primary total knee arthroplasty
TRANSCRIPT
Primary Total Knee Arthroplasty
Jatinder S. LuthraMS DNB MRCS
Historic Evolution
• 19th century – Soft tissue interposition
• 1950 Walldius Hinged knee replacement
• 1960 MacIntosh & McKeever Acrylic tibialplateau
• 1973 – Total condylar prosthesis
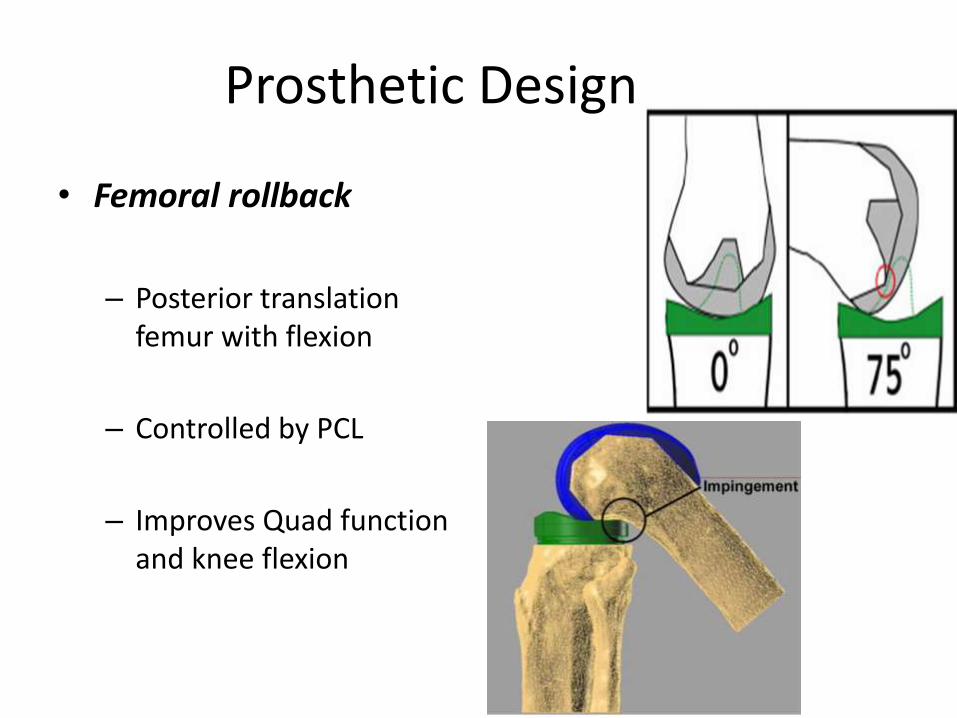
Prosthetic Design
• Femoral rollback
– Posterior translation femur with flexion
– Controlled by PCL
– Improves Quad function and knee flexion
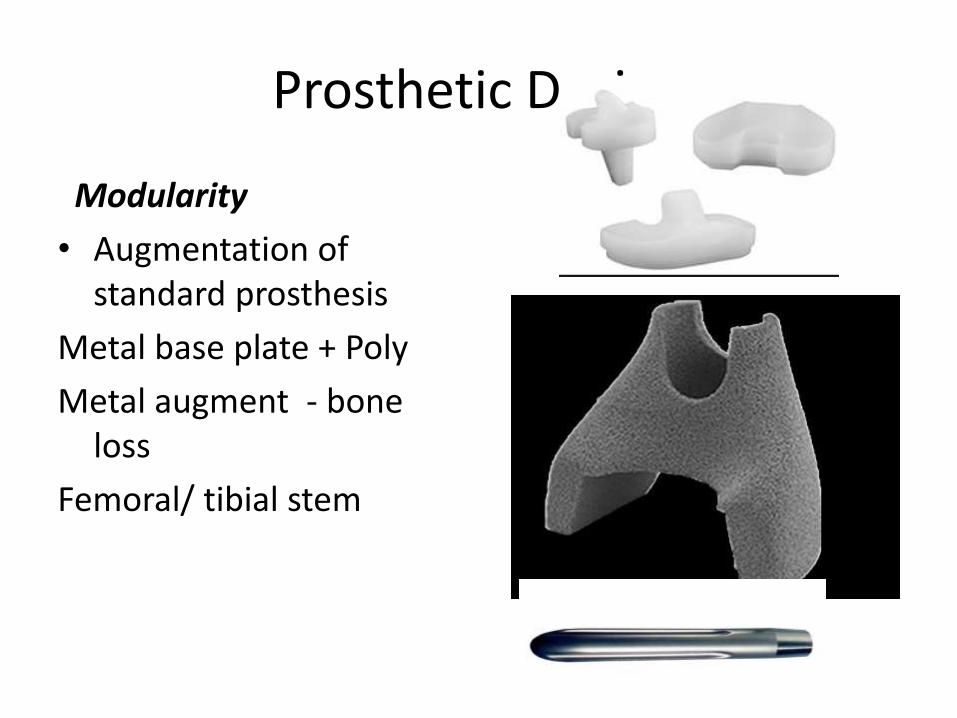
Prosthetic Design
Modularity
• Augmentation of standard prosthesis
Metal base plate + Poly
Metal augment - bone loss
Femoral/ tibial stem
Prosthetic Design
• Constraint
– Ability of prosthesis to provide varus – valgus and flexion –extension stability in presence of ligamentous laxity / bone loss
Prosthetic Design
• Cruciate retaining prosthesis (CR)
• Cruciate sacrificing prosthesis (CS)
• Varus – valgus constrained
• Hinged prosthesis
• Total condylar Prosthesis
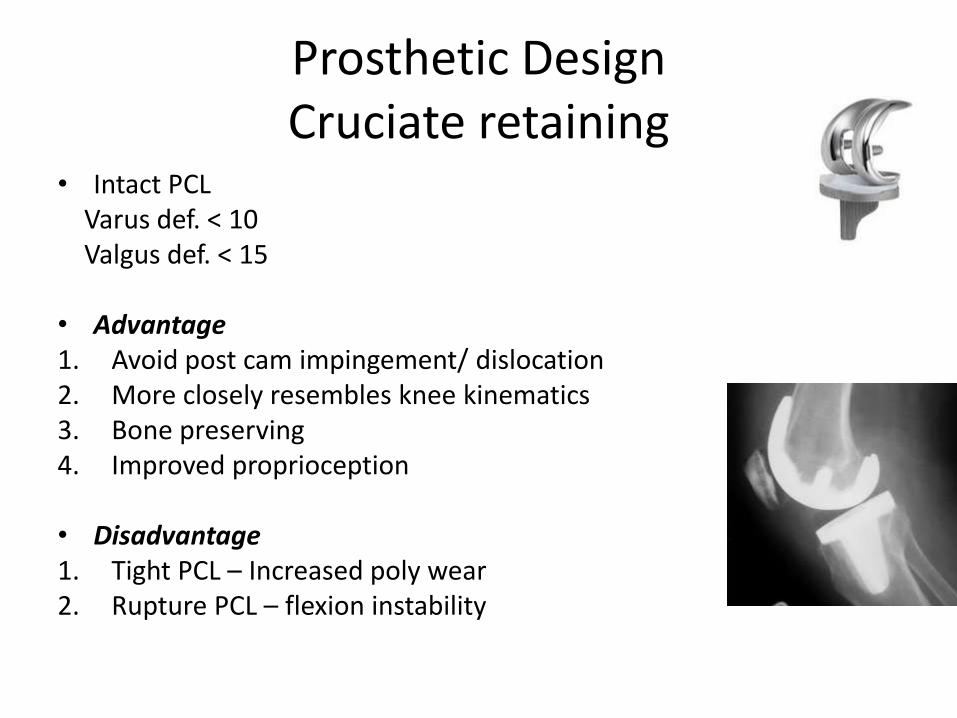
Prosthetic DesignCruciate retaining
• Intact PCLVarus def. < 10 Valgus def. < 15
• Advantage1. Avoid post cam impingement/ dislocation2. More closely resembles knee kinematics3. Bone preserving4. Improved proprioception
