prise en charge du lmnh diffus grandes cellules b...
TRANSCRIPT

Prise en charge du LMNH diffus
grandes cellules B (DLBCL)
ALGERIE
Mai 2014
Anne-Sophie Michallet
Diffuse large B-cell lymphoma (DLBCL), not otherwise specified (NOS)
Common morphologic variants
Centroblastic
Immunoblastic
Anaplastic
Molecular subgroups
Germinal-centre B-cell-like (GCB)
Activated B-cell-like (ABC)
Immunohistochemical subgroups
CD5-positive DLBCL
Germinal-centre B-cell-like (GCB)
Non-germinal-centre B-cell-like (Non-GCB)
DLBCL subtypes
T-cell/histiocyte-rich large B-cell lymphoma
Primary DLBCL of the CNS
Primary cutaneous DLBCL, leg type
Epstein-Barr virus–positive DLBCL of the elderly
Other lymphomas of large B cells
Primary mediastinal (thymic) large B-cell lymphoma
Intravascular large B-cell lymphoma
DLBCL associated with chronic inflammation
Lymphomatoid granulomatosis
ALK-positive DLBCL
Plasmablastic lymphoma
Large B-cell lymphoma arising in HHV8-associated multicentric Castleman disease
Primary effusion lymphoma
Borderline cases
between DLBCL and Burkitt lymphoma
between DLBCL and classical Hodgkin lymphoma
DLBCL WHO Classification (2008)

• Différents sous types de DLBCL
• Le traitement doit-il être différent en fonction
du sous type?
– Intermediate Burkitt or Hodgkin
– Plasmablastic (CD20-)
– “Double hit” myc+ bcl2+
– Primary CNS DLBCL

Alizadeh AA et al. Nature 2000;403:503-11.
GC B like
Activated B
like
Une origine différente?
Profil expression génique et DLBCL

Activated B-cell likeGC B-cell like
NFK B activation
BCL2 translocations, t(14;18)
C-rel amplification
LMO2 IgH M
BCL6
CD10
MUM1/IRF4
+3
18q21 amplification
BCL6 translocations
Mir-125b
Mir-17-92
Mir-155
Mir-21
Mir-223
BCL2
FOXP1
2 maladies différentes

Hans CP et al. Blood 2004;103:275-82
Immunohistochimie as surrogate

DLBCL = One Shot Cancer
• Seul les patients en RC après la première ligne
de traitement ont une chance d’être guéris!
• Une minorité des patients qui progressent
répondent alors au tt de rattrapage et peuvent
être intensifiés
• 40% des patients intensifiés ne rechutent pas
Objectif du treatment: obtention d’une RC durable

PFS et OS Etudes LNH 87/93/98
7 years: PFS = 47.5% [46-49%]; OS = 56% [54-57%]
8-9%
7400 patients
18-80 years old

