recent trends in colitis
TRANSCRIPT
RECENT TRENDS IN COLITIS
Moderator : Dr Kala
Presenter: Dr Shashikala C
Changes in recent years include:
-Wide spread use of full colonoscopy
-greater recognition of the effects of time and treatment
-improved documentation of variations in anatomical
distribution
-better understanding of the mimics of IBD
-Significant progress in clinical management
-modifications of terminology
Value of biopsy assessment
Confirmation of the diagnosis of IBD
Distinction between UC and CD
Exclusion of dysplasia
Exclusion of coexistent conditions or complications
Also…..
Disease activity
Disease extent
Tissue sampling
Taken from
Both endoscopically normal and abnormal mucosa
Samples of - ileum
-atleast four colonic sites
-the rectum
With minimum of two biopsies from each site
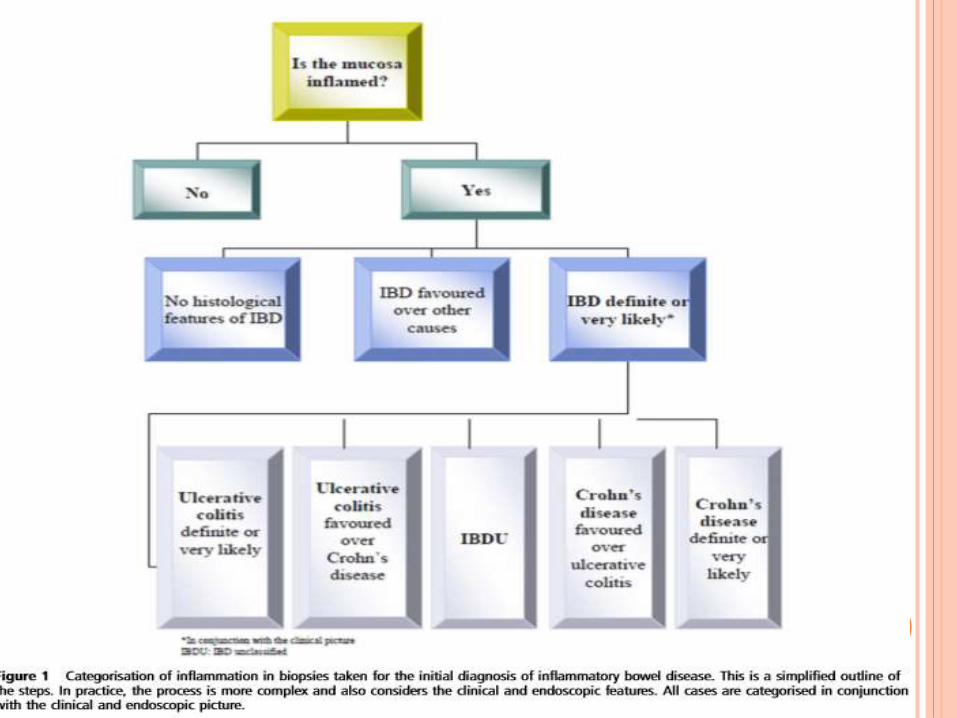
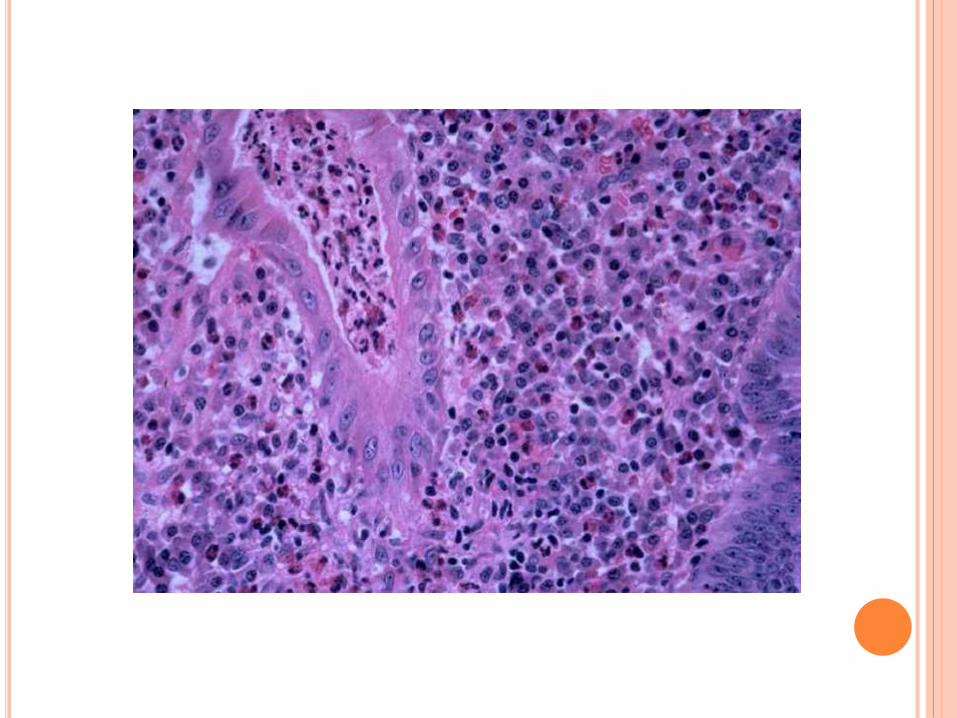
Is the mucosa inflammed?
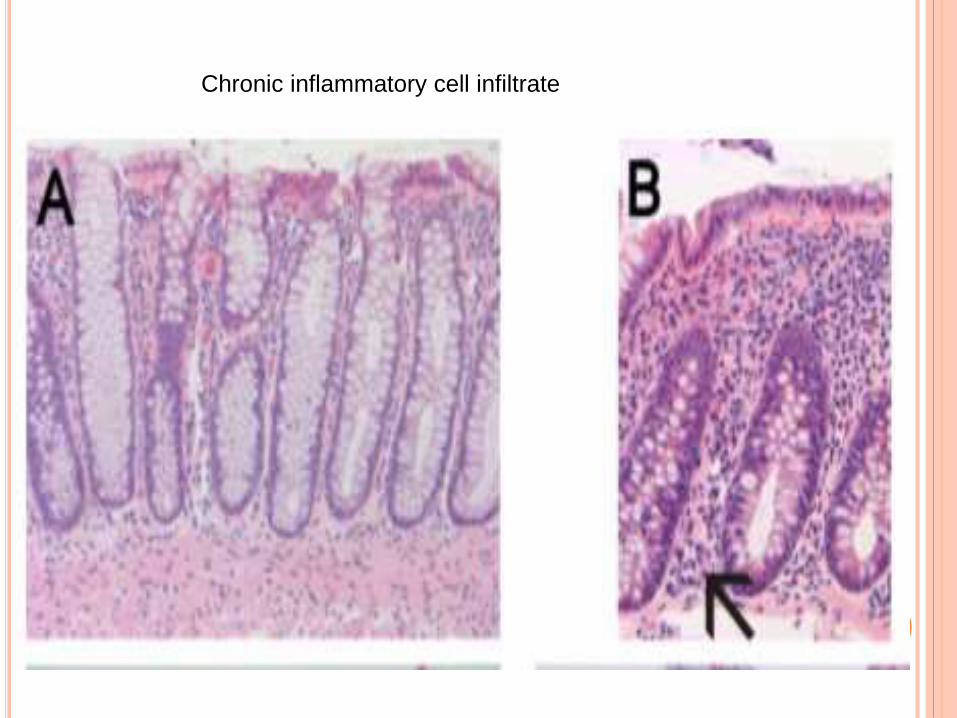
Chronic inflammatory cell infiltrate
Histiocyte/macrophages-
