problems coagulation disorders - journal of clinical...
TRANSCRIPT

J. clin. Path., 29, Suppl. (Roy. Coll. Path.), 10, 35-41
Haematological problems
Coagulation disordersJOHN BONNAR
From University of Dublin Trinity College Unit, Rotunda Hospital, Dublin
The risk of severe haemorrhage in pregnancy is wellrecognized, and uncontrolled bleeding remains amajor cause of maternal death throughout theworld, including the British Isles. The haemochorialsystem of human placentation carries with it aninherent risk of haemorrhage and this probablyexplains why the serious congenital disorders ofhaemostasis are predominantly found in the male.In pregnancy, complex physiological changes occurin the systems responsible for the control of bloodloss from the vascular tree.
Coagulation and Fibrinolysis during Normal Pregnancy
COAGULATION SYSTEMThe effect of pregnancy on the clotting factors can bedetected from as early as the first trimester. Plasmafibrinogen gradually increases and levels rangingbetween 400 mg and 600 mg per cent are usuallypresent in late pregnancy and labour. This elevationof fibrinogen is much greater than occurs in womentaking high doses of oestrogen and progestationalsteroids, and is thus not explained by the effect ofthese hormones. Factors VII and X likewise show adefinite increase and in the third trimester are usuallyin the range 120-180 per cent. Cold-promotedactivation of factor VII when the plasma is exposedto low temperatures for almost 20 hours is a pheno-menon which can readily be shown in the plasma ofpregnant women and in women using oestrogen/progestogen contraception; factor VII activity isenhanced as much as ten-fold and activation may bemediated through the kallikrein system (Gj0nnaess,1973).Factor VIII, as measured by two-stage techniques,
has an average value of around 200 per cent in latepregnancy, with a range from 80 to 450 per cent.During pregnancy, Bennett and Ratnoff (1972) foundthat factor VIII-related antigen (factor VIlI-RA)increased in proportion to factor VIII activity, butour own investigation and that of Bouma et al(1973) showed that the ratio of factor VIII-RA tofactor VIII activity, as measured by a clotting assay,
slightly increased during pregnancy and the ratiowas considerably higher in patients with severe pre-eclampsia. An increase of factor VIII activity duringpregnancy has also been noted in women withcongenital deficiency of factor VIII, as found in somecarriers of classical haemophilia and in Von Wille-brand's disease. Postpartum haemorrhage is acommon complication in women severely affected bythese congenital deficiencies, particularly where thefactor VIII level is seriously depressed and does notincrease during pregnancy. In such patients, theadministration of factor VIII concentrates or freshplasma before delivery and during the first three orfour days of the puerperium will obviate the risk ofuterine haemorrhage.
Several authors have reported slight elevations offactor IX during pregnancy. Studies on factor XIreported a decrease during pregnancy, with averagelevels between 60 and 70 per cent (Nossel et al, 1966).The level of fibrin-stabilizing factor (factor XIII) wasinvestigated by Coopland et al (1969) and a gradualdecrease was found during pregnancy with the levelsfalling to about 50 per cent at term. An increase inthe level of factor XII and a decrease in antithrombinIII was reported by Biland and Duckert (1973); in theauthor's laboratory a small decrease in the levels ofcoagulation inhibitors, antithrombin III and anti-factor Xa were found during normal pregnancy.
FIBRINOLYTIC ENZYME SYSTEMProfound changes occur in the components of thefibrinolytic enzyme system during pregnancy. Thelevel of plasminogen substantially increases and therise appears to parallel that of fibrinogen (Bonnaret al, 1969b). Fibrinolytic activity in plasma alsodecreases markedly during pregnancy, and Astedt(1972) found that the high fibrinolytic activity whichnormally occurs in blood in response to venousocclusion diminished progressively during pregnancy.In vein biopsies during pregnancy Astedt (1972)found that the fibrinolytic activity in the vessel wallsdecreased significantly. The placenta has been shownto contain inhibitors which block urokinase-induced
35
on 20 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.s3-10.1.35 on 1 January 1976. Dow
nloaded from
36
fibrinolysis (Kawano et al, 1968; Uszynski andAbildgaard, 1971).