Que faut il connaître avant d’initier le
traitement de première ligne?
• Age
– jeune (<61 y)
– âgé (60-80 y)
– Trés âgé (>80 y)
• IPI – age-adjusted IPI
– Score 0
– Score 1
– Score 2 or 3
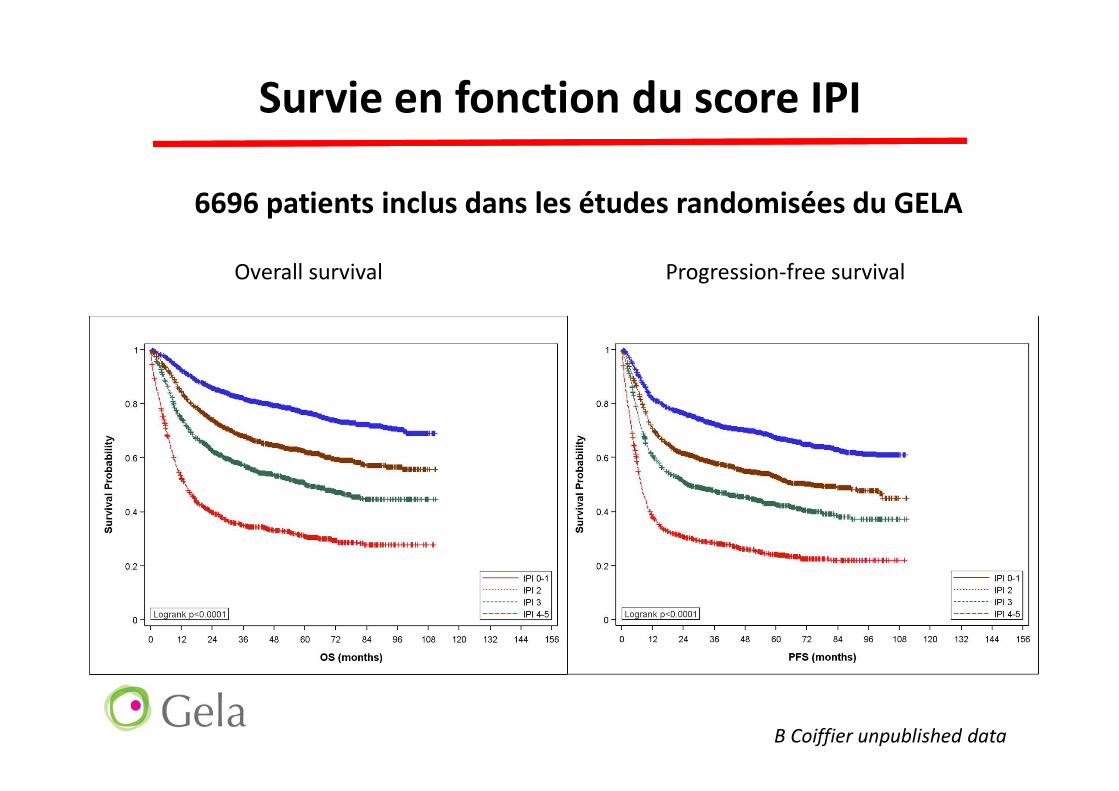
Survie en fonction du score IPI
6696 patients inclus dans les études randomisées du GELA
Overall survival Progression-free survival
B Coiffier unpublished data

Comment choisir le bon traitement?
• Patient
– Age, co-morbidités, dépendance
– Espérance de vie
• Lymphome
– Facteurs pronostics
• IPI, biologie …
– origine cellulaire: ABC vs GC
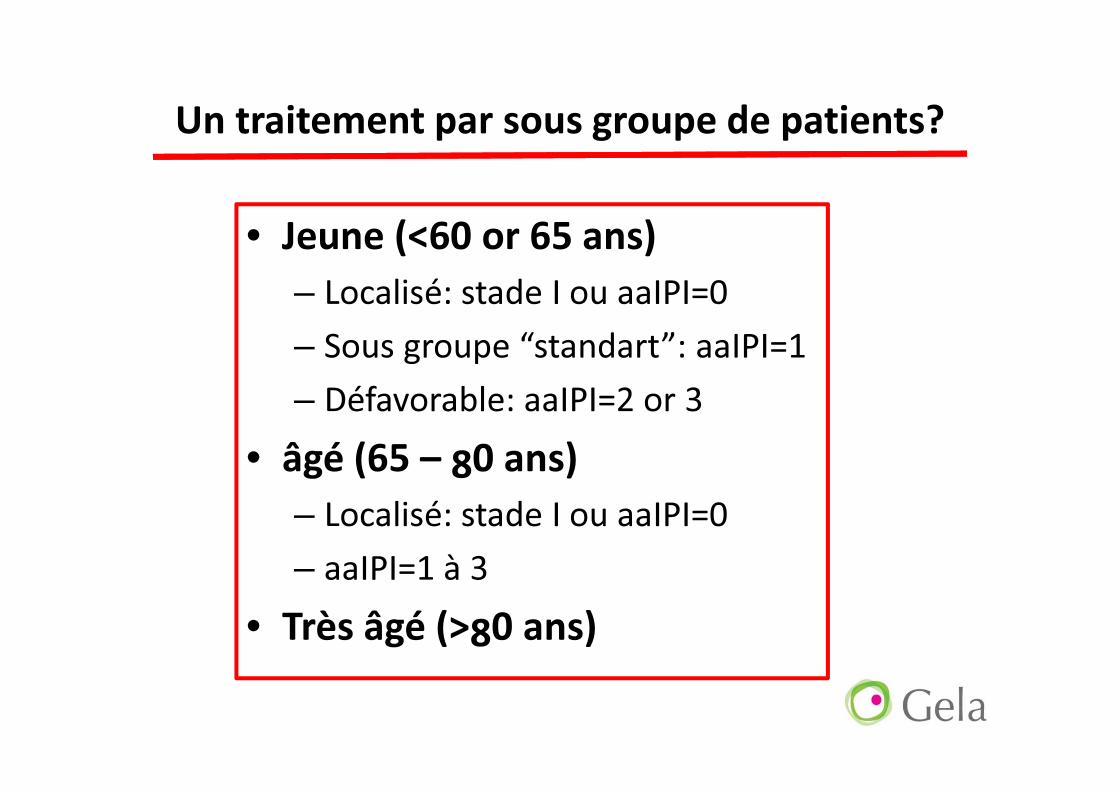
Un traitement par sous groupe de patients?
• Jeune (<60 or 65 ans)
– Localisé: stade I ou aaIPI=0
– Sous groupe “standart”: aaIPI=1
– Défavorable: aaIPI=2 or 3
• âgé (65 – 80 ans)
– Localisé: stade I ou aaIPI=0
– aaIPI=1 à 3
• Très âgé (>80 ans)

