rashmi mullur, md care: case-based clinical dgsom at ucla...
TRANSCRIPT

Integrative Diabetes Care: Case-based Clinical Application
Rashmi Mullur, MD
Associate Chief of Integrative Medicine
Greater Los Angeles VA Health System
Assistant Professor of Medicine
Division of Diabetes, Endocrinology, and Metabolism
DGSOM at UCLA

I have no financial conflicts of interest to disclose

“The practice of integrative holistic medicine integrates conventional and complementary therapies to promote optimal health and to prevent and treat disease by addressing contributing factors.”
--Mimi Guarneri, MD, FACC,
President, AIHM

Goals and Objectives
Understand the risks and benefits of mind-body techniques in the management of patients with DiabetesUnderstand
Identify the role of diet and micronutrient deficiencies in the management of diabetesIdentify
Assess the role of herbal and botanical supplements in addition to standard management of patients with DiabetesAssess

Caveat: Integrative techniques
• “Evolution”: – Former integrative approaches can evolve after years
of evidence and are now a part of standard medical care.• Vitamin D• Probiotics• B12 and metformin
• “The Entourage Effect”: – Herbal remedies are NOT the same as
pharmaceuticals and the proposed mechanism of action may be a result of the “active ingredient” as well as other non-measured compounds

Integrative Medicine Techniques• Whole Medical Systems:
– Traditional Chinese Medicine, Ayurveda, Homeopathy
• Mind-Body Medicine:
– Yoga, Tai-Chi, Meditation
• Nutrition
– Diet, Supplements, Additives
• Natural, Biologically Based Products
– Herbal/Botanical Medicine
• Manipulation and Body Based Practices
– Chiropractic Manipulation, Osteopathy
• Energy Medicine
– Healing Touch, Reiki, Light Therapy

Clarke TC et al. National health statistics reports; no 79. National Center for Health Statistics. 2015.
10 Most Common Integrative Modalities used by Adults, 2012

Top 6 Common Diseases for which CAIM techniques are used, 2012
Clarke TC et al. National health statistics reports; no 79. National Center for Health Statistics. 2015.

Case 1
• Mr. EM is a 32 yo man with a history of Type 1 Diabetes diagnosed at age 22. His glycemic control has been variable over the years, but it has certainly improved since he was started on an insulin pump.
• He has been prescribed a continuous glucose monitor in the past, but “it kept beeping” so he stopped using it.
• He is now in graduate school and he reports that he’s “stressed out constantly” and he can’t get his BG under control.
• His last A1c was 8.7%

Mindfulness
• Mindfulness is referred to as a mental state characterized by ‘full attention to internal and external experiences as they occur in the present moment’, and ‘an attitude characterized by non-judgment of, and openness to, this current experience.’
Kabat-Zinn et al. Journal of Behavioral Medicine, 8 (2) (1985), pp. 163–190

DiaMind Trial
• 139 outpatients with diabetes (type 1 or type 2) and low levels of emotional well-being (as evidenced by a score of <13 on the World Health Organization-5 Well-Being Index) were randomized to MBCT (n = 70) or a waiting list group (n = 69).
• Intervention:– 8 weekly 2-hour sessions in groups of 4 to 10 participants.
– 2-hour booster session 3 months after the end of the intervention
• Results:– MBCT was more effective in reducing stress (P < 0.001, Cohen d = 0.70), depressive symptoms
(P = 0.006, d = 0.59), and anxiety (P = 0.019, d = 0.44).
– MBCT was more effective in improving quality of life (mental: P = 0.003, d = 0.55; physical: P =0.032, d = 0.40).
– No significant effect on HbA1c or diabetes-specific distress
– Results were sustained at 6 months after intervention.
van Son, J., et al. BMC Public Health, 2011. 11: p. 131.van Son, J., et al. Diabetes Care, 2013. 36(4): p. 823-30.van Son, J., et al J Psychosom Res, 2014. 77(1): p. 81-4.