muciphages are normal findings especially in colon
Eosinophils-
normal in lamina propria
sparse intraepithelial eosinophils
Acute inflammatory cells-
A few intraepithelial neutrophils are normal[2-
3/biopsy]
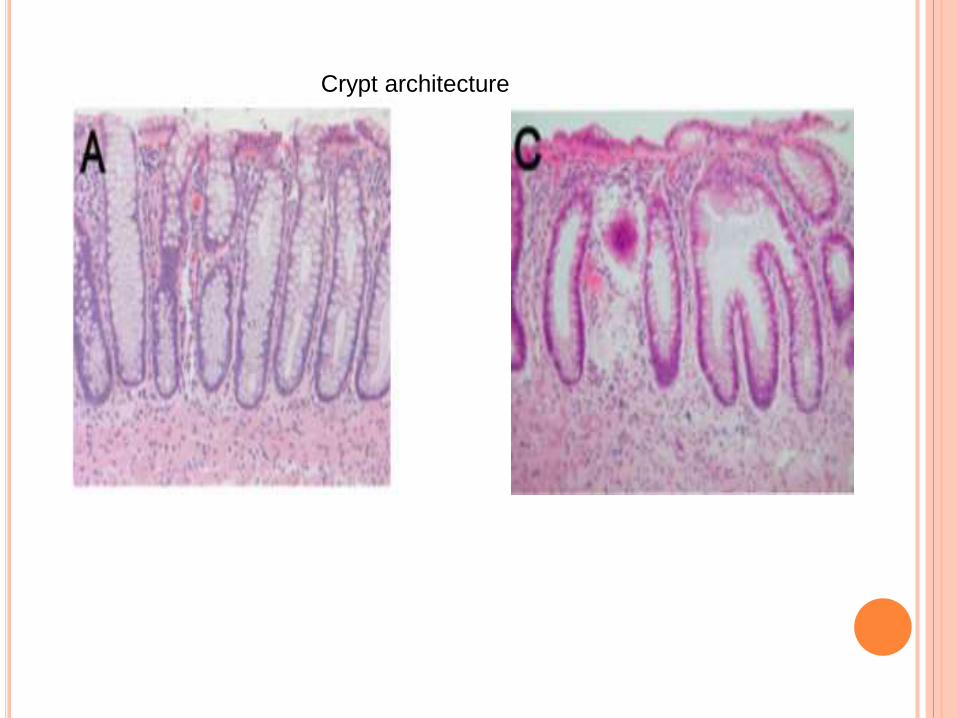
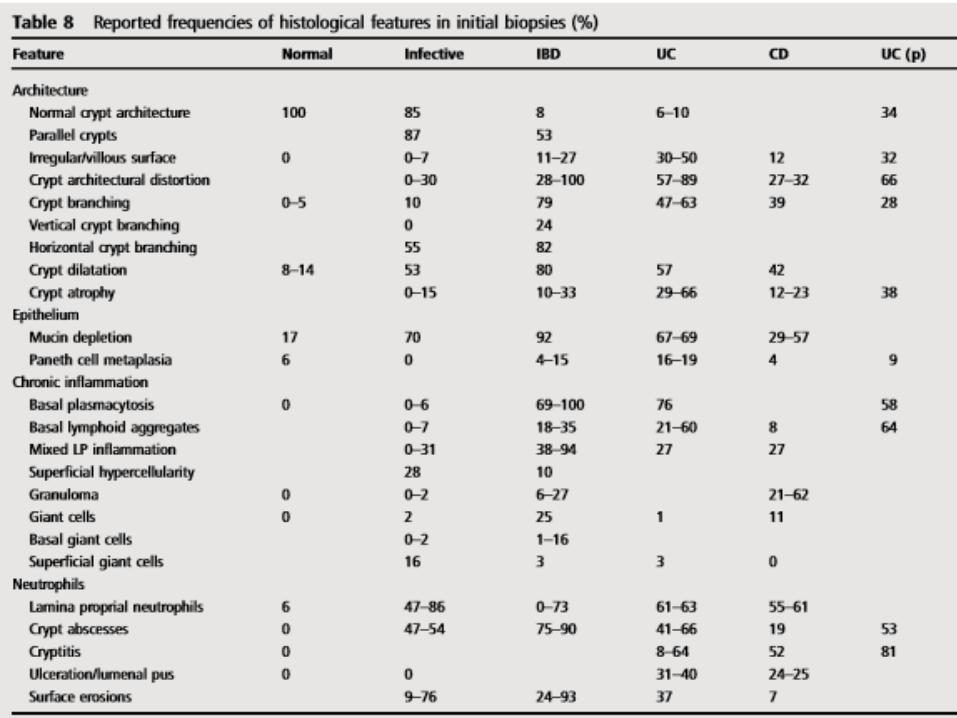
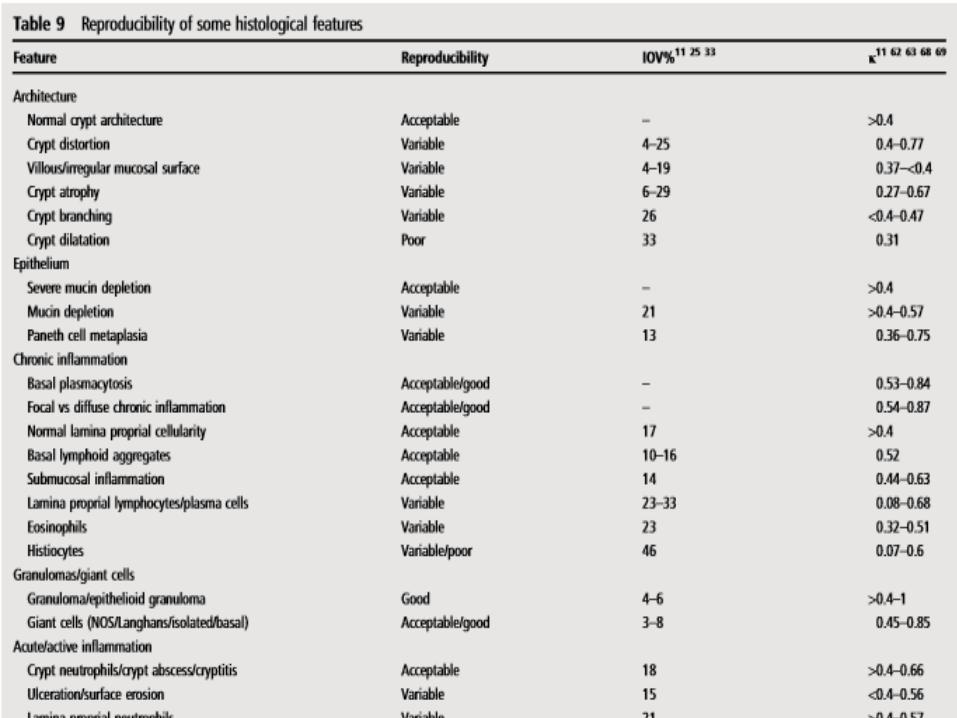
Crypt architecture
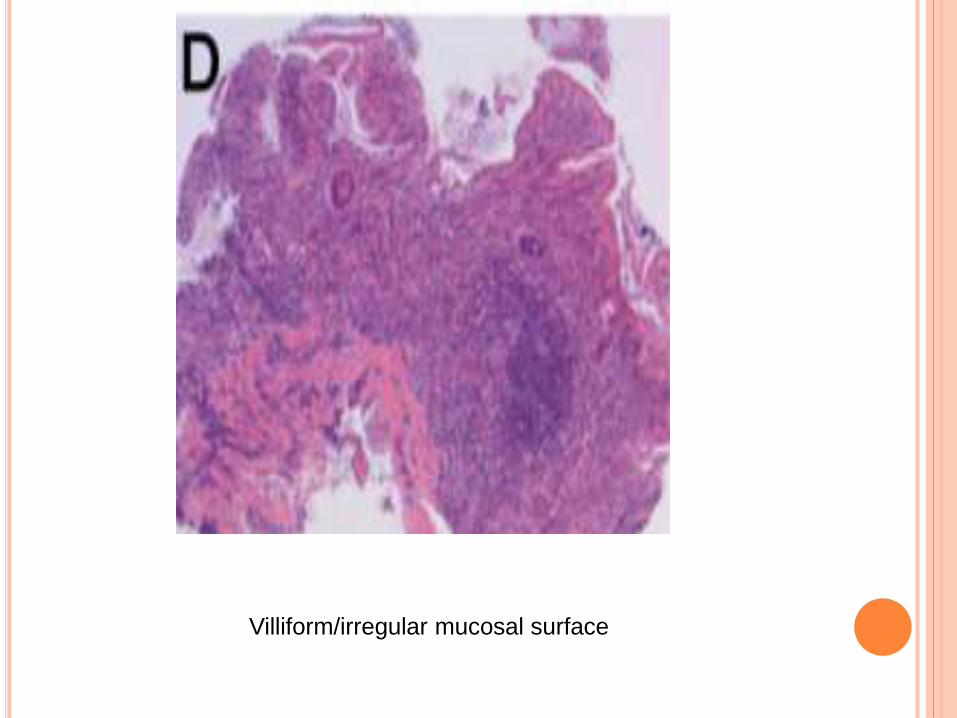
Villiform/irregular mucosal surface
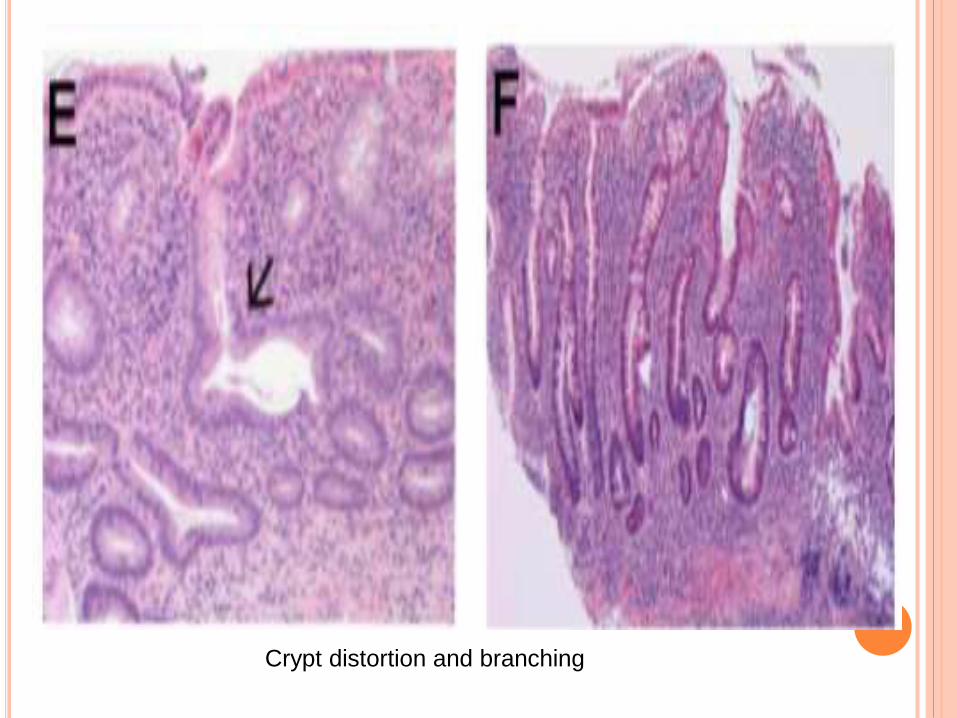
Crypt distortion and branching
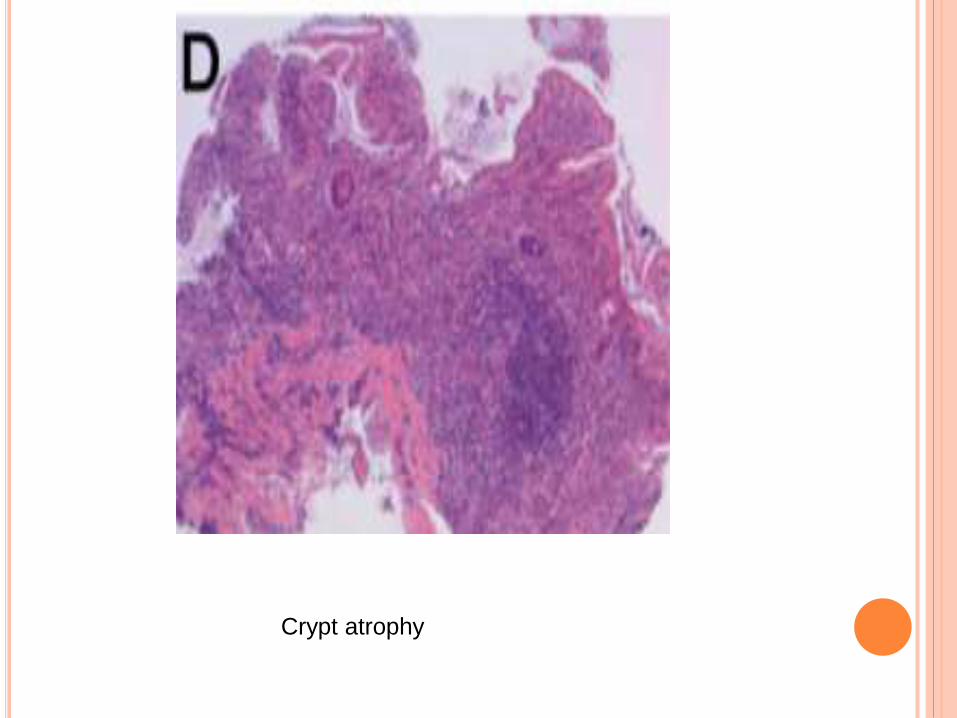
Crypt atrophy
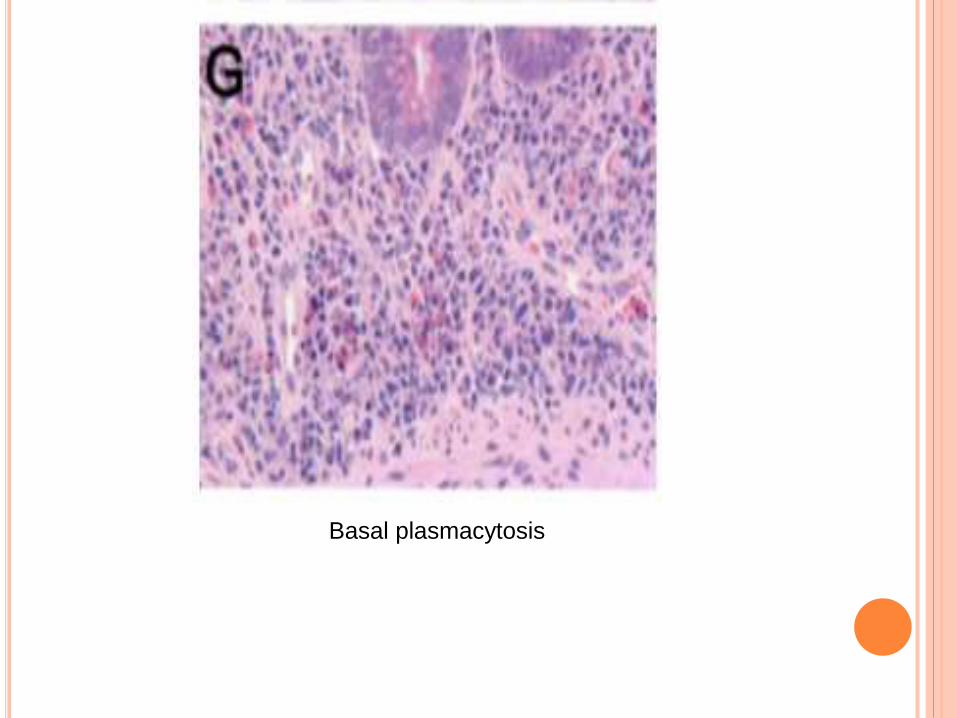
Basal plasmacytosis
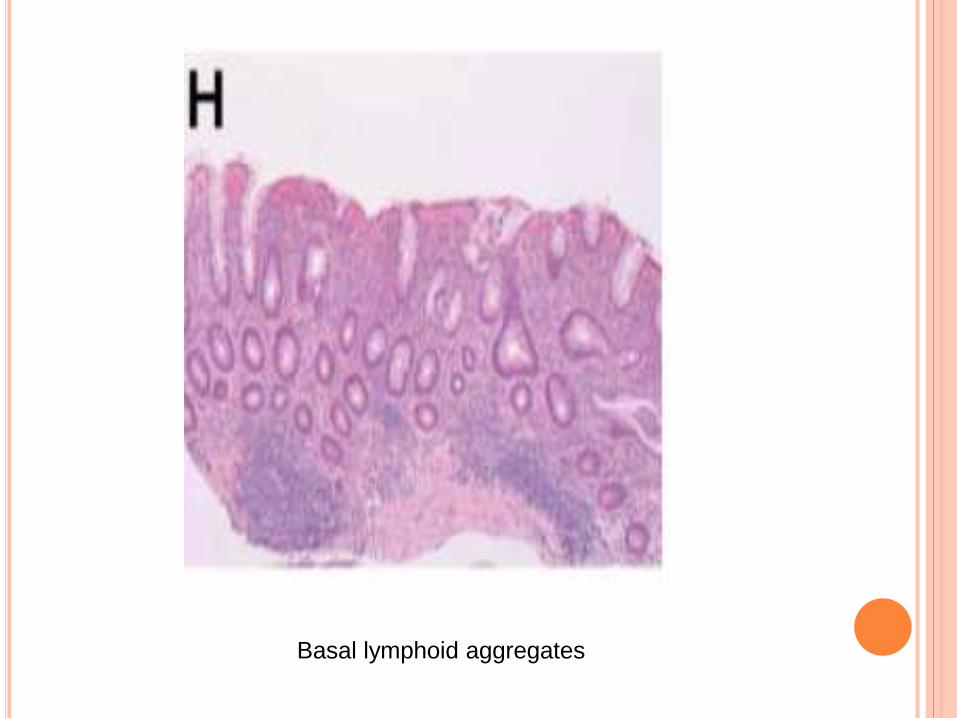
Basal lymphoid aggregates
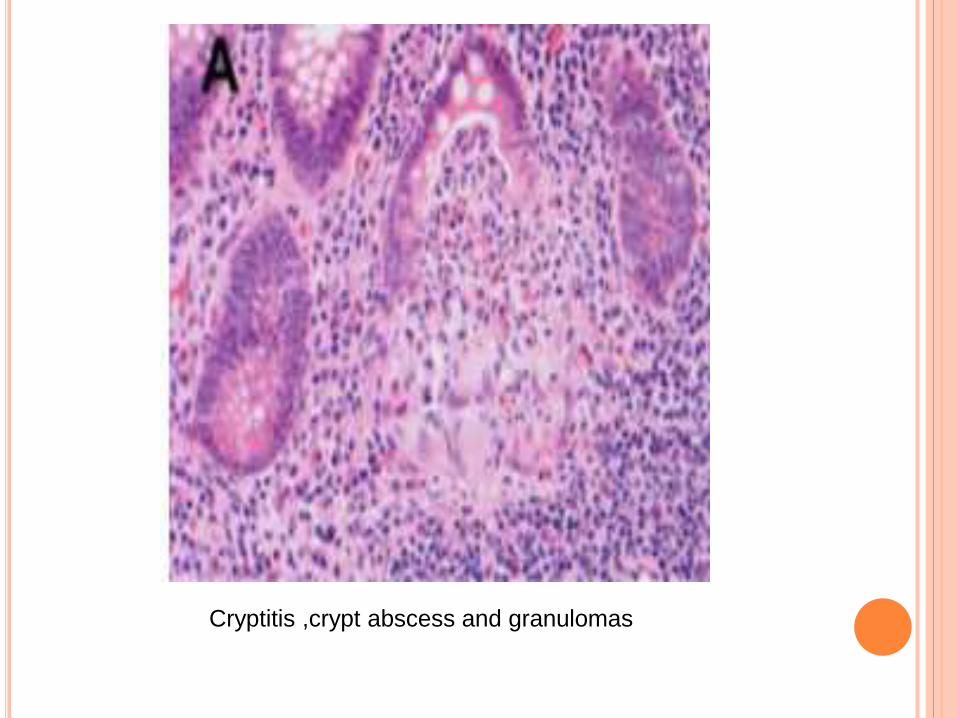
Cryptitis ,crypt abscess and granulomas
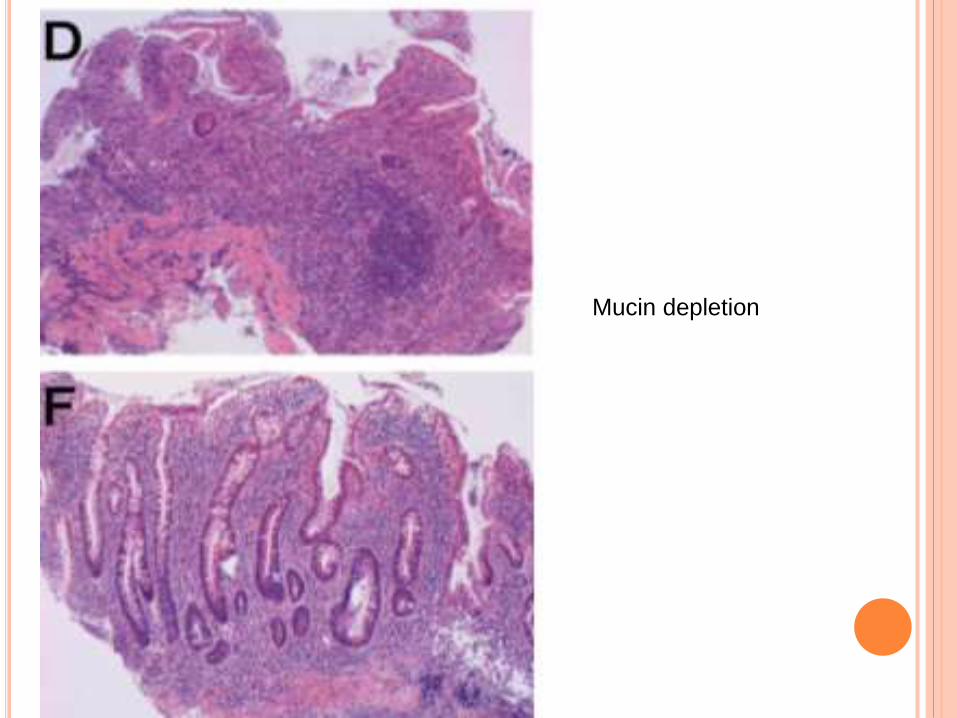
Mucin depletion
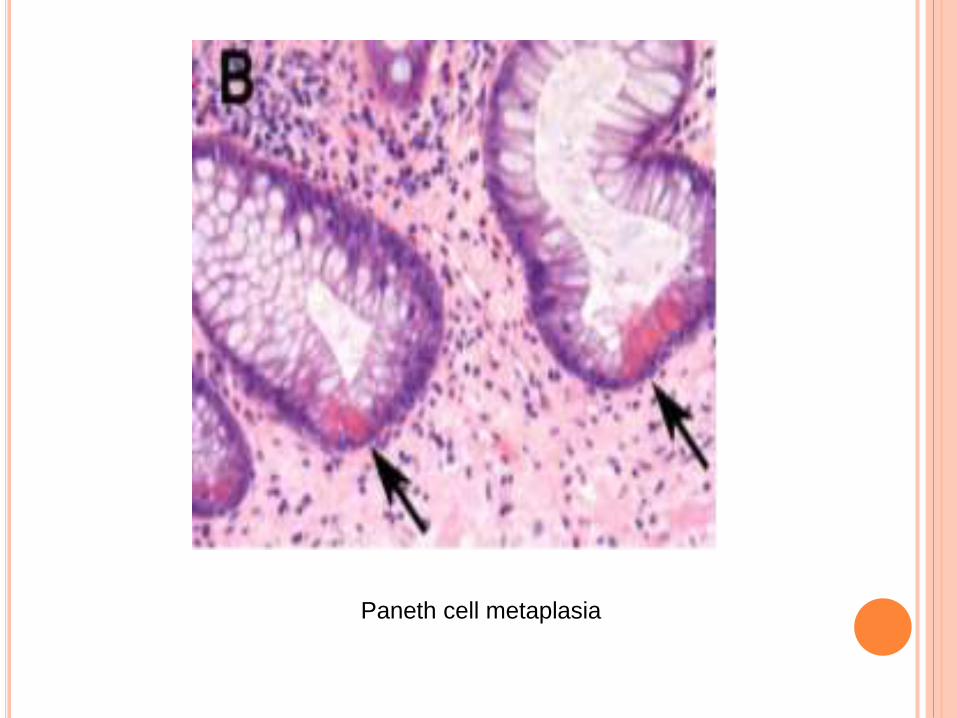
Paneth cell metaplasia
Distribution , Extent and Activity
Distribution of chronic inflammatory cells and crypt changes
Between anatomical sites