• Disadvantage1. Tight PCL – Increased poly wear2. Rupture PCL – flexion instability
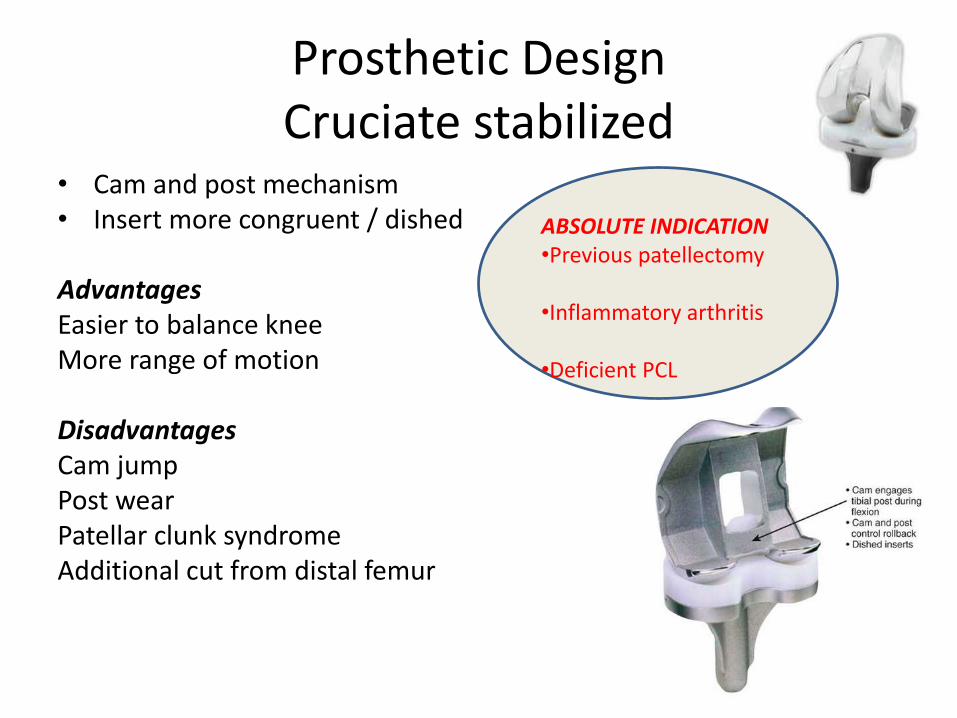
Prosthetic DesignCruciate stabilized
• Cam and post mechanism• Insert more congruent / dished
AdvantagesEasier to balance kneeMore range of motion
DisadvantagesCam jumpPost wearPatellar clunk syndromeAdditional cut from distal femur
ABSOLUTE INDICATION•Previous patellectomy
•Inflammatory arthritis
•Deficient PCL
Cruciate sacrifice / retain - Evidence
• PS increased ROM –No functional improvement
• No difference in ROM between PS and CR
• PCL does not work in CR knees
• Increased wear Ps knee – cam & post
Cochrane review – No difference in function whether cruciate retained
or sacrificed
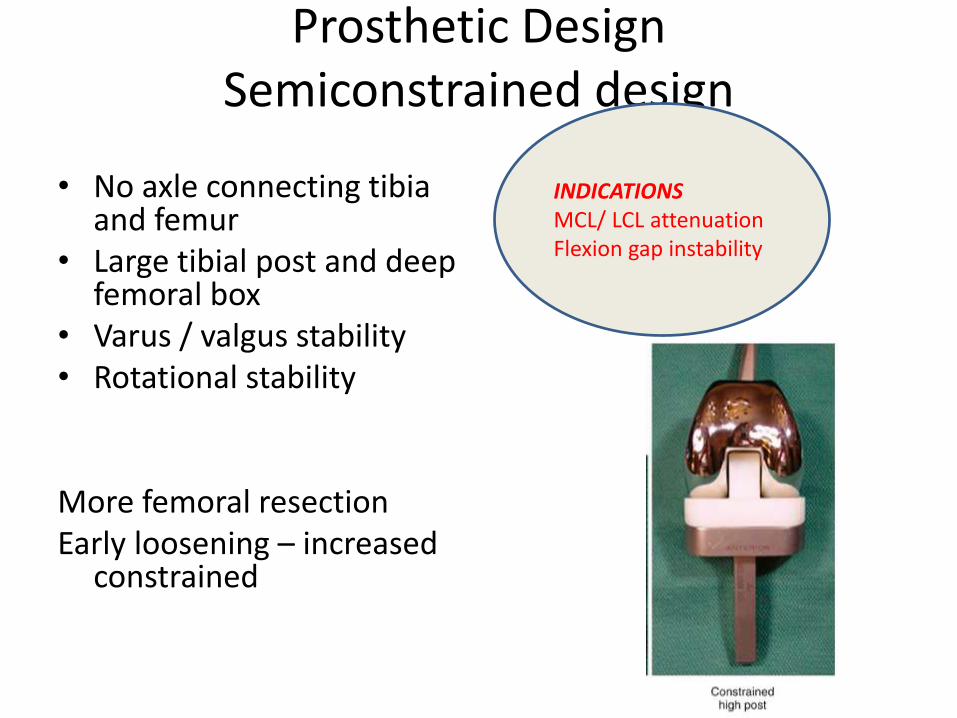
Prosthetic DesignSemiconstrained design
• No axle connecting tibia and femur
• Large tibial post and deep femoral box
• Varus / valgus stability• Rotational stability
More femoral resectionEarly loosening – increased
constrained
INDICATIONSMCL/ LCL attenuationFlexion gap instability
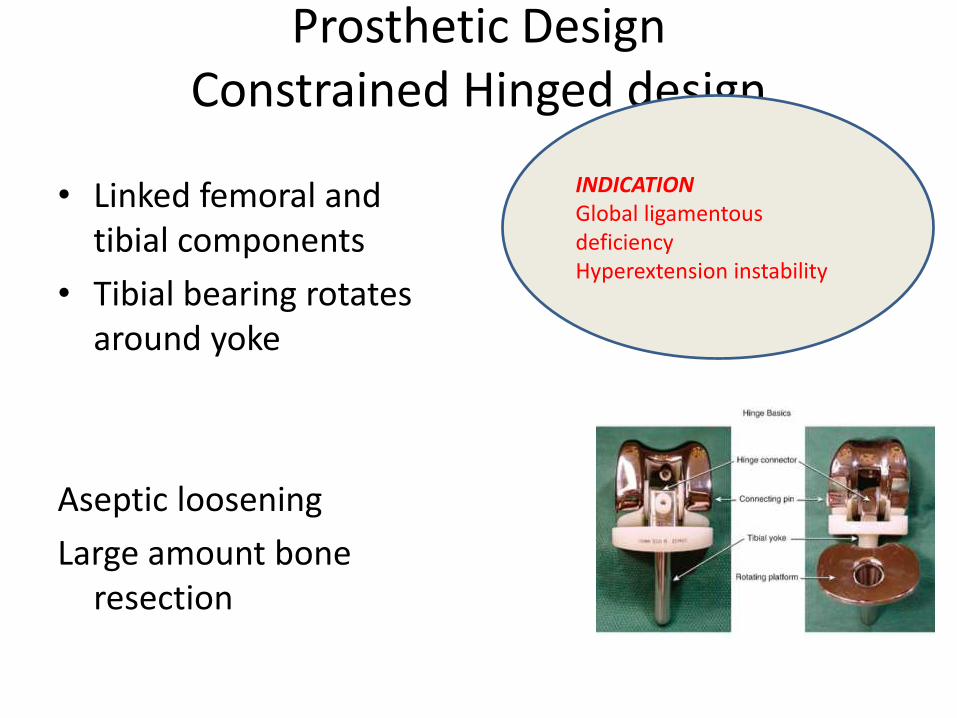
Prosthetic DesignConstrained Hinged design
• Linked femoral and tibial components