Friis AM et al. Diabetes Care. 2016 Jun 22
Mindfulness in Type 1 Diabetes

Friis AM et al. Diabetes Care. 2016 Jun 22
Mindfulness in Type 1 Diabetes

Diabetes-Related Distress
• Mindfulness and Mindful Awareness Practices have been shown to improve blood sugar control.
• A way to address DIABETES-RELATED DISTRESS!
Chicago Tribune online, 2-24-2017

Case 2:
• Mr. NF is a 67 yo man with a history of HTN, HL, poorly controlled Type 2 DM, and a recent CABG due to 3 v CAD who presents for f/u of his diabetes.
• He is watching his diet now and is taking all of his meds and his basal insulin. His morning FBG is now in the low 100s and all his post-prandial BGs are < 200.
• He is planning to start cardiac rehab.• He wants to know if he should start yoga because
he heard it was “good for his heart.”

Yoga for Diabetes
• A study of 123 DM2 patients, age 45-70 participated in a 3 month yoga intervention which involved 1 hour of active standing poses 3 times/week.
• There was no significant change in BP, but FPG, A1c, BMI, and markers of oxidative stress were improved at 3 months when compared to controls.
Hegde et al., Diabetes Care 34:2208–2210, 2011

Yoga for Lipids in Diabetic Patients
• 100 Dm2 patients, 52 males and 48 females, mean age = 45 participated in 1 hour of yoga (35 min postures, 10 min breathing, 15 min relaxation/meditation) daily for 3 months in addition to standard medical care.
Shantakumari et al. Indian Heart Journal. 65 (2013) 127-131

Yoga Effects on Blood Pressure
• Meta-analysis:– Yoga is associated with a
modest but significant reduction in blood pressure (≈4mmHg, systolic and diastolic).
• Subgroup analyses:– Larger, more clinically
significant reductions in BP if the yoga intervention included 3 basic elements:• Postures• Meditation• Breathing exercises
Hagins et al. Evid Based Complement Alternat Med. 2013; 2013: 649836.


BSR-Yoga for Diabetes
• A 10 minute gentle yoga-based program was developed at GLA, called Breathing, Stretching, Relaxation-Yoga.
• Pilot study recruited from the WLA-Diabetes clinic and randomize patients to the intervention arm (BSR) or control arm (information about yoga and general community-based classes at GLA).

Mullur RS, Ames D (2016) J Yoga Phys Ther 6: 224
BSR-Yoga for Diabetes


Case 3
• 66 yo man with hx of DM, HTN, CKD stage 2, and HL who is referred to clinic because he cannot tolerate statins.
• He has tried atorvastatin, simvastatin, and lovastatin. He complains of muscle pain with these medications
• Most recent lipid panel:– TChol 222, HDL 32, LDL 166, TG 199
• He wants to try Red Yeast Rice because he heard it was natural

Red Yeast Rice (RYR) (Monascus purpureus)
• The use of red yeast rice (RYR) has become very common as an alternative to statin therapies.
• RYR is produced by the red yeast that is grown on white polished rice. – It has been widely used in the
China as a food preservative, food colorant, and to make rice wine.
Nutrition Business Journal; 2009:44.A. Endo, et al. J Antibiot (1976), pp. 841–843

RYR Effectiveness
• In 2006, Liu et al. published a meta-analysis of 93 clinical trials.– Total cholesterol decreased by 35 mg/dl– LDL-cholesterol decreased by 28 mg/dl– TG decreased by 35 mg/dl– HDL-cholesterol increased by 6 mg/dl.
• Only one study conducted in the US:– Reported a 22% reduction of LDL-cholesterol after 12
weeks.
Liu et al. Chin Med. 2006 Nov 23;1:4Heber et al. Am J Clin Nutr February 1999 vol. 69 no. 2 231-236

Red Yeast Rice (RYR)• The fermentation of Chinese RYR produces a family
of monacolins. – Monacolin K, one of the produced monacolins from RYR, is the same
substance that is synthetically isolated from Aspergillus terreus and Food and Drug Administration (FDA) approved as lovastatin .
• The process of fermentation of RYR can largely impact the byproducts. – Citrinin is a mycotoxin produced by numerous Penicillium and
Aspergillus species.
– Citrinin has been shown to be nephrotoxic in animals with a reported median lethal dose (LD50) of 35 mg/kg.
– Citrinin in food colorants has been shown to be mutagenic at concentrations between 0.2 and 1.7 mg/g.
M.P. Bogsrud et al. Scand Cardiovasc J, 44 (2010), pp. 197–200 M. Sabater-vilar, et al. Mutation Red, 444 (1999), pp. 7–16

