prostate cancer diagnosis -...
TRANSCRIPT
Umeå University Medical Dissertations, New Series No 1406
Prostate Cancer Diagnosis Experimental and Clinical Studies With HRMAS NMR Spectroscopy
Katarina Stenman
Department of Radiation Sciences,
Diagnostic Radiology
Umeå 2011

Responsible publisher under Swedish law: the Dean of the Medical Faculty
This work is protected by the Swedish Copyright Legislation (Act 1960:729)
ISBN: 978-91-7459-154-5
ISSN: 0346-6612 1406
Omslagsbild: Katarina Stenman
Elektronisk version tillgänglig på http://umu.diva-portal.org/
Tryck/Printed by: VMC, KBC, Umeå University
Umeå, Sweden 2011
Dedicated to all men …
... and the women who care about them.

5
Table of Contents
Table of Contents 5 Abstract 7 Objective 9 Outline 10
Part I 10 Part II 10 Part III 10
Original Papers and My Contributions 11 Acknowledgements 12 Abbreviations 13 Part I 15 Chapter 1: Introduction 17 Chapter 2: The Prostate 20
2.1 What is a Prostate? Anatomy and Function 20 2.2 The Remarkable Metabolism of the Prostate 22 2.3 Man vs. Rat Prostate 26
Chapter 3: Diagnostic Methods of the Prostate 28 3.1 General Diagnostic Procedures 28 3.1.1 Digital Rectal Examination – DRE 28 3.1.2 Prostate Specific Antigen – PSA 28 3.1.3 Trans Rectal Ultra Sonography – TRUS 29 3.2 Imaging of the Prostate 29 3.2.1 Computerized Tomography - CT 30 3.2.2 Positron Emission Tomography - PET 30 3.2.3 Magnetic Resonance Imaging - MRI 31 3.2.4 Magnetic Resonance Spectroscopic Imaging – MRSI 31 3.2.5 Small Animal MRI/MRSI 32 3.3 Prostate Biopsy 33 3.4 Histopathological Interpretation of Tissue Specimens 33 3.4.1 The Gleason Score – GS 34 3.4.2 The TNM Table 35 3.4.3 Immunohistochemistry 35
Part II 37 Chapter 4: Nuclear Magnetic Resonance - NMR 39
4.1 General Introduction 39 4.2 The NMR Signal 39 4.3 The NMR Experiment 41 4.4 Chemical Shift 42 4.5 Spin-Spin Coupling 44
6
4.6 High-resolution Magic Angle Spinning (HRMAS) NMR 45 4.7 2-Dimensional NMR 46 4.7.1 TOtal Correlation SpectroscopY - TOCSY 46 4.7.2 Hetero-nuclear Single Quantum Coherence –HSQC 47
Chapter 5: Metabolomics Using HRMAS NMR 48 5.1 Concept of Metabolomics 48 5.2 Metabolomics in the Characterization of the Prostate 49 5.3 Metabolomics, Nutrition and Prostate Cancer 50
Part III 51 Chapter 6: Materials and Methods 53
6.1 Experimental Setup 53 6.1.1 Procedure of HRMAS NMR Spectroscopy 53 6.1.2 1D 1H HRMAS NMR 53 6.2 Prostate Tissue Samples 54 6.2.1 Patients 54 6.2.2 Rat 55 6.3 Interpretation of Data 55 6.3.1 Pathologic Analysis 56 6.3.2 Statistical Analysis 56
Chapter 7: Results and Comments 58 Paper I 58 Paper II 59 Paper III 61
Chapter 8: Discussion 64 Chapter 9: Suggestions for the Future 67 Chapter 10: References 68

7
Abstract
A few abnormal cells found in a small piece of prostate tissue are most consequential for a man’s future.
The prevalence of prostate cancer (PCa) is increasing globally. The main
instigating factor for this cancer is not yet known, but it appears to be the
consequence of many variables such as an increasingly older population, more
frequent PSA-testing, and factors involving lifestyle.
Prostate cancer screening, as an equivalent for breast cancer screening, has been
suggested but unfortunately there are no accurate diagnostic tools available for
this type of screening. The reason for this is simply that the prostate is one of the
most difficult organs to diagnose and, consequently, PCa screening would
generate far too many false-positive and false-negative results. The prostate is
not easily accessible as it is deeply-seated in the male pelvic area, wrapped
around the urethra and surrounded by sensitive vital organs. Furthermore, PCa
is frequently multi-focal, and the cancer cells have a tendency of assimilating
among normal cells and, thus, do not always form solid lumps. Therefore,
prostate tumors are often not felt by digital rectal examination (DRE) or
identified by imaging. The PSA-test is not reliable as it is more prostate-specific
than cancer-specific. Due to increasing prostate awareness, more early-stage
and locally confined PCas are being detected. This is saving lives, although there
is a high risk of over treatment and unnecessary side-effects. The increased
detection of PCa requires sophisticated diagnostic methods and highly skilled
clinicians who can discern between indolent and aggressive cancers. The current
“gold-standard” for PCa diagnosis is biopsy grading by pathologists using the
Gleason score system, which is a difficult task. Therefore, innovative methods to
improve the precision of prostate diagnosis, by increased biopsy sensitivity and
tumor localization, are of essence.
In light of these difficulties, the metabolomic approach using 1D and 2D high-
resolution magic angle spinning (HRMAS) NMR spectroscopy combined with
histopathology on intact prostatectomy specimens was evaluated in this research
project. The non-destructive nature of HRMAS NMR enables spectroscopic
analysis of intact tissue samples with consecutive histological examinations
under light microscope. Metabolomics aids in the unraveling and the discovery
of organ-specific endogenous metabolites that have the potential to be reliable
indicators of organ function and viability, extrinsic and intrinsic perturbations,
as well as valuable markers for treatment response. The results may, therefore,
be applied clinically to characterize an organ by utilizing bio-markers that have
the capacity to distinguish between disease and health.

8
The aim was to characterize the human and the rat prostate in terms of its
intermediary metabolism, which is shown here to differ between species and
anatomical regions. Furthermore, the aim is to seek the verification of HRMAS
NMR derived metabolites which are known to be a part of the prostate
metabolome such as, citrate, choline, and the polyamines which were performed,
but also the identification of metabolites not previously identified as part of the
local prostate metabolism, such as Omega-6, which was detected in tumors. The
extended aim was to elucidate novel bio-markers with clinical potential. In this
study, the common phyto-nutrient, inositol, which appears to possess protective
properties, was identified as being a potentially important PCa bio-marker for
the distinction between the more indolent Gleason score 6 and the more
aggressive Gleason score 7 in non-malignant prostate tissues with tumors
elsewhere in the organ. Further studies in this area of PCa research are therefore
warranted.

9
Objective
The main objective of this thesis was to investigate and evaluate the application
of HRMAS NMR on intact prostate tissues. During the course of the study, it
became clear that nothing about the prostate is easy, supporting the validity of
the statement below:
“Despite the major progress that has occurred in the biological sciences during the last 50
years, it is rather remarkable that we are about to enter the twenty-first century, and still
the specific function of the prostate gland is unknown. Indeed the prostate is the largest
organ of unknown specific function in the human body.”
Dr. John Isaacs John Hopkins School of Medicine
Therefore, as a result, the initial aims and goals have been revised several times
and finally resulted in a more comprehensive overview of the complexity of the
prostate and a presentation of HRMAS NMR spectroscopy, used in conjunction
with histopathology, as a powerful tool to gain a deeper understanding of the
intracellular local metabolism of the prostate. This method has proved to be
useful in providing valuable pieces to the, far-from-finished, puzzle of the
prostate and its diseases.
10
Outline
This thesis consists of three parts and a total of 10 chapters. The aim is to guide
the reader through the complexities that involves the prostate gland in general,
throughout the theory behind NMR spectroscopy and its utility and, finally,
towards the results and its interpretation and suggestions for future studies.
Part I
Chapter 1 presents a brief, but comprehensive, introduction about the research
topic in general; prostate cancer.
Chapter 2 provides information about the prostate such as anatomy, function,
and metabolism. It also includes an overview on the subject of experimental
rodent prostate cancer models.
Chapter 3 reviews the different diagnostic options available for prostate
diagnosis.
Part II
Chapter 4 and 5 presents the method used to generate the results in this thesis,
namely NMR, with a strong emphasis on HRMAS NMR and metabolomics.
Part III
Chapters 6-10 comprise the design of experiments, methods, results, and
discussions followed by research papers.
11
Original Papers and My Contributions
The following peer-reviewed papers are included in this doctoral dissertation
and referred to by their Roman numerals.
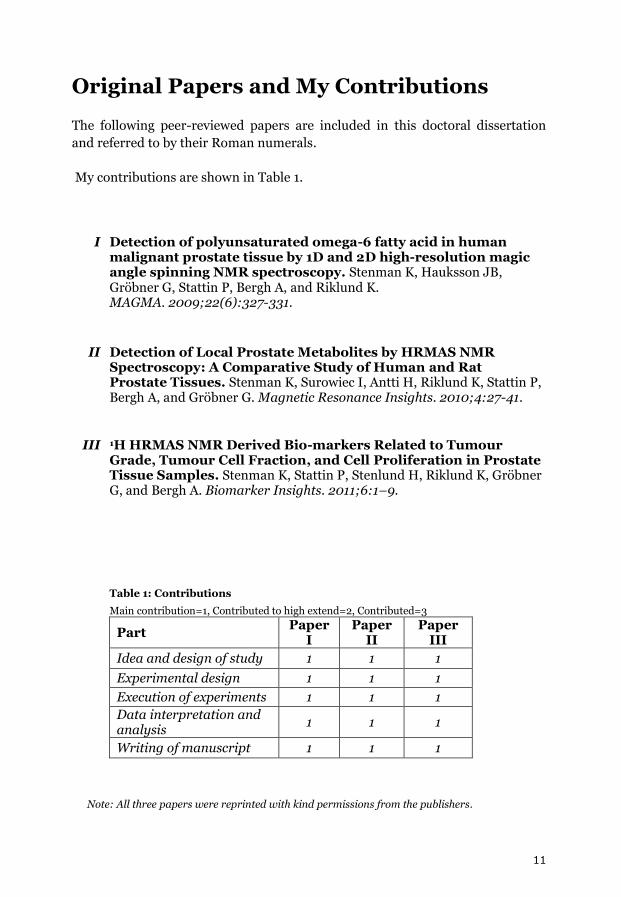
My contributions are shown in Table 1.
I Detection of polyunsaturated omega-6 fatty acid in human
malignant prostate tissue by 1D and 2D high-resolution magic angle spinning NMR spectroscopy. Stenman K, Hauksson JB, Gröbner G, Stattin P, Bergh A, and Riklund K. MAGMA. 2009;22(6):327-331.
II Detection of Local Prostate Metabolites by HRMAS NMR Spectroscopy: A Comparative Study of Human and Rat Prostate Tissues. Stenman K, Surowiec I, Antti H, Riklund K, Stattin P, Bergh A, and Gröbner G. Magnetic Resonance Insights. 2010;4:27-41.
III 1H HRMAS NMR Derived Bio-markers Related to Tumour Grade, Tumour Cell Fraction, and Cell Proliferation in Prostate Tissue Samples. Stenman K, Stattin P, Stenlund H, Riklund K, Gröbner G, and Bergh A. Biomarker Insights. 2011;6:1–9.
Table 1: Contributions
Main contribution=1, Contributed to high extend=2, Contributed=3
Part Paper
I Paper
II Paper
III
Idea and design of study 1 1 1
Experimental design 1 1 1
Execution of experiments 1 1 1
Data interpretation and analysis
1 1 1
Writing of manuscript 1 1 1
Note: All three papers were reprinted with kind permissions from the publishers.

12
Acknowledgements
“Haba na haba, hujaza kibaba”*
Swahili kanga writing
This study has been collaboration with Professor Anders Bergh, Pathology, the
Department of Medical Biosciences, Umeå University Hospital; Professor
Gerhard Gröbner, Physical Chemistry, the Department of Chemistry, Umeå
University; and Professor Katrine Åhlström Riklund, Diagnostic Radiology, the
Department of Radiation Sciences, Umeå University Hospital. This work has
been funded at large by the Lion’s Cancer Research Foundation and also by
generous grants from the Swedish Cancer Foundation, the JC Kempe Memorial
Foundation Academic Funds, and the Wallenberg Foundation. Thanks are due
to many people and as a precaution not to unintentionally exclude anyone, only
the people in close collaboration are therefore mentioned: Dr. Jón Haukson,
Professor Mikael Karlsson, Anna Wernblom, Christina Ericsson, Linda Kocsis,
Dept. of Radiation Sciences; Professor Pär Stattin, Dept. of Surgical and
Perioperative Sciences; Dr. Hans Stenlund, Dept. of Public Health and Clinical
Medicine; Professor Dan Johnels, Ingmar Sethson, Professor Jurgen
Schleucher, Dr. Izabella Surowiec, Dr. Henrik Antti, Dept. of Chemistry;
Birgitta Ekblom, Elisabeth Dahlberg, Pernilla Andersson, Dept. of Medical
Biosciences; Kerstin Almroth and Britt-Inger Dahlin, Dept. of Surgical and
Perioperative Sciences. Lisbeth, Erica, Eivor, Anna, Ann-Kristin, Margaret, and
Ronald, – thank you very much!! Again, special thanks to: Anders Bergh who
performed all of the, very difficult and time consuming, histopathological
evaluations of the prostate tissues, prior and subsequent HRMAS NMR analysis,
and also contributed significantly in the writing of manuscripts; Gerhard
Gröbner, who joined the group in a late stage and with his ambitious and
efficient ways proved to be the “missing piece” for the completion of this
dissertation; and my supervisor, Katrine Riklund, who administered this project.
Last but definitely not least, thanks to the patients who generously donated their
prostates for this study and thereby contributed to the highest degree to this
research and this dissertation. We wish all of you the best of health!
*“Small things, when combined together make up big things”.
As this Swahili proverb says, all things are possible if you just take it little by little, step by step.
13
Abbreviations
AA Arachidonic Acid
Acetyl-CoA Acetyl-Coenzyme A
ATP Adenosine Triphosphate
AUC Area Under the ROC Curve
BPH Benign Prostatic Hyperplasia
COX Cyclooxygenase
CPMG Carr-Purcell-Meibom-Gill
CT Computerized Tomography
D2O Deuterium Oxide
DLP Dorso-Lateral Prostate
DRE Digital Rectal Examination
EFA Essential Fatty Acid
EPA Eicosapentaenoic Acid
EtOH Ethanol/Ethyl alcohol
FID Free Induction Decay
GC-MS Gas Chromatography-Mass Spectrometry
GS Gleason Scores
HRMAS High Resolution Magic Angle Spinning
HSQC Hetero-nuclear Single Quantum Coherence
Hz Hertz
MRSI Magnetic Resonance Spectroscopic Imaging
MS Mass Spectrometry
NMR Nuclear Magnetic Resonance
NSAID Non-Steroidal Anti-Inflammatory Drug
OR Odds Ratios
PCa Prostate Cancer
PG Prostaglandin
PPM Parts Per Million
PSA Prostate Specific Antigen
PUFA Polyunsaturated Fatty Acid
RF Radio Frequent
ROC Receiver Operating Characteristic
TNM Tumor, Nodes (lymph), and Metastasis
TOCSY Total Correlation Spectroscopy
TRUS Trans Rectal Ultra Sonography
VP Ventral Prostate

