regional anesthesia and elderly - paws
TRANSCRIPT

C
Pain management in the elderly
and cognitively impaired patient:the role of regional anesthesia and analgesiaThomas M. Halaszynski
Department of Anesthesiology, Yale University Schoolof Medicine, New Haven, Connecticut, USA
Correspondence to Thomas M. Halaszynski,Department of Anesthesiology, Yale University Schoolof Medicine, 333 Cedar Street, New Haven, CT 06525,USATel: +1 203 785 2802; fax: +1 203 785 6664;e-mail: [email protected]
Current Opinion in Anaesthesiology 2009,22:594–599
Purpose of review
To review the rational for use of the many regional anesthetic/analgesic techniques and
acute pain management modalities in the elderly and cognitively impaired high-risk
patients, as increasing numbers of older adults are presenting for surgery.
Recent findings
There are numerous studies examining short and long-term consequences of regional
anesthesia/analgesia along with identification of the many potential advantages, but
those studying the influence and potential benefits in elderly and cognitively impaired
patients are only beginning to be developed as issues related to cognitive dysfunction
associated with surgery/anesthesia are beginning to be observed.
Summary
Pain management therapy, including regional anesthesia, along with multimodal
analgesia may help reduce the risk of negative influences in the elderly patient along with
reducing postoperative delirium and cognitive dysfunction. Improvements in analgesic
efficacy with regional anesthesia may attenuate pathophysiological surgical responses,
reduce the length of hospitalization, and accelerate patient rehabilitation and recovery.
Analgesic techniques that provide optimal pain control and low side effect profiles with
minimal opioid exposure should always be considered for elderly high-risk and
cognitively impaired patients.
Keywords
cognitively impaired, elderly/high-risk patient, neuraxial anesthesia, peripheral nerve
blocks, regional anesthesia
Curr Opin Anaesthesiol 22:594–599� 2009 Wolters Kluwer Health | Lippincott Williams & Wilkins0952-7907
Introduction
Over the past century, remarkable achievements in medi-
cine and public health have made it possible for people to
live longer with more productive life spans. For this
reason, physicians can expect to spend a significantly
larger portion of their practice dealing with disease man-
agement and operative procedures in older adults [1]. Yet,
despite advances in anesthesia, analgesia, and drug deliv-
ery systems, the debate continues as to whether neural
blockade and regional anesthesia/analgesia is more effi-
cacious and safer in elderly patients, particularly those
with co-morbidities and cognitive deficits. This article
will touch upon the physiological and pharmacological
implications of aging on surgical anesthesia and pain
management and focus on the potential benefits of
regional anesthesia/analgesia in geriatric and cognitively
impaired patients. Nevertheless, it is the lack of consist-
ency within regional anesthesia/analgesia studies that
has prevented firm recommendations, indications, and
guidelines, about which techniques offer the greatest
advantage for elderly and cognitively impaired patients
opyright © Lippincott Williams & Wilkins. Unautho
0952-7907 � 2009 Wolters Kluwer Health | Lippincott Williams & Wilkins
undergoing particular surgical procedures, but an oppor-
tunity exists to recommend a tailored perioperative pain
management plan focused on minimizing risk.
Physiologic function during agingOptimal anesthetic management of elderly patients
depends on knowledge and understanding of normal
age-related changes in anatomy, physiology, and response
to pharmacological agents. It is also important to dis-
tinguish between normal physiological alterations of
the nervous, cardiovascular, and hepato-renal systems
and disease-related pathophysiological changes. A general
approach to optimize perioperative pain management in
geriatric patients is to consider postoperative compli-
cations commonly associated with routine surgical pro-
cedures and to assess any potential benefits associated with
regional anesthesia/analgesia. Neurologic, pulmonary, and
cardiovascular complications are among the most common
observed in the elderly persons and occur most frequently
in orthopedic and general surgical settings. There are both
established and theoretical indications supporting the
rized reproduction of this article is prohibited.
