putting the quality in qapi · spo ntaneo us feedback fro m resident s, fam ilies, o r staff ( co m...
TRANSCRIPT

8/19/2019
1
PUTTING THE QUALIT Y IN QAPI
QUALITY ASSESSMENT AND
PERFORMANCE IMPROVEMENT
SO WHAT IS QAPI???
Quality Assessment and Performance
Improvement (QAPI) is a data-driven and
pro-active approach to “quality”
improvement. Activities of this
comprehensive approach are designed to
involve all members of an organization to
continuously identify opportunities for
improvement and addresses gaps in
systems through planned interventions in
order to improve the overall quality of
the care and services delivered to
patients.

8/19/2019
2
REGULATIONACCORDING TO CMS YOU MUST ENSURE YOU
CONTINUOUSLY IDENTIFY AND CORRECT QUALITY DEFICIENCIES AS WELL AS SUSTAIN PERFORMANCE
IMPROVEMENT.
QA (QUALITY ASSESSMENT) IS A PROCESS OF MEETING
QUALITY STANDARDS AND TYPICALLY SET TO COMPLY
WITH REGULATIONS.
PI (PERFORMANCE IMPROVEMENT) IS A PRO-
ACTIVE AND CONTINUOUS STUDY OF PROCESSES WITH THE INTENT TO PREVENT OR DECREASE THE LIKELIHOOD
OF PROBLEMS. FIX UNDERLYING CAUSES OF PERSISTENT/SYSTEMIC
PROBLEMS.
FEDERAL REGISTER –JULY 2019
• Quality Assurance and Performance Improvement (§483.75)
• We propose to revise the requirement for facilities to implement a Quality Assurance and Performance Improvement (QAPI) program by removing prescriptive requirements to allow facilities greater flexibility in tailoring their QAPI program to the specific needs of their individual facility.
• The current QAPI requirement at §483.75(c) requires facilities to establish requirements for QAPI program feedback, data systems and monitoring. Facilities must maintain effective systems to obtain and use feedback and input from direct care/direct access workers, other staff, residents, resident representatives and families to identify opportunities for improvement. The data collected under the QAPI requirement could be used to meet portions of the facility assessment requirements and vice versa.

8/19/2019
3
FEDERAL REGISTER –JULY 2019
• We believe that in facilities with a high staff turnover,
assessments should take place as frequently as necessary
and the issue should be addressed in the QAPI plan.
Facilities must present their QAPI plan at each annual
recertification survey and upon request during any other
survey and to CMS upon request. The QAPI program
must be ongoing, comprehensive, and address the full
range of care and services provided by the facility and
must present documentation and evidence of its ongoing
QAPI program’s implementation and the facility’s
compliance with the program requirements.
TIE IT ALL TOGETHER NOW
Emergency Preparedness
QAPIFacility
assessment

8/19/2019
4
PRESENTATION TO SURVEYORSUPON REQUEST
• Must present the QAPI plan at each
annual recertification survey
• Upon request during any other survey
and to CMS upon request
• Must present
– documentation and evidence of its
on-going QAPI program’s
– implementation and the facility’s
compliance with the program
CONCERNS SUBMITTED TO CMS
Concerns regarding how the QAPI documents will be used during facility surveys and
one commenter noted that QAPI-based citations in recent surveys have been used as a “gotcha”
citation instead of focusing on true quality outcomes.
• Commenters noted that requiring facilities to disclose their QAPI-related documents limits a facility’s ability to identify and prioritize what they believe is important and instead requires them to monitor everything all the time.

8/19/2019
5
CMS WANTS IN PLACE
Facilities to demonstrate compliance and to ensure that a facility’s QAPI program is ongoing.
As part of our certification and enforcement efforts, we have a responsibility to determine compliance using evidence provided by facilities to support compliance decisions.
Therefore, we note that to avoid the risk of facility noncompliance, facilities must be able to provide satisfactory evidence that demonstrates compliance with the requirements.
Furthermore, we expect that any review of QAPI related documents would occur at the end of the survey, after completion of investigation into all other requirements to ensure that concerns are identified by the survey team independent of the QAPI document review.
STAYING IN PLACE
• Facilities establish and implement written policies and procedures for feedback, data collection systems, and monitoring, including adverse event monitoring.
• Requires facilities to take actions aimed at performance improvement and, after implementing those actions, measure its success, and track performance to ensure that improvements are realized and sustained, and remove the detailed requirements for policies.
• Tailoring their QAPI programs to the specific needs of the facility.
• Making them consistent with the QAPI requirements for other Medicare and Medicaid participating providers, such as hospitals and other major inpatient provider types.