• Tibial bearing rotates around yoke
Aseptic loosening
Large amount bone resection
INDICATIONGlobal ligamentousdeficiencyHyperextension instability
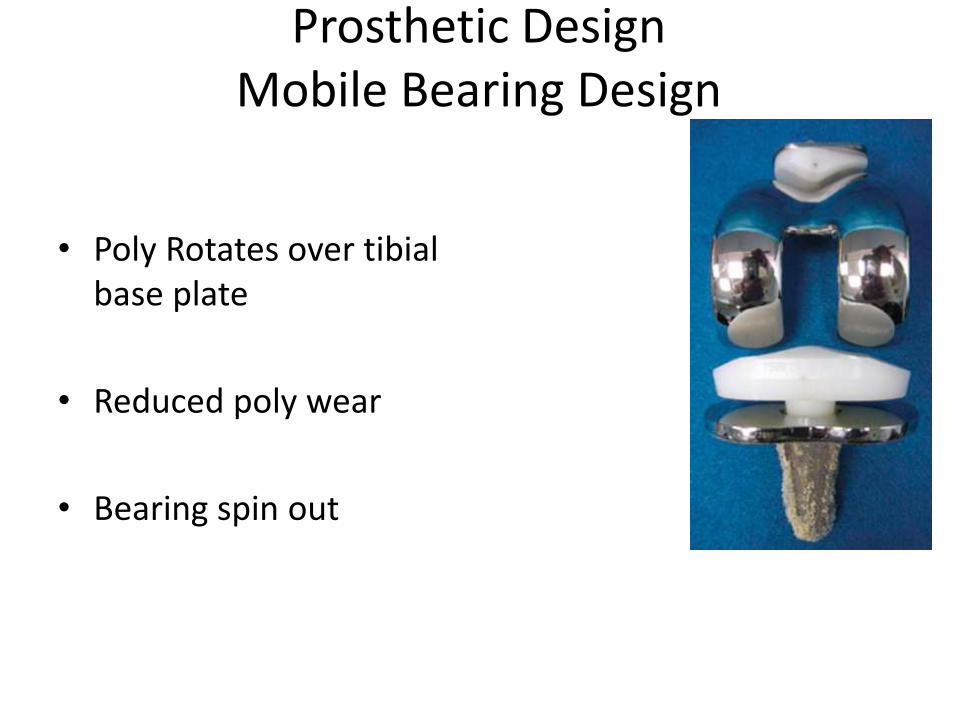
Prosthetic DesignMobile Bearing Design
• Poly Rotates over tibialbase plate
• Reduced poly wear
• Bearing spin out
Fixed Bearing or mobile bearing -Evidence
• No advantage of mobile bearing over fixed bearing
• Increased wear in undersurface of mobile bearing
Prosthetic DesignHi flex design
• Cultural / pt expectation
• Cut more posterior condyle
Preop flexion - most significant - Gatha etal 2008No difference in ROM - Mehin JBJS 2010
No difference in ROM Sumino Int Ortho 2010
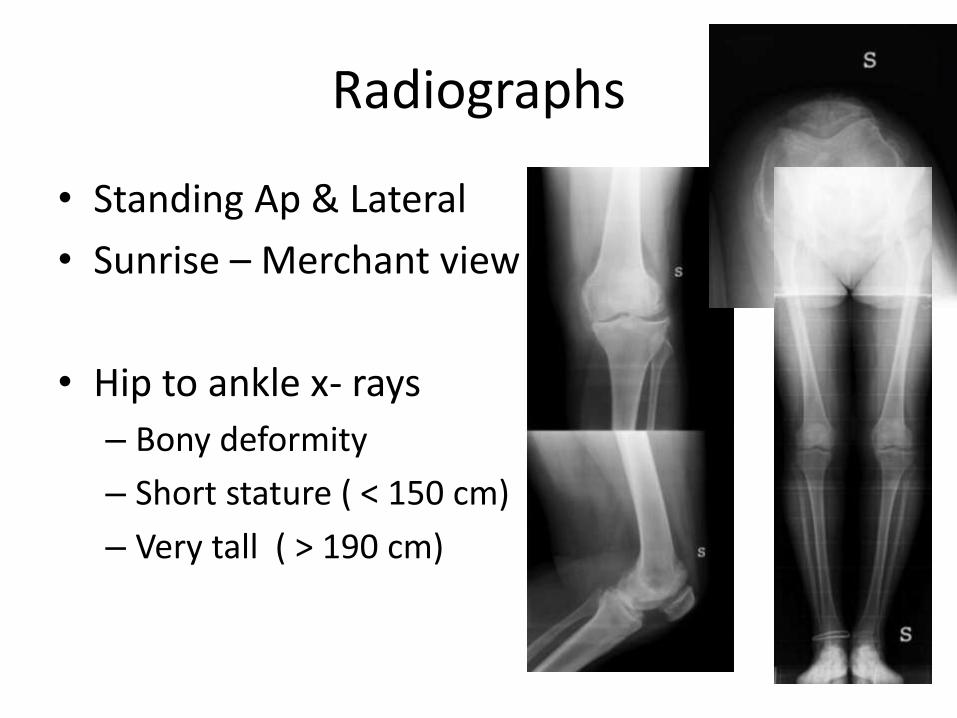
Radiographs
• Standing Ap & Lateral
• Sunrise – Merchant view
• Hip to ankle x- rays
– Bony deformity
– Short stature ( < 150 cm)
– Very tall ( > 190 cm)
Radiographs
• Femoral and tibial cut
• Position of femoral canal entry
• Bone defects
• Joint subluxation
• Ligament stretch out – Varus Thrust
• Ligament release
• Constraint needed
Approaches
• Multiple incision –choose lateral incision
• Previous transverse incision – cross at right angles
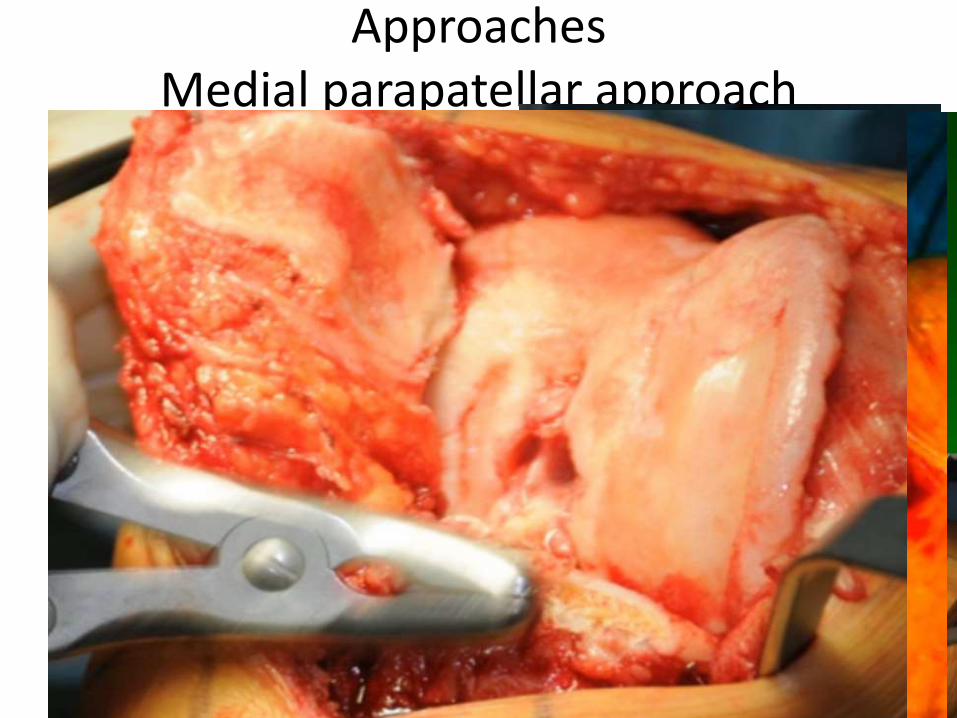