DOI:10.1097/ACO.0b013e32833020dc
C
Pain management in the elderly Halaszynski 595
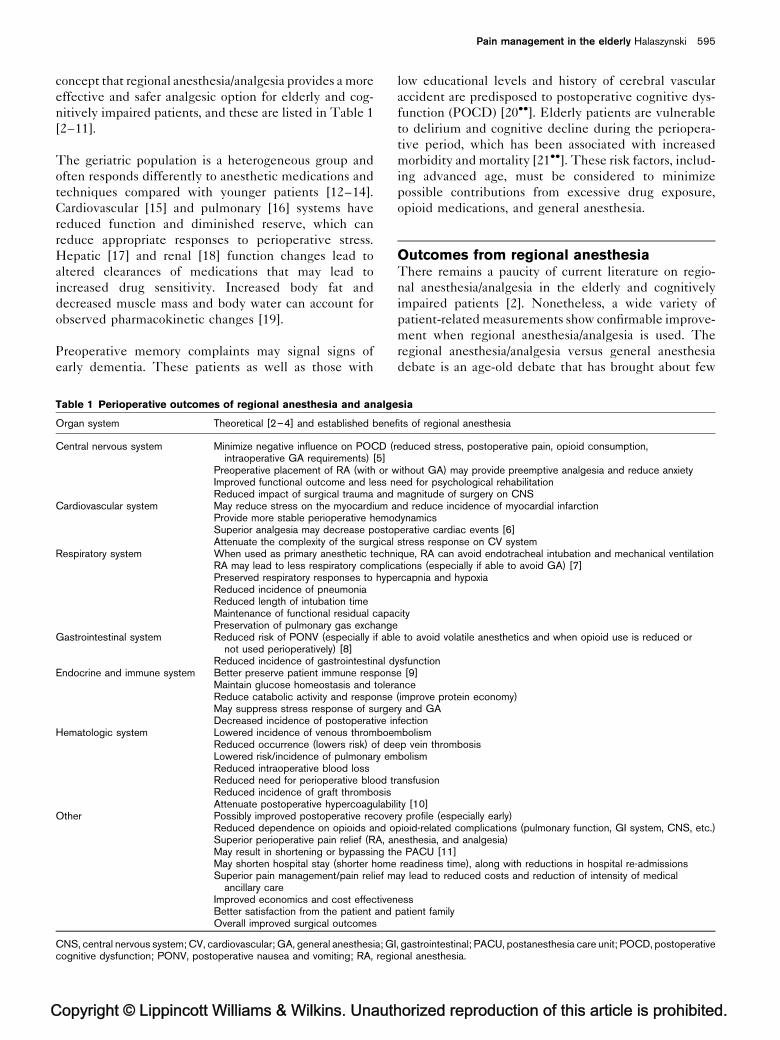
concept that regional anesthesia/analgesia provides a more
effective and safer analgesic option for elderly and cog-
nitively impaired patients, and these are listed in Table 1
[2–11].
The geriatric population is a heterogeneous group and
often responds differently to anesthetic medications and
techniques compared with younger patients [12–14].
Cardiovascular [15] and pulmonary [16] systems have
reduced function and diminished reserve, which can
reduce appropriate responses to perioperative stress.
Hepatic [17] and renal [18] function changes lead to
altered clearances of medications that may lead to
increased drug sensitivity. Increased body fat and
decreased muscle mass and body water can account for
observed pharmacokinetic changes [19].