Red Yeast Rice• In 2007, the Food and Drug Administration (FDA) issued a consumer
warning to avoid RYR products because they may contain unauthorized drug (lovastatin)
• The FDA have no information on the number of RYR manufacturers and their compliance with CGMP regulations.
• In 2013, Childress et al. evaluated a total of 101 RYR products and NO PRODUCT could be confirmed as passing an independent lab verification!
• A 2017 study of 28 brands of red yeast rice supplements resulted in widely variable amounts of monacolin K. – Quantity ranged from 0.09 mg to 5.48 mg per 1200 mg of red yeast rice.
Childress et al. J Clin Lipidol. 2013 Mar-Apr;7(2):117-22Cohen et al. Eur J Prev Cardiol. 2017 Sep;24(13):1431-1434

RYR Summary• The amount of monacolin K is unknown in most available RYR
products.– FDA has determined that RYR products that contain more than trace
amounts of monacolin K are unapproved new drugs and cannot be sold legally as dietary supplements.
• Some red yeast rice products contain a contaminant called citrinin, which can cause renal failure.– Would advise against use in anyone with CKD
• Consumers have no way of knowing how much monacolin K is present in most red yeast rice products. – As a general rule, patients should be discouraged from buying RYR supplements in
the US.

What can we do for this patient?
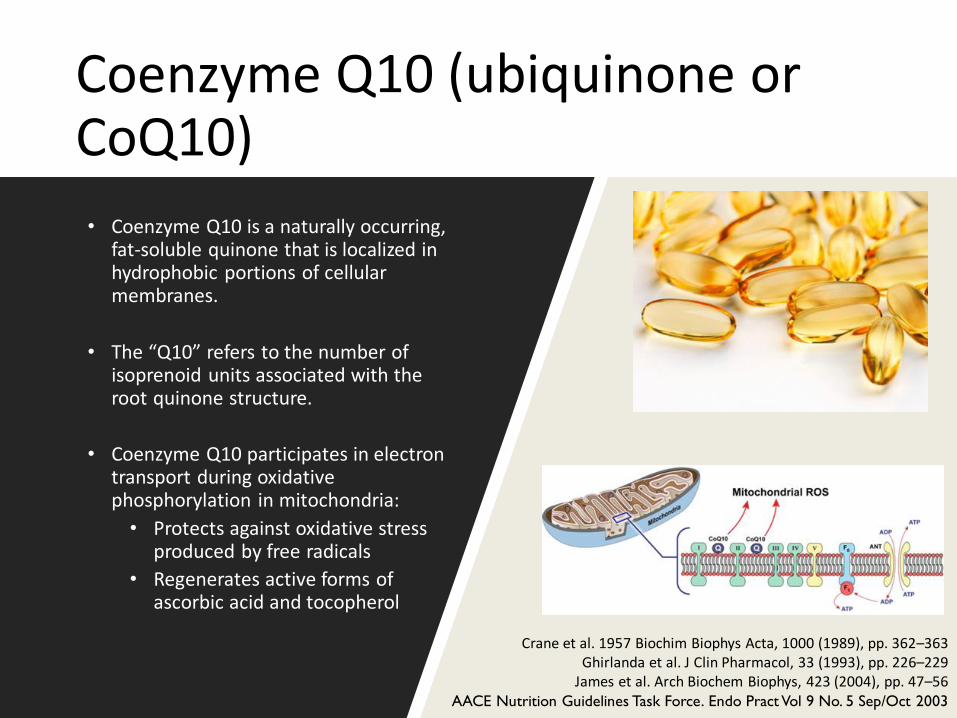
Coenzyme Q10 (ubiquinone or CoQ10)
• Coenzyme Q10 is a naturally occurring, fat-soluble quinone that is localized in hydrophobic portions of cellular membranes.
• The “Q10” refers to the number of isoprenoid units associated with the root quinone structure.
• Coenzyme Q10 participates in electron transport during oxidative phosphorylation in mitochondria:
• Protects against oxidative stress produced by free radicals
• Regenerates active forms of ascorbic acid and tocopherol
Crane et al. 1957 Biochim Biophys Acta, 1000 (1989), pp. 362–363Ghirlanda et al. J Clin Pharmacol, 33 (1993), pp. 226–229
James et al. Arch Biochem Biophys, 423 (2004), pp. 47–56AACE Nutrition Guidelines Task Force. Endo Pract Vol 9 No. 5 Sep/Oct 2003

