relation between qt rate new physiologically - heart.bmj.com · rickards, norman by pacing-induced...
TRANSCRIPT

Br Heart J 1981; 45: 56-61
Relation between QT interval and heart rate
New design of physiologically adaptive cardiacpacemakerA F RICKARDS, J NORMAN
From The National Heart Hospital, London
SUmmARY The relation between QT interval and heart rate has been studied in a group of patientsundergoing physiological exercise, in a group undergoing atrial pacing without exercise, and in a group
with complete heart block undergoing exercise at a fixed ventricular rate controlled by cardiac pacing.The expected shortening in QT interval during physiological exercise is only in part the result of theintrinsic effect of increased rate, since patients undergoing atrial pacing to comparable rates show only asmall decrease in measured QT interval and patients exercising at fixed rates in heart block exhibit adecreasing QT interval related to the independent atrial rate. QT interval changes appear mainlyto be governed by factors extrinsic to heart rate.
The physiological control of QT interval has been used to construct a cardiac pacemaker whichsenses the interval between the delivered stimulus and the evoked T wave, and uses the stimulus-evoked T wave interval to set the subsequent pacemaker escape interval. Thus physiological controlof cardiac pacing rate, independent of atrial activity, using conventional unipolar lead systems is possible.
The decrease in QT interval which occurs withexercise-induced changes in heart rate has longbeen recognised and has led to the use of formulaewhich correct the measured QT to a basic heartrate. The non-linear relation first described byBazettl has been widely applied to derive this ratecorrected QT interval (QTc) though Bazett himselfpointed out the wide variation in individual subjectsand only a limited amount of post-exercise data wasincluded in his study. We have previously notedthat during diagnostic atrial pacing the observedQT interval appeared to shorten less than duringexercise at comparable heart rates. We have there-fore re-examined the relation between heart rateand QT interval to determine those factors respon-sible for the change in ventricular repolarisationtime.
Patients and methods
EXERCISE IN SINUS RHYTHMA group of 25 patients undergoing a treadmillexercise test was studied to re-evaluate the relationbetween QT interval and heart rate. All subjectswere being investigated for ischaemic heart diseaseand were exercised according to the Bruce protocol.
Twelve lead electrocardiograph recordings weremade at a paper speed of 100 mm/s using aCambridge automatic three-channel recorder com-plying with AHA standards. Recordings were madeat rest, at 90 s intervals during exercise, immediatelyafter exercise, and at 90 s intervals after exerciseuntil the resting heart rate was reached. Measure-ments of rate and QT interval were made from thedirect recordings. Data were excluded if a changein the QRS-T morphology occurred either becauseof artefact, ischaemic changes, conduction defects,or ectopic beats. Data were analysed for the groupas a whole and subdivided into those patientstaking beta-blocking drugs (15) and those on nocardioactive therapy (10). Further analysis of therate-QT relation with increasing rate (exercise) andwith decreasing rate (recovery) was also made.
ATRIAL PACINGSimilar data were obtained from 15 patientsundergoing an atrial pacing stress test duringcardiac catheterisation for the evaluation of chestpain. Simultaneous 12 lead electrocardiograms wererecorded on a Cambridge photographic recorderat the resting rate and during atrial pacing from100 beats per minute (bpm) in increments of
56
on 16 February 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.45.1.56 on 1 January 1981. Dow
nloaded from
QT interval and heart rate
10 bpm until either the maximum rate of 180 bpmwas achieved or the test terminated because ofchest pain or atrioventricular block. A detaileddescription of the atrial pacing procedure has beenpreviously reported by ourselves.2
EXERCISE AT FIXED HEART RATENine patients in complete heart block withVVI (ventricular inhibited) pacemakers set at 70bpm were exercised according to the Bruce protocol.The relation between atrial rate and pacing stimulus-QT interval was measured during exercise andrecovery using the methods described above,except that by definition the paced QRS complex waswide and showed a left bundle-branch blockpattern caused by right ventricular endocardialpacing.
