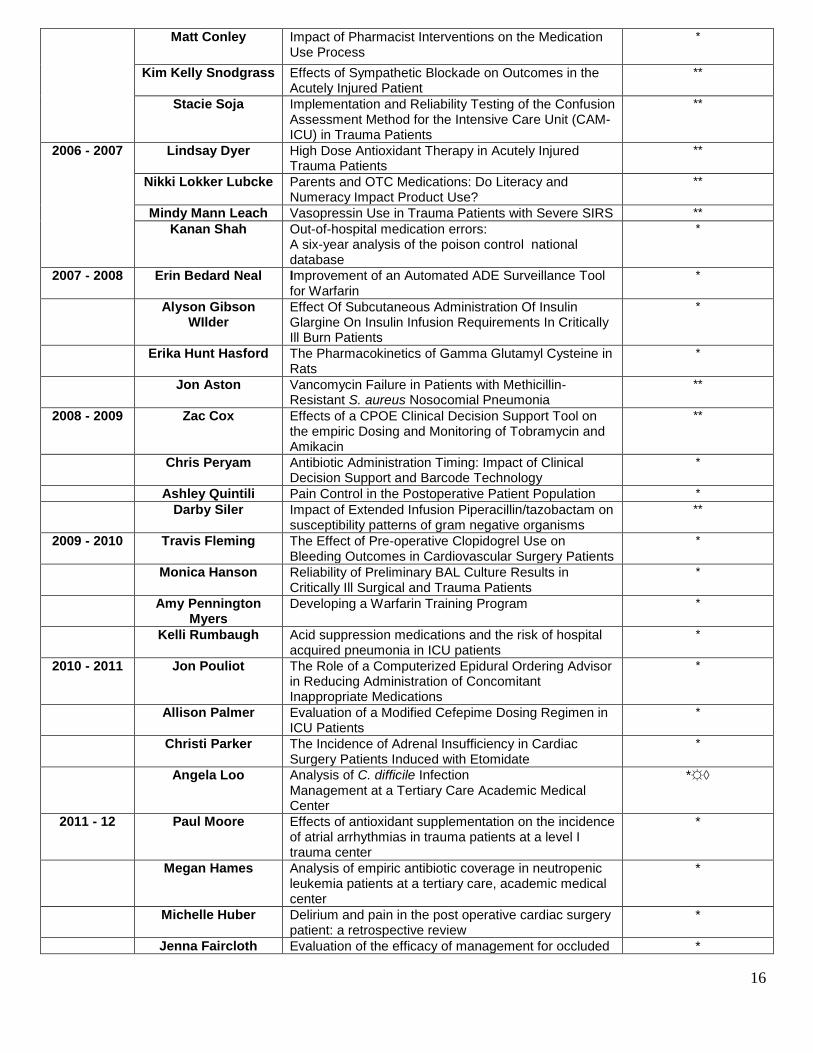
Past Residency Projects 1999 – 2013
Year Resident Title Comment
1998 - 1999 Darryl McGuire, Jr. Evaluation of Empiric Treatment of Community Acquired Pneumonia
*
1999 - 2000 Leigh Black Assessment of Pharmacists Knowledge and Attitudes Regarding Pain Management
* Submitted for publication
D’Andrea Forbish-Skipwith
Study of Dietary Supplement Use Among Medicine Patients
*
2000 2001 Amy Maulsby Potts Preparing and Modeling Pharmacy Analysis Techniques in a Managed Care Plan Physician Order Entry - Vanderbilt Health Systems
* ◊
2001 – 2002 Carly Feldott Pharmacist Involvement in a Managed Care Clinic Setting – A Focus on Asthma Disease Management, Cost Management, and Practitioner Prescribing Patterns
*
Lisa Izlar The Usage of Prophylactic Antibiotics in Coronary Artery Bypass Surgery
*
Kimberly Moyers Pharmaceutical Care in an Epilepsy Clinic *
Jill VonDielingen The Role of Pharmacists in Disease State Management (Diabetes Focus) in a Managed Care Setting
*
2002 – 2003 Marty Baker Reestablishment of an Institutional Antibiogram Phase I: Identifying Trends in Resistance
*◊
Christie Buchanan Pharmaceutical Intervention Improves Efficiency for High Risk Dyslipidemic Patients Compared to Usual Care – Part I
*◊
Lindy Taylor Factors and Issues to Consider in the Assessment of Adverse Drug Events among Hospitalized Patients
*◊ To be published in AJHP
November 2006
Karen Wilson Preventing Medication Errors with Smart Infusion Technology
*◊ Published in AJHP Jan
2004
2003 – 2004 James A. Carr Pharmaceutical Intervention Improves Efficiency for High Risk Dyslipidemic Patients Compared to Usual Care – Part II
*◊☼ To be submitted
Brian Fontenot Development and Implementation of a Pharmacy Discharge Counseling Service for the Patients of Vanderbilt Children’s Hospital
*◊☼
Brandy Greene Vancomycin Utilization Following Computerized Prescriber Order Entry (CPOE) Intervention
*◊☼
Natalie Kittrell Parks Protocol for Diagnosing and Treating Relative Adrenal Insufficiency
*◊☼
2004 - 2005 Paige Fuller Validation of an Innovative Computerized Vancomycin Dosing Nomogram Utilized by a Tertiary Care Teaching Hospital
◊☼
Shivani Patel Complications of Corticosteroid Therapy for Adrenal Insufficiency in Critically Ill Trauma Patients
◊☼*
Hayley Rector Assessment of an Alcohol Withdrawal Prevention Protocol
◊☼*
Katie Smith Glover Appropriate Use of Patient-Controlled Analgesia Infusion Devices
◊☼*
2005 - 2006 Jennifer Gray Effect of Bisphosphonates on Fracture Rates in Renal Transplant Patients
*
16
Matt Conley Impact of Pharmacist Interventions on the Medication Use Process
*
Kim Kelly Snodgrass Effects of Sympathetic Blockade on Outcomes in the Acutely Injured Patient
**
Stacie Soja Implementation and Reliability Testing of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) in Trauma Patients
**
2006 - 2007 Lindsay Dyer High Dose Antioxidant Therapy in Acutely Injured Trauma Patients
**
Nikki Lokker Lubcke Parents and OTC Medications: Do Literacy and Numeracy Impact Product Use?
**
Mindy Mann Leach Vasopressin Use in Trauma Patients with Severe SIRS **
Kanan Shah Out-of-hospital medication errors: A six-year analysis of the poison control national database
*
2007 - 2008 Erin Bedard Neal Improvement of an Automated ADE Surveillance Tool for Warfarin
*
Alyson Gibson WIlder
Effect Of Subcutaneous Administration Of Insulin Glargine On Insulin Infusion Requirements In Critically Ill Burn Patients
*
Erika Hunt Hasford The Pharmacokinetics of Gamma Glutamyl Cysteine in Rats
*
Jon Aston Vancomycin Failure in Patients with Methicillin-Resistant S. aureus Nosocomial Pneumonia
**
2008 - 2009 Zac Cox Effects of a CPOE Clinical Decision Support Tool on the empiric Dosing and Monitoring of Tobramycin and Amikacin
**
Chris Peryam Antibiotic Administration Timing: Impact of Clinical Decision Support and Barcode Technology
*
Ashley Quintili Pain Control in the Postoperative Patient Population *
Darby Siler Impact of Extended Infusion Piperacillin/tazobactam on susceptibility patterns of gram negative organisms
**
2009 - 2010 Travis Fleming The Effect of Pre-operative Clopidogrel Use on Bleeding Outcomes in Cardiovascular Surgery Patients
*
Monica Hanson Reliability of Preliminary BAL Culture Results in Critically Ill Surgical and Trauma Patients
*
Amy Pennington Myers
Developing a Warfarin Training Program *
Kelli Rumbaugh Acid suppression medications and the risk of hospital acquired pneumonia in ICU patients
*
2010 - 2011 Jon Pouliot The Role of a Computerized Epidural Ordering Advisor in Reducing Administration of Concomitant Inappropriate Medications
*
Allison Palmer Evaluation of a Modified Cefepime Dosing Regimen in ICU Patients
*
Christi Parker The Incidence of Adrenal Insufficiency in Cardiac Surgery Patients Induced with Etomidate
*
Angela Loo Analysis of C. difficile Infection Management at a Tertiary Care Academic Medical Center
*☼◊
2011 - 12 Paul Moore Effects of antioxidant supplementation on the incidence of atrial arrhythmias in trauma patients at a level I trauma center
*
Megan Hames Analysis of empiric antibiotic coverage in neutropenic leukemia patients at a tertiary care, academic medical center
*
Michelle Huber Delirium and pain in the post operative cardiac surgery patient: a retrospective review
*
Jenna Faircloth Evaluation of the efficacy of management for occluded *