ApproachesMedial parapatellar approach
• Most common
• Surgeon are familiar
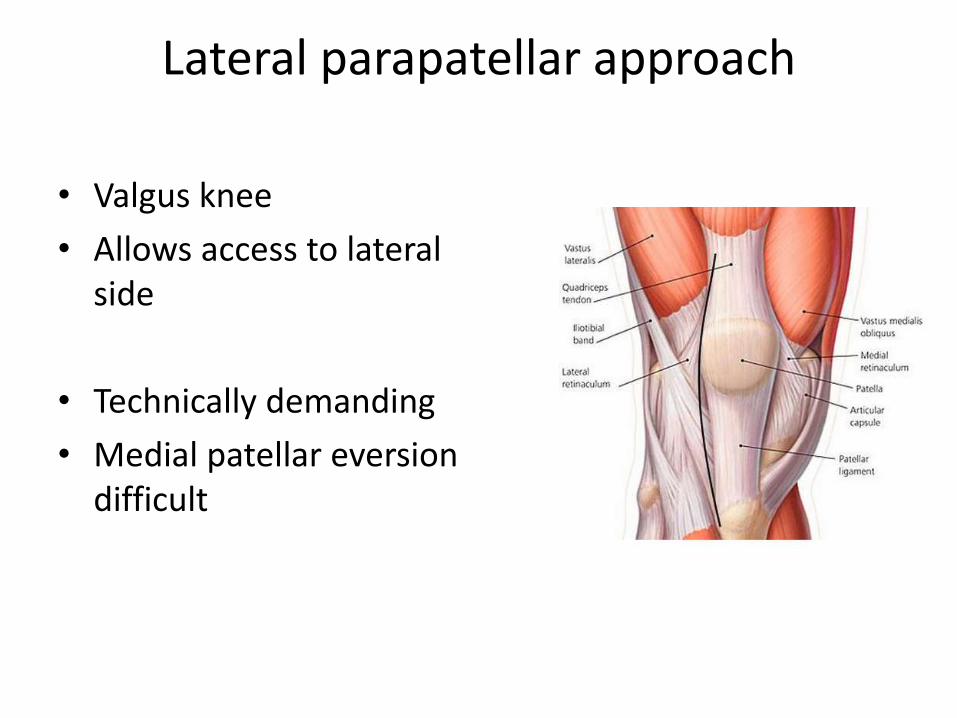
Lateral parapatellar approach
• Valgus knee
• Allows access to lateral side
• Technically demanding
• Medial patellar eversiondifficult
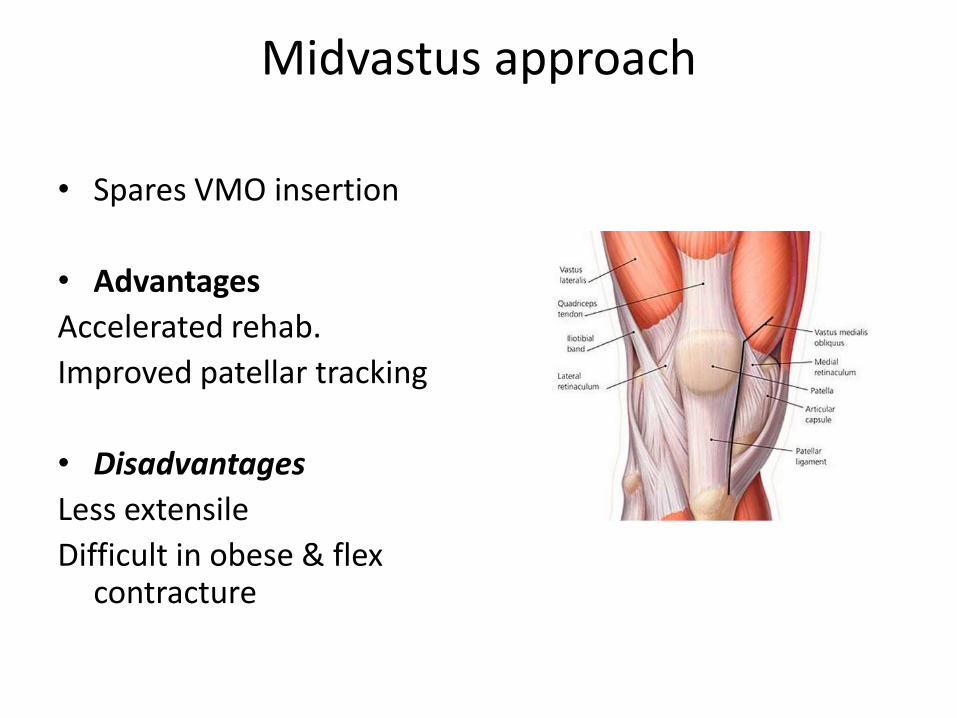
Midvastus approach
• Spares VMO insertion
• Advantages
Accelerated rehab.
Improved patellar tracking
• Disadvantages
Less extensile
Difficult in obese & flex contracture
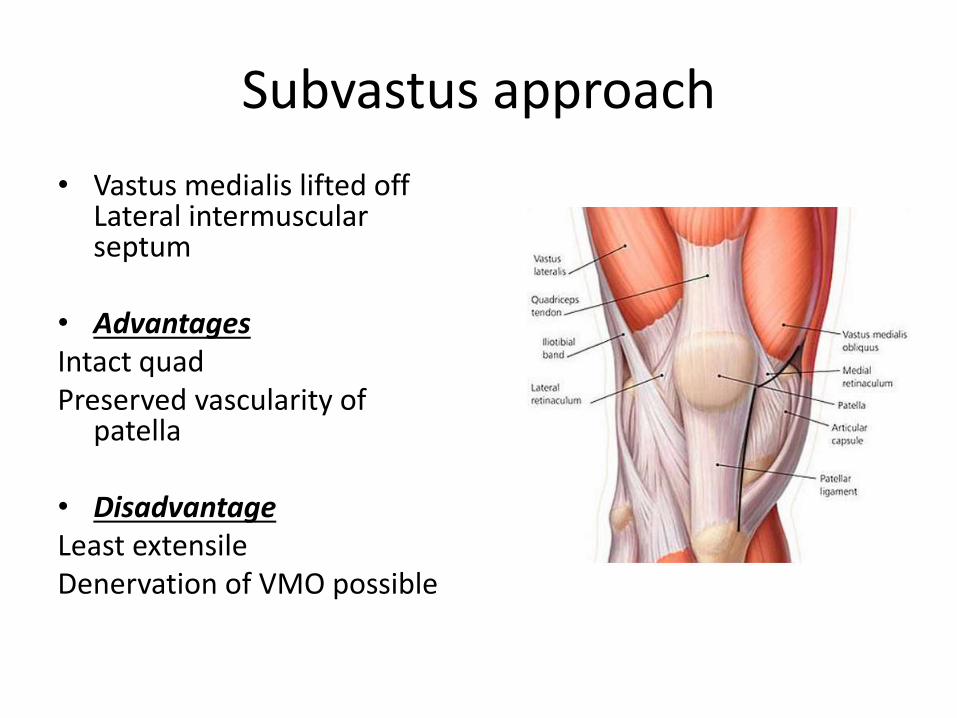
Subvastus approach
• Vastus medialis lifted off Lateral intermuscularseptum
• AdvantagesIntact quadPreserved vascularity of
patella
• DisadvantageLeast extensileDenervation of VMO possible
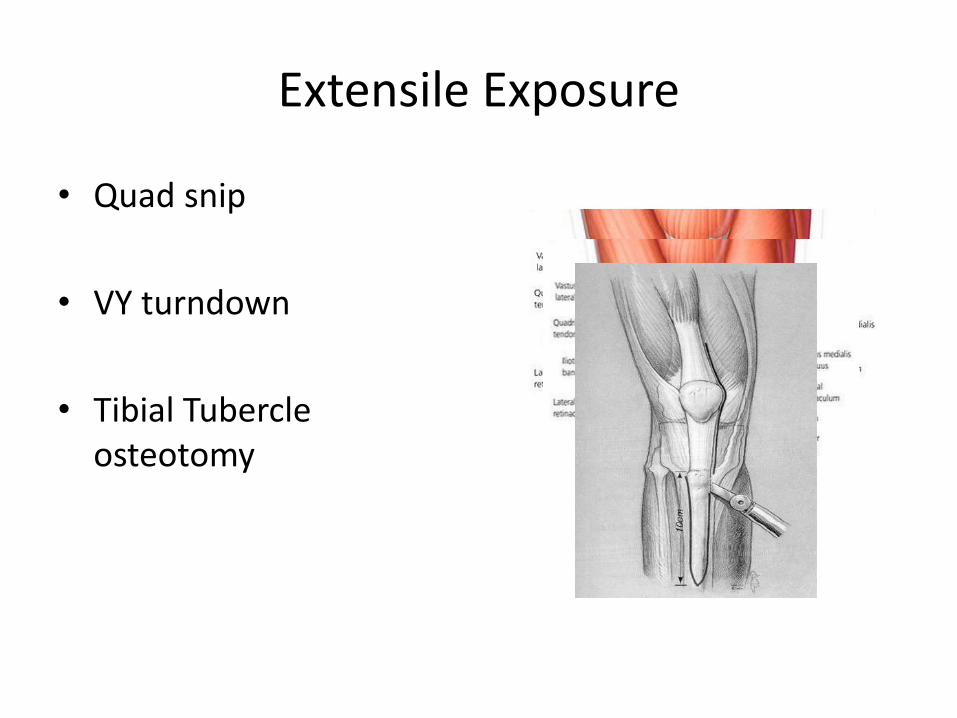
Extensile Exposure
• Quad snip
• VY turndown
• Tibial Tubercle osteotomy
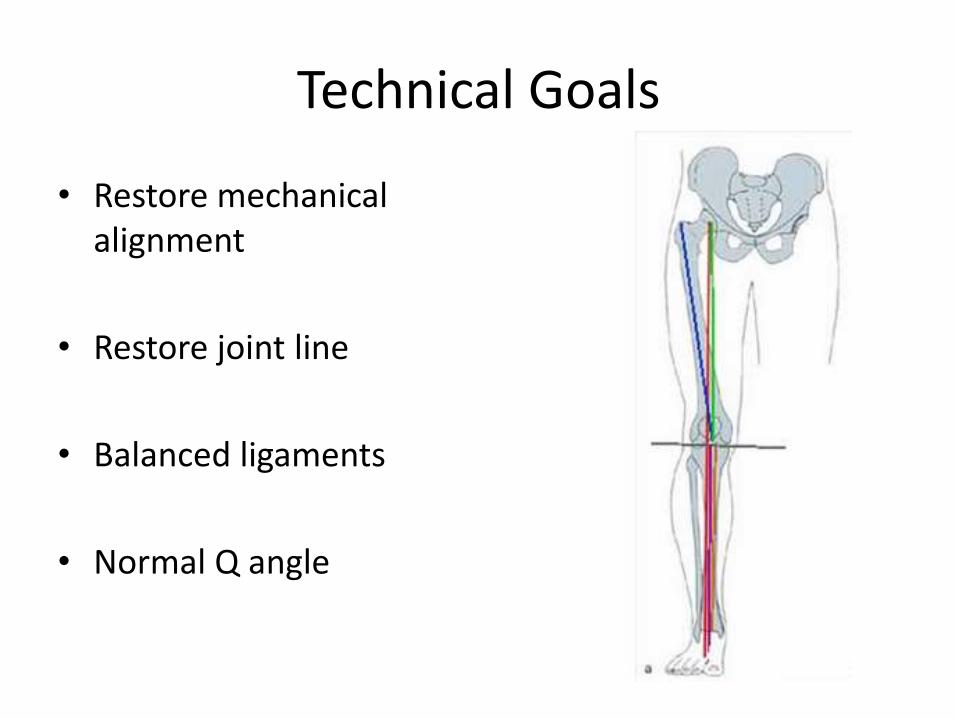
Technical Goals
• Restore mechanical alignment
• Restore joint line
• Balanced ligaments
• Normal Q angle
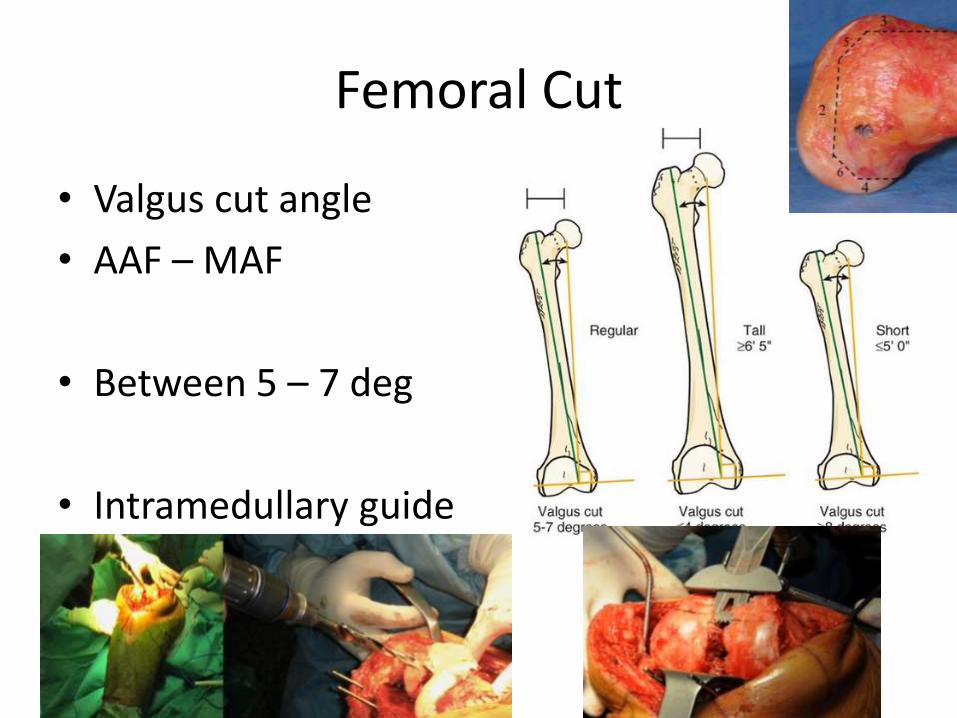
Femoral Cut
• Valgus cut angle
• AAF – MAF
• Between 5 – 7 deg
• Intramedullary guide
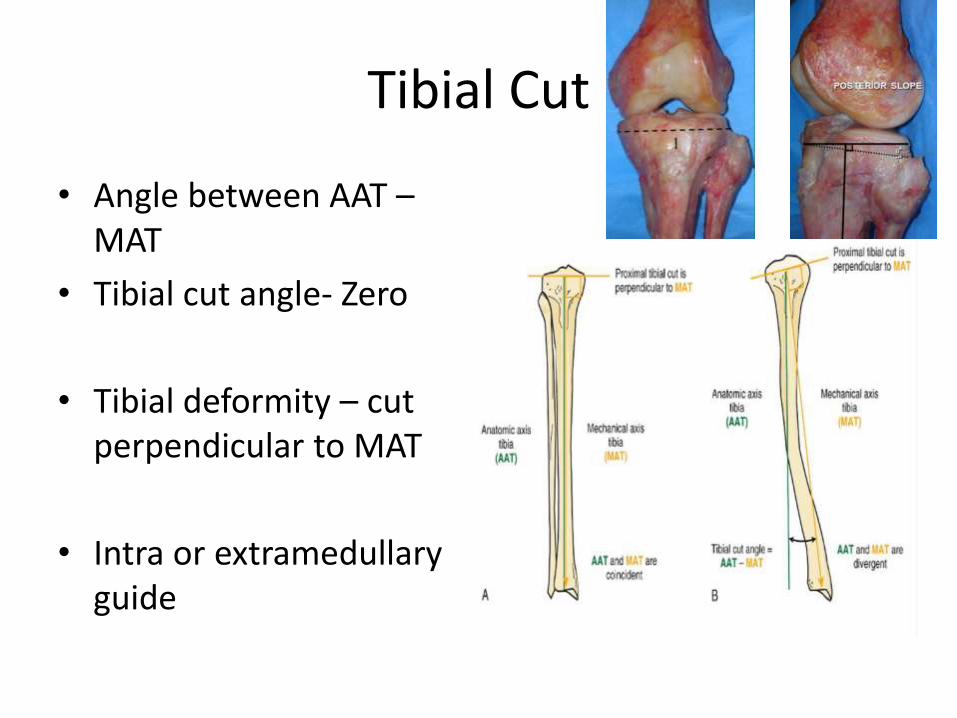
Tibial Cut
• Angle between AAT –MAT
• Tibial cut angle- Zero