8/19/2019
6
A LITTLE BACKGROUND
Mandated in the Affordable Care Act,
enacted March 2010
Legislation requires the Centers for
Medicare & Medicaid Services (CMS) to
establish QAPI program standards and
provide technical assistance to nursing
home providers.
F TAG – PHASE 2 & 3
• F865 - QAPI Program/Plan, Disclosure /Good Faith Attempt
• F866 - QAPI/QAA Data Collection and Monitoring
• F867 - QAPI/QAA Improvement Activities

8/19/2019
7
F865-QAPI
• §483.75(b) Program design and scope (Element 1)
‒ A facility must design its QAPI program to be ongoing, comprehensive, and to address the full range of care and services provided by the facility. It must:
• Address all systems of care and management practices;
• Include clinical care, quality of life, and resident choice;
• Utilize the best available evidence to define and measure indicators of quality and facility goals that reflect processes of care and facility operations that have been shown to be predictive of desired outcomes for residents of a SNF or NF.
• Reflect the complexities, unique care, and services that the facility provides.
F865-QAPI
• §483.75(f) Governance and leadership (Element 2)
‒ The governing body and/or executive leadership (or organized group or individual who assumes full legal authority and responsibility for operation of the facility) is responsible and accountable for ensuring that:
• An ongoing QAPI program is defined, implemented, and maintained and addresses identified priorities.
• The QAPI program is sustained during transitions in leadership and staffing;
• The QAPI program is adequately resourced, including ensuring staff time, equipment, and technical training as needed;

8/19/2019
8
F865-QAPI
• The QAPI program identifies and prioritizes problems and opportunities that
reflect organizational process, functions, and services provided to residents based
on performance indicator data, AND resident AND staff input, and other
information.
– Corrective actions address gaps in systems, and are evaluated for effectiveness;
– Clear expectations are set around safety, quality, rights, choice, and respect.
F865-QAPI§483.75(a) Quality assurance and performance improvement (QAPI) program. [§483.75 and all subparts will be implemented beginning November 28, 2019 (Phase 3), unless otherwise specified]
• Each LTC facility, including a facility that is part of a multiunit chain, must develop, implement, and maintain an effective, comprehensive, data-driven QAPI program that focuses on indicators of the outcomes of care and quality of life. The facility must:
– Maintain documentation and demonstrate evidence of its ongoing QAPI program that meets the requirements of this section.
– Present its QAPI plan to the State Survey Agency [implemented November 28, 2017 (Phase 2)]
– Present its QAPI plan to a State Survey Agency or Federal surveyor at each annual recertification survey and upon request during any other survey and to CMS upon request; and
– Present documentation and evidence of its ongoing QAPI program's implementation and the facility's compliance with requirements to a State Survey Agency, Federal surveyor or CMS upon request.
16

8/19/2019
9
F866-QAPI
• §483.75(c) Program feedback, data systems and monitoring. (Element 3)
• A facility must establish and implement written policies and procedures for feedback, data collections systems, and monitoring, including adverse event monitoring. The policies and procedures must include, at a minimum, the following:
– Facility maintenance of effective systems to obtain and use of feedback and input
– Facility maintenance of effective systems to identify, collect, and use data and information from all departments, including but not limited to the facility assessment required
F TAG 866 CONTINUED
• §483.75(c)(2) Facility maintenance of effective systems to identify, collect, and use data and information from all departments, including but not limited to the facility assessment required at §483.70(e) and including how such information will be used to develop and monitor performance indicators.
• §483.75(c)(3) Facility development, monitoring, and evaluation of performance indicators, including the methodology and frequency for such development, monitoring, and evaluation.
• §483.75(c)(4) Facility adverse event monitoring, including the methods by which the facility will systematically identify, report, track, investigate, analyze and use data and information relating to adverse events in the facility, including how the facility will use the data to develop activities to prevent adverse events.

8/19/2019
10
F867-QAPI
• §483.75(d) Program systematic analysis and systemic action. (Element 5-)
• The facility must take actions aimed at performance improvement and, after implementing those actions, measure its success, and track performance to ensure that improvements are realized and sustained.
• The facility will develop and implement policies addressing:
– How they will use a systematic approach;
– How they will develop corrective actions, and;
– How the facility will monitor the effectiveness to ensure that improvements are sustained.
F867-QAPI
• §483.75(e) Program activities (PIP-Element 4).
• The facility must set priorities for its performance improvement activities that focus on high-risk, high-volume, or problem-prone areas;
• Performance improvement activities must track medical errors and adverse resident events, analyze their causes, and implement preventive actions and mechanisms that include feedback and learning throughout the facility.
• The facility must conduct distinct performance improvement projects (PIP). The number and frequency of improvement projects conducted by the facility must reflect the scope and complexity of the facility's services and available resources, as reflected in the facility assessment required. Improvement projects must include at least annually a project that focuses on high risk or problem-prone areas.