14
15
Part I

16
17
Chapter 1: Introduction
Globally, prostate cancer (PCa) is rapidly becoming the most common form of
male specific cancer [Thun et al., 2010]. Consequently, a large international
research community is actively engaged in trying to learn more about this deep-
seated gland in the reproductive tract of the male body. The prostate, with its
heterogeneity and anomalous metabolism, [Costello et al., 1997, 1999, 2000] is
one of the most difficult human organs to diagnose. The PCa pathology poses a
great challenge for clinicians and scientists [Fleshner et al., 2002; Swindle et al.,
2008] and in order to understand this disorder, it is of absolute necessity to
build up a thorough comprehension of this organ and learn to interpret its
biochemical signals. The majority of PCa are slow-growing cancers and, in fact,
more men die from this disease than not. The main goal in the fight against PCa
is to find a reliable method that can differentiate between the indolent and the
aggressive types [Madu et al., 2010]. There are ongoing discussions about
diverse theories relevant to the cause and instigation of PCa. Although not
exclusively, PCa and other ailments of the prostate are by far more common in
older men [Sharma et al., 2010]. In addition to age, factors, such as, genetic
susceptibility, diet and lifestyle, infectious agents, inflammation, etc. are all
possible instigators for the development of PCa [Coffey et al., 2001; Gonzales et
al., 2010; American Cancer Society, 2010]. The incidence of PCa and other
diseases related to the prostate are expected to increase due to an ever increasing
aging male population [Thun et al., 2010].
One of the main obstacles involved in the diagnosis of the prostate is its
inaccessibility in the body. Furthermore, the prostate, especially a malignant
one, is a heterogeneous structure with different cell types and pathologies, and
cancer cells often infiltrate among normal cells [Zakian et al., 2005]. Contrary to
other solid tumors, prostate tumors do not normally develop into solid lumps.
Therefore, they are not always detectable by digital rectal examination (DRE),
which, jointly with the Prostate-Specific Antigen (PSA) test, is part of the clinical
routine examination when suspecting PCa [Kelloff et al., 2009]. Indirect
diagnosis of PCa is achieved through a simple blood test, using the PSA-test.
However, PSA is not cancer particular, but more so prostate specific even though
PSA is also expressed in other tissues and in women, and thus not a reliable
indicator. The value of PCa screening using the PSA-test is not determined given
that it generates frequent false-positive results, which involves the increased risk
of unnecessary biopsies and treatments [Wolf el al, 2010; Vickers et al., 2011].
PCa is multifocal and the cancer foci can be small, i.e., only millimeters in size,
thus making DRE and biopsy sampling a challenge for the clinician.
Furthermore, there is currently no imaging method available that can be used
with high accuracy to guide biopsies towards the tumors and particularly
18
towards the most aggressive ones. Multiple biopsies are therefore taken from
different parts of the prostate and as biopsies are small, many tumors are often
missed [Andriole, 2009]. Biopsy sampling is generally performed in conjunction
with Trans Rectal Ultra Sonography (TRUS) which provides an image of the
internal organs, i.e. the prostate, and thus aids in guiding of the sampling
towards the prostate although many tumors are often not seen. Requiring a
skilled pathologist, biopsy specimens are examined and rated through the
Gleason grading system; this diagnosis will be the basis for the treatment plan
[Berney et al., 2007]. A high Gleason score indicates a poor prognosis; most men
are detected with low or intermediate grade tumors and for them prognosis is
highly variable and unpredictable. The diagnosis and prognostication of PCa are
therefore complicated but research and technological advancements of clinical
diagnostic methods and instruments are hopefully changing the situation for the
better [Kelloff et al., 2009].
The prostate is often enlarged due to Benign Prostatic Hyperplasia (BPH) in men
past the age of 50, sometimes even younger [Kirby, 2000]. BPH and its
consequences such as inflammations [De Marzo et al., 2007], does not make PCa
diagnosis easier. In fact, it is difficult to know what a completely healthy prostate
looks like in a middle-aged man [McLaughlin et al., 2005] and as the senescence
factor is a major part of PCa [Sharma et al., 2010] it is, consequently, virtually
impossible to find completely healthy, older human controls for prostate cancer
research studies. A wide variety of experimental rodent PCa models are available
for pre-clinical studies. Many of these models are successfully utilized since it is
often not possible to use human subjects due to obvious ethical, practical and
economic reasons. However, the anatomy and the metabolisms of rodents differ
from that of man. This is a major drawback [Lamb et al., 2005; Kamb, 2005].
There is currently no standardized method that can accurately diagnose, stage
and predict the outcome for PCa that affects such a large proportion of the male
population [Kelloff et al., 2009; Wolf et al., 2010]. Histological evaluation of
prostate biopsies by skilled pathologists is presently the gold standard, used in
conjunction with the PSA-test [Rajinikanth et al., 2008; Chun et al., 2010].
Novel diagnostic methods that can detect and accurately stage non-palpable and
aggressive tumors at an early stage are urgently needed [Kelloff et al., 2009]. In-
vivo Magnetic Resonance Spectroscopic Imaging (MRSI) [Giusti et al., 2010;
Klijn et al., 2011; Scheenen et al., 2011], especially when used in conjunction
with ex-vivo High Resolution Magic Angle Spinning Nuclear Magnetic
Resonance (HRMAS NMR) spectroscopy, has shown to be a promising
alternative for the future [Kurhanewicz et al., 2002; Swanson et al., 2003;
Santos et al., 2010]. Spectroscopy generates a fingerprint of the metabolism
including a visualization of its perturbations due to disease, i.e., loss of
homeostasis, which often occurs before morphological changes [van der Greef et
19
al., 2005; Bathen et al., 2010]. HRMAS NMR spectroscopy is a non-destructive
method that allows the analyzed specimen to be examined under light
microscopy post NMR [Beckonert et al., 2010; Moestue et al., 2011]. This feature
makes it possible to correlate the spectrum with the specific pathology that can
be verified with advanced immunohistochemistry.
All of the factors involved in PCa and discussed above affect the metabolism one
way or another. Therefore, the focus of this study was to learn more about the
local metabolism of the prostate, malignant as well as non-malignant/healthy in
both man and rat. HRMAS NMR spectroscopy with subsequent
histopathological analysis was used to obtain a correlated spectroscopic and
morphologic “fingerprint” of the metabolism.
20
Chapter 2: The Prostate
2.1 What is a Prostate? Anatomy and Function
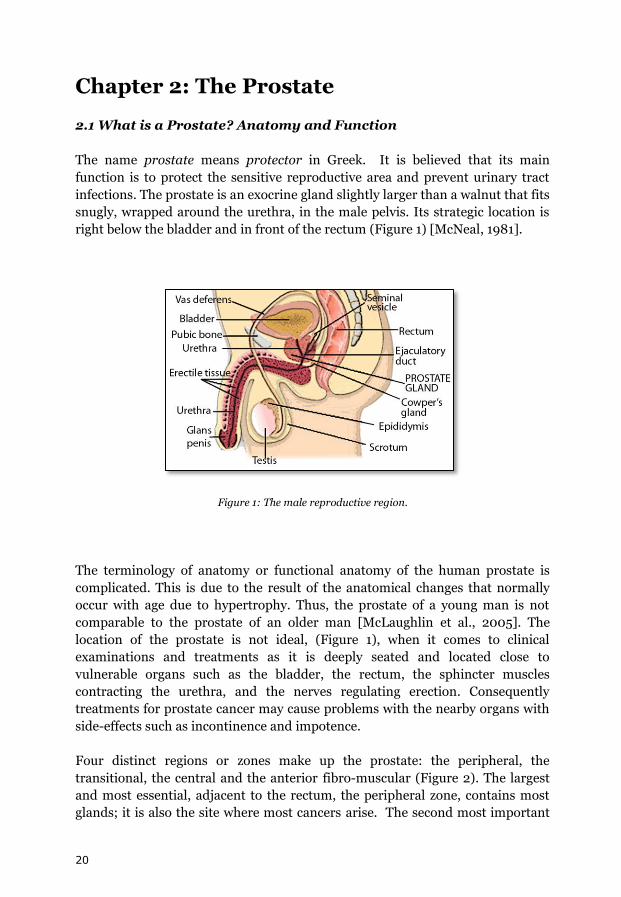
The name prostate means protector in Greek. It is believed that its main
function is to protect the sensitive reproductive area and prevent urinary tract
infections. The prostate is an exocrine gland slightly larger than a walnut that fits
snugly, wrapped around the urethra, in the male pelvis. Its strategic location is
right below the bladder and in front of the rectum (Figure 1) [McNeal, 1981].
Figure 1: The male reproductive region.
The terminology of anatomy or functional anatomy of the human prostate is
complicated. This is due to the result of the anatomical changes that normally
occur with age due to hypertrophy. Thus, the prostate of a young man is not
comparable to the prostate of an older man [McLaughlin et al., 2005]. The
location of the prostate is not ideal, (Figure 1), when it comes to clinical
examinations and treatments as it is deeply seated and located close to
vulnerable organs such as the bladder, the rectum, the sphincter muscles
contracting the urethra, and the nerves regulating erection. Consequently
treatments for prostate cancer may cause problems with the nearby organs with
side-effects such as incontinence and impotence.
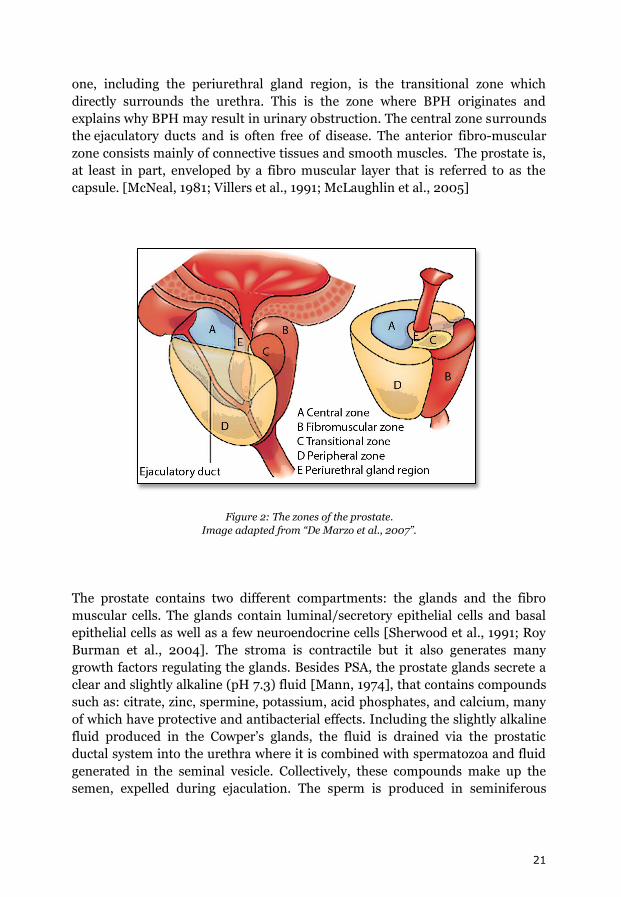
Four distinct regions or zones make up the prostate: the peripheral, the
transitional, the central and the anterior fibro-muscular (Figure 2). The largest
and most essential, adjacent to the rectum, the peripheral zone, contains most
glands; it is also the site where most cancers arise. The second most important
21
one, including the periurethral gland region, is the transitional zone which
directly surrounds the urethra. This is the zone where BPH originates and
explains why BPH may result in urinary obstruction. The central zone surrounds
the ejaculatory ducts and is often free of disease. The anterior fibro-muscular
zone consists mainly of connective tissues and smooth muscles. The prostate is,
at least in part, enveloped by a fibro muscular layer that is referred to as the
capsule. [McNeal, 1981; Villers et al., 1991; McLaughlin et al., 2005]
Figure 2: The zones of the prostate.
Image adapted from “De Marzo et al., 2007”.
The prostate contains two different compartments: the glands and the fibro
muscular cells. The glands contain luminal/secretory epithelial cells and basal
epithelial cells as well as a few neuroendocrine cells [Sherwood et al., 1991; Roy
Burman et al., 2004]. The stroma is contractile but it also generates many
growth factors regulating the glands. Besides PSA, the prostate glands secrete a
clear and slightly alkaline (pH 7.3) fluid [Mann, 1974], that contains compounds
such as: citrate, zinc, spermine, potassium, acid phosphates, and calcium, many
of which have protective and antibacterial effects. Including the slightly alkaline
fluid produced in the Cowper’s glands, the fluid is drained via the prostatic
ductal system into the urethra where it is combined with spermatozoa and fluid
generated in the seminal vesicle. Collectively, these compounds make up the
semen, expelled during ejaculation. The sperm is produced in seminiferous
22
tubules that are located in each testis and connected to the epididymal duce
which in turn is connected to the vas deferens (Figure 1).
2.2 The Remarkable Metabolism of the Prostate
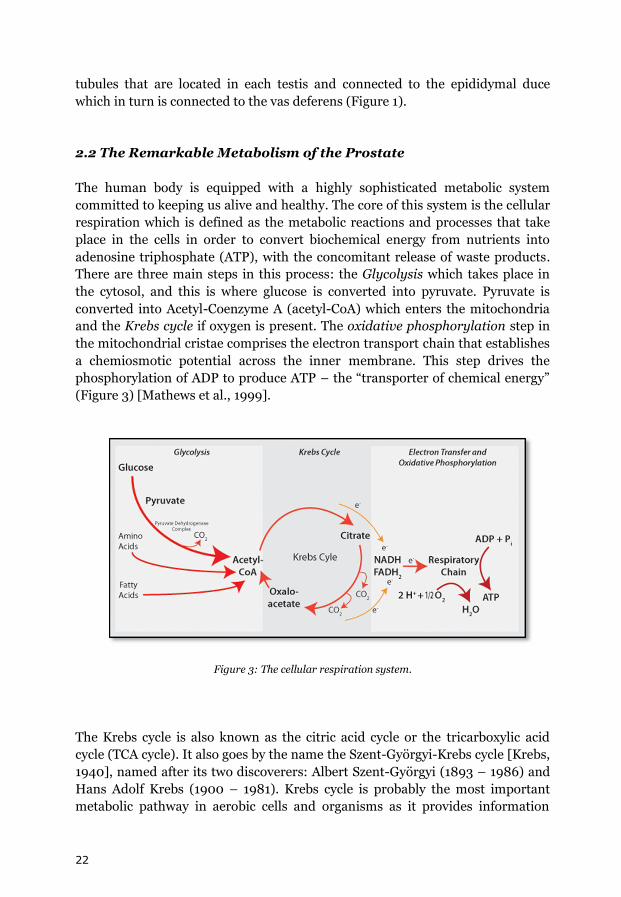
The human body is equipped with a highly sophisticated metabolic system
committed to keeping us alive and healthy. The core of this system is the cellular
respiration which is defined as the metabolic reactions and processes that take
place in the cells in order to convert biochemical energy from nutrients into
adenosine triphosphate (ATP), with the concomitant release of waste products.
There are three main steps in this process: the Glycolysis which takes place in
the cytosol, and this is where glucose is converted into pyruvate. Pyruvate is
converted into Acetyl-Coenzyme A (acetyl-CoA) which enters the mitochondria
and the Krebs cycle if oxygen is present. The oxidative phosphorylation step in
the mitochondrial cristae comprises the electron transport chain that establishes
a chemiosmotic potential across the inner membrane. This step drives the
phosphorylation of ADP to produce ATP – the “transporter of chemical energy”
(Figure 3) [Mathews et al., 1999].
Figure 3: The cellular respiration system.
The Krebs cycle is also known as the citric acid cycle or the tricarboxylic acid
cycle (TCA cycle). It also goes by the name the Szent-Györgyi-Krebs cycle [Krebs,
1940], named after its two discoverers: Albert Szent-Györgyi (1893 – 1986) and
Hans Adolf Krebs (1900 – 1981). Krebs cycle is probably the most important
metabolic pathway in aerobic cells and organisms as it provides information
23
about the chemical intracellular conversions of carbohydrates, fats and proteins
into carbon dioxide and water to generate energy. This dynamic and amphibolic
process involves a series of enzyme catalyzed chemical reactions that occurs in
the mitochondria of the cell. The citric acid cycle begins with the high energy
compound acetyl-CoA which condenses with oxaloacetate, and catalyzed by
citric acid synthetase, to generate citrate. Citrate is oxidized further in this cycle
through a series of isomerisation-, oxidation-, and decarboxylation-steps that
finally regenerate oxaloacetate in the final step in the Krebs cycle before the cycle
is repeated (Figure 3).
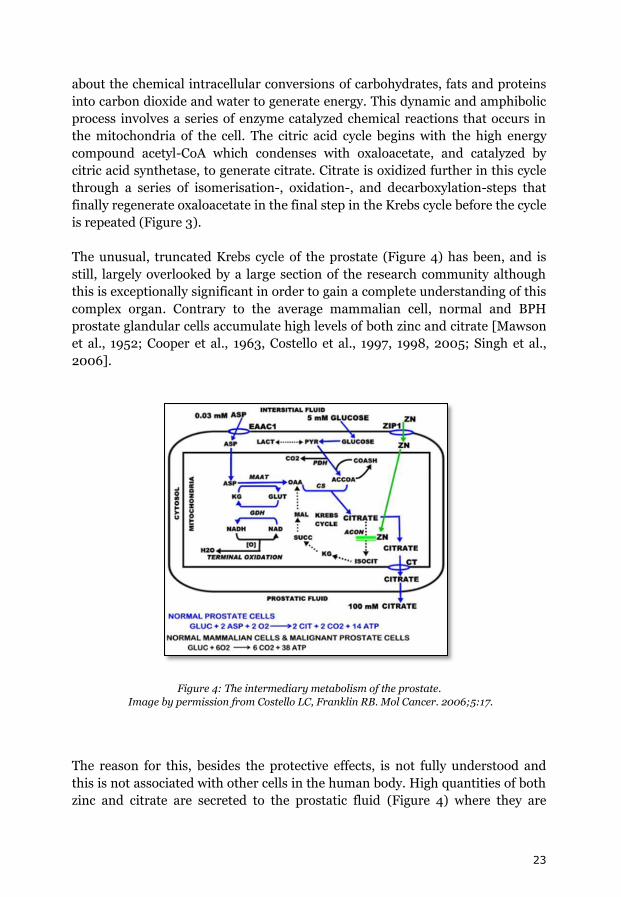
The unusual, truncated Krebs cycle of the prostate (Figure 4) has been, and is
still, largely overlooked by a large section of the research community although
this is exceptionally significant in order to gain a complete understanding of this
complex organ. Contrary to the average mammalian cell, normal and BPH
prostate glandular cells accumulate high levels of both zinc and citrate [Mawson
et al., 1952; Cooper et al., 1963, Costello et al., 1997, 1998, 2005; Singh et al.,
2006].
Figure 4: The intermediary metabolism of the prostate.
Image by permission from Costello LC, Franklin RB. Mol Cancer. 2006;5:17.
The reason for this, besides the protective effects, is not fully understood and
this is not associated with other cells in the human body. High quantities of both
zinc and citrate are secreted to the prostatic fluid (Figure 4) where they are
24
believed to function as antibacterial agents while the fluid is entering and
flushing the many ductal systems in the gland [Fair et al., 1976, 1981; Kavanagh,
1985,]. One of the functions of mitochondrial zinc is to inhibit mitochondrial
aconitase (m-aconitase) which in turn prevents the oxidation of citrate in the
Krebs cycle (Figure 4). Conversely, malignant epithelial cells are metabolically
transformed to citrate-oxidizing, energy producing cells that lose the ability to
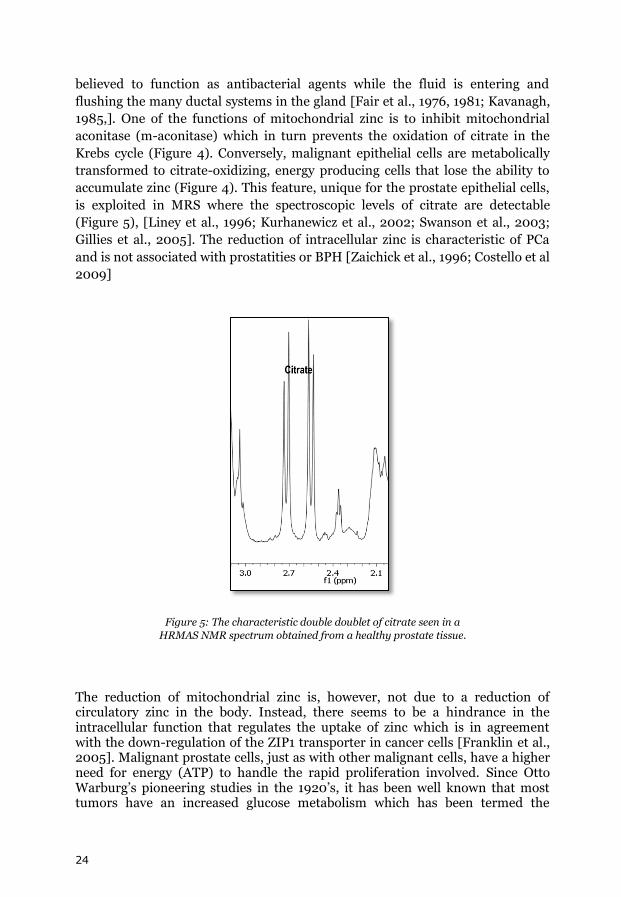
accumulate zinc (Figure 4). This feature, unique for the prostate epithelial cells,
is exploited in MRS where the spectroscopic levels of citrate are detectable
(Figure 5), [Liney et al., 1996; Kurhanewicz et al., 2002; Swanson et al., 2003;
Gillies et al., 2005]. The reduction of intracellular zinc is characteristic of PCa
and is not associated with prostatities or BPH [Zaichick et al., 1996; Costello et al
2009]
Figure 5: The characteristic double doublet of citrate seen in a
HRMAS NMR spectrum obtained from a healthy prostate tissue.
The reduction of mitochondrial zinc is, however, not due to a reduction of circulatory zinc in the body. Instead, there seems to be a hindrance in the intracellular function that regulates the uptake of zinc which is in agreement with the down-regulation of the ZIP1 transporter in cancer cells [Franklin et al., 2005]. Malignant prostate cells, just as with other malignant cells, have a higher need for energy (ATP) to handle the rapid proliferation involved. Since Otto Warburg’s pioneering studies in the 1920’s, it has been well known that most tumors have an increased glucose metabolism which has been termed the
25
Warburg effect [Warburg, 1956; Kim et al., 2006; Hsu et al., 2008]. However, the healthy prostate epithelial cell has a very slow metabolism, i.e., it is an energy inefficient cell with high aerobic glycolysis and low aerobic oxidation and its overall reaction is:
Glucose + 2 Aspartate + 2 O2 2 Citrate + 2 CO2 + 14 ATP
The malignant prostate epithelial cells transforms into energy producing cells
with a fully operational Krebs cycle with complete oxidation of glucose and with
a low glycolysis:
Glucose + 6 O2 6 CO2 + 38 ATP
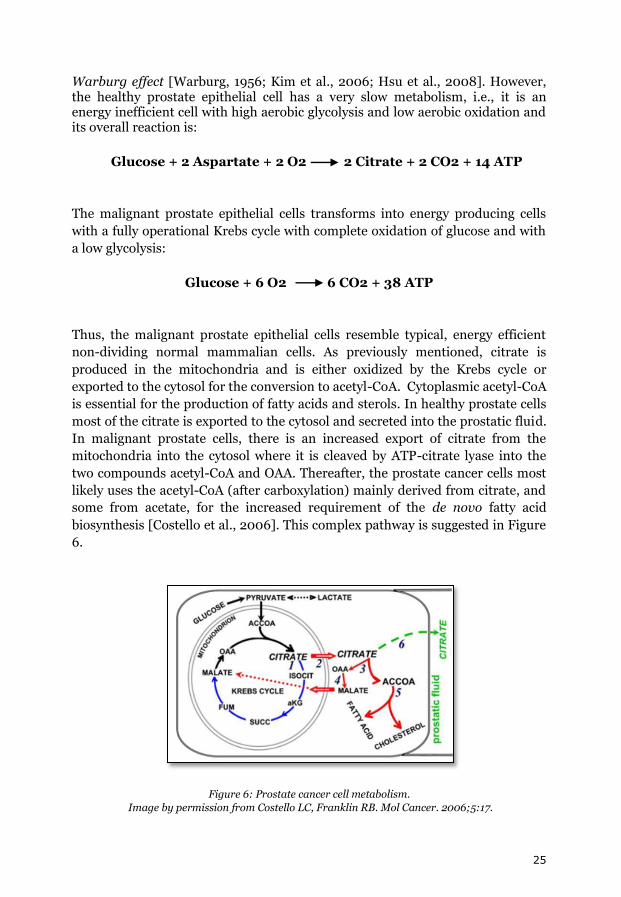
Thus, the malignant prostate epithelial cells resemble typical, energy efficient
non-dividing normal mammalian cells. As previously mentioned, citrate is
produced in the mitochondria and is either oxidized by the Krebs cycle or
exported to the cytosol for the conversion to acetyl-CoA. Cytoplasmic acetyl-CoA
is essential for the production of fatty acids and sterols. In healthy prostate cells
most of the citrate is exported to the cytosol and secreted into the prostatic fluid.
In malignant prostate cells, there is an increased export of citrate from the
mitochondria into the cytosol where it is cleaved by ATP-citrate lyase into the
two compounds acetyl-CoA and OAA. Thereafter, the prostate cancer cells most
likely uses the acetyl-CoA (after carboxylation) mainly derived from citrate, and
some from acetate, for the increased requirement of the de novo fatty acid
biosynthesis [Costello et al., 2006]. This complex pathway is suggested in Figure
6.
Figure 6: Prostate cancer cell metabolism.
Image by permission from Costello LC, Franklin RB. Mol Cancer. 2006;5:17.
26
Prostate tumors (selectively) over express fatty acid synthase (FAS) which is the
enzyme responsible for the de novo synthesis of fatty acids [Swinnen et al.,
2000; Baron et al., 2004]. However, an alternative pathway to provide OAA and
acetyl-CoA for the citrate initiated lipogenesis/cholesterogenesis pathway in PCa
is suggested; namely the glutamate pathway where the two major products are
citrate and alanine. Another option is the cytosolic direct synthesis of acetyl-Coa
[Costello et al., 2006]. As acetate takes part in the cytoplasmic lipogenesis, the
PET tracer 11C-Acetate is used and studied in PCa diagnosis; however, its role as
a tracer is not determined [Jadvar, 2011]. Choline compounds are increased in
prostate tumors and this feature is exploited by MRS [Swanson et al., 2003;
McLean et al., 2010] and 11C-Choline PET [Jadvar, 2011]. As citrate alone is not
sufficient for the discrimination between PCa and BPH its resonance is usually
combined with the choline compounds, which are increased in PCa vs. BPH, in
the (total-choline + creatine)/citrate (tCho+Cre/Cit) ratio [Gillies et al., 2005].
However, increases of choline compounds may not to be correlated with
proliferation [Gillies et al., 2005]. As a matter of fact, the increased de novo
lipogenesis in tumor cells may have a more complex role than earlier believed,
possible even as a cellular protector from endogenous and exogenous insults by
promoting membrane lipid saturation [Rysman et al., 2010].
Again, this points to the complexity of the human body and, consequently,
further studies to elucidate the prostate cancer pathways are warranted in order
to assess innovative bio-markers that can be used clinically with accurate results.
2.3 Man vs. Rat Prostate
For decades, researchers have tried to find experimental models that mimic the
human prostate and its diseases; however, the perfect model has yet to be
discovered [Kamb, 2005]. The underlying reason for these difficulties is, simply,
the fact that the prostate is a very complex organ with large species differences.
Factors such as heterogeneity, anatomical, zonal and cellular differences, and
unpredictable metabolic pathways etc. needs to be taken into considerations
when choosing an appropriate model. One important aspect that, unfortunately,
is often set aside is age [Badawai et al., 2004; Jara et al., 2004] since it is often
practically difficult to age match subjects in a research study. There is an
economic factor involved in this [Hahn, 2004], namely the cost and time it
requires to breed experimental animals to equal the age of an aging man which
is, after all, the main category that acquires problems with the prostate. Thus,
there is, unfortunately, not a universal tumor metabolism that is applicable to all
tumors, species and anatomical zones. Extrapolations of experimental PCa
results into clinical studies should therefore only be made under strict caution
[Costello et al., 2005].