Between biopsies from the same site
Within biopsies
Terms for distribution within biopsies and within single site:-
For chronic inflammatory infiltrate- diffuse , patchy, focal
For crypt changes and acute inflammation- diffuse , focal
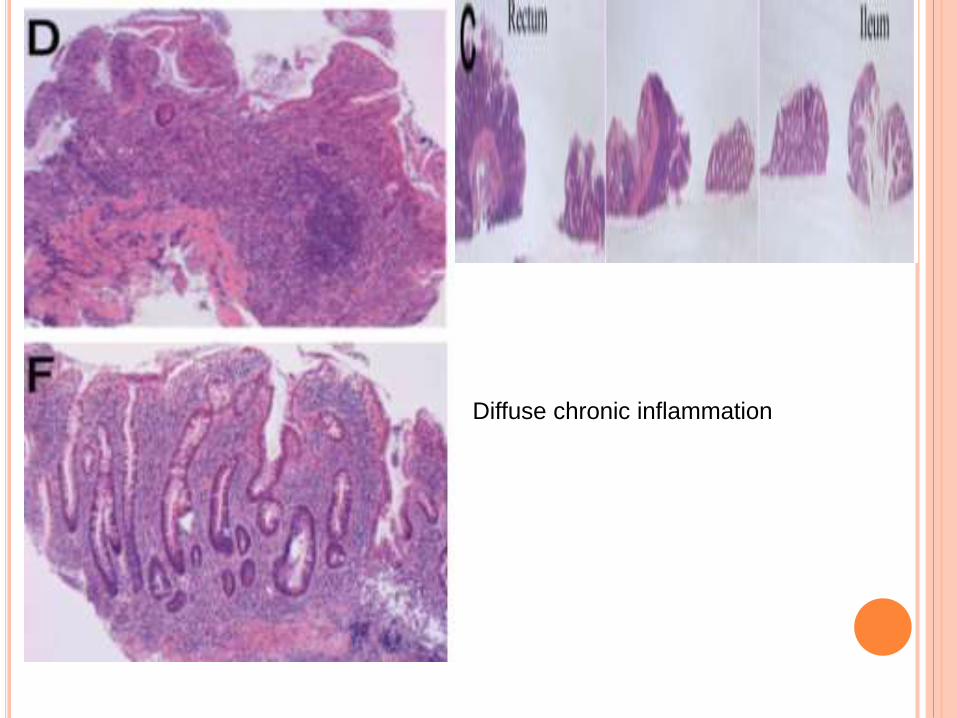
Diffuse chronic inflammation
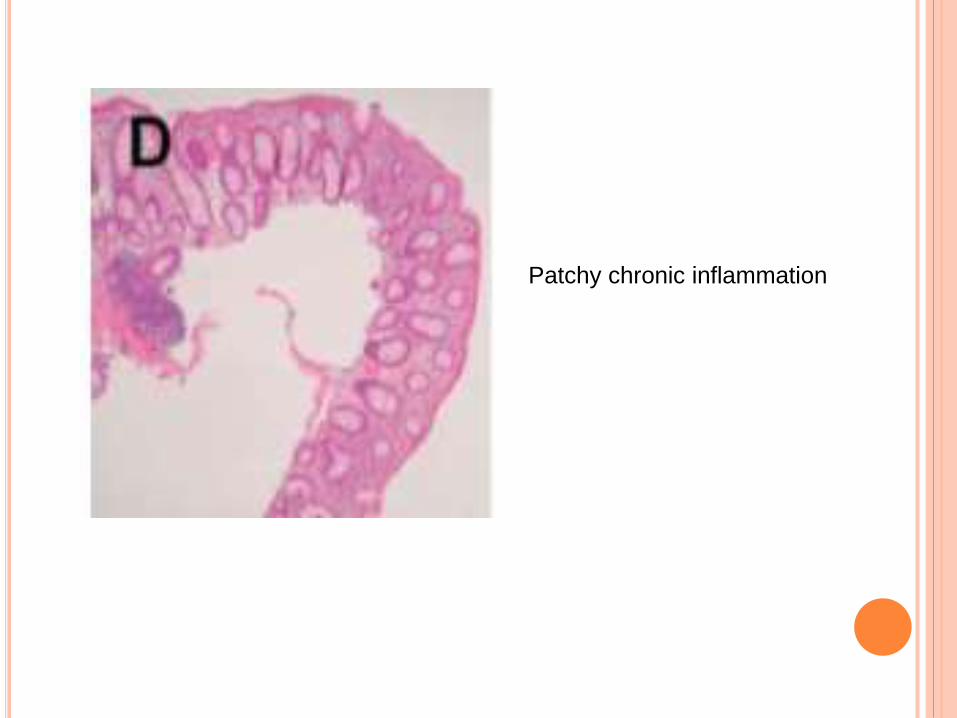
Patchy chronic inflammation
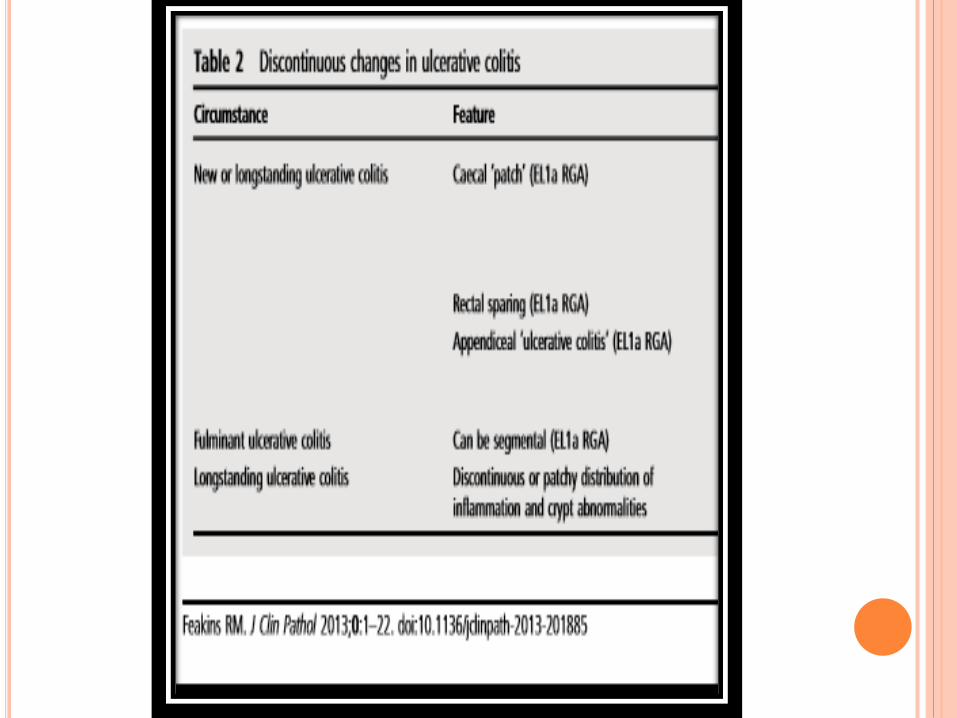
Terms for distribution between sites
-continuous between sites
-segmental/ discontinuous between sites
Diagnostic value :
Distribution between sites-
continuous favours UC and discontinuous/segmental
favour CD
Distribution within sites /within biopsies
diffuse favours UC and focal/ patchy favours CD
An increased severity from proximal to distal favours UC and
right sided predominance favours CD
Extent of disease
-Determined endoscopically
- Extent in UC helps to predict the risk of dysplasia
- Extent in CD is difficult to determine
- Histological extent does not always correlate with