FIBRIN/FIBRINOGEN DEGRADATION PRODUCTS(FDP) AND SOLUBLE COMPLEXESAn increase of FDP in parallel with gestation wasreported by Woodfield and colleagues (1968), butin other studies no consistent increase was found inhealthy pregnancy or was shown to occur in only aproportion of pregnant women (Bonnar et al, 1969a;van Royen, 1974). Hedner and Astedt (1970)investigated FDP levels in serum and urine of 1000women in the third trimester. None of the womenhad FDP in the urine and of 99 who had increasedFDP levels in the serum 85 per cent had conditionssuch as preeclampsia, hepatitis and Rh-immuniza-tion.
In a recent study, McKillop et al (1976) reportedsignificantly increased concentrations of solublefibrin/fibrinogen complexes during normal pregnancywhen compared with age-matched non-pregnantcontrols. In our studies of heparin tolerance duringpregnancy we also found that when heparin was
0-25 14 weeks 22 weeks
5000unitsSC 10000 units SCv
E 0-20
-E 0-15-
' O.
0
04
I
35 weeksiO 000 units SC
05
0 2 4 60 i 2i
6 8
Time (hours)
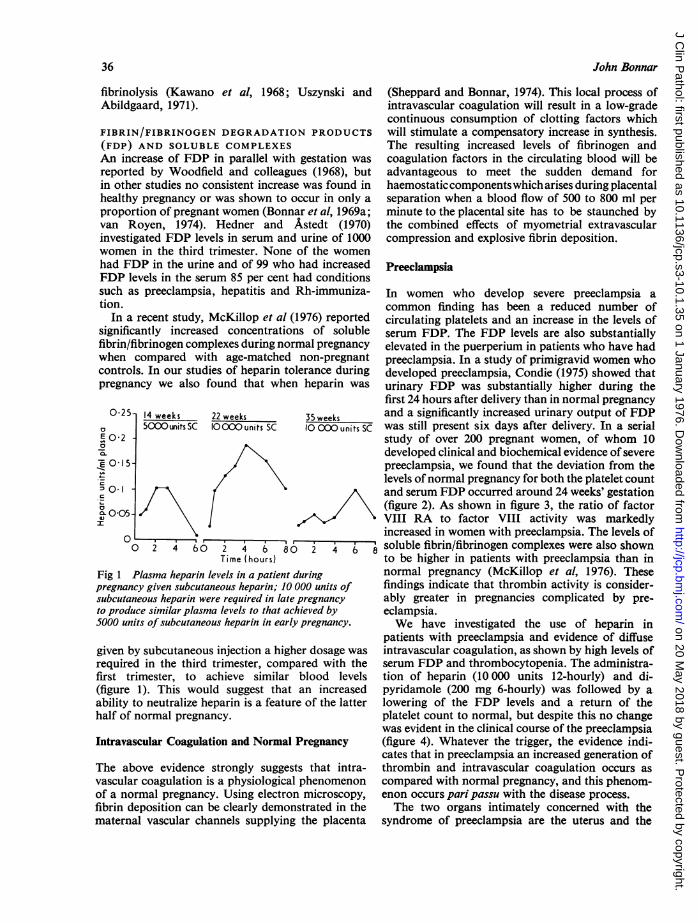
Fig 1 Plasma heparin levels in a patient duringpregnancy given subcutaneous heparin; 10 000 units ofsubcutaneous heparin were required in late pregnancyto produce similar plasma levels to that achieved by5000 units of subcutaneous heparin in early pregnancy.
given by subcutaneous injection a higher dosage was
required in the third trimester, compared with thefirst trimester, to achieve similar blood levels(figure 1). This would suggest that an increasedability to neutralize heparin is a feature of the latterhalf of normal pregnancy.
Intravascular Coagulation and Normal Pregnancy
The above evidence strongly suggests that intra-vascular coagulation is a physiological phenomenonof a normal pregnancy. Using electron microscopy,fibrin deposition can be clearly demonstrated in thematernal vascular channels supplying the placenta
John Bonnar
(Sheppard and Bonnar, 1974). This local process ofintravascular coagulation will result in a low-gradecontinuous consumption of clotting factors whichwill stimulate a compensatory increase in synthesis.The resulting increased levels of fibrinogen andcoagulation factors in the circulating blood will beadvantageous to meet the sudden demand forhaemostaticcomponentswhich arises during placentalseparation when a blood flow of 500 to 800 ml perminute to the placental site has to be staunched bythe combined effects of myometrial extravascularcompression and explosive fibrin deposition.