Preoperative memory complaints may signal signs of
early dementia. These patients as well as those with
opyright © Lippincott Williams & Wilkins. Unauth
Table 1 Perioperative outcomes of regional anesthesia and analge
Organ system Theoretical [2–4] and established bene
Central nervous system Minimize negative influence on POCD (rintraoperative GA requirements) [5]
Preoperative placement of RA (with or wImproved functional outcome and less nReduced impact of surgical trauma and
Cardiovascular system May reduce stress on the myocardium aProvide more stable perioperative hemoSuperior analgesia may decrease postoAttenuate the complexity of the surgical
Respiratory system When used as primary anesthetic technRA may lead to less respiratory complicPreserved respiratory responses to hypeReduced incidence of pneumoniaReduced length of intubation timeMaintenance of functional residual capaPreservation of pulmonary gas exchange
Gastrointestinal system Reduced risk of PONV (especially if ablnot used perioperatively) [8]
Reduced incidence of gastrointestinal dEndocrine and immune system Better preserve patient immune respons
Maintain glucose homeostasis and tolerReduce catabolic activity and responseMay suppress stress response of surgeDecreased incidence of postoperative in
Hematologic system Lowered incidence of venous thromboeReduced occurrence (lowers risk) of deLowered risk/incidence of pulmonary emReduced intraoperative blood lossReduced need for perioperative blood trReduced incidence of graft thrombosisAttenuate postoperative hypercoagulabi
Other Possibly improved postoperative recoveReduced dependence on opioids and oSuperior perioperative pain relief (RA, anMay result in shortening or bypassing thMay shorten hospital stay (shorter homeSuperior pain management/pain relief m
ancillary careImproved economics and cost effectivenBetter satisfaction from the patient andOverall improved surgical outcomes
CNS, central nervous system; CV, cardiovascular; GA, general anesthesia; Gcognitive dysfunction; PONV, postoperative nausea and vomiting; RA, regio
low educational levels and history of cerebral vascular
accident are predisposed to postoperative cognitive dys-
function (POCD) [20��]. Elderly patients are vulnerable
to delirium and cognitive decline during the periopera-
tive period, which has been associated with increased
morbidity and mortality [21��]. These risk factors, includ-
ing advanced age, must be considered to minimize
possible contributions from excessive drug exposure,
opioid medications, and general anesthesia.
Outcomes from regional anesthesiaThere remains a paucity of current literature on regio-
nal anesthesia/analgesia in the elderly and cognitively
impaired patients [2]. Nonetheless, a wide variety of
patient-related measurements show confirmable improve-
ment when regional anesthesia/analgesia is used. The
regional anesthesia/analgesia versus general anesthesia
debate is an age-old debate that has brought about few
orized reproduction of this article is prohibited.
sia
fits of regional anesthesia
educed stress, postoperative pain, opioid consumption,
ithout GA) may provide preemptive analgesia and reduce anxietyeed for psychological rehabilitationmagnitude of surgery on CNSnd reduce incidence of myocardial infarctiondynamicsperative cardiac events [6]stress response on CV systemique, RA can avoid endotracheal intubation and mechanical ventilationations (especially if able to avoid GA) [7]rcapnia and hypoxia
city
e to avoid volatile anesthetics and when opioid use is reduced or
ysfunctione [9]ance(improve protein economy)ry and GAfection
mbolismep vein thrombosisbolism
ansfusion
lity [10]ry profile (especially early)pioid-related complications (pulmonary function, GI system, CNS, etc.)esthesia, and analgesia)e PACU [11]readiness time), along with reductions in hospital re-admissions
ay lead to reduced costs and reduction of intensity of medical
esspatient family
I, gastrointestinal; PACU, postanesthesia care unit; POCD, postoperativenal anesthesia.

C
596 Pain medicine
clear answers, as most concur that multiple factors includ-
ing the patient, the surgery, the method of regional
anesthesia/analgesia and general anesthesia, and the
quality of perioperative care, all influence surgical out-
come. In an age of evidence-based medicine, the current
heterogeneous data available need to be reconciled with
advances in perioperative care and decipher the compli-
cations associated with the surgical process as a whole [22].
Regional anesthesia/analgesia is associated with superior
analgesia, is site-specific, can be long lasting (e.g., cathe-
ter placement) and effective. Surgical patient treatment
with an emphasis on outpatient surgery, improved patient
satisfaction and quality of care, healthcare cost contain-
ment, and shorter hospital stays with improved patient
outcomes are all benefits of improved perioperative pain
management. A focus on these goals provides good reason
for cause and reevaluation of anesthetic options, includ-
ing regional anesthesia/analgesia, during the periopera-
tive period.
Influences of numerous details including postoperative
length of hospital stay, unplanned hospital admissions
and hospital readmissions, and health-related quality of
life need to be evaluated in addition to the more com-
monly investigated parameters of major morbidity and
mortality. These issues maintain a correlation with the
incidence of surgical and anesthetic complications and
may be positively influenced by regional anesthesia/
analgesia through reduction or elimination of postopera-
tive pain, postoperative nausea and vomiting (PONV),
drowsiness, and cognitive dysfunction.
