primary care joint committees (pcjc) meetings care joint committees (pcjc) meetings . ... general...
TRANSCRIPT
Co-commissioning of Primary Care South East London’s CCGs and NHS England Primary Care Joint Committees
Primary Care Joint Committees (PCJC) Meetings
DATE OF MEETING: 11th February 2016
ENCLOSURE: J
Title: South East London CCGs and NHS England PMS Review Update
AUTHOR: Jill Webb, Head of Primary Care, South East London, NHS England SUMMARY: NHS England and the CCG’s in South East London have reviewed the services and standards currently commissioned through Local Personal Medical Services (PMS) agreements. The purpose of our review has been to ensure that PMS agreements deliver quality standards and meet the needs of the local population and are aligned to our current and future strategic objectives. The 2015/16 PMS review has considered how far PMS expenditure has been:
• paying for ‘core’ primary care services • paying for innovation and quality improvement in primary care, (premium payments) • paying for ‘enhanced’ primary care services (premium services).
The review will result in changes to current PMS agreements that ensure any additional investment in general practice services that goes beyond core national requirements will:
• reflect joint NHS England/CCG strategic plans for primary care • secure services or outcomes that go beyond what is expected of core general practice
or improve primary care • reduce health inequalities • give equality of opportunity to all GP practices, PMS, General Medical Services (GMS)
and Alternative Providers Medical Services (AMPS) • support fairer distribution of funding at a locality (borough) level.
1

NHS England (London) has now published the London Offer following consultation with London LMCs on behalf of primary care commissioners. Attached to this paper at Annexes 1-3 are:
• PMS Contract 2016/17 - Schedule 13 – Service Requirements • PMS Contract 2016/17 – Key Performance Indicators (KPIs) • PMS Premium Service Specification 2016/17
The key milestones following the relevant Joint Committees consideration and determination of local PMS Commissioning Intentions are as follows:
• Submission of Commissioning Intentions to NHS England (London) on 19 February 2016; CCGs complete outstanding work on local specifications and/or KPIs that underpin their local commissioning intentions, as appropriate, by 29th February 2016;
• Directors of Commissioning & Operations (DCOs) to review local CIs to assure these align with delivery of Strategic Commissioning Framework by 29th February 2016;
• Formal consultation with local LMCs (subject to confirmation of PMS practices’ mandates) on local commissioning intentions to be completed by mid-March 2016;
• NHS England (London) to write to PMS practices to set out local offer no later than 31 March 2016;
• Meetings with every PMS practices offered by NHS England (London) following conclusion of formal consultation with local LMCs. Meetings to be concluded by 20th May 2016;
• New contracts sent to PMS practices from 27th May 2016 for review and signature; • New PMS contract commences on 1st July 2016.
KEY ISSUES: This paper provides an update on the work and engagement that have been carried out by NHS England (London) and CCG officers in developing London-wide (the ‘London offer’) and local commissioning intentions. As Joint Commissioners of Primary Care, NHS England and CCGs have worked collaboratively on the development of commissioning intentions. This paper should be read in conjunction with the six attached (Annexes 4-9) cover sheets and completed Commissioning Intentions templates produced by the six south east London CCGs.
2
RECOMMENDATIONS: All Joint Committees are asked to note the London Offer documentation attached to this paper. The Bexley Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Bexley Clinical Commissioning Group subject to confirmation from NHS England (London) that an additional £1.13 pwpp is added to the CCG's budgets, as a first call on 2016/17 Primary Care growth, to cover the cost pressure of offering weekend additional capacity and to facilitate the offer of Improving Access through the use of technology specification. The Bromley Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Bromley Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Bromley Local Medical Committee, according to the timetable outlined. The Greenwich Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Greenwich Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Greenwich Local Medical Committee, according to the timetable outlined. The Lambeth Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Lambeth Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Lambeth Local Medical Committee, according to the timetable outlined. The Southwark Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Southwark Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Southwark Local Medical Committee, according to the timetable outlined. The Lewisham Primary Care Joint is recommended by the Lewisham Primary Care Programme Board to approve the PMS Commissioning Intentions for Lewisham Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Lewisham Local Medical Committee, according to the timetable
3
outlined.
NHS BEXLEY CCG CONTACT: Name: Theresa Osborne E-Mail: [email protected]
NHS BROMLEY CCG CONTACT: Name: Jessica Arnold E-Mail: [email protected]
NHS GREENWICH CCG CONTACT: Name: Simon Hall E-Mail: [email protected]
NHS LAMBETH CCG CONTACT: Name: Andrew Parker E-Mail: [email protected]
NHS LEWISHAM CCG CONTACT: Name: Diana Braithwaite E-Mail: [email protected]
NHS SOUTHWARK CCG CONTACT: Name: Caroline Gilmartin E-Mail: [email protected]
AUTHOR CONTACT: Name: Jill Webb E-Mail: [email protected]
4

South East London CCGs and NHS England PMS Review Update
1. Introduction Local Personal Medical Services (PMS) contracts are a patient-focused way of meeting specific needs, enabling GP Practices to be innovative in improving healthcare. The purpose of the PMS review is to ensure that PMS funding is aligned to services which best meet the needs of the whole local population, and that where it is not, it is reinvested into GP services across the Clinical Commissioning Group (CCG) area. There will be no reduction in the level of GP funding in each CCG area as a result of this review. Co-Commissioners (NHS England and CCGs) need to ensure that every GP practice across the country is paid according to the national principles for the review for the services they provide to patients and every penny spent gets maximum value for local people. PMS agreements are locally agreed contracts between NHS England and named members of a GP practice. PMS agreements were developed in 1998 to offer local flexibility compared to the nationally negotiated General Medical Services (GMS) contracts. They allowed commissioners and providers the opportunity to extend the range of services provided by the practice, the financial arrangements for those services and the provider structure (who can hold a contract). PMS agreements were formalised in 2004 to ensure they incorporated the mandated range of core services, as well as services which can go beyond standard requirements (premium services and standards). They frequently attracted additional funding. However it was not always clear how funding aligned to core services and premium services and standards. The additional services, standards and the funding attached to PMS contracts was negotiated locally by PCTs, and typically funded the provision of services for the specific practice population – e.g., diagnostic testing or specialist clinics. Nationally the extra funding in PMS (after taking into account equivalent funding in the General Medical Services [GMS] contract for the services expected of all practices and recycling of the Minimum Practice Income Guarantee) was calculated at £235 million in 2013-14. PMS funding for London amounted to £90 million in 2014-15. PMS contracts currently cover around 40% of GP practices across the country and 46% of GP practices in London. NHS England guidance is clear that any proposals to reduce the current level of funding that a PMS GP practice receives should reflect decisions on how the money will be reinvested into GP services in the CCG area. Timing of CCG proposals for reinvestment will be locally led, reflecting the need for PMS reviews to be carried with 2014/15 being year one. The review period started on April 2014 and all reviews should be completed by 31 March 2016 and implemented by 30 June 2016.
5
2. Context Nationally, there is no relationship between current PMS expenditure and deprivation. Modelling shows a random distribution of PMS premium against the Index of Multiple Deprivation (IMD) scores. There also appears to be no relationship between PMS premium funding and GP Outcome Standards measures. Any additional investment in general practice services that goes beyond core national requirements (whether this is deployed through PMS or through other routes) is expected to:
• reflect joint NHS England/ CCG strategic plans for primary care • secure services or outcomes that go beyond what is expected of core general practice • help reduce health inequalities • support fairer distribution of funding at a locality level
3. South East London PMS review (2015) On 1 April 2013, NHS England was given statutory responsibility for the direct commissioning of primary care contracts. The NHS England review of PMS agreements has consequently needed to be applied consistently across the four regions that make up NHS England. The intention of the national review was set out in guidance from Ben Dyson and Ann Sutton in February 2014. The guidance stated that all NHS England Area Teams must carry out PMS reviews by March 20161 and that the PMS review should:
• seek best value from the premium element of PMS practice funding • ensure that any funding over and above the core element should
be clearly linked to Area Team/CCG strategic plans for primary care should secure services or outcomes that go beyond what is expected of core
general practice of improving primary care premises make a clear contribution to reducing health inequalities Give equality of opportunity to all GP practices and not just PMS contracts Enable a fairer distribution of funding at locality level
• not reduce the overall level of investment going in to general practice In London key principles for delivering the review have been:
• The review will establish an agreed cost per weighted patient for the delivery of the agreed specification across all PMS providers at CCG level.
• Transitional financial support for up to 2 years and 4 years where exceptional circumstances are evidenced by practices as part of negotiations with NHS England following the initial offer to practices by the end of March 2016 (where appropriate);
1 To note: timescales for London were extended by 3 months in December 2015
6

• Funding not invested in PMS requirements will be invested in general practice for locally specific services.
Through a combination of the PMS review and primary care commissioners’ commitment to implementing the Strategic Commissioning Framework (SCF), NHS England (London), with its 32 CCGs aims to equalise the consequent service offer to all practices and their patients in a locality. This means that patients should not see a variation in the service offer within a CCG, where appropriate. CCGs are expected to equalise as soon as possible, with the contribution their PMS review is making to implementing the SCF and pace of equalisation clearly set out in their PMS Commissioning Intentions and Sustainability and Transformation Plans to be submitted in June 2016. Where a CCG has sufficient resources to achieve equalisation in 2016/17, it is expected that this should be implemented in order to achieve transformation at a greater pace of change. It is however acknowledged that the level of funding differs within CCGs and therefore needs to be assessed with regard to affordability.
4.1 South East London approach to the PMS review As Joint Commissioners of Primary Care, the CCGs and NHS England have a Joint role in making decisions relating to the review and ensuring that the review is implemented in line with the national mandate. In particular, on a practical basis, this means that the CCGs in South East London have been required to:
• Undertake a review of the outcomes and services currently delivered by PMS practices locally;
• Undertake a review of the current funding for services locally, looking specifically at PMS practices as part of the PMS review;
• Where there are differential levels of funding in PMS practices, identify an equitable pound per patient value for PMS premium services within the CCG and the services to be commissioned from the funding available;
• Provide NHS England with finalised commissioning intentions information at CCG level with details of local service specifications and KPIs to follow;
• Have a plan for equalisation to all practices within the CCG which will be delivered as soon as possible and before the end of the current planning cycle.
7