Preeclampsia
In women who develop severe preeclampsia acommon finding has been a reduced number ofcirculating platelets and an increase in the levels ofserum FDP. The FDP levels are also substantiallyelevated in the puerperium in patients who have hadpreeclampsia. In a study of primigravid women whodeveloped preeclampsia, Condie (1975) showed thaturinary FDP was substantially higher during thefirst 24 hours after delivery than in normal pregnancyand a significantly increased urinary output of FDPwas still present six days after delivery. In a serialstudy of over 200 pregnant women, of whom 10developed clinical and biochemical evidence of severepreeclampsia, we found that the deviation from thelevels ofnormal pregnancy for both the platelet countand serum FDP occurred around 24 weeks' gestation(figure 2). As shown in figure 3, the ratio of factorVIII RA to factor VIII activity was markedlyincreased in women with preeclampsia. The levels ofsoluble fibrin/fibrinogen complexes were also shownto be higher in patients with preeclampsia than innormal pregnancy (McKillop et al, 1976). Thesefindings indicate that thrombin activity is consider-ably greater in pregnancies complicated by pre-eclampsia.We have investigated the use of heparin in
patients with preeclampsia and evidence of diffuseintravascular coagulation, as shown by high levels ofserum FDP and thrombocytopenia. The administra-tion of heparin (10000 units 12-hourly) and di-pyridamole (200 mg 6-hourly) was followed by alowering of the FDP levels and a return of theplatelet count to normal, but despite this no changewas evident in the clinical course of the preeclampsia(figure 4). Whatever the trigger, the evidence indi-cates that in preeclampsia an increased generation ofthrombin and intravascular coagulation occurs ascompared with normal pregnancy, and this phenom-enon occurs pari passu with the disease process.The two organs intimately concerned with the
syndrome of preeclampsia are the uterus and the
0
on 20 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.s3-10.1.35 on 1 January 1976. Dow
nloaded from

Coagulation disorders
Platelet countE 300.
x
200-
0
100-
is-
-E
o- 10-0
E
%le 5-
Non- 16 24 30 34pregnant Gestation (weeks)
Fig 2 Comparison of the levels of serum,fibrinogen degradation products (FDP) anccount in 10 pregnant women who developeipreeclampsia, compared with 20 women wZnormalpregnancy (mean + standard error
Normal preqnoncyMean and ronqe
x Pre-eclampsia
I0
8 12 16Gestation (weeks)
x
x
It
20 24 28
Fig 3 Ratio offactor VIII-related antigeiVIII activity during normal pregnancy andwho had severe preeclampsia.
kidney. Of these, the uterus and itsprimarily involved, as evidenced byeffect of delivery or fetal death. The orof diffuse intravascular coagulation wa:studies in experimental animals wherefibrin deposition was readily shown. Irit is much more likely that the chang
_ 40-i
E
R 30-
o 20-
E 100.10-0L
. 300.
° 200-
to I%oo
001-
-: 0
. 0 -ZE
.ao6-
Caesarcon operation1430G female
37
- Dipyridamole i-(200mg/6hourly)
100001u 50001u 75001u 5000Lu~~~~~~~~~~i
Heparin
10000 Iu S2Ohou 750oIu 12 oLu
12hul ,2hul2hul 2hul
I I I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~29 30Gestation (weeks)
31 32 IweekPuerperium
Fig 4 Intravascular coagulation associated with severe38 preeclampsia treated with subcutaneous heparin and
dipyridamole. Despite correction of intravascular
fibrinl coagulation, as shown by the falling levels ofFDP andi the platelet rising platelet count, no change was evident in the clinicald severe course of the preeclampsia.ho had a
the peripheral blood are a reflection of localizedfibrin deposition, particularly in the uteroplacentalcirculation and in the kidney. The fact that heparintherapy will not reverse established preeclampsia does
3t not exclude intravascular coagulation as having animportant role in the pathogenesis of the disease.A controlled study of low-dose heparin and an anti-platelet agent throughout the second halfofpregnancyin a high-risk group would be of considerableinterest. On available evidence, abnormal fibrinogenmetabolism could still be the major pathway through
I, which the syndrome of preeclampsia is mediated.