8/19/2019
11
OTHER AREAS QAPI RELATED
• F607-Abuse
• §483.12(b)(4) Establish coordination with the QAPI program required under §483.75.
• F801-Food and Nutrition Staff
• Participating in the quality assurance and performance improvement (QAPI), as described in §483.75, when food and nutrition services are involved
• F944-Training Requirements
• §483.95(d) Quality assurance and performance improvement.
• A facility must include as part of its QAPI program mandatory training that outlines and informs staff of the elements and goals of the facility's QAPI program as set forth at § 483.75.
FIVE MAKE THAT SEVEN ELEMENTS FOR FRAMING QAPI IN NURSING HOMES
• CMS has identified five strategic elements that are basic
building blocks to effective QAPI. These provide a
framework for QAPI development.
1. Design & Scope
2. Governance & Leadership
3. Feedback, Data Systems & Monitoring
4. Performance Improvement Projects (PIPS)
5. Systematic Analysis & Systemic Action
6. Program Activities
7. Quality Assessment and Assurance
8/19/2019
12
E L E M E N T # 1 D E S I G N & S C O P EI N C I D E N T S / A D V E R S E E V E N T S / N E A R M I S S E S
S U R V E Y & C E R T I F I C AT I O N F I N D I N G S
S P O N T A N E O U S F E E D B A C K F R O M R E S I D E N T S , F A M I L I E S , O R S T A F F ( C O M P L A I N T S )
P O C - P L A N O F C O R R E C T I O N
DESIGN &
SCOPE
• Quality assurance and performance improvement program.
• (a) Program design and scope. A facility must design its QAPI program to be ongoing, comprehensive, and capable of addressing the full range of care and services provided by the facility.
• (b) Program feedback, data systems and monitoring. A facility must establish and implement written policies and procedures for feedback, data collections systems, and monitoring, including adverse event monitoring.
• (c) Program systematic analysis and systemic action. The facility must take actions aimed at performance improvement and, after implementing those actions, measure its success, and track performance to ensure that improvements are realized and sustained.
8/19/2019
13
E L E M E N T # 2G O V E R N A N C E &
L E A D E R S H I PMUST E S TAB L I SH A C L I MAT E O F O P EN COMMUN I CAT ION AND R E S P ECT.
E S TAB L I SH AN ENV I RONMENT WHER E CA R EG I V E R S , R E S I D ENT S , AND FAM I L I E S F E E L F R E E TO S P EAK U P TO I D ENT I F Y A R EA S THAT N E ED I M P ROV EMENT
EXPECT AND BU I LD E F F E CT I V E T EAMWORK AMONG D E PARTMENT S AND CAR EG I V E R S .
E L E M E N T # 2I T T A K E S A L L N U R S I N G H O M E
S T A K E H O L D E R S T O T H I N K A N D S O L V E T H E S E P R O B L E M S .
MAINTENANCE , HOUSEKEEP ING & LAUNDRY TEAM
BOARD OF D IRECTORS
OFF ICE TEAM
CORPORAT ION
NURS ING TEAM
ADMIN ISTRATOR & D IRECTOR OF NURS ING
D IETARY TEAM
NOT FROM THE TOP DOWN

8/19/2019
14
CMS NEWS BRIEF
• For successful implementation, QAPI cannot be imposed
from the “top down.” Rather, all levels of staff in nursing
homes must be involved in planning and improving
systems and processes in order to get effective results.
Direct care staff have valuable and unique input which
are vital to the success of performance improvement. It’s
easy to say all levels of staff should be involved, but
harder to put into practice.
OPEN DOOR/TEAR DOWN SILOSPERSON CENTERED CARE
Let direct care staff know that their experiences with the
residents are invaluable to the QAPI process. Their
hands-on knowledge of the resident and the day-to-day
processes of the nursing home are necessary to the
QAPI discussion and planning.
Residents should have control over their lives, influence
decisions which affect them, and know that their
opinions and preferences matter.
Put a family member on the PIP team.

