quiz cardiovascular part 2 of 3
DESCRIPTION
Quiz Cardiovascular Part 2 of 3TRANSCRIPT

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 1 -
Cardiology #1 – Cardiac Function & Circulatory Control
1.1) Which of the following is NOT true regarding cardiac muscle?
a) Fibers exhibit cross-striation and densely staining cross-bands
b) Large mitochondria and glycogen stores are adjacent to each myofibril
c) The cardiac muscle nucleus lies in the center of each cell
d) The subendocardial layer has an impulse-conducting system
e) The endocardium is the principle component of the cardiac muscle
1.2) Which of the following is considered a lateral, not transverse, component of cardiac
muscle?
a) Fascia adherens – binds to form the functional cardiac fiber
b) Macula adherens – prevents cells from pulling apart
c) Gap junctions – provides ionic continuity for syncytium behavior
2.1) Sarcoplasmic reticulum Ca++ ATPase (SERCA) activity is regulated by which of the
following?
a) Na+ release
b) Electrical depolarization
c) Phospholamban
d) Ca++ binding to troponin C
e) Actin/myosin interactions
2.2) Which of the following is most responsible for extruding Ca++ to maintain
homeostasis on a beat-to-beat basis?
a) SERCA
b) Ca++ ATPase proteins
c) Cardiac glycosides
d) Na+/Ca++ exchanger
e) Na+/K+ pump
3) Increased contractility, according to the Frank-Starling Law, is most dependent on:
a) Afterload
b) Preload
c) Heart rate
d) Pulse pressure
e) Ca++ absorption
4) During which phase(s) of the cardiac cycle is the mitral valve open?
a) Isovolumic contraction and filling phase
b) Ejection phase and isovolumic relaxation
c) Isovolumic relaxation and isovolumic contraction
d) Filling phase and ejection phase
e) None of the above
5.1) If total peripheral resistance (afterload) is increased, which of the following will also
increase?
a) Heart rate
b) Ejection fraction
c) Cardiac output
d) Stroke volume
e) Peak pressure
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 2 -
5.2) Which of the following is true of the end-diastolic force-length relationship
(EDFLR) and the end-systolic force-length relationship (ESFLR) when a patient is given
epinephrine (positive inotropic agent)?
a) EDFLR and ESFLR will increase
b) EDFLR will increase with little effect on ESFLR
c) ESFLR will increase with little effect on EEFLR
d) EDFLR and ESFLR will decrease
e) There will be little effect on both EDFLR and ESFLR
6) Which of the following determinants of cardiac performance is defined by sarcomere
stretching?
a) Preload
b) Afterload
c) Heart rate
d) Contractility (ventricular)
7) Which of the following is used clinically as a practical means to index the strength of
the heart? TPR = MAP – CVP / CO
a) Stroke volume
b) Ejection fraction
c) Cardiac output
d) Total peripheral resistance
e) Central venous pressure
8) Which of the following is NOT true regarding cardiovascular response to exercise?
a) Oxygen consumption increases about 18-fold and CO increases 6-fold
b) Venous oxygen saturation decreases from 75% to 25%
c) Arterial dilation is a result of released potassium and other vasodilators
d) Preload remains constant throughout exercise
e) Vagal tone is withdrawn and sympathetic drive is increased
9) Which of the following is NOT an age-related change to the cardiovascular system?
a) Sympathetic response to exercise decreases
b) Cellular hypertrophy occurs
c) Coronary perfusion decreases
d) Large arteries stiffen
e) Chronotropic and inotropic response to sympathetic mediation decreases
Cardiology #2 – Osteopathic Considerations in Cardiovascular Medicine
1.1) A patient presents with a myocardial infarction. After pharmacologic treatment has
been started, manipulative procedures can further decrease oxygen and energy demands.
Manipulation at which of the following areas would NOT be helpful?
a) T3
b) T7
c) T4
d) OA
e) AA
1.2) In patients presenting with arrhythmias or palpitations, somatic dysfunctions of what
vertebral areas should be treated?
a) T1-T4

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 3 -
b) T2-T8
c) T1-L2
d) T1-T6
e) T2-T5
1.3) A patient with an anterior wall myocardial infarction is likely to have paraspinal
musculoskeletal changes at which of the following levels?
a) C2 and the cranial base on the left
b) T1-T4 on the left
c) T5-T7 on the right
d) T9-T12 on the left
e) L1-L2 on the right
1.4) Supraventricular tachyarrhythmias that have been associated with hypersympathetic
activity are most likely to arise from:
a) Right sided sympathetic fibers originating from T1-T4
b) Left sided sympathetic fibers originating from T2-T5
c) Left vagus nerve
d) Pre-ganglionic fibers originating from the cervical chain ganglia
e) Stimulation of the oculocardiac reflex
2) What pattern of somatic dysfunction has been demonstrated in a significant percentage
of hypertensive patients?
a) OA, AA, and T6
b) C2, T1, and T7
c) C6, T2, and T6
d) C6, T1, and T3
e) OA, AA, C2, C6, and T1-T4
Cardiology #3 – Epidemiology of Cardiovascular Disease
1) Which of the following is NOT an immutable (unmodifiable) risk factor for coronary
artery disease (CAD)?
a) Race and gender
b) Family history
c) Homocysteine
d) Older age
2) Which of the following lipid and lipoprotein parameter equations is used to evaluate
dyslipidemia and is the best predictor of coronary artery disease risk in the general
population? VLDL = very-low density lipoprotein, HDL = high density lipoprotein
a) (LDL + VLDL + HDL) / HDL
b) (LDL + VLDL + HDL) / LDL
c) (LDL + VLDL + HDL) / VLDL
d) (HDL – VLDL + LDL) / HDL
e) (HDL – VLDL + LDL) / LDL
3.1) Regarding cardiovascular disease, short-term benefit of intervention is much greater
in ____ prevention and interventions with hazards are of greater importance in ____
prevention.
a) Primary; Primary
b) Primary; Secondary

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 4 -
c) Secondary; Secondary
d) Secondary; Primary
3.2) Which of the following is considered an atherosclerotic cardiovascular disease?
a) Valvular heart disease
b) Congenital heart disease
c) Myocardial disease
d) Electrophysiologic disorders
e) Peripheral vascular disease
Cardiology #4 – Approach to the Patient with Possible Cardiovascular Disease
1.1) A patent presents with retrosternal squeezing pain. Their pain had been temporarily
relieved by nitroglycerin in the ambulance. Physical exam reveals an S3 sound and a
slight murmur. Which of the following characteristics would differentiate this as either
stable or unstable angina?
a) Location of pain
b) Quality of pain
c) Onset and duration
d) Aggravating and relieving factors
e) Associated symptoms anf signs
1.2) A patient presents with substernal pressing pain and dyspnea. History reveals pain
and dyspnea is aggravated by effort and that the onset was slow. Which of the following
is most likely?
a) Myocardial infarction
b) Pericarditis
c) Aortic dissection
d) Pulmonary embolism
e) Pulmonary hypertension
1.3) A patient presents with knife-like pain over the sternum. Although the pain has
lasted many hours, the patient was reluctant to come to the hospital. Physical exam
reveals pain increases with deep breathing and auscultation reveals a rubbing sound.
Which of the following is most likely?
a) Myocardial infarction
b) Pericarditis
c) Aortic dissection
d) Pulmonary embolism
e) Esophageal reflux
1.4) A patient presents with excruciating pain on the anterior chest that developed
suddenly. History reveals the patient has not been taking their hypertension medication.
Physical exam reveals blood pressure asymmetry and neurologic defect of a lower limb.
Which of the following is most likely?
a) Myocardial infarction
b) Pericarditis
c) Aortic dissection
d) Gallbladder disease
e) Pulmonary hypertension

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 5 -
1.5) A patient presents with substernal squeezing pain. The ambulance staff notes say the
patient was found diaphoretic, dyspneic, and that nitroglycerin had no effect on pain.
Which of the following is most likely?
a) Myocardial infarction
b) Pericarditis
c) Aortic dissection
d) Pulmonary embolism
e) Pulmonary hypertension
1.6) A patient presents with left-sided substernal burning pain that began immediately
while they were on a business flight. Physical exam reveals pain with deep breathing,
dyspnea, and tachycardia. Which of the following is most likely?
a) Myocardial infarction
b) Pneumonia
c) Pneumothorax
d) Pulmonary embolism
e) Pulmonary hypertension
1.7) Which of the following is true of the distribution of a herpes zoster vesicular rash?
a) Follows hair pattern
b) Follows tension lines
c) Follows dermatome
d) Contained within a bone distribution
e) Contained within a muscle distribution
1.8) A patient presents with sharp, left-sided pain that began during a Judo match.
Physical exam reveals dyspnea, hyper-resonance on the left side, and no jugular vein
distension (JVD). You ask for a chest tube kit since the patient most likely has:
a) Pulmonary embolism
b) Pneumonia with pleurisy
c) Pulmonary hypertension
d) Myocardial infarction
e) Spontaneous pneumothorax
1.9) A patient presents with left-sided pain localized to the area of the 7th rib. Physical
exam reveals a fever, cough, and dull percussion over the localized area. Auscultation
reveals bronchial breath sounds. Which of the following is most likely?
a) Pulmonary embolism
b) Pneumonia with pleurisy
c) Pulmonary hypertension
d) Myocardial infarction
e) Spontaneous pneumothorax
1.10) A patient presents with aching pain over the chest. The area is tender to pressure
and painful with movement. History reveals the patient was helping a friend move when
the episode began. Which of the following is most likely?
a) Musculoskeletal disorder
b) Gallbladder disease
c) Anxiety state
d) Pulmonary embolism
e) Myocardial infarction

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 6 -
1.11) A patient presents with a substernal burning sensation that lasts for a few hours per
episode. History reveals the symptoms are not associated with food, but drinking milk
helps relieve the pain. Which of the following is most likely?
a) Musculoskeletal disorder
b) Gallbladder disease
c) Anxiety state
d) Peptic ulcer
e) Esophageal reflux
1.12) An obese patient presents with a substernal burning sensation that starts after eating
a large meal. History reveals the symptoms only last for a 30 minutes and sometimes the
patient has water brash. Which of the following is most likely?
a) Pneumonia with pleurisy
b) Gallbladder disease
c) Anxiety state
d) Peptic ulcer
e) Esophageal reflux
1.13) A medical student presents with localized precordial pain. During the physical
exam, the location of the pain changes. Chest wall tenderness is found and sighing
respirations are heard. Which of the following is most likely?
a) Musculoskeletal disorder
b) Gallbladder disease
c) Anxiety state
d) Peptic ulcer
e) Esophageal reflux
1.14) A patient presents with right upper quadrant pain that presents after eating fast
food. Which of the following is most likely?
a) Anxiety state
b) Peptic ulcer
c) Esophageal reflux
d) Gallbladder disease
e) Liver disease
2) A heart failure patient states, “My goal for the entire day is to be able to get up and use
the bathroom on my own.” Which of the following New York Heart Association
(NYHA) functional classes would this patient be given?
a) NYHA Class I
b) NYHA Class II
c) NYHA Class III
d) NYHA Class IV
Cardiology #5 – Radiology of the Heart
1.1) The superior most “bulge” on the left cardiac border seen on an anteroposterior (AP)
chest x-ray represents which of the following?
a) Right atrium
b) Left atrium
c) Aorta
d) Superior vena cava