5 PMS review Commissioning Intentions for 2016/17
5.1 London Offer engagement The London Offer has been developed by NHS England (London) in collaboration with Co-Commissioners via the London wide PMS Stakeholder Reference Group (SRG) attended by Strategic Planning Group (SPG) leads for Primary Care. As a result, a number of significant revisions have been made. NHS England (London) has specifically consulted London Local Medical Committees (LMCs) on the London offer. 5.2 The London Offer
The areas identified for inclusion within the London offer are based on the Strategic Commissioning Framework (SCF) for Primary Care in London, a Framework which was developed through wide spread engagement across a wide array of stakeholder groups. The offer has been shared with CCGs for consideration as part of local commissioning intentions. Local commissioning intentions should be agreed and submitted to NHS England (London) by 19 February 2016. The services included in the London offer are shown below.
CCGs are required to select, based on affordability, from a menu of options, with the mandatory KPI element compulsory for commissioners to ensure a London wide offer to PMS practices.
Element Description Cost per weighted patient
Mandatory for PMS?
Cor
e Core Contract
A description of core required services. Consistent with GMS
GMS Equivalent
Yes
Pre
miu
m
Weekend Additional Capacity (WAC)**
Each practice opening for 4 consecutive hours at the weekend, over and above core PMS service provision.
£4.00 (including clinical, non-clinical, overhead &
No
8

indemnity costs)
Additional Technology Use
• 50% of appointments should be available (& cancellable) online by 1st April 2017
• Patients should be able to order repeat prescriptions
• Practices must offer electronic consultations
£1 No
KP
I
Mandatory • Cervical screening • Childhood, flu &
Pneumococcal imms • Patient voice (2 indicators –
CCG choice)
£3.04 Yes
Additional • Breast screening • Access to services
£1.36 No
The total cost of London offer is £9.40 based on per weighted patient. **However, the WAC specification is priced based on actual, not weighted patents. This will therefore result in the price of the London Offer showing small differences from practice to practice & CCG to CCG, dependent on the relative difference between weighted and actual patients. This has been factored into CCG’s Commissioning Intentions templates – on a CCG average basis - where CCGs propose to commission WAC based on the London offer. The London Offer documentation can be viewed at Annex 1-3 and comprises:
9

• PMS Contract 2016/17 - Schedule 13 – Service Requirements • PMS Contract 2016/17 – Key Performance Indicators (KPIs) • PMS Premium Service Specification 2016/17
5.3 CCG Commissioning Intentions for Premium Funding South East London CCGs have considered how they will structure the local element of the offer to PMS and their plans for equalisation to GMS & APMS practices. The table below provides a CCG level summary of the impact of the cost of the mandatory London offer on each of the CCG’s premium funding for investment in their local commissioning intentions.
SOUTH LONDON CCGs
PMS Budget Ave PMS premium April 15
Mandatory KPI £PWP
Premium available for local commissioning
Southwark £ 5,179,304.00 £19.84 3.04 £16.80 Lambeth £ 4,862,317.00 £16.12 3.04 £13.09 Lewisham £ 3,359,365.00 £12.14 3.04 £9.10 Greenwich £ 2,615,698.00 £10.24 3.04 £7.20 Bromley £ 2,161,869.00 £11.38 3.04 £8.34 Bexley £ 1,410,853.00 £7.16 3.04 £4.12
The six SE London CCG’s actual Commissioning Intentions, together with cover papers with their high level summaries can be viewed at (Annexes 4 to 9). 5.4 Managing Impact and Transition Payments
South East London CCG’s will not be using the PMS premium to equalise to GMS & APMS practices, as each currently intends to invest additional funding into the equalisation of GMS and APMS practices. Please refer to their respective Commissioning Intentions templates.
10

6 Next steps The key milestones following the relevant Joint Committees consideration and determination of local PMS Commissioning Intentions are as follows:
• Submission of Commissioning Intentions to NHS England (London)on 19 February 2016; CCGs complete outstanding work on local specifications and/or KPIs that underpin their local commissioning intentions, as appropriate, by 29th February 2016;
• Directors of Commissioning & Operations (DCOs) to review local CIs to assure these align with delivery of Strategic Commissioning Framework by 29th February 2016;
• Formal consultation with local LMCs (subject to confirmation of PMS practices’ mandates) on local commissioning intentions to be completed by mid-March 2016;
• NHS England (London) to write to PMS practices to set out local offer no later than 31 March 2016;
• Meetings with every PMS practices offered by NHS England (London) following conclusion of formal consultation with local LMCs. Meetings to be concluded by 20th May 2016;
• New contracts sent to PMS practices from 27th May 2016 for review and signature; • New PMS contract commences on 1st July 2016.
11

Personal Medical Services Contract 2016/17: Service Requirements
Reviewer Date Change summary Version
Alex Mears 23/11/2016 Version control table added to beginning of service requirement, based on comments and feedback
received
V4
Kelly Poole 24/11/2015 Amendment to text, from “PCT” to “NHSE”
V4.1
Alex Mears/Kelly Poole
24/11/2015 Added evidence text box to links/documents applicable to the document
V5
Alex Mears 26/11/2015 IT issue so higher version control number added, no content change made.
V6-8
Alex Mears 27/11/2015 Amendments made to reflect recommendations from SR working group
V9
Kelly Poole/Alex Mears
2/12/2015 Rationale and Evidence added. V10
Alex Mears 7/12/2015 Amended to add training requirements
V11
Alex Mears 9/12/15 Add final KPIs to list in appendix V12
Alex Mears 11/12/2015 Remove draft highlighting, amend mandatory KPI value. Final version post PCMB (10/12/15)
V13
Alex Mears 14/12/2015 Remove rationale and evidence, add clause re closing for training
V14
Julie Sands 06/01/2016 Amend according to agreements with LMC 6/1/16
V15
Alex Mears 20/01/2016 Amended according to agreements with LMC 20/1/16
V16
Alex Mears 04/02/2016 Final typos amended following LMC advice
V17
12
Annex 1

Contents Part 1: general service delivery requirements ........................................................................................ 3
1. Equity of access ........................................................................................................................... 3
2. Patient Dignity & Respect ........................................................................................................... 3
3. Informed Consent ....................................................................................................................... 3
4. Children ...................................................................................................................................... 3
5. Clinical Safety & Medical Emergencies ........................................................................................ 4
6. Referrals ...................................................................................................................................... 5
8. Practitioner Skill Mix/Continuity................................................................................................. 5
9. Patient Records ........................................................................................................................... 5
10. Contractor Records ............................................................................................................... 6
Part 2 – Services ..................................................................................................................................... 7
1. Services To Be Provided By The Contractor ................................................................................. 7
2. Patient Voice ................................................................................................................................... 7
3. End of life care ................................................................................................................................ 7
4. Enhanced services ........................................................................................................................... 7
Part 3: access to services ........................................................................................................................ 7
1. Routine Opening hours............................................................................................................... 7
2. Provision of Reception Services ................................................................................................. 8
3. Registration Policy ...................................................................................................................... 8
4. Appointments .............................................................................................................................. 8
5. Booking an Appointment ............................................................................................................ 9
6. Length of Appointments ............................................................................................................. 9
APPENDIX 1: PATIENT REGISTRATION AREA AND OUTER BOUNDARY AREA .................. 10
APPENDIX 2: ONCE FOR LONDON GP PATIENT REGISTRATION OPERATING PRINCIPLES .......................................................................................................................................................... 11
13

Part 1: general service delivery requirements
1. Equity of access
1. The Contractor shall:
1.1. utilise professional translation services as commissioned for use by general practices in the local area as required for all non-English speaking Patients during consultations.
1.2. take reasonable steps to proactively deliver health promotion and disease prevention activities to all Patients including those from hard-to-reach groups.
1.3. The Contractor is encouraged to record the ethnic origin and first language of all Registered Patients.
2. Patient Dignity & Respect
2. The Contractor shall:
2.1. ensure that the provision of the Services and the Practice Premises protect and preservePatient dignity, privacy and confidentiality;
2.2. allow patients to have access to a clinician of the same gender where required by thepatient and if reasonably practicable;
2.3. provide a chaperone for intimate examinations if requested by the patient to preservePatient dignity and respect cultural preferences; and
3. Informed Consent
3. The Contractor shall comply with all requirements in relation to obtaining informed consentfrom patients as required by:
3.1. Department of Health Good Practice in Consent Implementation Guide: Consent toExamination or Treatment 2001;
3.2. Health Service Circular HSC 2001/023; and3.3. Seeking Patients' Consent - The Ethical Consideration: GMC November 1998
as amended or reissued from time to time.
4. Children
4. The Contractor shall:
14

4.1. provide services to children who attend the Premises in accordance with the standards contained in the National Service Framework for Children and protocols notified to the Contractor by the Commissioner, as amended from time to time; .
4.2. ensure that a review of health is offered to children within 30 days of receipt of the children’s records following their registration at the practice, where clinically appropriate. This review may take the form of a review of records. It is mandatory that the offer of review be made, but not that the review take place.
4.3. ensure that the Contractor’s clinical and reception/administrative staff and anyone working on behalf of the Contractor are familiar with, and receive regular training in, local Child protection policies as directed by the Commissioner and as amended from time to time;
5. Clinical Safety & Medical Emergencies
5. The Contractor shall:
5.1. ensure that all Contractor Staff that have contact with patients have and maintain basic lifesupport certification with competence in defibrillation, and comply with the UK Resuscitation Council guidelines on basic life support and the Use of automated external defibrillators (including following the recommended update period of 12 months as a maximum1)
5.2. the Contractor shall ensure that all staff are trained and competent to recognise life threatening emergencies and that they have access to clinical advice at all times during core hours and the necessary systems in place to respond to medical emergencies appropriately (e.g. dial 999, contact appropriate clinician, perform CPR etc).
5.3. possess the equipment and in-date emergency drugs including oxygen to treat life-threatening conditions such as anaphylaxis, meningococcal disease, suspected myocardial infarction, status asthmaticus and status epilepticus;
5.4. adhere to any national or local guidelines relating to clinical safety and medical emergencies in primary care as amended from time to time.
5.5. Ensure that for any health care professional that is
5.5.1. Performing clinical services under this agreement; or 5.5.2. Employed or engaged to assist in the performance of such services, there are in place
arrangements for the purpose of maintaining and updating their skills and knowledge in relation to the services which they are providing or assisting in performing
5.6. Afford to each employee reasonable opportunities to undertake appropriate training with a view to maintain that employee’s competence
15

6. Referrals
6. The Contractor shall:
6.1. record all referrals in the patient record using the appropriate Read Codes;
6.2. follow local or national clinical pathways to minimise inappropriate referrals and hospitaladmissions in line with best practice on use of resources as a defined by the GMC;
6.3. co-operate with and make effective use of:
6.3.1. NHS 111; 6.3.2. the community matron/case management team; 6.3.3. Commissioner - commissioned services provided outside acute hospitals, including
health promotion services; and 6.3.4. local authority services and employment advisers; 6.3.5. co-operate with service contractors carrying out Out of Hours Services to ensure safe
and seamless care for Patients, including exchanging information on, as clinically appropriate, to such contractors carrying out Out of Hours Services on Patients that may require their services or who have special clinical requirements;
6.4. use robust clinical pathways for referral, where these are agreed with other local healthcare Contractors and/or issued by the relevant CCG;
6.5. implement national referral advice including Referral Guidelines for Suspected Cancer and NICE guidance, in line with local guidance on transmission of information;
6.6. ensure urgent suspected cancer referrals are faxed or sent electronically within twenty-four (24) hours in accordance with local Trust protocols;
6.7. implement and operate the NHS e-Referral Service (formerly Choose and Book) at point of referral for services, and provide a booking facility unless this is managed by a third party under contract with the CCG. (in accordance with the NHS Choice agenda).
8. Practitioner Skill Mix/Continuity
8.1 When the Contractor determines that delivery of the Services under the contract is at risk due to workforce changes within the practice they shall inform the commissioner.
9. Patient Records
9.1 9. The Contractor shall at its own cost retain and maintain all the clinical records in accordance with:
16