Marcoff et al. Journal of the American College of Cardiology Volume 49, Issue 23 2007 2231 - 2237
Mevalonic Acid Pathway
Treatment
EffectSide Effect

Statin-Associated Myopathy
• Depletion of Coenzyme Q10 in muscle cells is thought to be one mechanism associated with statin-induced myopathy.
• Patients receiving statin therapy have been shown in most studies to have decreased serum concentrations of CoQ10 (from 16% to 54%).
Marcoff et al. Journal of the American College of Cardiology Volume 49, Issue 23 2007 2231 - 2237

CoQ10 Levels Decrease After Treatment With Statins
Study Intervention Duration Participants %Change
Elmberger et al. (RCT) Pravastatin20-40 mg/day 12 weeks12 patients with
heterozygous FH<, age 19-65
(-) 29
Ghirlanda et al. (RCT)Pravastatin, 20 mg/day
3 months
10 hypercholesterolemic patients, age 47 ± 8 yrs
(-) 50
Simvastatin, 20 mg/day10 hypercholesterolemic
patients, age 49 ± 10 yrs(-) 54
Bargossi et al. (RCT) Simvastatin, 20 mg/day 3 months34 patients with primary
hypercholesterolemia, age not reported
(-) 22.3
Davidson et al. (RCT)
Atorvastatin, 10-20 mg/day
1 yr
1049 patients with primary
hypercholesterolemia, age 18-80 yrs
(-) 38
Lovastatin, 20-40 mg/day (-) 27
Mortensen et al. (RCT)Lovastatin, 20-80 mg/day
18 weeks45 hypercholesterolemic patients, age 35-75 yrs
(-) 28.8
Pravastatin, 10-40 mg/day
(-) 19.7
De Lorgeril et al. (RCT) Simvastatin, 20 mg/day 12 weeks
32 patients with primary hypercholesterolemia
and previous Q-wave MI, mean age 54.1 yrs
(-) 19.4
Bleske et al. (RCT)Pravastatin, 20 mg/day
4 weeks12 healthy volunteers,
age 26 ± 5 yrs
NS
Atorvastatin, 10 mg/day NS
Jula et al. (RCT) Simvastatin, 20 mg/day 12 weeks120
hypercholesterolemic men, age 35-64 yrs
(-) 22
Berthold et al. (RCT) Simvastatin, 40 mg/day 2 weeks24 healthy men, age 31.9
± 8.8 yrs(-) 16
Adapted from Marcoff et al. Journal of the American College of Cardiology Volume 49, Issue 23 2007 2231 - 2237

Coenzyme Q10 Supplementation
• Bookstaver et al assessed the effect of CoQ10 supplementation on myalgias presumed to be caused by statins in 76 patients.– Included patients receiving a statin who developed new-onset myalgias in >2
extremities within 60 days of initiation or a dosage increase
– Patients continued statin therapy and were randomized to either CoQ10 60 mg twice daily or placebo for 3 months.
– Patients completed a 10-cm visual analog scale (VAS) and the Short-Form McGill Pain Questionnaire at baseline and at each monthly visit.
• CoQ10 did not produce a greater response than placebo in the treatment of presumed statin-induced myalgias.
Bookstaver et al. Am J Cardiol 2012;110:526 –529)

Coenzyme Q10 Supplementation
• Two other studies previously published also reported conflicting results on the use of CoQ10 supplementation
• The first study, used CoQ10 100 mg/day in 32 patients and showed that pain inventory scores decreased.
• In the second study, 44 patients experiencing myalgiaswith statins were d/c off meds for 2 weeks and then randomized to either CoQ10 200 mg/day or placebo, at which point simvastatin was reintroduced.
• The investigators reported no significant difference between the groups in the myalgia score.
Caso et al. Am J Cardiol 2007;99:1409 –1412.
Young et al. Am J Cardiol 2007;100:1400–1403.