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 7 -
1.2) In the AP radiograph, what is B?
a) Superior vena cava
b) Inferior vena cava
c) Right atrium
d) Left ventricle
e) Pulmonary trunk
1.3) In the AP radiograph, what is D?
a) Right atrium
b) Left atrium
c) Right ventricle
d) Left ventricle
e) Aorta
1.4) In the AP radiograph, what is C?
a) Superior vena cava
b) Inferior vena cava
c) Right atrium
d) Left ventricle
e) Pulmonary trunk
1.5) In the lateral radiograph, what is C?
a) Right atrium
b) Left atrium
c) Right ventricle
d) Left ventricle
e) Aorta
1.6) Using the two radiographs below of a cardiac
resynchronization therapy (CRT) device, which of
the following best describes the location of the tip
of the pacing lead indicated by an arrow?
a) Right atrium
b) Left atrium
c) Right ventricle
d) Left ventricle
e) Coronary sinus
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 8 -
2) Which of the following variables has the greatest effect on the apparent cardiac size on
a chest radiograph?
a) Race and gender
b) Last oral intake
c) Degree of inspiration
d) Location of 9th rib
e) Size of liver or spleen
3) Although magnetic resonance imaging (MRI) is allowed for pacemakers and
implantable cardioverter defibrillators (ICDs) under very specific guidelines, MRI is
generally contraindicated for which of the following major reasons?
a) Lead heating due to induced current
b) Dislodgement of the device due to magnetic pulling
c) Mode-switching of the device into an asynchronous mode
d) Closure of the device magnetic reed switch leading to multiple shocks
e) Distortion of the image leading to incorrect diagnosis
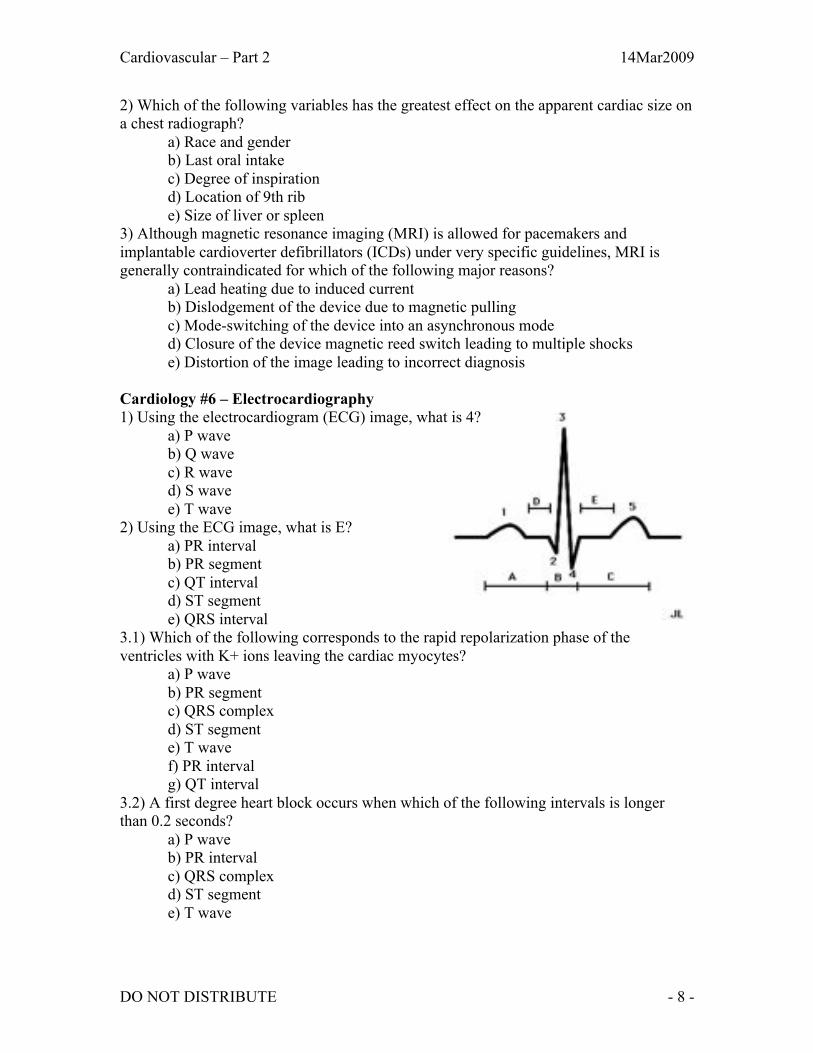
Cardiology #6 – Electrocardiography
1) Using the electrocardiogram (ECG) image, what is 4?
a) P wave
b) Q wave
c) R wave
d) S wave
e) T wave
2) Using the ECG image, what is E?
a) PR interval
b) PR segment
c) QT interval
d) ST segment
e) QRS interval
3.1) Which of the following corresponds to the rapid repolarization phase of the
ventricles with K+ ions leaving the cardiac myocytes?
a) P wave
b) PR segment
c) QRS complex
d) ST segment
e) T wave
f) PR interval
g) QT interval
3.2) A first degree heart block occurs when which of the following intervals is longer
than 0.2 seconds?
a) P wave
b) PR interval
c) QRS complex
d) ST segment
e) T wave

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 9 -
3.3) Which of the following represents an electrical pause at the atrioventricular (AV)
node and a mechanical pause as atrial blood fills into the ventricle?
a) P wave
b) PR segment
c) QRS complex
d) ST segment
e) T wave
f) PR interval
g) QT interval
3.4) Which of the following refers to ventricular systole and can lead to serious problems,
such as Torsade de Pointes (TdP), if it is prolonged?
a) QT interval
b) PR interval
c) QRS complex
d) ST segment
e) T wave
4) Bipolar limb lead ____ most closely parallels the electrical system of the heart (toward
the apex) with an upward deflection of the P wave, QRS, and T wave due to electrical
depolarization and repolarization traveling toward the ____ lead.
a) II; Right arm (RA)
b) II; Left leg (LL)
c) III; Left arm (LA)
d) III; Left leg (LL)
e) I; Left arm (LA)
5.1) The 3 augmented unipolar leads and 3 bipolar limb leads lie in the frontal plane.
a) True
b) False, only the augmented unipolar leads lie in the frontal plane
c) False, only the bipolar limb leads lie in the frontal plane
d) False, the 6 chest leads lie in the frontal plane
5.2) Which is true regarding the augmented voltage aVF lead?
a) The left foot is negative and the arms are positive
b) The right foot is negative and the arms are positive
c) The left foot is positive and the arms are negative
d) The right foot is positive and the arms are negative
e) The arms are positive and the foot (either) is negative
5.3) Which of the following augmented leads is a combination of leads I and III?
a) aVF
b) aVL
c) aVR
d) None of the above
5.4) A patient presents with a possible myocardial infarction due to blockage of the left
anterior descending (LAD) artery. This affects the left ventricle (lateral side) of the heart.
ECG changes might be found in which of the following chest leads?
a) V1 and V2
b) V3 and V4
c) V5 and V6

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 10 -
d) V1 and V6
e) V2 and V5
6.1) Atrial flutter is defined as a heart rate of how many beats per minute?
a) 20 - 60
b) 60 - 100
c) 100 - 250
d) 250 - 350
e) 350 - 450
6.2) An elderly patient presents with palpitations while exercising to Richard Simmons
“Sweatin’ To The Oldies.” Physical exam reveals an irregular and fast pulse. As a
technician sets up the cardiac monitor, you heard the monitor beep at a regularly irregular
rhythm. Which of the following is most likely?
a) Premature atrial contractions (PACs)
b) Premature ventricular contractions (PVCs)
c) Sinus tachycardia
d) Atrial flutter
e) Atrial fibrillation
7) Idioventricular rhythm (ventricular foci) will pace at what inherent rate?
a) 10-20 beats per minute
b) 20-40 beats per minute
c) 40-60 beats per minute
d) 60-80 beats per minute
e) 80-100 beats per minute
8) What is the approximate rate of the ECG below?
a) 275 beats per minute
b) 225 beats per minute
c) 175 beats per minute
d) 125 beats per minute
e) 75 beats per minute
9.1) What is the rhythm of the ECG below?

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 11 -
a) Premature atrial contraction
b) Atrial tachycardia
c) Atrial fibrillation
d) Atrial flutter
e) Sinus arrhythmia
9.2) What is the rhythm of the ECG below?
a) Atrial tachycardia with 2:1 block
b) Atrial fibrillation
c) Supraventricular tachycardia
d) Junctional tachycardia
e) Torsade de Pointes
9.3) What is the rhythm of the ECG below?
a) Torsade de Pointes
b) Supraventricular tachycardia
c) Junctional tachycardia
d) Ventricular tachycardia
e) Ventricular fibrillation
9.4) What is the rhythm of the ECG below?
a) First degree heart block
b) Second degree heart block type I (Mobitz I, Wenckebach)
c) Second degree heart block type II (Mobitz II)
d) Sinus third degree heart block with ventricular escape
e) Non-conducted premature atrial contraction

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 12 -
9.5) What is the rhythm of the ECG below?
a) Ventricular tachycardia
b) Ventricular fibrillation
c) Junctional tachycardia
d) Supraventricular tachycardia
e) Torsade de Pointes
10) A patient with chronic atrial fibrillation (Afib) is implanted with a pacemaker. During
an episode, the pacemaker evaluates the atrial rate and then paces the atrium at a higher
rate to terminate the episode. What concept is this device relying on?
a) Automaticity
b) Pre-excitation
c) Overdrive suppression
d) Parasystolic focus
e) Accessory pathway (James fibers, Kent fibers, or Mahaim fibers)
11) Diseased segments of the conduction system can retain the capacity for spontaneous
depolarization (impulse formation) while acquiring protection from passive discharge by
the sinus impulse (entrance block). Under these circumstances, the protected ectopic
pacemaker coexists with the sinus pacemaker and competes with it for control of the
cardiac rhythm. This is known as:
a) Automaticity
b) Pre-excitation
c) Accessory pathway
d) Parasystolic focus
e) Overdrive suppression
12.1) What is the approximate axis in the frontal plane for the ECG below?
a) -30 degrees
b) 0 degrees
c) +30 degrees
d) +60 degrees