9.2 Good Clinical Practice; and
9.3 Clause 29, 31 and 33 of this agreement
9.4 The Contractor shall at its own cost retain, maintain and keep retrievable all the paper based clinical records.
9.5 The Contractor shall comply with GMC guidance on record keeping.
10. Contractor Records
10. The Contractor shall comply with good record keeping guidance, including
10.1 contract management reporting;
10.2 national / data set reporting;
10.3 activity reporting, including: requisite data for payment purposes; 10.3.2 reporting in support of quarterly monitoring returns to the Department of
Health (as agreed and advised by the Commissioner); 10.3.3 KPI measures (where not covered elsewhere).
10.4 The Contractor shall, subject always to the provisions of relevant legislation and Directions
10.4.1 on request produce the Records for inspection by the Commissioner or, on receipt of reasonable notice, allow or procure for the Commissioner and/or its authorised representatives access to any premises where any Records are stored for the purposes of inspecting and/or taking copies of and extracts from Records free of charge and for the purposes of carrying out an audit of the Contractor’s compliance with this Contract, including all activities of the Contractor, the Charges and the performance, and the security and integrity of the Contractor in providing the Services under this Contract;
10.4.2 preserve the integrity of the Records in the possession or control of the Contractor and Contractor Staff and all data which is used in, or generated as a result of, providing the Services;
10.4.3 prevent any corruption or loss of the Records, including keeping a back-up copy; and
10.4.4 provide any assistance reasonably requested by the Commissioner in order to interpret or understand any Records.
10.4.5 Both the Contractor and Commissioner will at all times comply with Information Governance requirements when handling or moving patient identifiable data.
10.5 The Contractor shall ensure that during any Records inspection the Commissioner and/or its authorised representatives receive all reasonable assistance and access to all relevant Contractor staff, premises, systems, data and other information and records relating to this Contract (whether manual or electronic).
17

Part 2 – Services
1. Services To Be Provided By The Contractor
1. The Contractor shall provide:
1.1. GP led primary medical care services as set out in the PMS Agreement and this Schedule 2 Part 2 to patients residing in the Patient Registration Area and Outer Boundary Area, and/ or patients registered with the practice as temporary patients
2. Patient Voice
2.1 Patient Surveys 2.1.1 The Contractor shall be required to fully cooperate and assist the Commissioner in
measuring patient satisfaction on an on-going basis.
3. End of life care
3.1 The Contractor shall implement up to date end of life care guidance in line with local policies
and procedures;
4. Enhanced services
4.1 Contractors must ensure that their registered patients can access the full range of services commissioned by the local CCG and/or NHS England. This means informing and sign posting patients to available services locally and documenting this as appropriate and referring where clinically appropriate.
Part 3: access to services
1. Routine Opening hours
1.1 The practice shall be open and offer continuous reception and telephony services as defined at paragraph 2 below, and deal with clinical issues appropriately, being accessible within core hours, defined as 0800 to 1830 from Monday to Friday.
1.2 This is the minimum requirement, and there is nothing in this Agreement that prohibits the contractor from opening and providing clinical Services outside of PMS Core Hours.
18
1.3 It is permitted for the practice to close for 16 hours per year for staff training and/or development, provided the commissioner is notified, and reasonable steps are taken to inform patients.
2. Provision of Reception Services
2.1 The Contractor must provide full reception services at the Practice Premises throughout the PMS Core Hours
2.2 Reception services will include but not be limited to:
2.2.1 Answering the telephone by a practice staff member 2.2.2 Free access to the premises without the need to be physically admitted; 2.2.3 Booking appointments; 2.2.4 Answering and co-ordinating Patient queries and requests; 2.2.5 Signposting Patients to services. 2.2.6 Making arrangements for the issuing of repeat prescriptions
3. Registration Policy
3.1 The Contractor shall adhere to the Once for London GP Patient Registration Operating Principles (see appendix 2).
3.2 At point of registration and on-going patients should be made aware of their right so see a specific GP if they choose to do so, but that they may need to wait longer if they choose this option.
4. Appointments
4.1 The Contractor shall offer patients a choice of access options to a full range of consultation methods to best suit their needs, as appropriate based on system capability.
4.1.1 The contractor should consider the following consultation modes: face to face, telephone, e-consultation, video consultation.
4.2 Practices need to ensure that all information governance and safety issues have been addressed to ensure compliance when completing consultation methods such as skype.
4.3 The Contractor shall undertake continuous assessment of its appointment system and access, monitoring demand and supply and taking action to address gaps in provision.
19

5. Booking an Appointment
5.1 The Contractor shall ensure that, without recourse to further contact, upon contacting the practice during PMS Core Hours in person or by telephone or online:
5.2 Patients will be able to make an appointment when they get through to the practice and not be asked to call back;
5.3 Contractors shall endeavour to facilitate patients’ requests for appointments with a clinician of their choice.
5.4 Practices must offer the facility for patients to be able to book an appointment with the GP or other appropriate Health Care Professional of their choice at the practice up to four (4) weeks in advance, where appropriate.
5.5 If clinically urgent, a patient is able to book an appointment on the same day.
5.5.1 Patients who contact the practice will be able to speak to an appropriate clinician on the day, if they so wish, and receive appropriate clinical advice and care.
5.5.2 Patients who need to be seen on the same day will be able to do so within core hours. Consultations could be face-to-face or on the phone (or video phone) but will be provided by a GP or an appropriately skilled nurse on the same day, as appropriate.
5.5.3 If patients are being offered a locality hub service appointment, the practice must ensure they keep a record of this, as a number of patients being referred into this service will be requested on a quarterly basis. It is required that the hub is granted access to the patient’s medical record, subject to patient permission and local interoperability constraints.
5.6 A ‘Consultation’ may consist of a completed appointment with an outcome for the patient, or a triage leading to an appointment at a time in the future, within the criteria set out in 5.6 above.
6. Length of Appointments
6.1 Appointment length shall be tailored to the clinical needs of the patient.
20

APPENDIX 1: PATIENT REGISTRATION AREA AND OUTER BOUNDARY AREA
Reference: Clause 31.2
[INSERT DETAILS / MAP HERE]
21

APPENDIX 2: ONCE FOR LONDON GP PATIENT REGISTRATION OPERATING PRINCIPLES
Approach
A set of task and finish groups have been established to ensure that there is wide collaboration from across London. These task and finish groups have provided a forum through which primary care leaders have shared experiences, skills and knowledge to develop a unified approach to a basket of key QIPP challenges.
Approximately 45 primary care leaders have participated in this work to date with representatives from clusters, contractors, LMC, LDC, FHS organisations, clinicians, practice managers, public health, finance and contracting.
Each task and finish group is chaired by a Cluster Primary Care Director and is signed off by NHS London’s Primary Care PLG.
Aims
The operating principles aim to:
– Embed best practice approaches across all commissioning organisations
– Support continuing improvement in the quality and productivity of primary care services aspart of QIPP
– Ensure fairness, equity and transparency in the way general practice services are beingcommissioned across London
NHS London has overseen the successful production of operating principles for Local Enhanced Services, PMS Contract Review and List Maintenance. The second tranche of operating principles addresses GP Practice Contractual Compliance, GP Patient Registrations and Premises.
Introduction and Background
The NHS Act places an obligation on commissioners to secure primary care services for residents in their area.
NHS London wishes to establish operating principles for GP Practices for patient registrations that promote human rights and public health.
Who can register for free primary care services?
Nationality is not relevant in giving people entitlement to apply to register for NHS primary care services. Anyone who is in the UK is entitled to apply to receive NHS primary medical services at a GP Practice.
There is no set length of time that a patient must reside in the UK in order to become eligible to receive NHS primary care services.
A patient does not need to be “ordinarily resident” in the UK to be eligible for NHS primary care – this only applies to secondary care (see below)
The length of time that a patient is intending to reside in an area in the UK relates to whether a patient applies to be registered as a temporary or permanent patient. Patients should be offered the
22

option of applying to be registered as a temporary resident if they are resident in the practice area for more than 24 hours but less than 3 months.
This includes asylum seekers and refugees, overseas visitors, students, people on work visas and those who are homeless
Overseas visitors, whether lawfully in the UK or not, are also eligible to apply to register with a GP Practice even if those visitors are not eligible for secondary care services.
Patients should be offered the option of registering as a temporary resident if they are resident in the practice area for more than 24 hours but less than 3 months – unless the practice has “reasonable” grounds for refusing the application (see over)
Immediately necessary treatment
General Practices are also under a duty to provide emergency or immediately necessary treatment where clinically necessary irrespective of nationality or immigration status. They are also required to provide 14 days of further cover following provision of immediate and necessary treatment.
Documentation
Practices are not obliged to ask patients for official documentation in order to prove ID or proof of residence and there is no requirement in the regulations for them to do so.
However it is not unreasonable for practices to ask for documentation in order to establish where a patient lives, and who a patient is, if they choose to do so.
Any practice that does request such documentation must do so for every patient, inconsistent application of policy could lead to legal action against them under the 2010 Equalities Act.
Although all individuals working within the NHS have a duty to protect NHS resources it is not the role of general practice to police fraud. If a practice suspects a patient of fraud (such as fake or multiple ID) then they should register and treat the patient but hand the matter over to their local counter fraud specialist.
Determining if the patient lives in the practice area.
If a practice asks new patients for proof of residence then it must request this from all patients. Anyone who resides within the practices boundary is entitled to apply to register for primary care medical services and the practice boundary should be clearly advertised to patients on the GPs practice leaflet or website if they have one.
Proof of identity
If a practice asks new patients to provide some form of ID then it must request this from all patients. Seeing some form of ID will help to ensure the correct matching of a patient to the NHS central patient registry to ensure previous medical notes are passed onto the new practice.
Patients can reasonably be asked for their NHS card but if they do not have one then any other form of personal ID should be sufficient. This does not have to be photo ID (practices can not insist on seeing passports for example as this could be discriminatory). The following are examples of some of the types of documentation which patients may provide:
• Utility bill (gas, electricity, community charge etc.)
• Phone bill stating address
23

• Credit card / Bank statement
• Rent book or tenancy agreement
• Pension book
• Benefit / family credit book
• Home office permit to stay
• Bank card
• Document showing University / college hall of residence
• Driving License (with address)
• HM Revenue and Customs Statements
• Council Tax Bill / Council rent book
• Home insurance policy
• Documentation from a reputable source, for example a letter from a voluntary organisationor a refuge
Patients who cannot provide documentation (when it is the practice’s policy to ask for it)
The majority of patients will not find it difficult to produce ID/residence documentation, however there will be some patients who do live in the practice area, but are legitimately unable to produce any of the listed documentation. Reasonable exceptions therefore need to be considered as outlined below:
If a patient cannot produce the listed documentation but states that they reside within the practice boundary then practices should either:
• Accept the registration but a note should be made for them to bring documentation next timethey attend the surgery.
•Agree to register them as an NHS patient if he or she is accompanied to the practice by otherhousehold members who do have the necessary documentation
Registration and appointments should not be withheld because a patient does not have the necessary proof of residence or personal identification
Homeless & vulnerable patients
Some patients may not be able to produce any documentation. Vulnerable patients (for example street homeless patients, those with chaotic lifestyles or non‐English speaking elderly patients who live with their family) have often experienced difficulty trying to register with a GP due to a lack of documentation. People who are homeless face an increased risk of mental illness, physical illness, of contracting infectious disease and drink and drug abuse and it is therefore essential that practices provide primary care services to such patients.
Practices are expected to register homeless people or those legitimately unable to provide documentation living within their catchment area who wish to register with them in line with the guidance above.
24