8/19/2019
15
THE BIG PICTURE BASICS..
THE GOAL OF QAPI IS TO PROVIDE PERSON-CENTERED CARE – TO FOCUS ON THE
PERSON RECEIVING THE CARE.
•QAPI IS NOT ONLY A “PROGRAM” PER SAY; BUT IT IS “THE WAY WE DO OUR WORK”
•THE ABILITY TO THINK, MAKE DECISIONS, AND ACT AT ALL LEVELS OF MANAGEMENT IS A
PREREQUISITE FOR QAPI SUCCESS
IT’S EVERYWHERE
• QAPI is required in federally certified health
care Facilities
• –hospitals, transplant programs, dialysis
centers, ambulatory care, hospice,
nursing homes and many others
• QAPI is to be consistent across all settings at
a high level, but must also take into account
issues unique to the specific care setting

8/19/2019
16
E L E M E N T 3 – F E E D B A C K , D A T A S Y S T E M S A N D
M O N I T O R I N G
HOW DO YOU R EGULAR LY A S K FO R F E EDBACK F ROM R E S I D ENT S AND FAM I L I E S ?
HOW DO YOU DOCUMENT YOUR F E EDBACK ON A G R I E VANCE ?
A R E FAM I L I E S COMFORTAB L E COM ING TO SOMEONE I N TH E HOME ?
QAPI AS A
FOUNDATION
• Relies on the input of residents and families• Measurement of not only process but also outcomes
• For defining quality as ‘how work is done’• Broad scope – entire organization (all staff and all departments)
For person-centered care
• For systems thinking• Proactive analysis• Data and measurement driven• Supported by tools
Leadership expected to be a model
8/19/2019
17
HOW ARE WE HOW ARE WE HOW ARE WE HOW ARE WE GOING TO GOING TO GOING TO GOING TO GET ALL THIS GET ALL THIS GET ALL THIS GET ALL THIS DONEDONEDONEDONE
Data sources –
Publicly reported quality measures –survey results, census, marketing
MDS data/measures for Nursing Homes
Clinical data
Patient, family, and staff satisfaction surveys
QA MEETINGS
• How Often?
–Annually – right after
survey?
–Quarterly (required)
–Monthly
8/19/2019
18
QUALITY ASSURANCE AND PERFORMANCE IMPROVEMENT (QAPI)
• Definition (§483.75(g)(2)(ii)):
• “Quality Assurance and Performance Improvement (QAPI)”: Nursing home QAPI is the coordinated application of two mutually-reinforcing aspects of a quality management system: Quality Assurance (QA) and Performance Improvement (PI). QAPI takes a systematic, interdisciplinary, comprehensive, and data-driven approach to maintaining and improving safety and quality in nursing homes while involving residents and families, and all nursing home caregivers in practical and creative problem solving.
Q U A N T I T YQ U A N T I T YQ U A N T I T YQ U A N T I T YQ U A L I T Y
This Photo by Unknown Author is licensed under CC BY-SA-NC

8/19/2019
19
QAPI MUST…Involve all NH services
Prove that “priorities” were identified and chosen for
PI activities
Focus on indicators
Take actions to demonstrate improvement and are sustainable
Maintain documentary evidence of it’s operation and be able to demonstrate this to CMS
Developed, implemented and
maintained
Effective, ongoing, nursing facility-
wide – that is both clinical and non
clinical indicators of quality to be
measured
Data driven
E L E M E N T 4 – P E R F O R M A N C E I M P R O V E M E N T P R O J E C T : K E Y S
T O S U C C E S S C O N D U C T I N G P I P S D E V E L O P A S T E E R I N G C O M M I T T E E , A T E A M T H AT W I L L P R O V I D E Q A P I L E A D E R S H I P. T H E S T E E R I N G C O M M I T T E E M U S T L E A R N A N D U S E S Y S T E M S T H I N K I N G A N D :
has overall responsibility to develop and modify the plan,
review information and set priorities for PIPs
to work on particular problems, and
review results and determine the next steps.
M E D I C A L D I R E C TO R W H O I S A C T I V E LY E N G A G E D I N Q A P I .
P R O V I D E R E S O U R C E S F O R Q A P I — I N C L U D I N G E Q U I P M E N T A N D T R A I N I N G .
E S TA B L I S H A C L I M AT E O F O P E N C O M M U N I C AT I O N A N D R E S P E C T.
U N D E R S TA N D YO U R H O M E ’ S C U R R E N T C U LT U R E A N D H OW I T W I L L P R O M OT E P E R F O R M A N C E I M P R O V E M E N T.