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 13 -
12.2) What is the mean QRS vector (axis) in the frontal plane for an ECG showing a
negative/downward deflection in lead I and a positive/upward deflection in aVF? (For
more accuracy, the axis is 90 degrees from the most isoelectric lead)
a) Normal
b) Left axis deviation
c) Right axis deviation
d) Extreme right axis deviation
13) Which of the following is most likely true if leads V1 and V2 are isoelectric?
a) No rotation (normal)
b) Leftward rotation; Left ventricular hypertrophy
c) Leftward rotation; Left myocardial infarction
d) Rightward rotation; Left ventricular hypertrophy
e) Rightward rotation; Left myocardial infarction
14.1) What is the rhythm of the ECG below?
a) Premature atrial contraction (PAC)
b) Atrial bigeminy
c) Atrial trigeminy
d) Premature junctional contraction (PJC)
e) Junctional trigeminy
14.2) What is the rhythm of the ECG below?
a) Premature atrial contraction (PAC)
b) Atrial bigeminy
c) Atrial trigeminy
d) Premature junctional contraction (PJC)
e) Junctional trigeminy
14.3) A patient using amphetamines presents with the ECG below. What is the rhythm?
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 14 -
a) Sinus rhythm with first degree heart block
b) Second degree heart block type I (Mobitz I, Wenckebach)
c) Second degree heart block type II (Mobitz II)
d) Third degree heart block with junctional escape
e) Non-conducted premature atrial contraction
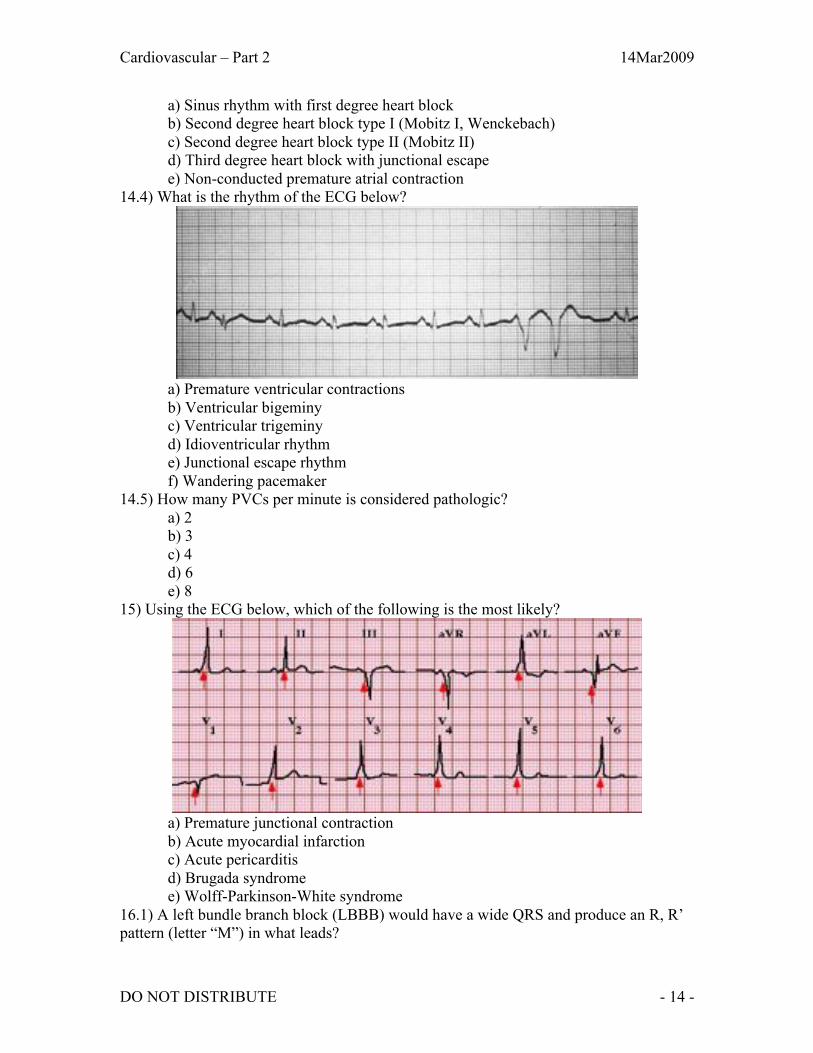
14.4) What is the rhythm of the ECG below?
a) Premature ventricular contractions
b) Ventricular bigeminy
c) Ventricular trigeminy
d) Idioventricular rhythm
e) Junctional escape rhythm
f) Wandering pacemaker
14.5) How many PVCs per minute is considered pathologic?
a) 2
b) 3
c) 4
d) 6
e) 8
15) Using the ECG below, which of the following is the most likely?
a) Premature junctional contraction
b) Acute myocardial infarction
c) Acute pericarditis
d) Brugada syndrome
e) Wolff-Parkinson-White syndrome
16.1) A left bundle branch block (LBBB) would have a wide QRS and produce an R, R’
pattern (letter “M”) in what leads?

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 15 -
a) V1 or V2
b) V3 or V4
c) V5 or V6
d) V1 or V3
e) II or III
16.2) A right bundle branch block (RBBB) would have a wide QRS and produce an R, R’
pattern (letter “M”) in what leads?
a) V1 or V2
b) V3 or V4
c) V5 or V6
d) V1 or V3
e) II or III
17.1) Which of the following best describes this ECG?
a) RA abnormality (p pulmonale)
b) LA abnormality (p mitrale)
c) Biatrial abnormality
d) Left ventricular abnormality
e) Right ventricular abnormality
17.2) Which of the following best describes this ECG?
a) RA abnormality (p pulmonale)
b) LA abnormality (p mitrale)
c) Biatrial abnormality
d) Left ventricular abnormality
e) Right ventricular abnormality
18) Which of the following best describes the ECG below?
a) RA abnormality (p pulmonale)
b) LA abnormality (p mitrale)
c) Acute pericarditis
d) Left ventricular abnormality
e) Right ventricular abnormality
19.1) When assessing an ECG for “significant” Q waves, what lead can be ignored?
a) V1
b) V6
c) aVL
d) aVR
e) aVF
19.2) Which of the following would be considered a significant Q wave?
a) +1/2 amplitude of QRS, +1mm tall, +0.04s wide
b) +1/3 amplitude of QRS, +1mm tall, +0.04s wide
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 16 -
c) +1/3 amplitude of QRS, +2mm tall, +0.08s wide
d) +1/2 amplitude of QRS, +2mm tall, +0.08s wide
e) Same amplitude as QRS, +3mm tall, +0.12s wide
20.1) Evidence of myocardial infarction in lead V1 and possibly V2 would most likely
mean what part of the heart is affected?
a) Inferior
b) Anterior
c) Septum
d) Lateral
e) Posterior
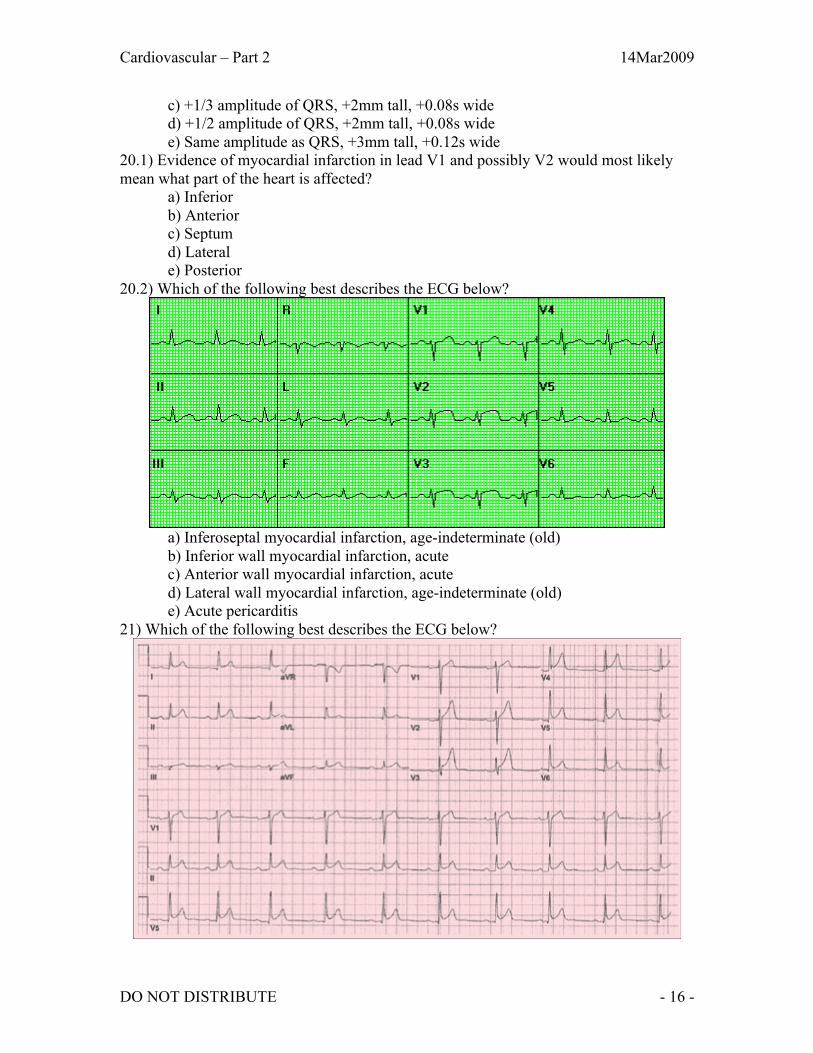
20.2) Which of the following best describes the ECG below?
a) Inferoseptal myocardial infarction, age-indeterminate (old)
b) Inferior wall myocardial infarction, acute
c) Anterior wall myocardial infarction, acute
d) Lateral wall myocardial infarction, age-indeterminate (old)
e) Acute pericarditis
21) Which of the following best describes the ECG below?

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 17 -
a) Inferoseptal myocardial infarction, age-indeterminate
b) Inferior wall myocardial infarction, acute
c) Anterior wall myocardial infarction, acute
d) Lateral wall myocardial infarction, age-indeterminate
e) Acute pericarditis
Cardiology #7 – Echocardiography
1) Echocardiography would NOT be indicated for a patient presenting with only:
a) Dyspnea
b) Murmur
c) Palpitations
d) Chest pain
e) Idiopathic syncope
2) Echocardiography is most useful in evaluating which of the following?
a) Valvular heart disease
b) Coronary artery disease
c) Electrophysiologic disorders
d) Hyperlipidemia
e) Diabetes mellitus
Cardiology #8 – Nuclear Cardiology
1) Redistribution of 201Thallium resolves post-stress defects by the time of repeat
imaging, usually how long after initial tracer injection?
a) 5 minutes
b) 30-60 minutes
c) 3-4 hours
d) 8-12 hours
e) 12-24 hours
2) Which of the following is NOT true when comparing the scintigram radionuclides
201Thallium (201TI) and 99mTechnetium (99mTc) for perfusion imaging?
a) 201TI has lower energy than 99mTc
b) 99mTc scintigrams are of higher quality
c) 201Tc has a longer half-life than 99mTc
d) 99mTc scans should be repeated due to redistribution
e) 99mTc scans would have less soft tissue attenuation artifact in obese or large-
breasted patients
3.1) Which of the following is NOT a reason to choose a pharmacologic stress test
(dipyridamole, adenosine, dobutamine) over a physical exercise stress test?
a) Aortic stenosis
b) Ventricular electronically paced rhythm
c) Caffeine ingestion in the last 12 hours
d) Left bundle branch block
e) Hypertrophic obstructive cardiomyopathy
3.2) A patient with a ventricular pacemaker is being prepared for a stress test. Which of
the following would be a pharmaceutical perfusion stress test option?
a) Dobutamine

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 18 -
b) Dipyridamole
c) Adenosine
d) A or B
e) B or C
3.3) Dipyridamole and adenosine should be avoided in stress testing for all of the
following situations EXCEPT:
a) Active wheezing
b) Left bundle branch block
c) Caffeine ingestion in the past 12 hours
d) Bronchospastic pulmonary disease
e) Recent treatment with theophylline or aminophylline
4) At what interval will a 99mTc-pyrophosphate scan demonstrate a “hot spot” in the
myocardium following a myocardial infarction?
a) 1-5 hours
b) 6-12 hours
c) 13-24 hours
d) 1-5 days
e) 6-12 days
5.1) Which of the following studies uses 111In-antimyosin?
a) Myocardial perfusion imaging
b) Infarct imaging
c) Viability studies
d) Equilibrium radionuclide angiography (ERNA)
e) First-pass radionuclide angiography (FPRNA)
5.2) Which of the following studies is used to monitor the left ventricle, especially in
patients with suspected aneurysm or those receiving cardiotoxic chemotherapy?
a) Myocardial perfusion imaging
b) Infarct imaging
c) Viability studies
d) Equilibrium radionuclide angiography (ERNA)
e) First-pass radionuclide angiography (FPRNA)
5.3) Which of the following studies most uses positron emission tomography (PET)?
a) Myocardial perfusion imaging
b) Infarct imaging
c) Viability studies
d) Equilibrium radionuclide angiography (ERNA)
e) First-pass radionuclide angiography (FPRNA)
5.4) Which of the following studies is used to monitor the right ventricle as well as
intracardiac shunts and valvular regurgitation?
a) Myocardial perfusion imaging
b) Infarct imaging
c) Viability studies
d) Equilibrium radionuclide angiography (ERNA)
e) First-pass radionuclide angiography (FPRNA)