17
enteral access
2012 - 13 Emily Bullington Incidence of refeeding syndrome with the initiation and advancement of parenteral nutrition
*
Juliana Kyle Open fracture prophylactic antibiotic protocol compliance and outcomes at an academic level I trauma center.
*
Jeremy Moretz Bleeding and the use of direct thrombin inhibitor anticoagulation in patients listed and evaluated for cardiac transplant.
*
Amory Cox Scott Review of pharmacist impact through a vancomycin pharmacokinetic consult service in an academic medical center
*
*Presented at the Southeastern Residents Conference in Athens, GA
**Published in a medical journal ◊ Presented at the ASHP Residency Poster Presentation ☼ Presented at the UHC Poster Presentation

18
RESIDENT REQUIREMENT/ACTIVITY TIMELINE** (For Guidance Purposes Only; Dates are subject to change based on individual resident goals/assigned tasks) **This may not be all inclusive – watch your residency requirements tracking form!**
July Baseline self-assessment (Entering resident interest and preference information)
Select and Develop 60 minute CE Presentation
Dates for Journal Club, Case Presentation Selected, CE Presentation
August Project topic/preceptor confirmed
Project literature review and bibliography completed and submitted.
MUE topic selected and timeline for completion established.
Register for ASHP Midyear Meeting
September Project design/Methods write-up complete
Project Proposal Presentation –IRB submissions
If taking a poster to MYCM, investigate deadlines for abstract submission
How many Criteria Based Assessments have you completed? Pace yourself!
Evaluate where you stand with longitudinal assignments (P&T Monograph, MUE)
If you have not started your MUE – start now!
October Project Proposal completion and submitting to IRB, establish timeline for project data collection
and analysis etc.
Are you working on your MUE? Just checking!!!
Recruitment Showcases
Case Presentations and Journal Clubs
November MUE timeline established and confirmed.
If taking a poster to MYCM need to complete slide by mid-November.
Recruitment Showcases
How many Criteria Based Assessments have you completed? Pace yourself!
Résumé preparation and interview skills
December ASHP Midyear – UHC Posters, showcase
January Register for SERC and Prepare SERC abstract
February Complete and submit SERC abstract
Wind up data collection for project
Case presentations and journal clubs
How many Criteria Based Assessments have you completed? Pace yourself!
Are you on track with your MUE?
March Project: begin organizing data – analyze data - results
April Pre-SERC project presentation I, II, III, IV, SERC
How many Criteria Based Assessments have you completed? Pace yourself!
May Project manuscript – first draft completed May 15th
June Final Project manuscript due June 15
All Criteria Based Assessment Requirements completed by June 15.
All requirements fulfilled no later than June 20.

