q4 t ~)qd d~ j p,'tpbt 3
TRANSCRIPT
STATE OF SOUTH CAROLINA
(Caption of Case)Example: Application for a Class C Charter Certificate from
John Doe dba Doe's Limo
)
t ppl;cc.J;, -f,~ ~ C.less C. )
)
Q4 / ) t Pt CCRC )
t:t-ed 'rta ~)qd d~)
J p,'tpbtjI i r~~po4J-'~))
(Please type o
Submitted
BEFORE THEPUBLIC SERVICE COMMISSION
OF SOUTH CAROLINA
TRANSPORTATION COVER SHEET
tf this is your first time filing an application with the PSC, you will noihave a Docket Number. The Commission will assign one io you. tf youhave filed with the Commission before, a Docket Number wss assignedsnd should be entered above.
Telephone: l 5 3 0 (DO
Address: Fax:
Other:
Email:Y t i")Cc 80 lYXhl t" O~NOTE: The cover sheet and information contained herein neither replaces nor supplements the filing and service of pleadings or other papersas required by law. This form is required for use by the Public Service Commission of South Carolina for the purpose of docketing and mustbe filled out com letel .
NATURE OF ACTION (Check all that apply)
Application - Class A/A Restricted
Application - Class C Taxi
g Application - Class C Charter
Application — Class C Charter Bus
Application - Class C Non-Emergency
Application - Class C Stretcher Van
Application - Class E Household Goods
Application - Class E Hazardous Waste
Application
pc'k $C@r/ktI / Qll(S
Request for Reinstatement
Request for Extension to Comply with Order
Request for Order Granting Authority to Obtain a Certiftcat~e~~t,of Public Convenience and Necessity toj~&e scinded
Request for Cancellation of Certificate I()) tJ I~~;())5
Request for Suspension
Letter
Proposed Order
Publisher's Affidavit
Reservation Letter
Response
Return to Petition
Other:
c'i)
OO~O
Request for Name Change on Certificate
Request to Amend Scope of Authority
Request to Amend Tariff (rate increase, etc.)
Request to Amend Passenger Limit
Request
Exhibit
Late-Filed Exhibit
If you have any questions about this form, please contact the PUBLIC SERVICE COMMISSION at 803-896-
PUBLIC SERVICE COMMISSION OF SOUTH CAROLINA101 Executive Center Drive, Suite 100
Columbia, South Carolina 29210(Mailing address: Post Office Drawer 11649, Columbia, SC 29211)
Phone: (803) 896-5100 Fax: (803) 896-5199
APPLICATION FOR CERTIFICATE OF PUBLIC CONVENIENCE AND NECESSITY FOROPERATION OF MOTOR VEHICLE CARRIER
Date:
CLASS C - CHARTER
Application is hereby made for~errificate of Public Convenience.and Necessity, in accordance with the provisionof S.C. Code Ann., I'I 58-23-10, et seq. (1976), and amendments thereto.
1. Name under which business is to be conducted (corporation, partnership, or sole proprietorship, with or without trade name.)
I"QA af. 0 On'I Po sr S ree.4 r e ori ('.) 05
Street Address of Applicant
Mailing Address of Applicant (if different from street address)
5 -8g"I-h 0'lgPhone
'4 I ricitss intil I, COEmail Address
2. If the Applicant is an LLC or a corporation, a copy of the Certificate of Existence from the South CarolinaSecretary of State and the Articles of Incorporation must be attached. (If incorporated outside of SC, attach SouthCarolina Secretary of State "Foreign Corporation" Certificate.)
3. Select Entity Type: (Check one)Individual Owner/Sole Proprietorship
g Partnership - List names arid addresses of all person having an interest in the business.
Corporation - List names and addresses of two principal officers.
s 61
1 of 9
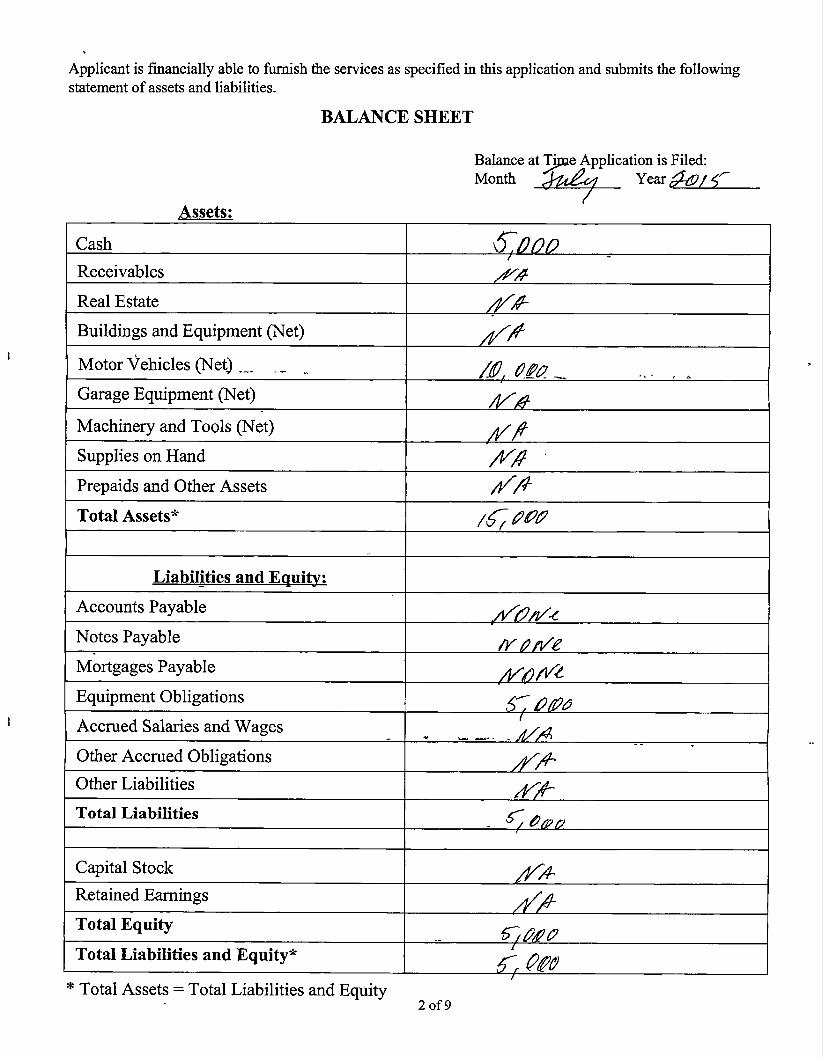
Applicant is financially able to furnish the services as specified in this application and submits the followingstatement of assets and liabilities.