endoscopic extent
Activity
Histologic activity confirmation requires
cryptitis
crypt abscesses
surface epithelial neutrophils
erosion or
ulceration
IBD VERSUS NON IBD
IBD vs acute infective colitis/ acute self limiting colitis/ non-
IBD colitis
History :
Infective colitis- bloody diarrhea and associated symptoms
lasts for shorter duration
no relapse
secondary to shigella, salmonella,
campylobacter
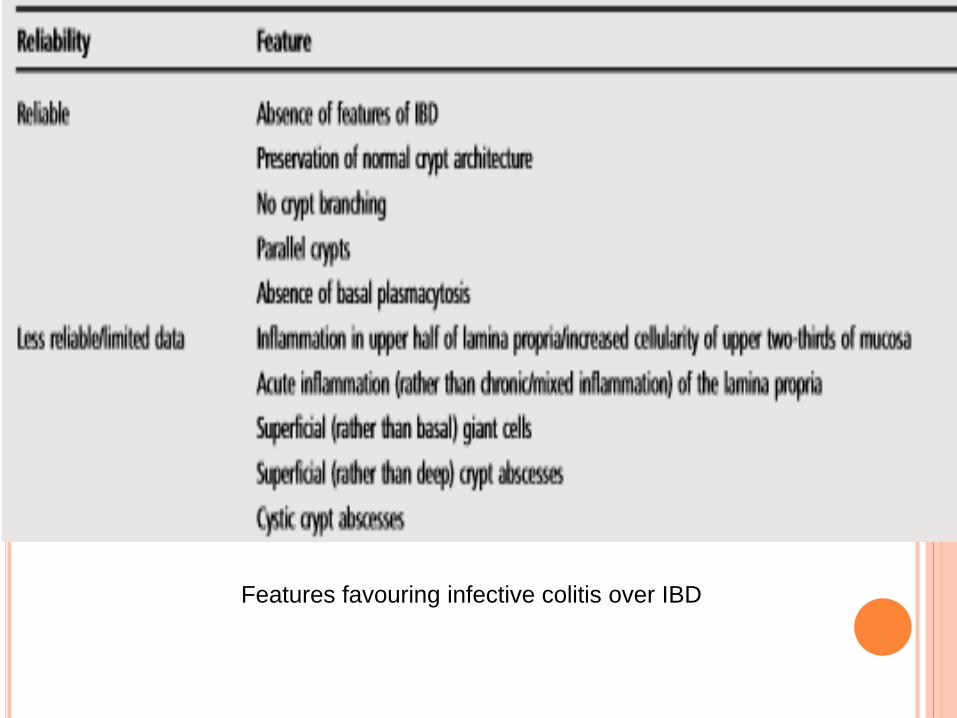
Features favouring infective colitis over IBD
IBD versus infective colitis: exceptions
▸ Crypt distortion occurs in a minority of infective coli- tides,
particularly in the healing phase or if infection is severe or
prolonged.
▸ A few infective colitis biopsies have basal plasmacytosis or
other evidence of chronic inflammation.
▸ Crypt abnormalities may be absent from IBD biopsies,
especially in early or treated disease.
▸ Some IBD biopsies have little or no basal plasmacytosis/
chronic inflammation, particularly early in the course of
disease or after treatment.