• Tibial deformity – cut perpendicular to MAT
• Intra or extramedullaryguide
Joint line preservation
• Inserting prosthesis prosthesis same size as removed bone and cartilage
• Elevate joint line –mid flexion instabilityAbnormal patellofemoral trackingEquivalent to Patella Baja
• Lowering joint lineLack of full extension
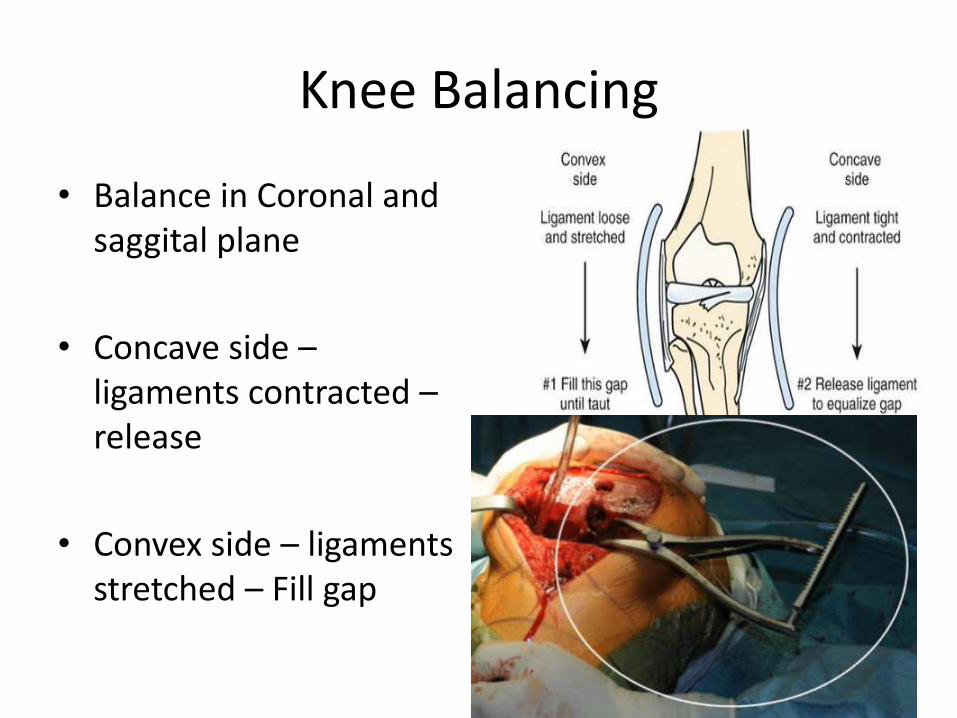
Knee Balancing
• Balance in Coronal and saggital plane
• Concave side –ligaments contracted –release
• Convex side – ligaments stretched – Fill gap
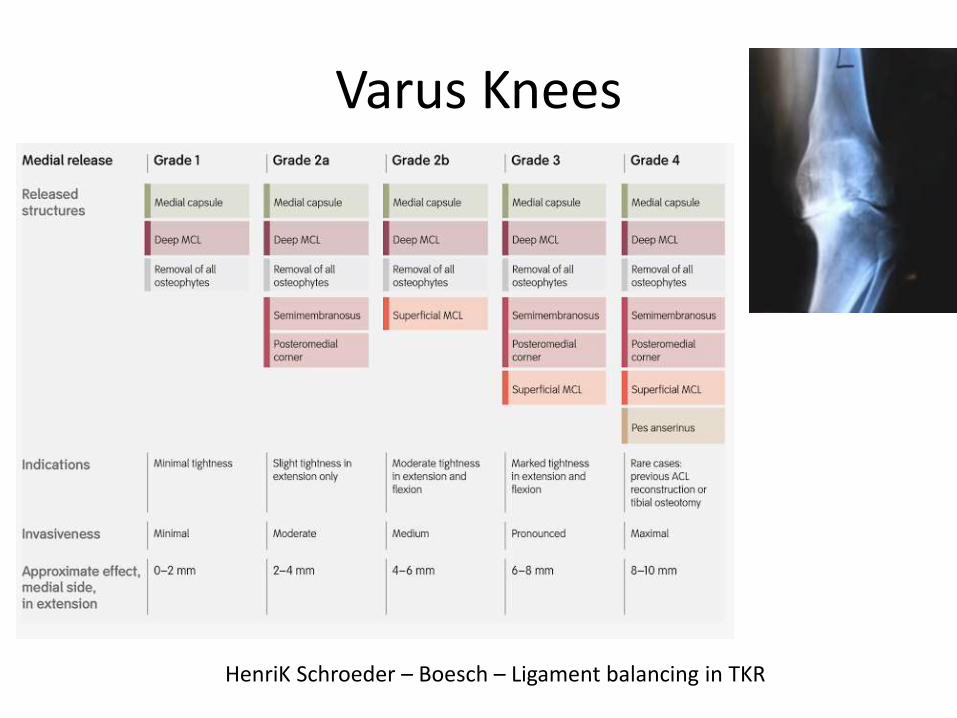
Varus Knees
HenriK Schroeder – Boesch – Ligament balancing in TKR
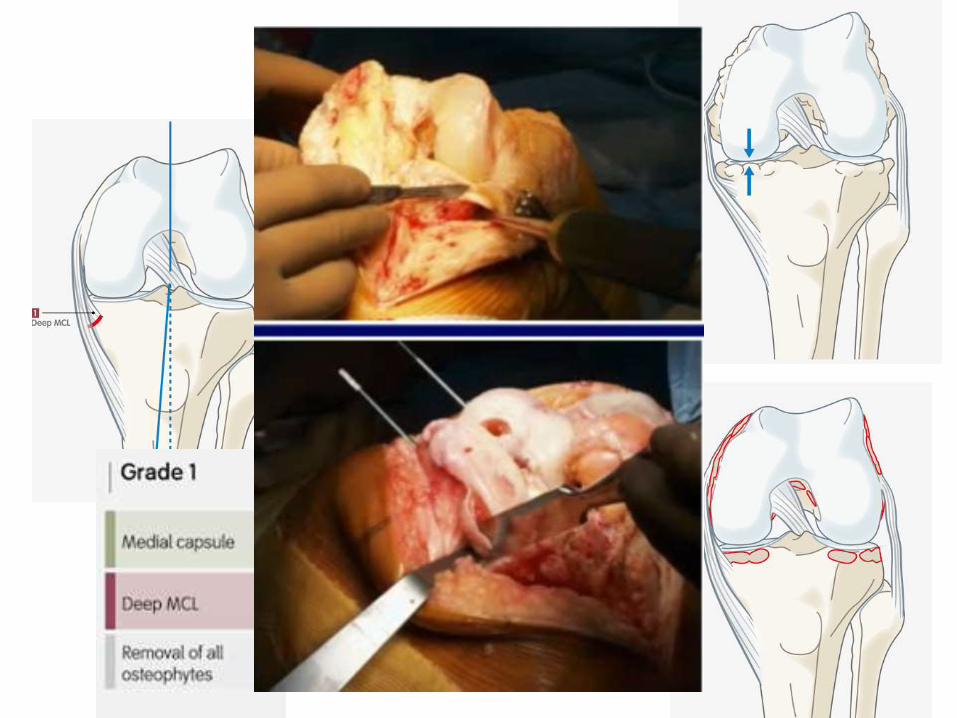
Grade 1 release
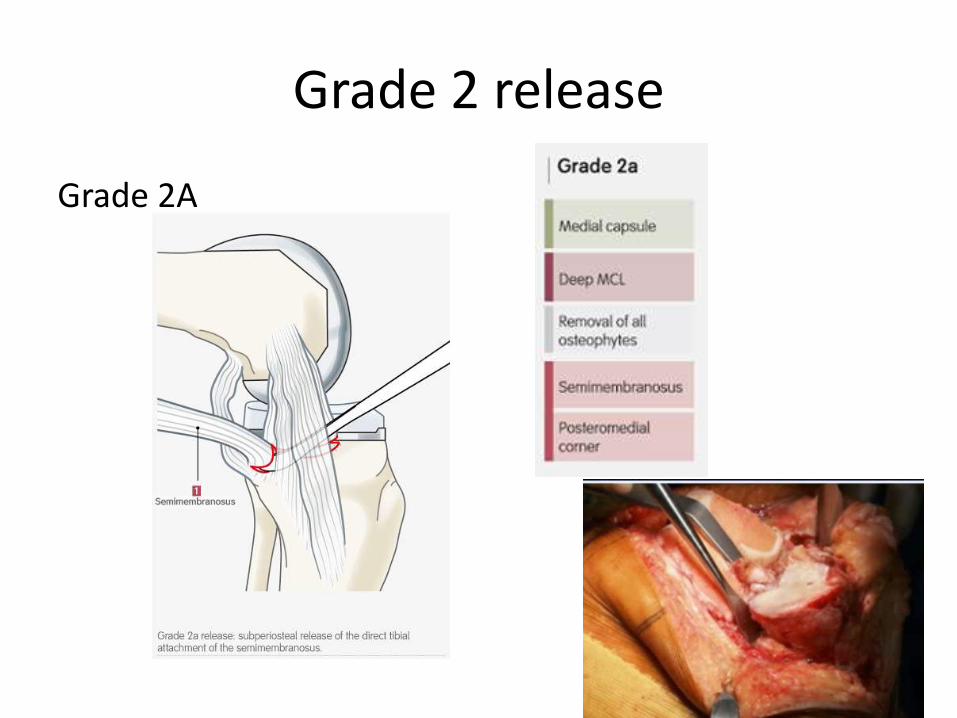
Grade 2 release
Grade 2A
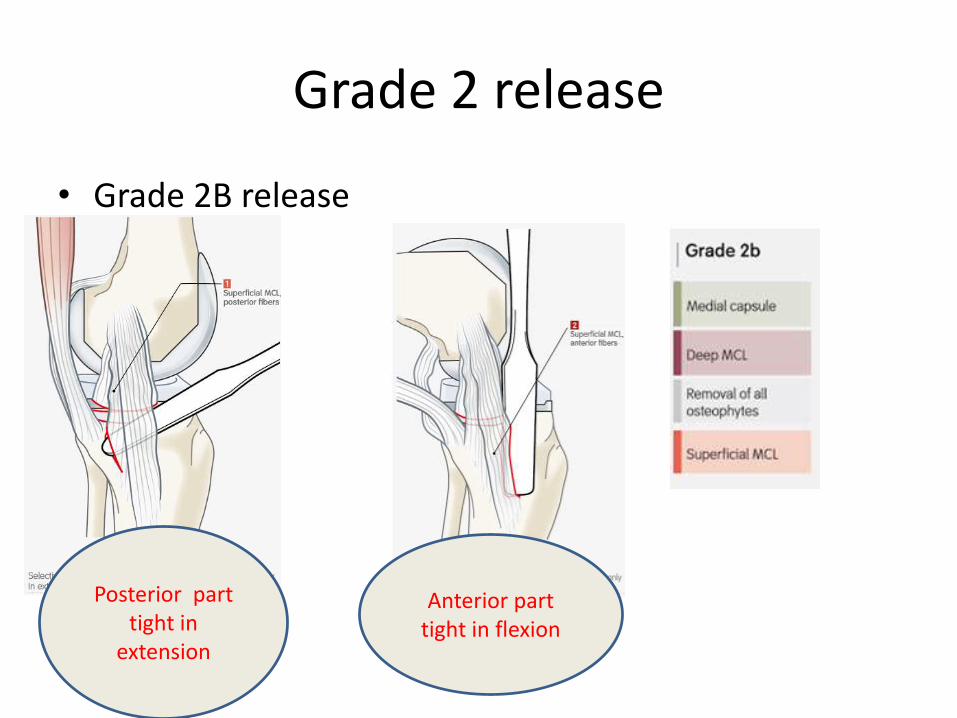
Grade 2 release
• Grade 2B release
Posterior part tight in
extension
Anterior part tight in flexion
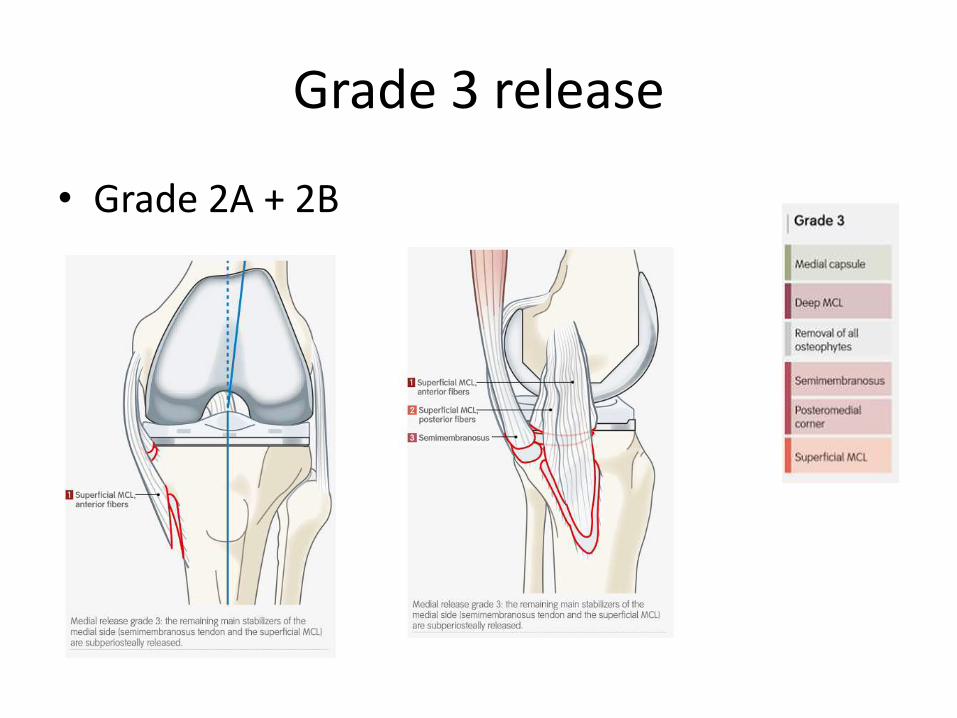
Grade 3 release
• Grade 2A + 2B
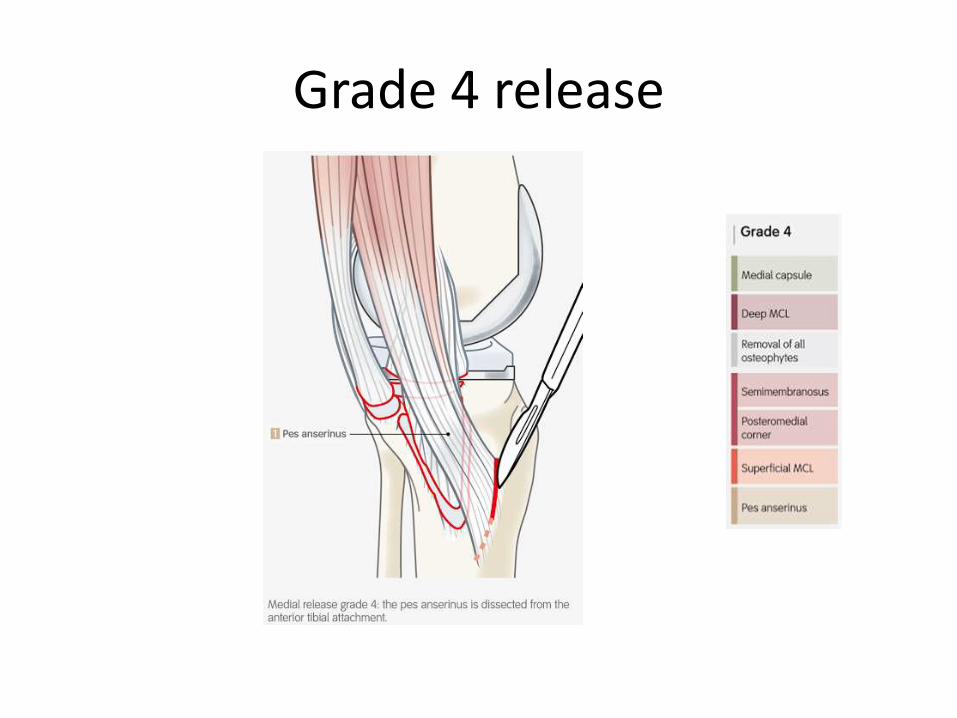
Grade 4 release
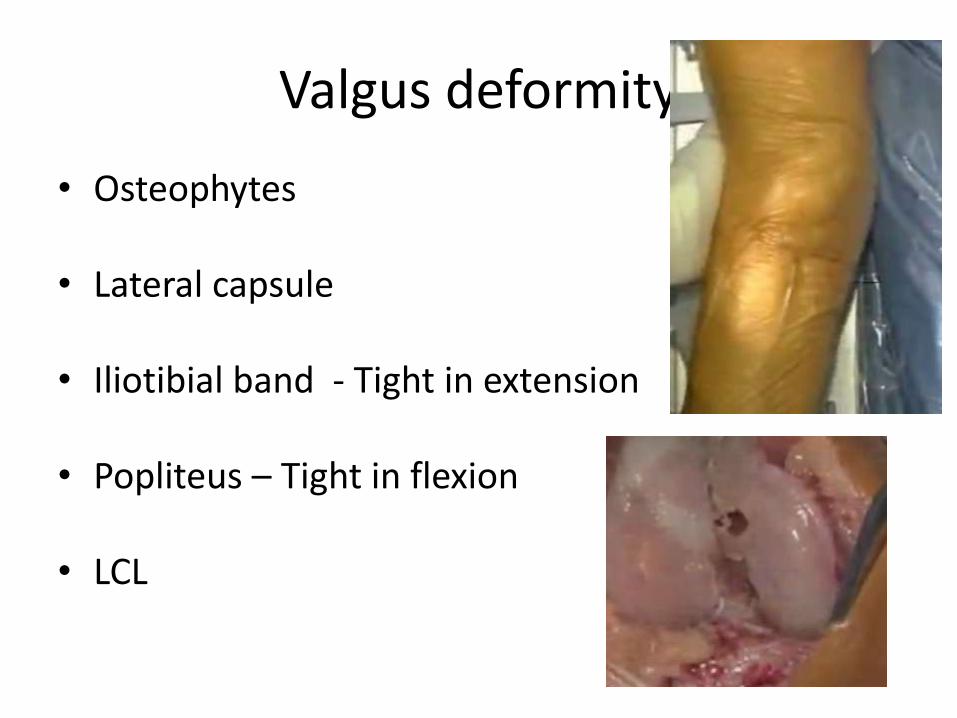
Valgus deformity
• Osteophytes
• Lateral capsule
• Iliotibial band - Tight in extension
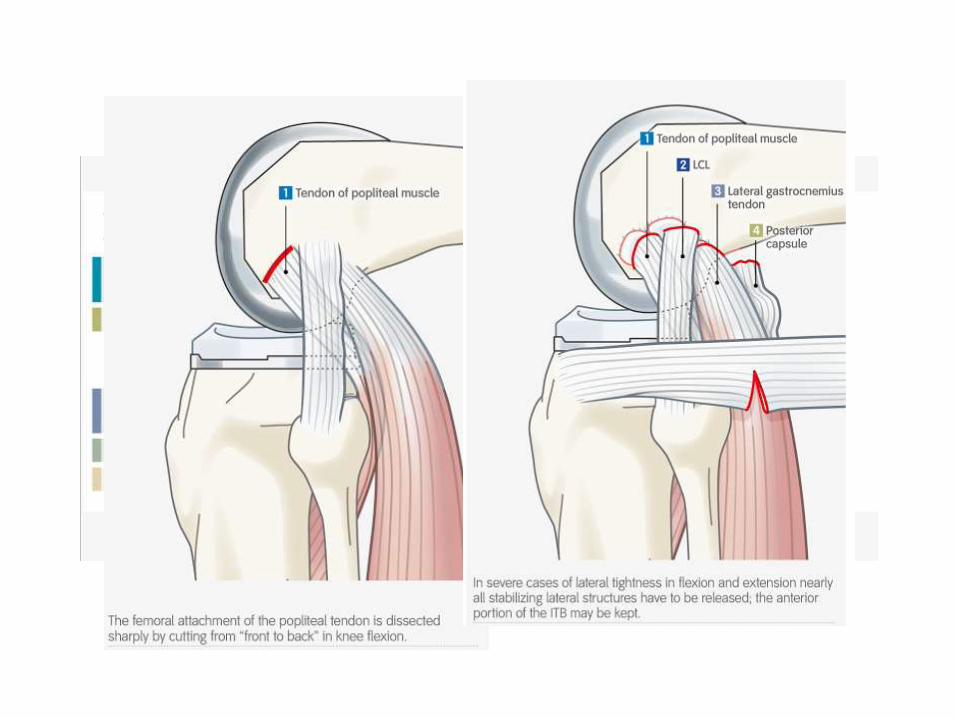
• Popliteus – Tight in flexion
• LCL