Regional anesthesia/analgesia may facilitate a ‘fast-track-
ing’ process and expedite a patient’s hospital course.
Patients may have reduced recovery room stays or com-
pletely bypass the phase 1 recovery unit. In addition, time-
to-home readiness and hospital discharge would permit
patients to resume their preoperative functional level more
quickly along with reduced exposures to the risky institu-
tional environment. These details add up to permit the
elderly and cognitively impaired patients reduced disrup-
tions and fastidious return to preoperative status, which
theoretically can reduce degrees of morbidity.
Postoperative painPostoperative pain continues to be one of the most
commonly reported complications of surgery. A large-
scale retrospective study by McGrath et al. [23] has
demonstrated that general, neurological, and orthopedic
surgeries had significantly higher pain levels postopera-
tively. The ability to provide pain management after
surgery has become a limiting factor in determining types
of procedures that can be performed in the ambulatory
center, and severe postoperative pain is associated with a
opyright © Lippincott Williams & Wilkins. Unautho
higher rate of unanticipated hospital admission, pro-
longed length of hospital stay, potential for developing
chronic pain conditions, and exacerbation of chronic pain
states [24�].
Pain management is essential and regional anesthesia/
analgesia provides excellent and prolonged postoperative
analgesia that provides quicker and more comfortable
patient mobility, decreases opioid requirements, facili-
tates participation in physical therapy, and expedites
return-to-normal activities [25,26��]. These character-
istics may result in faster recovery and improved
perioperative outcomes with increased patient and
patient family satisfaction. A combination of regimens
with regional anesthesia/analgesia as the foundation of
a multimodal approach can facilitate goals of optimal
analgesia, faster recovery, enhanced functional outcome,
and improved quality of life [27,28�].
Postoperative cognitive dysfunctionPOCD is a complication after both cardiac and noncardiac
surgery in the elderly patients, yet the mechanisms are
poorly understood [29�]. There remains an underlying
assumption that a decrease in the stress response, opioid
consumption [30�], and postoperative pain provided by
regional anesthesia/analgesia would lead to a reduction in
the incidence of POCD. Effects of neuraxial blockade on
cognitive function have been studied and analyzed eval-
uating neuraxial anesthesia versus general anesthesia on
POCD [31], but there are no randomized, blinded studies
comparing effects of peripheral nerve blocks versus gen-
eral anesthesia on POCD.
The high incidence of POCD in elderly patients raises
concern due to the significant negative impact and influ-
ence on quality of life [32], and regional anesthesia/analge-
sia may be beneficial in this patient population. Significant
sleep impairment and postoperative sleep disturbances
can present in patients with higher levels of pain and
can result in a more prolonged and difficult recovery
[33], which may be reduced in the setting of regional
anesthesia/analgesia. Pain may not be the only cause of
sleep disturbances as other factors may contribute, such as
inhalation agents, opioids, increased age, surgical stress,
and environmental factors, of which many could be mini-
mized by using regional anesthesia/analgesia. Indepen-
dent of the cause(s), sleep impairment may result in
decreased health-related life quality and postoperative
functional levels, increased postoperative fatigue, and
POCD. Regional anesthesia/analgesia may improve the
quality of postoperative sleep by reducing surgical stress
and opioid requirement along with superior analgesia.
The ability to resume normal daily activities equivalent
to preoperative levels remains a relevant postoperative
rized reproduction of this article is prohibited.

C
Pain management in the elderly Halaszynski 597
outcome and one devoid of POCD, impaired functional
status, and morbidity [34��]. Numerous symptoms and
complications after surgery may potentially impede
resumption of normal daily activities and negatively
influence functional capacity, leading to a longer time
to recommence return to preoperative functional status
[35]. Regional anesthesia/analgesia and optimal analgesia
permit patients to achieve early mobilization along with
earlier full participation and more benefit from physical
therapy yielding better range of motion and less joint
stiffness resulting in better functional results. Regional
anesthesia/analgesia techniques provide pain relief, thus
sparing the sedative effects of opioids facilitating faster
convalescence, early mobilization, and return to preo-
perative functional levels [36��].