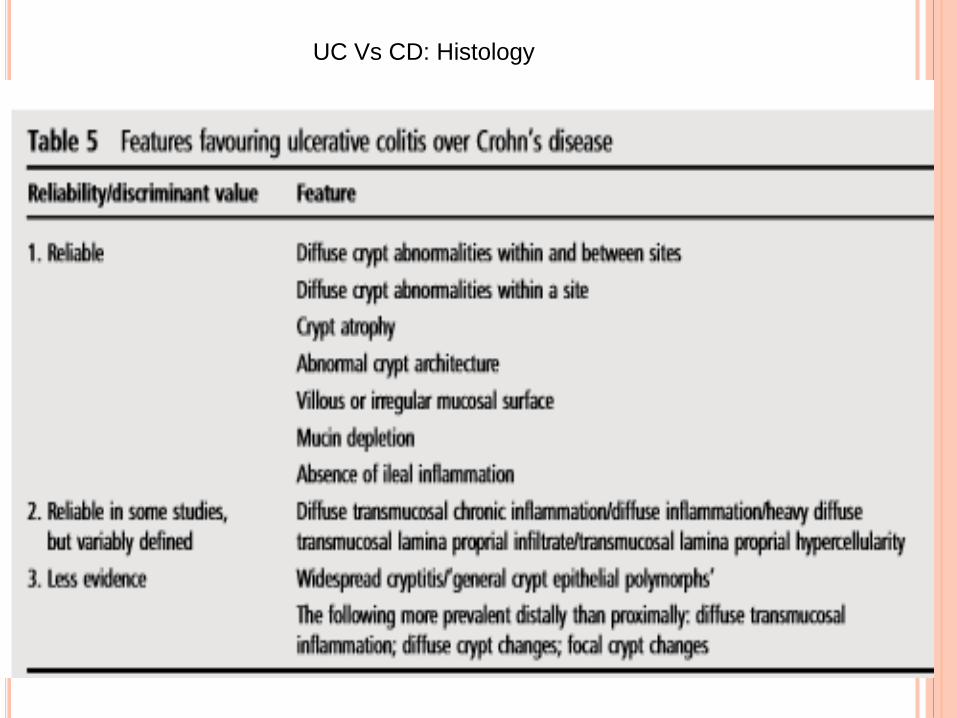
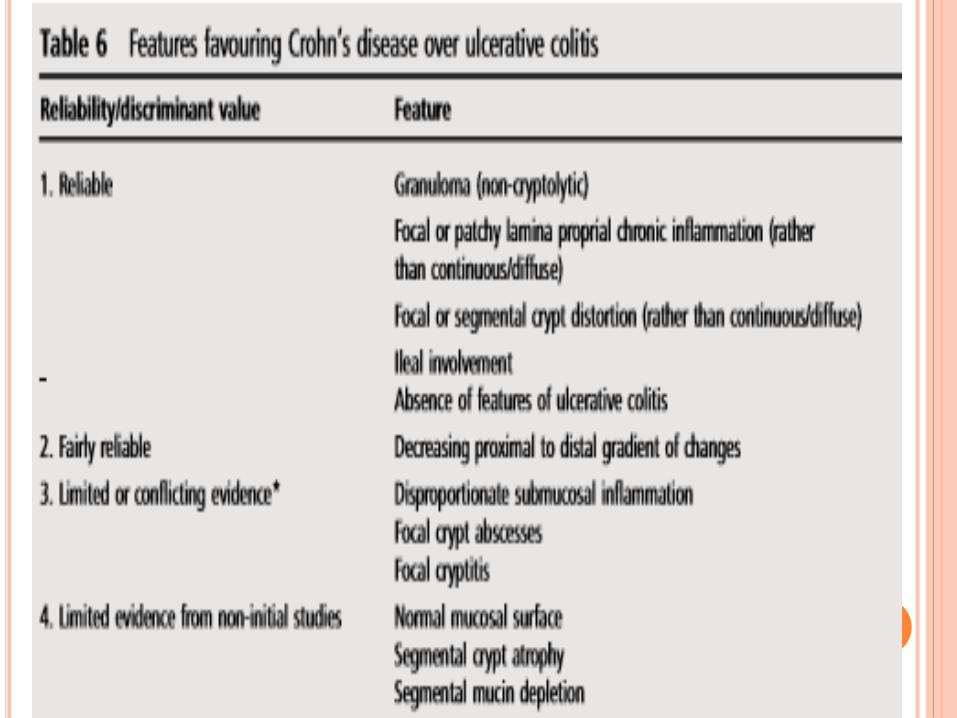
UC Vs CD: Histology
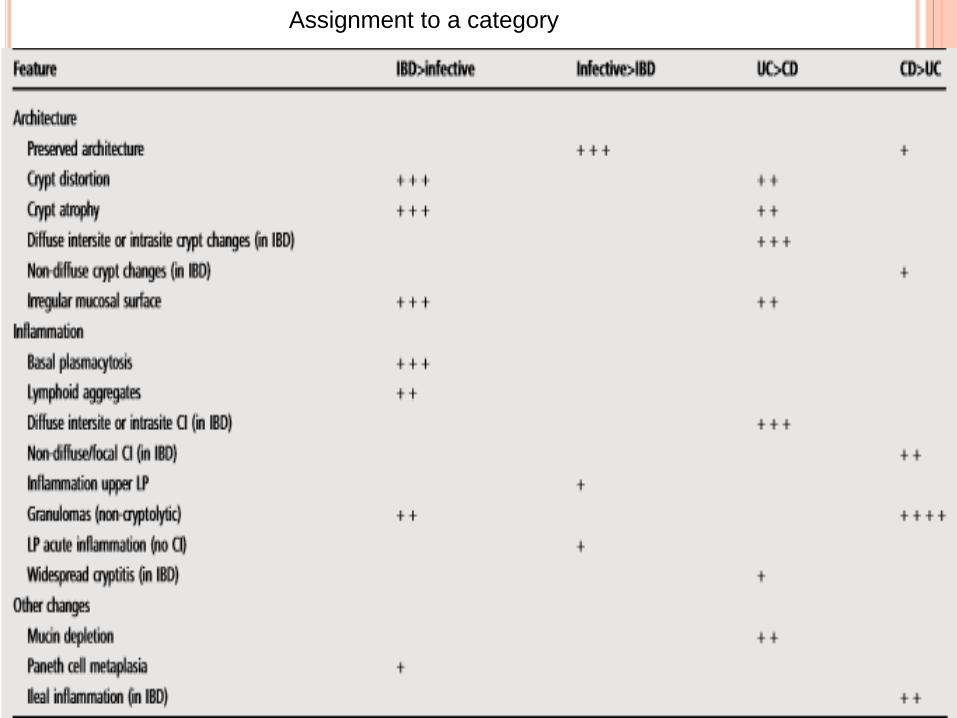
Assignment to a category
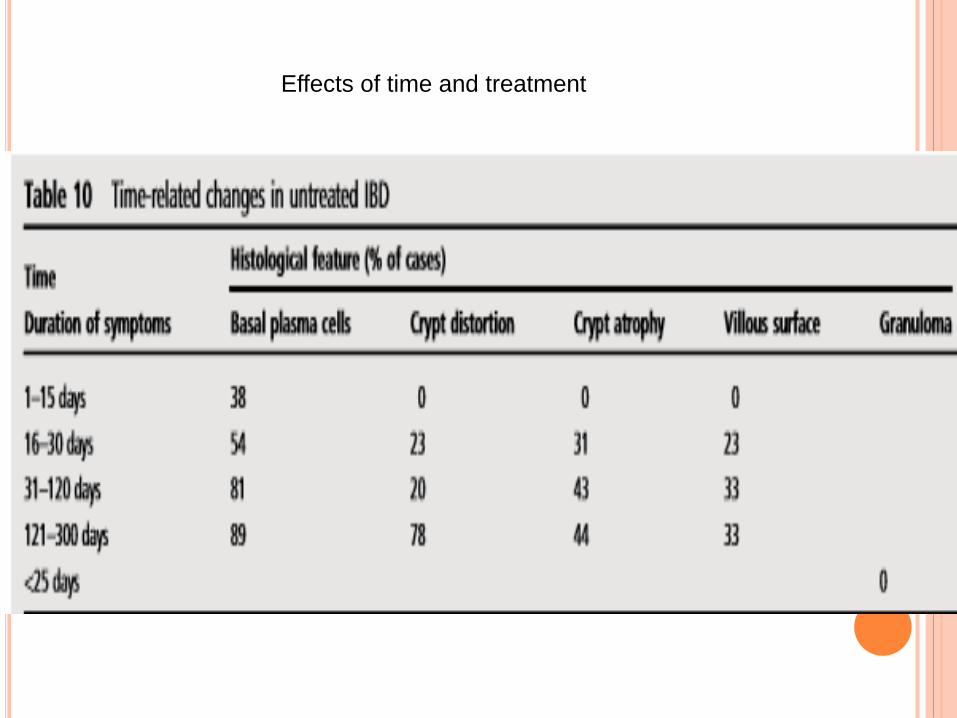
Effects of time and treatment
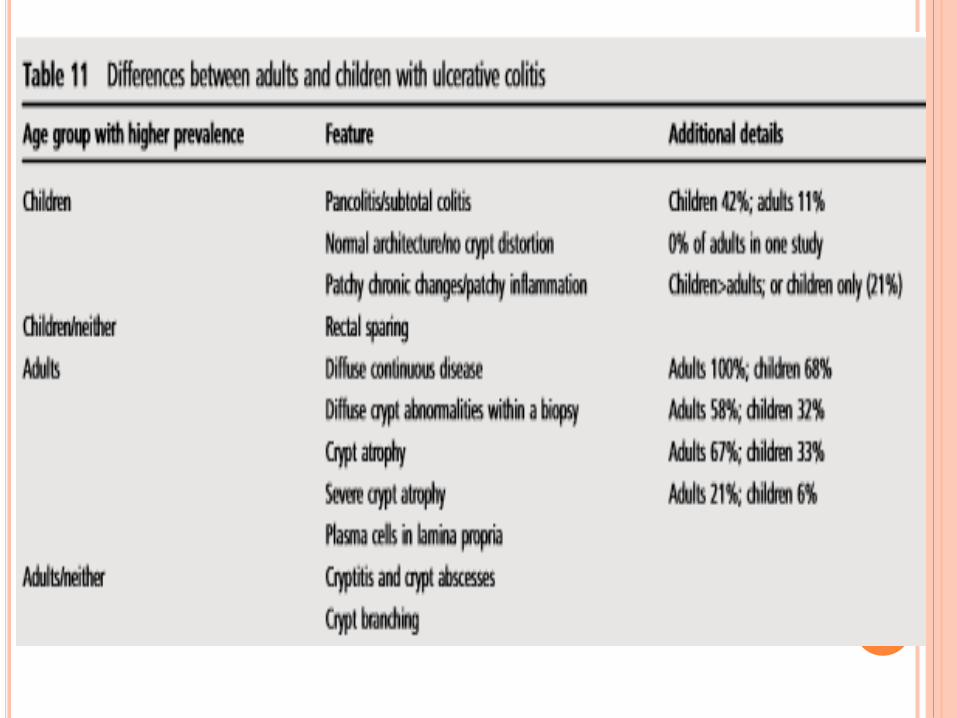
Pediatric UC
Children have higher prevalence of discontinuous disease
rectal sparing and pan colitis
Low prevalence of chronic histological changes
Upper GI involvement more in children
Ileal and upper gastrointestinal biopsies
Ileal biopsies:-
In setting of IBD ileal inflammation strongly favours CD over
UC.