Results
Fig 1 shows the results obtained during exercise forthe patients in sinus rhythm. The data for thegroup as a whole indicate that the rate-QT intervalrelation can be approximated by a linear regressionequation such that QT interval is predicted byQT = 522 - 1 87 x RATE. Thus a rate changeof 100 bpm would be accompanied by a change inQT interval of approximately 187 ms. Subdivisionof patients on and off beta-blocking agents indicatesthat though the resting and attained rates arenecessarily lower for those patients on beta-blockers there is no change in the rate-QT relation.The QT interval does not exhibit hysteresis in
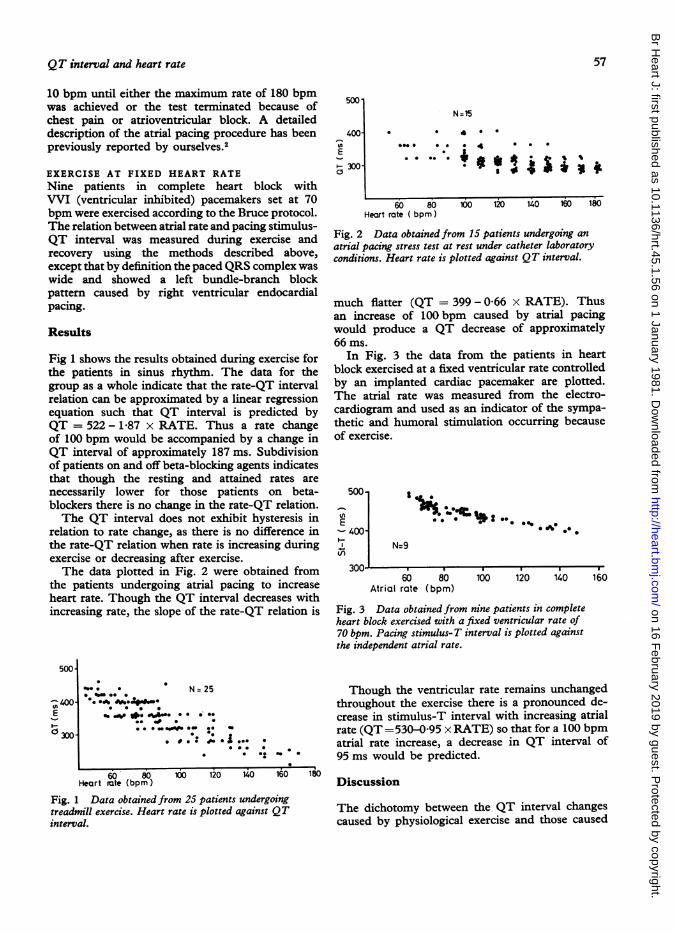
relation to rate change, as there is no difference inthe rate-QT relation when rate is increasing duringexercise or decreasing after exercise.The data plotted in Fig. 2 were obtained from
the patients undergoing atrial pacing to increaseheart rate. Though the QT interval decreases withincreasing rate, the slope of the rate-QT relation is
500
-, 400E1-
c: 300
*.. 0 N= 25*0 0@. 0
0S~00~*g 0 1.00 0 * 0
_ *-*0 *. .S *.00
*** . *" ~*j.*0 *-
60 80 100 120 140 160 180Heart iate (bpm)
Fig. 1 Data obtained from 25 patients undergoingtreadmill exercise. Heart rate is plotted against QTinterval.
500'
400-
E
~- 300-0
N=15
0 0 4 0 0
.-4-* * 4 * *
*-* * * e *I $I * it it
60 80 100Heart rate ( bpm)
120 140 160 180
Fig. 2 Data obtained from 15 patients undergoing anatrial pacing stress test at rest under catheter laboratoryconditions. Heart rate is plotted against QT interval.
much flatter (QT = 399 - 0-66 x RATE). Thusan increase of 100 bpm caused by atrial pacingwould produce a QT decrease of approximately66 ms.
In Fig. 3 the data from the patients in heartblock exercised at a fixed ventricular rate controlledby an implanted cardiac pacemaker are plotted.The atrial rate was measured from the electro-cardiogram and used as an indicator of the sympa-thetic and humoral stimulation occurring becauseof exercise.
5001
E-4001-IV)
300-_
A
0% 00
N=9
60 80ktrial rate (bpm)
100 120 140 160
Fig. 3 Data obtained from nine patients in completeheart block exercised with a fixed ventricular rate of70 bpm. Pacing stimulus-T interval is plotted againstthe independent atrial rate.
