rectal cancer - vanderbilt university medical …€¢ when is colorectal cancer considered rectal?...
TRANSCRIPT

Rectal Cancer
Jason Castellanos October 19, 2011

Colorectal Cancer
• Second leading cause of death from cancer • 147,000 new diagnoses annually • 50,000 deaths associated with disease/yr • In US, 61.2 (men) and 44.8 (women) cases per
100,000 • Screening of asymptomatic persons at
average risk can detect early and curable cancers – May also detect cancer-precursor lesions
Lieberman, DA. Screening for Colorectal Cancer. N Engl J Med 361;12.

Defining Risk
• High Risk: – First degree relative with CRC, age 50+
• Doubles lifetime risk of CRC among family members – If before age 50, concern for hereditary
syndromes (FAP, HNPCC) – Inflammatory Bowel Disease
• Average Risk: – High fat/low fiber and calcium diets, obesity, low
level of physical activity, tobacco use, high alcohol intake
Screening Program Attributes
• Screen at appropriate age to identify those with an increased likelihood of disease
• Ongoing screening at specified intervals for those with negative initial findings
• Appropriate follow-up for abnormal screening results
• Surveillance of high-risk pts for new lesions

Screening Strategies


Adenoma Carcinoma Sequence
• Most CRC arise from adenomatous polyps
• Progression to carcinoma takes at least 10 yrs on average
• Large, flat adenomas may be more likely to contain dysplastia
• Risk of CRC increases with adenoma size, #, and histology

Colonoscopy
• 0.5 – 1.0% of screened patients have cancer • 5 – 10% have removable advance neoplasia • Reduces incidence and mortality from CRC in
case-control studies • No randomized, controlled trials compare
outcomes with other screening measures • In pts with adenoma found, CRC may develop
in 0.3 – 0.9% within 3 – 5 years

Guidelines
• Multi-Society Task Force – Screen at age 50 for avg risk pts – Stop screening when life expectancy < 10 yrs – Personal preference of test choice (more inclusive)
• American College of Gastroenterology – Colonoscopy preferred; fecal immunochemical test if
colonoscopy declined – Screen African Americans at age 45
• US Preventive Services Task Force (USPSTF) – 3 screening options: fecal occult blood test, flex sig
q5yrs with FOBT q3yrs, colonoscopy q10yrs

Rectal Cancer
• Colorectal Cancer remains 2nd leading cause of cancer related deaths – 148,810 new cases 2008, 28% in
rectum • When is Colorectal cancer
considered Rectal? • Rectal cancer: neoplasm of
distal 10-12 cm in the extraperitoneal pelvis

Preoperative Evaluation
• History: assess for hereditary/familial syndromes • DRE: size, fixation, location • Rigid Sigmoidoscopy: measure distance from AV • Colonoscopy: at least 5% have synchronous lesions • CEA • CT Scan/PET scan • Endorectal Ultrasound vs. Pelvic MRI • Accurately stage disease
– Typically CT C/A/P to assess for metastatic disease, ERUS for locoregional staging
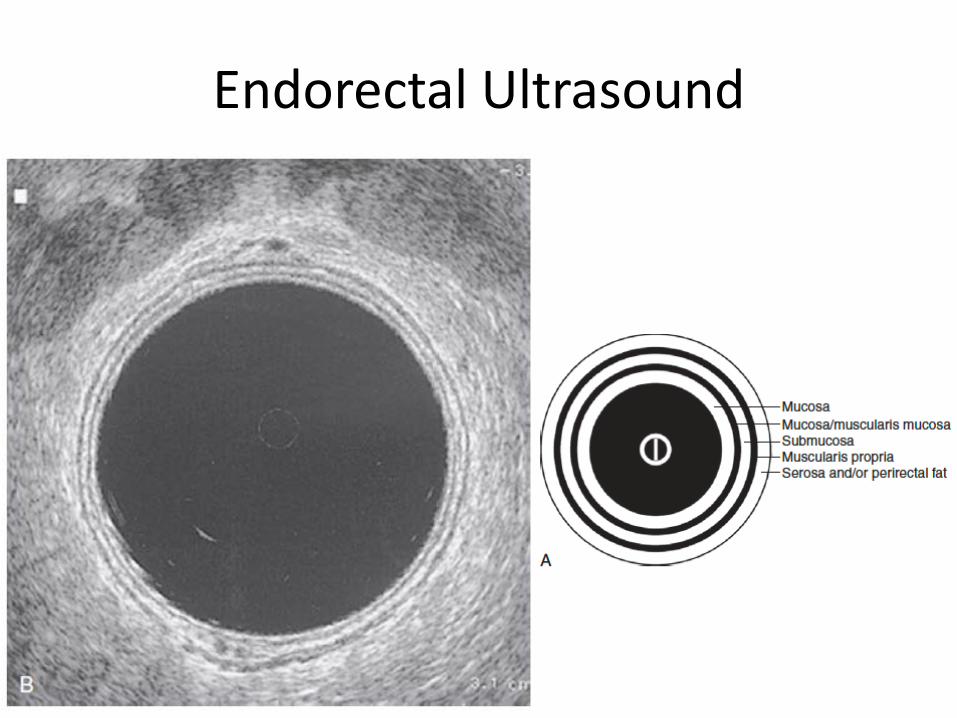
Endorectal Ultrasound

Staging
• Preop: Clinical staging to select treatment
T1 T2
T3

Staging

Staging

Treatment Algorithm

Carcinoma In Situ and T1N0 • Local Excision
– Lower morbidity, preserved anorectal function
• Local recurrance increased – 11-29%, MSK T1 5 yr rate: 15% vs.
3% after radical resection • Unresected regional LNs • Incomplete pathologic staging • LN metastasis up to 18% in T1 • Salvage surgery possible, but poor
survival (50% 5 year DSS)

T2N0
• Invasion of muscularis propria • Radical resection • If + LNs, postop adjuvant CRT • Preop XRT if close to sphincter to attempt
sphincter preservation (LAR vs. APR)

Locally Advanced Rectal Cancer
• T3/4 and/or N+ • Neoadjuvant CRT followed by radical resection • Metastatic disease – treatment tailored to
individual based on: – Primary lesion (sx’s, resectability) – Extent of metastases – Patient factors (age, comoribidites)

Neoadjuvant/Adjuvant Therapies
• High local failure rates highlighted need for adjuvant therapy
• NCCTG multi-institutional trial: 5-FU + rads – Contiguous infusion of 5-FU during radiation improved
DFS and OS • Preop radiation
– Potentially induce tumor regression – Improve sphincter preservation rates – Pathologic complete response rates of 10 – 20%,
associated with improved outcomes

Neoadjuvant/Adjuvant Therapies
• Dutch Colorectal Cancer Group – Assessed adding preop RT to TME surgery – Improved 5 year local recurrence rates (5.6 vs. 10.9%)
• German Rectal Cancer Group – Preop vs. postop CRT for Stage II or III disease – Less toxicity, improved 5 yr local recurrence rate (6 vs.
13%) • Surgical resection performed 6-8 weeks s/p CRT • ACOSOG – phase II trial, T2N0 cancers
– Aggressive neoadjuvant CRT local excision

Questions?

The History of Endoscopy
Colonoscopy: Principles and Practice, 2nd ed

Early Pioneers
• Very deep and labored breathing with normal or reduced frequency seen in severe diabetic ketoacidosis.
• Paradoxical rise in the JVP on inhalation in Constrictive pericarditis or COPD.



Strauss: Proctosigmoidoscope

Early Intraluminal Photography


Flexible Endoscopy