BALANCE SHEET
Cash
Receivables
Assets:
Balance at ~Ti e Application is Filed:M th ~ Y
Real Estate
Buildings and Equipment (Net)
Motor Vehicles (Net)
Garage Equipment (Net)
Machinery and Tools (Net)
Supplies on Hand
Prepaids and Other Assets
Total Assets*
Liabilities and E ui
Accounts Payable
Notes Payable
Mortgages Payable
Equipment Obligations
Accrued Salaries and Wages
Other Accrued Obligations
Other Liabilities
Total Liabilities
Capital Stock
Retained Earnings
Total Equity
Total Liabilities and Equity*
e Total Assets = Total Liabilities and Equity2 of 9
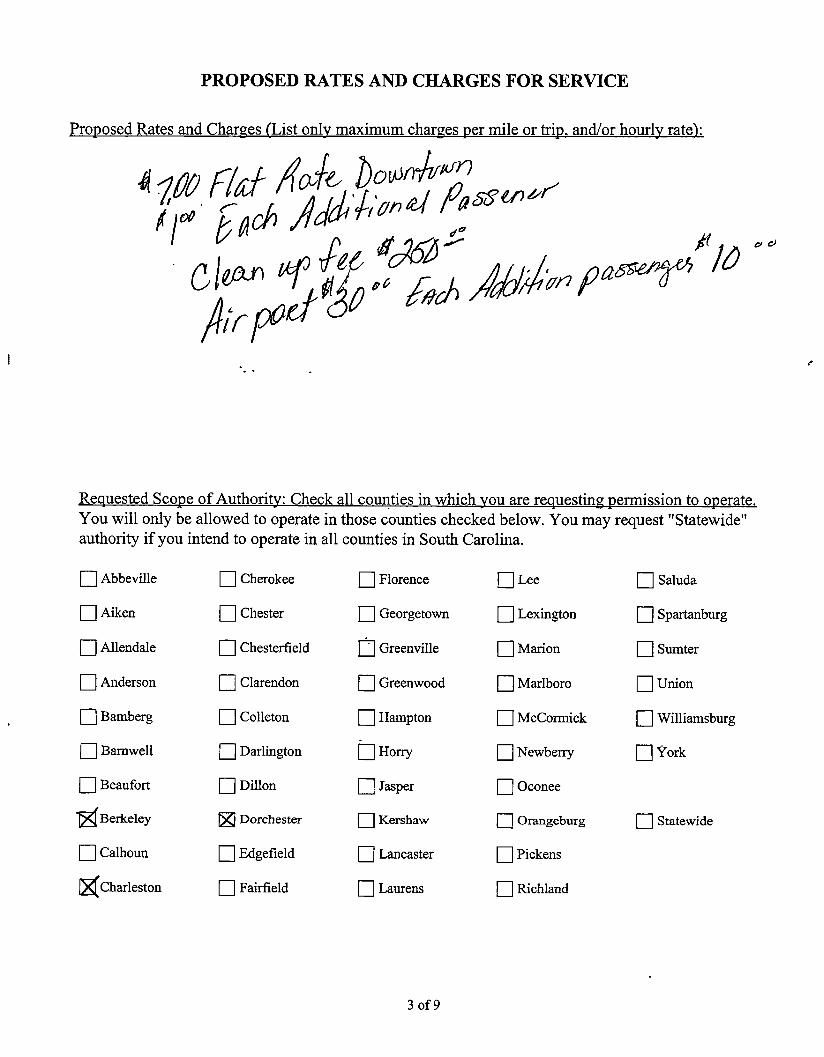
PROPOSED RATES AND CHARGES FOR SERVICE
Pro osed Rates and Char es List onl maximum char es ermile or tri and/orhourl rate
4gu Fl&E e,&"~gt Pfl
cia f „'z„+& gg4'~)'r
Re uested co e of Authori Check all counties in which ou are re uestin ermission to o crateYou will only be allowed to operate in those counties checked below. You may request "Statewide"authority if you intend to operate in all counties in South Carolina.