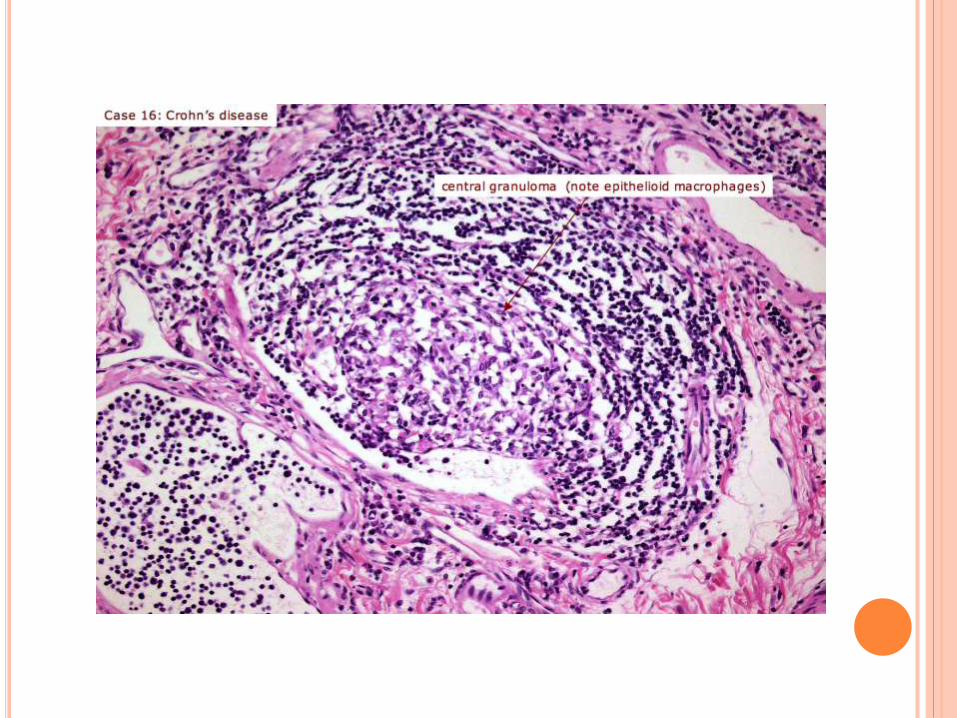
Granulomas[ non cryptolytic] in inflamed ileal biopsies help
discriminate CD from UC
Upper GI biopsies:-
CD> UC
GERD , H pylori to be excluded
In a setting of IBD upper GI granuloma favours CD over UC
- may raise the possibilities of new CD but caution is
advised
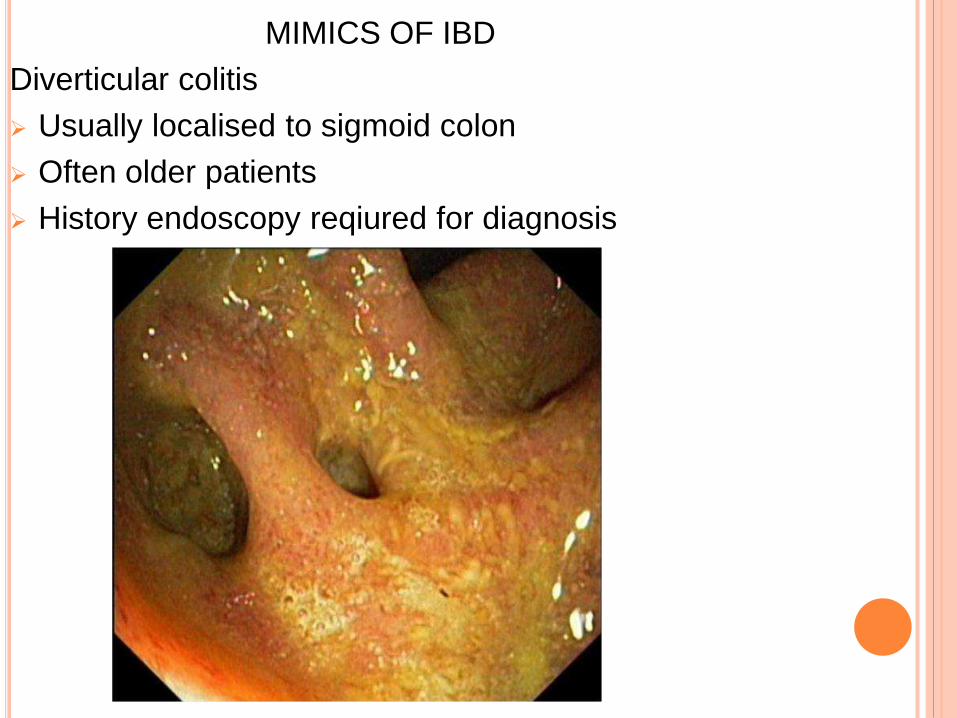
MIMICS OF IBD
Diverticular colitis
Usually localised to sigmoid colon
Often older patients
History endoscopy reqiured for diagnosis
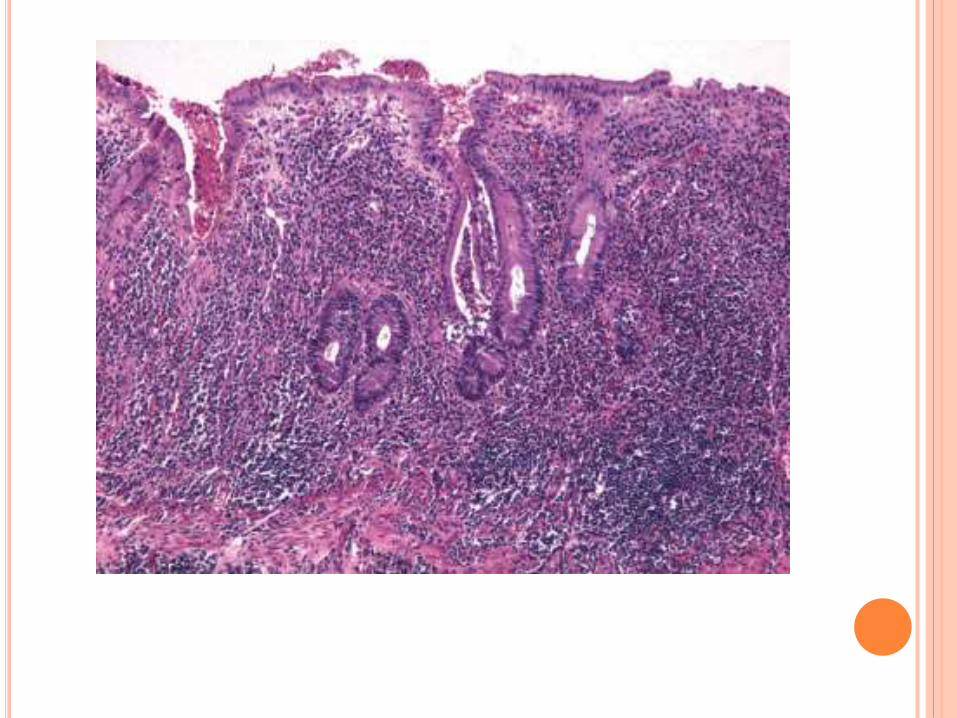
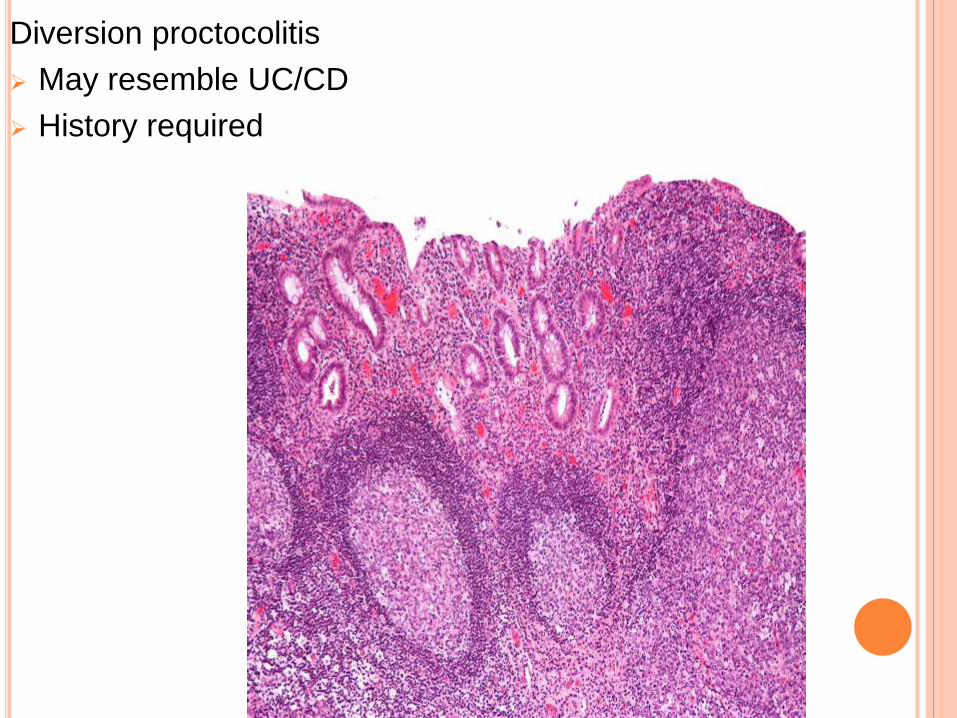
Diversion proctocolitis
May resemble UC/CD
History required
Ischaemic colitis
Basal plasma cells are absent
Mild acute inflammation
Hyalinisation of lamina propria and fibrosis are typical
Clinical picture and anatomic distribution helps to make
diagnosis
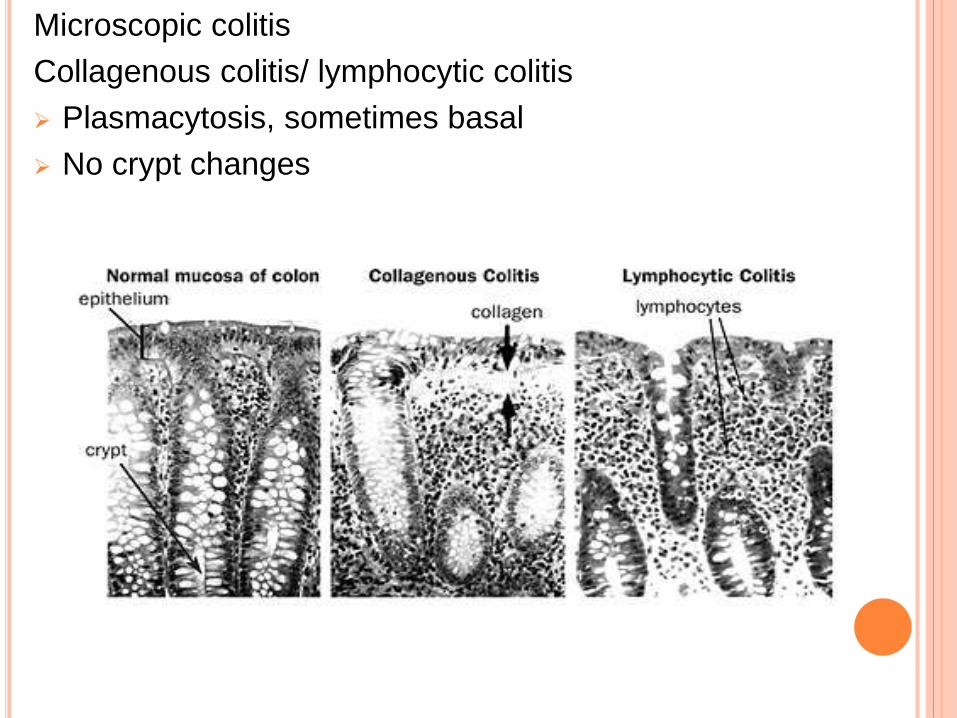
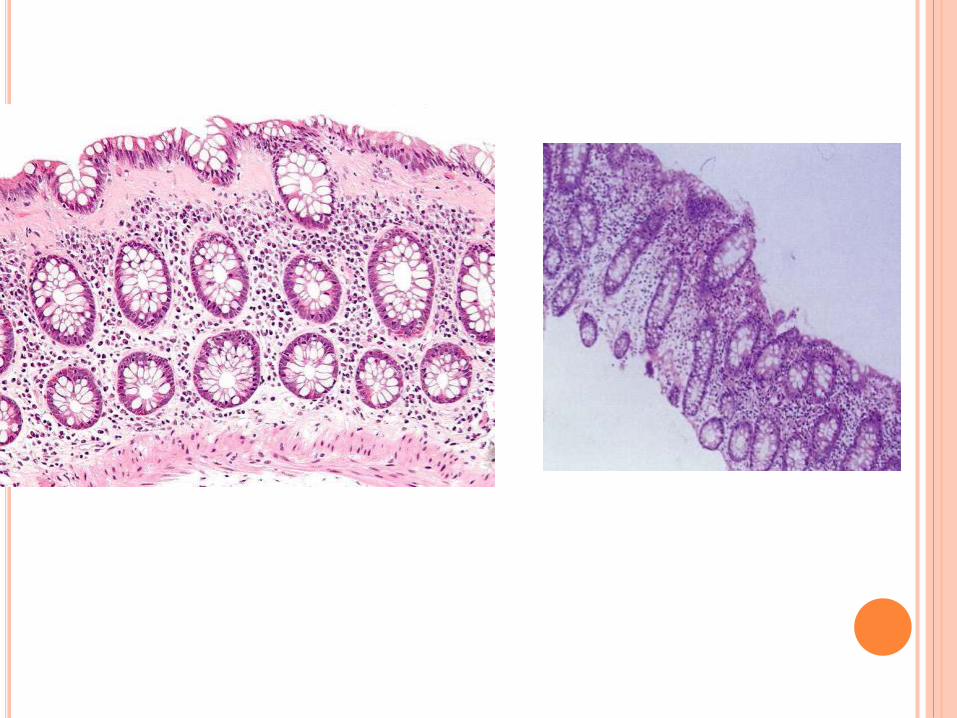
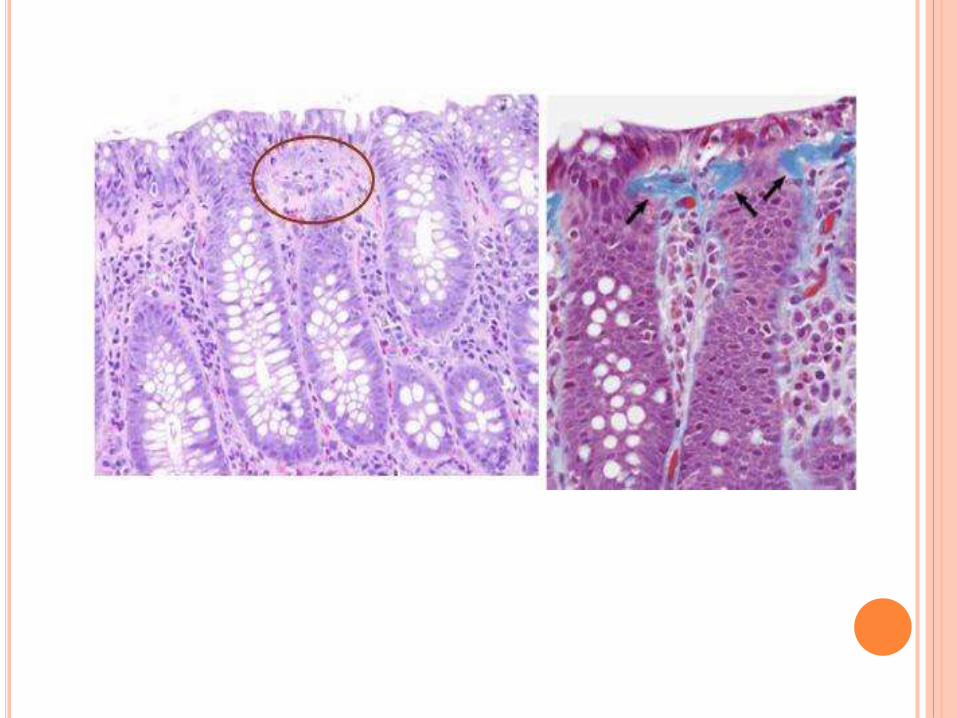
Microscopic colitis
Collagenous colitis/ lymphocytic colitis
Plasmacytosis, sometimes basal
No crypt changes
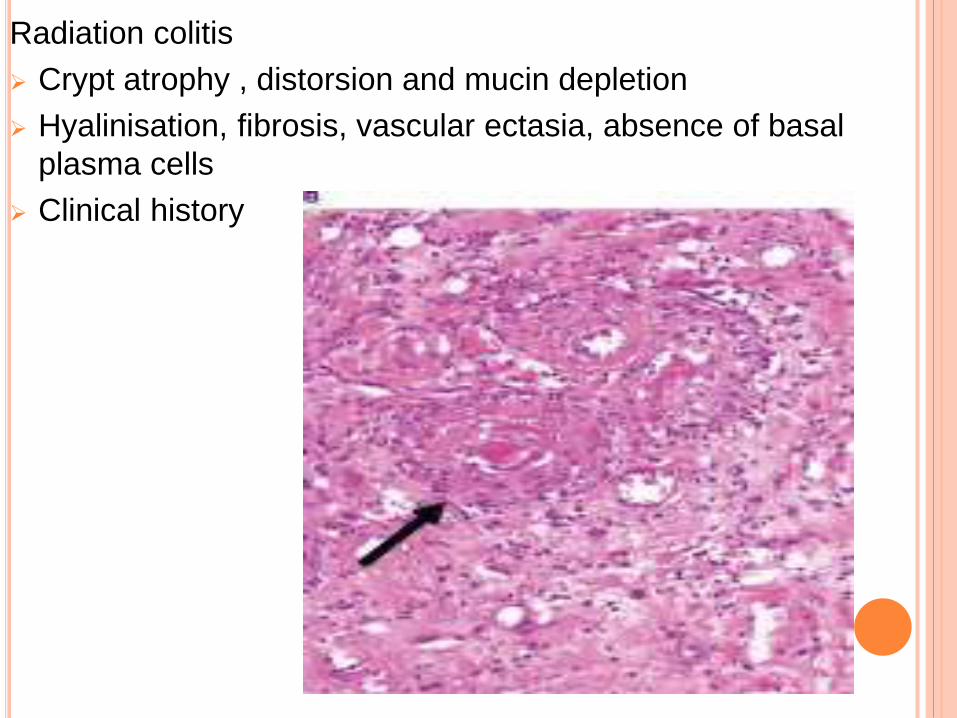
Radiation colitis
Crypt atrophy , distorsion and mucin depletion
Hyalinisation, fibrosis, vascular ectasia, absence of basal
plasma cells
Clinical history
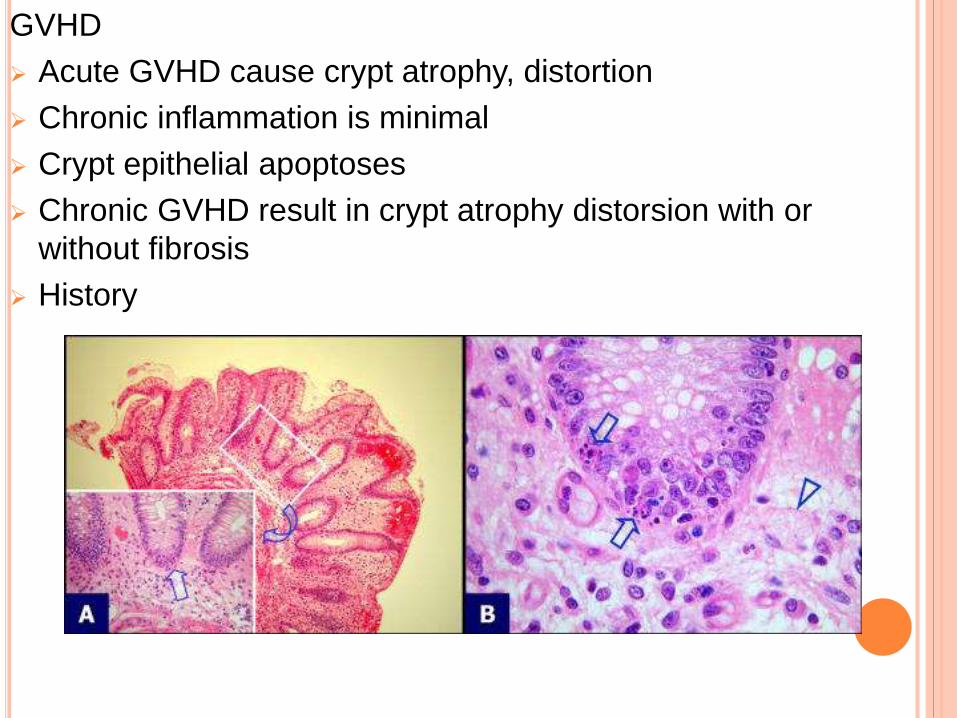