27
Rodent models are widely used in PCa studies, with variable success rate. Each
model possesses strengths and weaknesses and is more appropriate for some
disorders than others [Lucia et al., 1998]. The rat prostate (which is fairly similar
to that in mice) is a large gland surrounding the urethra and is, contrary to the
human prostate, composed of distinctly different lobes, the ventral, dorsal,
lateral, and anterior lobes. The anterior lobe is also called the coagulating gland.
The ventral prostate lobe has been in the focus of several studies although it has
no equivalent in the human prostate [Roy-Burman et al., 2004], one reason is
that it is easily accessible and comprises roughly half of the entire prostatic
complex. The dorsal and the lateral lobes are often combined as the dorsolateral
lobe (DLP) as the share the same ductal system and it is also practically difficult
to separate the two. The LP is the lobe of the rat prostate that is the most similar
to the human peripheral zone. The lateral lobe actually comprises two different
ductal systems: the lateral type 1, and the lateral type 2 [Hayasi et al., 1991]. It is
interesting to note that the lateral lobe of the rat prostate demonstrates similar
cellular citrate and zinc accumulating characteristics as with the human
glandular peripheral zone. The rat ventral lobe shares the same characteristics
but not the dorsal lobe [Costello et al., 1998].
28
Chapter 3: Diagnostic Methods of the Prostate
The main clinical challenges in PCa treatment and management rely on accurate
diagnosis and initial staging. As the PSA-test has become readily available
[Wever et al., 2010] more clinically localized PCa are detected by consecutive
histopathological diagnosis and Gleason grading on biopsies. Regrettably, the
treatment for early stage disease is poorly defined [Berney et al., 2007]. Early
detection of PCa has caused a rapid increase in terms of incidence [Wever et al.,
2010]. Early detection and treatment of prostate cancer saves lives [Schröder et
al., 2009]. Unfortunately however, early detection of cancer inevitably also leads
to an increased risk of overtreatment due to the difficulties involved in
determining disease aggressiveness and the accomplishment of accurate staging
[Berney et al., 2007; Reese et al., 2011].
3.1 General Diagnostic Procedures
The general procedure for a clinical prostate examination includes: Digital
Rectal Examination (DRE) and the Prostate Specific Antigen (PSA) test. Trans
Rectal Ultra Sonography (TRUS) imaging if often used to guide biopsies [Cupp
et al., 1993]. This examination provides basic, initial information.
3.1.1 Digital Rectal Examination – DRE
This is a routine examination that allows the doctor’s finger to feel the back wall
of the prostate through the rectum. Any abnormalities detected will warrant for
additional exams and tests. The front and the middle of the prostate are not felt
during this exam. This is a subjective test and an urologist most likely has an
advantage over a general practitioner.
3.1.2 Prostate Specific Antigen – PSA
PSA is a kallekrein (an enzyme that cleaves peptide bonds in proteins), which is
produced by the prostate epithelial cells and it is a major component of the
semen, where its function is to break down coagulated semen post-ejaculation.
PSA is secreted via the prostatic ductal system and leaks into the bloodstream
where it can be detected by a simple blood test. An elevation of PSA may be a
sign of PCa since prostate cancer do not have a functioning ductal system that
drains the fluid into the urethra. The lack of free passage forces the PSA into the
29
prostate where it eventually leaks into the blood stream. However, increased
values can also be due to BPH, irritations of the prostate such as inflammation
and infection. The PSA-test is prostate specific and not cancer specific. Therefore
the optimal way to interpret a PSA-test and use it as an indicator for PCa may be
to include factors such as: age, race, free vs. bound PSA, PSA velocity (when
monitoring yearly), volume of prostate (especially the transition zone where
BPH arises), and decide individual cut-off levels based on its baseline value
[Oesterling, 1991]. However, a total PSA cutoff value of 3.0 ng/ml is often used
as an indication for biopsy although some countries prefer 2.5 ng/ml while
others prefer 4.0 ng/ml. The value of prostate cancer screening using the PSA-
test is unclear [Vickers et al., 2011], although there seems to be a reduction in
mortality albeit with a risk of overtreatment as high as 50% [Schröder et al.,
2009]. PSA expression has also been reported in other tissues and also in
females [Kraus et al., 2010]
3.1.3 Trans Rectal Ultra Sonography – TRUS
TRUS provides an ultrasound (harmless sound waves) generated image of the
prostate and surrounding tissue and allows the physician to access prostate
volume and examine the gland for abnormalities. Although this technique is able
to detect many of the palpable tumors, it is of less value for early stage
diagnostics where the tumors are non-palpable and, furthermore, some tumors
are iso-echogenic and are therefore not visualized by TRUS. TRUS is valuable to
guide biopsy sampling and to monitor treatments. Technical advancements in
this field include contrast-enhanced (microbubble contrast) agent techniques
[Aigner et al., 2010], and image fusion with TRUS and MRI [Turkbey et al.,
2011].
3.2 Imaging of the Prostate
Abnormal DRE and/or PSA-test calls for a more advanced evaluation using
image based diagnostic procedures including, anatomical, functional and
molecular imaging techniques. Imaging techniques, such as Computerized
Tomography (CT), Magnetic Resonance Imaging (MRI) (Figure 7), and Positron
Emission Tomography (PET), facilitates the evaluation of internal organs
without the need for surgery. Imaging of the prostate holds an important role in
the integrative approach for a patient with PCa where diagnosis, staging, and
monitoring in watchful waiting or the response of treatment are part of the
regimen. The field of imaging has expanded from the characterization of locally
advanced or metastatic disease to include intra and extra prostatic tumor
delineation, including morphology and zonal anatomy. Current clinical imaging
30
techniques cannot detect early disease and consequently generate limited
information to be used for accurate staging; therefore, new techniques that can
provide anatomical, functional and molecular imaging information are urgently
needed [Kelloff et al., 2009].
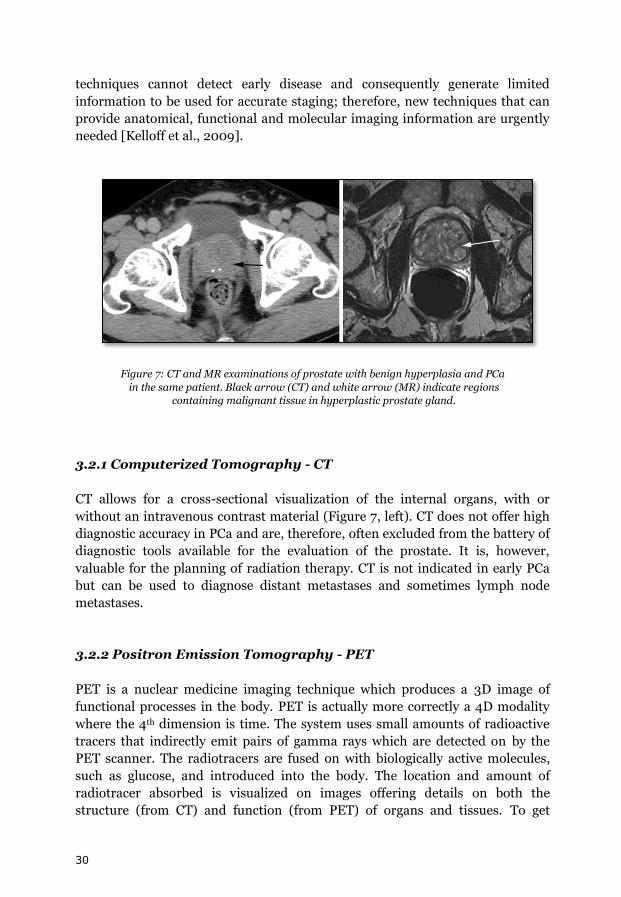
Figure 7: CT and MR examinations of prostate with benign hyperplasia and PCa
in the same patient. Black arrow (CT) and white arrow (MR) indicate regions
containing malignant tissue in hyperplastic prostate gland.
3.2.1 Computerized Tomography - CT
CT allows for a cross-sectional visualization of the internal organs, with or
without an intravenous contrast material (Figure 7, left). CT does not offer high
diagnostic accuracy in PCa and are, therefore, often excluded from the battery of
diagnostic tools available for the evaluation of the prostate. It is, however,
valuable for the planning of radiation therapy. CT is not indicated in early PCa
but can be used to diagnose distant metastases and sometimes lymph node
metastases.
3.2.2 Positron Emission Tomography - PET
PET is a nuclear medicine imaging technique which produces a 3D image of
functional processes in the body. PET is actually more correctly a 4D modality
where the 4th dimension is time. The system uses small amounts of radioactive
tracers that indirectly emit pairs of gamma rays which are detected on by the
PET scanner. The radiotracers are fused on with biologically active molecules,
such as glucose, and introduced into the body. The location and amount of
radiotracer absorbed is visualized on images offering details on both the
structure (from CT) and function (from PET) of organs and tissues. To get
31
optimal anatomical, functional and molecular information PET combined with
CT is used as; PET/CT [Bouchelouche et al., 2010].
18F-18-fluorodeoxyglucose is the most common PET tracer for tumors; however,
it is not useful in local PCa detection [Avril et al., 2010]. The roles of 11C/18F-
acetate or 11C/18F-choline as PCa PET tracers for primary diagnosis are not clear
[Jambor et al., 2010].
3.2.3 Magnetic Resonance Imaging - MRI
MRI, preferably with an endorectal coil, is used to improve prostate tumor
detection. MRI offers high-quality images of the internal organs (Figure 7, right).
The method is based on the magnetic behavior of hydrogen atoms as part of the
body’s inherent biomolecules and water in an outer magnetic field and their
manipulation by radiofrequency waves; an approach which generates images
with valuable information about the human anatomy and morphology.
Normally, a T2-weighted MRI obtained by with standard 1.5 Tesla scanners
equipped with endorectal coils, is used to detect and localize PCa. Tumors are
characterized by decreased signal intensity compared to the normal peripheral
zone. 3.0 Tesla scanners provides increased spatial resolution and thus
improved localization and staging. However, this MRI method does not provide
the sensitivity and specificity needed for accurate results of early stage PCa as
the cancer cell clusters often are minuscule. Additionally, there are problems
detecting tumors in zones other than the peripheral one [McMahon et al., 2009].
Multiparametric MRI combines T2-weighted imaging with one or more of
following approaches: Diffusion Weighted Imaging (DWI), Magnetic Resonance
Spectroscopy (MRS), and Dynamic Contrast Enhanced (DCE) functional
techniques. This is performed in one single study combining the different
imaging protocols [De Visschere et al., 2010; Weidner et al., 2011].
Contrast agents such as Ultra Small Supermagnetic Iron Oxide (USPIO) particles
add additional, valuable information to an MRI scan by increasing the signal of
PCa cells in lymph nodes [Thoeny et al., 2009]. However, lymph node staging is
still limited, also with MR. Currently MRI is of great value in difficult cases,
although it is not part of the clinical routine.
3.2.4 Magnetic Resonance Spectroscopic Imaging – MRSI
MRSI is a highly promising, non-invasive method, useful in the field of PCa
diagnosis. This cross-sectional technique offers an excellent overview of the
32
organ in all dimensions in-vivo, and possibilities for longitudinal assessments of
therapy, short and long-term changes related to disease and healing, volume and
density changes etc.
MRSI, preferably with an endorectal coil, provides visual anatomical and
morphological information simultaneous with spectral information about the
local metabolism and provides assessment of metabolic changes during a disease
process or treatment responses. This is of special interest since metabolic
perturbations often occur before the concomitant morphological changes. The
most commonly studied bio-markers for PCa found in the prostate metabolism
include citrate, choline compounds, and creatine. The ratio of choline
compounds (t-choline) and citrate are by far the most utilized biomarker for the
discrimination of malignant and non-malignant tissue, however, it may not be
the most optimal one [Swindle et al., 2003].
MRSI is not used routinely for prostate evaluations since it is more in the
experimental stage with room for improvements and furthermore, it is both
costly and time consuming. The present drawbacks of MRSI include difficulties
in obtaining optimal spectral resolution, poor spatial resolution, artifacts that
are, for example, caused by movements, in homogeneous external magnetic
field, metals, radiofrequent “noise” etc., but also the requirements for specialized
software and experienced personnel to acquire and interpret the data since this
technique is very much operator dependent and thus, as with most other
diagnostic tools, highly subjective [Kreis, 2004]. Furthermore, the prostate is, as
mentioned earlier, a heterogeneous organ and the tumor foci are often infiltrated
among normal tissue and, thus, will not appear clearly with MRSI. Moreover, a
more precise definition and understanding of functional anatomy of the prostate
is needed [McLaughlin et al, 2005]. However, MRSI is of immense use in
difficult cases. Technological advancements, such as functional, 2D and 3D
techniques and higher field strength, will improve tumor localization and render
MRSI a highly promising technique for the future [Thomas et al., 2008; Kelloff
et al., 2009; Larson et al., 2010].
3.2.5 Small Animal MRI/MRSI
Small animal MRI/MRSI scanners are rapidly emerging in modern research
facilities around the world. Animal models, particularly rodents, and the use of
MRI/MRSI have greatly advanced researchers’ understanding of various
pathologies and the effects of treatments etc. Since this technique is non-
invasive it has drastically reduced the number of animals needed since each
animal can be used more than once and thus followed longitudinally, i.e. each
animal can be used as its own control [Nastiuk et al., 2007]. However, given the
33
small size of rodents and the associated technical challenges, however, prostate
imaging studies in live animals only recently have become feasible, thanks to
technological improvements.
3.3 Prostate Biopsy
Taking and evaluating prostate biopsies are a team effort between the urologist
and the pathologist, and this is the most significant factor for the final diagnostic
verdict which strongly influences decisions regarding options for therapy. TRUS
guided biopsy sampling is most commonly used where the needle is inserted
through the thin rectal membrane into the prostate. Tissue samples are
extracted, with the biopsy needle, from different areas of the prostate. As tumors
often cannot be detected by imaging the prostates are systematically sampled
with 10-12 or more specimens along the sides of the peripheral zone and it is
recommended to sample a few laterally. Prostate tumors usually grow like thin
sheets laterally and consequently it is easy to misguide the biopsy needle past the
target. A larger prostate requires a more extensive sampling than a smaller size.
The biopsies in total however sample less than 1% of the prostate volume. This
means that there can be a significant amount of aggressive cancer present that
will be undetected by the biopsies. Again, imaging methods such as TRUS, CT or
MRI do not have the diagnostic accuracy to detect microscopic disease. Thus,
image guided biopsy sampling is not straight forward. PCa awareness, in the era
of PSA-testing, has increased the number of men diagnosed with low-grade/low-
risk cancers. This has led to treatment options such as focal therapy and active
surveillance to avoid unnecessary radical therapy with its many negative side-
effects. Since PCa often is multi-focal, both treatment options require improved
diagnostic methods in order to rule out aggressive tumor foci elsewhere in the
gland [Lazzeri et al., 2010; Ukimura et al., 2011]. Biopsy is an invasive
procedure with risks for complications such as: infection, bleeding, and in some
cases sepsis. Therefore, it is highly desirable to avoid unnecessary biopsies and
to discover bio-markers that possess the ability to detect microscopically small
amounts of aggressive cancer cells in the specimen and perhaps indicate that a
cancer could be present in the nearby tissue.
3.4 Histopathological Interpretation of Tissue Specimens
Prostate tissue is exceptionally heterogeneous by nature which complicates
classification and grading. Tumor grading and staging of prostate cancer is
fundamental in characterization and prognosis. The Gleason score system
provides information regarding the type of cancer cells while the TNM staging
system provides additional information concerning the extent of the cancer.
34
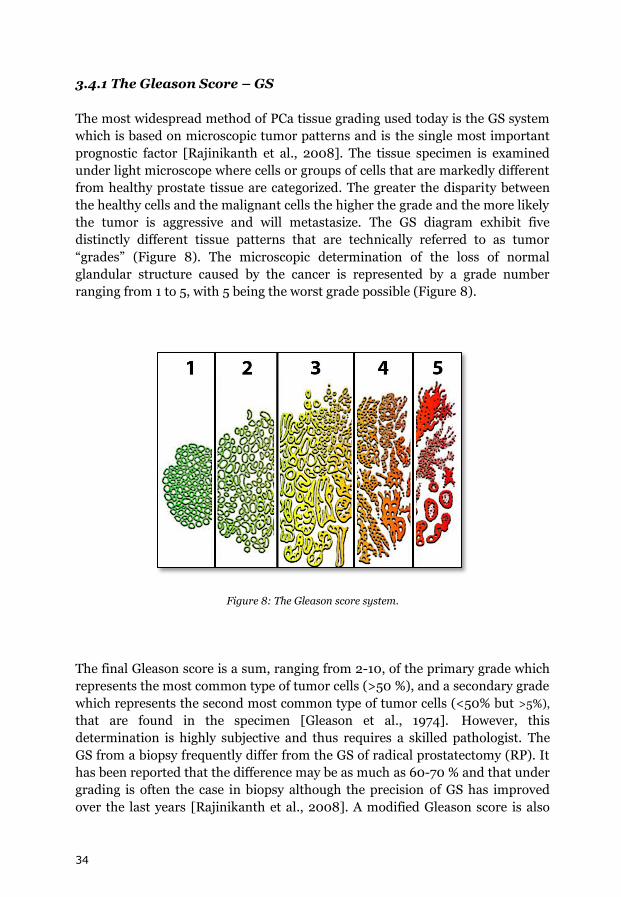
3.4.1 The Gleason Score – GS
The most widespread method of PCa tissue grading used today is the GS system
which is based on microscopic tumor patterns and is the single most important
prognostic factor [Rajinikanth et al., 2008]. The tissue specimen is examined
under light microscope where cells or groups of cells that are markedly different
from healthy prostate tissue are categorized. The greater the disparity between
the healthy cells and the malignant cells the higher the grade and the more likely
the tumor is aggressive and will metastasize. The GS diagram exhibit five
distinctly different tissue patterns that are technically referred to as tumor
“grades” (Figure 8). The microscopic determination of the loss of normal
glandular structure caused by the cancer is represented by a grade number
ranging from 1 to 5, with 5 being the worst grade possible (Figure 8).
Figure 8: The Gleason score system.
The final Gleason score is a sum, ranging from 2-10, of the primary grade which
represents the most common type of tumor cells (>50 %), and a secondary grade
which represents the second most common type of tumor cells (<50% but >5%),
that are found in the specimen [Gleason et al., 1974]. However, this
determination is highly subjective and thus requires a skilled pathologist. The
GS from a biopsy frequently differ from the GS of radical prostatectomy (RP). It
has been reported that the difference may be as much as 60-70 % and that under
grading is often the case in biopsy although the precision of GS has improved
over the last years [Rajinikanth et al., 2008]. A modified Gleason score is also
35
suggested, a score based on the most common and the worst grades present
[Epstein et al., 2010].
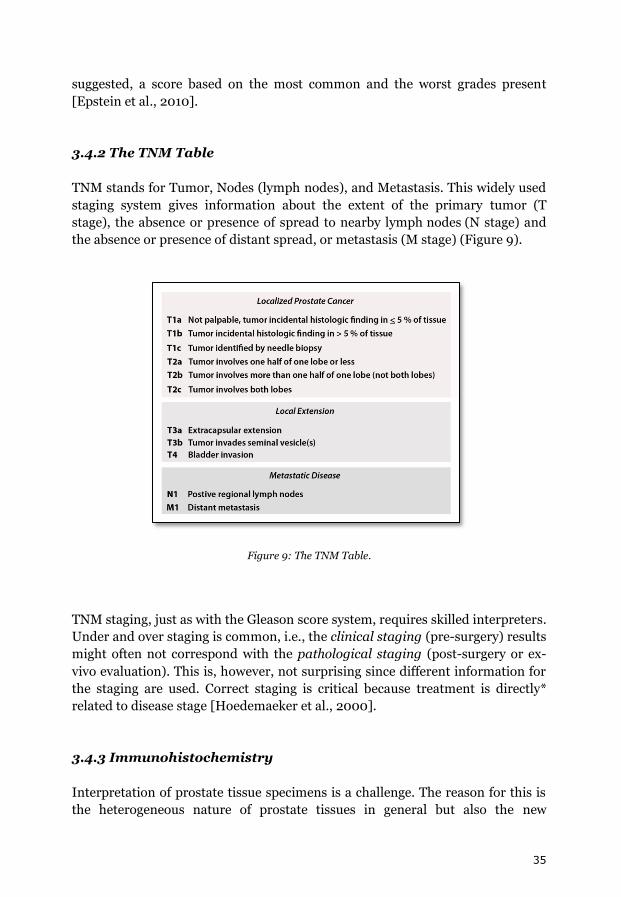
3.4.2 The TNM Table
TNM stands for Tumor, Nodes (lymph nodes), and Metastasis. This widely used
staging system gives information about the extent of the primary tumor (T
stage), the absence or presence of spread to nearby lymph nodes (N stage) and
the absence or presence of distant spread, or metastasis (M stage) (Figure 9).
Figure 9: The TNM Table.
TNM staging, just as with the Gleason score system, requires skilled interpreters.
Under and over staging is common, i.e., the clinical staging (pre-surgery) results
might often not correspond with the pathological staging (post-surgery or ex-
vivo evaluation). This is, however, not surprising since different information for
the staging are used. Correct staging is critical because treatment is directly*
related to disease stage [Hoedemaeker et al., 2000].
3.4.3 Immunohistochemistry
Interpretation of prostate tissue specimens is a challenge. The reason for this is
the heterogeneous nature of prostate tissues in general but also the new