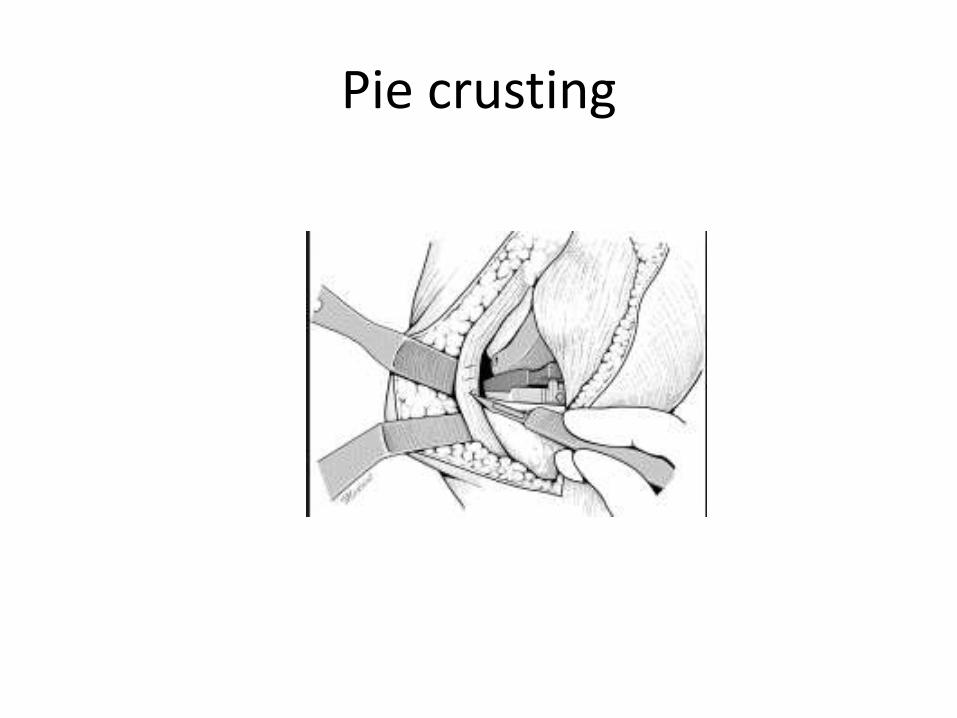
Pie crusting
Flexion contracture
• Osteophytes
• Posterior capsule
• Gastrocnemius ( Medial and lateral head)
• Inreased distal femoral cut
Sagital plane balancing
• Mc Pherson’s rule
Symmetric gap – address tibia
Asymmetric gap – address femur
Tight in Extension Tight in flexion
Symmetric gap Cut more tibia
Loose in Extension Loose in Flexion
Symmetric gap•Thicker poly •Tibial Metal augmentation
Extension good
Loose in flexionAsymmetric gap
1. Increase size femoral component
2. Translate femoral component posterior
3. Use thicker poly and readdress as tight extension gap
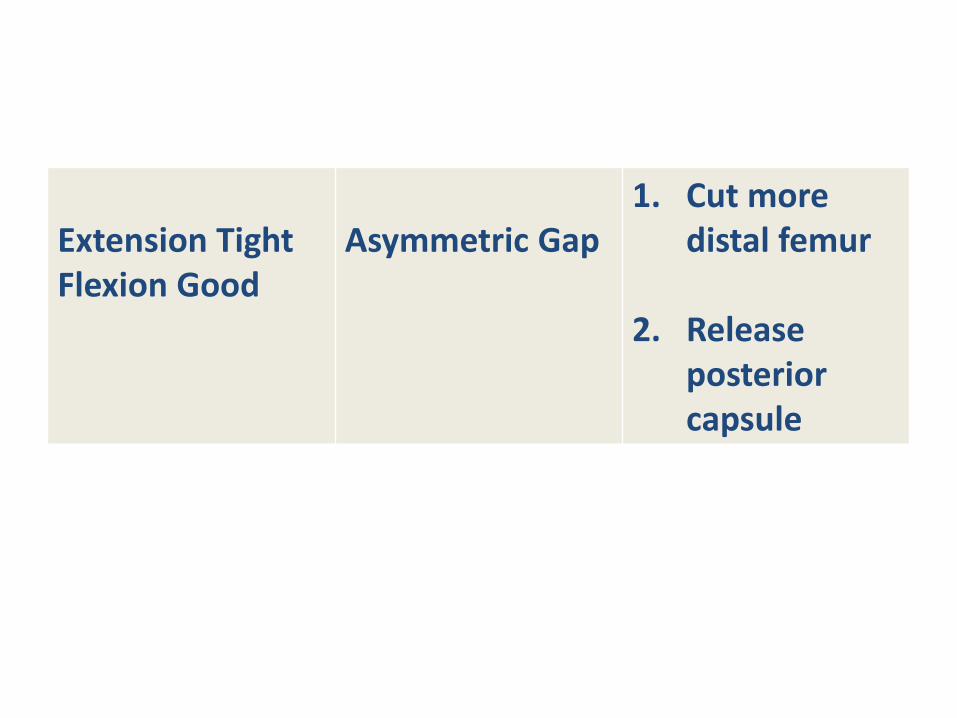
Extension TightFlexion Good
Asymmetric Gap1. Cut more
distal femur
2. Release posterior capsule
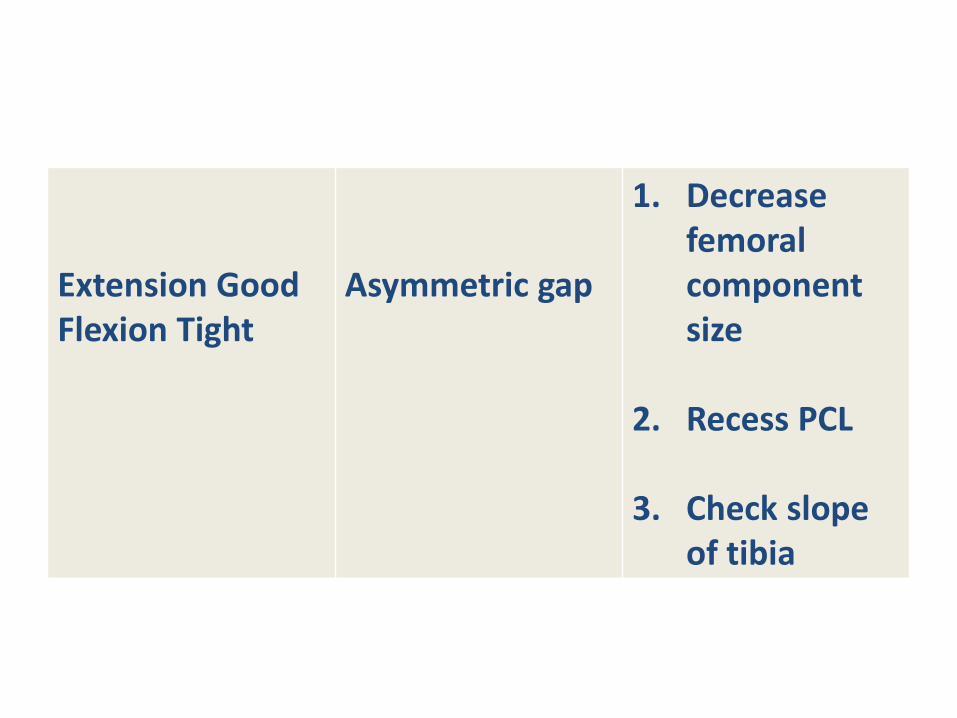
Extension GoodFlexion Tight
Asymmetric gap
1. Decreasefemoral component size
2. Recess PCL
3. Check slope of tibia
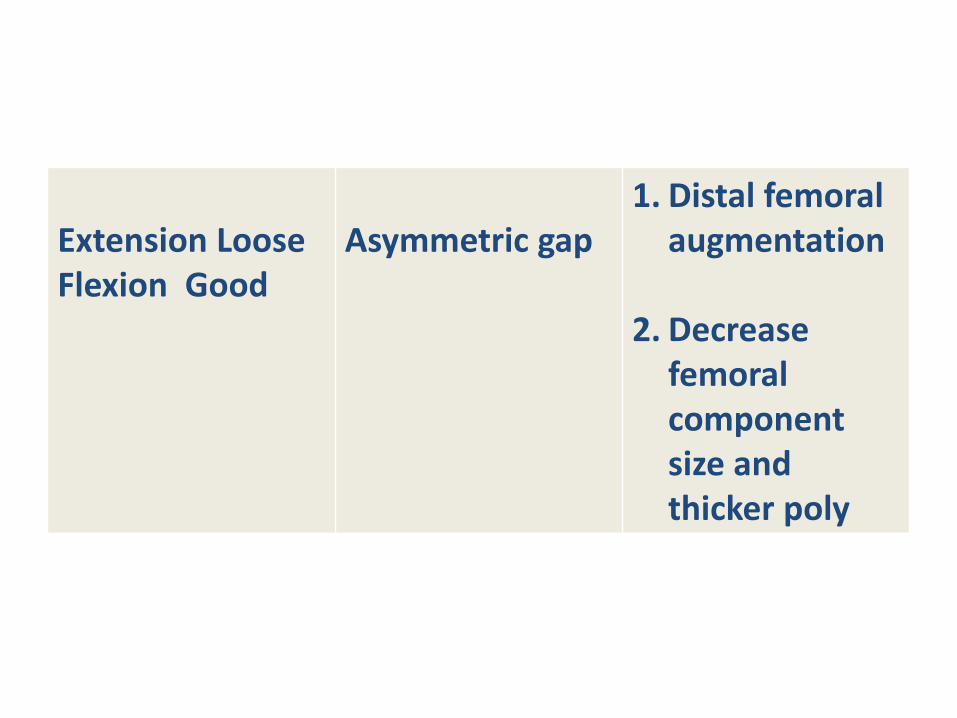
Extension LooseFlexion Good
Asymmetric gap1. Distal femoral
augmentation
2. Decrease femoral component size and thicker poly
Patellofemoral alignment
• Most common complication
• Maintain Q angle
• Proper component rotation
• Maintain normal patellofemoral tension