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 19 -
6) Combining stress with myocardial perfusion imaging during a nuclear stress test will
create heterogeneity (differences) in myocardial blood flow between territories supplied
by non-obstructed coronary arteries and those with significant obstructive disease.
a) True
b) False, it speeds redistribution time allowing for a faster scan
c) False, it allows for radionuclides to pass through obstructed emboli
Cardiology #9 – Cardiac Catheterization & Angiography
1.1) Which of the following would be used to assess the severity and extent of coronary
heart disease?
a) Electrocardiography
b) Echocardiography
c) Nuclear imaging
d) Cardiac catheterization
e) Cardiac angiography
1.2) A patient presents with ST-elevation on a limb-lead (3-lead) ECG. Which of the
following would be best to determine the nature and extent of the problem if
interventional therapy is anticipated?
a) 12-lead ECG
b) Echocardiography
c) Nuclear imaging
d) Cardiac catheterization
e) Cardiac angiography
2) Cardiac catheterization and angiography are contraindicated (relative) in which of the
following situations as the dye can worsen the problem or lead to anaphylactic shock?
a) Active GI bleed
b) Bacteremia
c) Acute renal failure
d) Pulmonary edema
e) Acute stroke
3.1) Which of the following complications of cardiac catheterization and angiography is
the most common, especially in diabetic patients?
a) Mortality
b) Stroke
c) Myocardial infarction
d) Life threatening anaphylaxis
e) Contrast induced renal failure
3.2) If 100 patients undergo either cardiac catheterization or angiography, how many will
develop an allergic reaction to the contrast dye?
a) 1
b) 3
c) 5
d) 10
e) 25
f) 50

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 20 -
Cardiology #10 – Atherosclerosis, Thrombosis, & Vascular Biology
1.1) Which of the following has a prominent internal elastic membrane?
a) Elastic arteries
b) Muscular arteries
c) Arterioles
d) Capillaries
1.2) which of the following is true of small arteries and arterioles?
a) The tunica intima is very thin
b) The tunica intima is very thick
c) The tunica media is very thin
d) The tunica media is very thick
e) The tunica adventitia is very thin
1.3) Which of the following has the thickest tunica intima, with the tunica media being
the largest of the three layers?
a) Elastic arteries
b) Muscular arteries
c) Arterioles
d) Capillaries
2) In the image here, what does the star designate?
a) Artery tunica intima
b) Artery tunica media
c) Artery tunica adventitia
d) Vein tunica intima
e) Vein tunica media
3) Which of the following best describes atherosclerosis?
a) Hardened arteries of any size
b) Hardened medium/large arteries due to plaque usually found in the intima
c) Hardened medium/large arteries due to plaque usually found in the media
d) Hardened medium/large arteries due to plaque usually found in the adventitia
e) Hardened arteries of any size due to plaque
4.1) Which of the following is NOT true of the effects of lipoproteins on vascular
endothelium?
a) Macrophages that ingest lipid accumulations within damaged endothelium can
become foam cells
b) When foam cells die, they release lipids and free radicals
c) LDL enters the endothelium through the injured wall
d) Death of foam cells causes vasodilation
e) HDL prevents LDL oxidation and contributes to reverse cholesterol transport
4.2) The onset of angina pectoris begins at which phase of atherosclerosis?
a) Phase 1
b) Phase 2
c) Phase 3
d) Phase 4
e) Phase 5
5.1) VLDL, IDL (intermediate density lipoprotein), and LDL lipoproteins contain B100,
which is synthesized in the:
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 21 -
a) Kidney
b) Liver
c) Gallbladder
d) Spleen
e) Thymus
5.2) An HMG-CoA reductase inhibitor (statins) would most affect and lower which of the
following?
a) Chylomicrons
b) VLDL
c) LDL
d) HDL
5.3) Which of the following is formed in the intestine, carries triacylglycerols through
lymph into the circulation, and is broken down by lipoprotein lipase (LPL)?
a) Chylomicrons
b) VLDL
c) LDL
d) HDL
Match the lipoprotein with its function:
5.4) Carry triacylglycerols from the liver to adipose tissue a) HDL
5.5) Carry cholesterol from the liver to body cells b) LDL
5.6) Carry cholesterol from the body to the liver c) VLDL
5.7) A patient with a damaged liver (hepatocytes) would likely have difficulty removing
which of the following from the body?
a) Chylomicrons
b) VLDL
c) LDL
d) HDL
6.1) A 41-year-old female in apparent good health is worried because her father just had a
heart attacked and a screening found that she had a moderately elevated cholesterol level.
She is overweight and eats a diet with a lot of saturated and partially hydrogenated fat. If
she avoids most of these fats for the next year, what is the most likely affect on her
coronaries, which would not happen otherwise?
a) Most existing vascular occlusions will reopen
b) Calcified plaques will decrease considerably in size
c) Progression of atherosclerosis will be unaffected
d) Some fatty streaks will disappear
e) Thrombotic changes in the coronaries will partially revert
6.2) A 62-year-old male comes into your office complaining of chest pain. He is obese,
doesn't get much exercise, and eats a diet high in saturated fat. If you could see inside the
patient's coronary arteries, you would most likely find:
a) The lumen blocked by cholesterol and cellular debris
b) Fatty streaks covering most of the luminal surface
c) Thrombi blocking most coronary arteries
d) VLDL and chylomicron remnants narrowing the lumen
e) Bulges of endothelium due to intima deposits

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 22 -
6.3) Which nutritional risk factors are likely to increase the risk of thrombotic coronary
occlusion and atherogenesis?
a) High fruit consumption
b) High vitamin K intake
c) Moderate to severe obesity
d) Use of calcium supplements
e) Iron deficiency
7.1) Which lipoprotein delivers dietary cholesterol to the liver?
a) Lp(a)
b) LDL
c) HDL
d) VLDL remnants
e) Chylomicron remnants
7.2) Which food constituent is transported with chylomicrons from the intestines to the
liver and other tissues?
a) Vitamin B1
b) Folate
c) Vitamin B12
d) Biotin
e) Vitamin E
8.1) What is the first organ to receive fatty acids, starting and the gut?
a) Heart
b) Lungs
c) Liver
d) Kidneys
e) Spleen
8.2) Following extensive abdominal surgery, an elderly patient receives total parenteral
nutrition with 100% fat (emulsion containing medium-chain and long-chain fat). Which
of the following metabolic events is the essential first step to allow energy generation
from the infused fat?
a) The infused fat is incorporated into chylomicrons
b) Adipocytes take up the circulating fat particles
c) Free fatty acids are released from adipose tissue
d) Lipoprotein lipase cleaves emulsified triglycerides
e) Muscle cells take up albumin-bound fatty acids
8.3) A new patient comes to see you. From the chart you learn that the patient has a
genetic defect and is unable to make chylomicrons. In which nutrient will this patient
most likely be deficient without high-dose supplementation?
a) Thiamin
b) Riboflavin
c) Vitamin C
d) Vitamin D
e) Vitamin E
8.4) An overweight 23-year-old college student comes to see you about allergies. While
you are talking, he asks about the risk of heart disease. He eats a reasonable diet but gets

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 23 -
little exercise. You explain to him that exercise will not only help him keep his weight at
a healthy level, but it will also aid in transport of cholesterol from the:
a) Liver to the adrenals
b) Liver to adipose
c) Arteries to liver
d) Arteries to adipose
e) Adipose to liver
9.1) Which of the following is considered atherogenic?
a) VLDL
b) LDL
c) VLDL remnants
d) A & B
e) B & C
9.2) A major function of VLDL is:
a) To scavenge cholesterol from non-hepatic tissues
b) To deliver triglycerides from liver to muscle and fat cells
c) To deliver cholesterol to growing tissues
d) To transport fatty acids from the intestine to the liver
e) To transform newly formed cholesterol into bile
10.1) A 51-year-old female comes in to see you about menopausal symptoms. She is
clearly overweight. Her LDL cholesterol has recently increased from 145 to 165. You
decide to talk to her about the risks of heart disease. You tell her that even a modest
weight loss is likely to decrease her LDL cholesterol. The most important mechanism for
this is that:
a) Cholesterol is not absorbed without fat
b) VLDL synthesis decreases
c) Fewer chylomicrons are converted to LDL
d) LDL receptors are down regulated
e) Apo B synthesis increases
10.2) A high cholesterol diet would increase which of the following due to delayed
clearance via receptor down-regulation?
a) Chylomicrons
b) VLDL
c) LDL
d) HDL
10.3) A 55-year-old male has had symptomatic atherosclerosis for several years. For the
past 6 months, he has been taking marine oil supplements. He wants to know when he
can expect regression of his atherosclerotic lesion. You respond that:
a) It is too early to tell
b) Progression of his atherosclerosis cannot be influenced by diet
c) He might expect a reduction in thrombosis risk
d) If there were an effect, he should have noticed by now
e) With a decrease in atherogenic lipoproteins there should be fewer lesions
10.4) Which of the following would most reduce total serum cholesterol if a change was
being made from a typical U.S. diet?
a) Vegetable shortening
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 24 -
b) Stick margarine
c) Olive oil
d) Safflower oil
e) Soybean oil
10.5) What is an especially good food source for the type of dietary fiber that lowers
LDL cholesterol concentrations by more than a percent with each daily serving?
a) Oats and fruits
b) Low-fat milk and cheese
c) Fat-free pasta
d) Lean white meats
e) Unsweetened tea and coffee
11.1) A 66-year-old man comes to your office. He recently read an article that said
vegetables would protect against heart disease. He wants to know more about these anti-
oxidants. The anti-oxidants that protect lipoproteins from oxidation are:
a) Alpha-tocopherol and carotenoids
b) Selenium
c) Nitric oxide and homocysteine
d) Retinoic acid
e) Folate
11.2) What explains the high susceptibility of low-density lipoproteins to oxidation?
a) Their lack of antioxidant defenses
b) The presence of heme-proteins in their core
c) Their prominent exposure to dietary free radicals
d) The chemical instability of their free cholesterol
e) Their high content of polyunsaturated fatty acids
11.3) How does extensive exposure to free radicals change the metabolic fate of LDL?
a) Free-radical-induced changes promote LDL conversion to VLDL
b) Hepatic LDL uptake becomes more effective
c) More circulating LDL ends up in extra-hepatic tissues
d) Oxidized LDL cholesterol is a preferred bile acid precursor
e) Oxidation shortens LDL half life in circulation
11.4) What is a mechanism that might explain beneficial effects of high fruit and
vegetable consumption on coronary smooth muscle cell function?
a) Preventing the free radical interference with nitric oxide signaling
b) Increasing the transport of trans-fatty acids to nuclear targets
c) Inhibiting the expression of peroxisomal beta-oxidation
d) Activating G-protein-linked nitric oxide synthase
e) Promoting the transcription of HMG-CoA reductase
12.1) A 31-year-old woman comes to see you because of low back pain. After an
extensive analysis of the situation, you recommend regular exercise, such as walking. To
encourage the patient, you tell her that exercise might increase her HDL levels. Higher
HDL levels are beneficial because they:
a) Lower LDL cholesterol levels
b) Inhibit lipoprotein lipase activity
c) Slow apolipoprotein B transfer to LDL
d) Accelerate receptor-mediated LDL uptake