36
demands that comes with earlier detection in the era of PSA-tests/screening
[Paner et al., 2008; Chun et al., 2010]. Differentiation of minimal cancer (<5 %
of biopsy specimen), atypical small acinar proliferation (ASAP), and high-grade
prostatic intraepithelial neoplasia (HGPIN) have increased the use of
immunohistochemical methods detection; α-methyl-acyl-coenzyme A racemase
(AMACR), nuclear p63, and the basal cell cytokeratin (34βE12). With the use of
such markers cancer can generally be distinguished from other conditions, but
as there are several mimickers of prostatic adenocarcinoma these
immunohistochemical markers are not universally applicable [Epstein, 2004].
37
Part II

38
39
Chapter 4: Nuclear Magnetic Resonance - NMR
4.1 General Introduction
In the recent decades, NMR spectroscopy [Pople et al., 1959; Ernst et al., 1987]
emerged as a powerful method to provide structural and dynamical information
of molecules at atomic level as well as unique diagnostic information in
medicine. Therefore, not surprisingly, a range of Nobel Prizes was awarded in
connection with NMR; Otto Stern (USA, 1943), Isidor I. Rabi (USA, 1944), Felix
Bloch, and Edward M. Purcell (USA, 1952), Richard R. Ernst (Switzerland, 1991),
Kurt Wüthrich (Switzerland, 2002), [The Nobelprize., 2010]. Chemist Paul C.
Lauterbur, USA and physicist Peter Mansfield, United Kingdom shared the
Nobel Prize in Medicine 2003 for the development of magnetic resonance
imaging (MRI). MRI, which has become an invaluable diagnostic method in
medicine, is directly derived from NMR, a fact that is often neglected in the
medicinal community [Fry et al., 2004].
The technique relies on the property of various nuclei, to possess a nuclear spin,
whose size is defined by the quantum number I. The nuclear spin is connected
with specific nuclear magnetic properties whose discovery by Rabi was awarded
the Nobel Prize in 1944. These magnetic properties, mainly the magnetic nuclear
moment, enabled researchers to study these nuclei in magnetic fields for
obtaining unique structural, chemical, physical and electronic information about
molecules since 1958.
4.2 The NMR Signal
The most common nuclei used in NMR in life science are 1H, 13C, 19F and 31P. In
general, these NMR active nuclei possess a property called spin with a value of
1/2. Insertion of a sample into a permanent outer magnetic field (Bo) causes the
nuclear magnetic moment of these nuclei to adopt different positions with
respect to this magnetic field, accompanied by a splitting up of their energy into
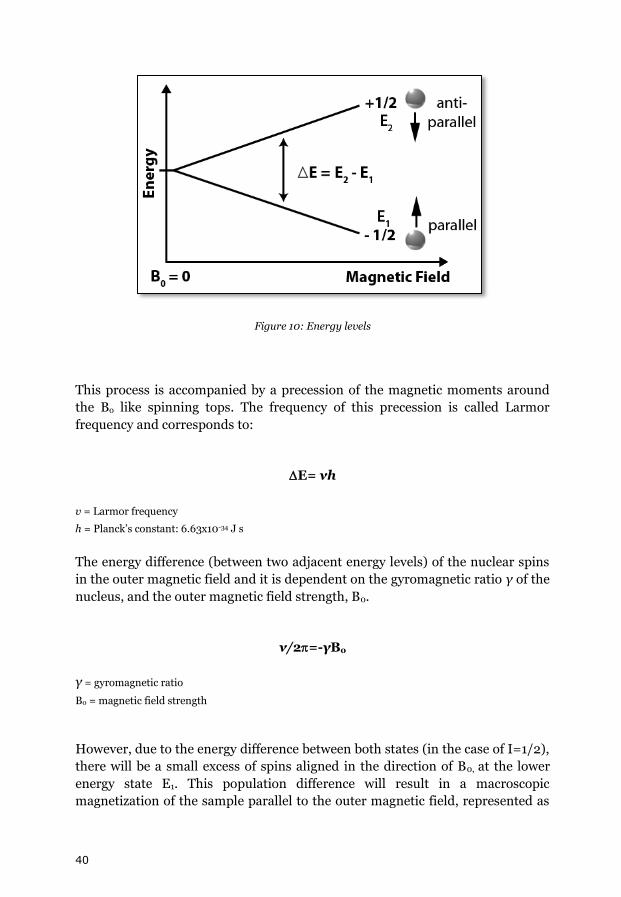
discrete energy levels. A nucleus with a spin of ½ adopts two possible magnetic
quantum states; m=1/2 which is the lower energy state also called α state or E1,
and m=-1/2 which is the higher energy state also called the β state or E2 (Figure
10).
40
Figure 10: Energy levels
This process is accompanied by a precession of the magnetic moments around
the Bo like spinning tops. The frequency of this precession is called Larmor
frequency and corresponds to:
E= νh
v = Larmor frequency
h = Planck’s constant: 6.63x10-34 J s
The energy difference (between two adjacent energy levels) of the nuclear spins
in the outer magnetic field and it is dependent on the gyromagnetic ratio γ of the
nucleus, and the outer magnetic field strength, B0.
ν/2=-γBo
γ = gyromagnetic ratio
B0 = magnetic field strength
However, due to the energy difference between both states (in the case of I=1/2),
there will be a small excess of spins aligned in the direction of B0, at the lower
energy state E1. This population difference will result in a macroscopic
magnetization of the sample parallel to the outer magnetic field, represented as

41
equilibrium magnetization vector, M0. This resulting vector Mo equals MZ since it
is aligned along the Z-axes. MZ is referred to as the longitudinal magnetization
(Figure 11).
Figure 11: NMR coordinate system.
The size of MZ is dependent on the Boltzmann distribution, as it is determined
by the following equation;
NE2/NE1 = e-∆E/kT
NE2 = higher energy state
NE1 = lower energy state
∆E = energy difference between the spin states
k = Boltzmann's constant: 1.3805 x 10-23 J/Kelvin
T = temperature in Kelvin.
4.3 The NMR Experiment
By applying in an NMR experiment radio frequency pulses at a frequency
which corresponds to the energy difference E between both states, it is possible
to flip the nuclear spins from their respective to the states via absorption of
this energy. An absorption of energy occurs when the energy E of the radio
frequent pulse meets the resonance conditions, namely the Larmor frequency
corresponding to the energy difference ∆E between the two spin states E2 and E1
which is described in the formula;
E =∆E=ħγB0
42
The radio frequent (RF) pulse applied along the X-axis creates a secondary
magnetic field that disturbs the alignment of the magnetic moments and causes
them to flip away from the equilibrium state. The required frequency is
dependent upon the static magnetic field, B0, and the nuclei observed. A
perpendicular flip of the initial magnetization Mz from the Z-axis to the XY-
plane where the transverse magnetization MY can be detected, requires a 900
pulse along the X-axes. This net magnetization may be described as an
oscillating magnetic field in excess that induces an alternating voltage in the
detection coil. This is the NMR signal also called free induction decay (FID). In
general, this signal diminishes over time due to the decay of the transverse
magnetization MXY in the XY-plane, characterized by the spin-spin relaxation
time T2 according to:
MXY =MXYoe-t/T2
In addition, there is a process, called spin lattice relaxation, which describes the
return of the longitudinal MZ magnetization towards its equilibrium (as prior to
the application of the NMR pulse). This process is characterized by a sample
specific spin lattice relaxation time, T1, and is described in the equation:
Mz = Mo
(1 - e-t/T1)
In an NMR experiment, the FID is time-dependent and can be converted into
the frequency domain by Fourier transformation [Jacobsen, 2007]. This will
provide the typical NMR spectrum, where frequency differences (magnetic field
differences) are plotted as a function versus intensity on a graph (spectrum).
This allows the visual observation of specific quantum mechanical magnetic
properties of the selected atomic nuclei. The most common type of nuclei
frequently analyzed by NMR is hydrogen (1H) which is, besides being the
lightest, by far the most abundant atom in the universe. NMR is nowadays
frequently utilized in the medical fields in the form of MRSI.
4.4 Chemical Shift
The chemical shift is a function of the nucleus and its local chemical
environment, thereby giving detailed information about the part of the molecule
where the nucleus is residing. By understanding different chemical
environments it is possible to obtain structural information about the molecule
in a sample [Chamberlain, 1959]. This is because the electronic environment,
that shields the nucleus from the magnetic field, is distinctive of the particular
nucleus and, thus, provides the exact resonance frequency of the nucleus. The
difference between the applied magnetic field and the field at the nucleus is
43
termed the nuclear shielding. The differences in the resonance frequency are
referred to as the chemical shift and it provides the information needed to
identify the compounds visible by NMR spectroscopy. The frequency shifts are
extremely small in comparison to the fundamental NMR frequency. In order to
detect the minuscule frequency differences the applied magnetic field must be
kept constant throughout the whole sample volume. This is done by using shim
coils. Since B0 differs to some extent between spectrometers the frequency
measurement in Hertz (Hz) was converted to a standardized scale that measures
in parts per million (ppm). This was done in a way that the NMR chemical shift
can be universally compared in ppm regardless of magnetic field strength. For 1H-NMR the chemical shift range is just over 10 ppm. The chemical shift is
calibrated using an internal standard as a reference; such as the commonly used
(tetramethylsilane) TMS [Van Dyke Tiers, 1958]. The chemical shift is obtained
by using the following calculations:
δ = (ν - ν0)/ν0
δ = chemical shift
ν = resonant frequency
ν0 = standard frequency
Frequently, a secondary reference of known chemical shift can be used instead of
the common standards such as TMS. A chemical reference standard of known
concentration is added to the sample and the concentration of the solute can
then be determined by comparing the integrals of the signals. The secondary
references are often the residual solvent signals or the unsuppressed H2O signal
[Cheng et al., 1998].
The secondary references are often used in quantitative NMR. However, there
are challenges involved in this, especially when quantitating HRMAS spectral
data. The standard to be used must be compatible with the sample, be
chemically inert, have a longitudinal relaxation time (T1) that, preferably, is
shorter than that of the sample, and furthermore, not generate resonances that
cause overlaps [Akoka et al., 1999]. A semi-quantitative approach is to compare
spectral ratios within each sample which does not require the need for suitable
internal standards. However, this method does not allow for separate resonances
to be studied independent from each other [Swanson et al., 2006; Sitter et al.,
2009]. Technological advancements have contributed to the development of new
types of internal standards such as the Electronic REference To access In vivo
Concentrations (ERECTIC). As the ERETIC signal is generated by an electronic
device it is therefore not dependent on the sample. This electronic reference
signal aids in the determination of absolute concentrations [Akoka et al., 1999;
44
Albers et al., 2009]. Modification and improvements of the ERETIC reference
include, as an example, the Amplitude-corrected Referencing Through Signal
Injection or ARTSI [Mehr et al., 2008].
4.5 Spin-Spin Coupling
Spin-spin coupling is an essential attribute of NMR as it provides detailed
structural and conformational information of the molecule. This spin-coupling
describes the phenomena that one nucleus feels the presence and spin state of
another nucleus nearby via connecting bonds (transferred via the magnetic
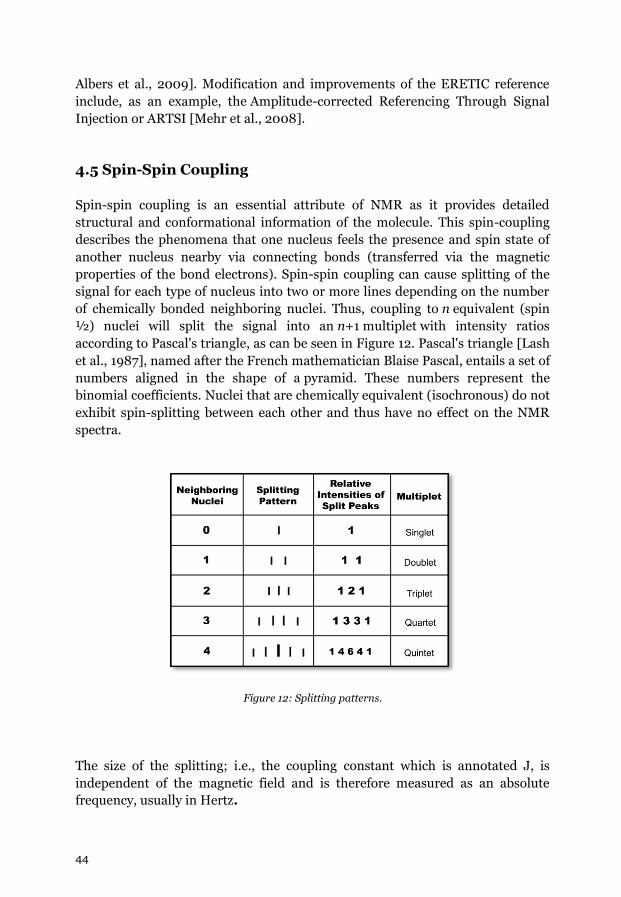
properties of the bond electrons). Spin-spin coupling can cause splitting of the
signal for each type of nucleus into two or more lines depending on the number
of chemically bonded neighboring nuclei. Thus, coupling to n equivalent (spin
½) nuclei will split the signal into an n+1 multiplet with intensity ratios
according to Pascal's triangle, as can be seen in Figure 12. Pascal's triangle [Lash
et al., 1987], named after the French mathematician Blaise Pascal, entails a set of
numbers aligned in the shape of a pyramid. These numbers represent the
binomial coefficients. Nuclei that are chemically equivalent (isochronous) do not
exhibit spin-splitting between each other and thus have no effect on the NMR
spectra.
Figure 12: Splitting patterns.
The size of the splitting; i.e., the coupling constant which is annotated J, is
independent of the magnetic field and is therefore measured as an absolute
frequency, usually in Hertz.