Though the ventricular rate remains unchangedthroughout the exercise there is a pronounced de-crease in stimulus-T interval with increasing atrialrate (QT =530Q0495 x RATE) so that for a 100 bpmatrial rate increase, a decrease in QT interval of95 ms would be predicted.
Discussion
The dichotomy between the QT interval changescaused by physiological exercise and those caused
! _
57
on 16 February 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.45.1.56 on 1 January 1981. Dow
nloaded from
Rickards, Norman
by pacing-induced changes in heart rate has beenpreviously described by ourselves.3We have suggested that the sensitivity of the
sinus node in the sick sinus syndrome might bedetermined by examining the relation betweensinus rate and QT interval on exercise.A recent publication from Milne et al.4 studying
the changes in QT interval induced by propranololat fixed atrial pacing rates confirms that the QTinterval is not only dependent on rate but is alsodependent on the change in catecholamine sensitivityof the heart induced by propranolol.
Observations on isolated mammalian cardiacmuscle5 confirm that catecholamines enhance therate of relaxation independent of rate, but addition-ally a purely rate-dependent abbreviation of theaction potential has also been demonstrated.6 7Both of these effects are responsible for the abbrevia-tion of systole necessary in the mammalian heartat high rates to maintain adequate diastolic filling.The results from the atrial pacing study here
described indicate that the intact heart does showsome sensitivity of repolarisation time to rate, butof a smaller magnitude than during physiologicalexercise.From the data obtained when exercising patients
in heart block it is apparent that stimulus-Tinterval is shortening independent of heart rateand therefore presumably as a result of the effectsof circulating catecholamines, as there is effectivelyno direct communication between the autonomicnervous system and the ventricular myocardium.The maintenance of the normal relation between QTinterval and rate during exercise under the influenceof propranolol implies that the effect of propranololin blocking the sinus response to circulatingcatecholamines is accompanied by a similar blockingof the effect of circulating catecholamines onrepolarisation time of the ventricular myocardium.
St
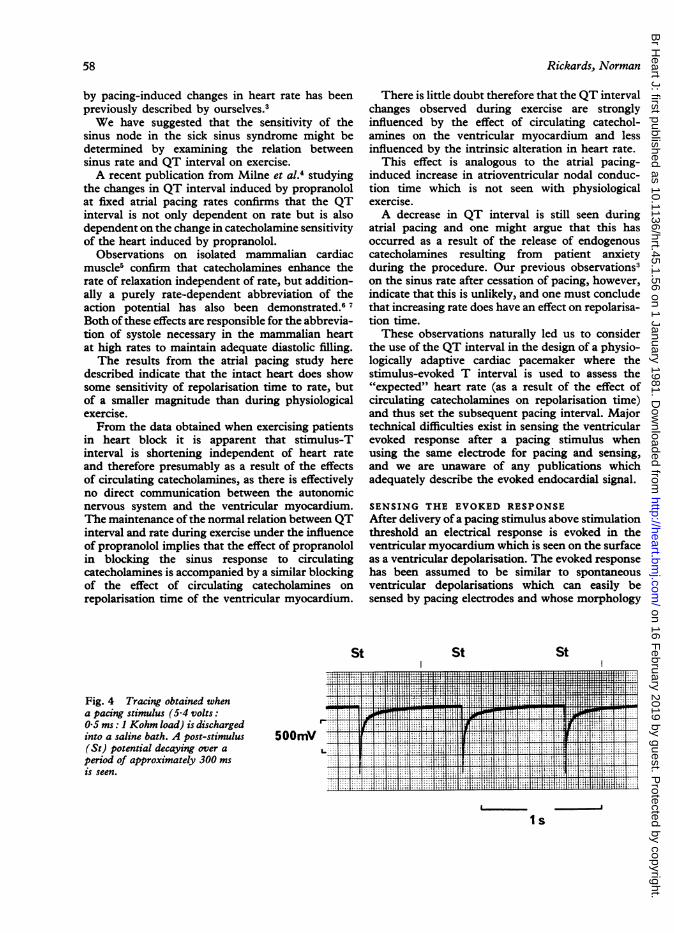
Fig. 4 Tracing obtained whena pacing stimulus (5 4 volts:0 5 ms: 1 Kohm load) is dischargedinto a saline bath. A post-stimulus(St) potential decaying over aperiod of approximately 300 msis seen.