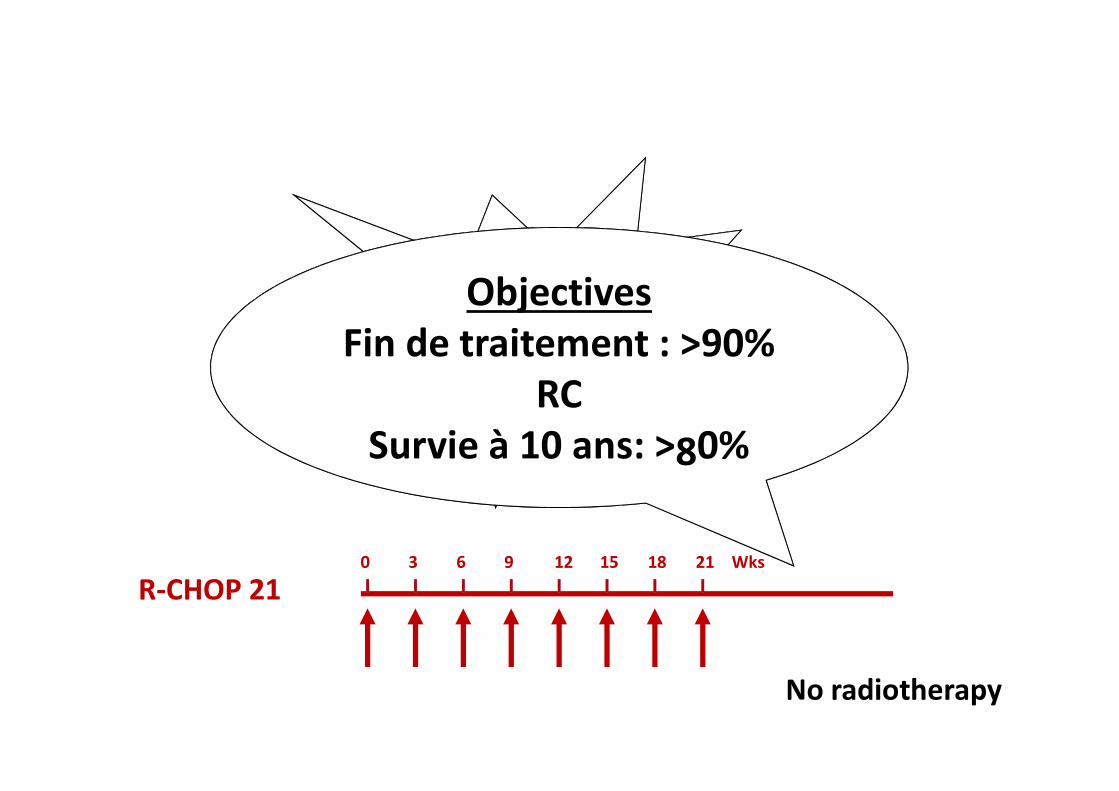
Un traitement de réfèrence
R-CHOP
60 3 12 15 189 21 Wks
No radiotherapy
R-CHOP 21
R-CHOP
60 3 12 15 189 21 Wks
No radiotherapy
R-CHOP 21
Objectives
Fin de traitement : >90%
RC
Survie à 10 ans: >80%