8/19/2019
20
QUALITY ASSURANCE AND PERFORMANCE IMPROVEMENT (QAPI)
QUALITY ASSURANCE (QA)
• QA is the specification of standards for
quality of care, service and outcomes,
and systems throughout the facility for
assuring that care is maintained at
acceptable levels in relation to those
standards. QA is on-going and both
anticipatory and retrospective in its
efforts to identify how the organization is
performing, including where and why
facility performance is at risk or has
failed to meet standards.
PERFORMANCE IMPROVEMENT (PI)
• PI (also called Quality Improvement - QI) is the continuous study and improvement of processes with the intent to improve services or outcomes, and prevent or decrease the likelihood of problems, by identifying opportunities for improvement, and testing new approaches to fix underlying causes of persistent/systemic problems or barriers to improvement. PI in nursing homes aims to improve facility processes involved in care delivery and enhanced resident quality of life. PI can make good quality even better.
WHAT IS A PIP?
Performance Improvement Project
Purpose of the PIP…. To examine and improve care or services in areas that you have identified in needing attention.
These areas of attention vary from home to home.
Prioritize opportunities from collected data
Solicit departments for Performance Improvement Projects (or require them)
--Measure
–Process
–Outcome
8/19/2019
21
GUIDE FOR DEVELOPING A QAPI PIP TEAM
Describe how this group of people will work together,
communicate, and coordinate QAPI activities. This could include but is
not limited to:
Establishing a format and frequency for meetings
Establishing a method for communication between
meetings
Establishing a designated way to document and track
plans and discussions addressing QAPI.
Describe how the QAPI activities will be reported to the governing body; ( i.e., Board of Directors or
owner).
YOUR FIRST PIP!
Educating and training ALL staff on QAPI
Involve all NH services and employees! Everyone has ownership.
Explain that “priorities” will need to be identified and chosen for performance improvement. They can and need to be involved.
Action plans and PIP teams--members of the PIP team have EQUAL voice.
They will be asked to maintain documentary evidence of progress. Developed, implemented and maintained quality indicators and data collection—both clinical and nonclinical.
8/19/2019
22
ROOT CAUSE ANALYSIS
• Finding the real cause of the problem and dealing with it
rather than simply continuing to deal with the symptoms
• Asks why, why, why at each level
• Interdisciplinary- involves those closest to the situation
• Identifies changes that need to be made
• Identifies risks and how they contributed
• Leads the team to potential process improvements
HOW DO YOU DETERMINE YOUR PIP?
Collect data and prioritize….
-Residents at high-risk, high-volume
- Problem-prone areas
-How frequent is the problem
-The scope and severity
-Areas which affect health, outcomes,
patient safety, and quality of care.

8/19/2019
23
CHARACTERISTICS OF TEAMWORK
Characteristics of an effective team include the following:
• Having a clear purpose
• Having defined roles for each team member to play
• Having commitment to active engagement from each member. The roles of team workers may grow out of their original discipline (e.g., nurse, social worker, physical therapist) or their defined job responsibilities.
• Each team should be composed of interdisciplinary members (Family members and residents may be team members, though for confidentiality reasons, they may not review certain data or information that identifies individuals).
DATA SOURCES
Publicly reported quality measures –survey results, census, marketing
•MDS data/measures for Nursing Homes
•Clinical data
•Patient, family, and staff satisfaction surveys
Incidents/adverse events/near misses
•Survey & Certification findings
•Spontaneous feedback from residents, families, or staff (complaints)
•Other data measured at variable intervals (unexpectedly)
8/19/2019
24
GET FEEDBACK
•QUESTIONNAIRES •FEEDBACK INTERVIEWS
•OBSERVATION •DAILY REVIEWS
•CHART AUDIT
•DATA OBTAINED FROM EXISTING
DATABASES & SYSTEMS ..ARTIFACTS OF
CULTURE CHANGE
DATA COLLECTION
For all data sources, create a process to collect and document
• –Everyone can identify data for QAPI
Select a range of data that reflects your Homes unique characteristics and services

8/19/2019
25
EVERYONE'S RESPONSIBILITY
Assign responsibilities for data collection and monitoring – GIVE ownership
•–EVERYONE has a role (no more silos!)
•–Everyone should feel IMPORTANT/VALUED Assign
Have EQUAL voiceHave
Determine appropriate frequency based on the type of data Determine
NURSING DATA COLLECTION
ANTIPSYCHOTICS—DECREASE, DECREASE, DECREASE
MED ERRORS
CATHETERS—UTI’S
WEIGHTS
PERSONAL ALARMS