GVHD
Acute GVHD cause crypt atrophy, distortion
Chronic inflammation is minimal
Crypt epithelial apoptoses
Chronic GVHD result in crypt atrophy distorsion with or
without fibrosis
History
Mass lesion
Mucosa overlying intramural and subserosal mass may show
features IBD
Infections
LGV/ syphilis- may resemble CD
left sided > right
HIV/risk factors
Tuberculosis and yersinia
- -Caseous necrosis and demonstrable AFB indicate TB
- -langhans gaint cells, lymphoid cuff around granuloma and
granuloma > 4oomicrometer
- Additional to these presence of stellate abscess favours
yersinia
Drugs
NSAID colitis -
IBD like changes- crypt distortion , granulomas
Clues- epithelial cell apoptosis
increased intraepithelial lymphocytes
Mycophenolate mofetil
Can mimic IBD
But most often confused with GVHD than IBD
FOCAL ACTIVE COLITIS
Focal cryptitis/crypt abscess formation in the absence of other
changes
Represents – IBD, infection, ischaemia, drugs,other causes
It is not regarded as diagnoses
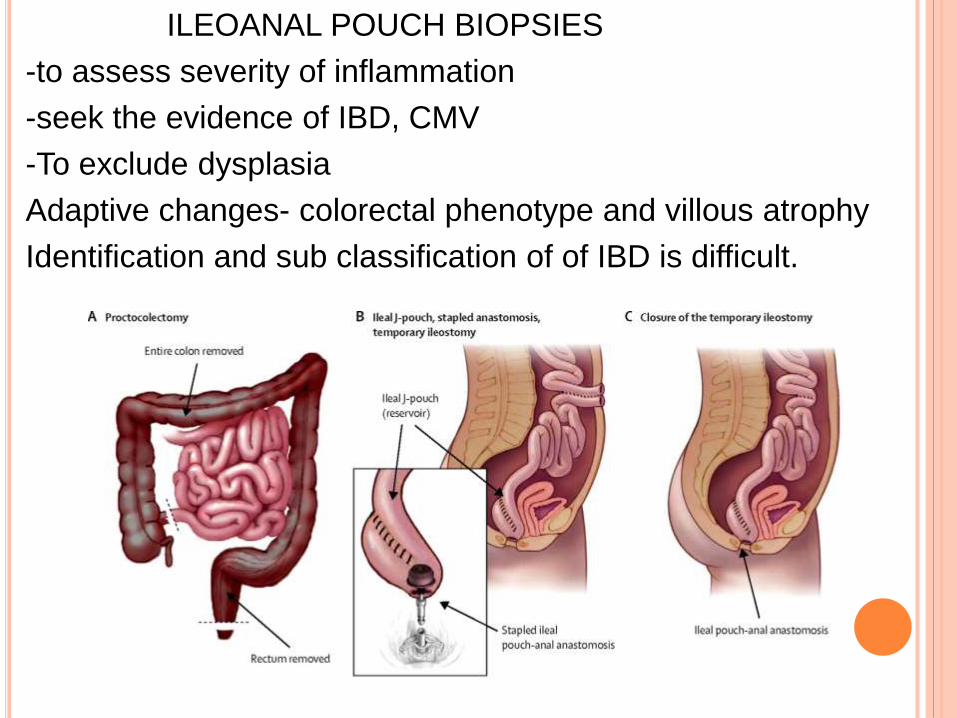
ILEOANAL POUCH BIOPSIES
-to assess severity of inflammation
-seek the evidence of IBD, CMV
-To exclude dysplasia
Adaptive changes- colorectal phenotype and villous atrophy
Identification and sub classification of of IBD is difficult.