Acute Coagulation Defects in Obstetrics
3-23,6 40, The obstetric complications in which diffuse intra-32 36 40 vascular coagulation and defective haemostasis may
arise are shown in the table. A large number of testsinto factor are available for diagnosing coagulation failure in the
'in JO patients obstetric patient, but given the emergency nature ofthe clinical situation time-consuming assays are oflittle value in clinical management. The most useful
contents are screening tests are those concerned with the level andthe dramatic ability to clot of the plasma fibrinogen and with the
riginal concept platelet count. As bedside procedures, the whole.s derived from blood clotting time and the thrombin clotting timedisseminated are recommended. The fibrinogen 'titre', which can
i preeclampsia be performed in citrated blood, is of value for provid-,es detected in ing a rapid estimate of the level of plasma fibrinogen.
t-->
A!D 3 -
0r_a 2-
0
0
01- _
c)
a
x
Jt
on 20 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.s3-10.1.35 on 1 January 1976. Dow
nloaded from

John Bonnar
Complication
Abruptio placentaeAmniotic fluid embolismEclampsia and preeclampsiaInduced (saline) abortionRetained dead fetus or missed abortionIntrauterine infection:
Septic abortionAnte- and postpartum infection
Hydatidiform molePlacenta accretaRupture of the uterusProlonged shock of any aetiologyTransfusion of incompatible bloodSevere fetomaternal bleeding
Table Complications associated with diffuse intra-vascular coagulation and defective haemostasis
The platelet count will reflect, not only the degree ofintravascular coagulation, but also the effect of thetransfusion of a large quantity of banked blood.Where delivery of the patient is not imminent, lowlevels of circulating platelets, eg, less than 30 000 percmm, emphasize the need for obtaining supplies ofplatelet-rich fresh blood or platelet concentrates.
ABRUPTIO PLACENTAEThis is by far the commonest cause of serious coagu-lation failure and, in general, the greater the degreeof placental separation the more likely defectivehaemostasis. The severe concealed or mixed varietyof abruptio placentae is practically always accom-panied by diffuse intravascular coagulation withreduced levels of coagulation factors and increasedlevels of FDP. The depletion of fibrinogen inabruptio placentae is well recognized, but is oftenoveremphasized to the neglect of the other essentialhaemostatic components. In patients with severeabruptio placentae we have found factor VIIIactivity as low as 10 per cent with the factor VIIIRA at 300 per cent. In a series of 15 patients withsevere abruptio placentae and coagulation failure noevidence of pathological fibrinolytic activity wasdetected. The high levels of FDP which are presentare most likely due to breakdown of intravascularfibrin by local release of activator. High levels ofFDP, as well as being a major factor in defectivehaemostasis, will also have a beneficial role ininhibiting the process of fibrin deposition within thevascular tree.
Placental separation at normal delivery is usuallyrapid and the associated activation of the clottingsystem is largely confined to the uterine circulation.In abruptio placentae, partial or complete separationof the placenta occurs, usually before the patient isin labour, and this situation is maintained until theprocess oflabour anddelivery iscomplete. During thistime, a substantial blood flow continues to the
uterus and the placental site, allowing the entry ofprocoagulant substances into the systemic circulationfrom the damaged placenta and decidua. The processof intravascular coagulation is therefore likely tocontinue until the placenta is delivered and theuterus empty and retracted.Shock will also promote intravascular coagulation
and the rapid and adequate correction of thedepleted blood volume by monitoring of the centralvenous pressure and the urinary output will thereforebe a major factor influencing the process of intra-vascular fibrin formation. Where serious haemor-rhage and defective coagulation are present, thetransfusion of fresh blood to maintain the circulatingblood volume will be the best management. If freshblood cannot be obtained, then fresh frozen plasmarather than concentrated fibrinogen should be given;this will provide a supply of factors V and VIII aswell as fibrinogen and the coagulation inhibitor
250-
E 200-
_ 150-ISO-cr
- 100-
50-
0
140-
- 100-
, 60-
20-
3'a
80-
60-
--Blood 4 stored 5 fresh-.Fibrinogen (4G) Plasma fibrinogenIII
I I
,1 ,,~~~~~~~~~~~~~~~~~~~~~~~~~~ISerum fibrinogen related antiqen-
II
I Antithrombin III
~~~~~F_~~~~~~~~~~~401W § |; 1
04 06 08 10 12 14 l6 18 20 22 09Time (hours) Delivery
Fig 5 Abruptio placentae with defective bloodcoagulation. Antithrombin III showed a marked decreaseduring infusion of concentratedfibrinogen.
antithrombin III. When the concentrated fibrinogenis given alone, we have found a sharp decrease ofantithrombin III which suggests that the fibrinogenconcentrates may aggravate the intravascularcoagulation (fig 5).