Quand le R-CHOP est-il insuffisant?
• Si taux de RC < 90%
• Si taux de rechute >10%
• Sujet âgé
– Maladie non localisée
• Patients jeune
– aaIPI score 1
– aaIPI score 2/3
– “double hit”

Maladie localisée / IPI=0
Quelque soit l’âge!
R-CHOP x 6
PAS DE RADIOTHERAPIE

LNH 93-4: IPI=0; >60y
R
CHOP X 4
CHOP X 4 +
IF RT
CHOP
CHOP plus radiotherapy
Pro
ba
bilit
y o
f E
ve
nt
Fre
e S
urv
iva
lP = 0.5
5y EFS: 64%
5y EFS: 61%
n=277
n=299
median f-up= 7y
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12
Years after Randomization
CHOP
CHOP plus radiotherapy
Pro
ba
bilit
y o
f O
ve
rall S
urv
iva
l
n=299
n=277
5y OS: 72 %
5y OS: 68 %
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12
Years after Randomization
P = 0.5 median f-up= 7y
G Fillet, JCO 2007
- Identical CR rates
- More secondary
cancers with RT

R
CHOP X 4
CHOP X 4 +
IF RT
CHOP
CHOP plus radiotherapy
Pro
ba
bilit
y o
f E
ve
nt
Fre
e S
urv
iva
l
P = 0.5
5y EFS: 64%
5y EFS: 61%
n=277
n=299
median f-up= 7y
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12
Years after Randomization
50% survie n’est pas acceptable!
DONC
Adjonction de rituximab
6 cycles of R-CHOP

Maladie localiséetraitement basé sur le PET scanner
R-CHOPx3
R-CHOPx1
IFRTPET Pos
PET Neg
L Sehn et al. ICML 2011
134 patients, 57% stage I & 43% stage II

TTP associé au résultat du PET
6543210
1.0
.9
.8
.7
.6
.5
.4
.3
.2
.10.0
PET- positive
PET- negativeP
erc
en
t S
urv
iva
l
Time (years)
L Sehn et al. ICML 2011

Etude en cours
aaIPI = 0

Avant traitement Après traitement
..
..
..
Tomographie par emission de positons : le PET-scanner
Parfois couplé au scanner conventionnel
Place de la TEP-FDG dans les
Lymphomes
Le point de vue de l’’’’hématologue

Intérêt du PET-TDM dans les Lymphomes
• STADIFICATION = FACTEUR PRONOSTIQUE
– Sites anatomiques (extra-ganglionnaires+++)
– Taille des lésions
• EVALUATION DE LA REPONSE AU TRAITEMENT
– Evaluation précoce de la chimiosensibilité (2 cures)
– Valeur pronostique positive (4 cures)
• SURVEILLANCE =
DIAGNOSTIC DE MALADIE RESIDUELLE
– Chimiothérapie de rattrapage

Importance du STADE
Rôle déterminant du PET dans le « staging »?

– LMNH Agressifs diffus grandes cellules B = 100%
– MALADIE DE HODGKIN = 98%
Les interrogations : Fixations variables?
� LMNH indolents
cas du Folliculaire
Diagnostique de transformation
� LMNH T périphériques
� cas particulier du POPPEMA
L’’’’Efficacité du PET dépend du type histologique!

Evaluation précoce de la réponse en cours de traitement :
PET indicateur pour un traitement « personnalisé »
Evaluation précoce de la chimiosensibilité
Définir les bons et mauvais répondeurs
�MALADIE DE HODGKIN
PET 2 et PET 4 : Données du Protocole H10
� LMNH AGRESSIF
Protocole LNH037B

FDG-PET (+)
..
..
..
Before treatment At 2 cycles At 4 cycles

Before treatment At 2 cycles At 4 cycles
FDG-PET (-)..
..
..