19
Pharmacy Practice Residency:
Evaluation Process and Requirements
Evaluation Process Description
Resident Documentation Requirements

20
EVALUATIONS
An essential component of developing the skills of a resident is frequent two-way feedback between residents
and preceptors. The preceptors, program director, and residents will frequently provide feedback to one another via formal
evaluation. Evaluation will occur as described below:
a. Rotation Summative Evaluations: Due no later than 5 days after the end of the previous rotation period (5
business days). This is a written evaluation of the resident’s performances in meeting the objectives of each
rotation. The resident and preceptor will review these evaluations together. The resident will also complete a
preceptor and rotation evaluation and a self-evaluation. Additionally, the resident will complete selected
criteria assessment instrument’s as a self-evaluation to be discussed with appropriate preceptor and/or
program director.
b. Pharmacy Practice Quarterly Evaluation (Staffing/Project): PP is a longitudinal evaluation where a written
evaluation of the resident’s progress is completed. Rotation and preceptor evaluations must also be completed
on a quarterly basis for these experiences.
c. Criteria Based Assessments: evaluations of selected activities will be completed as a self-evaluation as well as
a designated preceptor will evaluate the resident.
Counseling (evaluation preceptor = primary preceptor during that experience)
Documentation (evaluation preceptor = primary preceptor during that experience)
Problem solving (evaluation preceptor = primary preceptor during that experience)
Researched DI Questions (evaluation preceptor = primary preceptor during that experience)
Case Conferences (evaluation preceptor will be assigned)
Journal Club (evaluation preceptor will be assigned)
Therapeutic Exchange (evaluation preceptor will be assigned)
Monograph (evaluation preceptor will be assigned)
d. Residency Council Reports – a written evaluation based on period review by the residency council. This
evaluation examines overall progress, including integration of skills learned in separate rotations, non-rotation
objectives/experiences, progress on longitudinal requirements/rotations (residency project, criteria
assessments etc.) and any pertinent trends or information found in evaluations to that date. This report will
track resident progress by goal quarterly using the 5 point scale established in this programs residency
evaluation system. Progress of the resident’s strengths, weaknesses and career goals will be documented. To
satisfactorily complete the residency, the resident must have shown improvement over the course of the year
in both resident and preceptor scoring. For any goals in which less than a score of 3 is averaged, the resident
and program director will work together to develop individualized plans to assist in making progress in those
areas by residency end. If the resident does not work towards those plans and progress improvement,
residency completion with certificate may be compromised. On a quarterly basis, goals in which the resident
has scored an average of 5 for two consecutive quarters will be removed from further evaluation.
a. Progress on yearly goals/objectives
b. Acute Care progress (rotations)
c. Staffing
d. CBAs
e. Practice Mgmt: Inter-professional communications/relations
f. Practice Mgmt: Professional presentation (verbal communication, dress, style, content)
g. Practice Mgmt: Planning and Organizing/meeting deadlines
h. Enthusiasm/initiative/disposition
i. Status of: scheduled presentations, residency project, MUE, Performance Improvement, drug
information, criteria based assessments, time worked, time off
All evaluations are to be discussed personally between resident and preceptor. All evaluations (rotation summative on
resident, resident on preceptor and resident on rotation overall), CBAs, and self-assessments, should be forwarded to the
resident program director or designee in electronic format. A hard copy should be printed and signed by resident and
evaluator and maintained in the resident’s residency portfolio binder. The electronic database will document the
review by the residency program director.

21
RESIDENT DOCUMENTATION
Each resident will maintain/submit the following documentation:
1. Summative Self-Evaluation (Final Comments section): Required for each rotation, concentrated
experience, longitudinal experience. Due 5 business days after the completion of the previous
Rotation period.
Self -Assessment on progress of goals and objectives assigned to the learning experience.
Summary of how your residency goals and objectives were met/unmet during the rotation period.
Summary of your professional strengths and weaknesses during the rotation period.
As the year progresses, compare to previous time periods and always include what is a focus for
improvement for the next time period as well as what has been achieved.
2. Rotation and Preceptor evaluations will be submitted to the preceptor and then program director or designee
5 business days following the completion of the rotation or designated quarterly evaluation completion
dates. This should be presented to the preceptor the same day that the preceptor presents the block or
longitudinal evaluation to the resident. The preceptor must sign off on this in the evaluation database as
reviewed.
3. Many Criteria Based Assessments (CBAs) are to be initiated by the resident as opportunities are
encountered then evaluated with corresponding preceptor and then forwarded to the program director or
designee. Resident initiated CBAs:
Counseling
Documentation
Problem solving
Drug Information Researched Questions
Case Conferences (evaluation preceptor will be assigned)
Journal Club (evaluation preceptor will be assigned)
Therapeutic Exchange (evaluation preceptor will be assigned)
4. A record of interventions is to be compiled on an ongoing basis. Many preceptors request a list of these
pertaining to the rotation as part of the rotation summative evaluation.
5. Each resident will compile a residency notebook for the year to include: The contents is to include
suggestions/edits/drafts/final copies as worked on between resident and preceptor(s) as well.
1. Documents described above
2. All evaluations
3. In-services presented (handouts and outlines, slides)
4. Cases presented
5. Any education programs presented
6. MUEs, monographs, reports etc.
7. Written projects or proposals
*The contents of the residency notebook serve as documentation of activities completed during the residency
year. The residency yearbook is a permanent record which is the property of Vanderbilt University Medical
Center.*