Abbeville
Aiken
Allendale
Anderson
Bamberg
Barnwell
Beaufort
@Berkeley
Calhoun
gCharleston
Cherokee
Chester
Chesterfield
Clarendon
Colleton
Darlington
Dillon
Q Dorchester
Edgefield
Fairfield
Florence
Georgetown
Greenville
Greenwood
Hampton
Horry
Jasper
Kershaw
Lancaster
Laurens
Lee
Lexington
Marion
Marlboro
McCormick
Newherry
Oconee
Orangeburg
Pickens
Richland
Selude
Spartanburg
Sumter
Union
Williamsburg
York
Statewide
3of9
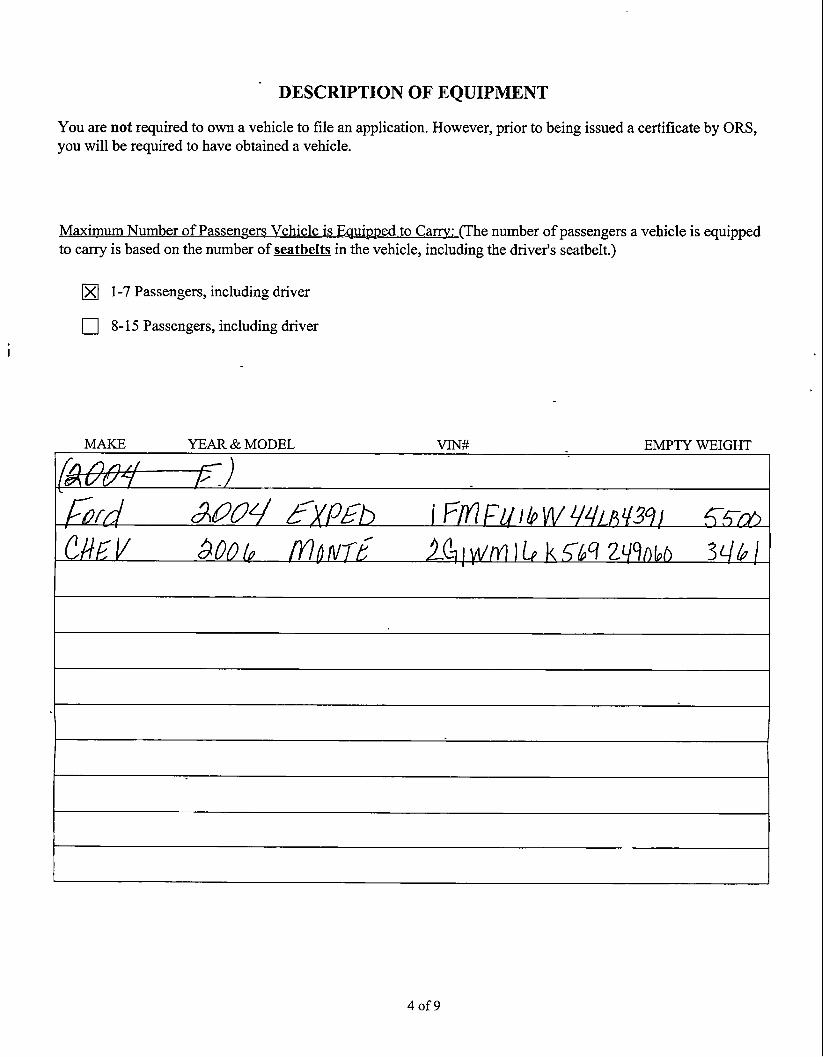
DESCRIPTION OF EQUIPMENT
You are not required to own a vehicle to file an application. However, prior to being issued a certificate by ORS,you will be required to have obtained a vehicle.
xim Nu er ofPasse e s Vehicle i E ui ed to Ca . (The number ofpassengers a vehicle is equippedto carry is based on the number of seatbelts in the vehicle, including the driver's seatbelt.)
X 1-7 Passengers, including driver
8-15 Passengers, including driver
MAKE YEAR & MODEL VINtt EMPTY WEIGHT
4of9
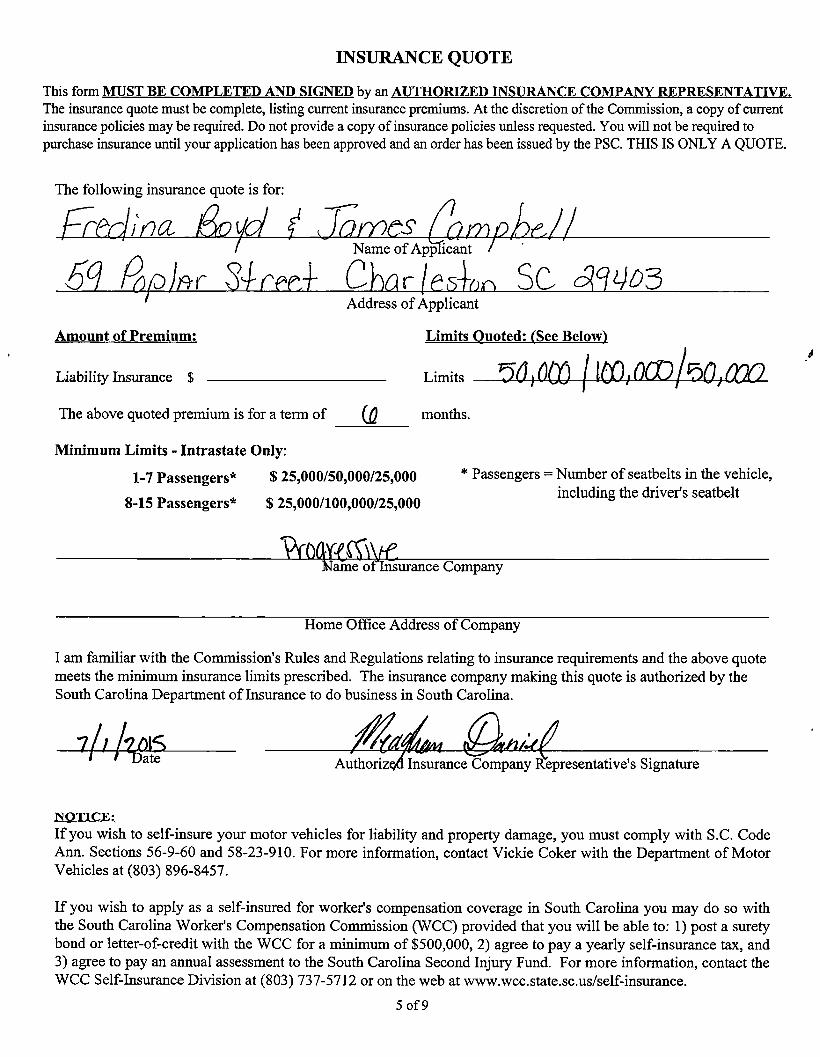
INSURANCE QUOTE
This form CO L D D SIGNED by an AUTHORIZED IN U CE CO REPRESENTAT VEThe insurance quote must be complete, listing current insurance premiums. At the discretion of the Commission, a copy of currentinsurance policies may be required. Do not provide a copy of insurance policies unless requested. You will not be required topurchase insurance until your application has been approved and an order has been issued by the PSC. THIS IS ONLY A QUOTE.
The following insurance quote is for:
Name ofApp icant
Address ofApplicant
Amount of Premium: Limits uoted See Below
Liability Insurance $ Limits
The above quoted premium is for a term of (g months.
Minimum Limits - Intrastate Only:
1-7 Passengers* $ 25,000/50,000/25,000
8-15 Passengers* $ 25,000/100,000/25,000