45
4.6 High-resolution Magic Angle Spinning (HRMAS) NMR
The line width of an NMR resonance depends on orientation-dependent factors,
such as chemical shift, chemical shielding anisotropy, and magnetic
susceptibility of the sample and susceptibility differences within the sample. The
rapid isotropic motion of the molecules in liquid state NMR averages the
anisotropic interactions and reduces broadenings due to dipolar couplings
resulting in narrow line widths. Furthermore, by choosing the correct sample
geometry, the broadenings, due to magnetic susceptibilities, are minimized
[Brown et al., 2001].
Solid or semi-solid samples are more difficult to analyze by NMR due to the lack
of molecular mobility and therefore the anisotropic nature of the corresponding
NMR spectra, which are usually wideline spectra without any significant
resolution. Due to this anisotropic nature, the NMR signal depends on the
orientation of the individual molecules with respect to the outer magnetic field;
an orientation dependence which for most NMR relevant interactions can be
described (in the case of spin I=1/2 systems) by the 2nd Legendre Polynom
P2(cosθ), with P2(cosθ)=(3cos2θ-1)/2. This term becomes zero when:
(3cos2θ-1)/2 = 0
cos2θ = 1/3
θ = 54.74º
This 54.74º angle is called the “Magic Angle” [Andrew et al., 1959]. By spinning
the sample rapidly at the magic angle, 54.74º with respect to B0 the orientation
dependent P2 term will be time averaged to zero. This will reduce anisotropic
interactions to zero, or in the case of chemical shift anisotropy to their isotropic
value and will break up the wideline NMR spectra into a set of individual narrow
lines which can be assigned as in the case of liquid NMR spectroscopy (Figure
13), [Maas et al., 1996].
46
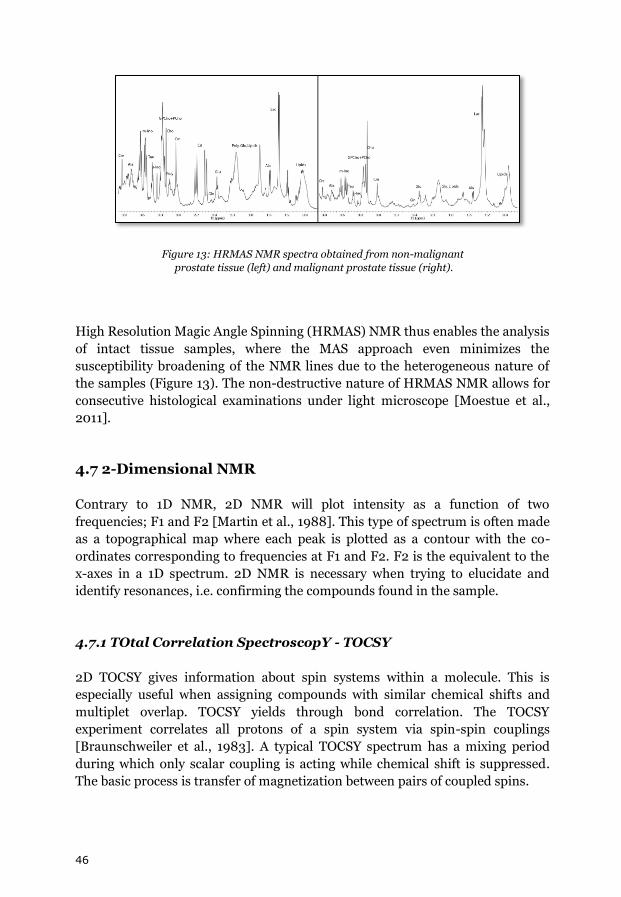
Figure 13: HRMAS NMR spectra obtained from non-malignant
prostate tissue (left) and malignant prostate tissue (right).
High Resolution Magic Angle Spinning (HRMAS) NMR thus enables the analysis
of intact tissue samples, where the MAS approach even minimizes the
susceptibility broadening of the NMR lines due to the heterogeneous nature of
the samples (Figure 13). The non-destructive nature of HRMAS NMR allows for
consecutive histological examinations under light microscope [Moestue et al.,
2011].
4.7 2-Dimensional NMR
Contrary to 1D NMR, 2D NMR will plot intensity as a function of two
frequencies; F1 and F2 [Martin et al., 1988]. This type of spectrum is often made
as a topographical map where each peak is plotted as a contour with the co-
ordinates corresponding to frequencies at F1 and F2. F2 is the equivalent to the
x-axes in a 1D spectrum. 2D NMR is necessary when trying to elucidate and
identify resonances, i.e. confirming the compounds found in the sample.
4.7.1 TOtal Correlation SpectroscopY - TOCSY
2D TOCSY gives information about spin systems within a molecule. This is
especially useful when assigning compounds with similar chemical shifts and
multiplet overlap. TOCSY yields through bond correlation. The TOCSY
experiment correlates all protons of a spin system via spin-spin couplings
[Braunschweiler et al., 1983]. A typical TOCSY spectrum has a mixing period
during which only scalar coupling is acting while chemical shift is suppressed.
The basic process is transfer of magnetization between pairs of coupled spins.

47
4.7.2 Hetero-nuclear Single Quantum Coherence –HSQC
HSQC has been used since its invention in 1980 [Bodenhausen et al., 1980]. This
type of 2D spectrum displays the chemical shift of 1H on the x-axes and the
indirect chemical shift of a hetero-nucleus such as 13C or 15N on the y-axes. The
spectrum show the cross peaks for each unique proton attached to the hetero-
nucleus. This provides the chemical shift of both the proton and the hetero-
nucleus coupled to the same proton, and thus, important qualitative information
for the identification of a compound [Soubias et al., 2003].
48
Chapter 5: Metabolomics Using HRMAS NMR
5.1 Concept of Metabolomics
Metabolomics is part of the omics sciences, such as genomics, proteomics,
transcriptomics, in systems biology. Although the term “metabolomics” is rather
novel this type of approach to elucidate metabolic perturbation in biological
systems due to disease is not new. The notion that changes in tissues and
biological fluids, such as urine, are indicative of disease were explored in the
ancient Greece and China [van der Greef et al., 2005; Nicholson et al., 2008],
and Dalgliesh et al investigated metabolic patterns in urine and tissue by using
GC-MS in 1966 [Nordström et al., 2010].
There has been some confusion regarding the definitions of the terms
“metabolomics” and “metabonomics”. Nicholson et al introduced the expression
“metabonomics” in 1999 [Nicholson et al., 1999], while Fiehn et al launched the
term “metabolomics” just a year later [Fiehn et al., 2000]. Although
metabolomics is the more common term in use today, there are differences
between the two slightly similar terms: “metabolomics” is usually referred to as
the more comprehensive method covering a global range of metabolites typically
analyzed by mass spectrometry (MS). “Metabonomics” is often referred to as
being based on the use of NMR and thus not as comprehensive as MS. This is
due to the fact that MS detects metabolites that are present at concentrations
orders of magnitude lower than what can be detected by NMR [German et al.,
2006]. The term metabolomics, though NMR based, will be used in this thesis.
The metabolome is defined as the complete set of small molecule metabolites,
endogenous as well as exogenous, found in a biological sample, i.e., specific cell,
organ or organism [Wishart et al., 2007]. The exploration of the metabolome
aids in the search for unique fingerprints responsible for different phenotypes
[Koulman et al., 2008]. The distinction between phenotype and genotype was
proposed in 1911 by Wilhelm Johannsen with the aim of clarifying the difference
between an organism's heredity and what that heredity produces [Johannsen,
1911]. Phenotypes are the outcome of genetic expressions as well as the influence
of environmental factors, and the interactions between the two; and this may be
detected in the metabolome.
Both extrinsic and intrinsic factors have input on the metabolome. Extrinsic
factors may include lifestyle choices, nutrients and non-nutrients, physical
activity, stress, drugs, and colonic micro flora (micro biome). Intrinsic factors
may comprise genotype, age, body composition, tissue turnover, reproductive
49
status, and diurnal cycle [Koulman et al., 2008, Goodacre, 2007]. The
metabolites present in a metabolome include metabolic intermediates, amino
acids, fatty acids, etc. Metabolomics aids in the unraveling and the discovery of
organ-specific endogenous metabolites that has the potential to be reliable
indicators of organ function and viability as well as valuable markers for
treatment response [Conti et al., 2006]. The metabolites may be viewed
individually but in a more holistic context or as a group in, what is termed,
metabolic profiling [Beckonert et al., 2007]. Metabolomics is an excellent tool in
translational research as it provides a reflection of, for example, the unique
metabolism of experimental models where the results ultimately are to be
applicable clinically. This is of special interest in the emerging field of molecular
imaging where diagnostic technologies such as MRSI or PET are utilized
[Spratlin et al., 2009]. The comprehensive investigation of the metabolome will
provide a more holistic picture of the biochemical perturbations which are
expressed subsequent gene expressions and protein activities [Bathen et al.,
2010]. The results may therefore be applied clinically in-vivo to characterize an
organ by utilizing bio-markers that have the capacity to discriminate between
disease and health. A powerful application of metabolomics is in the
differentiation of malignancy vs. non-malignancy. However, despite this, the
approach is not commonly used in the clinics for oncology [Spratling et al.,
2009].
5.2 Metabolomics in the Characterization of the Prostate
Successful therapy for PCa depends on early diagnosis and accurate evaluation
of progression and outcome. Bio-markers aimed for the characterization of the
prostate are especially difficult due to the heterogeneity of the prostate,
especially when malignant, and the fact that it is difficult to differentiate
between the aggressive type vs. the indolent type of PCa [Madu et al., 2010], and
in addition, there is a variability between patients which presents a challenge
using the diagnostic tools available [Abate-Shen et al., 2009]. Thus, clinical
indicators in the form of robust bio-markers are important in modern medicine.
The human prostate metabolome, visible by HRMAS NMR spectroscopy,
consists of small, freely rotating organic molecules [Swanson et al., 2003, 2006;
Tessem et al., 2008]. The Krebs cycle intermediate citrate is one of the most
important metabolites found in the prostate metabolism and has been
researched thoroughly by different means. By assessing the biochemistry of, for
example, the Krebs cycle intermediates using the metabolomic approach where
extrinsic and intrinsic factors are included, a more comprehensive observation
will be provided [Griffin et al., 2004].

50
5.3 Metabolomics, Nutrition and Prostate Cancer
The prevention of the development of disease and prostate cancer is even more
important than the search for bio-markers [Silberstein et al., 2010]. There is a
growing body of evidence suggesting a relationship between nutrition, health,
and PCa risk, and where there seems to be a particularly strong link between
obesity and PCa [Coffey, 2001; Ornish et al., 2009; Gonzales et al., 2010; Kahn
et al., 2010; Thun et al., 2010). Furthermore, the roles of certain food
components as protectors against disease are documented [Davis et al., 2004;
Afman et al., 2006]. By defining an individual’s healthy metabolome at baseline
under specific nutritional conditions and lifestyle factors may ultimately lead to
personalized medicine. The baseline metabolome would aid in the interpretation
of disease and a comprehension of optimal nutritional intake and the
maintaining of homeostasis on an individual basis [van der Greef 2004; German
et al., 2005; Gibney et al., 2005; Trujillo et al., 2006; Goodacre, 2007; Holmes et
al 2008]. Essential nutrients are especially interesting since they must be
obtained by dietary means. These nutrients: vitamins, dietary minerals, essential
fatty acids, and essential amino acids, are required for normal body functioning.
The essential polyunsaturated fatty acids (PUFAs) omega-6 and omega-3 has
received much attention. Omega-3 is believed to possess protective properties
while omega-6 has been known as an instigator for PCa. These PUFAs, along
with numerous other nutrients, are detectable by HRMAS NMR.
51
Part III