Benefits from regional anesthesia/analgesia compared
with the negative influences associated with general
anesthesia have demonstrated that regional anesthesia/
analgesia provides superior pain relief and early return to
preoperative functional levels [37,38�]. In addition, post-
operative fatigue is distressing and unpleasant, often
decreasing the ability to return to preoperative functional
levels, inability to perform activities of daily living,
impact on quality of life, and creation of added stress
for patients. Postoperative fatigue can affect all patients,
may become prolonged postoperatively, or remain a
persistent problem. Possible causes of fatigue include
surgical stress, opioid use, general anesthesia, inflamma-
tory and negative endocrine responses, de-conditioning
of cardiac and pulmonary systems, nutritional deficiency
and immobilization to identify some, many of which
could be positively influenced by regional anesthesia/
analgesia [39,40,41��]. Regional anesthesia/analgesia may
alter the influence and course of postoperative fatigue by
providing superior analgesia, enhanced postoperative
sleep, early and more active mobilization with the aim
of returning to preoperative functional levels [40].
Pulmonary morbidityPostoperative pulmonary dysfunction can be significant
after upper abdominal and thoracic surgery. Regional
anesthesia/analgesia can significantly decrease the
incidence of pulmonary morbidity and provide effective
analgesia that would facilitate proper pulmonary function
and improve respiratory therapy [42��]. Pain and opioid
therapy can impair normal pulmonary function and regio-
nal anesthesia/analgesia techniques may prevent atelec-
tasis, hypoxia, and pulmonary infection by permitting deep
breathing, full chest expansion, and coughing [43��].
Cardiovascular morbidityPostoperative cardiac complications remain a concern for
patients undergoing surgery and the risk factors always
opyright © Lippincott Williams & Wilkins. Unauth
need to be considered. Studies suggest that postoperative
pain management using regional anesthesia/analgesia
techniques compared with systemic opioids may decrease
the incidence of cardiac events through superior post-
operative analgesia [6,22,31,44]. In addition, regional
anesthesia/analgesia can attenuate hypercoagulability,
reduce perioperative blood loss, and minimize or eliminate
surgical stress leading to improved cardiac outcomes.
Controversial results from studies suggest debatable con-
clusions regarding anesthetic types and direct cardiac
influences for surgery in elderly patients [45]. A host of
conflicting results and study design flaws may help to
explain, but intuitively, the pooled known advantages of
regional anesthesia/analgesia must be considered in the
multimodal approach to pain management and elderly
patient care. There are a variety of morphological and
functional changes in the cardiovascular system with
aging that have important clinical implications for the
treatment of elderly surgical patients toward consider-
ations of postoperative pain management with regional
anesthesia/analgesia.
Surgical stress responses can precipitate a hypercoagulable
state and lead to deep vein thrombosis formation and
pulmonary embolism after vascular and orthopedic sur-
geries. These events are causes of cardiovascular disability
and death, but regional anesthesia/analgesia can prevent
hypercoagulability and decrease vascular thrombosis [46].
ConclusionRegional anesthesia/analgesia provides highly effective,
intense, and site-specific anesthesia/analgesia, often with-
out or with fewer side effects than most other analgesic
techniques, including parenteral opioids. Additionally, the
return to important preoperative functional status such as
eating and drinking, ambulating, and resuming proper
sleep may be enhanced. As a result, concentration diffi-
culties, sedation, PONV, negative cognitive influence,
disruption of routine daily living activities, and post-
operative immune dysfunction may be minimized
when regional anesthesia/analgesia is used in appropriate
surgical settings. These advantages may further facili-
tate prompt discharge and earlier recovery resulting in
savings in medical care cost along with high patient and
patient family satisfaction.
There is extensive literature on the use of both neuraxial
and peripheral nerve blocks for perioperative pain man-
agement. The discussions on the studies and reviews
speak on the many advantages of the individual blocks,
but lack focus related specifically to the elderly and
cognitively impaired patient. The beneficial analgesic
effects of regional anesthesia continue to expand and
are well demonstrated, although additional research
orized reproduction of this article is prohibited.