* Passengers = Number of seatbelts in the vehicle,including the driver's seatbelt
arne o urance Company
Home Office Address of Company
I am familiar with the Commission's Rules and Regulations relating to insurance requirements and the above quotemeets the minimum insurance limits prescribed. The insurance company making this quote is authorized by theSouth Carolina Department of Insurance to do business in South Carolina.
Authoriz Insurance Company Representative's Signature
NOTICE:If you wish to self-insure your motor vehicles for liability and property damage, you must comply with S.C. CodeAnn. Sections 56-9-60 and 58-23-910. For more information, contact Vickie Coker with the Department of MotorVehicles at (803) 896-8457.
If you wish to apply as a self-insured for worker's compensation coverage in South Carolina you may do so withthe South Carolina Worker's Compensation Commission (WCC) provided that you will be able to: 1) post a suretybond or letter-of-credit with the WCC for a minimum of $500,000, 2) agree to pay a yearly self-insurance tax, and3) agree to pay an annual assessment to the South Carolina Second Injury Fund. For more information, contact theWCC Self-Insurance Division at (803) 737-5712 or on the web at www.wcc.state.sc.us/self-insurance.
5 of 9
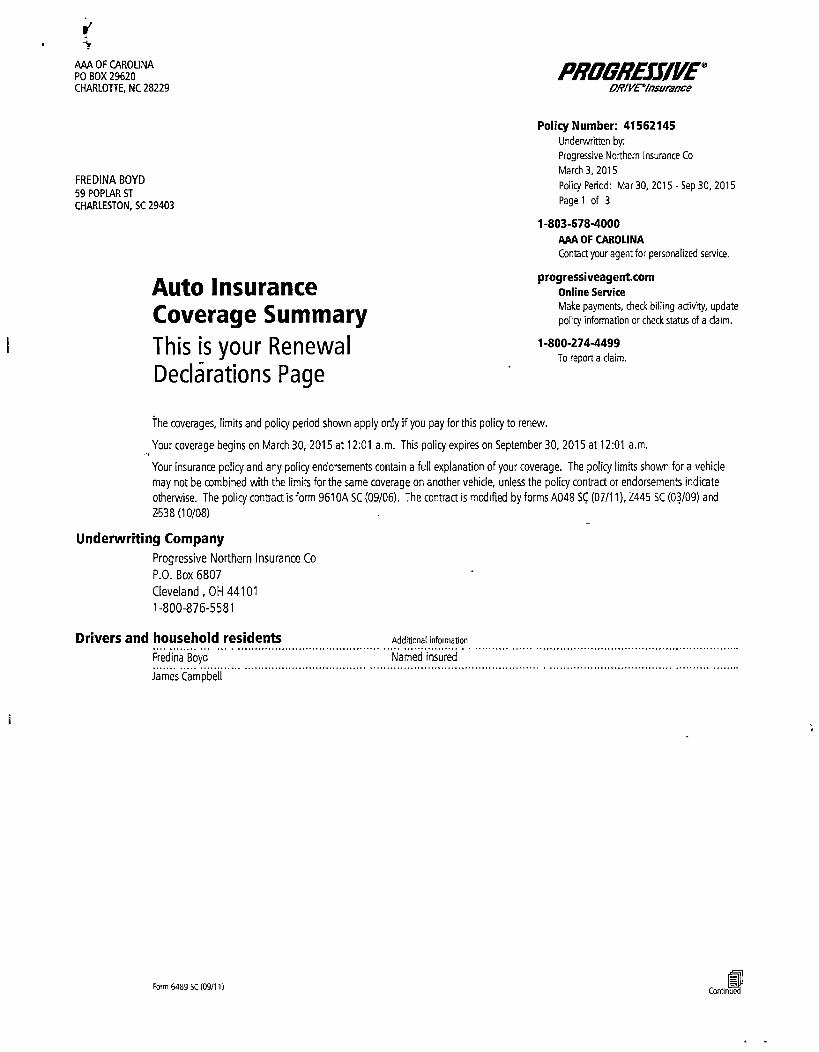
AAA OF CAROLINAPO BOX 29620CHARLOTTE, NC 28229
PRC78REJJIVE'27P/red/esurience
FREDINA BOYD
59 POPLAR ST
CHARLESTON, SC 29403
Auto InsuranceCoverage SummaryThis is your RenewalDeclarations Page
Policy Number: 41562145Underwditten by:
Progressive Northern Insurance Co
March 3, 2015
Policy Period: Mar 30, 2015 - Sep 30, 2015
Page I of 3
1-803-678&000AAA OF CAROLINA
Contact your agent for personalized service.
