rectal cancer: 2015 updates
TRANSCRIPT

Mohamed Abdulla M.D.Prof. of Clinical OncologyCairo University
GSO – Raffles Hotel – Istanbul – 28/03/2015

Amgen. Merck Serono. Roche. Jansen Cilag. Astellas. MSD. pfizer. Novartis.

Cecum 14 %
Ascending colon 10 %
Transverse colon 12 %
Descending colon 7 %
Sigmoid colon 25 %
Rectosigmoid junct 0.9 %
Rectum 23 %
CA Cancer J Clin 2011;61:69–90. VC 2011 American Cancer Society, Inc.

CA Cancer J Clin 2011;61:69–90. VC 2011 American Cancer Society, Inc.
50 Years

Risk Factors• Genetic• FH• IBD• Obesity• Smoking• Alcohol
• Aspirin• NSAIDS• Vegetables• Physical
Activity• Adequate
Folate• Decreased
Caloric Intake
Primary prevention of colorectal cancer. Gastroenterology 2010; 138:2029.
Better Life Style

Good prognostic factors Old age
Gender(F>M)
Asymptomatic pts
Polypoidal lesions
Non circumferential lesions
Diploid
Poor prognostic factors Obstruction
Perforation
Ulcerative lesion
Adjacent structures involvement
Positive margins
LVSI
Signet cell carcinoma
High CEA
Tethered and fixed cancer

Tis T1 T2 T3 T4
Extension to an adjacent organ
Mucosa
Muscularis mucosae
Submucosa
Muscularis propria
Subserosa
Serosa
TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
Tis Carcinoma in situ: intraepithelial or invasion of lamina propria
T1 Tumor invades submucosa
T2 Tumor invades muscularis propria
T3 Tumor invades through the muscularis propria into pericolorectal tissues
T4a Tumor penetrates to the surface of the visceral peritoneum
T4b Tumor directly invades or is adherent to other organs or structures


Stage 5-year Survival (%)
0,1 Tis,T1;No;Mo > 90I T2;No;Mo 80-85II T3-4;No;Mo 70-75
III T2;N1-3;Mo 70-75III T3;N1-3;Mo 50-65III T4;N1-2;Mo 25-45IV M1 <3

History: Polyps & Colorectal Malignancy. Physical Examination: DRE. Routine laboratory investigations (CEA) Rigid Segmoidoscopy. Full Colonoscopy. Biopsy.
Journal of Surgical Oncology 2009;99:65–70

80-95% accurate in tumor staging 70-75% accurate in mesorectal lymph node
staging Use is limited to lesion < 14 cm from anus, not
applicable for upper rectum, for stenosingtumor
Very useful in determining extension ofdisease into anal canal (clinical important forplanning sphincter preserving surgery)
Figure. Endorectal ultrasoundof a T3 tumor of the rectum,extension through themuscularis propria, and intoperirectal fat.

Part of routine workup. Useful in identifying enlarged pelvic and extra-pelvic lymph-
nodes and visceral metastasis. Limited utility in:
1. small primary cancer.
2. T – Stage assessment.
3. Peri-rectal lymph nodes assessment.
Sensitivity 50-80% Specificity 30-80%
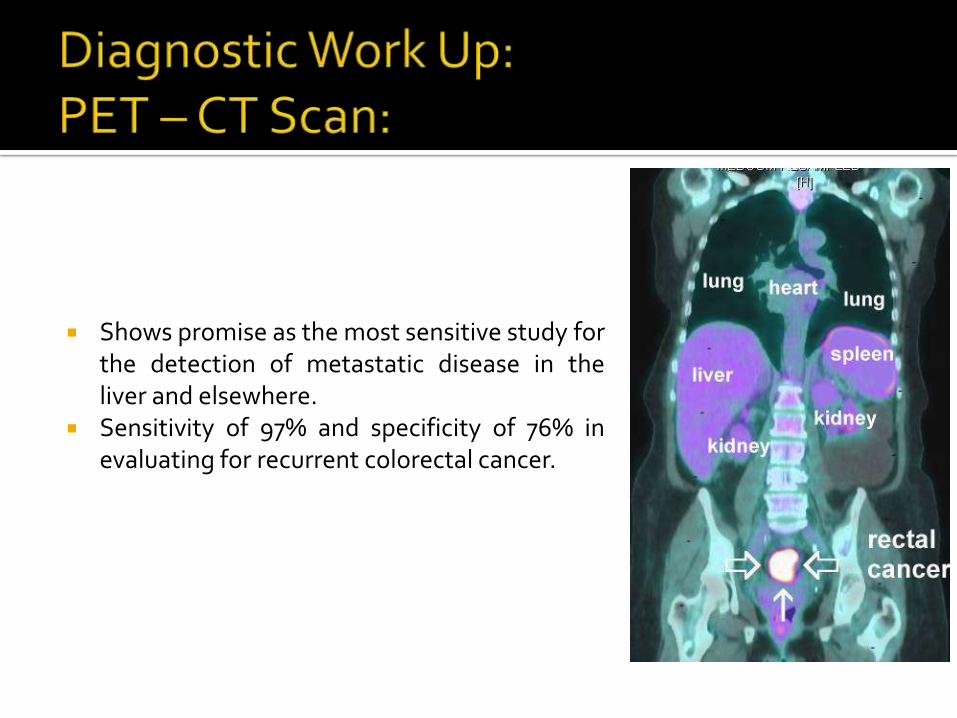
Shows promise as the most sensitive study forthe detection of metastatic disease in theliver and elsewhere.
Sensitivity of 97% and specificity of 76% inevaluating for recurrent colorectal cancer.