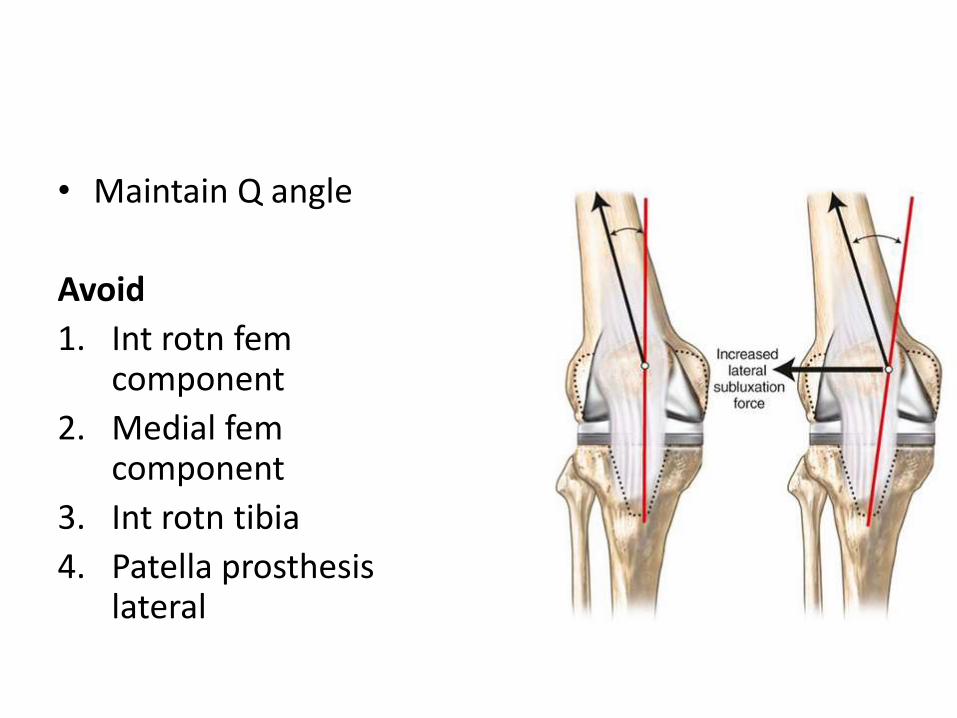
• Maintain Q angle
Avoid
1. Int rotn fem component
2. Medial fem component
3. Int rotn tibia
4. Patella prosthesis lateral
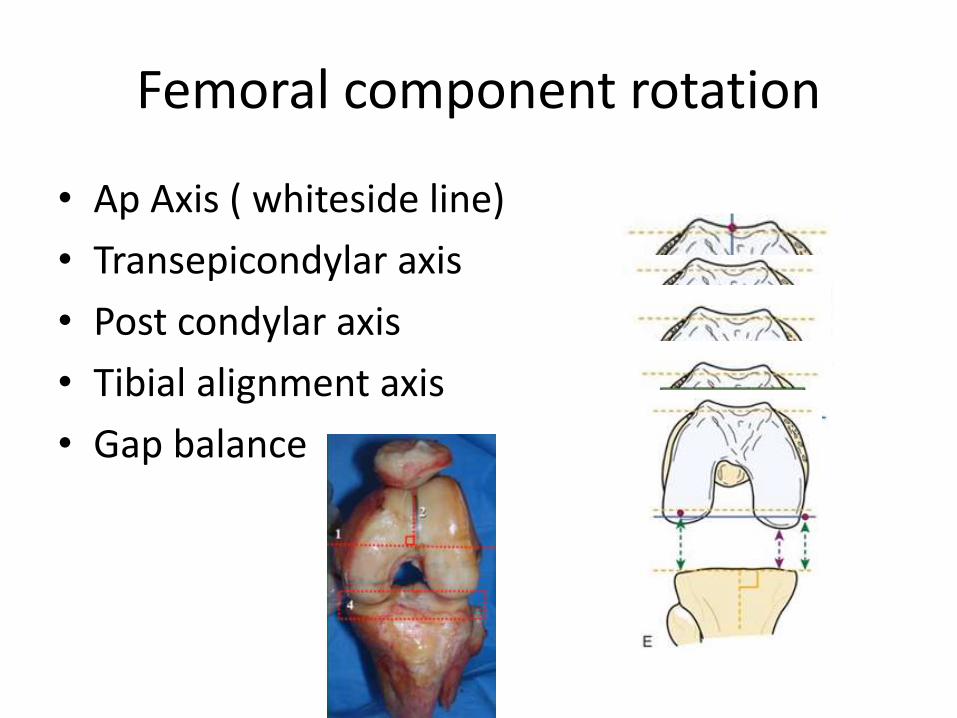
Femoral component rotation
• Ap Axis ( whiteside line)
• Transepicondylar axis
• Post condylar axis
• Tibial alignment axis
• Gap balance
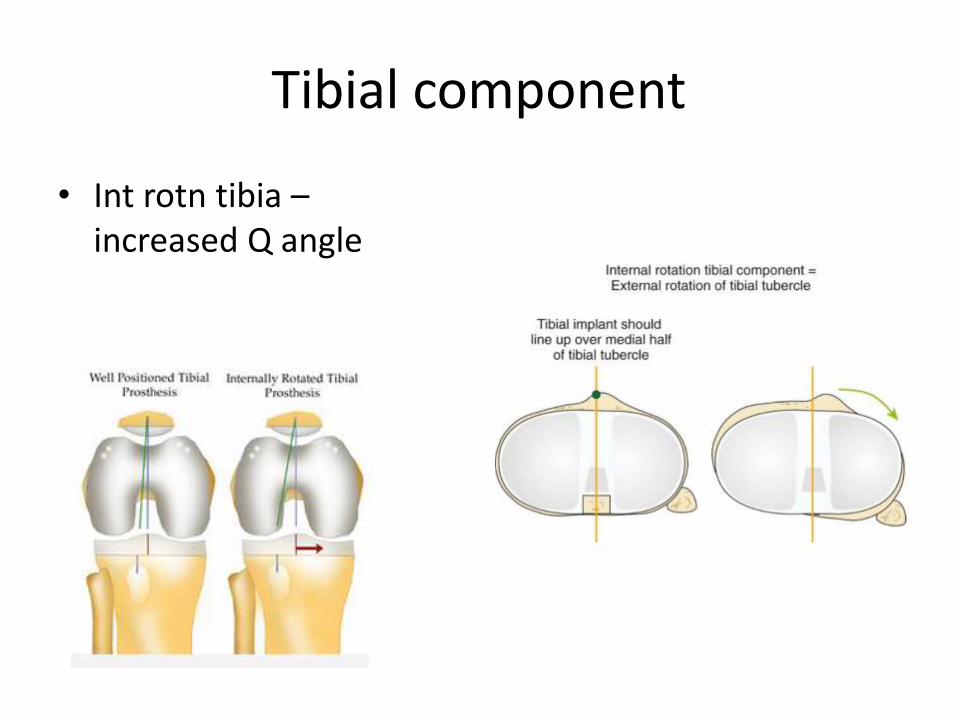
Tibial component
• Int rotn tibia –increased Q angle
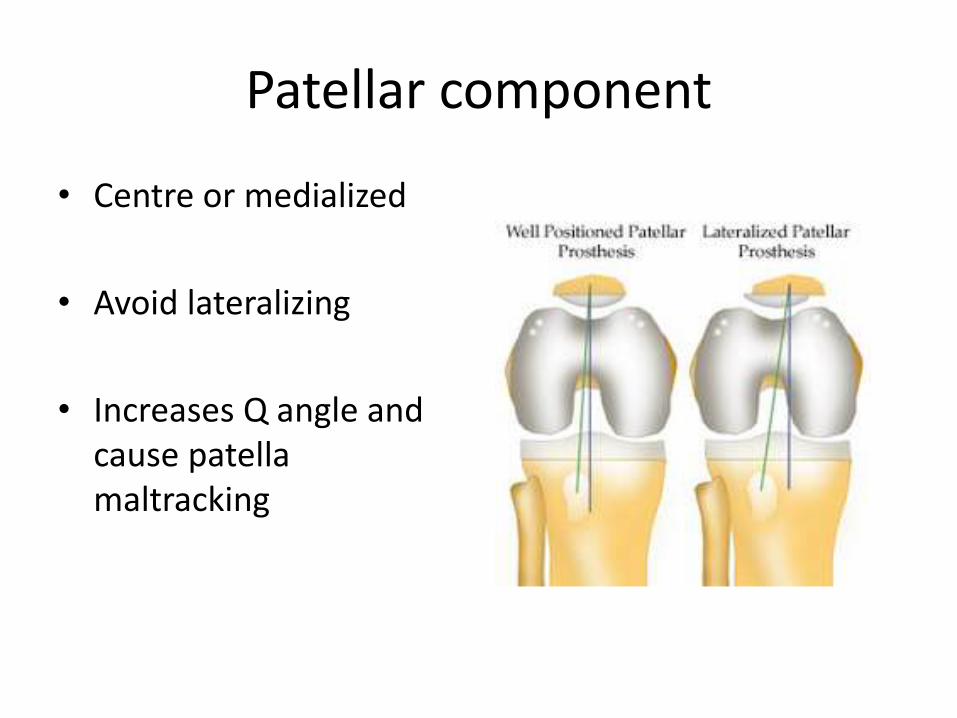
Patellar component
• Centre or medialized
• Avoid lateralizing
• Increases Q angle and cause patella maltracking
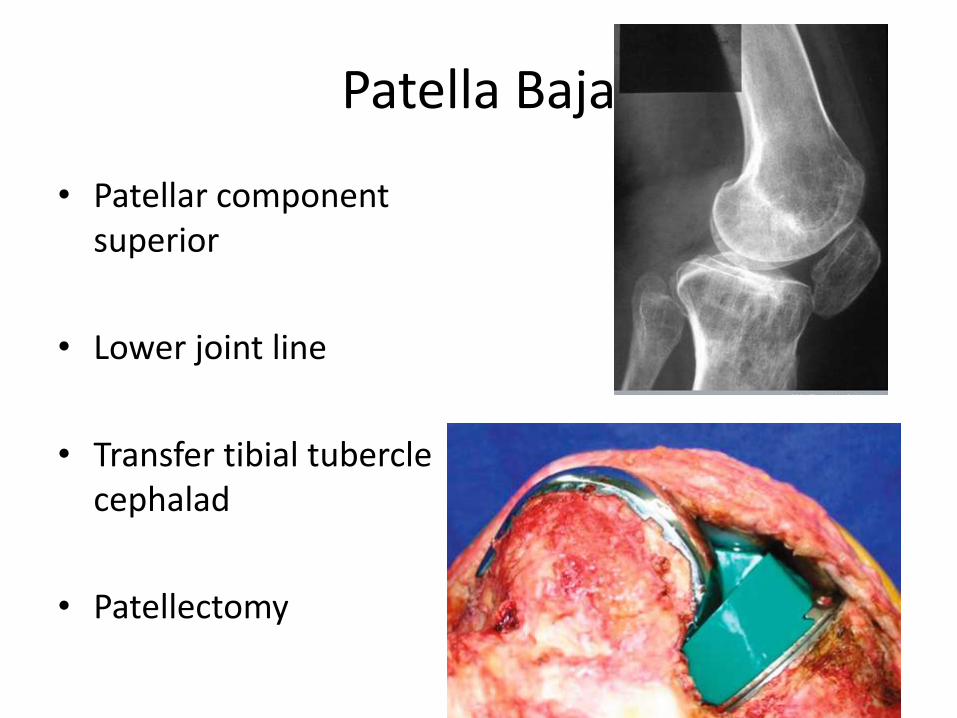
Patella Baja
• Patellar component superior
• Lower joint line
• Transfer tibial tubercle cephalad
• Patellectomy
Patella resurfacing vs non resurfacing
• Resurfacing
– Component loosening
– Clunk
– Fracture
– AVN
• Non resurfacing
– Anterior knee pain
– May require second resurfacing
Patellar resurfacing Vs non resurfacing - Evidence
• Metal backed patella higher complications
• Patellar replacement does not guranteepainless Patellofemoral joint
• No significant benefit of patellar replacement
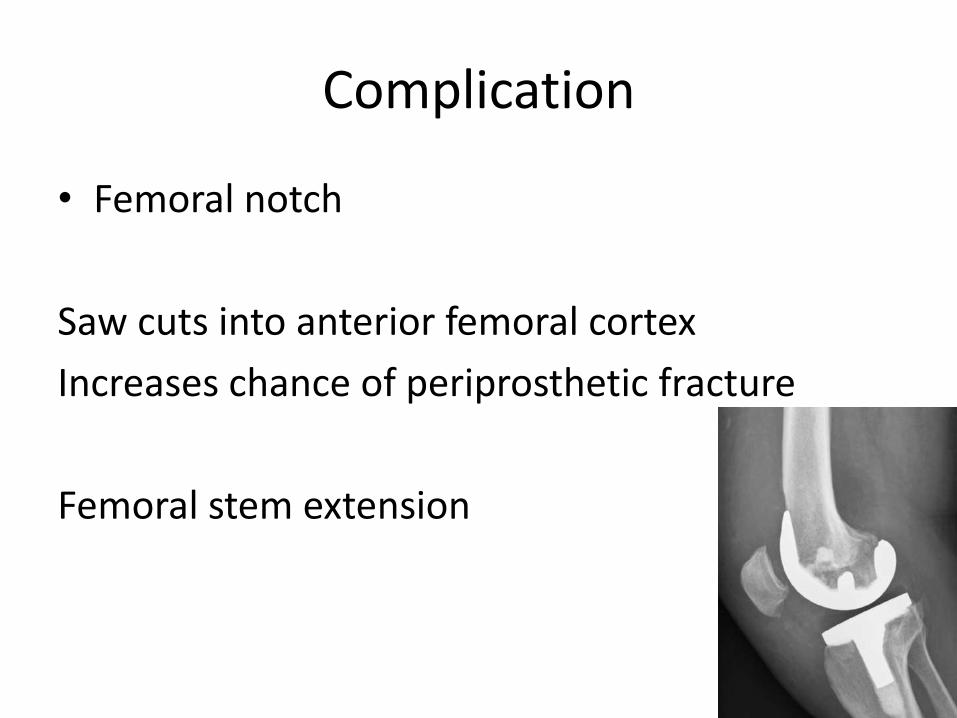
Complication