progressiveageat.cornOnline ServiceMake payments, check billing activity, update
policy information or check status of a da)m.
1-800-274-4499To report a claim.
The coverage, limits and policy period shown apply only if you pay for this policy to renew.
Your coverage begins on March 30, 2015 at 12:01 a.m. This policy expires on September 30, 2015 at 12:01 a.rn,
Your insurance policy and any policy endorsements contain a full explanation of your coverage. The policy fimits shown for a vehicle
may not be combined with the limits for the same coverage on another vehicle, unless the policy contract or endorsements indicate
otherwise. The policy contract is form 9610A SC (09/06). The contract is mcd)fied by forms A048 SC (07/11). Z445 SC (03/09) and
2538 (10/08)
Underwriting CompanyProgressive Northern Insurance Co
P.O. Box 6807
Cleveland, OH 441011-800-876-5581
Drivers and household residentsFredina Boyd
)ames Campbell
Add|))onal information
Named insured
n)rm 6489 sc (os/) n NICan/)nued
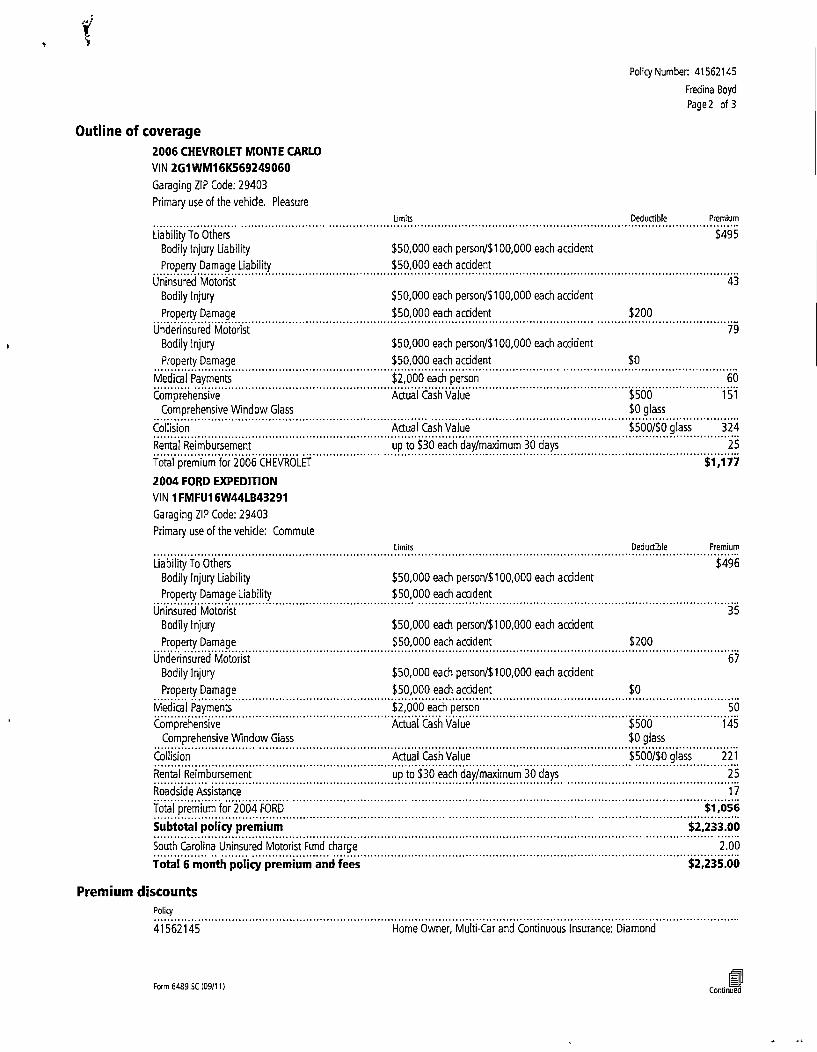
Outline of coverage2006 CHEVROLET MONTE CARLO
VIN 2GTWMI 6K569249060
Garaging ZIP Code: 29403
Primary use of the vehicle. Pleasure
Policy Number: 41562145
Fredina Boyd
Page2 of 3
Limits Oeduttrble Premium
Liability To Others
Bodily Injury Liability
Property Damage Liability
Uninsured Motorist
Bodily Injury
Property Damage
Underinsured Motorist
Bodily Injury
Property Damage
Medical Payments
ComprehensiveComprehensive Window Glass
Collision
Rental Reimbursement
Total premium for 2006 CHEVROLET
2004 FORD EXPEDITION
VIN 1FMFU1 6W44LB43291
Garaging ZIP Code: 29403
Primary use of the vehide: Commute
$ 50,000 each person/5 I 00,000 each acddent
$ 50,000 each accident
$ 50,000 each person/f100,000 each accident
$ 50,000 each accident
$ 50,000 each person/$ 100,000 each accident
$ 50,000 each accident
$2,000 each person
Actual Cash Value
Aetna I Cash Value
up to $ 30 each day/maximum 30 days
Ltmtts
$495
43
$ 200
79
60
$ 500 151
ID glass
$ 500/$0 glass 324
25
$1,177
Oedunrble Premium
Liability To Others
Bodily Injury Liability
Property Damage Liability
Uninsured Motorist
Bodily Injury
Property Damage