500mV
There is little doubt therefore that the QT intervalchanges observed during exercise are stronglyinfluenced by the effect of circulating catechol-amines on the ventricular myocardium and lessinfluenced by the intrinsic alteration in heart rate.
This effect is analogous to the atrial pacing-induced increase in atrioventricular nodal conduc-tion time which is not seen with physiologicalexercise.A decrease in QT interval is still seen during
atrial pacing and one might argue that this hasoccurred as a result of the release of endogenouscatecholamines resulting from patient anxietyduring the procedure. Our previous observations3on the sinus rate after cessation of pacing, however,indicate that this is unlikely, and one must concludethat increasing rate does have an effect on repolarisa-tion time.These observations naturally led us to consider
the use of the QT interval in the design of a physio-logically adaptive cardiac pacemaker where thestimulus-evoked T interval is used to assess the"expected" heart rate (as a result of the effect ofcirculating catecholamines on repolarisation time)and thus set the subsequent pacing interval. Majortechnical difficulties exist in sensing the ventricularevoked response after a pacing stimulus whenusing the same electrode for pacing and sensing,and we are unaware of any publications whichadequately describe the evoked endocardial signal.
SENSING THE EVOKED RESPONSEAfter delivery of a pacing stimulus above stimulationthreshold an electrical response is evoked in theventricular myocardium which is seen on the surfaceas a ventricular depolarisation. The evoked responsehas been assumed to be similar to spontaneousventricular depolarisations which can easily besensed by pacing electrodes and whose morphology
St St
_ !: ~~~~~T.. _,77 [ ig3W:Xa.~~~~~~~~~~~~~~~~~~~~~. ..-.X.Il..... i ,Im_.....
,... .... ... . .. .!4.*X. *' t£ 3it{55 ||t
X-L"' f i-'-4pitl5isilil lii 'l5 3.1353¢1 | | 3 W---4
t3i4,~.
I s
58
on 16 February 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.45.1.56 on 1 January 1981. Dow
nloaded from

QT interval and heart rate
has been well documented and has formed the basisfor the design of sensing circuits in non-competitiveventricular pacemakers.A typical pacing pulse delivers in excess of 5 volts
for a time of 0 5 ms into a load of 500 ohms. Thisstimulus produces polarisation effects at the inter-faces between the electrodes and tissue such thatafter the termination of the pacing pulse itself adecaying voltage exists between cathode and anodeof opposite polarity to the pacing stimulus and of amagnitude and time course depending on theenergy delivered, the materials employed as cathodeand anode, and the surface area of contact betweenthe electrodes and tissue.
Furthermore, most pacemaker output circuits arecapacitor coupled in such a way that the capacitordischarges across the electrodes after chargingduring the pacing pulse.The summation of these effects is shown in
Fig. 4 where a conventional pacemaker and electrodelead system was discharged into a saline bath. Thesignal measured directly from the electrode leadshows a large potential opposite in polarity to thepacing stimulus with a magnitude of hundredsof millivolts and decaying over a period of morethan 300 ms.
It is not surprising therefore that it has provedtechnically difficult to isolate an evoked response of
the order of a few millivolts in magnitude from thepost-stimulus period. Conventional pulse generatorsuse absolute refractory periods of the order of300 to 350 ms to avoid the polarisation and capacitordischarge effects created at the electrode/heartinterface before enabling spontaneous beat sensing.
Preston and Bowers8 in 1973 reported the designof a threshold tracking system which sensed theevoked response within 50 ms of the pacing stimulusand delivered a backup pacing pulse of higherenergy if the initial pulse failed to capture the heart.No recordings of the evoked response were demon-strated and subsequent development of this conceptwas limited by the reliability with which the evokedresponse could be sensed. Mugica et al.9 in 1973used an independent intracardiac electrode to sensethe evoked response when pacing and came to therather surprising conclusion that evoked responsesof the order of 500 to 800 millivolts were present25 to 90 ms after the pacing pulse.