8/19/2019
26
NURSING
Restraints—bed rails, positioning devices
Falls... Trends by shift with interventions documented, falls with injuries investigated
Hand washing/glovingWounds—acquired, admitted with, improving?
ADMINISTRATION
Survey activity—hot line calls?
• Resident, family satisfaction?
01Physician trends–meeting their schedule in seeing their residents?
02Pharmacy trends–drug regimen reviews done timely, problems with availability of drugs
03Consultant reports—reviewed, interventions
04

8/19/2019
27
ADMINISTRATION
New Hires
• Criminal background checks
• EDL checked
• I-9 completed
• C.N.A. registry
• Family Care Registry
• Two step TB testing
• Hep B consents/documentation
• Corporate Compliance
• OIG
ADMINISTRATION
CULTURE CHANGE ARTIFACTS OF CULTURE CHANGE IS A CMS TOOL THAT CAN BE USED FOR YOUR QAPI DATA
WWW.ARTIFACTSOFCULTURECHANGE.ORG/ACCTOOL

8/19/2019
28
THERAPY DATA
PART A AND PART B NUMBER RECEIVING PT, OT, SPEECH
ARE ADMISSIONS BEING SCREENED TIMELY
DIETARY DATA
Hot food hot, cold food cold? (test trays, food temps? )
All food in freezers, coolers, storage
labeled and dated-- food grade containers
Refrigerators and freezer temps logged
Dishwashing temps logged

8/19/2019
29
ACTIVITY DATA
Evening and weekend activities
Resident council meetings
concernsresolved
residents informed of outcome
Individual and group activities
Are you meeting the needs of EACH elder
SOCIAL SERVICE DATA
Track Discharges—Hospital admissions
Code status reviewed on admission and at least quarterly with
care plan
Concerns and Lost articles
When not if resolved residents informed of
outcome
Residents rights taught to elders and
staff

8/19/2019
30
MAINTENANCE/LAUNDRY/HOUSEKEEPINGQA CONCERNS
Fire drills completed at varied times
Water temps
Fire extinguisher testing and maintenance
Generator logs/tests, emergency lighting logs/tests
Sprinkler inspections and are ALL heads clean
STAFFING!!!!
• Turnover rate?
• http://www.primaris.org/sites/
default/files/resources/Person-
Centered%20Care/Staff%20St
ability%20Toolkit_2010.pdf

8/19/2019
31
GOAL OF FEEDBACK, DATA SYSTEMS AND MONITORING
Create a system that allows your Home to effectively examine its performance
Make data-driven decisions about which improvement efforts to undertake
Evaluate how effective those improvement efforts are
DON’T JUST WATCH DATA
•IDENTIFY A BASELINE
•SET A GOAL •SET A THRESHOLD
•BENCHMARK
8/19/2019
32
WHAT’S THE DIFFERENCE?
QA IDENTIFIED THE MOUNTAIN SO YOU CAN FIX THE PROBLEM. (REACTIVE)
QAPI IDENTIFIES THE MOLEHILL BEFORE IT BECOMES THE MOUNTAIN. (PROACTIVE)
MOVING FROM FIGHTING FIRES TO PREVENTING
THEM!
A NEW WAY OF DOING BUSINESS
24 hour report… reactive Watch list…. proactive