52
53
Chapter 6: Materials and Methods
“Mti hawendi ila kwa nyenzo”*
Swahili kanga writing
6.1 Experimental Setup
6.1.1 Procedure of HRMAS NMR Spectroscopy
All spectroscopic data were acquired at 11.7 T on a Bruker AMX2 NMR
spectrometer (Bruker Biospin GMBH, Karlsruhe, Germany), operating at a 1H
NMR frequency of 500.13 MHz and equipped with a 4 mm dual band, 1H/13C,
HRMAS probe head from Bruker. NMR spectra were acquired at room
temperature (20◦C). The magic angle spinning rate was set to 5 kHz for all
experiments except for the 2D rotor-synchronized TOCSY experiments were a
41.8 ms mixing time at 2.25 kHz sampling was used. The 2D 1H-13C GE-HSQC
(phase-sensitive) was performed at 5 kHz. The MAS spinning rate suppresses
chemical shift anisotropy and the line broadening effects due to dipolar
couplings.
Prostate tissues were cut with a surgical steel blade into smaller specimens
weighing ~15+5 mg so as to fit the MAS rotor with insert. 4 mm cylindrical ZrO2
rotors with spherical inserts were utilized. Kel-F caps were used to secure the
rotors. D2O were used for 2H field locking and ten micro liters of D2O were
added to each specimen and allowed to soak in for a few minutes. Prostate tissue
specimens were packed in rotors and where either immediately placed in the
HRMAS probe to be analyzed or temporarily stored at -20◦ C. In order to avoid
possible errors all samples were treated as identically as possible.
6.1.2 1D 1H HRMAS NMR
For the 1D HRMAS NMR spectroscopy a rotor-synchronized Carr-Purcell-
Meibom-Gill (CPMG) [Meiboom et al., 1958], pulse sequence (90o-(τ-180o- τ)n-
acquisition) with a 5 kHz spinning rate was used. A T2 filter of 20 ms duration
*You need to have proper tools to carry out any task.
54
was used to suppress broad signal contributions from macromolecular
components. The T2=20 ms was chosen based on T2 time studies performed in-
house. The excitation band width was set to 10309 Hz and each spectrum was
recorded with 256 transients, using 16K complex time domain data points and
with a repetition time of 5.0 seconds. To suppress the resonances arising from
H2O a presaturation pulse during the relaxation delay prior to the CPMG pulse
sequence. All 1D spectra were generated, from start to finish, at a maximum time
of 30 minutes.
Spectral 1D data were analyzed off-line using Mestre-C 4.9.9.6 and/or MNova
6.0.4. (Mestrelab Research, A Coruña, Spain). The free induction decays (FID’s)
of the CPMG edited 1H HRMAS spectra were subjected to a 1.5 Hz exponential
multiplication, zero-filled to 60k complex points preceding Fourier
transformation. The resulting spectra were manually phased and baseline
corrected using a multi-point polynomial function. The spectra were referenced
to the residual water peak by setting the chemical shift of the lactate doublet
equal to exactly 1.33 ppm. A selection of metabolites, that were relatively clear of
spectral overlaps, was subjected to a line-fitting procedure/deconvolution so as
to obtain metabolite peak areas.
6.2 Prostate Tissue Samples
Excised tissues are no longer under enzymatic control outside of its natural
environment, which is the body. Therefore, all biological specimens: tissues, and
fluids, require strict handling to avoid unnecessary oxidation and degradation
[Sitter et al., 2009]. It is not practically feasible to analyze fresh tissues,
therefore all excised tissue samples were immediately snap-frozen in N2(l) and
thereafter stored in a freezer with a temperature of -70C◦. Thawing does have an
effect on the specimens [Middleton et al., 1998; Wu et al., 2003] which needs to
be taken into consideration when interpreting the results.
6.2.1 Patients
Informed consent was obtained from the patients and the studies were approved
by the Research Ethics Committee of Umeå University Hospital, Umeå, Sweden.
Forty patients with PCa were included in this study. All of them underwent
prostatectomy and agreed to donate the surgical specimen by a form of written
consent. Study participants, aged between 41 and 71 years, were drawn from the
northern part of Sweden. The tumor stage was in the range of 1 to 3, and the
Gleason scores were GS 6 (3+3) and GS 7 (3+4). Serum PSA value was 12.41 +
55
13.02 (range 3.42 – 50.03). None of the patients had undergone any form of
treatment before surgery.
Specimens were chilled immediately after surgery. Prostate surfaces were inked
for anatomical identification purposes and thereafter the gland was cut into
horizontal 1 cm thick sections. Between 2 and 20 tissue punches, approximately
0.5 cm in diameter, were obtained from the peripheral zone of each section. All
specimens were snap-frozen in N2(l) within 30 minutes after surgery and
thereafter stored in -70 C freezers. In order to identify the punches sampled
each prostate slice were fixed using formalin and embedded in paraffin before
being cut into 5-µm thick sections. Each section was stained with haematoxylin
and eosin, thus enabling tumor foci identification using microscopy. The foci
were thoroughly marked and the frozen punches were preliminary classified as
malignant or non-malignant by studying the tissue surrounding the holes from
where the punches originated from. The frozen tissue punches were randomly
cut into smaller specimen and analyzed by HRMAS NMR.
6.2.2 Rat
The study protocol for the animal experiments was approved by the Animal
Research Ethics Committee of Umeå, Umeå, Sweden.
Nine adult male Sprague-Dawley rats (B&K, Stockholm, Sweden) were included
in this study. The Sprague Dawley strain is an outbred multipurpose model. The
rats were anaesthetized according to the previously described method [Lissbrant
et al., 2004], and their ventral prostate (VP) and dorso-lateral (DLP) lobes were
removed and immediately frozen in liquid nitrogen.
Six adult male Copenhagen x Fisher F1 rats (ALAB, Uppsala, Sweden) were
transplanted subcutaneously with pieces of highly differentiated Dunning R3327
PAP rat prostatic adenocarcinoma in their right flank as earlier described
[Häggström et al., 1998]. Upon growth to 1-2 cm in diameter each tumor was
removed and immediately frozen in liquid nitrogen.
6.3 Interpretation of Data
The interpretation of NMR data requires, besides obligatory spectroscopic skills,
a thorough comprehension of the particular species analyzed, and general
biochemical knowledge. Assignments of the spectral resonances in this study
were made by consulting published data, and by 2D TOCSY, and 2D GE-HSQC
experiments. The 2D NMR experiments are valuable when assigning overlapping
56
resonances which are common in HRMAS spectra. It is not uncomplicated to
quantify this type of spectral data due to the overlapping resonances, as already
mentioned, furthermore, there are challenges involved in weighing the samples
correctly due to the natural variation in tissue composition of intact biological
specimens. In this study the basic deconvolution method to quantify spectral
data was used: linefitting of resonances and thereafter using the spectral ratios
within each sample [Inouye et al., 2010].
6.3.1 Pathologic Analysis
Formalin fixed, paraffin embedded specimens were cut in 5 micron thick
sections and stained with hematoxylin-eosin (H&E). Frozen samples were cut
unfixed and then stained either with H&E or immunostained for high molecular
weight cytokeratin (cytokeratin-hmw, DAKO, Stockholm, Sweden) detecting
basal epithelial, or the cell proliferation marker Ki67 (DAKO).
The slides were reviewed by a highly experienced uro-pathologist who
determined the percentage of non-malignant glandular, non-malignant stroma,
and the percentage and grade of prostate cancer. Cancer-containing prostate
tissues (glands lacking cytokeratin-hmw positive basal epithelial cells) were
compared to non-malignant tissues (glands with an intact basal epithelial cell
layer) regardless of relative glandular and stromal composition. The fraction of
malignant vs. non-malignant prostate tissue was established using a light
microscope with a square-lattice mounted in the eye-piece to count the number
of grid-intersections falling on each tissue compartment. The distance between
the remaining holes from the punches and the closest tumour was measured on
the whole mount sections. As “completely healthy,” i.e. benign, prostate tissues
were lacking non-malignant were used as such.
6.3.2 Statistical Analysis
Upon the completion of the NMR measurements and post NMR processing, the
results, in the form of integral areas, were brought into Excel (Microsoft Office
Excel 2003) for the generation of a matrix. The results from the
histopathological analysis and pathological staging were added.
The data matrix was calculated with: SPSS (v. 16.0, SPSS, Chicago, IL, USA)
where basic descriptive statistics such as means and SD was generated, and
STATA (v. 10, StataCorp LP, College Station, TX, USA), where the data was
standard error-adjusted in order to take clustering (dependencies between
samples obtained from the same patient) into considerations. The following
57
statistical methods was used; Multivariate Linear Regression, Binary Logistic
Regression, Receiver Operating Characteristic (ROC) and Area Under the ROC
Curve (AUC). Odds Ratios (ORs) and 95% confidence intervals (CIs) were
calculated. P-values <0.05 were considered to be statistically significant.
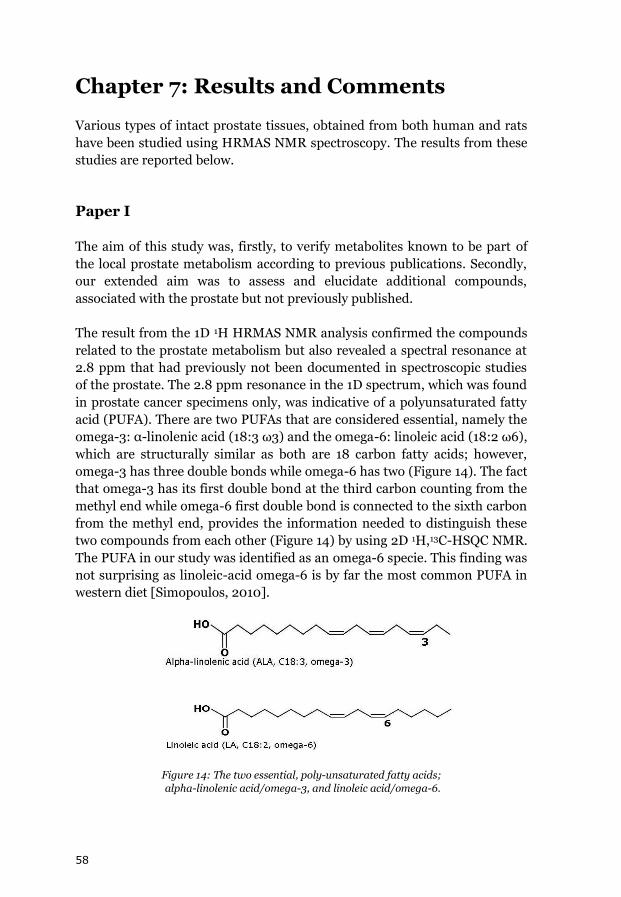
58
Chapter 7: Results and Comments
Various types of intact prostate tissues, obtained from both human and rats
have been studied using HRMAS NMR spectroscopy. The results from these
studies are reported below.
Paper I
The aim of this study was, firstly, to verify metabolites known to be part of
the local prostate metabolism according to previous publications. Secondly,
our extended aim was to assess and elucidate additional compounds,
associated with the prostate but not previously published.
The result from the 1D 1H HRMAS NMR analysis confirmed the compounds
related to the prostate metabolism but also revealed a spectral resonance at
2.8 ppm that had previously not been documented in spectroscopic studies
of the prostate. The 2.8 ppm resonance in the 1D spectrum, which was found
in prostate cancer specimens only, was indicative of a polyunsaturated fatty
acid (PUFA). There are two PUFAs that are considered essential, namely the
omega-3: α-linolenic acid (18:3 ω3) and the omega-6: linoleic acid (18:2 ω6),
which are structurally similar as both are 18 carbon fatty acids; however,
omega-3 has three double bonds while omega-6 has two (Figure 14). The fact
that omega-3 has its first double bond at the third carbon counting from the
methyl end while omega-6 first double bond is connected to the sixth carbon
from the methyl end, provides the information needed to distinguish these
two compounds from each other (Figure 14) by using 2D 1H,13C-HSQC NMR.
The PUFA in our study was identified as an omega-6 specie. This finding was
not surprising as linoleic-acid omega-6 is by far the most common PUFA in
western diet [Simopoulos, 2010].
Figure 14: The two essential, poly-unsaturated fatty acids;
alpha-linolenic acid/omega-3, and linoleic acid/omega-6.

59
Linoleic acid is the omega-6 compound which is considered to be the
“parent” of several n-6 compounds varying in length from 14 to 40 carbons
and thus would be the essential fatty acid (EFA) [Cunnane, 2003]. Several
studies have indicated an excess of omega-6 and its derivatives as instigators
of inflammation and also PCa [Kelavkar et al., 2006, 2009; Ukoli et al.,
2010]. One of the more known n-6 EFAs arachidonic acid (AA); 20:4 ω6, is a
precursor in the production of eicosanoids which are compounds involved in
the regulation of inflammation and immunity [Funk, 2001]. The n-3
eicosapentaenoic acid (EPA) competes with AA for prostaglandin and
leukotriene synthesis at the cyclooxygenase (COX) and lipoxygenase (LOX)
level [McEntee et al., 2010]. However, the term EFA is ambiguous and the
metabolism of essential and non-essential fatty acids is very complex and
more interconnected than previously recognized. The requirements and
health effects of EFAs are individual and dependent on variables such as: age
and tissue type, but also on genetic differences in metabolism [Simopoulos,
2010]. α-linolenic acid and linoleic acid cannot be synthesized endogenously
“de novo”, but it seems that this is possible with the 16 carbon precursors;
16:3 ω3, and 16:3 ω6 [Cunnane, 2003]. Both ω6 and ω3 are readily β-
oxidized and recycled into cholesterol and palmitic acid, which is the most
common saturated fatty acid in mammals [Beare-Rogers et al., 2001], and,
less easily replaced in tissue lipids than the non-essential common fatty acids
such as palmitic and stearic acid [Cunnane et al., 2003].
HRMAS NMR detects freely rotating compounds in the semi-solid and intact
tissue specimens investigated. Furthermore, a filter to suppress signals from
macro-molecules was used therefore limiting the detection of compounds
tightly bound to membranes. As arachidonic acid is the most biologically
important PUFA of cell membranes and, when released by phospholipase,
directly affect cell signaling pathways and serve as substrate in the COX and
LOX pathways, a hypothesis is therefore that this n-6 PUFA was released
from membrane phospholipids due to inflammatory activation. Other
options include: the conversion of PUFAs for the, apparently, protective
properties of membrane lipid saturation [Rysman et al., 2010], or simply
from a PUFA buildup needed for the generation of unsaturated fatty acids or
cholesterol to be used for the increased synthesis of cellular membranes due
to increased proliferation.
Paper II
This study was designed to be a comparative investigation where both
human and rat prostate tissues were scrutinized. The human specimens
originated from the peripheral zone only, and the rat specimens were
60
obtained from three different lobes, whereas two of them were combined
into one entity. In addition, a subcutaneous experimental rat PCa tumor was
also included in the design. The HRMAS NMR spectrum provides an image
depicting the local metabolism found in the specimen analyzed, hence,
comparison of tissues obtained from different species is straightforward. Our
result revealed obvious spectral differences between the diverse prostate
tissue types, indicating metabolic distinctions.
Rat, mouse, and man share approximately 99 % of the same genes [Gibbs et
al., 2004], which clarifies the popularity of using rodents as experimental
PCa models [Shirai et al., 2000]. However, a similar genome does not,
unfortunately, provide the key to perform realistic comparisons [Buttyan et
al., 1993; Lamb et al., 2005]. The rat lateral prostate is the closest analogue
to the human peripheral zone where most cancers occur. Furthermore, the
LP, but not the DP, contains citrate producing cells. As it is difficult to
separate the LP from the DP these lobes are usually combined into the DLP
entity, which is what we used in our study. One of the finding was the
presence of a 2.8 ppm resonances stemming from omega-6 fatty-acids, in all
of the Dunning tumors specimens and in some of the DLP specimens. This is
in line with our findings in Paper I, i.e., this 2.8 ppm resonance was found in
some PCa specimens. One of the questions here is to why the completely
healthy DLP show similar characteristics as the Dunning tumors and human
PCa tissues. One answer is suggested: the Dunning tumor is believed to
originate from the DP and consequently both should therefore share similar
metabolic characteristics. Furthermore, the DP is the lobe in the DLP entity
that lacks citrate accumulating cells. When comparing the spectra obtained
from the DLP and the Dunning tumor it is evident that they share similar
metabolic characteristics as compared with the VP which expresses a vastly
different metabolism. The Dunning tumor spectra most closely resemble the
spectra obtained from human PCa tissue. The one important feature that
indicates cancer in both human PCa and the Dunning tumor is the increased
resonance of (GPCho+PCho) over the free choline resonance. However, this
sign is also evident in completely healthy DLP. Therefore, it would be of
great value to study the metabolism of the DP and the LP separately. Another
important reason for this is to further study and to clarify the functions of
these two lobes in regards to hormonally induced PCa and senescence.
Obviously, it is not optimal to compare a prostate tissue sampled from a 65
years old man with one obtained from a 12 wks old rat. This is of special
interest in this study as age-dependent overgrowth and pathological changes
that leads to cancer usually arises in the DLP but not in the VP. Interestingly,
the COX-2 pathway expression is both higher and dependent on the ageing
process in the DLP as it increases with age, but seems to be unaffected in the
VP. [Badawi et al., 2004]. It is logical that inflammation increases with age.
61
As already discussed above in Paper I, the COX enzymes convert the omega-
6 fatty acid arachidonic acid into the pro-inflammatory, and also pain
producer, prostaglandin E2 (PGE2). There exist two forms of the COX
enzyme; COX-1, which is expressed in most tissues and organs, and the
inducible enzyme COX-2 which is primarily localized in inflammatory cells.
COX-2 is therefore considered to be the key enzyme in fatty acid metabolism
and inflammation. To inhibit the conversion of AA to PGE non-steroidal
anti-inflammatory drugs (NSAIDs), including COX-2 inhibitors, are
frequently used, in spite of significant negative side effects [Seibert et al.,
1994]. Omega-3 is believed to function as a natural inhibitor of COX-2 and
by reducing inflammation indirectly decreases the risk of PCa. Importantly,
however, this potential effect appears to be modified by genetic variation in
COX-2 [Fradet et al., 2009; Simopoulos, 2010]. Furthermore, a recent study
showed that dietary modification that increased tumor EPA and LA (n-3)
content enhanced responses to hormone ablation therapy. Conversely, a
relapse to androgen independent growth (measured by PSA and tumor
volume) positively correlated with tumor AA (n-6) content [McEntee et al.,
2008]. As mentioned earlier, the optimal study would be to separately
scrutinize the DP and the LP obtained from senescent rats and compare with
human PCa tissue samples. In addition, a thorough dietary investigation is
recommended to be included in the study to evaluate the therapeutic effects
of PUFAs.
Paper III
The third study entailed a more comprehensive metabolomic investigation,
based upon the knowledge generated from study I and II. The aim was to
discover spectral bio-markers that correlate/relate to the various dependents
obtained from the clinical examinations of human prostate tissues. In this
study, bio-markers known to be part of the prostate metabolism were
investigated by exploiting peak ratios and their variation due to metabolic
perturbations, using the basic deconvolution method. This approach is
termed as “the use of biochemical prior knowledge” and is used to decrease
uncertainties with overlapping resonances [Inouye et al., 2010]. This
method, using ratios with arbitrary units, circumvent the problems involved
in finding the optimal standard reference and leak-proofing the rotors, and
the need for T2 value adjustments, all in order to make accurate quantitative
calculations [Swanson et al., 2006; Albers et al., 2009].
Histological evaluation of needle biopsy cores from the prostate is the initial
step in diagnosis and treatment decision making. A representative biopsy
may provide an indication as to the nature of the cancer in the prostate gland
62
based on the Gleason score and the volume of disease. Cores containing
sufficient amount of cancer are essential for the evaluation. However, there
is no imaging method available that can guide towards the most malignant
part of the prostate. Because more men are now being diagnosed with local
PCa, due to increased PSA-testing, it is necessary to evaluate and improve
diagnostic options with the aim of minimizing under grading of biopsies. As
many prostate tumors are latent and will not pose a threat, it is desirable to
find a biomarker than is able to differentiate between the indolent and
aggressive types in order to avoid overtreatment. Therefore, the aim of this
study was to identify potential bio-markers for the discrimination of
aggressive vs. the more latent type of cancer and also to estimate the fraction
of tumor cells in any given prostate tissue specimen.
As most PCa studies have focused on the tumor, and as it is not possible to
accurately detect tumors in-vivo by the imaging methods currently available,
we used an opposite approach, i.e., by searching for bio-markers in the non-
malignant tissue. The metabolomic bio-marker that was prominent in our
study was the naturally occurring nutrient inositol which apparently has the
potential of sensing tumors and their corresponding grades elsewhere in the
organ. Inositol can be phosphorylated in seven variations to form
phosphoinositides that act as cellular mediators of signal transduction,
metabolic regulation, and overall growth [Mathews et al., 2000].
By exploiting the ratio of myo-inositol/scyllo-inositol discrimination
between GS 6 and GS 7 was achieved. This is potentially a very important
finding as GS 6 tumors usually have a better prognosis than GS 7. There are
also different treatment approaches for these two different types of prostate
cancer. This novel finding needs to be explored further as bio-markers that
have the power to detect tumors and also estimate their Gleason score in
non-malignant tissue is highly desired. Such feature would minimize the
number of biopsy cores sampled as it would therefore not be necessary to
aim for the tumor itself. This type of bio-marker is currently lacking and is
essential for successful focal therapy and/or active surveillance [Lazzeri et
al., 2010]. This finding suggests protective properties of inositol which is in
line with numerous other studies [Vucenic et al., 2003, 2006; Fardet, 2010].
The detection of loss/failure of cellular protection at an early stage has the
potential of being the basis for preventative medicine.
Curiously, we did not find an equivalent bio-marker in malignant prostate
tissue. The ratio of citrate/creatine came close to statistic significance when
not adjusting for clustering (uneven sampling among the patients in our
study). The focal point here is the complexity of biochemical pathways in all
living organisms and the importance of viewing each patient as an individual