Homeless patients are entitled to register with a GP using a temporary address which may be a friend's address or a day centre. The practice may also use the practice address to register them if they wish. Practices should try to ensure they have a way of contacting the patient if they need to (for example with test results).
Some boroughs will have special services for homeless patients and practices may refer homeless patients into those services in line with local arrangements where it is in the best interests and with the agreement of the patient.
Practices should ensure there is equitable access for all patients who wish to register with them.
Registration should be available to all patients every day rather than on particular days and throughout the practice’s advertised opening hours.
Patients should be informed of the most suitable times of day for them to register.
Where possible it is good practice for practices to provide pre‐registration documentation in advance e.g. on line prior to a patient attending to register in person.
Patients have the right to change practices if they wish. If a patient is registered at another practice this is not a reason to prevent them from registering at another practice.
New patient health checks
It is desirable that patients, once they are registered, should be invited to have a new patient check.
However, neither registration or appointments to see the doctor should be delayed because of the unavailability of a new patient check appointment.
Practice boundary areas
Most practices are required to agree an “inner” and “outer” practice boundary with their area.
Patients who move out of a practice’s inner boundary area but still reside in the outer boundary area may be able to remain registered with the practice where appropriate. Patients in both the inner and outer boundaries will be entitled to receive home visits if clinically indicated.
Secondary care
Not all patients who are entitled or eligible to receive NHS primary care medical services are entitled or eligible to receive NHS secondary care services without charge.
Only patients who are “ordinarily resident” in the UK are entitled to receive secondary care services. Patients who are classed as “overseas visitors” are subject to charges for secondary care (unless there is a reciprocal agreement with their country of residence).
“Overseas visitors” are eligible to receive primary care services.
Where a GP refers an overseas visitor for hospital services they should inform the patient that the hospital may charge them for treatment even though the GP may have treated them on the NHS.
Visiting nationals from the European Economic Area in possession of a Form E128, E112 or European Health Insurance (EHIC) or nationals from any state with which the UK has a reciprocal agreement are eligible to receive free NHS care. However they may not be entitled to free treatment for a pre‐existing condition or where it is reasonable for to delay treatment until the visitor returns home.
25

The Department of Health has a series of helpful leaflets which the practice may wish to utilise when referring such patients to secondary care.
It is not however the responsibility of the practice to establish entitlement to NHS hospital treatment as hospitals have overseas visitor managers who are trained to formally determine this.
Advice on entitlement to free NHS hospital services can be found here:
http://www.dh.gov.uk/en/Healthcare/Entitlementsandcharges/OverseasVisitors/Browsable/DH_074373
Summary of principles
• Practice GP registration policies must be clear, transparent, equitable and consistentlyapplied.
• A patient is entitled to join a practice list if they live in the practice area.
• In order to register with a practice, patients can provide their medical card and/or completea GMS1 form (or equivalent).
• Practices may request some form of proof of residence and ID but these requests must beasked of all patients and it may be necessary to apply this sympathetically to an individual’s particular circumstances
• Immigration status does not affect eligibility to primary care (see page 7 for secondary careregulations) ‐ practices should not enquire about patients immigration status
• All individuals working within the NHS have a duty to protect NHS resources. If a practicesuspects a patient of fraud (such as fake or multiple ID) then they should register the patient but contact their local counter fraud specialist for advice.
• Practices should endeavour to allow patients to register everyday that they are open andnot on selected days of the week.
• Practices should register those who live in their practice area, including those who wish tochange practices from another local practice, unless they have reasonable non‐discriminatory grounds for refusing (see below).
• Appointments to see the doctor should not be withheld where the patient has need of one,because of the unavailability of a new patient check appointment.
• Appointments should also not be withheld because of the unavailability of proof of residenceor personal ID
• Practices must keep a record of patients that they refuse to register and make this availableto the CCG on request. The practice must have reasonable non‐discriminatory grounds, and they should inform the applicant in writing of their refusal and reason for it.
• Practices should ensure that their registration process and practice boundary is clearlyoutlined on their practice leaflet, relevant NHS Choices section or website if they have one
26

Version 10 Shared as part of London offer on 3/11/2015.
Reviewer Date Change summary Version
Alex Mears 23/11/2015Version control table added to beginning tab of KPIs, based on comments and feedback
receivedV11
Alex Mears 26/11/2015 Actions from KPI post-feedback review meeting implemented V12Alex Mears 27/11/2015 Add data availability table V13Alex Mears 30/11/2015 Remove status statement V14Alex Mears 07/11/2015 Amends following MD meeting 7/11/15 V15Alex Mears 08/12/2015 Addition of level descriptors for PV metrics V16Alex Mears 14/12/2015 Amendment of PV metric costing V17Alex Mears 05/01/2016 Addition of numerator and denominator columns; addition of data source table V18Liam Crosby 08/01/2016 Add comments and more detail to data source table V19Alex Mears 29/01/2016 Amend as per comments from LMC V20Alex Mears 02/02/2016 Amend breast screenign KPI V21Alex Mears 03/02/2016 Amend flu<65 KPI V22Alex Mears 03/02/2016 Move breast screening to local KPIs V23
Elizabeth Lyon 04/02/2016
Changes to Childhood imms by year 1 - description of 5-in-1 vaccine added, reference to Hep B removedChildhood imms - 2 - 5: band values changedFlu immunisation <65 - bands all changedPatient Voice - add note referring to choices and wording in BandsBreast Screening - all measures removed and replaced with 'To be determined locally'PV - heading on patient voice and bands copied from previous page
V24
Dean Musson 04/02/2016 Amendments to bandings V25
27
Annex 2

Status of KPI set
- those KPIs listed as mandatory must be added to all PMS contracts. - those listed as suggested local KPIs may form part of a wider premium package, including the items within the premium specification and/ or locally agreed KPIs.
Impact of bandings
- each KPI has 4 bandings in which the practice will be located in terms of performance. The impact of performance is as follows:
1) Band D: no payment2) Band C: 50% of full payment3) Band B: 75% of full payment4) Band A: 100% of full payment
Performance implications
Performance on these KPIs carries no contractual implications at all, the only impact is on additional premium funding. There is in addition not clawback of other funding attached to performance.
Breast screening KPI
Proposed cohort of patients (denominator) will include women who have defaulted during the period 1st October to 30th September of the preceding years. For example in reviewing the KPIs for 2016/17 the denominator would be women who were notified as defaulting from 1st October 2015 to 30th September 2016. This will allow a 6 month window between 1st October 2016 to 31st March 2017 for practices to follow up patients who have defaulted in order to re-attend and for the practice to receive a report to confirm attendance. Practices will be required to submit a template verifying their denominator and numerator to confirm patient attendance.
28
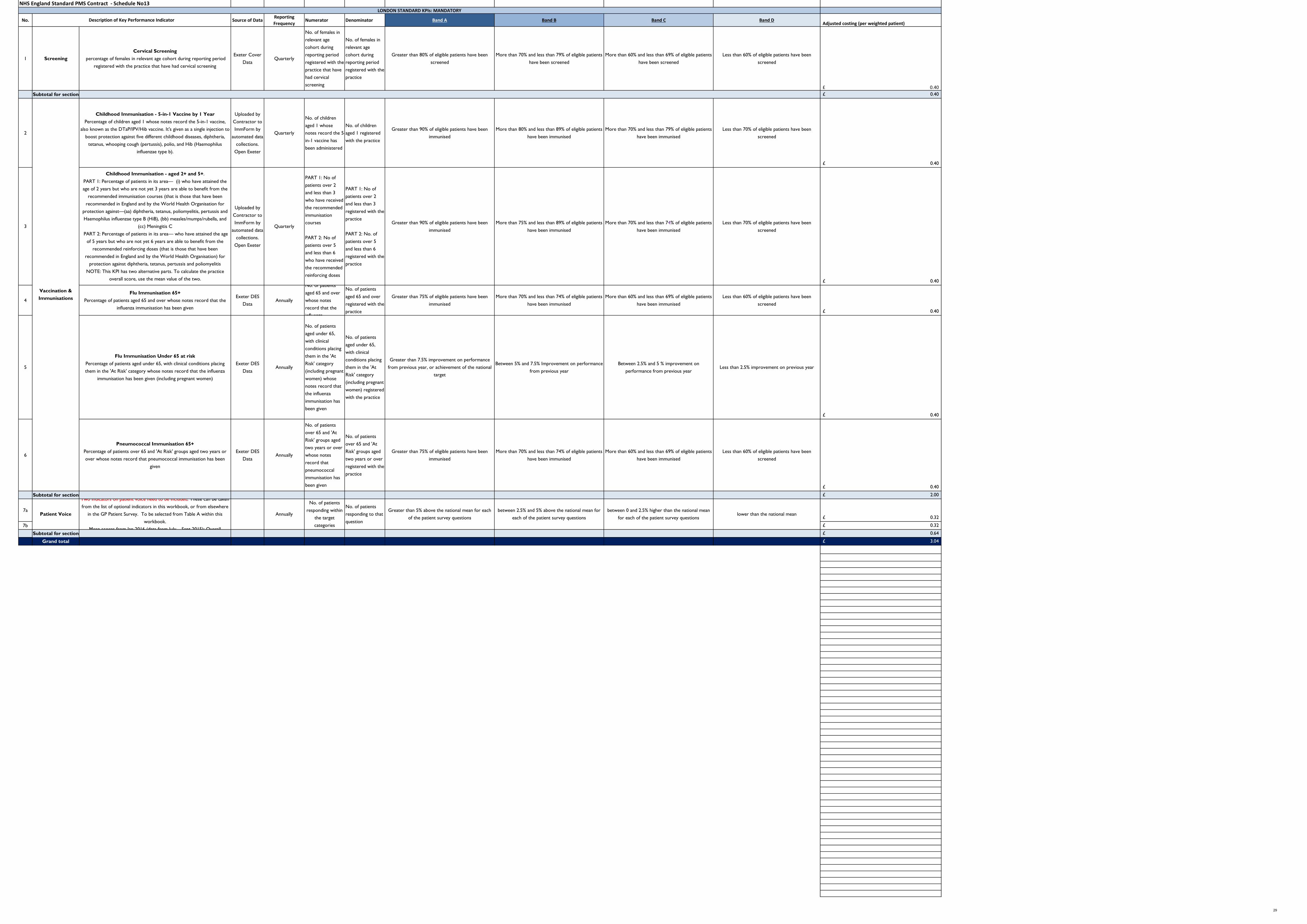
NHS England Standard PMS Contract - Schedule No13
No. Source of Data Reporting Frequency
Numerator Denominator Band A Band B Band C Band DAdjusted costing (per weighted patient)
1 ScreeningCervical Screening
percentage of females in relevant age cohort during reporting period registered with the practice that have had cervical screening
Exeter Cover Data
Quarterly
No. of females in relevant age cohort during reporting period registered with the practice that have had cervical screening
No. of females in relevant age cohort during reporting period registered with the practice
Greater than 80% of eligible patients have been screened
More than 70% and less than 79% of eligible patients have been screened
More than 60% and less than 69% of eligible patients have been screened
Less than 60% of eligible patients have been screened
0.40£ Subtotal for section 0.40£
2
Childhood Immunisation - 5-in-1 Vaccine by 1 YearPercentage of children aged 1 whose notes record the 5-in-1 vaccine,
also known as the DTaP/IPV/Hib vaccine. It's given as a single injection to boost protection against five different childhood diseases, diphtheria,
tetanus, whooping cough (pertussis), polio, and Hib (Haemophilus influenzae type b).
Uploaded by Contractor to ImmForm by
automated data collections.
Open Exeter
Quarterly
No. of children aged 1 whose notes record the 5-in-1 vaccine has been administered
No. of children aged 1 registered with the practice
Greater than 90% of eligible patients have been immunised
More than 80% and less than 89% of eligible patients have been immunised
More than 70% and less than 79% of eligible patients have been immunised
Less than 70% of eligible patients have been screened
0.40£
3
Childhood Immunisation - aged 2+ and 5+. PART 1: Percentage of patients in its area— (i) who have attained the age of 2 years but who are not yet 3 years are able to benefit from the
recommended immunisation courses (that is those that have been recommended in England and by the World Health Organisation for
protection against—(aa) diphtheria, tetanus, poliomyelitis, pertussis and Haemophilus influenzae type B (HiB), (bb) measles/mumps/rubella, and
(cc) Meningitis C PART 2: Percentage of patients in its area— who have attained the age
of 5 years but who are not yet 6 years are able to benefit from the recommended reinforcing doses (that is those that have been
recommended in England and by the World Health Organisation) for protection against diphtheria, tetanus, pertussis and poliomyelitis
NOTE: This KPI has two alternative parts. To calculate the practice overall score, use the mean value of the two.
Uploaded by Contractor to ImmForm by
automated data collections.
Open Exeter
Quarterly
PART 1: No of patients over 2 and less than 3 who have received the recommended immunisation courses
PART 2: No of patients over 5 and less than 6 who have received the recommended reinforcing doses
PART 1: No of patients over 2 and less than 3 registered with the practice
PART 2: No. of patients over 5 and less than 6 registered with the practice
Greater than 90% of eligible patients have been immunised
More than 75% and less than 89% of eligible patients
have been immunised
More than 70% and less than 74% of eligible patients have been immunised
Less than 70% of eligible patients have been screened
0.40£
4Flu Immunisation 65+
Percentage of patients aged 65 and over whose notes record that the influenza immunisation has been given
Exeter DES Data
Annually
No. of patientsaged 65 and over whose notes record that the influenza
No. of patients aged 65 and over registered with the practice
Greater than 75% of eligible patients have been immunised
More than 70% and less than 74% of eligible patients have been immunised
More than 60% and less than 69% of eligible patients have been immunised
Less than 60% of eligible patients have been screened
0.40£
5
Flu Immunisation Under 65 at riskPercentage of patients aged under 65, with clinical conditions placing them in the 'At Risk' category whose notes record that the influenza
immunisation has been given (including pregnant women)
Exeter DES Data
Annually
No. of patients aged under 65, with clinical conditions placing them in the 'At Risk' category (including pregnant women) whose notes record that the influenza immunisation has been given
No. of patients aged under 65, with clinical conditions placing them in the 'At Risk' category (including pregnant women) registered with the practice
Greater than 7.5% improvement on performance from previous year, or achievement of the national
target
Between 5% and 7.5% Improvement on performance from previous year
Between 2.5% and 5 % improvement on performance from previous year
Less than 2.5% improvement on previous year
0.40£
6
Pneumococcal Immunisation 65+Percentage of patients over 65 and 'At Risk' groups aged two years or over whose notes record that pneumococcal immunisation has been
given
Exeter DES Data
Annually
No. of patients over 65 and 'At Risk' groups aged two years or over whose notes record that pneumococcal immunisation has been given
No. of patients over 65 and 'At Risk' groups aged two years or over registered with the practice
Greater than 75% of eligible patients have been immunised
More than 70% and less than 74% of eligible patients have been immunised
More than 60% and less than 69% of eligible patients have been immunised
Less than 60% of eligible patients have been screened
0.40£
Subtotal for section 2.00£
7a0.32£
7b 0.32£
Subtotal for section 0.64£
Grand total 3.04£
Greater than 5% above the national mean for each of the patient survey questions
Description of Key Performance Indicator
LONDON STANDARD KPIs: MANDATORY
Vaccination & Immunisations
Patient Voice
Two indicators on patient voice need to be included. These can be takenfrom the list of optional indicators in this workbook, or from elsewhere
in the GP Patient Survey. To be selected from Table A within this workbook.
Mean scores from Jan 2016 (data from July – Sept 2015): Overall
between 2.5% and 5% above the national mean for each of the patient survey questions
between 0 and 2.5% higher than the national mean for each of the patient survey questions
lower than the national mean
No. of patients responding within
the target categories
No. of patients responding to that question
Annually
29