..
..
..
Identification des patients susceptible de rechuterimportance du PET
Valeur du PET intermédiaire
2 cycles
2 cycles
4 cycles
4 cycles
C Haioun Blood 2005; 106: 1376–81
BON REPONDEUR
MAUVAIS REPONDEUR

Intérêt du PET précoce
Si sa valeur prédictive est importante :
tous les patients “non-respondeurs” doivent
immédiatement bénéficier d’une thérapeutique
aggressive

LNH07-3B
DLBCL ; <60 yearsaa-IPI = 2-3
PET 4
Arm A
A1
A2
B2
B1
R-ACVBP14 + MTX IT + G-CSF
PET 2PET 4
R-CHOP14 + MTX IT + G-CSF
Z-BEAM + ASCTMTX iv
MTX iv AraCR- IFM / VP16
Salvage : CORAL
PETPET
4+
PET Results
Salvage : CORAL
Arm B
A1
A2
B2
B1
2- /4 -
2+ /4 -
2- /4 -
4+
PET 0 PET 4 PET FinalR
R-CHOP14 + G-CSF
Thérapeutique personnalisée : PET indicateur

P < 0.001log rank
0.00 0.25 0.750.50 1.00 1.25 1.751.50 2.000.00
0.25
0.50
0.75
1.00
2.250.00 0.25 0.750.50 1.00 1.25 1.751.50 2.000.00
0.25
0.50
0.75
1.00
P < 0.001log rank
OS EFS
92 %80%
43 %
53 %
yearsyears
Negative Pet Positive PET
p log rank = 0.0003 p log rank = 0.0002
JF Filmont et al ; Cancer 2007

Y a t’’’’il une place pour le PET dans
l’’’’évaluation des lymphomes indolents?
Les critères d’’’’évaluation
1- réponse thérapeutique par rapport au
bilan initial
2-% de réduction tumorale
Evaluation scannographique seule

Patients âgés- IPI > 0
R-CHOP x 8
Existe t’il un meilleur
traitement?

Etudes du GELA: 10 ans de suivi
B Coiffier et al. Blood 2010;116:2040

Autres options?
• R-CHOP-14
• R-CHOP + X
• R-CHOP suivi par X
• Chimiothérapies fortes doses

LNH 03-6B
3 months
C5 FU1
Randomisation Response
Induction Phase Consolidation Phase
Consolidation Phase
Rituximab + CHOP14
+ MTX IT
Rituximab + CHOP21
Response
C2 C7 C8
Induction Phase
C1 C2 C3 C4 C5 C6 C7 C8 FU1FU0
FUn
Rituximab + CHOP21
+ MTX IT
Response
8 weeks 10 weeks
12 weeks 13 weeks
C1
FUn
FU0
Rituximab + CHOP14
C3 C4 C6
3 months
3 months 3 months
Aranesp, one weekly subcutaneous injection in Arms A1 and B1
Filgrastim ou Pegfilgrastim according to physician decision R Delarue et al. ICML 2011

Etude R-CHOP 14/21
3y-PFS : 60% vs 62%
HR: 0.99 (95%CI: 0.78-1.26); p=0.94
PFS OS
3y-OS : 69% vs 72%
HR: 0.93 (95%CI: 0.76-1.26); p=0.76