22
Pharmacy Practice Residency:
Longitudinal Rotation Experience Descriptions
Hospital Pharmacy Practice (Staffing)

23
HOSPITAL PHARMACY PRACTICE (STAFFING)
(This is a guideline and will be dependent on staffing location assignment)
Expectations for Residents in First Quarter – Staffing Assignment
Orient to the Central Pharmacy and learn the procedures of both the unit dose area and the sterile
products preparation areas.
Adjust to the scheduling assignments and focus on being present and ready to work in the assigned area
at the assigned time. Stay in the work area during your entire shift and be available to focus on the work
at hand. Observe appropriate break time such as 30 minutes for lunch breaks. Learn to indicate any
scheduling adjustments on the posted pharmacist schedule such as swaps in assignments
Develop an understanding of the systems and processes and develop skills such as with CPOE order
processing (“VOP”).
Develop relationships with the Central Area team. Be careful to ask a more senior pharmacist before
making changes to work processes. Follow the established dress code and other workplace policies. Be
sensitive to the needs of the other staff in the area and do not routinely ask to leave early. Make sure that
work is caught up prior to leaving your assignment.
Begin to develop a broader view of the work place and rotate among the various stations (AcuDose
check or cart check, extemp prep, packaging machine, phones, tube station, IV Room, etc.) in order to
maintain and effective work flow and efficiency level.
Learn to collaborate with other staff members shift regarding work flow issues or whenever time may
become available to work on projects but remain available to return your focus to the work at hand
whenever workload increases.
Remain flexible and ask questions.
Work on Clinical Dashboards.
Once initial training is complete, primary assignment will be in the Unit Dose area.
Resident will check in with the pharmacist and technician mentors at the end of each weekend shift to
see if there are suggestions for improvement. If mentors are not working on the same weekend, resident
will check in with their mentors at the next available opportunity to discuss any questions.
Expectations for Residents in Second Quarter – Staffing Assignment
Demonstrate proficiency in all areas of the Central Pharmacy.
Demonstrate proficiency with systems and processes and manage the established levels of efficiency.
Demonstrate a broad view of the work place and rotate among the various stations maintaining effective
work flow and efficiency.
Primary assignment will be to float between the IV Room and Unit Dose areas
Work on Clinical Dashboards
Resident will check in with the pharmacist and technician mentors at the end of each weekend shift to
see if there are suggestions for improvement. If mentors are not working on the same weekend, resident
will check in with their mentors at the next available opportunity to discuss any questions.
Expectations for Residents in Third Quarter – Staffing Assignment
As above with more autonomy
Responsible for Clinical Dashboards
Expectations for Residents in Fourth Quarter – Staffing Assignment
Begin training in the Junior Pharmacist in Charge (PIC) role

24
The resident (junior) and the normal (senior) management person on the weekend will both be
designated as PIC. These two persons will work together to manage the personnel and workflow. The
normal management person can help teach the resident how to solve problems that arise during a shift.
The resident will not be in the float position unless scheduling dictates this as a need. However, part of
being PIC includes assessing both the unit dose and IV areas and helping in all areas.
The resident has an increased responsibility to keep in touch with the workflow and employees during
the shift. The resident should assure all work has been completed for the shift prior to approving anyone
to leave early (then check with the lead tech and check who is working in an overtime slot to help with
these decisions).
Communicate end of shift issues to the unit dose area evening pharmacist prior to leaving.
Personnel conflicts, staffing problems, catastrophes, occupational health issues will defer to the senior
management person designated for the weekend.
Resident will check in with the pharmacist and technician mentors at the end of each weekend shift to
see if there are suggestions for improvement. If mentors are not working on the same weekend, resident
will check in with their mentors at the next available opportunity to discuss any questions.
Continued responsibility of Clinical Dashboards
Expectations for Mentors
Check in with residents at the end of each weekend workday or as soon as possible after their weekend
to work to discuss their staffing and PIC roles and answer any questions that arise.
Observe and obtain direct feedback from pharmacists directly staffing with the residents during their
staffing and PIC roles and offer tips and suggestions for improvement.
Provide feedback to the resident from other staff members as appropriate regarding their work
performance.
Prepare the quarterly evaluations for the residents in regard to their overall experiences.
Expectation of Residents
Submit a report of activities learned, accomplishments, problems solved etc. as well as areas in need of
clarification or focus for the next weekend by Monday following your weekend worked.

25
Appendix

26
QUARTERLY RESIDENT TRAINING PLAN
SELF ASSESSMENT ASSISTANCE SHEET
If you want to grow personally and/or professionally you have to take an honest look at where you are before you can decide where
you want to go. A serious self-evaluation is very helpful if done on a regular interval basis. Prepare a summary of how your residency
goals and objectives were met/unmet during the rotation period, what were your professional strengths and weaknesses during the
rotation period and the progress you have made on longitudinal requirements (projects, criteria based assessments etc.) and an
assessment of personal/professional life balance.
The following questions facilitate a positive self-reflection and make the process more effective. These questions will be fuel for
helping you understand how progress is being made and what course corrections are necessary. They also open the door for some
serious career mentoring. You may want to discuss the answers you arrive at, or not. Most importantly, the questions may help you
discover the skills you need to achieve your goals.
Think about these types of questions when completing your progress review form. Use the Assessment FORM to complete this
exercise.
Career
1. What are my desired professional outcomes for the next year?
2. What are the most significant professional challenges for the next year?
3. What are the most significant professional opportunities for the next 3 to 5 years?
4. Who am I not working well with, and how can I make the relationship better?
5. What issues keep me up at night?
6. What have I learned about myself while working at my job?
7. What would I like to see my hospital modify?
8. What have I learned from my staff/co-workers and from working for my hospital?
9. What will I commit to make me better and to make those around me better?
Personal
1. What are the most valuable achievements/goals I attained in the past 4 months?
2. How can I improve the way I am dealing with the current challenges in my life?
3. What are my most significant personal goals for the next period?
4. What do I need to keep doing?
5. What would I like to change about myself?
6. What are my most significant personal challenges for the next period?
7. How am I treating the most important people in my life?
8. How could I treat the most important people in my life better?
9. How will I add joy to my life in the next period?
10. What do I wish for the future?
Preparing for my next step 1. Would I work better in a large or small organization?
2. Do I prefer working in a team environment or on my own?
3. Am I more comfortable following than leading?
4. Do I prefer to analyze situations and projects over actual implementation of an action plan?
5. Do I prefer to work with people or things?
6. How do I work under pressure?
7. Am I a good planner or idea person?
8. Am I a good listener?
9. Am I able to think quickly and articulate myself “on the spot”?
10. Am I able to make decisions in a timely manner?
11. Do I express myself well verbally and in writing?
12. What characteristics do I admire in others?
13. What do I enjoy most about my major?
14. What aspects of my current job do I enjoy? What do I dislike?
15. In the next five years what would I like to accomplish?
16. What level of responsibility do I hope to reach in the future?
17. How will I achieve my career goals? What skills, knowledge, and experience do I need?