NHS England Standard PMS Contract - Schedule No13
No. Source of Data Numerator Denominator Band A Band B Band C Band D Adjusted costing
(per weighted patient)
8 ScreeningBreast Screening
percentage of females in relevant age cohort during reporting period registered with the practice that have defaulted and subsequently attend the breast screening service
Exeter Uptake Data 0.40£
9Capacity & Access
Measures
Average Attendance at local unscedhuled care facilities (including WIC, UCC and A&E) for non-admitted patients during Core PMS hours sus £ 0.96
10Overall Experience
Percentage of patients responding within the 'good' range to the question "Overall, how would you recommend your experience of your GP Surgery?"
National GP Patient Survey (locally administered in
year 1)
Number of patients responding within the 'good' range to the question "Overall, how would
you recommend your experience of your GP
Surgery?"
Number of patients responding to the
question "Overall, how would you recommend your experience of your
GP Surgery?"
Greater than 5% above the national mean for the patient survey question
between 2.5% and 5% above the national mean for the patient survey question
between 0 and 2.5% higher than the national mean for the patient survey
question
lower than the national mean for the patiet survey question
£ 0.32
11Telephone
Percentage of patients responding within the 'easy' range to the question "Generally, how easy is it to get through to someone at your GP Surgery on the phone?"
National GP Patient Survey (locally administered in
year 1)
Number of patients responding within the 'easy' range to the
question "Generally, how easy is it to get through to someone
at your GP Surgery on the phone?"
Number of patients responding to the
question "Generally, how easy is it to get through to someone at your GP Surgery on the phone?"
Greater than 5% above the national mean for the patient survey question
between 2.5% and 5% above the national mean for the patient survey question
between 0 and 2.5% higher than the national mean for the patient survey
question
lower than the national mean for the patiet survey question
£ 0.32
12
Convenience of appointmentPercentage of patients responding within the 'convenient' range to the question "How
convenient was the appointment youwere able to get?"
National GP Patient Survey (locally administered in
year 1)
Number of patients responding within the
'convenient' range to the question "How convenient was
the appointment youwere able to get?"
Number of patients responding to the
question "How convenient was the appointment you
were able to get?"
Greater than 5% above the national mean for the patient survey question
between 2.5% and 5% above the national mean for the patient survey question
between 0 and 2.5% higher than the national mean for the patient survey
question
lower than the national mean for the patiet survey question
£ 0.32
13
Experience of making an appointmentPercentage of patients responding within the 'good' range to the question "Overall, how
would you describe yourexperience of making an appointment?"
National GP Patient Survey (locally administered in
year 1)
Number of patients responding within the 'good' range to the question "Overall, how would
you describe yourexperience of making an
appointment?"
Number of patients responding to the
question "Overall, how would you describe yourexperience of making an
appointment?"
Greater than 5% above the national mean for the patient survey question
between 2.5% and 5% above the national mean for the patient survey question
between 0 and 2.5% higher than the national mean for the patient survey
question
lower than the national mean for the patiet survey question
£ 0.32
14
RecommendationPercentage of patients who would definitely or probably recommend their GP Surgery
National GP Patient Survey (locally administered in
year 1)
Number of patients who would definitely or probably
recommend their GP Surgery
Number of patients responding to the
question 'wouyld you recommend your GP
Surgery?'
Greater than 5% above the national mean for the patient survey question
between 2.5% and 5% above the national mean for the patient survey question
between 0 and 2.5% higher than the national mean for the patient survey
question
lower than the national mean for the patiet survey question
£ 0.32
13
LONDON STANDARD KPIs: OPTIONAL suggested KPIs for potential local mandation
Patient Voice
Description of Key Performance Indicator
To be locally determined
To be locally determined
Table A
30

PMS Premium Service Specification
Reviewer Date Change summary Version Alex Mears 23/11/2015 Version control table added to
beginning of specification, based on comments and feedback received
V7
Kelly Poole 24/11/2015 1.5 – Amendment to text, changed from “Skype” to “video
conferencing”
V7.1
Alex Mears 27/11/2015 Amends made following Medical directorate meeting
V8
Alex Mears 30/11/2015 Amend section 2 V9 Alex Mears 07/12/2015 Amends from MD meeting 7/12/15 V10 Alex Mears 11/12/2015 Amends post PCMB 11/12/15,
addition of clinician capacity to part 1 V11
Alex Mears 29/01/2016 Amends post LMC comments V12 Alex Mears 02/02/2016 Add in specific service requirements V13 Alex Mears 03/02/2016 Amendments and comments from Jill
Web and Christina Windle V14
Alex Mears 03/02/2016 Further amendments following teleconference
V15
Alex Mears 03/02/2016 Final amends after consultation with MD
V16
Alex Mears 04/02/2016 Amends following LMC meeting V17 Dean Musson 04/02/2016 Minor amends and addition of Sunday V18 Alex Mears 05/02/2016 Amends following notes from Julius
parker (Surrey & Sussex LMC), plus re-order to improve flow
V19
Alex Mears 05/02/2016 Minor amends V20 Alex Mears 05/02/2016 Removal of red flagging of amends V21
Specific premium provisions
None of the offers listed below are mandatory for CCGs to adopt, but can form part of an overall
premium offer.
Weekend Additional Capacity (WAC)
31
Annex 3
1.1 The locally commissioned component of the PMS premium London Offer includes provision for
practices to receive additional funds for opening on a weekend. This is in addition to core opening
hours of 0800 to 1830 during the working week.
1.2 The services provided during this period shall include those that are ordinarily available to registered
patients at the practice during core contract hours1 (with the exception of home visits, which are not
part of a weekend offer, and minor amendments to the Core Service Requirements which are included
in Appendix 2). The specification and pricing in this document relate specifically to delivery of this
service at practice level.
1.3 Where this requirement is to be met by an obligation within this contract, the costing model below
must be followed. It is also possible to meet this obligation by a collective approach or federated
model, provided that the following criteria are met:
1.3.1 All registered patients across the practices involved must have access to the services
1.3.2 Medical records for all patients must be accessible and editable
1.3.3 Accessibility for patients must be reasonable (e.g. travel distances not significant etc)
1.4 A costing model has been developed as below:
1.4.1 NHS England’s model is based on 4 hours of clinical time, provided by a GP2 in addition to
reception services throughout that period, including overheads costs. The cost per raw registered
patient based on an average practice of 6000 patients3 is £4.00. This model includes costs for
medical indemnity. This service must be provided for fifty out of fifty-two weekends in each
calendar year.
1.5 The extension to include weekend opening has as its foundation the requirement in clause 7.3 of the
PMS contract that contractors provide ‘Essential Services’ within core PMS hours. ‘Essential Services’ is
defined within the GMS contract at clause 8.1
1.6 Any service provided needs to meet the requisite criteria as specified in the PMS contract. These are
set out in the PMS Contract Core Service Requirements (schedule 13 to the Main Agreement), and are
adopted in full for weekend opening, save for amendments specific to weekend opening (listed in
1 the number of appointments that should be provided should take into account the needs of registered patients, skill mix and funding available to commissioners for weekend services 2 This represents a minimum: practices with larger list sizes are at liberty to adjust the skill mix to meet their population needs. 3 NHS England recognises that this will be challenging to offer for smaller practices. Where this is the case it is expected that practices work together and with their commissioner to agree a solution.
32