• Femoral notch
Saw cuts into anterior femoral cortex
Increases chance of periprosthetic fracture
Femoral stem extension
Complication
• Peroneal Nerve palsy ( .3 to 2 %)
Pre op Flexion and Valgus defTourniquete time > 120 min.Epidural anaesthesia post opAberrant retractor placement
EMG & NCV at 3 months
Nerve decompression at 3 months
Complication
• Vascular complication ( <.17% - .2%)
• Risk factor
– Sharp dissection
– Posterior retractor placement
– Pre existing vascular disease
– Immediate vascular repair
Complications
• Extensor mechanism rupture ( .17% - 2.5% )
– Direct repair with suture - < 30 % avulsion
– Primary repair and augment with graft
– Allograft repair
Complications
• Stiffness
– Flexion contracture 10 – 15 % deg
– Flexion < 90 deg
• Treatment
– Manipulation under Anaesthesia
– Arthroscopic lysis of adhesion
– Revision TKR
Complications
• Hypersensitivity
Rare ( nickel)
• Patch testing
• Lymphocyte transformation test
• Revise to non allergic metal prosthesis
Summary
• Choose correct pt
• Plan properly
• Adequate exposure
• Follow principles to align and balance knee
• Meticulous closure
Hope for the best because 20 % of pt. with well performed TKR are not happy !!

THANK YOU