27

28
@ Warfarin Sentri 7 back-up only for anticoag pharmacist; # Aminoglycoside Sentri 7 daily check at 2:30 to wrap-up non-covered patients. * Vancomycin Sentri 7 daily check at 2:30to wrap-up non
non-covered patients when TDM pharmacist unavailable. The @, #, and * residents will work together if necessary to complete the dashboards. If one of the residents is off, the other will check both
dashboards. On-call resident and Backup On Call Pharmacist covers when both preceptors and both residents are out.
Andy Bodiford
Jason Tomichek
Jennifer Hale
Meghan Caylor
Megan Perry Sarah Baggett PGY2 CC Jeremy Moretz
Juliana Kyle Anuj Thirwani Will Walker Megan Bodge
Liver 7/1- 10/4
Aug Heme/Onc-Jon
Card@ Med* MICU TICU SICU# HF Clin Systems LU/Acad Hematology
Sept Card@ Nutrition ID# TICU* Admin SOT HF Phm Systems Phm Systems
Pediatric BMT (Elective)
Oct TICU# MICU* NICU Cards@ Nutrition
Gen Peds CV surgery
Heart/Lung 10/7 – 1/17
ID Clin Rotation
Data Stds Intergrat
IDS (Elective)
Nov NICU Informatics Nutrition* Admin Cards@ ID# MCS CDS CDS Medical Oncology
Dec Project Month / Midyear Project Research
Project EP/Project
Jan MICU@ Admin SICU Med* ID# HIV- Outpt TICU
Renal/Panc 1/20 – 4/25
Data Mngt Data Mngt Pain/Symptom Management
Feb Med ID# SOT SICU* MICU@ Admin Cards Txplnt
Med Safety Med Safety Elective
Mar HemeOnc/BMT
Med* Cards@ ID# HemeOnc Mahsa
MICU CV Stepdown
CDS II CDS II ID Transplant
April HIV-Outpt TICU@ HemeOnc Jon
Nutrition SICU# Med* MICU
Txpant ID
4/28 – 6/30
Tech Concepts Med Safety II
Adult BMT
May Admin SICU MICU* SOT Med #1@ TICU# CV surgery AdminRx Vendor
LU Drug Info Clinic
June ID# Gen Peds Admin Gen Peds Med #2* Cards@ MCS Amb Care Elective Elective

29
Resident Presentation Series 2013-2014 Draft
PCR 12-1:00
Journal Club Resident Evaluator
August 27 Juliana Kyle
September 10 Megan Bodge Megan Hames
September 24
October 8
October 22
November 5
January 14
February 4
Feb 25
Mar 4
Mar 25
April 1
Apr 15 Jeremy Moretz Dan Johnson
May 6 Megan Bodge Mahsa Talbott
Case Conference Resident Evaluator
September 17 Jeremy Moretz Dan Johnson
September 17
October 15
October 15
November 19 Susan Hamblin
November 19 Megan Bodge Jon Aston
January 21
January 21
February 18
February 18 Juliana Kyle
March 18
March 18
April 8 Juliana Kyle Stefanie Bala
April 8
May 20
May 20
Therapeutic Exchange Resident Evaluator
August 22
August 29
September 5
September 12
September 19
September 26
Oct 3 Juliana Kyle Jennifer Gray
Oct 10 Jeremy Moretz Dan Johnson
Oct 17
June 5 Megan Bodge Research Preceptor

30
Orientation- First Week
Items you will need July 1:
Bring Car Registration; License Plate Number
Bring 2 forms of ID (Drivers License, Passport, Birth Certificate)
Copy of current Immunizations
Check book: cancelled check if you would like direct deposit; check to order lab coats
Pen
Monday, July 1 (Wear Walking Shoes; Picture will also be taken this day)
Tuesday, July 2
Wednesday, July 3
Time Activity
8:00 am-10 am Meet Gayle Lane (VUH B131) for pictures Name Badges (Pictures Again)
Distribute Computer access codes
Keys to office
Parking sign up (bring car registration)
Pagers
Take Website Pictures
10 am-1050 am David Gregory— Department and Residency Policy Review
11 am-12:30 pm Lunch and Tour - David Gregory, Gayle Lane
12:30 to 3:30 pm Meet with David (PCR B130 VUH) Write a brief biosketch each to be sent with picture and be posted on website
Complete Interest Inventory/Learning plan/Goals
Review Orientation Schedule
Staffing Orientation schedule and checklist
Time Activity
8-9 BLS Pre-work (for tomorrow) Here are a few details to help you prepare for class schedule for tomorrow, 7/3 @8 am: • It is imperative that you come prepared.
• Per American Heart Association guidelines, students will have 2 attempts at each testing station (1 written exam, 3 skills
tests). You must repeat the whole course if unable to pass each test within 2 attempts. • A BLS study guide is available on our website www.vanderbiltcpr.com.
• Visit our website www.vanderbiltcpr.comfor a map and directions to our office. We have a hard location to find so please
print and use the map.
• The course is scheduled to last 3.5 hours. Please make plans to be available for the duration of the course.
9-12 N Additional Orientation (PCR B130 VUH) Veritas/Medication Safety – Carly Feldott (9:00)
Distribute Residency Manuals (David Gregory)
Review Rotation Schedules (David Gregory)
12 to 1 pm Lunch on Own
1 - 3 RLS Overview- David Gregory
3-5 Citi Training (On your Own)- or complete BLS Prework
Time Activity
8:11:30 am BLS Training
11:30-12:30 Lunch on Your Own
12:30-1 Check in with David
1-3:30 Eskind Library Orientation (David or Gayle will walk you here)