8/19/2019
33
•You cannot become what you need to be by remaining what you are.
--Zig Ziglar
E L E M E N T # 5S Y S T E M A T I C A N A L Y S I S &
S Y S T E M I C A C T I O N
Identify Your Organization’s Guiding Principles
§483.75(b)(1) Address all systems of care and
management practices;
8/19/2019
34
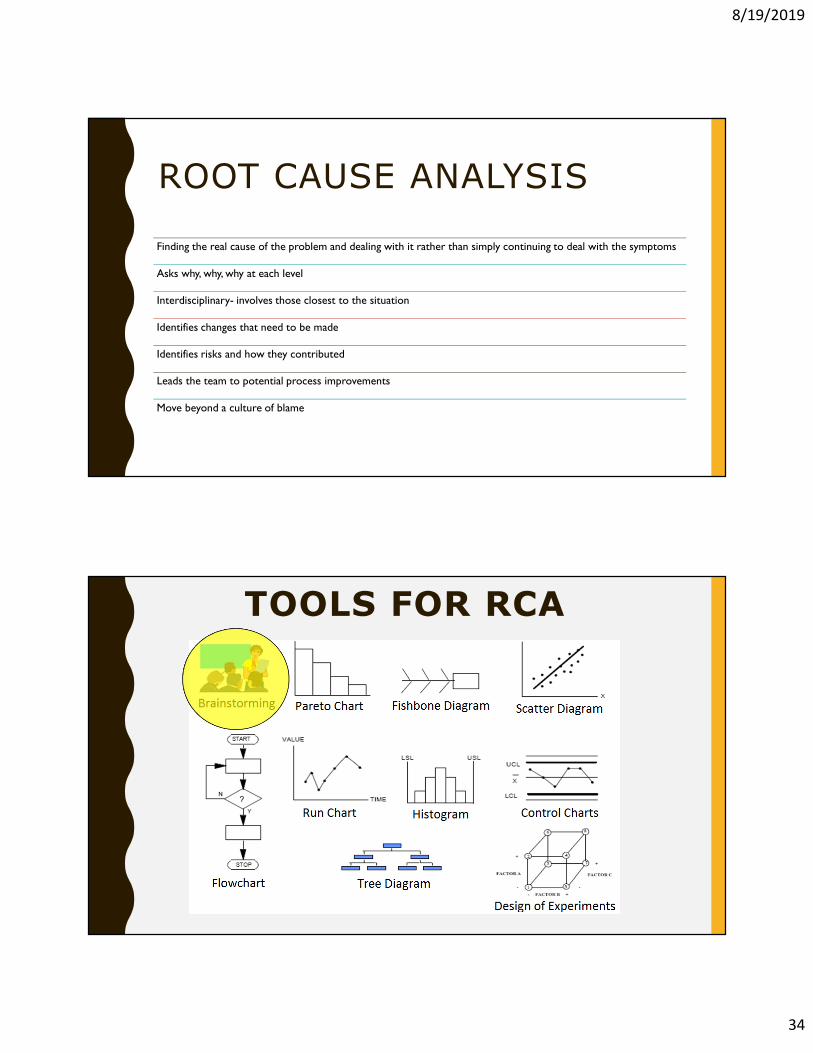
ROOT CAUSE ANALYSIS
Finding the real cause of the problem and dealing with it rather than simply continuing to deal with the symptoms
Asks why, why, why at each level
Interdisciplinary- involves those closest to the situation
Identifies changes that need to be made
Identifies risks and how they contributed
Leads the team to potential process improvements
Move beyond a culture of blame
TOOLS FOR RCA
8/19/2019
35
Resident fell last night
Resident pushed called light
Resident always just gets up
even though not steady
Therapist told resident to be
more independent
It was dark and tripped
going to bathroom
No staff member helped
1. Dark bathroom
2. Staffing
3. Toileting
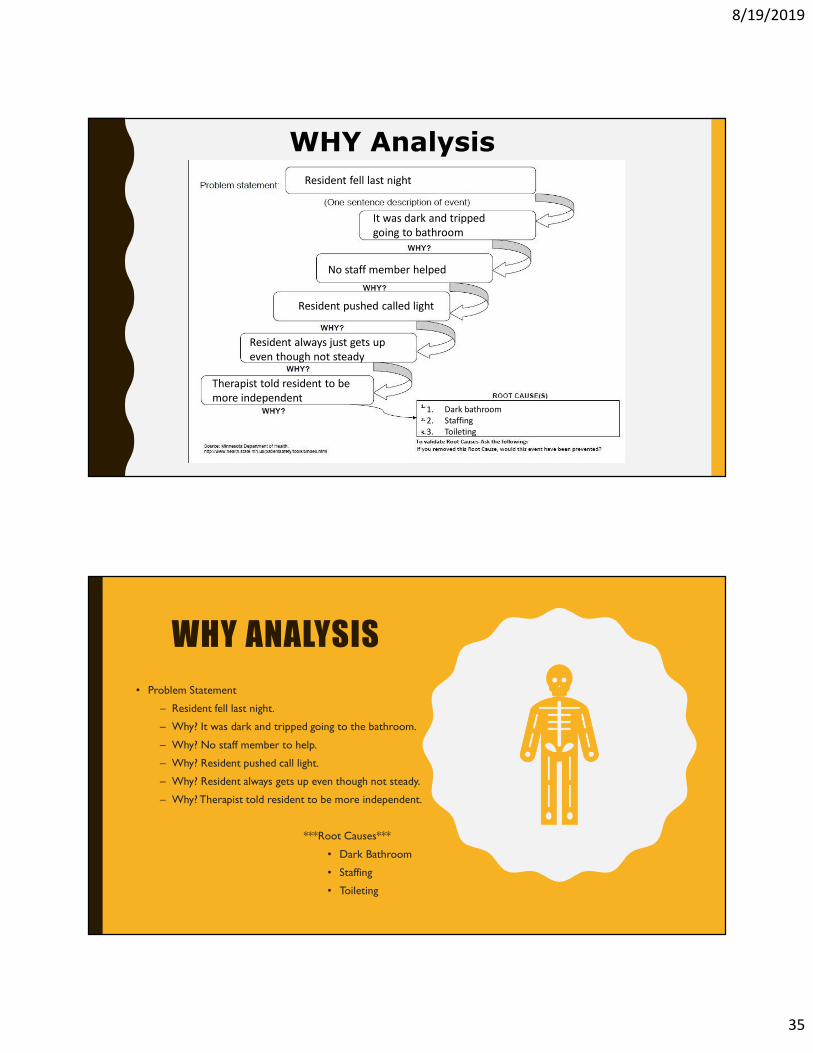
WHY Analysis
WHY ANALYSIS
• Problem Statement
– Resident fell last night.
– Why? It was dark and tripped going to the bathroom.
– Why? No staff member to help.
– Why? Resident pushed call light.
– Why? Resident always gets up even though not steady.
– Why? Therapist told resident to be more independent.
***Root Causes***
• Dark Bathroom
• Staffing
• Toileting
8/19/2019
36
“In God we trust. All
others bring data” W.E Deming
NOW WHAT? PDSA WILLIAM DEMING -
PLAN, DO, STUDY AND ACT
1. Planning is the identifying of hazards and risk - Develop a
Plan
2. Do is the implementing of interventions to reduce risks
and hazards - Activate your Plan (just Do it)
3. Study is the monitoring of effectiveness - Auditing,
rounding and accountability - Study your findings (re-
evaluate)
4. Act is the effectiveness and modifying as necessary
Choose measures that will tell you if a change worked -
Set realistic performance thresholds
5. If something didn’t work—Re-design (Act)