In the presence of a severe abruptio placentae witha dead fetus, the aim should be to expedite vaginaldelivery, avoiding any soft tissue damage to thegenital tract. The delivery of the fetus and placenta isusually followed by spontaneous correction of the
.38
e
on 20 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.s3-10.1.35 on 1 January 1976. Dow
nloaded from

Coagulation disorders
coagulation defect and until such time as this occursmyometrial retraction will greatly reduce bleedingfrom the placental site. In severe abruptio placentaewith a dead fetus, delivery by caesarean section israrely indicated, and in the presence of a coagulationdefect the danger of bleeding from surgical incisions,especially following operation, must be appreciated.In the vast majority of cases, conservative manage-ment with maintenance of the blood volume will befollowed by spontaneous delivery. In the exceptionalcase where this does not occur and defective clottingis present, any operative interference should bedelayed until normal blood clotting is restored withfresh blood and, if necessary, platelet concentrates.Treatment with fibrinolytic inhibitors, such as
aminocaproic acid or aprotinin (Trasylol), could bepotentially harmful in that such agents will inhibitplasminogen activation and the clearance of intra-vascular fibrin deposits. In rare cases, one to twohours after delivery severe postpartum haemorrhagecan occur from the placental site. In this postpartumsituation, it is possible that enhanced fibrinolysis inthe uterus may be contributing, and, if the bleedingcannot be controlled by manual and pharmacologicalstimulation of myometrial contraction, EACA 4 gintravenously may prove effective in arresting thehaemorrhage.
In patients with abruptio placentae, treatment withheparin has been suggested to block the consumptionof coagulation factors. In the presence of an intactvascular compartment, this concept would beattractive but in the patient bleeding into the retro-placental space and myometrium due to prematureplacental detachment, heparin would be likely toaggravate the blood loss or be neutralized by thelarge amount of platelet factor 4 in circulation. Thevalue ofheparin therapy would seem therefore almostimpossible to evaluate given the disruption of thecoagulation system and the emergency situationwhich prevails with an acute coagulation disorder.
AMNIOTIC FLUID EMBOLISMThis is the most serious catastrophe which can occurduring labour or shortly after delivery. Massiveintravascular coagulation occurs and consumption ofthe clotting factors can be almost total (Bonnar,1973). The pulmonary vasculature appears to beextensively obstructed with a large amount ofplatelet-fibrin material. This being so, the rapidtransfusion of fluids or blood can precipitate cardiacfailure. The aim should be to sustain the circulationuntil the fibrin deposits are cleared by the activefibrinolytic process present in the pulmonarycirculation. The speed of transfusion should becontrolled by monitoring the central venous pressureto avoid precipitating cardiac failure. If catastrophic
39
bleeding from the placental site can be controlledby myometrial contraction, then the most logicaltreatment is a careful controlled transfusion of freshblood and heparin administration.
ABORTIONSevere bleeding tendencies and maternal deaths havebeen reported as a complication of saline-inducedabortion (Spivak et al, 1972). Changes in the bloodcoagulation system compatible with diffuse intra-vascular coagulation have been described by Standerand colleagues (1971) and by van Royen (1974).Hypertonic urea solutions can also precipitate intra-vascular coagulation (MacKenzie et al, 1975). Thestimulus would appear to be the placental damageinduced by the hypertonic solutions. In patients whosuffer from endotoxic shock in association withpregnancy, eg, septic abortion, coagulation failurecan arise as a result of diffuse intravascular clotting.In pregnant animals only one exposure to bacterialendotoxin is required to produce the Schwartzmanreaction and this may be the result of the diminishedfibrinolytic activity in pregnancy which facilitatesintravascular fibrin deposition. Where severe bleed-ing from the uterus is not a problem and evidence ofdiffuse intravascular coagulation is present, treat-ment with heparin would seem logical.
Anticoagulant Therapy during Pregnancy
An increasing number of women in the reproductiveyears are receiving long-term anticoagulant therapy
0/0.1 _ ....-k -r30u- _ Newoorn " Mother
200-
1Fr-
Factor II VII IX X VI11
VII
Fig 6 A comparison of the coagulation factors in thenewborn and the mother immediately after birth (15 casesmean + standard error).
because of thromboembolic incidents and heartvalve prostheses. Oral anticoagulants during preg-nancy are associated with an unusually high fetalmortality. This is not fully explained by the haemor-rhagic complications which can arise in the fetus orin the newborn when these drugs are employed inlate pregnancy.