63
rather than a gross average, as there are many factors that have an effect on
the metabolome. A tumor marker was identified in a previous study (Paper
II); (GPCho+PCho)/Cre. An increased choline metabolism is a well known
marker for cancer and is verified in other PCa studies. Our study investigated
the correlative strength of this bio-marker ratio; (GPCho+PCho)/Cre, and
the fraction of tumor cells in any given prostate tissue sample. Indeed, we
found statistically significant correlation. We also found a significant,
although very weak, correlation with the proliferation marker Ki67 and
(GPCho+PCho)/Cre. This raises questions about the underlying reasons for
the increased choline metabolism, which in fact, is poorly understood
[Moestue et al., 2010], and as it might not to be correlated with proliferation
[Gillies et al., 2005], our observation with Ki67 and (GPCho+PCho)/Cre
might be a coincidence. Our study showed large variations in the
concentration of choline compounds, especially in prostate specimens
containing >50 % cancer cells. A recent study where choline metabolic
profiles in breast cancer xenograft models was investigated found
associations with differences in gene expression for basal-like vs. luminal-
like breast cancer [Moestue et al., 2010]. However, there are no such types of
prostate cancer.
Despite uncertainties regarding the exact function of choline metabolites its
increase is still a marker for tumors. This feature is valuable for tumor
verification and localization and may be used parallel with other bio-markers
such as inositol.
64
Chapter 8: Discussion
A few abnormal cells found in a small piece of prostate tissue are most
consequential for a man’s future.
As thoroughly discussed in this dissertation, the prostate is a very difficult
organ to diagnose [Chun et al., 2010; Colleselli et al., 2011] thus the concerns
about incorrect diagnosis and treatments are most valid. Prostate health
awareness, involving PSA-testing and biopsy, has increased the number of
early stage and localized PCa [Wolf et al., 2010; Wever et al., 2010].
Treatment options for this diagnosis are radical therapy such as surgery
and/or radiotherapy and brachytherapy where there are side effects such as
urinary and sexual dysfunctions. The alternative option is active surveillance
with the risk of under treatment but also the psychological burden involved.
Prostate sparing focal therapy is an alternative treatment option although its
effects are not determined yet [Lazzeri et al., 2010]. As PCa more often than
not is multifocal, focal therapy has a higher demand for increased biopsy
sensitivity and precise tumor localization [Meiers et al., 2007; Scheenen et
al., 2011]. Bio-markers with the power of accurately discriminating between
aggressive and indolent prostate tumors are most important as this diagnosis
will be the basis for therapy choice [Xu et al., 2010]. Therefore, innovative
methods to increase the precision of prostate diagnostic are of essence in the
field of prostate research. The ex-vivo and non-destructive method of
HRMAS NMR spectroscopy, in combination with histopathology, shows
promise in this area as it provides metabolomic information, both spectral
and morphologic, with the potential of being used as pre-clinical information
for the development of clinical diagnostic imaging methods for MRSI and
PET [Spratlin et al., 2009]. HRMAS NMR also holds the potential of being
used as a complement to clinical histopatological evaluations, although this
has to be investigated further [van Asten et al., 2008; Santos et al., 2010].
There are many positive aspects and strengths in this approach using
HRMAS NMR in combination with histopathological analysis as is presented
here. Firstly, this is a non-destructive method, thus detecting both lipophilic
and hydrophilic compound in their present form simultaneously and the
tissue is preserved for post-NMR analysis and verification under light
microscope. This strength is exploited in Paper I: “Detection of
polyunsaturated omega-6 fatty acid in human malignant prostate tissue by
1D and 2D high-resolution magic angle spinning NMR spectroscopy”,
where both fatty acids and small organic, water soluble compounds such as
citrate are discussed. Furthermore, Paper I presents the versatility of
HRMAS NMR where unexpected resonances in the spectra arising from
65
unknown compounds may be identified by various 2D methods. The
spectrum depicts the metabolism as it is and this is correlated with results
from histopathology, and thus metabolic profiling is possible. This offers the
characterization and visualization of the diverse metabolism in different
species, organs, anatomical regions, and different types of cells. This type of
characterization is presented in Paper II: “Detection of Local Prostate
Metabolites by HRMAS NMR Spectroscopy: A Comparative Study of
Human and Rat Prostate Tissues”. Such information is of key value when
designing experiments [Costello et al., 2006], especially in translational
research [Ruttenberg et al., 2007]. Paper II further discusses spectrally
derived bio-markers which are applicable on humans may not be suited for
experimental rodent models. HRMAS NMR detects cellular perturbations
due to disease vs. health, in other words; the dynamics of cellular
homeostasis. The loss of homeostasis, detected at an early stage, is an
important key in the understanding of disease [van der Greef, et al 2005].
This type of perturbation/loss is presented in Paper III: “1H HRMAS NMR
Derived Bio-markers Related to Tumour Grade, Tumour Cell Fraction, and
Cell Proliferation in Prostate Tissue Samples”, where it appears as the
homeostasis of non-malignant cells in the prostate, with tumors elsewhere in
the organ, is being disturbed. The key metabolite here is the common phyto-
nutrient inositol which apparently possesses protective properties [Vucenik
et al., 2003, 2006; Roy et al., 2009; Bacić et al., 2010] and is presently under
clinical trials investigations [www.ClinicalTrials.gov]. Thus, jointly with the
finding in Paper I regarding essential PUFA omega-6, HRMAS NMR
provides a window into the area of nutrition. This is of particular interest as
lifestyle choices, especially diet, have impact on prostate health and disease
[Moyad et al., 2008; Gonzales et al., 2010]. Thus, chemoprevention of
prostate cancer/disease using dietary means, and other preventative
measures, is a promising area in prostate research [Silberstein et al., 2010].
This approach, using HRMAS NMR in combination with subsequent
histopathology, is an excellent way of detecting the metabolome, however, it
cannot be stressed enough that this method, like with any other study
involving ex-vivo biological tissues, requires strict handling and a robust
study protocol as there are many possible short-comings. Biological tissues
without the enzymatic control and exposed to oxygen are at high risk of
oxidation and degradation. The time from the freezer to post-NMR handling
must be as short and efficient as possible to avoid metabolic break down and
steady, low temperature is of essence [Beckonert et al., 2010]. The shimming
of the NMR probe to generate a homogeneous magnetic field is equally
important as this affects the line-width and thus resolution which is critical
for line-fitting. Tuning and matching for the correct nucleus is equally
important factor to increase the signal-to-noise ratio [Kreis, 2004]. As both

66
shimming and tuning are manually adjusted it is important to decrease
operator dependent errors. This may be done by using the same operator for
all the experiments as we did in our study. Operator dependent errors should
also be considered when processing the spectra.
The results presented here are merely a fraction of what can be examined
using the metabolomic approach of HRMAS NMR spectroscopy combined
with histopathology.
67
Chapter 9: Suggestions for the Future
“Akufukuzae hakwambii toka”*
Swahili kanga writing
When reviewing my years involved in studying the prostate, I realize that the
most valuable knowledge has been gained simply by trials and errors. I have
also come to the conclusion, like many others, that this is a very complex,
highly multi-facetted, organ to study. It requires skills in many, widely,
separate areas such as, urology, pathology, chemistry, biology, radiology,
physics, statistics, demography, sociology, politics etc., and most
importantly, a thorough knowledge about the anatomy and function of both
human and experimental prostate models. This realization has made me
question the current approach of performing prostate cancer research (and
research in general), i.e., by separate entities of research groups specializing
in proprietary areas with very little, if any, intra-communication. This is
unfortunate since it is, simply, necessary in order to gain complete
understanding of this complex organ.
Interdisciplinary research is, however, becoming more popular and should
be highly encouraged. My one suggestion for the future is, therefore,
consequently, to encourage separate research groups to communicate and
share and discuss findings and not view conflicting results as intimidating
but as valuable information to be used for collective improvements that will
ultimately benefit the single most important factor – the patient.
*Inner feelings are mostly communicated through attitude and behavior and much less
through words.
68
Chapter 10: References
Abate-Shen C, Shen MM. Diagnostics: The prostate-cancer metabolome. Nature. 2009;457:799-800.
Afman L, Muller M. Nutrigenomics: From molecular nutrition to prevention of disease. J Am Diet Assoc. 2006;106:569–576.
Aigner F, Mitterberger M, Rehder P, Pallwein L, Junker D, Horninger W, Frauscher F. Status of transrectal ultrasound imaging of the prostate. J Endourol. 2010;24(5):685-691.
Akoka S, Barantin L, Trierweiler M. Concentration measurement by proton NMR using the ERETIC method. Anal Chem. 1999;71(13):2554–2557.
Albers MJ, Butler TN, Rahwa I, Bao N, Keshari KR, Swanson MG, Kurhanewicz J. Evaluation of the ERETIC method as an improved quantitative reference for 1H HR-MAS spectroscopy of prostate tissue. Magn Reson Med. 2009;61(3):525–532.
American Cancer Society. Cancer Prevention & Early Detection Facts & Figures 2010. Atlanta: American Cancer Society; 2010.
Andrew ER, A. Bradbury A, Eades RG. Removal of dipolar broadening of nuclear magnetic resonance spectra of solids by specimen rotation. Nature.1959;183:1802-1803.
Andriole GL. The lottery of conventional prostate biopsy. Nat Rev Urol. 2009;6:188-189.
Avril N, Dambha F, Murray I, Shamash J, Powles T, Sahdev A. The clinical advances of fluorine-2-D-deoxyglucose--positron emission tomography/computed tomography in urological cancers. Int J Urol. 2010;17(6):501-11.
Bacić I, Druzijanić N, Karlo R, Skifić I, Jagić S. Efficacy of IP6 + inositol in the treatment of breast cancer patients receiving chemotherapy: prospective, randomized, pilot clinical study. J Exp Clin Cancer Res. 2010;29:12.
Badawi AF, Liu Y, Eldeen MB, Morrow W, Razak ZR, Maradeo M, Badr MZ. Age-associated changes in the expression pattern of cyclooxygenase-2 and related apoptotic markers in the cancer susceptible region of rat prostate. Carcinogenesis. 2004;25(9):1681-1688.
Baron A, Migita T, Tang D, Loda M. Fatty acid synthase: a metabolic oncogene in prostate cancer? J Cell Biochem. 2004;91:47–53.
69
Bathen TF, Sitter B, Sjøbakk TE, Tessem MB, Gribbestad IS. Magnetic resonance metabolomics of intact tissue: a biotechnological tool in cancer diagnostics and treatment evaluation. Cancer Res. 2010;70(17):6692-6696.
Beare-Rogers J, Dieffenbacher A, Holm JV. Lexicon of lipid nutrition (IUPAC Technical Report). Pure Appl Chem. 2001;73(4): 685-744.
Beckonert B, Coen M, Keun HC, Wang Y, Ebbels T, Holmes E, Lindon JC, Nicholson JK. High-resolution magic-angle-spinning NMR spectroscopy for metabolic profiling of intact tissues. Nature Protocols. 2010;5:1019-1032.
Beckonert O, Keun HC, Ebbels TMD, Bundy J, Holmes E, Lindon JC, Nicholson JK. Metabolic profiling, metabolomic and metabonomic procedures for NMR spectroscopy of urine, plasma, serum and tissue extracts. Nat Protocols. 2007;2(11):2692–2703.
Berney DM, Fisher G, Kattan MW, Oliver TD, Scardino P, Foster CS, et al. (Trans-Atlantic Prostate Group). Major shifts in the treatment and prognosis of prostate cancer due to changes in pathological diagnosis and grading. BJU Int. 2007;100:1240-1244.
Bodenhausen G, Ruben DJ. Natural abundance nitrogen-15 NMR by enhanced heteronuclear spectroscopy. Chem Phys Lett. 1980;69:185-188.
Bouchelouche K, Turkbey B, Choyke P, Capala J. Imaging prostate cancer: an update on positron emission tomography and magnetic resonance imaging. Curr Urol Rep. 2010;11(3):180-190.
Braunschweiler L, Ernst RR. Coherence transfer by isotropic mixing: Application to proton correlation spectroscopy. J Magn Reson. 1983;53:521-528.
Brown SP, Spiess HW. Advanced solid-state NMR methods for the elucidation of structure and dynamics of molecular, macromolecular, and supramolecular systems. Chem Rev. 2001;101(12):4125-4156.
Buttyan R, Slawin K. Rodent models for targeted oncogenesis of the prostate gland. Cancer Metastasis Rev. 1993;12(1):11-19.
Chamberlain NF. Determining molecular structure by nuclear magnetic resonance of hydrogen. Anal Chem. 1959;31:56-77.
Cheng LL, Chang IW, Smith BL, Gonzalez RG. Evaluating human breast ductal carcinomas with high-resolution magic-angle spinning proton magnetic resonance spectroscopy. J Magn Reson. 1998;135(1):194-202.
Chun FK, Epstein JI, Shariat SF, Schröder FH, Scattoni V, et al. Optimizing performance and interpretation of prostate biopsy: a critical analysis of the literature. Eur Urol. 2010;58(6):851-864.
70
Coffey DS. Similarities of prostate and breast cancer: Evolution, diet, and estrogens. Urology. 2001;57(4,S1):31-38.
Colleselli D, Hennenlotter J, Schilling D, Krueger SA, Stenzl A, Schwentner C, et al. Impact of clinical parameters on the diagnostic accuracy of endorectal coil MRI for the detection of prostate cancer. Urol Int. 2011 (In press).
Conti F, Manganaro M, Miccheli A. Metabolomics and medical practice. Clin Ter. 2006;157(6):549-552.
Cooper JE, Farid I. The role of citric acid in the physiology of the prostate. A chromatographic study of citric acid cycle intermediates in benign and malignant prostatic tissue. J Surg Res. 1963;3:112–121.
Costello LC, Franklin RB. Citrate metabolism of normal and malignant prostate epithelial cells. Urology. 1997;50:3–12.
Costello LC, Franklin RB. Novel role of zinc in the regulation of prostate citrate metabolism and its implications in prostate cancer. Prostate. 1998;35(4):285-296.
Costello LC, Franklin RB, Narayan P. Citrate in the diagnosis of prostate cancer. Prostate. 1999;38(3)237-245.
Costello LC, Franklin RB. The intermediary metabolism of the prostate: a key to understanding the pathogenesis and progression of prostate malignancy. Oncology. 2000;59:269-282.
Costello LC, Franklin RB, Feng P. Mitochondrial function, zinc, and intermediary metabolism relationships in normal prostate and prostate cancer. Mitochondrion. 2005;5(3):143-153.
Costello LC, Franklin RB. ’Why do tumour cells glycolyse?’: From glycolysis through citrate to lipogenesis. Mol Cell Biochem. 2005;280(1–2):1–8.
Costello LC, Franklin RB. The clinical relevance of the metabolism of prostate cancer; zinc and tumor suppression: connecting the dots. Mol Cancer. 2006;5:17.
Costello LC, Franklin RB. Prostatic fluid electrolyte composition for the screening of prostate cancer: a potential solution to a major problem. Prostate Cancer Prostatic Dis. 2009;12:17–24.
Cunnane SC, Ryan MA, Nadeau CR, Bazinet RP, Musa-Veloso K, McCloy U. Why is carbon from some polyunsaturates extensively recycled into lipid synthesis? Lipids. 2003;38(4):477.
Cunnane SC. Problems with essential fatty acids: time for a new paradigm? Prog Lipid Res. 2003;42(6):544-568.
71
Cupp MR, Oesterling JE. Prostate-specific antigen, digital rectal examination, and transrectal ultrasonography: their roles in diagnosing early prostate cancer. Mayo Clin Proc. 1993;68(3):297-306.
Davis CD, Milner J. Frontiers in nutrigenomics, proteomics, metabolomics and cancer prevention. Mutat Res. 2004;551:51–64.
De Marzo AM, Platz EA, Sutcliffe S, Xu J, Grönberg H, Drake CG, Nakai Y, Isaacs WB, Nelson WG. Inflammation in prostate carcinogenesis. Nat Rev Cancer. 2007;7(4):256-269.
De Visschere P, Oosterlinck W, De Meerleer G, Villeirs G. Clinical and imaging tools in the early diagnosis of prostate cancer, a review. JBR-BTR. 2010;93(2):62-70.
Epstein JI. Diagnosis and reporting of limited adenocarcinoma of the prostate on needle biopsy. Modern Pathology. 2004;17:307–315.
Epstein JI. An update of the Gleason grading system. J Urol. 2010;183(2):433-440.
Ernst RR, Bodenhausen G, Wokaun A. Principles of Nuclear Magnetic Resonance in One and Two Dimensions. Oxford University Press, NY, USA. 1987. ISBN-0-19-855647-0.
Fair WR, Couch J, Wehner N. Prostatic antibacterial factor. Identity and significance. Urology. 1976;7(2):169-177.
Fair WR, Parrish RF. Antibacterial substances in prostatic fluid. Prog Clin Biol Res. 1981;75A:247-264.
Fardet A. New hypotheses for the health-protective mechanisms of whole-grain cereals: what is beyond fibre? Nutr Res Rev. 2010;23(1):65-134.
Fiehn O, Kopka J, Dormann P, Altmann T, Trethewey RN, Willmitzer L. Metabolite profiling for plant functional genomics. Nature Biotechnology. 2000;18(11):1157-1161.
Fleshner N, Klotz L. Role of ”saturation biopsy” in the detection of prostate cancer among difficult diagnostic cases. Urology. 2002;60:93-97.
Fradet V, Cheng I, Casey G, Witte JS. Dietary omega-3 fatty acids, cyclooxygenase-2 genetic variation, and aggressive prostate cancer risk. Clin Cancer Res. 2009;15(7):2559-2566.
Franklin RB, Feng P, Milon B, et al. hZIP1 zinc uptake transporter down regulation and zinc depletion in prostate cancer. Mol Cancer 2005;4:32.
Fry CG. The Nobel Prize in Medicine for Magnetic Resonance Imaging. J Chem Educ. 2004;81(7)922.
72
Funk CD. Prostaglandins and leukotrienes: advances in eicosanoid biology. Science. 2001;294(5548):1871-1875.
German JB, Hammock BD, Watkins SM. Metabolomics: building on a century of biochemistry to guide human health. Metabolomics. 2005;1:3–9.
Gibbs RA, Weinstock GM, Metzker ML, Muzny DM et al. Genome sequence of the Brown Norway rat yields insights into mammalian evolution. Nature. 2004;428(6982):493-521.
Gibney MJ, Walsh M, Brennan L, Roche HM, German B, van Ommen B. Metabolomics in human nutrition: opportunities and challenges. Am J Clin Nutr. 2005;82:497–503.
Gillies RJ, Morse DL. In vivo magnetic resonance spectroscopy in cancer. Annu Rev Biomed Eng. 2005;7:287-326.
Giusti S, Caramella D, Fruzzetti E, Lazzereschi M, Tognetti A, Bartolozzi C. Peripheral zone prostate cancer. Pre-treatment evaluation with MR and 3D (1)H MR spectroscopic imaging: correlation with pathologic findings. Abdom Imaging. 2010;35(6):757-763.
Gleason DF, Mellinger GT. Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical staging. J Urol. 1974;111:58–64.
Gonzales CA, Riboli E. Diet and cancer prevention: Contributions from the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Eur J Cancer. 2010;46(14):2555-2562.
Goodacre R. Metabolomics of a superorganism 1–3. J Nutr. 2007;137:259S–266S.
Griffin JL, Shockcor JP. Metabolic profiles of cancer cells. Nat Rev Cancer. 2004;4(7):551–561.
Häggström S, Wikström P, Bergh A, Damber JE. Expression of vascular endothelial growth factor and its receptors in the rat ventral prostate and the Dunning R3327-PAP adenocarcinoma before and after castration. Prostate. 1998;36:71-79.
Hahn WC. Experimental models of human cancer. Cell Cycle. 2004;3(5):604-605.
Hayashi N, Sugimura Y, Kawamura J, Donjacour AA, Cunha GR. Morphological and functional heterogeneity in the rat prostatic gland. Biol Reprod. 1991;45(2):308-321.
Hoedemaeker RF, Vis AN, Van Der Kwast TH. Staging prostate cancer. Microsc Res Tech. 2000;51(5):423-429.
73
Holmes E, Loo RL, Stamler J, Bictash M, Yap IKS, Chan Q, Ebbels T, Nicholson JK, Elliott P. Human metabolic phenotype diversity and its association with diet and blood pressure. Nature. 2008;453:396-400.
Hsu PP, Sabatini DM. Cancer cell metabolism: Warburg and beyond. Cell. 2008;134:703-707.
Inouye M, Kettunen J, Soininen P, Silander K, Ripatti S, Kumpula LS, Peltonen L. Metabonomic, transcriptomic, and genomic variation of a population cohort. Molecular Systems Biology. 2010;6:441.
Jacobsen NE. NMR Spectroscopy Explained: Simplified Theory, Applications and Examples for Organic Chemistry and Structural Biology. 2007. John Wiley & Sons, Inc. Hoboken, NJ, USA.
Jadvar H. Prostate Cancer: PET with 18F-FDG, 18F- or 11C-Acetate, and 18F or 11C-Choline. J Nucl Med. 2011;52(1):81–89.
Jambor I, Borra R, Kemppainen J, Lepomäki V, Aronen HJ, Minn H, et al. Functional imaging of localized prostate cancer aggressiveness using 11C-acetate PET/CT and 1H-MR spectroscopy. J Nucl Med. 2010;51(11):1676-1683.
Jara M, Carballada R, Esponda P. Age-induced apoptosis in the male genital tract of the mouse. Reproduction. 2004;127:359-366.
Johannsen W. The genotype conception of heredity. American Naturalist. 1911;45:129-159.
Kamb A. What's wrong with our cancer models? Nat Rev Drug Discov. 2005;4(2):161-165.
Kavanagh JP. Sodium, potassium, calcium, magnesium, zinc, citrate and chloride content of human prostatic and seminal fluid. J Reprod Fert. 1985;75:35-41.
Kelavkar U, Lin Y, Landsittel D, Chandran U, Dhir R. The yin and yang of 15-lipoxygenase-1 and delta-desaturases: Dietary omega-6 linoleic acid metabolic pathway in prostate. J Carcinog. 2006;5:9.
Kelavkar UP, Hutzley J, McHugh K, Allen KG, Parwani A. Prostate tumor growth can be modulated by dietarily targeting the 15-lipoxygenase-1 and cyclooxygenase-2 enzymes. Neoplasia. 2009;11(7):692-699.
Kelloff GJ, Choyke P, Coffey DS. Challenges in clinical prostate cancer: role of imaging. AJR. 2009;192:1455-1470.
Khan N, Afaq F, Mukhtar H. Lifestyle as risk factor for cancer: Evidence from human studies. Cancer Lett. 2010;293(2):133-143.
74
Kim J, Dang CV. Cancer’s molecular sweet tooth and the Warburg effect. Cancer Res. 2006;66(18)8927-8930.
Kirby RS. The natural history of benign prostatic hyperplasia: what have we learned in the last decade? Urology. 2000;56(5,S1):3-6.
Klijn S, De Visschere PJ, De Meerleer GO, Villeirs GM. Comparison of qualitative and quantitative approach to prostate MR spectroscopy in peripheral zone cancer detection. Eur J Radiol 2011 (in print).
Koulman A, Volmer DA. Perspectives for metabolomics in human nutrition: an overview. Nutrition Bulletin. 2008;33(4):324–330.
Kraus TS, Cohen C, Siddiqui MT. Prostate-specific antigen and hormone receptor expression in male and female breast carcinoma. Diagn Pathol. 2010;5:63.
Krebs HA. The citric acid cycle and the Szent-Györgyi cycle in pigeon breast muscle. Biochem J. 1940;34(5):775-779.
Kreis R. Issues of spectral quality in clinical 1H-magnetic resonance spectroscopy and a gallery of artifacts. NMR Biomed. 2004;17:361-381.
Kurhanewicz J, Swanson MG, Nelson SJ, Vigneron DB. Combined magnetic resonance imaging and spectroscopic imaging approach to molecular imaging of prostate cancer. J Magn Reson Imaging. 2002;16:451-463.
Lamb DJ, Zhang L. Challenges in prostate cancer research: animal models for nutritional studies of chemoprevention and disease progression. J Nutr. 2005;135(12):3009S-3015S.
Larson PEZ, Bok R, Kerr AB, Lustig M, Kurhanewicz J, Vigneron DB, et al. Investigation of tumor hyperpolarized [1-13C]-pyruvate dynamics using time-resolved multiband RF excitation echo-planar MRSI. Magn Reson Med. 2010;63(3):582–591.
Lash TD, Shirkey Lash S. The use of Pascal-like triangles in describing first order NMR coupling patterns. J Chem Educ. 1987;64(4):315.
Lazzeri M, Guazzoni G. Focal therapy meets prostate cancer. Lancet. 2010;376(9746):1036-1037.
Liney GP, Lowry M, Turnbull LW, Manton DJ, Knowles AJ, Blackband SJ, Horsman A. Proton MR T2 maps correlate with the citrate concentration in the prostate. NMR Biomed. 1996;9(2):59-64.
Lissbrant IF, Hammarsten P, Lissbrant E, Ferrara N, Häggström Rudolfsson S, Bergh A. Neutralizing VEGF bioactivity with a soluble chimeric VEGF-receptor protein flt(1-3)IgG inhibits testosterone-stimulated prostate growth in castrated mice. Prostate. 2004;58:57–65.
75
Lucia SM, Bostwick DG, Bosland M, Cockett ATK, Knapp DW, Watkins BA, et al. Workgroup 1: Rodent models of prostate cancer. Prostate. 1998;36:49-55.
Maas WE, Laukien FH, Cory DG. Gradient, High Resolution, Magic Angle Sample Spinning NMR. J Am Chem Soc.1996;118(51):13085–13086.
Madu CO, Lu Y. Novel diagnostic bio-markers for prostate cancer. J Cancer. 2010;1:150-177.
Mann T. Secretory function of the prostate, seminal vesicle and other male accessory organs of reproduction. J Reprod Fert. 1974;37:179-188.
Martin GE, Zekter AS. Two-Dimensional NMR Methods for Establishing Molecular Connectivity. 1988. John Wiley & Sons, Inc. NY, USA.
Mathews CK, van Holde KE, G. Ahern KG. Biochemistry. 3rd Edition, 2000. Addison Wesley Longman, Inc. San Francisco, Ca, USA.
Mawson CA, Fischer MI. The occurrence of zinc in the human prostate gland. Can J Med Sci. 1952;30:336–339.
McEntee MF, Carol Ziegler C, Reel D, Tomer K, Ahmed Shoieb A, Lih FB, O’Rourke D, Whela J. Dietary n-3 polyunsaturated fatty acids enhance hormone ablation therapy in androgen-dependent prostate cancer. Am J Pathol. 2008;173:229–241.
McLaughlin PW, Troyer S, Berri S, Narayana V, Meirowitz A, Roberson PL, Montie J. Functional anatomy of the prostate: implications for treatment planning. Int J Radiat Oncol Biol Phys. 2005;63(2):479-491.
McLean MA, Barrett T, Gnanapragasam VJ, Priest AN, Joubert I, Lomas DJ, Neal DE, Griffiths JR, Sala E. Prostate cancer metabolite quantification relative to water in 1H-MRSI in vivo at 3 Tesla. Magn Reson Med. 2010 (In print).
McMahon CJ, Bloch BN, Lenkinski RE, Rofsky NM. Dynamic contrast-enhanced MR imaging in the evaluation of patients with prostate cancer. Magn Reson Imaging Clin N Am. 2009;17(2):363-383.
McNeal JE. The zonal anatomy of the prostate. Prostate. 1981;2(1):35-49.
Mehr K, John B, Russell D Avizonis D. Electronic referencing techniques for quantitative NMR: pitfalls and how to avoid them using amplitude-corrected referencing through signal injection. Anal Chem. 2008;80(21):8320–8323.
Meiboom S, Gill D. Modified spin-echo method for measuring nuclear relaxation times. Rev. Sci. Instrum. 1958;29:688-691.