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 25 -
e) Promote cholesterol transport from arteries to the liver
12.2) The rate-limiting step in cholesterol synthesis is the conversation of HMG-CoA to:
a) Acetyl CoA
b) Geranyl PP
c) Lanosterol
d) Mevalonate
e) Desmosterol
13) Which dietary change is most likely to decrease HDL concentrations?
a) Excessive weight gain
b) Greater use of butter
c) Increased cholesterol intake
d) Alcohol consumption
e) Switching to a low-carb diet
14.1) An overweight (BMI 29.1kg/m^2) 35-year-old American male of Lebanese
ancestry has a family history of myocardial infarction. His current lipoprotein profile is as
follows: total cholesterol 302, LDL cholesterol 250mg/dL, and HDL cholesterol
32mg/dL. What is the likely impact on his lipoproteins of a combined exercise/portion-
control program that decreases his waist circumference from 103 to 99cm over a period
of 3 months?
a) The program will lower LDL cholesterol from 250 to 226mg/dL
b) The program will lower HDL cholesterol from 32 to 29mg/dL
c) The program will leave total cholesterol unchanged at 302mg/dL
d) The program will raise chylomicron cholesterol from 25 to 36mg/dL
e) The program will increase VLDL cholesterol from 20 to 40mg/dL
14.2) A frustrated 42-year-old obese female comes to see you with continued high LDL
cholesterol levels. She can't understand why. She reports following an extremely low-fat,
low-cholesterol diet during this time; she satisfies her appetite with carbohydrates
instead. You explain to her that people who are very overweight make more:
a) HDL
b) VLDL
c) Chylomicrons
d) HDL remnants
e) Chylomicron remnants
14.3) People with moderate alcohol use (not more than one drink per day for women and
two for men) have lower cardiovascular risk than both non-drinkers and excessive
drinkers.
a) True
b) False
c) False, only lower than non-drinkers
d) False, only lower than excessive drinkers
Cardiology #11 – Antihyperlipidemic Therapy
1.1) A patient presents with massive fasting hyperchylomicronemia after normal dietary
fat intake, resulting in greatly elevates serum triacylglycerol. They are diagnosed with
Type I familial hyperchylomicronemia. What is the most likely cause of the increased
serum levels?
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 26 -
a) Decreased clearance of VLDL and chylomicrons
b) Overproduction of VLDL triacylglycerol in serum
c) Lipoprotein lipase deficiency
d) Decrease in LDL receptors
e) Overproduction of VLDL by the liver
1.2) A patient presents with a genetic defect leading to Type V familial
hypertriglyceridemia. This may be due to either an overproduction of VLDL and
chylomicrons, or decreased clearance. Which of the following is most likely to occur?
a) VLDL, LDL, and chylomicrons will be increased
b) VLDL, LDL, and HDL will be increased, chylomicrons will decrease
c) HDL and VLDL will decrease, chylomicrons will increase
d) Chylomicrons and HDL will decrease
e) VLDL and chylomicrons will be increased, LDL will decrease
1.3) Which of the following is caused by a lack of LDL receptors, leading to elevated
LDL but normal VLDL?
a) Type I Familial Hyperchylomicronemia
b) Type IIa Familial Hypercholesterolemia
c) Type IIb Familial Combined Hyperlipidemia
d) Type III Familial Dysbetalipoproteinemia
e) Type IV Familial Hypertriglyceridemia
1.4) Which of the following is caused by an overproduction or underutilization of IDL
due to a mutant apolipoprotein E?
a) Type I Familial Hyperchylomicronemia
b) Type IIa Familial Hypercholesterolemia
c) Type IIb Familial Combined Hyperlipidemia
d) Type III Familial Dysbetalipoproteinemia
e) Type IV Familial Hypertriglyceridemia
1.5) Which of the following would most likely occur with overproduction of VLDL by
the liver?
a) Increased serum triacylglycerol but normal serum cholesterol
b) Increased serum cholesterol but normal serum triacylglycerol
c) Increased serum triacylglycerol and decreased serum cholesterol
d) Increased serum triacylglycerol and increased serum cholesterol
e) Decreased serum triacylglycerol and decreased serum cholesterol
2.1) What are the most common types of hyperlipidemias?
a) Type I and V
b) Type IIb and IV
c) Type III and IIa
d) Type I and II
e) Type IV and V
2.2) What hyperlipidemias most often occur in obese or diabetic patients?
a) Type I and V
b) Type IIb and IV
c) Type III and IIa
d) Type I and II
e) Type IV and V

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 27 -
3) Which of the following is NOT associated with tobacco smoking, which increases the
risk of coronary artery disease (CAD)?
a) Increased levels of HDL
b) Cytotoxic effects on the endothelium
c) Increased oxidation of lipoproteins
d) Stimulation of thrombogenesis
e) Impairment of cholesterol retrieval
4.1) Which of the following is NOT a desirable value?
a) Total cholesterol > 200
b) LDL < 130
c) HDL > 40 for men
d) HDL > 50 for women
e) Triglycerides < 150
4.2) Which of the following dietary changes is NOT correct?
a) Omega-3 fatty acids can help lower triglyceride levels
b) Switching to monounsaturated fats can help lower LDL levels
c) Use of complex carbohydrates and fiber can help lower LDL levels
d) Lowering calorie and alcohol intake can help lower VLDL levels
e) Omega-6 fatty acids can help lower triglyceride levels
5) A patient presents with primary chylomicronemia and is treated immediately by
sharply restricting dietary oral fat intake. Which of the following supplements would be
least useful for this patient?
a) Vitamin A (Retinol)
b) Vitamin C (Ascorbic acid)
c) Vitamin D (Calciferol)
d) Vitamin E (Tocopherol)
e) Vitamin K (Phylloquinone)
6) Restricting dietary protein intake to levels that a sufficient for amino acid replacement
can decrease which of the following, thus protecting from proatherogenic changes in the
endothelium?
a) Tocopherols
b) Selenium
c) Homocysteine
d) Ascorbic acid
e) Carotenoids
7) Which of the following is NOT true regarding the prescription of antihyperlidemic
drugs?
a) Antihyperlipidemic drugs should not be prescribed to a patient who is pregnant
or who may become pregnant
b) Antihyperlipidemic drugs are useful in patients with elevated LDL levels
c) Antihyperlipidemic drugs are safe for lactating women if they take vitamin E
and folate supplements
d) Antihyperlipidemic drugs are rarely prescribed to patients under the age of 18
e) Children with heterozygous familial hypercholesterolemia can be treated with
certain drugs such as resin or a reductase inhibitor but only after the age of 7
when the myelination of the CNS is complete

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 28 -
8) What is the major mechanism for niacin, which alters plasma levels of VLDL, LDL,
and HDL?
a) Reducing levels of tissue plasminogen activator
b) Retention of neutral sterols in the stool
c) Increased HDL catabolic rate
d) Inhibition of VLDL secretion
e) Decreased VLDL clearance via the LPL pathway
9) Which of the following is NOT true regarding niacin alone or in combination with a
bile acid-binding resin or a reductase inhibitor?
a) In combination, niacin normalizes LDL in patients with hypercholesterolemia
b) In combination, niacin is useful for patients with nephrosis
c) In severe mixed lipidemia, niacin markedly reduces triglycerides
d) Niacin is the least effective drug for enhancing levels of HDL
e) Niacin is useful in patients with combined hyperlipoproteinemia and familial
dysbetalipoproteinemia
10) Patients taking niacin should be evaluated every six months for what reason?
a) Hyperuricemia precipitating gout
b) Acute hepatotoxicity
c) Carbohydrate intolerance with hyperglycemia
d) Skin rashes and acanthosis nigricans
e) Cutaneous flushing and vasodilation
11) Niacin would be contraindicated in what situation?
a) Diabetics
b) Peptic ulcer disease
c) Pseudo-gout
d) Glaucoma
e) Severe hyperlipidemia
12.1) What is the mechanism of action of fibrates (gemfibrozil, fenofibrate) with regard
to peroxisome proliferators-activated receptor alpha (PPAR-alpha)?
a) They enhance the action of PPAR-alpha
b) They attenuate the action of PPAR-alpha
c) They act as ligands for PPAR-alpha
d) They double plasma levels of PPAR-alpha
e) They half plasma levels of PPAR-alphas
12.2) A patient presents with hyperlipidemia and is given gemfibrozil (Lopid). Which of
the following is the major effect on plasma lipoprotein levels?
a) Decreases LDL levels
b) Decreases VLDL levels
c) Increase HDL levels
d) Decreases chylomicrons levels
e) Blocks VLDL receptors
13) Fenofibrate (Tricor, Lofibra, Lipanthyl) and gemfibrozil (Lopid) are indicated for
which types of hyperlipidemias?
a) Types I, II, and III
b) Types II, III, and IV
c) Types III, IV, and V

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 29 -
d) Types IV, V, and I
e) Types V, I, and II
14) Which of the following is the most common side effect of gemfibrozil and
fenofibrate?
a) Eczema and skin reactions
b) Acute appendicitis
c) Vertigo and nausea
d) Rash and hypokalemia
e) Gastrointestinal reactions
15) An obese Native American patient presents with a hyperlipidemia. Which of the
following is NOT completely true regarding the prescription of gemfibrozil or
fenofibrate?
a) They should not be given in combination with cerivastatin (Baycol, Lipobay)
b) They should not be given if the patient has gallbladder disease
c) They should not be given if the patient has hepatic dysfunction
d) They should not be given if the patient has renal dysfunction
e) They should not be given if the patient is taking anticoagulants
16) Which of the following is NOT an indication for using bile acid-binding resins, such
as colestipol (Colestid) and cholestyramine (Questran)?
a) Hypertriglyceridemia
b) Hypercholesterolemia
c) Digitalis toxicity
d) Cholestasis
e) Bile salt accumulation
17) What is the mechanism of action for bile acid-binding resins?
a) Enhanced biliary excretion of bile acids for binding
b) Enhanced biliary retention of bile acids for binding
c) Selective inhibitor of biliary absorption of cholesterol
d) Blocking of 7-alpha-hydroxylation in the liver
e) Decreased cholesterol synthesis in the liver
18) What is the most common side effect associated with bile acid-binding resins?
a) Malabsorption of vitamin K leading to hypoprothrombinemia
b) Increased formation of gallstones
c) Steatorrhea
d) Diverticulitis
e) Constipation
19) Bile acid-binding resins are contraindicated in patients with:
a) Hypoprothrombinemia
b) Gallstones
c) Steatorrhea
d) Diverticulitis
e) Constipation
20) What is the mechanism of action for ezetimibe (Zetia, Ezetrol)?
a) Enhanced biliary excretion of bile acids for binding
b) Enhanced biliary retention of bile acids for binding
c) Selective inhibitor of biliary absorption of cholesterol

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 30 -
d) Blocking of 7-alpha-hydroxylation in the liver
e) Decreased cholesterol synthesis in the liver
21) Which of the following is a toxicity (rare) associated with ezetimibe or
ezetimibe/simvastatin (Vytorin)?
a) Simvastatin (Zocor) overdose
b) Rhabdomyolysis
c) Myopathy
d) Liver dysfunction
e) Kidney dysfunction
22) Which of the following statins is the strongest acting for hyperlipidemia?
a) Atorvastatin (Lipitor)
b) Rosuvastatin (Crestor)
c) Lovastatin (Mevacor)
d) Simvastatin (Zocor)
e) Pravastatin (Pravachol)
23) Which of the following describes the mechanism of action for statins?
a) Prevent mevalonate formation and decrease LDL receptors
b) Prevent desmosterol formation and increase LDL receptors
c) Prevent lanosterol formation and decrease LDL receptors
d) Prevent mevalonate formation and increase LDL receptors
e) Prevent desmosterol formation and decrease LDL receptors
24) Statins has a preferential effect on which of the following tissues due to a marked
first-pass extraction in these tissues?
a) Renal
b) Hepatic
c) Biliary
d) Splenic
e) Cardiac
25) Which of the following is NOT an effect of HMG-CoA reductase inhibitors?
a) Major increase in bile acid production
b) Reduction in plasma LDL
c) Decrease in plasma triglycerides
d) Small increase in HDL
26) Statins are effective alone or in combination with other drugs to reduce levels of
LDL. For a patient who is prescribed a statin, when is the best time for them to take the
drug due to enhanced absorption?
a) In the morning an hour prior to eating
b) In the morning with food
c) In the afternoon or during an active period
d) In the evening an hour prior to eating
e) In the evening with food
27) Which of the following is the weakest acting statin for hyperlipidemia?
a) Atorvastatin (Lipitor)
b) Rosuvastatin (Crestor)
c) Fluvastatin (Lescol)
d) Simvastatin (Zocor)