In 1978 we first developed a pacing input/outputcircuit which was capable of allowing direct re-cordings of the cardiac evoked response from aconventional electrode lead system. The system hasbeen refined in collaboration with a commercialorganisation* and depends on a modified pulsewaveform and automatic postpulse compensation to* Vitatron Medical BV, Dieren, The Netherlands.
I .
II / I'
III ,
'---- -X - - - -
RA
LEAD ~ ~g-1.--'N/5
LEAD~~ ~ ~ |u.nBnnmen . . s _. wn||~~~~~~~~~~~~~~~~~--1
Fig. 5 A recording from a patient in complete heart block paced at 70 bpm. I, II, III = scalar leads. RA, bipolaratrial electrogram showing independent atrial activity. LEAD, recording from a chronically implanted unipolar lead(Vitatron Helifix) using a stainless steel indifferent electrode in the supramammary pacemaker site. Current, 6-5 mAat 0-5 ms. Note the negative evoked QRS complex followed by a positive T wave. The arrow indicates the point atwhich the current was reduced to below stimulation threshold and shows the absence of an evoked response.
59
on 16 February 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.45.1.56 on 1 January 1981. Dow
nloaded from

Rickards, Norman
eliminate polarisation and discharge effects. Thissystem is capable of sensing the evoked responsewithin 5 ms of the pacing pulse delivered across aconventional unipolar lead system and has a trulyDC response, so that the evoked response is seenunaffected by any form of filtering. The outputcircuit has been incorporated into an externalventricular demand pulse generator.
Fig. 5 shows a recording made of the evokedresponse using this system. The evoked response isseen as a negative QRS complex which reaches amaximum amplitude approximately 45 ms afterthe pacing pulse and is followed by a clearly definedpositive T wave. Both QRS and T wave durationtend to be shorter than those observed on thesurface electrocardiogram but are of higher ampli-tude than spontaneous complexes sensed by thepacing lead. The Table details observations on theQRS and T durations and amplitudes made in agroup of 12 patients studied at pacemaker implanta-tion or pulse generator change.Both QRS and T wave polarity depend on the
sensing dipole. Thus, a positive T wave is sensed bya unipolar endocardial electrode, but the T wavebecomes negative if a bipolar endocardial or aunipolar epicardial lead system is used.
ALTERATION OF PACING RATE AS FUNCTIONOF STIMULUS-T INTERVALThe pacing system has been further refined toincorporate measurement of the peak of the evokedT wave and to use the stimulus-evoked T interval todetermine the subsequent pacing rate. The relation
Table Measurements made of timing and amplitudes ofevoked response in 12 patients at time of pacemakerimplantation or pulse generator change
A A A
Case St-QRS QRS QRSD St-T T St-TWo. (ms) (mV) (ms) (ms) (mV) (ms)
1 38 -23 160 360 3-2 4402 60 -12 5 170 385 3 0 4603 44 -16 180 308 7 0 4304' -22-4 180 250 3 2 4105 42 -14-7 160 280 88 4106 45 -11 5 150 290 7 5 4457 45 -14 155 280 12-0 4108 44 -18 9 150 280 7-8 3909 55 -15 200 320 8 8 42510 40 -13 180 270 5 0 38011 36 -21*7 160 250 13 0 35012 40 -10-0 150 285 5 0 405
R 44-5 -16 1 166 297 7-0 413SD 7 2 - 44 16 41 3-3 30
St-QRS = time from pacing stimulus to peak QRS.QR, = peak QRS amplitude. QRSD = QRS dujgation.St-T = time from stimulus to peak of T wave. T = peak Twave amplitude. St-T = time from stimulus to end of T wave.
X = mean values. SD = standard deviation of mean.
0 900 ...E . ,7- 800
a# 700.-
a.a.