Conclusion R-CHOP 14 vs. 21
• Hypothèse
– R-CHOP-14 supérieur au R-CHOP-21
• Résultats
– UK: PAS DE DIFFERENCE
– GELA: PAS DE DIFFERENCE
• Conclusion
R-CHOP tous les 21 jours est le STANDART
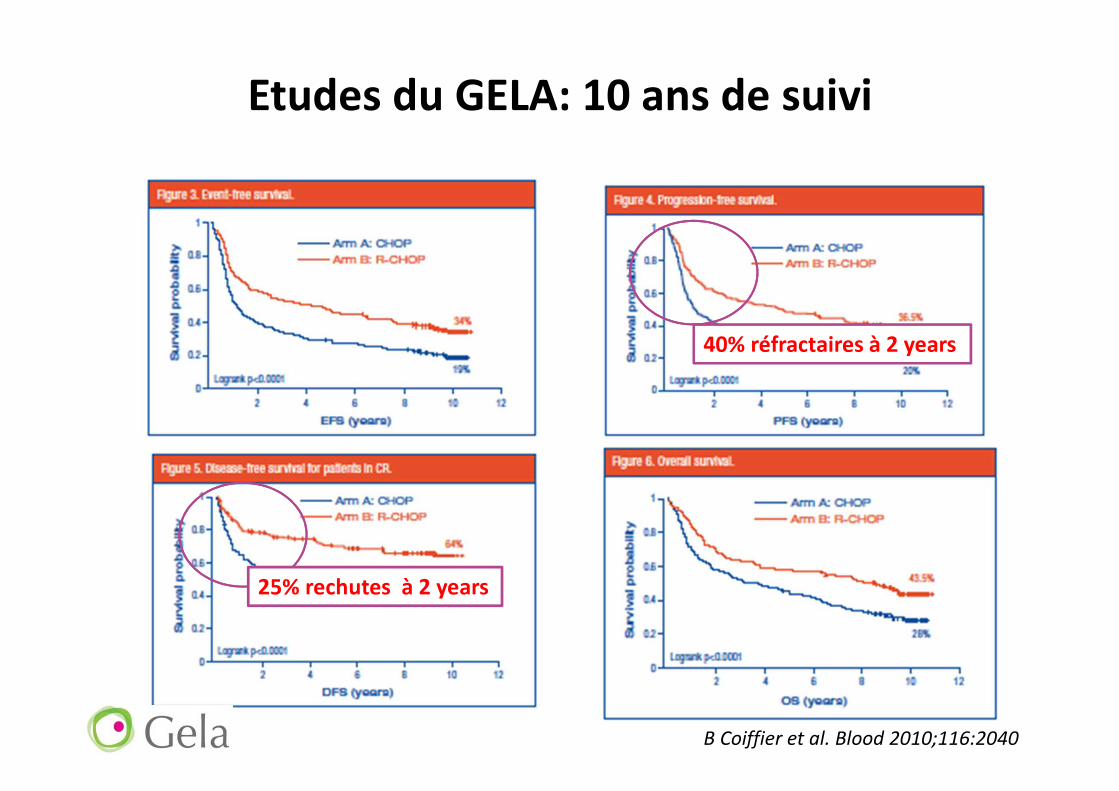
Etudes du GELA: 10 ans de suivi
40% réfractaires à 2 years
25% rechutes à 2 years
B Coiffier et al. Blood 2010;116:2040

Patient jeune, IPI =1
R-CHOP 14 vs. 21
R-ACVBP

Patients jeunes: quelles options?
• Traiter tous les patients de façon identique?
– Indépendament des facteurs pronostiques
• Stratifier selon IPI
• Rechercher de nouveaux indicateurs de survie

LNH 03-2B: R-ACVBP vs R-CHOP
*Pas de radiothérapie dans les 2 bras de tt
R
60 3 12 15 189 21
R-ACVBP 14
R-CHOP 21
Wks
MTX R-IFM-VP16 Ara-C
0 2 4 6 10 14 24 Wks
4 IT-MTX
C Rechert et al. Lancet 2011;378:1858

Taux de réponses à la fin du tt
ORR R-ACVBP
92%
ORR R-CHOP
88%
84
82 4
80
81
9
0
10
20
30
40
50
60
70
80
90
100
CR/CRu PR SD PD
%o
f re
spo
nd
ing
pa
tie
nts
R-ACVBP
R-CHOP
p-value: 0.5727
C Rechert et al. Lancet 2011;378:1858

Etude LNH 03-2B
C Rechert et al. Lancet 2011;378:1858
EFS
OSDFS
PFS

R-ACVBP ou R-CHOP?
• R-CHOP une chimiothérapie mieux tolérée
MAIS INFERIEURE AU R-ACVBP
• Solution:
– Evaluation des facteurs pronostics avant tt
– R-CHOP= pronostiques favorables
– R-ACVBP= pronostiques défavorables

Patient jeune IPI= 2/3
R-ACVBP
Intérêt d’une intensification thérapeutique
(Autogreffe)?