Underinsured Motorist
Bodily Injury
Property Damage
Medical Payments
ComprehensiveComprehensive Window Gian
$ 50,000 each persorV$ 1 00,000 each accident
$ 50,000 each acodent
$ 50,000 each person/$ 100,000 each acrident
$ 50,000 each acddent
$ 50,000 each person/$ 100,000 each accident
$ 50,000 each acddent
$2,000 each person
Actual Cash Value
$ 200
$ 0
$ 500$0 glass
$ 496
67
50
145
Collision
Rental Reimbursement
Roadside Assistance
Total premium for 2004 FORD
Subtotal policy premium
South Carolina Uninsured Motorist Fund charge
Total 6 month policy premium and fees
Actual Cash Value
up to $ 30 each day/maximum 30 days
$ 500/$0 glass 221
25
17
$1,056
$2,233.00
2.00
$2,235.00
Premium discountsPdrtqr
41562145 Home Owner, Multi-Car and Continuous Insurance: Diamond
Corm 9489 SC t09/11) CoououedNj
Lienholder informationWe send certain notices such as coverage summaries and cancellation notices to the following:
Vehicle Lienholder
Policy Number: 41562145
Fredina Boyd
Page3 of 3
2006 CHEVROLET MONTE CARLO
2GIWMI6K569249060Rmc Financial Servic
N Charleston, SC 29406
2004 FORD EXPEDITION
I FMFU16W44LB43291
CREDIT ACCEPTANCE
SOUTHFIELD, Ml 48037
rrrrn 6/ss sc (090 ) )
Fax recipient informationTo:
Fax ry:
Number of pages faxed: 3
PRD8REJ3/bEE'R/YE'Insurance
Policy Number: 41562145Underwritten by:
Progressive Northern insurance Co
Policyholder:Fredina Boyd
July1, 2013
Page 1 of 1
t 403-678-4000AAA OF CAROUNA
Contea your agent for personalized service.
Here are the policy documents you requestedVerification of InsuranceVerification of Insurance
Thank you for choosing Progressive.
Progressive offers several convenient service options:Contact your agent for personalized service and counsel when you are thinking about making changes to your policy.
Visit progressiveagent.corn 24 hours a day to view and pdint policy documents, quote a change to your policy, updatepolicy information, and view claims information. While on progressiveagent.corn be sure to provide us with your e-mail
address to receive reminders about upcoming payments, transaction confirmations, and claims instructions.