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 31 -
e) Pravastatin (Pravachol)
28) Patients on HMG-CoA reductase inhibitors should be monitored via which of the
following?
a) BMP, basal metabolic panel
b) CBC, complete blood panel
c) TSH, thyroid-stimulating hormone
d) ATL and AST, aminotransferases
e) ApoE, apolipoprotein E genotyping
29) What is the reason for monitoring patients taking HMG-CoA reductase inhibitors?
a) Possible bile duct occlusion
b) Possible renal toxicity
c) Possible hepatotoxicity
d) Possible vitamin E deficiency
e) Possible anorexia and malaise
30) Which of the following drugs would NOT compete with lovastatin, simvastatin, and
atorvastatin for catabolism by the liver cytochrome P450 3A4 pathway and thus may
produce elevated plasma levels of these statins?
a) Fibrates
b) HIV protease inhibitors
c) Phenytoin (Dilantin)
d) Tacrolimus (Fujimycin)
e) Macrolides, ketoconazole, cyclosporine
31) Which of the following drugs would NOT increase plasma levels of lovastatin,
simvastatin, and atorvastatin by increasing CYP3A4 expression?
a) Griseofulvin (Grisovin)
b) Nefazodone (Serzone)
c) Rifampin (Rifadin)
d) Barbiturates
e) Thiazolidinediones (Glitazones)
32) What is the affect of grapefruit juice (>1L/day) on lovastatin, simvastatin, and
atorvastatin?
a) Causes hepatotoxicity
b) Increases plasma statin concentration
c) Decreases plasma statin concentration
d) Causes nausea and vomiting
e) Causes vertigo
33) Which of the following is NOT a CYP2CP inhibitor, which would cause an increase
in plasma levels of fluvastatin?
a) Cyclosporine
b) Metronidazole (Flagyl)
c) Sulfinpyrazone (Anturane)
d) Amiodarone (Cordarone)
e) Cimetidine (Tagamet)
34) Combination statins and bile acid-binding resins are indicated for which of the
following?
a) Type I Familial Hyperchylomicronemia

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 32 -
b) Type IIa Familial Hypercholesterolemia
c) Type III Familial Dysbetalipoproteinemia
d) Type IV Familial Hypertriglyceridemia
e) Type V Gamilial Mixed Hypertriglyceridemia
35) A patient presents with heterozygous Familial Hypercholesterolemia. Which of the
following would be the best pharmaceutical treatment?
a) Statins
b) Niacin
c) Bile acid-binding resins
d) A & C
e) B & C
36) A patient presents with Type IIb Familial Combined Hyperlipidemia. A lipid profile
shows increased VLDL and LDL levels. Which of the following is the most efficacious
and practical for this patient?
a) Statins
b) Niacin
c) Bile acid-binding resins
d) A & B
e) A & C
37) A combination of statins, niacin, and bile acid-binding resins may be beneficial for
patients with severe disorders involving elevated LDL. Which of the following describes
how these should be administered?
a) Together to improve absorption
b) In higher doses than when used alone
c) In lower doses than when used alone
d) With a lipid-rich food such as whole milk
e) With a half-glass of antioxidant rich wine
Match the drug with the best use/prescription:
38.1) Initally for high LDL levels a) Ezetimibe
38.2) Hyperlipidemia with low HDL levels b) Fibrate
38.3) High triglyceride levels where VLDLs predominate c) Niacin
38.4) High LDL levels with maximum dose of statins d) Statin
Cardiology #12 – Angina Pectoris & Non-STEMI Acute Coronary Syndromes
Match the following clinical presentation or description with the syndrome:
1.1) Consistent over time, stenosis of epicardial coronary artery a) Atypical angina
1.2) Increasing, frequent, or prolonged substernal chest discomfort b) Syndrome X
2) Two of three criteria: quality, location, trigger for pain c) Prinzmetal angina
3) Pain upon waking, transient ST segment elevation d) Unstable angina
4) Normal coronary angiography, altered perception of pain e) Stable angina
5) Which of the following classes of antianginal drugs venodilates (reduces preload) and
arteriodilates (reduces afterload)?
a) Beta blockers
b) Nitrates
c) Calcium channel blockers
6) Which of the following should be avoided in Prinzmetal (variant) angina?

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 33 -
a) Beta blockers
b) Nitrates
c) ACE inhibitors
d) Digoxin
e) Calcium channel blockers
7) Which of the following describes the affect of a calcium channel blocker (e.g.
Verapamil) on vascular smooth muscle via myosin light chain kinase?
a) Vasoconstricts leading to increased blood pressure
b) Vasocontricts leading to a continually decreased heart rate
c) Vasodilates leading to decreased blood pressure
d) Vasodilates leading to a continually increased heart rate
e) Vasodilates due to increased guanylyl cyclase and cGMP
8) What is the affect of nitrates and nitrites on vascular smooth muscle?
a) Vasoconstricts leading to increased blood pressure
b) Vasocontricts leading to a continually decreased heart rate
c) Vasodilates leading to decreased blood pressure
d) Vasodilates leading to a continually increased heart rate
e) Vasodilates due to increased guanylyl cyclase and cGMP
9) Which major determinant of myocardial oxygen demand is affected by beta-blockers?
a) Heart rate
b) Ventricular volume
c) Blood pressure
d) Contractility
10) Which major determinant of myocardial oxygen demand is affected by nitrates?
a) Heart rate
b) Ventricular volume
c) Blood pressure
d) Contractility
11) A patient presents after being awoken with chest pain. The patient reports the pain
continuing during an ECG and transient ST segment elevation is seen. Cardiac diagnostic
tests reveal coronary vasospasm. The patient should be prescribed ____ to relieve the
spasm and ____ to prevent further spasms.
a) Nitrates; Beta blockers
b) Beta blockers; Nitrates
c) Calcium channel blockers; Beta blockers
d) Nitrates; Calcium channel blockers
e) Calcium channel blockers; Nitrates
12) What is the preferred route of administration for organic nitrates such as
nitroglycerine?
a) Inhaled ampule
b) PO (oral)
c) IV (intra venous)
d) SQ (sub cutaneous)
e) SL (sub lingual)
13) A patient is being brought to the emergency room via ambulance. The patient reports
7 out of 10 chest pain and is dyspneic and diaphoretic. Prior to administration of
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 34 -
nitroglycerine, the ambulance personnel ensures that systolic blood pressure is
>100mmHg and that the patient has not taken any phosphodiesterase inhibitors (e.g.
Viagra, Cialis, Levitra). How long will the effects of the nitroglycerine last?
a) 15-30 seconds
b) 1-2 minutes
c) 5-10 minutes
d) 15-30 minutes
e) About 60 minutes
14) What is the route of administration for nitrites, such as amyl nitrite?
a) Inhaled ampule
b) PO (oral)
c) IV (intra venous)
d) SQ (sub cutaneous)
e) SL (sub lingual)
15) Which of the following is NOT true regarding the administration of nitrates?
a) For angina of effort, nitrates increase the caliber of epicardial coronaries
b) For variant angina, coronary arteries are relaxed and spasm is reduced
c) For unstable angina, there are several mechanisms known for vasodilation
d) Nitroglycerin reduces platelet aggregation
16) What is the primary effect of organic nitrates, which is helpful for patients with
congestive heart failure?
a) Increased venous capacitance and increased preload
b) Venodilation and decreased preload
c) Vasodilation and decreased afterload
d) Vasodilation and increased afterload
e) Venodilation and increased preload
17) Which of the following would NOT occur with organic nitrates?
a) Baroreceptor tachycardia
b) Orthostatic hypotention
c) Temporal artery pulsation
d) Increased arterial resistance
e) Syncope
18) Which of the following is NOT a compensatory response induced by vasodilators?
a) Retention of salt and water
b) Increased cardiac contractility
c) Increased baroreceptor firing
d) Tachycardia
19) What affect would nitroglycerine have on sexual function?
a) Constricts erectile smooth muscle leading to erection
b) Constricts erectile smooth muscle reducing priapism
c) Dilates erectile smooth muscle leading to erection
d) Dilates erectile smooth muscle reducing priapism
e) Has no effect on sexual function
20) Which of the following drugs does NOT help erectile dysfunction by increasing
levels of cGMP leading to smooth muscle relaxation?
a) Nitroglycerine

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 35 -
b) Cialis
c) Levitra
d) Viagra
e) Enzyte
21) A patient who works in an explosives chemical industry presents with headache,
tachycardia, and dizziness that occur every Monday (“Monday Disease”). What is the
most likely mechanism for this?
a) Diminished release of nitric oxide during the weekend
b) Systemic compensation from nitroglycerine during the workweek
c) Retention of salt and water during the weekend
d) Development of drug tolerance during the workweek
22) Nitrates, such as nitroglycerine, should be administered around-the-clock to ensure
stable plasma concentrations.
a) True
b) False, this will lead to an allergic reaction
c) False, this will lead to drug tolerance
23) The major clinical effect for nitrates in angina of effort is reduction in oxygen
consumption.
a) True
b) False, the major effect is reduction in oxygen demand
c) False, the major effect is reducing platelet aggregation
24) What is the minimal nitrate-free period for patients taking these drugs?
a) 1-hour
b) 4-hours
c) 8-hours
d) 12-hours
e) 24-hours
25) Calcium channel blockers, such as verapamil, block voltage-gated “L-type” calcium
channels. What phase of the cardiac action potential do these drugs affect, reducing
angina?
a) Phase 4 (pacemaker potential)
b) Phase 0 (tapid depolarization)
c) Phase 2 (plateau)
d) Phase 3 (repolarization)
e) Phases 2 and 4
26) Which of the following would have the most cardiac potency but the least vascular
potency (weakest vasodilator)?
a) Nicardipine (Cardene)
b) Diltiazem (Cardiazem)
c) Verapamil (Covera)
d) Nifedipine (Procardia)
e) Amlodipine (Norvasc)
27) A patient presents with a second-degree type II AV conduction block. Which of the
following drugs, along with verapamil, should be avoided?
a) Diltiazem (Cardiazem)
b) Amlodipine (Norvasc)

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 36 -
c) Sildenafil (Viagra)
d) Nifedipine (Procardia)
e) Atropine
28) Dihydropyridine agents block the AV node selectively and have a greater ratio of
smooth muscle effects relative to cardiac effects than diltiazem and verapamil.
a) True
b) False, the ration is only greater than diltiazem
c) False, the ration is only greater than verapamil
d) False, diltiazem has a greater ration than dihydropyridines and verapamil
e) False, verapamil has a greater ration than dihydropyridines and diltiazem
29) Which of the following is NOT a mechanism for which beta-blockers relieve angina?
a) Decreased myocardial oxygen consumption
b) Decreased blood pressure
c) Reduced heart rate
d) Decreased myocardial oxygen demand
30.1) Which of the following is an adverse effect of beta-blockers (e.g. propranolol,
metoprolol, timolol)?
a) Decreased afterload
b) Increased preload
c) Decreased ejection time
d) Increased end-systolic volume
e) Increased end-diastolic volume
30.2) All of the following beta blockers have been shown to decrease mortality in MI
patients. Which one, along with atenolol, is contraindicated in asthma or COPD?
a) Propranolol
b) Metoprolol
c) Timolol
31) Beta blockers are contraindicated for patients with which of the following?
a) Diverticulitis
b) Chronic kidney disease (CKD)
c) Cirrhosis of the liver
d) Epileptic seizures
e) Chronic obstructive pulmonary disease (COPD)
32) Which of the following is the preferred therapy for chronic stable angina in
hypertensive patients?
a) Long-acting nitrates
b) Slow-release or long-acting Ca++ channel blocker or beta-blocker
c) Combined calcium channel blocker and beta-blocker
d) Two different calcium channel blocker
e) Long-acting nitrates and a Ca++ channel blocker
33) Which of the following patients would receive anticoagulant drugs (e.g. heparin),
antiplatelet drugs (e.g. clopidogrel), and antilipid drugs?
a) Palpitations due to atrial fibrillation
b) Normotensive stable angina
c) Hypertensive stable angina
d) Unstable angina