appendix 2). Weekend provision, as defined by this specification aligns with the SCF accessible care,
but it is recognised that it only represents partial delivery of this SCF.
1.7 To attract premium funding, there is a requirement that practices provide a minimum of four
consecutive hours at the weekend of this services at a time to be determined by the Contractor, which
should be regular and consistent unless exceptional circumstances apply. The clinical offer will require
the contractor to provide sufficient clinical capacity to meet the reasonable needs of patients. As a
minimum, a General Practitioner shall be available during two-thirds of these four hours to provide
clinical consultations with registered patients. The minimum clinical personnel available may be GP or
nursing (costings are based on a GP for 4 hours as per 1.5.1).
1.8 A full reception service should be available during the 4 hours opening.
1.9 The consulting General Practitioner must have full access to the patient’s medical health record during
the consultation.
1.10 Only patients registered with the practice can pre-book a consultation during this period.
Consultations must be available to pre-book up to five working days prior to the weekend service.
1.11 Consultations may occur face-to-face, by telephone or other modalities.
1.12 The availability of this service must be publicised by the contractor via its website and at the
practice.
1.13 This is the minimum requirement, and there is nothing in this Agreement that prohibits the
contractor from opening and providing Reception Services outside of PMS Core Hours.
1. Improving Access through Use of Technology
1.1. The practice will be required to make at least 50% of all appointments available online for booking
and cancellation by 1st April 2017.
1.2. An incentive model is included, with incremental payments for achievement from July 2016 to June
2017 as follows:
33

• 25% target 2015/16 Q3 Fixed payment based on 25p per weighted patient
• 37.5% Target 2015/16 Q4 Fixed payment based on 25p per weighted patient
• 50% Target 2016/17Q1 Fixed payment based on 50p per weighted patient (to reward)
1.3. The contractor is required to offer electronic consultations (for example video conferencing).
1.4. The Contractor shall proactively offer registered patients access to the services referred to in
paragraph 2.1 above, providing clear information necessary to do so.
1.5. The Contractor shall issue passwords and verify the identity of registered patients wishing to
access the services in 2.1 above, as recommended by guidance from the Royal College of General
Practitioners (RCGP).
1.6. The Contractor shall ensure that its pages on NHS Choices are updated regularly, and provide
complete and accurate information regarding the practice at all times.
34
Appendix 1: monitoring or evidence required by NHSE for this service specification
• Practice to include opening hours on the practice website. Practices must submit self-declarationsbased on the following metrics:
o Proportion of weekend appointments offered, those used and DNAso Proportion of appointments offered onlineo Responses will be assured using a PPV undertaken by NHSE on a sample of practices.
• Practices must give a self-declared annual report on any adjustments, or measures already in placeto ensure that reasonable adjustments to remove access barriers for patients, such asconsiderations for the homeless or non-English speakers, as well as adhering to the Equality Act(2010) for physical access needs ramps, hearing loops etc. have been made. This will be subject toPPV by NHSE on a sample of practices.
• Contractor must submit a quarterly report (by the 10th April, Jul, Oct, Jan) of the total number ofappointments, the number taken up and the ratio of on the day and appointments ahead. Practiceshould give full details on the results of their demand and capacity analyses which should include areview of the skill mix they have within the practice providing service to the practices. A templatewill be provided to do this.
• Annual report from practice on the % of patients signed up to use the online booking service versusthe amount that actually use the service.
• Practices will be required to submit a quarterly report of the % appointments made available onlineeach quarter. Evidence should be provided from the clinical system to support it.
• Contractor must submit an annual report of the total number of appointments, the number takenup and breakdown of what form the appointments took eg. telephone, video conference, face toface.
35

Appendix 2: specific amendments to provisions within the Core Service Requirements
Please note: as referenced these elements indicate where there is a change to the core specification. Therefore should be read in conjunction with the full specification document
Part 3: access to services
Provision of Reception Services
2.1 The Contractor must provide full reception services at the Practice Premises throughout the PMS Core Hours
2.2 Reception services will include but not be limited to:
2.2.1 Answering the telephone by a receptionist; 2.2.2 Free access to the premises without the need to be physically admitted; 2.2.3 Booking appointments; 2.2.4 Answering and co-ordinating Patient queries and requests; 2.2.5 Signposting Patients to services. 2.2.6 Making arrangements for the issuing of repeat prescriptions
4 Appointments
4.1 The Contractor shall offer patients a choice of access options to a blend of consultation methods to best suit their needs, as appropriate based on system capability.
4.1.1 The contractor should consider the following consultation modes: face to face, telephone, e-consultation, video consultation.
4.2 Practices need to ensure that all information governance and safety issues have been addressed to ensure compliance when completing consultation methods such as skype.
4.3 The Contractor shall undertake continuous assessment of its appointment system and access, monitoring demand and supply and taking action to address gaps in provision.
5. Booking a future Appointment
5.1 The Contractor shall ensure that, without recourse to further contact, upon contacting the practice during PMS Core Hours in person or by telephone or online:
36

5.2 Patients will be able to make an appointment when they get through to the practice and not be asked to call back;
5.3 Contractors shall endeavour to facilitate patients’ requests for appointments with a clinician of their choice.
5.4 Practices must offer the facility for patients to be able to book an appointment with the GP or other appropriate Health Care Professional of their choice at the practice up to four (4) weeks in advance, where appropriate.
5.5 If clinically urgent, a patient is able to book an urgent appointment on the same day.
5.5.1 Patients who contact the practice will be able to speak to a clinician on the day, if they so wish, and receive appropriate clinical advice and care.
5.5.2 Patients who need to be seen the same day will be able to do so within core hours. 5.5.3 If patients are being offered a locality hub service appointment, the practice must ensure they keep
a record of this, as a number of patients being referred into this service will be requested on a quarterly basis. It is required that the hub is granted access to the patient’s medical record, subject to patient permission and local interoperability constraints.
5.6 A ‘Consultation’ may consist of a completed appointment with an outcome for the patient, or a triage leading to an appointment at a time in the future, within the criteria set out in 5.6 above.
37

Appendix 3: excerpt from the Primary Care Strategic Commissioning Framework4
A3: Routine opening hours Patients will be able to access pre-bookable routine appointments with a primary health care professional (see ‘workforce implications’ for the proposed primary care team) at all practices 8am – 6.30pm Monday to Friday and 8am to 12 noon on Saturdays. An alternative equivalent patient offer may be provided where there is a clear, evidenced local need.
There is significant variation in opening hours across London. This specification will create an equitable offer to patients across the capital. During the specified hours, all practices will be open to allow patients to access all services, including attending an appointment, speaking to a receptionist, and collecting or ordering a prescription.
A4: Extended opening hours Patients will be able to access a GP or other primary care health professional seven days per week, 12 hours per day (8am to 8pm or an alternative equivalent offer based on local need) in their local area, for pre-bookable and unscheduled care appointments. This service will be delivered by networks of practices working together at scale. In most cases a larger practice in the local community will take the lead to provide this service on behalf of other practices. A suggested offer of 8am to 8pm is described here, however there could be a suitable alternative equivalent offer based on local population needs, for which the totality of the offer (seven days, 12 hours) is not reduced.
4 https://www.england.nhs.uk/london/wp-content/uploads/sites/8/2015/03/lndn-prim-care-doc.pdf
38

Co-commissioning of Primary Care South East London’s CCGs and NHS England Primary Care Joint Committees
Primary Care Joint Committees (PCJC) Meetings
DATE OF MEETING: 11 February 2016
ENCLOSURE: J
Title: PMS Commissioning Intentions: NHS Bexley CCG AUTHOR: Theresa Osborne, Chief Financial Officer and Director lead for Primary Care
SUMMARY:
Assessment of local position following the confirmation of the final London offer between NHS England and London LMCs: NHS Bexley CCG has the lowest premium in London, an average of £7.16. As such it cannot carry out the full London offer. It will therefore offer the mandatory KPI suite and the weekend additional capacity, which is slightly above the available premium (an average of £7.29) and a cost pressure of £25,979. The CCG is therefore requesting this additional sum as a first call on primary care growth monies. The CCG currently has no further monies available to invest in primary care and is not planning any additional services to include in the PMS contract.
Summary of how the remaining funds/premium will be spent: The CCG has no remaining funds available after the mandatory KPI suite and the weekend additional capacity. However, this is due to the late change in the calculation of the weekend capacity on raw list size. Therefore, the CCG would like to formally request funding of £1 per patient to offer Improving Access through the use of technology to all practices (£218,866) (in addition to the above cost pressure) as a first call on primary care growth. The current PMS premium will be reinvested in general practice.
KEY ISSUES:
London Transformation programme: The CCG has very little investment funding available in 2016/17 to progress the SCF. However, it is intending to continue to increase investment in primary care over the 5-year planning period, as funding becomes available. The CCG has a thriving Primary Care Development working group, with significant stakeholder representation and a LCN Programme Board to take this agenda forward. The CCG would therefore wish to make an argument that NHS Bexley CCG should receive a higher level of the primary care growth than others across London, who without exception already have higher premiums to invest in
39
Annex 4

the SCF. This will also support London in moving to a more equalised position within and across SPGs.
Impact on GMS and APMS practices: The CCG intends to equalise the offer to GMS practices in 2016/17. However, the additional funding requested for Improving Access through the use of technology would also be required from the 2016/17 primary care growth for GMS practices (this is included in the above numbers).
NHSE has recognised that Bexley’s APMS contract is out of alignment with the London APMS contract and is proposing, regardless of the national requirement to equalise, to re-negotiate the Bexley APMS contract based on the ongoing London APMS contract programme. Co-commissioners would wish to ensure that the APMS contract is also aligned to the Bexley PMS offer, which would result in a cost neutral outcome for Bexley CCG
Summary of any additional local issues: The CCG will discuss Saturday Morning opening with practices once they have received their PMS offer letters. Other options to delivery include: collective, Local Care Network and federated provision, which will all be considered should GP practices not be in a position to deliver Saturday morning opening by practice. This is in line with the premium service specification which states: "It is also possible to meet this obligation by a collective approach or federated model"
Furthermore this offer may need to be re-considered dependant on any national enhanced hours DES or voluntary contract offer.
CCG CONTACT: Name: Theresa Osborne, Chief Financial Officer E-Mail: [email protected]
RECOMMENDATIONS:
The Bexley Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for NHS Bexley CCG subject to confirmation from NHS England (London) that the cost pressure of £25,979 to fund Saturday morning openings, and an additional £1 pwpp, to facilitate the offer of Improving Access through the use of technology specification, are added to the CCG's budgets, as a first call on 2016/17 Primary Care growth.
40