Call our Customer Service number, 1-800-876-5581, to make or confirm payments over the phone, order ID cards and
Dedarations pages, and more.
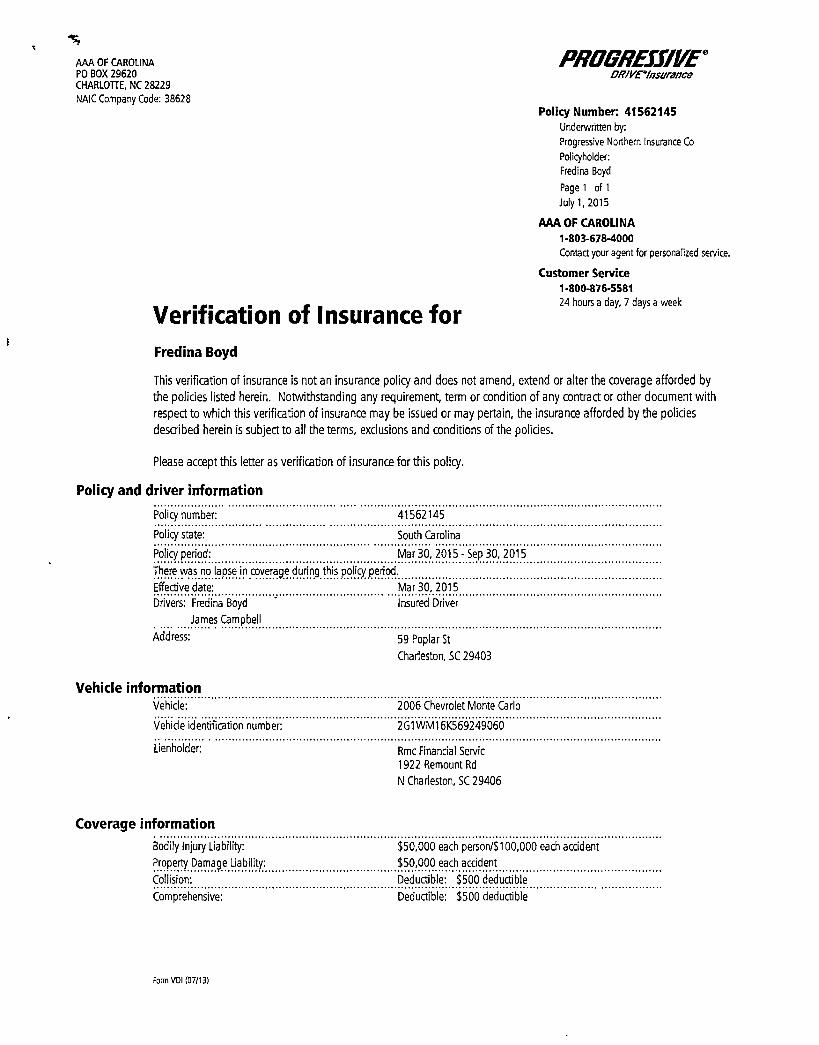
AAA OF CAROLINAPO BOX 29620CHARL01TE, NC 28229NAIC Company Code: 38628
Yerification of Insuranre forFredina Boyd
P8ÃiFEff/YEDRIVE'Insunrnnn
Policy Number: 41562145Underwniten by:
Progressive Northern Insurance Co
Policyhoider:
Fredma Boyd
Page1 oi1
July I, 201 5
AAA OF CAROLINA1-803-628-4000Contact your agent for personalized rewire.
Customer Service1-800-876-558124 hours a day, 7 days a week
This vedification of insurance is not an insurance policy and does not amend, extend or alter the coverage afforded by
the polides listed herein. Notwithstanding any requirement, term or condition of any contract or other document with
respect to which this verification of insurance may be issued or may pertain, the insurance afforded by the policies
described herein is subject to all the terms, exclusions and conditions of the policies.
Please accept this letter as verification of insurance for this policy.
Policy and driver information
Policy number:
Policy state:
Policy period
41562145
South Carohna
Mar 30, 2015- Sep 30, 2015
There was no lapse in coverage during this poiiryperiod.
Effective date: Mar 30, 2015
Drivers: Fredina Boyd Insured Driver
James Campbell
Address: 59 Poplar St
Charleston, SC 29403
Vehicle informationVehicle:
Vehide identification number:
Uenholder:
2006 Chevrolet Monte Carlo
201WMI6K569249060
Rmc Financial Servic
1922 Remount Rd
N Charleston, SC 29406
Coverage information
Bodily Injury Liability:
Property Damage Liability:
Collision:
Comprehensive:
$ 50,000 each person/$ 100,000 each accident
$ 50,000 each auident
Deductible: $ 500 deductible
Deductible; $ 500 deductible
Form VOI 107/11)
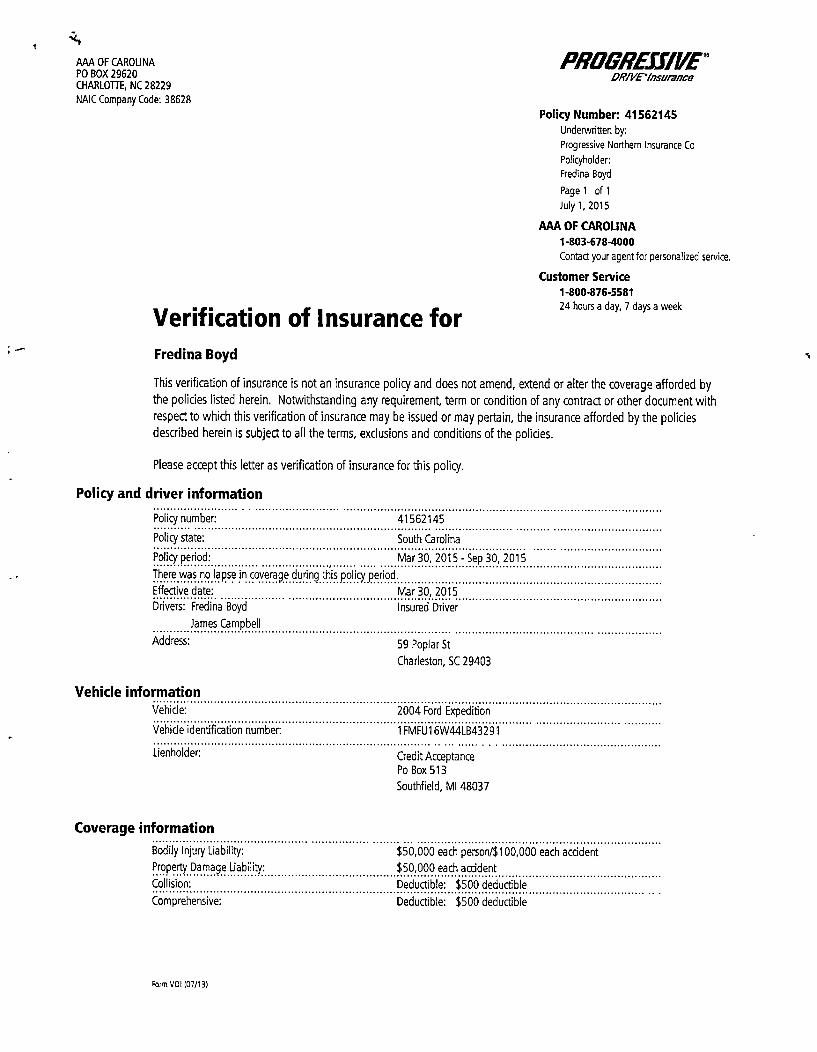
AAA OF CAROLINAPO BOX 29620CHARLOTTE, NC 28229NAIC Company Code: 38628
Verification of Insurance forFredina Boyd
PE88ÃEJJIYEeDRIVE'azsurrusu
Policy Number. 41562145Underwritten by:
Progressive Northern Insurance Co
Policyholder:
Fredina Boyd
Pager or1
July I, 2015
AAA OF CAROLINA
1-803-678-4000Contactyouragentfor personalized service.