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 37 -
e) AV conduction defect
Cardiology #13 – Acute Myocardial Infarction
1) What is the most common pathophysiologic mechanism responsible for acute
myocardial infarction?
a) In situ thrombosis
b) Vasculitis or primary vasospasm
c) Atherosclerotic plaque rupture
d) Coronary emboli
e) Trauma
2) Which of the following, according to the World Health Organization (WHO), would
diagnose an acute myocardial infarction?
a) Symptoms consistent with acute MI (e.g. chest discomfort)
b) EKG changes consistent with acute MI (e.g. ST elevation)
c) Serum cardiac markers consistent with acute MI (e.g. troponin I, T)
d) Any two of the above
e) All three of the above (triad)
3.1) Which of the following serum cardiac markers is elevated 2-4 hours after myocardial
infarction, stays elevated for 5-10 days, and peaks at 10-24 hours?
a) Myoglobin
b) MB2 isoform
c) CK-MB
d) Troponin I and T
3.2) Which of the following serum cardiac markers is elevated the soonest (1-2 hours)
after an acute myocardial infarction?
a) Myoglobin
b) MB2 isoform
c) CK-MB
d) Troponin I
e) Troponin T
4) Which of the following is NOT an indication for thrombolytic therapy (streptokinase
or tPA)?
a) Chest discomfort for 30-minutes to 12-hours
b) Presumed new ST-segment elevation
c) Hypertension <220/110
d) Presumed new LBBB with MI symptoms
e) MI symptoms, ST-segment elevation, lack of intracranial neoplasm
5) Primary percutaneous coronary intervention (PCI, ballooning) or percutaneous
transluminal coronary angioplasty (PCTA, stenting) is indicated for relatively healthy
patients who have:
a) Post-MI hypovolemic shock
b) Post-MI cardiogenic shock
c) LBBB or RBBB
d) Second degree type II heart block or worse
e) Significant loss of cardiac conduction due to MI

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 38 -
6) Which of the following would be given during acute myocardial infarction to reduce
myocardial oxygen demand?
a) Nitrates
b) Beta-blockers
c) Calcium channel-blockers
d) A & B
e) B & C
7) During what time-frame after an MI would a patient NOT require invasive
electrophysiologic testing regarding the occurrence of ventricular fibrillation or sustained
ventricular tachycardia?
a) 12-hours after the MI
b) 24-hours after the MI
c) 48-hours after the MI
d) 5-days after the MI
e) The patient should be tested immediately if these rhythms occur
8) Which of the following is descriptive of subendocardial myocardial infarction and not
transmural myocardial infarction?
a) Hypotension leading to death of a large part of the heart
b) Shock causing infarction in the distribution of multiple coronary arteries
c) Ischemic necrosis involving the full thickness of the ventricular wall
d) Dissolved thrombus that caused necrosis to the inner 1/2 of the wall
9) Which of the following is NOT true regarding atherosclerotic stenosis with thrombosis
and complete occlusion of a coronary artery with or without thrombolytic therapy?
a) Infarct damage does not become reversible until 20 to 40 minutes of ischemia
b) Reperfusion injury occurs through the generation of oxygen free radicals
c) Damaged cells can take days to heal and are called stunned cells
d) Cells injured prior to reperfusion will not recover
e) Cardiac damage begins at the inside (endocarium) and moves outward
f) Severe artery stenosis will cause damage to the epicardium only
g) About 75% of post-MI patients have cardiac complications
Cardiology #14 – Percutaneous Coronary Interventions
1) Restenosis occurs in 50% of patients after a percutaneous coronary intervention (PCI)
within what time frame?
a) 7-days
b) 1-month
c) 3-months
d) 6-months
e) 1-year
2) The majority of restenosis after PCI is due to what mechanism?
a) Elastic recoil and mechanical narrowing of the vessel
b) Neointimal hyperplasia
c) Stent failure
d) Thrombosis
e) Use of corticosteroids

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 39 -
3) What is the incidence of myocardial infarction due to a percutaneous coronary
intervention procedure?
a) 1%
b) 3%
c) 5%
d) 10%
e) 15%
Cardiology #15 – Surgical Treatment of Coronary Artery Disease
1) Coronary artery bypass graft (CABG) surgery is appropriate for patients with single
vessel stenosis affecting which of the following arteries?
a) Posterior descending artery (PDA)
b) Right coronary artery (RCA)
c) Posterolateral artery (PLA)
d) Left anterior descending artery (LAD)
e) Left circumflex artery (Cx)
2) What vascular conduit has the best (expected) long-term patency as a coronary artery
bypass graft?
a) Saphenous vein (long or short)
b) Internal thoracic artery
c) Radial artery
d) Right gastroepiploic artery
e) Arm vein
3) What is the approximate risk of death from elective coronary artery bypass surgery?
a) < 1%
b) 2%
c) 4%
d) 6%
e) 8%
Cardiology #16 – Atherosclerotic Peripheral Artery Disease
1) Which of the following is most associated with coronary artery disease (CAD), not
atherosclerotic peripheral arterial disease (PAD)?
a) Reduced HDL and increased triglycerides
b) Type II diabetics four times more likely
c) Risk increases 10% with a 10mg/dL increase in total cholesterol
d) Elevated LDL levels
e) Hypertension and reduced homocysteine levels
2) Abnormality in which of the following evaluation techniques for suspected peripheral
arterial disease would indicate the need to perform an ankle blood pressure?
a) Hypertension
b) Carotid bruits
c) Abdominal aortic aneurysm
d) Loss of unilateral pulse
e) Loss of leg hair

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 40 -
3) Which of the following has been documented to relieve claudication and improve
exercise performance for patients with peripheral arterial disease?
a) Ramipril (Altase)
b) Clopidogrel (Plavix)
c) Cilostazol (Pletal)
d) Angioplasty
e) Exercise therapy
f) Bypass operations
Cardiology #17 – Other Arterial Diseases
1) A patient presents with ulcerations and gangrene of the left fingertips. History reveals
recurrent inflammation and pain of the hand. Thromboangiitis obliterans (Buerger's
disease) is suspected. Which of the following is the most effective treatment for this
patient?
a) Exercise thereapy
b) Clopidogrel (Plavix)
c) Aspirin regimen
d) Atorvastatin (Lipitor)
e) Smoking ceasation
2) In chronological order, what is the classic triphasic color response of the digits to cold
exposure or stress in patients with Raynaud phenomenon?
a) White (palor), blue (cyanosis), red (erythema)
b) White (palor), red (erythema), blue (cyanosis)
c) Red (erythema), white (palor), blue (cyanosis)
d) Red (erythema), blue (cyanosis), white (palor)
e) Blue (cyanosis), white (palor), red (erythema)
3) A patient presents with suspected vasculitis. HbsAg and circulating immune
complexes are found in the serum. Which of the following is the most likely etiology of
this patient’s suspected vasculitis?
a) Drug (sulfonamide, iodide, penicillin)
b) Immunologic reaction (Arthus reaction)
c) Autoimmune condition (SLE, Sjögren syndrome)
d) Underlying disease
Match the anti-neutrophilic cytoplasmic antibody (ANCA) disorders:
4.1) Allergic rhinitis, asthma, pseudo-pneumonia a) Microscopic polyangitis
4.2) Most common, no immune deposits, affects kidneys b) Wegener granulomatosis
4.3) Confined to skin, 7-21 days after medication change c) Churg Strauss disease
4.4) Upper respiratory tract infection, lungs, kidneys d) Drug induced vasculitis
5) Which of the following forms of vasculitis has histological granulomatous infiltrations
(like Churg-Strauss), as opposed to neutrophils with fibrin deposits?
a) Polyarteritis nodosa (PAN)
b) Kawasaki disease
c) Takayasu arteritis
d) Microscopic polyangitis
e) Systemic lupus erythematosus (SLE)

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 41 -
6) A patient presents with severe headaches, pain in the temple, blurred vision, and jaw
claudication. They are prescribed high dose prednisone. Which of the following is most
likely?
a) Takayasu arteritis
b) Temporal arteritis
c) Polyarteritis nodosa
d) Wegener granulomatosis
e) Thromboangiitis obliterans (Beurger)
f) Mucocutanous lymph node syndrome (Kawasaki)
g) Leukocytoclastic vasculitis (hypersensitive angiitis)
7) A 25-year-old female is undergoing a routine physical. The clinician is having
difficulty detecting peripheral pulses. Carotid bruits are ascultated. Which of the
following is most likely?
a) Takayasu arteritis
b) Temporal arteritis
c) Polyarteritis nodosa
d) Wegener granulomatosis
e) Thromboangiitis obliterans (Beurger)
f) Mucocutanous lymph node syndrome (Kawasaki)
g) Leukocytoclastic vasculitis (hypersensitive angiitis)
8) A patient presents with fever, sweats, weight loss, and severe muscle and joint pain.
Purpura and ulcerations are found and are painful for the patient. Which of the following
is most likely?
a) Takayasu arteritis
b) Temporal arteritis
c) Polyarteritis nodosa
d) Wegener granulomatosis
e) Thromboangiitis obliterans (Beurger)
f) Mucocutanous lymph node syndrome (Kawasaki)
g) Leukocytoclastic vasculitis (hypersensitive angiitis)
9) An infant presents with unexplained fever lasting five days. Examination reveals
conjunctival injection, strawberry tongue, peripheral edema, and a polymorphous rash.
Which of the following is most likely?
a) Takayasu arteritis
b) Temporal arteritis
c) Polyarteritis nodosa
d) Wegener granulomatosis
e) Thromboangiitis obliterans (Beurger)
f) Mucocutanous lymph node syndrome (Kawasaki)
g) Leukocytoclastic vasculitis (hypersensitive angiitis)
10) A patient presents with an itchy palpable purpura. A biopsy is taken for pathologic
examination. Under microscopy, inflammatory cells are seen scattered in the dermis but
most concentrated near the vessels. The inflammatory cells are clearly fragmented,
appearing smaller than normal. Which of the following is most likely?
a) Takayasu arteritis
b) Temporal arteritis

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 42 -
c) Polyarteritis nodosa
d) Wegener granulomatosis
e) Thromboangiitis obliterans (Beurger)
f) Mucocutanous lymph node syndrome (Kawasaki)
g) Leukocytoclastic vasculitis (hypersensitive angiitis)
11) A patient presents with sinusitis, nasal ulcerations, otitis media, and unilateral hearing
loss. Kidney dysfunction is suspected. Which of the following is most likely?
a) Takayasu arteritis
b) Temporal arteritis
c) Polyarteritis nodosa
d) Wegener granulomatosis
e) Thromboangiitis obliterans (Beurger)
f) Mucocutanous lymph node syndrome (Kawasaki)
g) Leukocytoclastic vasculitis (hypersensitive angiitis)
12) A male smoker presents with color changes to the hands in a cold or stressful
environment. Which of the following is most likely?
a) Takayasu arteritis
b) Temporal arteritis
c) Polyarteritis nodosa
d) Wegener granulomatosis
e) Thromboangiitis obliterans (Beurger)
f) Mucocutanous lymph node syndrome (Kawasaki)
g) Leukocytoclastic vasculitis (hypersensitive angiitis)
13) Systemic vasculitis could be found in all of the following systemic diseases
EXCEPT:
a) Hepatitis B or Aspergillus
b) Rheumatoid arthritis
c) Leukemia or lymphoma
d) Myocardial infarction
e) Scleroderma
14) An IV drug user presents with chest pain. Diagnostic tests find a saccular structure
arising eccentrically from the ascending aortic wall. Which of the following is most
likely?
a) Aortic dissection
b) Berry aneurysm
c) Mycotic aneurysm
d) Rasmussen aneurysm
e) Charcot-Bouchard aneurysm
15) Which of the following would be considered Raynaud disease, not Raynaud
phenomenon?
a) Cyanosis of the hands due to beta-blocker use
b) 15-minute episodes of hand numbness and tingling
c) Hand color changes with associated SLE
d) New color changes of the hand in a teenage girl
e) Carpal tunnel syndrome causing white, blue, red hand color changes