8/19/2019
37
STRUCTURAL MEASURES
• A measure that evaluates whether needed structure is in place and working well.
Examples
– –All mattresses replaced
– –New workstations installed
– –All audible alarms removed
OUTCOME MEASURES EXAMPLES
• The number of falls that occurred during a
lift transfer.
• The number of patients identified as high
risk that developed a facility acquired
pressure ulcer.
• Number of incidents when a patient
received the wrong medication.
• The number of patients that had a fall --
risk assessment tool completed in the
expected timeframe.
• The number of patients with a Braden
score of 12 or lower that received a
wound care nurse consult.

8/19/2019
38
OUTCOME MEASURES
A measure which evaluates the result of an intervention
–For example, the impact on the condition or well-being of patients
Assesses whether the change you have put in place had the desired effect.
REMEMBER…
Quality improvement measurement is for learning, not research
Watch for measurement fatigue
All measures have limitations
Don’t measure everything!
Try to add to existing measurement (build on what you have)
FEEDBACK
Give Feedback and give lots of it!
•Everyone who is involved in the measure
•Everyone who cares about the results
•To upper-level management,
•To board members. If it’s important to a department---
Share with staff-- If it’s important to patients & families—
Share
BE TRANSPARENT - when you can.
8/19/2019
39
CMS TOOLS :
“Not all change is
improvement, but
all improvement is
change.” (Donald
Berwick, MD
Former CMS
Administrator)

8/19/2019
40
QAPI RESOURCES
• CMS QAPI Homepage-Wide range of resources available
https://www.cms.gov/Medicare/Provider-Enrollment-and-
Certification/QAPI/qapiresources.html
• QAPI At a Glance https://www.cms.gov/Medicare/Provider-Enrollment-and-
Certification/QAPI/Downloads/QAPIAtaGlance.pdf
• QAPI Written Plan How-To Guide https://www.cms.gov/Medicare/Provider-
Enrollment-and-Certification/QAPI/Downloads/QAPI-Plan-How-to-Guide.pdf
• Institute for Healthcare Improvement-PDSA
http://www.ihi.org/resources/Pages/HowtoImprove/default.aspx
• Quality Innovation Network-QIOs (QIN-QIOs) https://qioprogram.org/
• Nursing Home Help (QIPMO/Leadership Coaching)
https://nursinghomehelp.org/
79
8/19/2019
41
www.nursinghomehelp.org(573) 882-0241
Long Term Care Leadership [email protected]
(660) 651-3778