C
598 Pain medicine
showing improved elderly and cognitively impaired
patient outcomes and impetus for the expanded use of
regional anesthesia/analgesia remain necessary.
References and recommended readingPapers of particular interest, published within the annual period of review, havebeen highlighted as:� of special interest�� of outstanding interest
Additional references related to this topic can also be found in the CurrentWorld Literature section in this issue (pp. 689–690).
1 Administration of Aging. A profile of older Americans. Washington DC:Department of Health and Human Services; 2000.
2 Tsui BC, Wagner A, Finucane B. Regional anesthesia in the elderly: a clinicalguide. Drugs Aging 2004; 21:895–910.
3 Moraca RJ, Sheldon DG, Thirby RC. The role of epidural anesthesia analgesiain surgical practice. Ann Surg 2003; 238:663–673.
4 Wu CL, Fleisher LA. Outcomes research in regional anesthesia and analgesia.Anesth Analg 2000; 91:1232–1242.
5 Rasmussen LS, Johnson T, Kuipers HM, et al. Does anesthesia cause post-operative cognitive dysfunction? A randomized study of regional versusgeneral anesthesia in 438 elderly patients. Acta Anaesthesiol Scand2003; 47:260–266.
6 Yeager MP, Glass DD, Neff RK, Brinck-Johnson T. Epidural anesthesia andanalgesia in high-risk surgical patients. Anesthesiology 1987; 66:729–736.
7 Rodger A, Walker N, Scgug S, et al. Reduction of postoperative morbidity andmortality with epidural or spinal anaesthesia: results from overviews ofrandomized trials. Br Med J 2000; 321:1493.
8 Klein SM, Bergh A, Steele SM, et al. Thoracic paravertebral block for breastsurgery. Anesth Analg 2000; 90:1402–1405.
9 Berlin B, Shavit Y, Trabekin E, et al. The effects of postoperative painmanagement on immune response to surgery. Anesth Analg 2003; 97:822–827.
10 Hollmann MW, Weiczorek KS, Smart M, Durieux ME. Epidural anesthesiaprevents hypercoagulation in patients undergoing major orthopedic surgery.Reg Anesth Pain Med 2001; 26:216–222.
11 Hadzic A, Arliss J, Kerimoglu B, et al. A comparison of infraclavicular nerveblock versus general anesthesia for hand and wrist day-case surgeries.Anesthesiology 2004; 101:127–132.
12 McLean AJ, Le Couteur DG. Aging biology and geriatric clinical pharmacol-ogy. Pharmacol Rev 2004; 56:163–184.
13 Gafni A. Structural modifications of proteins during aging. J Am Geriatr Soc1997; 45:871–880.
14 Turnheim K. When drug therapy gets old: pharmacokinetics and pharmaco-dynamics in the elderly. Exp Gerontol 2003; 38:843–853.
15 Lakatta EG. Age-associated cardiovascular changes in health: impact oncardiovascular disease in older persons. Heart Fail Rev 2002; 7:29–49.
16 Sprung J, Gajic O, Warner DO. Review article: age related alterations inrespiratory function – anesthetic considerations. Can J Anaesth 2006;53:1244–1257.
17 Lortat-Jacob B, Servin F. Pharmacology of intravenous drugs in the elderly.In: Sieber FE, editor. Geriatric anesthesia. New York: McGraw-Hill; 2006.pp. 91–103.
18 Lamb EJ, O’Riordan SE, Delaney MP. Kidney function in older people:pathology, assessment and management. Clin Chim Acta 2003; 334:25–40.
19 Cepeda MS, Farrar JT, Baumgarten M, et al. Side effects of opioids duringshort-term administration: effect of age, gender and race. Clin Pharmacol Ther2003; 74:102–112.
20
��Monk TG, Weldon BC, Garvan CW, et al. Predictors of cognitive dysfunctionafter major noncardiac surgery. Anesthesiology 2008; 108:18–30.