CCG Name NHS Bexley CCG
London Offer
1 London Standard Key Performance Indicators (KPIs)
Is CCG going to offer? Additional Comments
Cervical screening
Childhood Immunisation ‐ 5‐in‐1 Vaccine by 1 Year
Childhood Immunisation ‐ aged 5 years and over.
Flu Immunisation 65+
Flu Immunisation Under 65 at risk
Pneumococcal Immunisation 65+
Overall Experience
Percentage of patients responding within the 'good' range to the question "Overall, how
would you recommend your experience of your GP Surgery?"
Yes This was debated at the CCG's Co‐
Commissioning Board and has been
selected based on strong feedback
received from the CCG's Patient's
Council and Healthwatch. As this is an
annual target, the CCG will review
performance annually, reviewing
information from the Patient Survey
and Friends and Family test, as well as
consulting with the Patient Council and
Healthwatch, to inform selection of
future years' KPIs.
Telephone
Percentage of patients responding within the 'easy' range to the question "Generally,
how easy is it to get through to someone at your GP Surgery on the phone?"
No
Convenience of appointment
Percentage of patients responding within the 'convenient' range to the question "How
convenient was the appointment you
were able to get?"
No
Experience of making an appointment
Percentage of patients responding within the 'good' range to the question "Overall, how
would you describe your
experience of making an appointment?"
Yes This was debated at the CCG's Co‐
Commissioning Board and has been
selected based on strong feedback
received from the CCG's Patient's
Council and Healthwatch. As this is an
annual target, the CCG will review
performance annually, reviewing
information from the Patient Survey
and Friends and Family test, as well as
consulting with the Patient Council and
Healthwatch, to inform selection of
future years' KPIs.
Recommendation
Percentage of patients who would definitely or probably recommend their GP Surgery
No
Capacity & Access Measures
Average Attendance at local unscheduled care facilities (including WIC, UCC and A&E)
for non‐admitted patients during Core PMS hours
No The CCG is concerned that this KPI will
incentivise GPs to not send patients to
these facilities when it is necessary. The
CCG's limited available premium also
prohibits selection of this KPI.
2 Premium Access Service Specification
Is CCG going to offer? Additional Comments
No
Is CCG going to offer? Additional Comments
Patient Voice
Vaccinations and Immunisations
PMS Commissioning Intentions ‐ Which must be completed as a minimum for CCG Commissioning intentions return
documentation.
CCG to confirm that they are going to complete the full Mandatory KPI suite?
CCG to confirm which two patient voice areas they are going to add to their mandatory KPI suite from the below options:
London Standard KPIs
Screening
Yes
If the CCG is not planning to offer any of the service specification, please given comment on rationale for this :
Is the CCG going to complete the full access service specification? If answer is Yes ‐ move to question 3, If answer is no, but the
CCG is going to choose some areas from the service specification , complete rows 32‐34 with Yes/No answers. Additional
comments can be added as required.
Premium Access Service Specification
CCG to confirm if they will include the optional KPI on capacity and access:
Premium Access Service Specification ‐ Service areas :
42

Yes
The CCG will discuss Saturday Morning
Opening with practices once they have
received their PMS offer letters. Other
options to delivery include: collective,
Local Care Network and federated
provision, which will all be considered
should GP practices not be in a position
to deliver Saturday morning opening by
practice. This is in line with the
premium service specification which
states: "It is also possible to meet this
obligation by a collective approach or
federated model"
Due to the late change of this being
costed on raw patients, this presents
the CCG with a £26k cost pressure,
which it is requesting is first call on the
2016/17 primary care growth.
Furthermore this offer may need to be
re‐considered dependant on any
national enhanced hours DES or
voluntary contract offer.
Yes
The CCG's limited available premium
prohibits selection of this KPI. The CCG
would therefore like to agree with
NHSE that an additional £1 pwpp (in
addition to the above cost pressure) is
added to the CCG's budgets, as a first
call on 2016/17 Primary Care growth, to
facilitate the offer of this KPI to
practices. This would enable the CCG to
maximise the opportunity to
implement the SCF, within resources
available. This is also in consideration
that the CCG is contributing funding
from its own resources to equalise GMS
practices in 2016/17. However, the CCG
is working directly with practices
through the Primary Care Development
Working Group to facilitate
implementation of improved access to
on‐line appointments, electronic
prescribing and e‐consultations. Work
is also ongoing to facilitate further use
of Omnijoin and implement Vibe across
practices.
3 Other commissioning intentions
4 Engagement
5 Impact assessments on practice stability following PMS contract changes
6 Transition
7 Equalisation
N/A
What other commissioning intentions are the CCG planning, including any potential out of hospital services, or interpractice services?
CCG must detail any service/s in full, how service will be measured, what the outcomes are/expected, is it equitable across the CCG, is it value for money, how does it meet the needs of the local
population, and does service meet the requirements of the Strategic Commissioning Framework (SCF ‐available upon request)
The CCG has considered whether to include any additional funding in the PMS offer. This has been discussed with NHS England, the Primary Care Co‐Commissioning Board members, Governing Body
members and the LMC. These committees are all in agreement that they would not wish the current monies invested in the Primary Care Improvement Funds (Kitemark) to be added to the PMS
contract. This is to ensure that the funding can be protected locally, with KPIs based on local strategy. The CCG currently has no further monies available to invest and is not therefore planning any
additional services in respect of the PMS review, or to include in the PMS contract.
The CCG has insufficient information to complete impact assessments on services offered within practices. However, as the CCG's premium is so low (£7.16 average), this is not been highlighted as a
problem. However, in the CCG's PMS Commissioning Intentions 9 practices will lose a proportion of their funding (dependant on the payment of a KPI for additional technology use) as well as
potentially not achieving the full level of funding offered through KPIs. This may de‐stabilise smaller practices and risk services provided by all practices. In addition there is a risk that practices will
revert to GMS and deliver just those services included in the GMS contract, thereby reducing services currently provided to patients.
The CCG presented details of the PMS review to the December patient council, and followed this up in January. It is expected that further details will be provided at the March meeting. The CCG has
also discussed the PMS review with practices at engagement events, locality meetings and the Primary Care Development Working Group. Meetings have also taken place with the LMC and HWBB.
The Commissioning Intentions were discussed at the Primary Care Co‐Commissioning Board on 4th February.
Please give details as to what engagement has taken place with practices, patients or other third party services to complete your PMS commissioning intentions :
Has the CCG completed any impact studies on services that potentially will need to cease in practices, or if funding will cease that currently may financially support clinicians in practices and to
ensure that practice stability can be maintained throughout the transition? Please give details :
2 years of transition is allowable for practices in line with national guidance. Following further national clarification, it is confirmed that a longer transitional period can be considered by regional
teams with CCGs on a case by case basis as part of negotiations but this will not be considered on a CCG wide basis. All transitional periods must end by March 2020/21.
CCG to give full explanation as to how they will transition to new services they have advised they will be commissioning above. This should included as a minimum how it will be rolled out across
the CCG. Length of time it will take to be up and running, any risks or additional costs involved.
Improving Access through the use of technology
Weekend Additional Capacity
43

8 Costs and Investment planning
9 Wider Commissioning Intentions
10 Other Information
Has the CCG got any other information/documents to support these PMS commissioning intentions?
The PMS Commissioning Intentions are in line with the SCF, 'Our Healthier South East London' strategy and the CCG's Primary Care Strategy (available upon request).
The CCG’s average premium equates to £7.16 and it is proposed that is invested as follows:
Premium available £7.16
Mandatory KPIs suite £3.04
Weekend additional capacity £4.25
Sub total £7.29
Balance available £(0.13)
Improving Access through the use of Technology £(1.00)
Balance required as first call from the 2016/17
primary care growth £1.13
The CCG has only small investment funding available in 2016/17, other than the GMS equalisation detailed above, to progress the SCF. However, in 2017/18, the CCG has planned to invest an
additional £500k in primary care. This will be used to further implementation of the SCF and start to deliver 8‐8 (outside of the required core hours and Saturday mornings offered as part of the PMS
review), all of which will require significant investment. The CCG is intending to continue to increase investment in primary care over the 5‐year planning period, as funding becomes available, to
deliver the SCF. The CCG has a thriving Primary Care Development working group, with significant stakeholder representation and a LCN Programme Board to take this agenda forward. The CCG's
Primary Care Strategy is also attached for information.
The PMS Commissioning Intentions are in line with the SCF which the CCG and its practices are working towards. The SCF is also reflected in the CCG's Primary Care Strategy.
How do the PMS Commissioning intentions described above fit in with the wider CCG commissioning intentions for the following year (2016/2017) where applicable note how this fits in with the
Joint Strategic Needs Assessment (JSNA) :
CCG to give full details of any costs and investment plans they have for the following 2 years, including any impacts this will have on service delivery of the commissioning intentions noted above
or any new incentives they may wish to deliver.
The CCG has calculated the cost of equalising GMS practices to the offer to be made to PMS practices. This cost is c£150k. The intention is to equalise in 2016/17. In respect of the CCG's one APMS
contract, the CCG's intention is to bring this is line with PMS contracts when APMS contracts are reviewed. The risks are considered minimal.
Equalisation to GMS in 2016/17 should be delivered where strategically and financially possible. In cases where this is not possible, CCG areas will be required to set out their plans for
equalisation in their commissioning intentions submission in February and show strategic plans for achieving it as part of Sustainability and Transformation plans submitted in June 2016. Plans
will need to show equalisation before 2021 to ensure equalisation is achieved in the planning period. Note that as a minimum, where CCGs have not achieved funding equalisation within PMS
practices this will need to be achieved by 2016/17.
CCG to give explanation of how they will seek to achieve equalisation within the prescribed timeframe. This should include a timescale for implementation, any risks and additional costs involved.
44
Co-commissioning of Primary Care South East London’s CCGs and NHS England Primary Care Joint Committees
Primary Care Joint Committees (PCJC) Meetings DATE OF MEETING: 11 February 2016
ENCLOSURE: J
PMS Commissioning Intentions: Bromley CCG AUTHOR: Jessica Arnold, Head of Primary and Community Care
SUMMARY:
Bromley CCG, following confirmation of the final London offer between NHS England and London LMCs and considerable local engagement with GP practices and stakeholders, has commissioning intentions to offer the following services within the PMS contract:
• London offer KPIs (cervical screening, immunisations and patient voice measures relating torecommending the surgery and confidence in the GP)
• Additional technology use to provide online booking and cancellation, repeat prescriptions andelectronic consultations Local priorities to include end of life care planning, bowel and breastscreening, suture removal and housebound visiting
• Transformational priorities to include practice development to secure sustainable and qualityprimary care services and deliver Integrated Care Networks in Bromley
The current PMS premium of £2.16 million in Bromley will be reinvested entirely in PMS practices and augmented by additional investment into GMS practices or other providers to provide these top priority services to the whole Bromley population by 2017/18.
The CCG recognises that there will be a cost pressure of £167,000 because not all PMS practices currently sign up to all elements of the PMS contract; however, the CCG is aiming to provide this ‘top up’ investment to bring all PMS practices up to the same offer and therefore providing the same services for their patients.
KEY ISSUES:
London Transformation programme: Bromley CCG’s commissioning intentions support the London transformation programme by weighting a large proportion of the PMS premium on delivery of Integrated (Local) Care Networks as well as supporting the High Impact priority of End of Life care.
Impact on GMS and APMS practices: Bromley CCG is committed to offering equalisation of the offer to GMS practices and patients compared with PMS practices and patients. GMS practices comprise 19 of Bromley’s 45 practices and account for 37% of patients. The CCG is currently undertaking full financial modelling and aspires to offer all GMS practices the option to deliver all PMS services from 1st October 2016. The risk exists that few GMS practices will take up the offer to deliver PMS contract services. The CCG is engaging with GMS practices as part of local discussions and also working with the GP Alliance and other stakeholders to better understand appetite and capacity. Both APMS contracts held by NHS England (London) with 45
Annex 5