31
Thursday, July 4th
Holiday OFF
Friday, July 5
July 8th
Hospital Orientation: You Make a Difference 8:00-4:15
July 9th
Hospital Orientation: Hearts & Minds 8:00-4:15
July 10th
and 11th
Computer Training with Philip Stewart
July 12th
: Presentation and Other Residency Requirements with Erin Neal
July 15th
– July 24th Operational Staffing Hands-On Training (Molly Knostman)
July 25th to July 31st Clinical and Resident Responsibilities Hands-On Training
Time Activity
8-11 am Quantifi, Med Use Policy, Monograph, MUE, TE Expectations (Bob)
11-12:30 Ken Sinclair- Department Compliance –Annual Requirements (PCR B130
12:30-1:30 Lunch
1:30- 4:30 Work on Your Therapeutic Exchange or Complete CitiTraining

32
Pharmacy Resident
Orientation Checklist
2013-2014
Central Pharmacy
Orientation Checklist Orientation Items Resident Initials Trainer Initials Date Reviewed
General Daily work flow Unit Dose Area Times and associated tasks
Review Pharmacist Shift slots and associated duties Pharmacist in charge IV/Central UD Float Central UD IV/TPN
Review how to read/interpret staffing schedule
Review daily Technician slots and associated responsibilities
Procurement Process Storeroom Staff Storeroom Responsibilities Storage locations: walk in fridge, storeroom, Med Carousels, PakPlus room Over fill cart, IV/TPN room
Med Carousel/Connect Rx Process Log In code given Pull on demand pick Review of AcuDose/Cartfill Process Pharmacist Scan process Acceptance of AcuDose zones
AcuDose Fill Process AcuDose Orientation with Frank Ray Checking AcuDose Doses AcuDose Log-in and Filling AcuDose Machines Narcotic Check in Narcotic Room
Medication Error Recording Process in the Central Area Internal Errors External Errors
Narcotic Room Procedures CII Safe Log-in and orientation with Charity Prater Checking process Discrepancy resolution Narcotic orders attachment in HMM (patient specific)
Cart Fill Process Pull process from Med Carousel Check Process Catch-up Doses Delivery of meds to patient specific med drawers
Look alike – Sound alike medications
Extemp Process Set up/Filling Process Checking Process
Non-Sterile Compounding area Orientation to Area What type of products made Who to ask if questions PCCA
Order Processing (Vopping) in Central Areas Central order processes for What to send to the ED
Resident:________________

33
How to Clarify an order (resident pager list/operator)
Crash Carts 6 month expiration Red Locks Charges ED Trays
Specific References: Psych book, IV reference manual etc. Blood Factor book, Clozaril, MSDS, etc.
Borrow/Loan policy and procedures
Unit dose packaging TadPoles Bar coding Responsibilities of Pharmacy Unit Dose Packaging Options How to check items in Pak Plus
Tube system policy and procedures Tube System Competency Check List
*Outpatient prescriptions, Stallworth and Psych Hospital Procedures on weekends (cover on first weekend)
IV/TPN/IDS Room Orientation Checklist Orientation Items Resident Initials Trainer Initials Date Reviewed
General workflow and distribution of responsibilities amongst pharmacists and technicians
How to find things in the IV room
IV preparation policy and procedures Set up of IV Preparations and Batches Reconstitution of vials Preparation of syringes, PB, LVP and checking these Storage of medications prior to delivery Delivery Schedule
Sterile products preparation check off
Call for medications
Review of how we meet USP 797
Latex allergy policy and procedures
Review of IV resources: how to determine compatibilities, expirations, Vandy IV manual, IV room website , latex website
Narcotic Preparation and wastage Log sheets Wastage record Record of RX number in patient maintenance
Standard Time Schedules
Investigational Drug Area
TPN Area
Outpatient Areas Orientation Checklist Orientation Items Resident Initials Trainer Initials Date Reviewed
Review of what and where all outpatient pharmacy services are located, hours, key persons
**Indigent Med Program: policy and procedures – please learn the process of who is eligible, what the policy is, how patients are approved, how much medication can be dispensed.
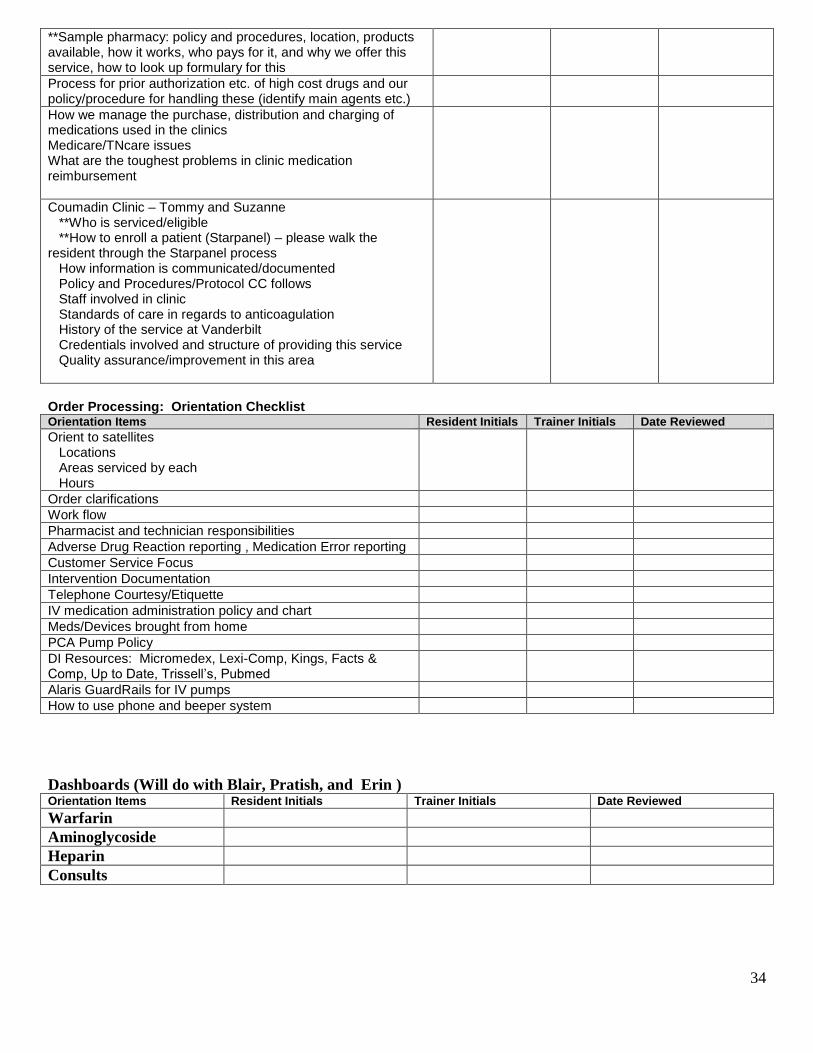
34
**Sample pharmacy: policy and procedures, location, products available, how it works, who pays for it, and why we offer this service, how to look up formulary for this
Process for prior authorization etc. of high cost drugs and our policy/procedure for handling these (identify main agents etc.)
How we manage the purchase, distribution and charging of medications used in the clinics Medicare/TNcare issues What are the toughest problems in clinic medication reimbursement
Coumadin Clinic – Tommy and Suzanne **Who is serviced/eligible **How to enroll a patient (Starpanel) – please walk the resident through the Starpanel process How information is communicated/documented Policy and Procedures/Protocol CC follows Staff involved in clinic Standards of care in regards to anticoagulation History of the service at Vanderbilt Credentials involved and structure of providing this service Quality assurance/improvement in this area
Order Processing: Orientation Checklist Orientation Items Resident Initials Trainer Initials Date Reviewed
Orient to satellites Locations Areas serviced by each Hours
Order clarifications
Work flow
Pharmacist and technician responsibilities
Adverse Drug Reaction reporting , Medication Error reporting
Customer Service Focus
Intervention Documentation
Telephone Courtesy/Etiquette
IV medication administration policy and chart
Meds/Devices brought from home
PCA Pump Policy
DI Resources: Micromedex, Lexi-Comp, Kings, Facts & Comp, Up to Date, Trissell’s, Pubmed
Alaris GuardRails for IV pumps
How to use phone and beeper system
Dashboards (Will do with Blair, Pratish, and Erin ) Orientation Items Resident Initials Trainer Initials Date Reviewed
Warfarin
Aminoglycoside
Heparin
Consults