11I M-OL-,
L-i
on 20 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.s3-10.1.35 on 1 January 1976. Dow
nloaded from

1-72Y, 1-04
Deliv,eryHome Re admitted 3350G mole Home Fig 7 Plasma heparin levels in a
10 00o0u 4 patient with bilateral ileofemoral12 hours., *thrombosis at the 29th week ofColcium heparin- Sodiumn Calcium heparin pregnancy. Patient used self-20000e1inu 00I amnstrd uctaeu12 hours 10hoIur 12 hours <_Breast feedLn_q_ amnitrd__otae12 hours heparin forfour months and breast
fed her baby.
29 30 31 32 33 34 35 36 37 38 39 40 2 3 4Gestation (weeks) Puerperium (weeks)
In the fetus and newborn, the levels of the vitamin-K-dependent factors II, VII, IX and X are normallylow (figure 6). Coumarin derivatives readily cross theplacenta and when given to the mother will furtherdeplete the low level of these vitamin-K-dependentfactors in the fetus. Haemorrhage which may befatal or cause non-fatal brain damage is an obvioushazard in the infant during labour or after delivery.
Heparin is the safest anticoagulant to use duringpregnancy, and using a regime of self-administeredsubcutaneous injections we have now treated 60women for periods of up to six months. In 15 womenwho received heparin during labour or duringcaesarean section for prophylaxis or treatment ofthromboembolic complications we found no evidenceof any heparin in the cord blood with a specificanti-XA assay for heparin. Our experience suggeststhat long-term treatment with low-dosage, sub-cutaneous heparin using a self-administrationregime, is feasible during pregnancy and the puer-
perium. A further advantage of this treatment is thatit allows breast feeding in the puerperium (figure 7).For safe and effective therapy, monitoring of the
heparin levels in the plasma is required so thatadequate heparin is given during the third trimesterwhen neutralization of the heparin takes place dueto the intravascular coagulation in the uteroplacentalcirculation. On average, 7500 to 10 000 units12-hourly are required in late pregnancy to achieve a
heparin level between 0-1 and 0-4 units per ml.We have not encountered any bleeding problems inpatients where the heparin level was less than 0 4 unitsper ml when heparin treatment was continued duringlabour and delivery or caesarean section. Because ofthe risk of local bleeding, however, epidural anaes-thesia should be avoided in patients receiving heparinprophylaxis (Bonnar et al, 1976).Ancrod (Arvin), the purified fraction of the
venom of the Malayan pit viper, should not be givenin pregnancy. In the mouse and rabbit a highincidence of fetal death associated with haemorrhageat the placental site was found (Penn et al, 1971).
Streptokinase and urokinase, if administered whendelivery is imminent or within one week of child-birth, can produce severe haemorrhage from theuterus. In view of this hazard, streptokinase andurokinase are not recommended save in the excep-tional situation where fatal pulmonary embolismappears likely without their use and the risk of severehaemorrhage is accepted.
Conclusion
Pregnancy induces extensive physiological changesin the haemostatic system. Local intravascularcoagulation in the uteroplacental circulation is afeature of normal pregnancy which is most likelyresponsible for the increased production of coagula-tion factors. The resulting 'hypercoagulability' willalso be of benefit to meet the demands on thehaemostatic components which inevitably arise atthe time of placental separation. These physiologicalchanges produce a vulnerable state for intravascularcoagulation and varying degrees of this phenomenonoccur in several complications of pregnancy. Inpreeclampsia, increased intravascular coagulation,as compared to normal pregnancy, is now welldocumented. In the acute coagulation disorders suchas arise with abruptio placentae and amniotic fluidembolism, extensive intravascular coagulation associ-ated with life-threatening haemorrhage can arise.The most effective treatment in such patients is atpresent the transfusion of fresh blood to maintainthe circulating blood volume until the stimulus tointravascular clotting is removed and spontaneouscorrection takes place.
0-8
02
E 0 6
04c
It 0 2.
40 John Bonnar
on 20 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.s3-10.1.35 on 1 January 1976. Dow
nloaded from

Coagulation disorders
The research work reported in this presentation wassupported by the Medical Research Council (grantno. G971/755/C).
References
Astedt, B. (1972). On fibrinolysis. Acta obstet. gynec. scand.,51, Suppl. 18, 1-45.