Etudes GELA
DLBCL/ Autogreffe
< 60 ans , 2-3 aa-IPI factors
ACVBP
0 2 4 6
R
HD-MTX
CBVM
PBSCT
13
Wk
R-ACVBP
0 2 4 6
R
HD-MTX
BEAM
PBSCT
13
Wk
LNH98-3B
241 pts
LNH03-3B
209 pts
R
Rituximab
Observation
Introduction Rituximab

With rituximab
Without rituximab
Fitoussi O et al. Hematologica 2011;96:1136
ACVBP vs R-ACVBP + PSCTLNH98-3/LNH03-3B aaIPI=2,3

Quels sont les patients à intensifier?
• Réponses partielles (PET+ après induction)=
rattrapage+ autogreffe
• Tous les patients IPI> 1
• Tous les patients “high risks”(Double hit…)
• Les répondeurs “lents” (PET intermédiaire +)
?

Patients âgés
patient “FIT”: R-mini CHOP
Patient”UNFIT”: R-Chemo

Patients >80 ans
6 cycles of R-miniCHOP, 3 weeks interval
• CD20+ Diffuse large B-cell lymphomahistologically proven
• Age > 80 years
• Non pretreated patient
• aaIPI 0, 1, 2 or 3
• Ann Arbor Stages I bulky to IV
• Perfomance status 0 to 2
• Bone marrow biopsy, lumbar punctionand TEP-TDM were non mandatory
3 months
C5 FU1C1
Inclusion
R-miniCHOP
C2 C3 FU0
3 w
C4
3 w3 w3 w3w 4 w
C6
R-miniCHOP
FUn
RESPONSERESPONSE
R-miniCHOP Dose D1 D2 D3 D4 D5 Prednisone 40 mg/m² X X X X X Rituximab 375 mg/m² X Doxorubicin 25 mg/m² X Cyclophosphamide 400 mg/m² X Vincristine 1 mg DT X
Peyrade F, et al. Lancet Oncol; 2011 12(5):460-8

Causes de décés
ToxicityLymphoma
progressionOthers Total
Treatment
Period
12(including 5
during the
first cycle)
8 7
1 bleeding
27
2 chest pain
1 poor general condition
1 pneumopathy
2 unknow causes
Follow-up
Period0 25
1 stroke
31
1 acute renal insufficiency
1 poor general condition
3 unknown
Total 12 33 13 58
6
F Peyrade et al. Lancet Oncol 2011;12:460

Median OS: 29 months
At two years: 59% ( CI: 49-67)
Survie globale
Intention de traitement
Median FU: 20 months
F Peyrade et al. Lancet Oncol 2011;12:460

Points importants
• “Double hit” DLBCL
• Prophylaxie CNS
• Transformation DLBCL
• Primary CNS lymphome
• Primary cutaneous lymphome
• Association HP DLBCL localisation gastrique