MRI may be Superior For:
1. Large field of view.
2. Better for proximal & stenotic lesions.
3. Less operator and technique dependent.
4. Size & morphologic characterization of peri-rectal nodes.
EUS may be Superior for:
1. More specific for muscularis propria invasion (T1 versus T2).
2. Significantly higher sensitivity for T3 disease.
High Resolution MRI & EUS Complementary Information.
Bipat et al.Radiology. 2004;232(3):773.

MDTSurgery
Radiation Therapy
Systemic Therapy
Imaging
Psychologist &
Rehabilitation

MDT & Multimodality Treatment Outcome is improving over time
Sauer et al. N Engl J Med 2004;351:1731-40.

High LR following APR and AR: 20-50% (35%). Sphincter preservation. To live with a stoma. Infections and sexual dysfunction. The perfect scenario.

Clinical Colorectal Cancer, Vol. 4, No. 4, 233-240, 2004

Removal of peri-rectaltissues involving lateral &circumferential margins ofmesorectal envelop.
Dis Colon Rectum. 2013 May;56(5):535-50.

Clinical Colorectal Cancer, Vol. 4, No. 4, 233-240, 2004

Clinical Colorectal Cancer, Vol. 4, No. 4, 233-240, 2004

GITSG. NCCTG. NSABP R-01.
N Engl J Med 1986; 315:1294.FJ Natl Cancer Inst 1988; 80:21. N Engl J Med 1991; 324:709.
Adjuvant Fluoroupyremidine
X 2 monthsCRT – 6 Weeks
Adjuvant Fluoroupyremidine
X 2 months

N Engl J Med 2004;351:1731-40.

10 -Year RTh + S S P
LR 5% 11% < 0.0001
OAS 48% 49% 0.86
CCSD 17% 22% 0.04
Lancet Oncol 2011; 12: 575–82

Lancet Oncol 2011; 12: 575–82

1. T3 –T4 Lesions: The only definitive indication.2. cT3N0: Should be treated (understaging).3. Depth of Extramural Invasion:
T3 lesions (>5 mm) ++ LNs involvement HigherCancer Specific Survival (54% Versus 85%).
Selection of high risk T3 for treatment.
Approved outside US.
4. T1 – 2 lesions with Positive Nodes.5. Low situated lesions.6. Invasion of mesorectal fascia.
Br J Cancer 2000; 82:1131.

Grade Regression Fibrosis
0 No All cells are viable
1 Minor < 25% fibrosis
2 Moderate 26 – 50%nFibrosis
3 Good >50%
4 Total No Viable Cells
Grade 10 – year DM P 10 –Year DFS P
0 - 1 39.6%0.005
63%0.0082 - 3 29.3% 73.6%
4 10.5 % 89.5%
J Clin Oncol 32:1554-1562. © 2014

British Journal of Surgery 2012; 99: 918–928
Can we Avoid Surgery?

The Cancer Journal • Volume 13, Number 3, May/June 2007
EQUIVALENT

Curr Opin Oncol 2012, 24:441–447

Curr Opin Oncol 2012, 24:441–447

Curr Opin Oncol 2012, 24:441–447

Polish TrialTrans-Tasman
Radiation Oncology Group
• Local Recurrence.• DFS• Distant Recurrence• OAS• Severe Late Toxicity
EQUIVALENT
J Clin Oncol 2012; 30:3827.Br J Surg 2006; 93:1215

Rectal cancer should be treated by MDT. Surgery is still the mainstay of treatment. Neoadjuvant CRT is more appealing than
postoperative schedule regarding outcome and toxicity profile for patients with stage II & III rectal cancer.
Fluoroupyremidine therapy is still the backbone of any regimen and can be substituted by the oral form.
Long course radiation therapy is still preferred by majority of treating groups.
pCR is associated with significant improvement in outcome.
Still more research is awaited.