Bennett, B., and Ratnoff, 0. D. (1972). Changes in anti-hemophilic factor (AHF, factor VIII) procoagulant activityand AHF-like antigen in normal pregnancy, and followingexercise and pneumoencephalography. J. Lab. clin. Med.,80, 256-263.
Biland, L., and Duckert, F. (1973). Coagulation factors of thenewborn and his mother. Thrombos. Diathes. haemorrh.(Stuttg.), 29, 644-651.
Bonnar, J. (1973). Blood coagulation and fibrinolysis inobstetrics. Clin. Haemat., 2, 213-233.
Bonnar, J., Davidson, J. F., Pidgeon, C. F., McNicol, G. P.,and Douglas, A. S. (1969a). Fibrin degradation products innormal and abnormal pregnancy, and parturition. Brit.med. J., 3, 137-140.
Bonnar, J., Denson, K. W. E., Haddon, M., and Thornton,C. (1976). Long-term treatment with self-administeredheparin in pregnancy. (In preparation.)
Bonnar, J., McNicol, G. P., and Douglas, A. S. (1969b).Fibrinolytic enzyme system and pregnancy. Brit. med. J.,3, 387-389.
Bouma, B. N., Sixma, J. J., van Mourik, J. A., and Mochtar,I. A. (1973). Immunological determination of anti-haemophilic factor A (factor VIII). (Abstr.) Neth. J. Med.,16, 54.
Condie, J. (1975). MD Thesis, University of Aberdeen.Coopland, A., Alkjaersig, N., and Fletcher, A. P. (1969).
Reduction in plasma factor XIII (fibrin stabilising factor)concentration during pregnancy. J. Lab. clin. Med., 73,144-153.
Gj0nnaess, H. (1973). Cold promoted activation of factor VII.Cynaec. Invest., 4, 61-721
41
Hedner, U., and Astedt, B. (1970). Fibrinolytic split productsin serum and urine in pregnancy. Acta obstet. gynec.scand., 49, 363-366.
Kawano, T., Morimoto, K., and Uemura, Y. (1968). Uro-kinase inhibitor in human placenta. Nature (Lond.), 217,253-254.
MacKenzie, I. Z., Sayers, L., Bonnar, J., and Hillier, K.(1975). Coagulation changes during second-trimesterabortion induced by intra-amniotic prostaglandin E2 andhypertonic solutions. Lancet, 2, 7944, 1066-1069.
McKillop, C., Howie, P. W., Forbes, C. D., and Prentice,C. R. M. (1976). Soluble fibrinogen/fibrin complexes inpre-eclampsia. Lancet, 1, 56-58.
Nossel, H. L., Lanzkowsky, P., Levy, S., Mibashan, R. S.,and Hansen, J. D. L. (1966). A study of coagulation factorlevels in women during labour and in their newborn infants.Thrombos. Diathes. haemorrh. (Stuttg.), 16, 185-197.
Penn, G. B., Ross, J. W., and Ashford, A. (1971). The effectsof Arvin on pregnancy in the mouse and the rabbit.Toxicol. appl. Pharmacol., 20, 460-473.
van Royen, E. A. (1974). Thesis on haemostasis in humanpregnancy and delivery. University of Amsterdam.
Sheppard, B. L., and Bonnar, J. (1974). The ultrastructure ofthe arterial supply of the human placenta in early and latepregnancy. J. Obstet. Gynaec. Brit. Cwlth, 81, 497-511.
Spivak, J. L., Spangler, D. B., and Bell, W. R. (1972).Defibrinogenation after intra-amniotic injection of hyper-tonic saline. New Engl. J. Med., 287, 321-323.
Stander, R. W., Flessa, H. C., Glueck, H. I., and Kisker, C. T.(1971). Changes in maternal coagulation factors afterintra-amniotic injection of hypertonic saline. Obstet. andGynec., 37, 660-666.
Uszynski, M., and Abildgaard, U. (1971). Separation andcharacterization of two fibrinolytic inhibitors from humanplacenta. Thrombos. Diathes. haemorrh. (Stuttg.), 25,580-589.
Woodfield, D. G., Cole, S. K., Allan, A. G. E., and Cash,J. D. (1968). Serum fibrin degradation products throughoutnormal pregnancy. Brit. med. J., 4, 665-668.
on 20 May 2018 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.s3-10.1.35 on 1 January 1976. Dow
nloaded from