DLBCL “Double hit”
• BCL2 et MYC translocation ou hyperexpression
• Rare, GCB subtype
– Incidence <10% DLBCL
– Environ 20% pour transformation en DLBCL
• Mauvaise réponse à la chimiothérapie
• une survie globale courte
PRONOSTIQUE DEFAVORABLE
RC Lindsey et al. Cur Op Hematol 2012;19:299. S Li et al. Mod Pathol 2012;25:145
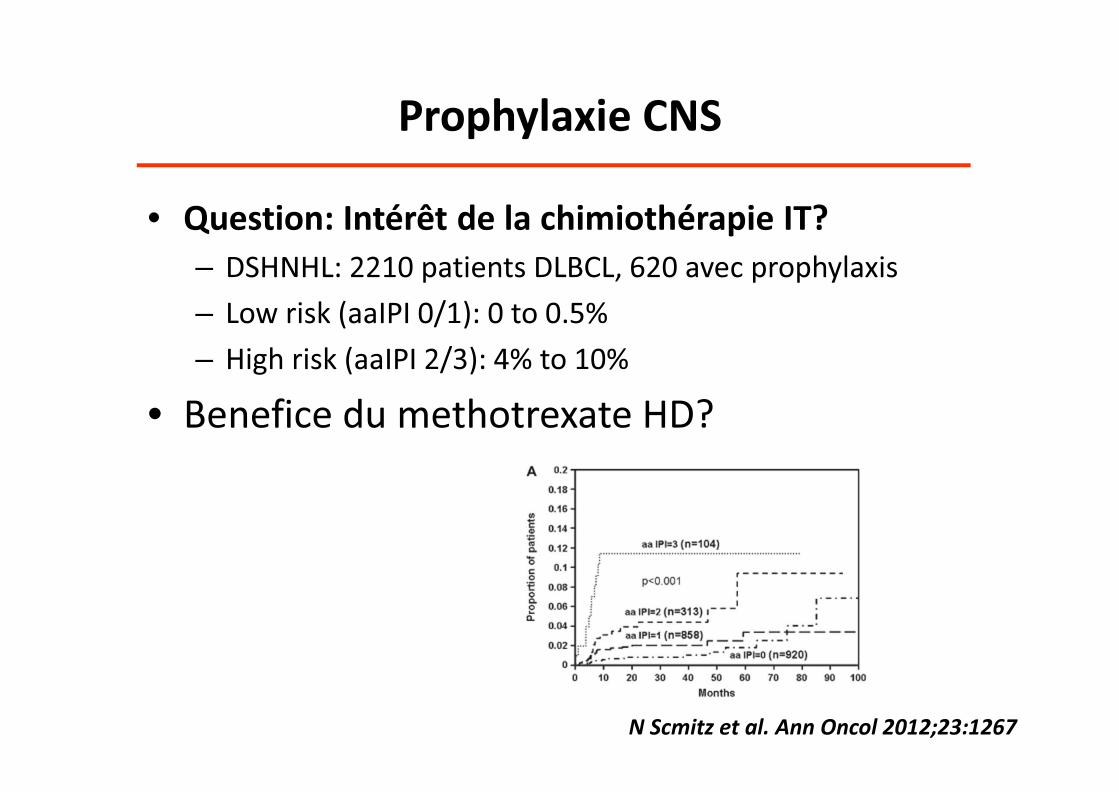
Prophylaxie CNS
N Scmitz et al. Ann Oncol 2012;23:1267
• Question: Intérêt de la chimiothérapie IT?
– DSHNHL: 2210 patients DLBCL, 620 avec prophylaxis
– Low risk (aaIPI 0/1): 0 to 0.5%
– High risk (aaIPI 2/3): 4% to 10%
• Benefice du methotrexate HD?

DLBCL= transformation d’un iLMNH
• Situation fréquente, souvent méconnue
• Doit être traité comme un DLBCL primitif
– HDT avec autogreffe en première RC?
• Rechutes tardives plus fréquentes
– Forme indolente (1/3)
– Forme agressive
• Pronostique défavorable/ DLBCL primitif

DLBCL: primitif CNS
• PRONOSTIQUE DEFAVORABLE
• “HD methotrexate-containing regimen” reste
le traitement standart
• Radiothérapie complémentaire trés discutée

Helicobacter pylori-DLBCL localisation gastrique
• Etude rétrospective: 50 patients stade I-II
• Non antérieurement traités
ANTIBIOTHERAPIE: 69% RC
– 11/16 DLBCL
– 18/32 DLBCL (transformation MALT)
• Suivi médian de 7.7 ans: tous les patients en
RC sont vivants sans maladie
Kuo et al. Blood 2012;119:4838

Age <60 y 60 - 80 y >80 y
aaIPI score 0 1 >1 0 >1 All
R-CHOP R-ACVBP R-CT + HDT R-CHOP R-mCHOP
1st line
Relapse Rattrapage + HDT
Nouvelles drogues
x6 x6 x6x8
Proposition Algorithme thérapeutique
Conclusion

Conclusions
• Rechutes après R-CHOP reste difficile à traiter
• Quels traitements pour les rechutes tardives?
• Pas de stratégie curative au moment de la
rechute
PREVENIR LES RECHUTES
ONE SHOT TRAITEMENT