76
Meiers I, Waters DJ, Bostwick DG. Preoperative prediction of multifocal prostate cancer and application of focal therapy: review 2007. Urology. 2007;70(6S):3-8.
Middleton DA, Bradley DP, Connor SC, Mullins PG, Reid DG. The effect of sample freezing on proton magic-angle spinning NMR spectra of biological tissue. Magn Reson Med. 1998;40(1):166–169.
Moestue S, Sitter B, Bathen TF, Tessem MB, Gribbestad IS. HR MAS MR spectroscopy in metabolic characterization of cancer. Curr Top Med Chem. 2011;11(1):2-26.
Moestue SA, Sitter B, Børresen-Dale AL, Engebraaten O, Gribbestad IS, et al. Distinct choline metabolic profiles are associated with differences in gene expression for basal-like and luminal-like breast cancer xenograft models. BMC Cancer. 2010;10:433.
Moyad MA, Lowe FC. Educating patients about lifestyle modifications for prostate health. Am J Med. 2008;121(8,S2):S34-42.
Nastiuk KL, Liu H, Mark Hamamura M, Muftuler LT, Orhan Nalcioglu O, and John J Krolewski JJ. In vivo MRI volumetric measurement of prostate regression and growth in mice. BMC Urology. 2007;7:12.
Nicholson JK, Lindon JC, Holmes E. 'Metabonomics': understanding the metabolic responses of living systems to pathophysiological stimuli via multivariate statistical analysis of biological NMR spectroscopic data. Xenobiotica. 1999;29(11):1181-1189.
Nicholson JK, Lindon JC. Systems biology: Metabonomics. Nature. 2008;455(7216):1054-1056.
Nordström A, Lewensohn R. Metabolomics: moving to the clinic. J Neuroimmune Pharmacol. 2010;5(1):4-17.
Oesterling JE. Prostate specific antigen: a critical assessment of the most useful tumor marker for adenocarcinoma of the prostate. J Urol. 1991;145(5):907-923.
Ornish D, Magbanua MJM, Shinohara K, Haqq CM, Carroll PR, et al. Changes in prostate gene expression in men undergoing an intensive nutrition and lifestyle intervention. Proc Natl Acad Sci USA. 2008;105(24):8369–8374.
Paner GP, Luthringer Dj, Amin MB. Best practice in diagnostic immunohistochemistry. Prostate carcinoma and its mimics in needle core biopsies. Arch Pathol Lab Med. 2008;132:1388-1396.
Pople JA, Schneider WG, Bernstein HJ. High-Resolution Nuclear Magnetic Resonance. 1959. McGraw-Hill, NY, USA.

77
Rajinikanth A, Manoharan M, Soloway CT, Civantos FJ, Soloway MS. Trends in Gleason score: concordance between biopsy and prostatectomy over 15 years. Urology. 2008;72(1):177-182.
Reese AC, Sadetsky N, Carroll PR, Cooperberg MR. Inaccuracies in assignment of clinical stage for localized prostate cancer. Cancer. 2011;15(117):283-289.
Roy S, Gu M, Ramasamy K, Singh RP, Agarwal C, Siriwardana S, Sclafani RA, Agarwal R. p21/Cip1 and p27/Kip1 Are essential molecular targets of inositol hexaphosphate for its antitumor efficacy against prostate cancer. Cancer Res. 2009;69(3):1166-73.
Roy-Burman P, Wu H, Powell WC, Hagenkord J, Cohen MB. Genetically defined mouse models that mimic natural aspects of human prostate cancer development. Endocr Relat Cancer. 2004;11:225–254.
Ruttenberg A, Clark T, Bug W, Samwald M, Bodenreider O, Herman I, Cheung KH, et al. Advancing translational research with the Semantic Web. BMC Bioinformatics. 2007;8(S3):S2.
Rysman E, Brusselmans K, Vanderhoydonc F, Smans K, Waelkens E, Verhoeven G, Swinnen JV, et al. De novo lipogenesis protects cancer cells from free radicals and chemotherapeutics by promoting membrane lipid saturation. Cancer Res. 2010;70(20):8117-8126.
Santos CF, Kurhanewicz J, Tabatabai ZL, Carroll PR, Ha CM, Swanson MG, et al. Metabolic, pathologic, and genetic analysis of prostate tissues: quantitative evaluation of histopathologic and mRNA integrity after HR-MAS spectroscopy. NMR Biomed. 2010;23(4):391-398.
Scheenen TW, Fütterer J, Weiland E, van Hecke P, Roell S, Heerschap A, et al. Discriminating cancer from noncancer tissue in the prostate by 3-Dimensional proton magnetic resonance spectroscopic imaging. A prospective multicenter validation study. Invest Radiol. 2011;46(1):25-33.
Schröder FH, Hugosson J, Roobol MJ, Tammela TLJ, Ciatto S, Nelen V, Auvinen A. Screening and prostate-cancer mortality in a randomized european study. N Engl J Med. 2009;360:1320-1328.
Seibert K, Zhang Y, Leahy K, Hauser S, Masferrer J, Perkins W, Lee L, Isakson P. Pharmacological and biochemical demonstration of the role of cyclooxygenase 2 in inflammation and pain. Proc Natl Acad Sci USA. 1994;91(25):12013-12017.
Sharma S, Shin JS, Grimshaw M, Clarke RA, Lee CS. The senescence pathway in prostatic carcinogenesis. Pathology. 2010;42(6):507-511.
78
Shirai T, Takahashi S, Cui L, Futakuchi M, Kato K, Tamano S, Imaida K. Experimental prostate carcinogenesis - rodent models. Mutat Res. 2000;462(2-3):219-226.
Silberstein JL, Parsons JK. Prostate cancer prevention: concepts and clinical recommendations. Prostate Cancer Prostatic Dis. 2010;13(4):300-306.
Simopoulos AP. Genetic variants in the metabolism of omega-6 and omega-3 fatty acids: their role in the determination of nutritional requirements and chronic disease risk. Exp Biol Med (Maywood). 2010;235(7):785-795.
Singh KK, Desouki MM, Franklin RB, Costello LC. Mitochondrial aconitase and citrate metabolism in malignant and nonmalignant human prostate tissues. Mol Cancer. 2006;5:14.
Sitter B, Bathen TF, Tessem MB, Gribbestad IS. High-resolution magic angle spinning (HR MAS) MR spectroscopy in metabolic characterization of human cancer. Prog Nucl Mag Res Sp. 2009;54(3-4):239-254.
Soubias O, Piottob M, Saurela O, Assematb O, Réata V. Milon A. Detection of natural abundance 1H–13C correlations of cholesterol in its membrane environment using a gradient enhanced HSQC experiment under high resolution magic angle spinning. J Magn Reson. 2003;165(2):303-308.
Spratlin JL, Serkova NJ, Eckhardt GS. Clinical applications of metabolomics in oncology: a review. Clin Canc Res. 2009;15(2):431-440.
Swanson MG, Vigneron DB, Tabatabai ZL, Males RG, Schmitt L, Carroll PR, James JK, Hurd RE, Kurhanewicz J. Proton HR-MAS spectroscopy and quantitative pathologic analysis of MRI/3D-MRSI targeted post-surgical prostate tissues. Magn Reson Med. 2003;50(5):944–954.
Swanson MG, Zektzer AS, Tabatabai ZL, Simko J, Jarso S, Keshari KR, Schmitt L, Carroll PR, Shinohara K, Vigneron DB, Kurhanewicz J. Quantitative analysis of prostate metabolites using 1H HR-MAS spectroscopy. Magn Reson Med. 2006;55(6):1257–1264.
Swindle P, McCredie S, Russell P, Himmelreich U, Khadra M, Lean C, Mountford C. Pathologic characterization of human prostate tissue with proton MR spectroscopy. Radiology. 2003;228:144-151.
Swindle P, Ramadan S, Stanwell P, McCredie S, Russell P, Mountford C Proton magnetic resonance spectroscopy of the central, transition and peripheral zones of the prostate: assignments and correlation with histopathology. Magn Reson Mater Phy. 2008;21:423-434.
Swinnen JV, Vanderhoydonc F, Heyns W, Verhoeven G, et al. Selective activation of the fatty acid synthesis pathway in human prostate cancer. Int J Cancer. 2000;88(2):176-179.

79
Tessem MG, Swanson MG, Nelson SJ, Vigneron DB, Gribbestad IS, Kurhanewicz J, et al. Evaluation of lactate and alanine as metabolic bio-markers of prostate cancer using 1H HR-MAS spectroscopy of biopsy tissues. Magn Reson Med. 2008;60(3):510–516.
The Nobel Prizes. Nobelprize.org.2010. http://nobelprize.org/nobel_prizes/
Thoeny HC, Triantafyllou M, Vermathen P, Studer UE, et al. Combined ultrasmall superparamagnetic particles of iron oxide–enhanced and diffusion-weighted magnetic resonance imaging reliably detect pelvic lymph node metastases in normal-sized nodes of bladder and prostate cancer patients. Eur Urol. 2009;55(4):761-769.
Thomas AM, Lange T, Velan SS, Nagarajan R, Raman S, Boesiger p, et al. Two-dimensional MR spectroscopy of healthy and cancerous prostate in vivo. MAGMA. 2008;21(6):443-458.
Thun MJ, DeLancey JO, Center MM, Jemal A, Ward EM. The global burden of cancer: priorities for prevention. Carcinogenesis. 2010;31(1):100-110.
Trujillo E, Davis C, Milner J. Nutrigenomics, proteomics, metabolomics,and the practice of dietetics. J Am Diet Assoc. 2006;106:403–413.
Turkbey B, Xu S, Kruecker J, Locklin J, Pinto PA. Documenting the location of prostate biopsies with image fusion. BJU International. 2011;107(1):53–57.
Ukimura O, Hung AJ, Gill IS. Innovations in prostate biopsy strategies for active surveillance and focal therapy. Curr Opin Urol. 2011;21(2):115-120.
Ukoli FA, Fowke JH, Akumabor P, Oguike T, Taher KA, et al. The association of plasma fatty acids with prostate cancer risk in African Americans and Africans. J Health Care Poor Underserved. 2010;21(1S):127-147.
van Asten J, Cuijpers V, Hulsbergen-van de Kaa C, Soede-Huijbregts C, Witjes JA, Verhofstad A, Heerschap A. High resolution magic angle spinning NMR spectroscopy for metabolic assessment of cancer presence and Gleason score in human prostate needle biopsies. Magn Reson Mater Phy. 2008;21:435-442.
van der Greef J, Smilde AK. Symbiosis of chemometrics and metabolomics: past, present, and future. J Chemometrics. 2005;19:376–386.
Van Dyke Tiers G. Reliable proton nuclear resonance shielding values by
“Internal Referencing” with Tetramethyl-silane. J PhysChem.
1958;62(9):1151–1152.
Vickers AJ, Till C, Tangen CM, Lilja H, Thompson IM. An empirical evaluation of guidelines on prostate-specific antigen velocity in prostate cancer detection. J Natl Cancer Inst. 2011;103:1–8.
80
Villers A, Steg A, Boccon-Gibod L. Anatomy of the prostate: review of the different models. Eur Urol.1991;20(4):261-268.
Vucenik I, Shamsuddin AM. Cancer inhibition by inositol hexaphosphate (IP6) and inositol: from laboratory to clinic. J Nutr. 2003;133(11,S1):3778S-3784S.
Vucenik I, Shamsuddin AM. Protection against cancer by dietary IP6 and inositol. Nutr Cancer. 2006;55(2):109-125.
Warburg O. On the origin of cancer cells. Science. 1956;123:309-314.
Weidner AM, Michaely HJ, Lemke A, Breitinger L, Wenz F, Marx A, Schoenberg SO, Dinter DJ. Value of multiparametric prostate MRI of the peripheral zone. Z Med Phys. 2011 (in print).
Wever EM, Draisma G, Heijnsdijk EA, Roobol MJ, Boer R, Otto SJ, de Koning HJ. Prostate-specific antigen screening in the United States vs in the European Randomized Study of Screening for Prostate Cancer-Rotterdam. J Natl Cancer Inst. 2010;102(5):352-355.
Wishart DS, Tzur D, Knox C, Eisner R, Guo AC, Young N, et al. HMDB: the Human Metabolome Database. Nucl. Acids Res. 2007;35(S1):D521-D526.
Wolf AMD, Wender RC, Etzioni RB, Thompson IM, D’Amico AV, et al. American Cancer Society guideline for the early detection of prostate cancer. CA Cancer J Clin. 2010;60:70–98.
Wu CL, Taylor JL, He WL, Zepeda AG, Halpern EF, Bielecki A, Gonzalez RG, Cheng LL. Proton high-resolution magic angle spinning NMR analysis of fresh and previously frozen tissue of human prostate. Magn Reson Med. 2003;50(6):1307–1311.
Xu J, Zheng SL, Isaacs SD, Wiley KE, Wiklund F, Grönberg H, Isaacs WB. Inherited genetic variant predisposes to aggressive but not indolent prostate cancer. Proc Natl Acad Sci U S A. 2010;107(5):2136-2140.
Zaichick VY, Sviridova TV, Zaichick SV. Zinc concentration in human prostatic fluid: normal, chronic prostatitis, adenoma and cancer. Int Urol Nephrol. 1996;28:687–694.
Zakian KL, Sircar K, Hricak H, Chen H-N, Shukla-Dave A, Eberhardt S. Correlation of proton MR spectroscopic imaging with Gleason score based on step-section pathologic analysis after radical prostatectomy. Radiology. 2005;234:804-814.