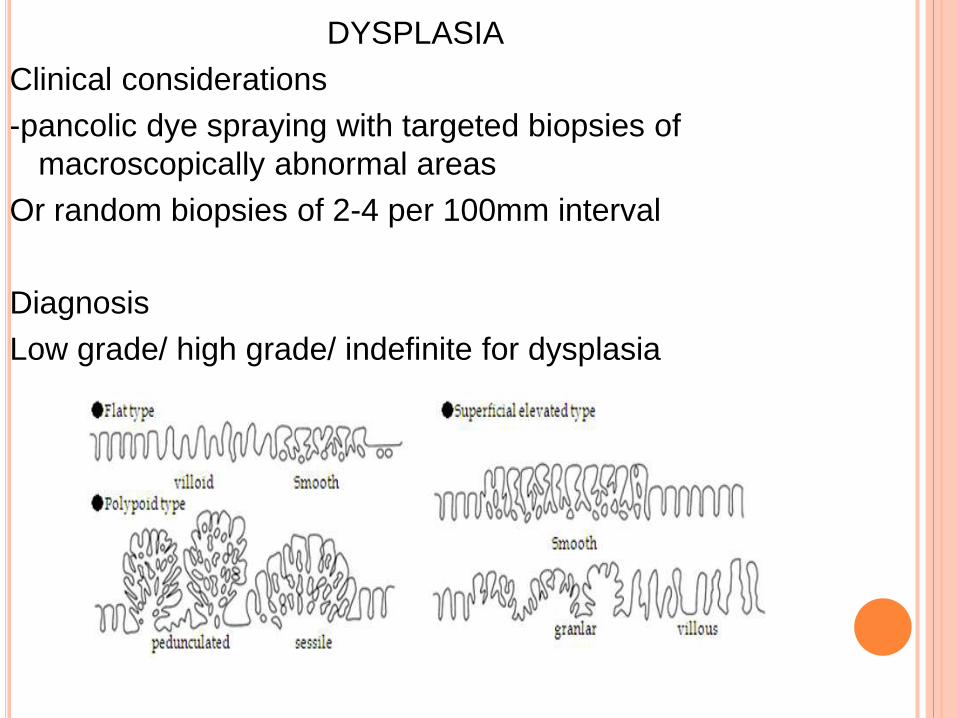
DYSPLASIA
Clinical considerations
-pancolic dye spraying with targeted biopsies of
macroscopically abnormal areas
Or random biopsies of 2-4 per 100mm interval
Diagnosis
Low grade/ high grade/ indefinite for dysplasia
Features favouring high grade dysplasia over low grade:
Cytological features-
Complete loss of nuclear polarity
Nuclei larger, more hyperchromatic, more stratified round
ovoid rather than pencil shaped
Mitoses is more
Architecturul changes are severe with cribriform areas
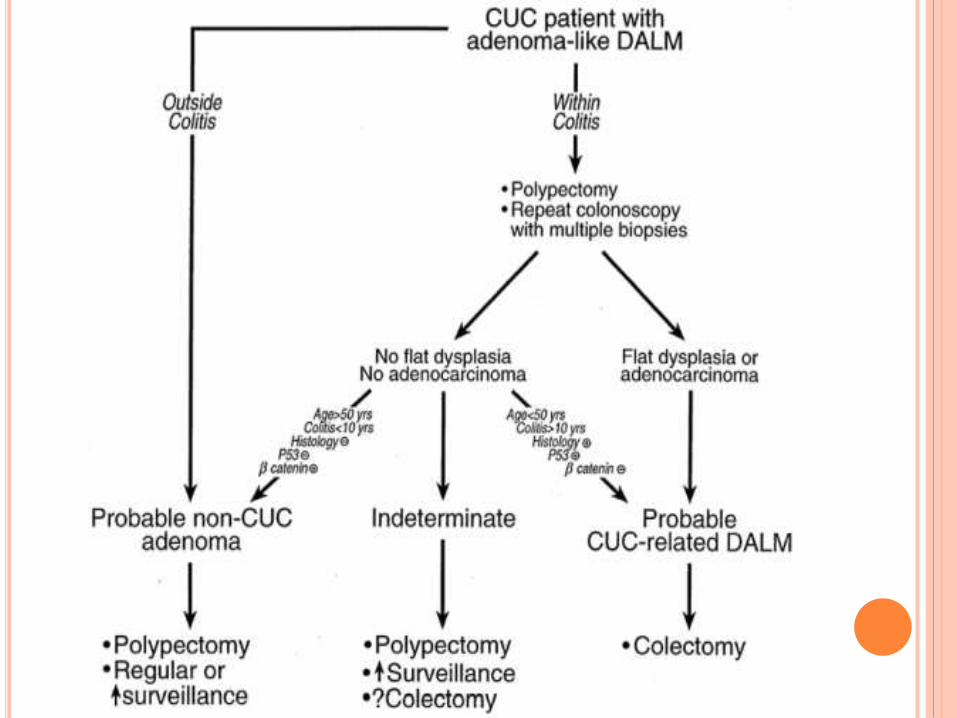
DALM vs adenoma
Depends on endoscopic features
Whether they are located inside or outside the area of IBD
Histology does not distinguish reliably between two
diagnoses
Dual reporting of dysplasia is recommended
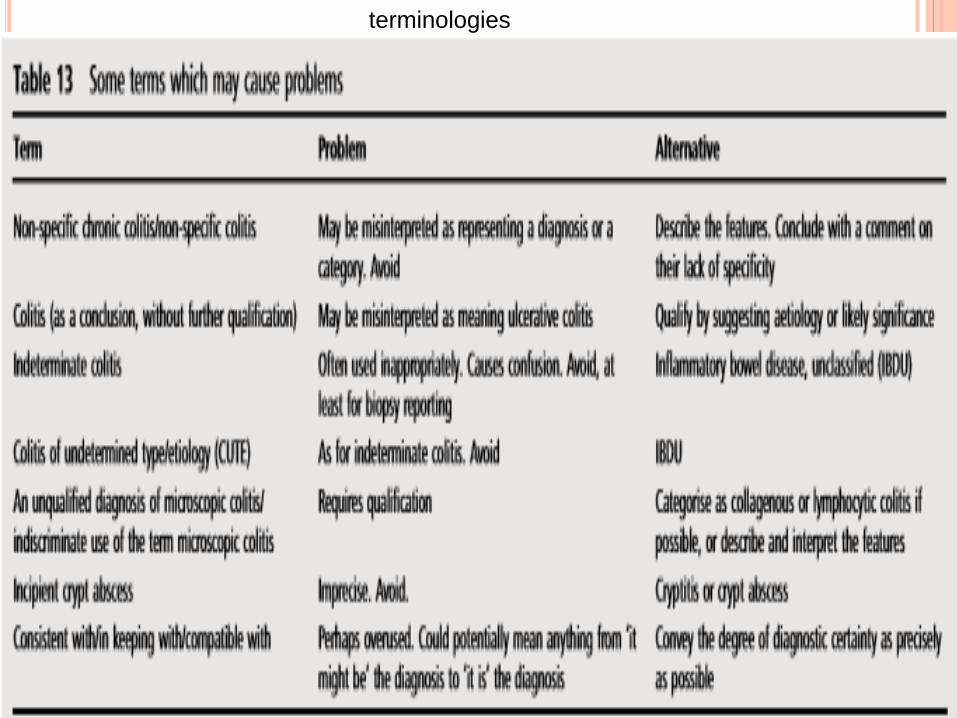
terminologies
REPORTING SCHEME FOR IBD BIOPSIES (PAID) Approach
and suggested scheme
The acronym ‘PAID’ is a suggested aide memoire for the
layout of the conclusion to an IBD biopsy report.
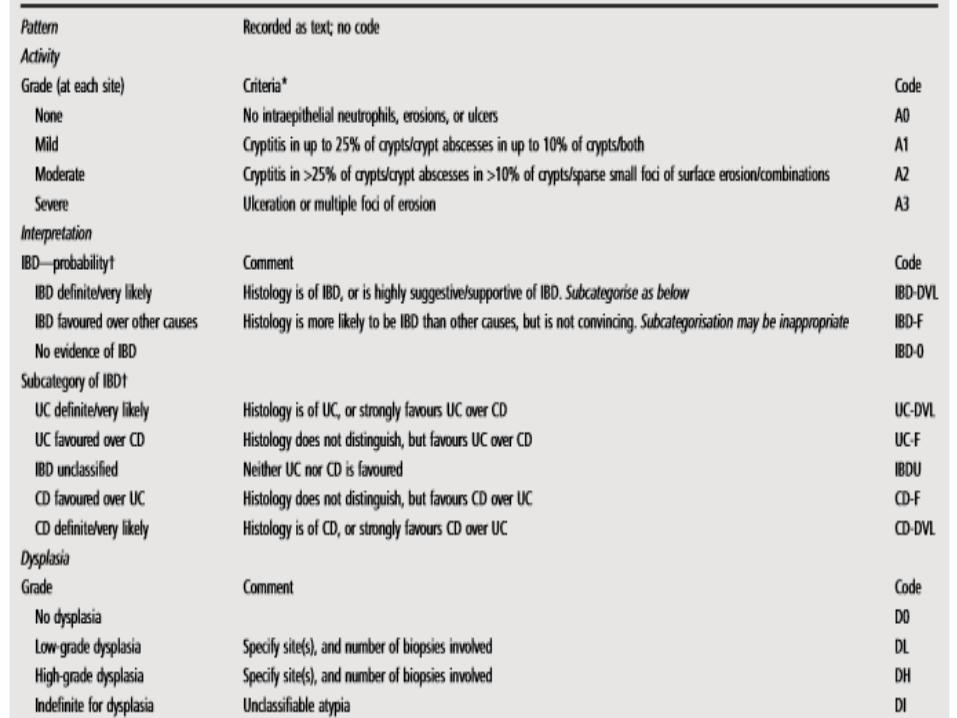
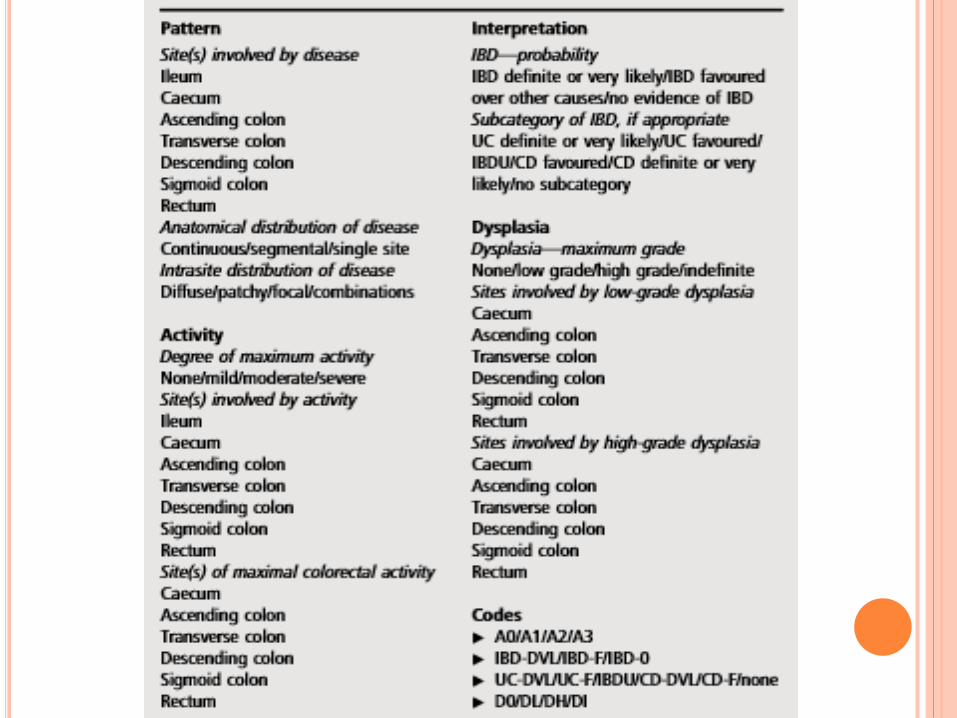
P- Pattern: of chronic changes: presence, distribution, extent
A - Activity: maximum grade, location
I- Interpretation: probability of IBD and, if relevant, probability
of UC or CD
D- Dysplasia: location, severity
SUMMARY
Remember
The context when dealing with colitis
Coherence when using terminologies
Corroborate histology with endoscopic findings
Communicate the inability of being more specific
Follow the recent guidelines to screen the high risk
individuals
Pathologist should assist the clinician in diagnosis to
implement appropriate treatment
References
Robbins and cotran pathologic basis of disease- 9th edition
Inflammatory bowel disease biopsies: updated British
Society of Gastroenterology reporting guidelines
Feakins RM. J Clin Pathol 2013;0:1–22.
doi:10.1136/jclinpath-2013-201885
Morson and dawsons gastrointestinal pathology
Pictures from journals of AJG
Thank You