Customer Service1-8004376-558124 hours a day. 7 days a week
This verification of insurance is not an insurance policy and does not amend, extend or alter the coverage afforded bythe policies listed herein. Notwithstanding any requirement, term or condition of any contract or other document withrespect to which this verification of insurance may be issued or may pertain, the insurance afforded by the policiesdescribed herein is subject to all the terms, exclusions and conditions of the policies.
Please accept this letter as verification of insurance for this policy.
Policy and driver information
Policy number:
Policy state
Policy period
41562145
South Carolina
Mar 30, 2015 - Sep 30, 2015
There was no lapse in coverage during this policy period.
Effective date: Mar 30, 2015Drivers: Fredina Boyd Insured Driver
James Campbell
Address: 59 Poplar St
Charleston, SC 29403
Vehicle informationVehicle
Vehide identification number:
Lienholder;
2004 Ford Expedition
I FMFU16W44LB43291
Credit AcceptancePo Box 513
Southfield, Ml 48037
Coverage informationBodily Injury Liability
Property Damage Liability:
Collision:
Comprehensive:
$ 50,000 each person/$ 100,000 each accident
$ 50,000 each acddent
Deductible: $ 500 deductible
Deductible: $ 500 deductible
Form vol Inr/I 31
Exhibit Fit Willin and Able FWA
Name of Applicant
I. Are there currently any outstanding judgments against the Applicant?
0 Yes g No
IfYes, indicate nature ofjudgement(s) against applicant.
2. Is Applicant familiar with all statutes and regulations, including safety regulations and governing for-hire motorcarrier operations in South South Carolina, and does Applicant agree to operate in compliance with thesestatutes and regulations?
@ Yes 0 No
3. Is Applicant aware of the Commission's insurance requirements and the insurance premium costs associatedtherewith?0 Yes Pl No
6of9
Exhibit on Driver ualifications
1. Applicant understands that all drivers must be a minimum of 18 years of age.
Yes Q No
2. Applicant understands that a certified copy of the driver's three (3) year driving record issued by the SC DMVand such record from the DMV of the state in which the driver is or has been domiciled for such period mustbe maintained in the Applicant's business office.
Q Yes Q No
3. Applicant understands that a criminal history background check from the state where the driver currently livesmust be maintained in the Applicant's business office. Yes Q No
4. Applicant understands that all drivers operating a vehicle under a Class C Certificate must have intheir possession when operating a charter vehicle, a valid driver's license issued by the SC DMV or the currentstate of residence of the driver.
P Yes Q No
5. Applicant understands that all Class C Certificate holders are prohibited from employing or leasingvehicles to drivers who are registered, or required to be registered, as sex offenders with the South CarolinaState Law Enforcement Division or any national registry of sex offenders.
5i Yes Q No
7of9
PUBLIC SERVICE COMMISSION OF SOUTH CAROLINAPOST OFFICE DRAWER 11649
COLUMBIA, SOUTH CAROLINA 29211
Applicant is familiar with the provision of S.C. Code Ann. II58-23-10, et seq.(1976), and amendments thereto,and R.103-100 through R.103-241 of the Commission's Rules and Regulations for Motor Carriers (Volume 26,S.C. Code Ann. Regs., 1976), and R.38-400 through R.38-503 of the Department of Public Safety's Rules andRegulations for Motor Carriers (Volume 23A, S.C. Code Ann., 1976) and amendments thereto, and herebypromises compliance therewith.
S.C. Code Ann. Section 58-3-250 states, in part, that every final order of the Commission must be served byelectronic service, registered or certified mail, upon the parties to the proceeding or their attorneys.
Please check the applicable box:e Applicant AGREES to receive future Commission orders related to the Applicant's authority in South Carolina
through the Commission's eService System. The Applicant authorizes the Commission to serve its orders by using the e-mail address as it appears on page one of this Application. To sign up for eService notifications, please visit www.psc.sc.gov to create a My DMS account.
The Applicant DOES NOT AGREE to receive future Commission orders related to the Applicant's authority in SouthCarolina through the Commission's eService System.
The Applicant for the Certificate of Public Convenience and Necessity as set forth in the foregoing, swear oraffirm that all statements contained in the above application are true and correct.
Title of Applicant (e.g. President, Owner, etc.)
STATE OF SOUTH CAROLINA
rOUNTY ()I )
=-==o=aZ -tva-.r ~Jell, 20/u
=. -Noi" ty Public -: .
gg (hill r-.Commission Expires a " " . -'-%55CI24 2(if/
8of9