Negative influences can be seen in all patients presenting for surgery andanesthesia, but additional concerns must be extended to the elderly patientsand those with underlying neurological diseases. The influences from anestheticadministration and other environmental factors may have a long-term impact.
21
��Price CC, Garvan CW, Monk TG. Type and severity of cognitive decline inolder adults after noncardiac surgery. Anesthesiology 2008; 108:8–17.
Preoperative patient assessment must always consider type and severity ofcognitive decline in older adults presenting for surgery. The findings will proveto have relevance for patients and caregivers, and research needs to continue toexamine how perioperative factors influence neuronal systems.
opyright © Lippincott Williams & Wilkins. Unautho
22 Gulur P, Nishimori M, Ballantyne JC. Regional anaesthesia versus generalanaesthesia, morbidity and mortality. Best Pract Res Clin Anaesthesiol 2006;20:249–263.
23 McGrath B, Elgendy H, Chung F, et al. Thirty percent of patients havemoderate to severe pain 24 hr after ambulatory surgery: a survey of 5,703patients. Can J Anaesth 2004; 51:886–891.
24
�Pergolizzi J, Boger RH, Budd K, et al. Opioids and the management of chronicsevere pain in the elderly: consensus statement of an International ExpertPanel with focus on the six clinically most often used World Health Organiza-tion Step III opioids (buprenorphine, fentanyl, hydromorphone, methadone,morphine, oxycodone). Pain Pract 2008; 8:287–313.
The use of opioids in treating pain and the criteria for selecting analgesics for paintreatment in the elderly patients must include overall efficacy, overall side effectprofile, onset of action, drug interactions, abuse potential, and practical issuessuch as cost and availability of the drug, as well as the severity and type of pain(nociceptive, acute/chronic, etc.). This proves to be a good consensus statementfrom an International Expert Panel, with focus on the clinically most often usedWorld Health Organization Step III opioids.
25 Grant SA, Neilsen KC, Greengrass RA, et al. Continuous peripheralnerve block for ambulatory surgery. Reg Anesth Pain Med 2001; 26:209–214.
26
��Santiveri Papiol X, Castillo Monsegur J, Bisbe Vives E, et al. Epidural analgesiaversus femoral or femoral-sciatic nerve block after total knee replacement:comparison of efficacy and safety. Rev Esp Anestesiol Reanim 2009; 56:16–20.
Pain subsequent to many surgical procedures can be intense, and this studyidentifies only one surgical procedure, but the results can be modeled toward manyother different types of surgical procedures. Pain can often be treated moreeffectively and is associated with less postoperative morphine consumption with aperipheral nerve block. In addition, peripheral nerve block techniques often havefewer adverse side effects than epidural analgesia.
27 Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome.Am J Surg 2002; 183:630–641.
28
�Sundarathiti P, Ruananukul N, Channum T, et al. A comparison of continuousfemoral nerve block (CFNB) and continuous epidural infusion (CEI) in post-operative analgesia and knee rehabilitation after total knee arthroplasty (TKA).J Med Assoc Thai 2009; 92:328–334.
The search for the tailored anesthetic plan should focus on optimal analgesia whileminimizing side effect profiles of the chosen anesthetic technique.
29
�Minville V, Asehnoune K, Salau S, et al. The effects of spinal anesthesiaon cerebral blood flow in the very elderly. Anesth Analg 2009; 108:1291–1294.
This study identifies the potential of exacerbation or cumulative influence of themany details and the impacts they may play significant roles in patient care.
30
�Cecile M, Seux V, Pauly V, et al. Adverse drug events in hospitalized elderly ina geriatric medicine unit: study of prevalence and risk factors. Rev Med Interne2009; 30:393–400.
This recent paper once again identifies a need for diligence in formulatingthe anesthetic plan tailored according to considerations of patient disorder,co-morbidities, medications, and adverse drug potentials.
31 Wu CL, Hsu W, Richman JL, et al. Postoperative cognitive function as anoutcome of regional anesthesia and analgesia. Reg Anesth Pain Med 2004;29:257–268.
32 Canet J, Raeder J, Rasmussen LS, et al. Cognitive dysfunction after minorsurgery in the elderly. Acta Anaesthesiol Scand 2003; 47:1204–1210.