E 870
> 830-'C 790-
,,- 750
2Time (min)
4 6 8
Fig. 6 A plot of PP interval and stimulus-stimulus interval against time in a patient with completeheart block. Each point represents a 6 s rate average.The arrows indicate the intravenous injection of 2 Vgisoprenaline. Pacing rate-stimulus T sensitivity was setat 0 4 beats/ms. Note the increase in atrial rate(decrease in PP interval) which reaches a maximumapproximately 90 s after isoprenaline. The pacing systemresponds to the decreasing stimulus-evoked T intervaland increases rate (decreasing St-St interval) to amaximum approximately one minute after the peak atrialresponse. Both atrial and pacemaker responses arecomplete at five minutes and the isoprenaline challengethen repeated.
between the stimulus-T interval and pacing rate isadjustable so that a decrease in stimulus-T intervalof say 10 ms would be accompanied by an increasein pacing rate of 10 bpm if the sensitivity of thesystem is set to 1 beat/ms. Such a system has theadvantage that pacing rate can be determined as afunction mainly of the physiological demands of thebody resulting from the effect of circulatingcatecholamines, while using conventional unipolarelectrode lead systems.The pacing rates of atrial, ventricular, or atrio-
ventricular pacemakers can be altered physio-logically independent of atrial activity and therequirement to sense the atrial electrogram.
Fig. 6 shows data obtained from a patient incomplete heart block studied at the time of pulsegenerator change. The atrial rate was determinedfrom a bipolar atrial electrode and changes in atrialrate and stimulus-T interval were produced byintravenous injections of 2 ,ug isoprenaline.
Alterations in the pacing rate can be seen tofollow stimulation with isoprenaline. The effect ofisoprenaline on the stimulus-T interval andsubsequent increase in pacing rate is delayed by
60
-
4- 0 . .. . 0
.. . . 0 .
on 16 February 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.45.1.56 on 1 January 1981. Dow
nloaded from

QT interval and heart rate
about one minute in relation to the effect on sinusrate, but an increase in pacing rate as a result ofisoprenaline with recovery over a period of fiveminutes is clearly shown and is reproducible.
Conclusions
Data are presented which show that the decrease inQT interval seen during exercise occurs notprimarily as a result of an increase in heart rate butmainly results from the effects of circulatingcatecholamines which accompany exercise. Thissensitivity of the repolarisation of the ventricularmyocardium has been used to design a pacingsystem which offers the advantage of physiologicalcontrol of pacing rate, independent of atrial activity,using conventional endocardial electrode leadsystems.
The authors wish to express their thanks to VitatronMedical BV and especially to Mr A C M Renirieand Mr F H M Wittkampf for help in the develop-ment of this concept.
References
1 Bazett Hcg. An analysis of the time-relations of
electrocardiograms. Heart 1920; 7: 353-70.
2 Rickards AF, Seabra-Gomes R. Observations on theeffect of angina on the left ventricle with specialreference to diastolic behaviour. Eur J Cardiol 1978;7, suppl: 213-38.
3 Rickards AF, Akhras F, Baron DW. Effects of heartrate on QT interval (abstract). In: Meere C, ed.Proceedings of the VI world symposium on cardiacpacing. Montreal: Laplante & Langevin, 1979; 2: 7.
4 Milne JR, Camm AJ, Ward DE, Spurrell RAJ.Effect of intravenous propranolol on QT interval. Anew method of assessment. Br Heart J 1980; 43: 1-6.
5 Morad M, Rolett E. Relaxing effects of catechol-amines on mammalian heart. J Physiol 1972; 224:537-58.
6 Hoffman BF, Cranefield P. Electrophysiology of theheart. New York: McGraw-Hill, 1960.
7 Boyett MR, Jewell BR. A study of the factorsresponsible for rate-dependent shortening of theaction potential in mammalian ventricular muscle.J Physiol 1978; 285: 359-80.
8 Preston TA, Bowers DL. Report of a continuousthreshold tracing system. In: Thalen HJTh, ed.Cardiac pacing. Assen: Van Gorcum, 1973: 295-9.
9 Mugica J, Lazarus B, Buffet J, Catte M. Pacemakerwith automatic adaptation to the pacing threshold. In:Thalen HJTh, ed. Cardiac pacing. Assen: VanGorcum, 1973: 150-5.
Requests for reprints to Dr Anthony Rickards, TheNational Heart Hospital, Westmoreland Street,London WlM 8BA.
61
on 16 February 2019 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.45.1.56 on 1 January 1981. Dow
nloaded from