35

36
VUH PGY1 Pharmacy Resident On-Call and Weekend Staffing Responsibilities On-Call/Drug Information Pager: 835-0687
Kinetics Consult Pager: 831-6560
** PGY1 Pharmacy Residents work on site at VUH every 3rd
weekend. Weekend duties will alternate between Weekend Staffing and Clinical On-Call roles every 3 weeks. Each weekend there will be two residents on site
- one serving in the Weekend Staffing role, and the other in the Clinical On-Call role. **
Definitions: Weekend Staffing Resident— performs operational staffing role
On Call Resident (Clinical on Call)--performs mostly clinical functions (some staffing)
Monday- Friday Saturday, Sunday
7:00 am Weekend Staffing Resident staffs
from 7 am- 3:30 pm.
8:00 am On Call Resident rolls the DI pager to their
personal pager on Monday (24 hrs/day) until
the next Monday at 8 am.
11:30 am On Call Resident assists with clinical
responsibilities from 11:30am-3:30pm (unless transition time is adjusted based on the
clinical workload and on a collaborative
decision made by the lead clinical pharmacist
and the pharmacist in charge in Central)
3:30 pm Fridays:
On Call Resident staffs from 3:30-7 pm
On Call Resident rolls the PK pager to
their personal pager and responds to any
new consults and follows up with any
consults if requested to do so by clinical
specialists.
On Call Resident staffs from 3:30 pm-
7 pm.
4:00pm On Call Resident rolls the PK pager to their
personal pager and responds to any new
consults and follows up with any consults if
requested to do so by clinical specialists.
6:30 pm
11:00 pm See below for specifics