33 Kain ZN, Caldwell-Andrews AA. Sleeping characteristics of adults under-going outpatient elective surgery: a cohort study. J Clin Anesth 2003;15:505–509.
34
��Fecho K, Lunney AT, Boysen PG, et al. Postoperative mortality afterinpatient surgery: incidence and risk factors. Ther Clin Risk Manag 2008;4:681–688.
This study deciphered details specific to perioperative management of patient careto come to conclusions versus merely looking at the outcome. It identified riskfactors and the effects of anesthetic choices collectively to evaluate efficacy thathas important consequences following treatment.
35 Pavlin DJ, Chen C, Penaloza DA, et al. A survey of pain and other symptomsthat affect the recovery process after discharge from ambulatory surgery units.J Clin Anesth 2004; 16:200–206.
36
��Lagger V, Mahrer Imhof R, Imhof L. Pain management in patients withcognitive impairment: a research implementation project. Pflege 2008; 21:149–156.
Elderly patients and those with cognitive impairment and consecutive commu-nication disturbance are, due to their age and illness, a very vulnerable group.They are particularly at risk because their pain is not well assessed and,therefore, often not treated adequately. Insufficient pain management, however,impacts health status and decreases cognitive functioning and the patients’ qualityof life.
rized reproduction of this article is prohibited.

C
Pain management in the elderly Halaszynski 599
37 Kuramochi K, Osuga Y, Yano T, et al. Usefulness of epidural anesthesia ingynecological laparoscopic surgery in comparison to general anesthesia.Surg Endosc 2004; 18:847–851.
38
�Lee DK, Mulder GD. Foot and ankle surgery: considerations for the geriatricpatient. J Am Board Fam Med 2009; 22:316–324.
The changes in surgical approaches for the geriatric patient have permitted moreeffective and rapid intervention in problems affecting ambulation and quality of lifein our aged population.
39 Schroeder D, Hill GL. Predicting postoperative fatigue: importance of pre-operative factors. World J Surg 1993; 17:226–231.
40 Rubin GJ, Hotopf M. Systemic review of meta-analysis of interventions forpostoperative fatigue. Br J Surg 2002; 89:971–984.
41
��Saniova B, Drobny M, Sulaj M. Delirium and postoperative cognitive dysfunc-tion after general anesthesia. Med Sci Monit 2009; 15:81–87.
Administration of chemical agents that induce reversible unconsciousness caninfluence cognitive function with negative effects on consciousness and brainmechanisms underlying cognitive function. Central nervous system dysfunctionafter anesthesia and/or surgery can occur at any age but is a particular issue forelderly patients.
opyright © Lippincott Williams & Wilkins. Unauth
42
��Kimball WR, Carwood CM, Chang Y, et al. Effect of effort pain after upperabdominal surgery on two independent measures of respiratory function.J Clin Anesth 2008; 20:200–205.
Effort pain interacts dramatically with changing pulmonary function after upperabdominal and thoracic surgeries. There remains a direct relationship betweenresolution of pain with effort and direct measures of respiratory muscle effort that isoften enhanced with regional anesthesia.
43
��Popping DM, Elia N, Marret E, et al. Protective effects of epidural analgesiaon pulmonary complications after abdominal and thoracic surgery: a meta-analysis. Arch Surg 2008; 143:990–1000.
Regional anesthesia versus systemic analgesia on postoperative pulmonary com-plications continues to show superior analgesic benefit. There are also some datathat may show that regional anesthesia protects against other morbidities followingabdominal or thoracic surgery.
44 Nishimori M, Ballantyne JC, Low JH. Epidural pain relief versus systemicopioid-based pain relief for abdominal aortic surgery. Cochrane DatabaseSyst Rev 2006: CD005059.
45 Roy RC. Choosing general versus regional anesthesia for the elderly.Anestheiol Clin N Am 2000; 18:91–104.
46 Edelsberg J, Ollendorf D, Oster G. Venous thromboembolism following majororthopedic surgery: review of epidemiology and economics. Am J Health SystPharm 2001; 58:4–13.
orized reproduction of this article is prohibited.