Variable Outcomes with CoQ10
• CoQ10 dosage and bioavailability is not standardized.
• Recently, genomic variations have been evaluated with respect to inter-individual differences in response to statin therapy, both in terms of LDL-lowering and clinical outcomes
• A case report suggested that two siblings with statin intolerance also had primary CoQ10 deficiency:
– Each was homozygous for a missense mutation in the COQ2 gene encoding para-hydroxybenzoate-polyprenyl transferase which is the second enzyme in the CoQ10 biosynthetic pathway.
Maitland-van der Zee et al. Curr Atheroscler Rep 2005, 7(3):204-208.Quinzii C et al. Am J Hum Genet 2006, 78(2):345-349.

Case 3 Follow Up: RYR/CoQ10 Summary
• Advised pt NOT to take RYR, especially given CKD
• CoQ10 is relatively well tolerated and has very little risk of toxicity.– Rx CoQ10 200 mg Qday
• Started on Hydrophilic statin (prava, rosuva) that had less metabolism by CYP3A4 (prava, fluva, pitava)– Pravastatin 20 mg

Case 4
• A 55 yo man with history of obesity, CAD, OSA, HTN, HL, and poorly controlled DM2 is referred to the clinic because his “insulin isn’t working.”
• He heard about studies with cinnamon for diabetes and wants to know if this would help him.
• DM Hx:– Dx in 2013 with sx of polyuria, polydipsia, polyphagia with A1c =8%.– Initially on metformin and glipizide, but A1c trended up so glargine was added
within 6 months– In 2015, referred to DM clinic b/c his A1c is > 11%; started on basal/bolus
regimen– In 2016, pt had gained weight on insulin (BMI = 35.4%) and his A1c was still >
9%. Given a trial of liraglutide + insulin– Pt could not tolerate the liraglutide is now taking Glargine 45 units BID, Aspart
30 TID/AC and metformin 1 gm BID

Cinnamon
• Cinnamon contains biologically active substances that have demonstrated insulin-mimetic properties.
• Enhances glucose uptake by activating insulin receptor kinase activity, autophosphorylation of the insulin receptor, and glycogen synthase activity in both in vitro and in vivo studies
• Cinnamon has also been shown to reduce lipid levels in fructose-fed rats, potentially via inhibiting hepatic HMG-CoA reductase activity
Jarvill–Taylor KJ et al. J Am Coll Nutr 20:327–336, 2001Qin B et al. Diabetes Res Clin Pract 62:139–148, 2003
Khan A et al. Diabetes Care 26:3215–3218, 2003

Cinnamon
• A meta-analysis by Baker et al evaluated five clinical trials (n = 282 subjects, follow-up 5.7–16.0 weeks). – All used cinnamomum cassia, and doses from 1-6 gm.
– Median duration of treatment and follow-up was 12 weeks
– Results: cinnamon did not demonstrate statistically or clinically significant changes in A1C, FBG, or lipid parameters in comparison with subjects receiving placebo.
– Discrepancy:• ? Power: probably needed > 1000 patients.
• Ethnic/dietary/baseline differences in Khan’s study.
• Included trials with type 1 DM
Baker et al. Diabetes Care. 2008 Jan;31(1):41-3

Cinnamon Summary
• Cinnamon does not appear to show consistent benefit in patients with Diabetes.
• Cinnamon appears to be safe for most people when taken by mouth in amounts up to 6 grams daily for 6 weeks or less.
– ? Allergic reactions to cinnamon or its parts.
• Cassia cinnamon contains coumarin

Is there another nutraceutical that may be useful for this patient?