37
VUH Pharmacy PGY1 Resident Weekend Staffing
The weekend staffing responsibilities are meant to provide the resident with longitudinal experience with processing orders,
verifying extemporaneous preparations, answering phone calls, and maintaining effective and efficient work flow. The second half
of the residency year will also incorporate IV Room experience into the weekend staffing responsibilities.
Every 6 weeks, each resident staff in the Pharmacy and perform strictly staffing responsibilities from 7 am to 3:30 pm.
The week following the resident’s staffing weekend, they will receive one half day (4 hours) off on the Monday following
the call weekend. The time off must be taken on Monday or it will be forfeited unless prior approval is received from the
Residency Program Director.
VUH Pharmacy PGY1 Resident Clinical Call
The On-Call Resident (Clinical On-Call) provides a resource to help with pharmacy consults (kinetics, etc.) after regular business
hours and on weekends and also with drug information questions 24/7 for one-week every 6 weeks. When residents are not available
(orientation, Midyear, SERC, etc.) the Backup On-Call Clinical Pharmacist will fill this role.
I. On-Call Resident Role on Weekdays (Monday through Friday)
a. Drug Information: At 8 am on Monday morning of the call week, the on-call resident will roll the Drug Information pager
to their personal pager. Calls should be referred to the responsible patient care area Clinical Pharmacist during business
hours unless the Clinical Pharmacist is off. For all other patient care areas and after hours, the on-call resident will be
available to medical, nursing and pharmacy staff for drug information questions as needed.
1. Drug information questions received when Resident is on-site should receive initial follow-up within 15 minutes
of page being received. When off-site, the Resident should respond for initial follow-up within 30 minutes of the
page being received.
2. The Backup On-Call Pharmacist should be contacted if any issues arise or guidance is needed.
3. All drug information calls should be documented on the drug information documentation form.
b. Consults: The Therapeutic Drug Monitoring (TDM) pharmacist (or designee) will manage consults until 4pm on weekdays.
1. At 4 pm Monday through Thursday, the On-call Resident will roll the consult pager to their personal pager.
2. From 4 pm until 11pm each day, when a page is received for a pharmacokinetics consult, the On-call Resident will
ensure that the patient is appropriately dosed and covered until the next morning, when the TDM pharmacist (or
designee) can address the consult.
3. The Backup On-Call Pharmacist should be contacted if any issues arise or guidance is needed.
c. Dashboards: Residents on specific rotations are generally assigned to certain dashboards. The On-call Resident
occasionally covers dashboards for clinical pharmacists and residents during the week when requested to do so due to lack
of adequate coverage.
II. On-Call Resident Role on Weekends
a. Clinical Responsibilities: From 11:30 am to 3:30 pm, the On-call Resident provides support to the lead clinical pharmacist,
who is responsible for the management of weekend clinical functions. From 3:30 pm to 11 pm, the resident is still
responsible (as on weekdays) for new consults and any levels returning that evening which the clinical lead pharmacist has
asked them to address.
1. Consults:
i. On Friday afternoon the on-call resident will roll the kinetics pager to their personal pager at 3:30 pm.
ii. On Saturday and Sunday, the lead clinical pharmacist should roll the consult pager to their personal pager
from 7 am until 3:30 pm, when it can then be rolled to the on-call resident. The on-call resident will
respond to consults via the kinetics pager from 3:30 pm to 11 pm on Friday, Saturday and Sunday.
iii. The Backup On-Call Pharmacist should be contacted if any issues arise or guidance is needed.

38
2. Dashboards: Weekend dashboard responsibilities include the aminoglycoside, vancomycin and anticoagulation
alerts in the “Weekend” tab of the dashboard. These responsibilities are generally shared between clinical
pharmacists and resident and will be delegated by the lead clinical pharmacist.
3. Drug Information: The On-call Resident will be available to medical, nursing and pharmacy staff for drug
information questions 24/7 as needed.
i. Drug information questions received when Resident is on-site should receive initial follow-up within 15
minutes of page being received. When off-site, the Resident should respond for initial follow-up within
30 minutes of the page being received.
ii. The Backup On-Call Pharmacist should be contacted if any issues arise or guidance is needed.
i. All drug information calls should be documented on the drug information documentation form.
b. Staffing Responsibilities: The on-call resident will transition from clinical to staffing duties from 3:30 pm to 7 pm on
Saturday and Sunday. Based on the clinical workload and on a collaborative decision made by the lead clinical pharmacist
and the pharmacist in charge in Central, the on-call resident may need to remain focused on clinical responsibilities beyond
the 3:30 pm transition time. The Resident will, at a minimum, cover for meal breaks in the Central Pharmacy. After 7 pm,
the resident is free to leave after any remaining dashboards activities are completed.
III. Backup to On-Call Resident Role
The Backup On-Call Pharmacist provides oversight and guidance to the on-call resident when needed. The Backup Clinical
Pharmacist should be readily available to the on-call resident 24/7 during the call week via pager or phone. The Backup On-Call
Pharmacist serves as a preceptor for the on-call function and mentors each resident to the appropriate level that is individualized to
each resident. When residents are not available (orientation, Midyear, resident conferences, etc.), a Clinical Pharmacist will perform
the on-call responsibilities but will not work additional weekends.
IV. Other Key Clinical Call Points
Residents may swap call weeks with each other. The Backup On-Call Pharmacist for the weeks involved and Molly
Knostman should be notified when this occurs.
The on-call resident is not required to come in on unassigned holidays.
Transplant consults and drug information questions should always be directed to or discussed with the respective transplant
pharmacist.
o Liver Transplant: Christie Truscott 615-496-0086
o Renal/Pancreas Transplant: Stefanie Bala 615-587-1340 and TBA
o Heart/Lung Transplant: Jennifer Gray 615-484-3129
o Solid Organ Transplant PGY2 Resident: TBA
If anticoagulation or other consults are received by the on-call resident, they should ensure the patient is appropriately
managed until the next morning, when the inpatient anticoagulation or other pharmacist can address the consult.
From 4 pm to 11 pm (3:30 pm to 11 pm on Friday, Saturday and Sunday), the on-call resident is not responsible for writing
consult notes in StarPanel. They should amend the consult request to acknowledge the consult, note any immediate changes
that are made to the patient’s therapy, and state that pharmacy will be following and a consult note will be written the
following day. If it is an existing consult patient, the on-call resident may need to amend an existing consult note if
requested to do so by a Clinical Pharmacist when following up on that patient after hours for that Clinical Pharmacist.
Pages received from the PREDICT program go to voice mail in the 5-GENE mailbox. To access the voice mail, call 936-
0000 and press the # key. Enter the mailbox # of 54363 and the password of 543631. Messages should be responded to
within 1 business day.
The week following the resident’s call week and weekend, they will receive one half day (4 hours) off on the Monday
following the call weekend. The time off must be taken on Monday or it will be forfeited unless prior approval is received
from the Residency Program Director.
If the on-call resident receives a consult for drugs other than vancomycin, an aminoglycoside, or warfarin, they should
contact the Backup On-Call Pharmacist for advice on how to proceed if they are unsure.