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 43 -
Cardiology #18 – Peripheral Venous Disease
1) When starting warfarin therapy for a patient with deep venous thromboses (DVTs),
why should heparin be started as well for the first 4-5 days?
a) Heparin increases the plasma concentration of warfarin
b) Heparin will immediately dissolve any current DVTs
c) Due to heparin-induced thrombocytopenia thrombosis (HITT)
d) Warfarin can cause thrombosis via proteins C and S
e) Warfarin has a delayed onset of anticoagulant effect
2) Which of the following people is the most predisposed to venous thromboembolism?
a) A 25-year-old male involved in a motorcycle crash
b) A 19-year-old non-smoking female who does not believe in birth control
c) A 50-year-old obese male traveling on an international flight
d) A 6-year-old with croup and epiglottitis
e) A 16-year-old female with endometriosis
3) For the treatment of DVT, low-molecular-weight heparin (LMWH) can be given in a
fixed subcutaneous dose while unfractionated heparin must be adjusted for the patient’s
weight.
a) True
b) False, both must be adjusted for weight
c) False, LMWH must be adjusted for weight
4) A patient presents with heparin-induced thrombocytopenia. Which of the following
drugs can bind to heparin, reversing its affects?
a) Fondaparinux
b) Protamine sulfate
c) Danaparoid
d) Arvin (snake venom)
e) Hirudin (leech saliva)
5) Which of the following is NOT a potential complication of heparin therapy?
a) Osteoporosis
b) Thrombocytopenia
c) Acute asthma
d) Bleeding
e) Death
6) What is the recommended therapeutic international normalized ration (INR) range for
heparin treatment of DVT or pulmonary embolism (PE)?
a) 0.5 to 1.0
b) 1.0 to 2.0
c) 2.0 to 3.0
d) 3.0 to 4.0
e) 3.5 to 4.0
7) A female patient presents with tortuous, elongated, and scarred veins of the legs.
Which of the following is NOT a direct risk factor for varicose veins?
a) Pregnancy
b) Obesity
c) Menopause
d) Aging

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 44 -
e) IV drug use
8) Shortly after giving birth, a patient develops plegmasia alba dolens (painful white leg)
involving the iliofemoral vein. Which of the following best categorizes this disease?
a) Thrombophlebitis
b) Phlebothrombosis
c) Lymphangitis
d) Lymphedema
9.1) Familial Milroy disease is considered which of the following?
a) Thrombophlebitis
b) Phlebothrombosis
c) Lymphangitis
d) Lymphedema
9.2) Which of the following microbes would most likely be associated with
lymphangitis?
a) Streptococcus pyogenes
b) Staphylococcus aureus
c) Streptococcus pneumoniae
d) Staphylococcus epidermidis
e) Enterococcus
Cardiology #19 – Extra: DeQuervain Tendosynovitis & Carpal Tunnel Syndrome
1) Keinböck disease affects which of the following?
a) Hamate
b) Scaphoid
c) Lunate
d) Pisiform
e) Trapezium
2) Of the following overuse injuries seen in the primary care setting, which occurs most
frequently?
a) Gymnast wrist
b) Scapholunate ligament sprain
c) DeQuervain tendosynovitis
d) Intersection syndrome
e) Triangular fibrocartilage complex injury
3) DeQuervain tendosynovitis affects which of the following tendons, making up the
radial border of the anatomic snuffbox?
a) Extensor pollicis brevis and extensor pollicis longus
b) Extensor pollicis brevis and abductor pollicis longus
c) Extensor pollicis longus and abductor pollicis longus
d) Abductor pollicis longus and abductor pollicis brevis
e) Adductor pollicis and abductor pollicis brevis
4) DeQuervain tendosynovitis may improve with an injection of betamethasone sodium
phosphate (Celestone) and bupivacaine (Sensorcaine) at the point of maximal tenderness,
which is usually located:
a) On the ulnar side of the palmaris longus tendon
b) On the radial side of the palmaris longus tendon

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 45 -
c) At the ulnar styloid
d) At the radial styloid
e) In the anatomical snuffbox
f) Mid-wrist if the palmaris longus tendon is absent
5) A patient presents with ulnar neuropathy, trigger finger, and median nerve neuropathy
that wakes the patient at night. While taking the patient’s history, which of the following
is least likely to be heard?
a) Takayasu arteritis
b) Current pregnancy
c) Overuse of the hand
d) Diabetes and thyroid disease
e) Amyloidosis
6) The patient has a positive Finkelstein test and is prescribed a thumb spica splint.
Which of the following is most likely?
a) Keinböck disease
b) Carpal tunnel syndrome (CTS)
c) Ulnar neuropathy
d) Externsor carpi ulnaris tendinitis
e) DeQuervain tendosynovitis
7) Which of the following tests is consistent with carpal tunnel syndrome?
a) Finkelstein test
b) Tinel test
c) Phalen test
d) A & B
e) B & C
8) Patients with carpal tunnel syndrome should, in general, have a radiograph of the wrist
to examine the extent of damage.
a) True
b) False
9) CTS may improve with Celestone injection, although signs of progressive disease
should be treated surgically. Where is the insertion point in patients with CTS receiving
the steroid injection?
a) On the ulnar side of the palmaris longus tendon
b) On the radial side of the palmaris longus tendon
c) At the ulnar styloid
d) At the radial styloid
e) In the anatomical snuffbox
10) About 3% of stress fractures occur in the upper extremity. Which of the following
would NOT be prescribed for a patient with a stress fracture?
a) Rest
b) Plain film radiograph
c) Triple-bone scan SPECT
d) Splinting
e) Steroid injection
James Lamberg
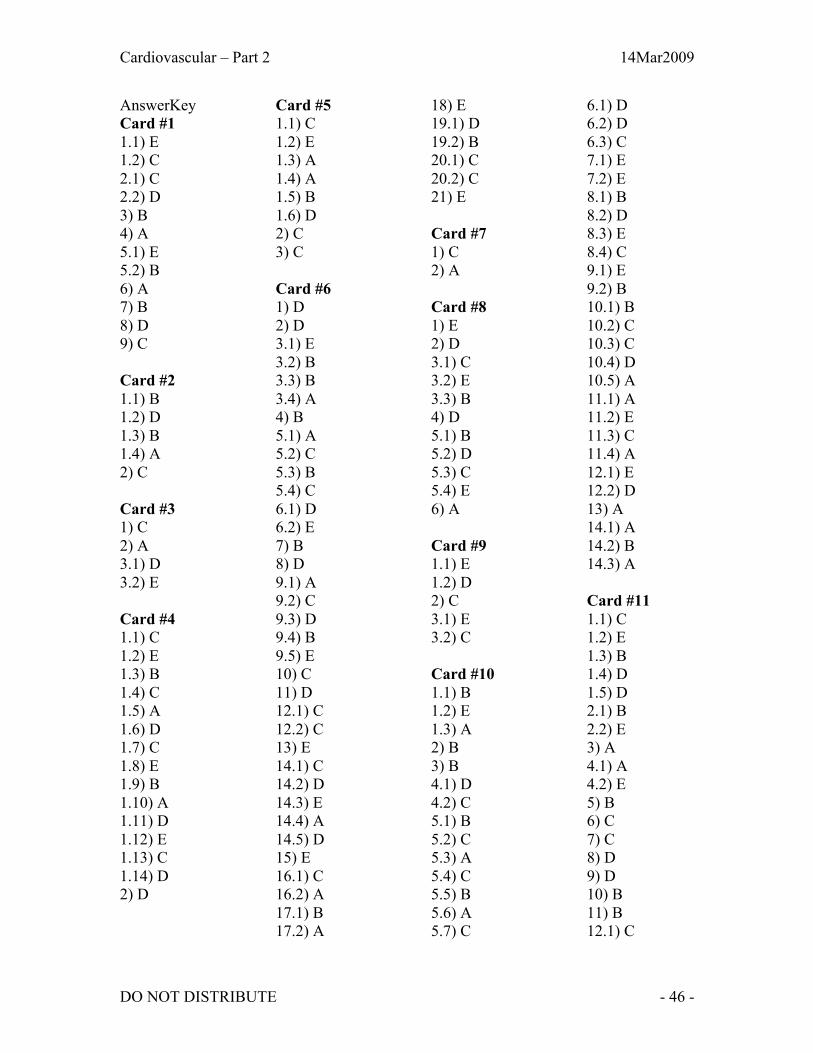
Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 46 -
AnswerKey
Card #1
1.1) E
1.2) C
2.1) C
2.2) D
3) B
4) A
5.1) E
5.2) B
6) A
7) B
8) D
9) C
Card #2
1.1) B
1.2) D
1.3) B
1.4) A
2) C
Card #3
1) C
2) A
3.1) D
3.2) E
Card #4
1.1) C
1.2) E
1.3) B
1.4) C
1.5) A
1.6) D
1.7) C
1.8) E
1.9) B
1.10) A
1.11) D
1.12) E
1.13) C
1.14) D
2) D
Card #5
1.1) C
1.2) E
1.3) A
1.4) A
1.5) B
1.6) D
2) C
3) C
Card #6
1) D
2) D
3.1) E
3.2) B
3.3) B
3.4) A
4) B
5.1) A
5.2) C
5.3) B
5.4) C
6.1) D
6.2) E
7) B
8) D
9.1) A
9.2) C
9.3) D
9.4) B
9.5) E
10) C
11) D
12.1) C
12.2) C
13) E
14.1) C
14.2) D
14.3) E
14.4) A
14.5) D
15) E
16.1) C
16.2) A
17.1) B
17.2) A
18) E
19.1) D
19.2) B
20.1) C
20.2) C
21) E
Card #7
1) C
2) A
Card #8
1) E
2) D
3.1) C
3.2) E
3.3) B
4) D
5.1) B
5.2) D
5.3) C
5.4) E
6) A
Card #9
1.1) E
1.2) D
2) C
3.1) E
3.2) C
Card #10
1.1) B
1.2) E
1.3) A
2) B
3) B
4.1) D
4.2) C
5.1) B
5.2) C
5.3) A
5.4) C
5.5) B
5.6) A
5.7) C
6.1) D
6.2) D
6.3) C
7.1) E
7.2) E
8.1) B
8.2) D
8.3) E
8.4) C
9.1) E
9.2) B
10.1) B
10.2) C
10.3) C
10.4) D
10.5) A
11.1) A
11.2) E
11.3) C
11.4) A
12.1) E
12.2) D
13) A
14.1) A
14.2) B
14.3) A
Card #11
1.1) C
1.2) E
1.3) B
1.4) D
1.5) D
2.1) B
2.2) E
3) A
4.1) A
4.2) E
5) B
6) C
7) C
8) D
9) D
10) B
11) B
12.1) C

Cardiovascular – Part 2 14Mar2009
DO NOT DISTRIBUTE - 47 -
12.2) B
13) C
14) E
15) E
16) A
17) A
18) E
19) D
20) C
21) D
22) B
23) D
24) B
25) A
26) E
27) C
28) D
29) C
30) C
31) B
32) B
33) A
34) B
35) E
36) D
37) C
38.1) D
38.2) C
38.3) B
38.4) A
Card #12
1.1) E
1.2) D
2) A
3) C
4) B
5) B
6) A
7) C
8) E
9) A
10) C
11) D
12) E
13) D
14) A
15) C
16) B
17) D
18) C
19) C
20) E
21) D
22) C
23) A
24) C
25) C
26) B
27) A
28) A
29) D
30.1) E
30.2) B
31) E
32) B
33) D
Card #13
1) C
2) D
3.1) D
3.2) A
4) C
5) B
6) D
7) C
8) C
9) D
Card #14
1) D
2) B
3) C
Card #15
1) D
2) B
3) B
Card #16
1) D
2) D
3) E
Card #17
1) E
2) A
3) D
4.1) C
4.2) A
4.3) D
4.4) B
5) C
6) B
7) A
8) C
9) F
10) G
11) D
12) E
13) D
14) C
15) D
Card #18
1) D
2) C
3) A
4) B
5) C
6) C
7) E
8) B
9.1) D
9.2) A
Card #19
1) C
2) C
3) B
4) D
5) A
6) E
7) E
8) B
9) A
10) E