Chromium
• 1970s Case Report:
– A patient receiving TPN developed severe hyperglycemia and weight loss, refractory to increasing insulin doses.
• Supplemented with chromium (150-200 mcg) and within 2 weeks, signs and symptoms of diabetes improved with markedly improved glycemic status and greatly reduced insulin requirements (45 u TDD 0!!)
• Subsequent studies report beneficial effects of chromium in patients receiving TPN, and it is now routinely added.
Jeejeebhoy KN et al. Am J Clin Nutr 30:531–538, 1977Anderson RA. Nutrition 11:83–86, 1995

Chromium: Mechanism of Action
• Chromium activates the insulin receptor via phosphorylation of the insulin receptor kinase
• Chromium also inhibits phosphotyrosine phosphatase, the enzyme that cleaves phosphate from the insulin receptor.
• Dual role: – Activation of insulin receptor
kinase – Inhibition of insulin receptor
phosphatase
Davis CM et al. Biochemistry 35:12963–12969, 1996Cefalu and Hu. Diabetes Care November 2004 vol. 27 no. 11 2741-2751

Chromium Supplementation in Diabetes
• >60 published articles on chromium supplementation and diabetes in humans with variable results.
• Quality of study, dose, source, subject selection
• Balk et al. published a meta-analysis of 14 studies of variable quality but concluded that “among participants with type 2 diabetes, chromium supplementation improved HbA1c levels by 0.6%
Balk EM et al. Diabetes Care2007, 30:2154–2163. .

Chromium Summary
• Dose: Chromium picolinate 1000 mcg
• No consistent effect of chromium supplementation to improve insulin action or glycemic control across all the reported study cohorts.
• Clinical response to chromium may be more likely in insulin-resistant individuals with type 2 diabetes who have more elevated fasting glucose and HbA1c levels
Case 5
• Ms. MV is a 54 yo female with a strong family history of diabetes and an A1c = 5.7%.
• She is very concerned because her PCP told her she has “prediabetes” and she wants to avoid “drugs”.
• She wants to discuss herbal remedies that she can use to prevent diabetes
• She has already met with an RD and is working on counting carbohydrates.

Berberine
• Berberine is an ammonium salt found in the roots, rhizomes, stems, and bark of several different plant species
• Goldenseal, yellow root, barberry, etc
• It is a plant alkaloid that has a long history of use in Ayurvedic and Chinese medicine
• A 2008 study published in JCEM revealed that 1 gm berberine decreased body weight, fasting and post-prandial glucose, Tchol, LDL, TG, and resulted in a 0.9% A1c change.
Zhang et al. JCEM 2008 Jul;93(7):2559-65

Berberine
• Mechanism of action is thought to be via AMPK activation
• Source of extract is key• Can be associated with P450 drug interactions
• As an alkaloid compound, need to monitor LFTs.
Zhang et al. JCEM 2008 Jul;93(7):2559-65

Apple Cider Vinegar
• Two small studies from Diabetes Care:
– Initial study: Apple cider vinegar prior to a high CHO meal
• Patients with prediabetes had lower post-prandial rise in BG and a higher insulin response to the meal
– Same group evaluated use of apple cider vinegar prior to an HS snack in patients with Type 2 DM
• Patients taking apple cider vinegar had lower AM FBG.
Johnston et al. Diabetes Care. 2004 Jan;27(1):281-2White and Johnston. Diabetes Care 2007 Nov; 30(11): 2814-2815

Apple Cider Vinegar
• Proposed mechanism of action:
• Delay gastric emptying rating
• Acetic acid in vinegar can suppress disaccharidaseactivity and may work in a similar fashion as Acarbose.
Johnston et al. Diabetes Care. 2004 Jan;27(1):281-2White and Johnston. Diabetes Care 2007 Nov; 30(11): 2814-2815

Case 5 Follow UpPatients with Prediabetes
• Monitor LFTs if patients are taking berberine
• Counseled on the Mediterranean diet
• Apple Cider Vinegar is generally considered safe if patients are not on insulin or a sulfonylurea.

Summary
• Integrative medicine is more than simply incorporation of mind-body techniques
• Integrative medicine is not “an alternative” to traditional therapies.
• Herbal remedies for diabetes do have some therapeutic role and a careful discussion of the risks/benefits should be individualized to the patient.