Bromley practices are being reviewed in synergy with the London offer and the CCG is committed to achieving equalisation of both of these practices within the financial year 2016/17.
Summary of any additional local issues: Bromley CCG’s commissioning intentions have been informed by robust and ongoing discussions with lay members, GP practices and the LMC. Affordability in light of the 2016/17 allocations is currently being worked through and the CCG is exploring options to offer full equalisation within relatively short time periods. As some elements of the proposed new PMS contract will be transformational, the definitions and service specifications will be developed in the period until contract finalisation up to 31st March.
RECOMMENDATIONS:
The Bromley Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Bromley Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Bromley Local Medical Committee, according to the timetable outlined.
CCG CONTACT: Name: Angela Bhan E-Mail: [email protected]
AUTHOR CONTACT: Name: Jessica Arnold E-Mail: [email protected]
46

BROMLEY CCG PMS COMMISSIONING INTENTIONS
1 London Standard KPIs
CCG to confirm that they are going to complete the full Mandatory KPI suite?
Bromley CCG can confirm that they will be offering the full mandatory KPI suite, covering screening and immunisations, and the following two patient voice indicators:
a) Would you recommend your GP surgery to someone who has just moved into your local area?
b) Did you have confidence or trust in the GP you saw or spoke to?
These patient voice indicators have been selected because the CCG feels that recommending one’s practice is a good measure of overall satisfaction and is in line with the Friends and Family Test. Confidence and trust in one’s GP is a good measure of the quality of the consultation from past experience and likelihood of using primary care services before going through emergency care in the future.
The achievement in 2015 of patients probably or definitely recommending their GP practice to someone loving into the area was 75%. The achievement in 2015 of patients reporting they had confidence or trust in their GP was 92%, with variability in performance between practices being 79% - 99%.
The CCG chose not to offer the other patient voice indicators because:
‘Overall experience of the GP surgery’ is a duplication of asking patients if they wouldrecommend their surgery, and the latter is more in line with the FFT so it was selected
‘Ease of reaching the surgery by telephone’ could be redundant in the future for some patientsif electronic access is improved and successful
‘Convenience of the appointment’ was not deemed by the CCG to be as important as quality ofthe consultation and thus a measure of confidence and trust in the GP was selected instead
‘Overall experience of making an appointment’ was supported by the CCG as a good measurebut only two patient voice measures can be selected, and the CCG felt overall recommendationof the surgery and confidence in the GP were stronger measures of what the PMS contractaims to achieve locally
The CCG will not be offering the optional KPI of attendance at unscheduled care facilities during core hours within the PMS contract as this will be subject to factors beyond the control of individual PMS GP practices.
2 Premium Access Service Specification
Is the CCG going to complete the full access service specification? If answer is Yes - move to question 3, If answer is no, but the CCG is going to choose some areas from the service specification, complete rows 32-34 with Yes/No answers. Additional comments can be added as required.
No. Only one of the three proposed premium access service specifications will be offered to Bromley PMS practices.
47
If the CCG is not planning to offer any of the service specification, please given comment on rationale for this:
Not applicable.
a) Weekend additional capacity
After careful consideration and in-depth discussion with practices, the CCG feels that mandatory Saturday morning opening would not be suitable for all PMS practices. This is for a combination of reasons:
• Many practices open on Saturday mornings already through the Enhanced Hours DESscheme. To receive monies from both the PMS premium and the DES, practices wouldneed to do their extended hours another time (evenings or Sundays) or open for longer ona Saturday than the 9am-1pm session proposed within the London Offer. This will not befeasible in some practices, in particular smaller practices or those experiencing significantworkforce problems. Therefore, there is a risk that affected PMS practices would forfeitDES monies received if they cannot offer both extended hours and Saturday opening inaddition to the 8.30am-6pm core hours
• Bromley has two primary care access hubs in place offering booked appointments onSaturdays (and Sundays) whereby the GP has access to patient records and can makeonward referrals. This offers 100% population coverage. The hubs were opened on 1st
December and ongoing evaluation and adjustment during this time means the hubs willalso take urgent appointments via NHS 111 and out-of-hours GPs from Easter 2016, aswell as routine and semi-urgent appointments via GP practices. The CCG is also looking atoptions for a third hub in line with the out-of-hospital transformational plans for threeIntegrated Care Networks in Bromley. Average utilisation of hub appointments onSaturdays in the first five weeks of operating is 64% suggesting there is surplus capacity atthe current time. As the hubs continue, we expect utilisation to increase as GP practicesbecome more familiar with referring for Saturday appointments and NHS111 and out-of-hours GPs also start referring. The CCG will continue to monitor and adjust the scheme aspatient need dictates and in line with the Strategic Commissioning Framework ambitions forSaturday morning opening
• Some practices are facing significant workforce difficulties that mean they would be unableto accommodate Saturday morning opening. Bromley has amongst the highest proportionof GPs within five years of retirement age, increasing numbers of GPs who are choosing toretire in their 50s and a shortage of practice nurses. Therefore, the sustainability of thegeneral practice workforce is a priority
• Some practices report that they have offered Saturday morning opening in the recent pastbut utilisation of appointments was low. While no formal evaluation of this has taken placeand reports of low utilisation are anecdotal, the CCG is working with the GP Alliance to lookat weekend access hub referrals by GP practice to boost utilisation from practices that donot open on Saturdays
b) Technology to improve access
Yes. Bromley CCG including member practices were in support of making appointments available and cancellable online, and ordering repeat prescriptions online. There was some concern that 50% of appointments being available online would disadvantage patients without internet access (who arguably have a greater need for appointments, e.g. if they are elderly or poor). This would be partly mitigated because greater online access would free up telephone lines to improve access by telephone.
48

Provision of electronic consultations received a mixed response from both clinical leaders and the wider GP membership. Some were doing this already and felt it was very successful; many were concerned about a range of difficulties that email consultations might present. These included:
• increased risk of missing symptoms• difficulties with ‘closing down’ a conversation• unfairness to patients who have to wait for an appointment• risk of missing urgent cases that are emailed out of hours• information governance threats by emailing unsecure email addresses• inability to identify who is actually emailing• risk of abuse• GP time requirements• lack of an evidence base that email consultations reduce patients afterwards coming into
the practice or going to secondary care
The CCG will seek to address these concerns as part of the local implementation plan working with NHS England, the LMC and GP practices. This will have regard for the raft of recent guidance issued on managing electronic or remote consultations in general practice by NHS England, HSCIC and the GMC. Options include offering email consultations as follow ups rather than first appointments with the GP and expanding the definition to include telephone consultations and videoconferencing.
The CCG recognises that the adoption of additional technologies to improve access for patients will require support and varying amounts of lead-in time by practice. Once the new PMS contract is agreed and definitions of the service specification for additional technology use have been clarified through the London Offer, Bromley CCG will first scope from PMS practices what systems and provision they already have in place, and then dedicate a project manager with IT expertise to working with practices in readiness for adoption from 1st July 2016. There will also be Communications support offered by the CCG to manage the communications to patients of PMS practices that they can soon expect appointments and repeat prescription ordering to be available and cancellable online, and email consultations.
There is a risk that some practices are unwilling to do electronic consultations. For practices that felt concern and resistance to offering email consultations, the CCG will broker arrangements whereby these can offer email consultations as follow ups and alongside telephone consultations in the first instance. This will be scoped with practices and experts prior to finalisation of the new PMS contract on 31st March.
Minimal additional costs are expected to be incurred, comprising mostly of amendments to practice websites and electronic systems. Where equipment might be needed, e.g. headsets for telephone consultations or videoconferencing facilities, this will be assessed and agreed on a practice-by-practice basis.
3 Other commissioning intentions
What other commissioning intentions are the CCG planning, including any potential out of hospital services, or interpractice services? CCG must detail any service/s in full, how service will be measured, what the outcomes are/expected, is it equitable across the CCG, is it value for money, how does it meet the needs of the local population, and does service meet the requirements of the Strategic Commissioning Framework?
Bromley CCG’s local offer commissioning intentions are set out in this section. The allocation of funding to each of these services is set out in section 8 of this template.
49

• End of Life care planning (KPI)This is currently an optional service within the PMS contract, which 23 of the 24 PMS practices(96%) have opted to deliver. In Bromley, this KPI is working well towards managing care forend of life patients. Practices have supported keeping this KPI in the contract and some reportthat they are exceeding the 0.25% target for care plans. In recognition that at any one time, 1%of the population is at the end of life, the CCG proposes to extend this KPI in scope to target0.5% of list size.
End of Life care planning is being supported by wider End of Life projects such as roll out ofthe Coordinate My Care tool across the borough and by local services including communityand hospice palliative care services. Inclusion of this KPI in the PMS contract is in line withBromley’s strategic priorities and position as a recognised leader for excellent End of Life care,and the CCG proposes to enhance this further through the PMS contract.
This is low risk as it is already happening and no additional costs on top of those alreadyearmarked for End of Life care will be incurred.
• Bowel screening (KPI)This KPI aims to achieve an increase in both referrals and uptake of referrals for bowelscreening and subsequently improve early and overall diagnosis rates for bowel cancer. Thespecification for GP practices to undertake enhanced referrals to bowel screening will involve:
o proactive referring people for bowel screening (which practices should be doing already)o chasing up non-responders (which, as practices already get notification of non-responders,
requires only staff time rather than putting any new systems into place)o distributing kits (this will be a relatively simple task for the GP once the patient has been
identified for screening). The CCG is aiming to distribute testing kits through GP practices,if possible subject to discussion with the national bowel screening campaign
The CCG will work with the national bowel screening campaign over coming months to make arrangements for kits to be distributed into practices and any required training or information materials to be supplied for GPs and for patients. This is expected to be achieved by the commencement of the new PMS contract from 1st July 2016.
The risk exists that bowel screening uptake will remain low and bowel cancer late detection and detection in A&E will persist. This will be mitigated by working with the practices and the national campaign to understand what works and what does not work when referring patients for screening, support with patient engagement and communications, and working with Public Health to understand trends as they persist or change.
• Breast screening (KPI)This KPI aims to achieve an increase in referrals and uptake of referrals for breast screening,and subsequently improve early and overall diagnosis rates for breast cancer. It will involveGPs following up patients who do not take up screening and encouraging attendance. TheCCG will utilise the work conducted on this KPI by NHS England as part of the PMS review.This is a local priority for Bromley’s population (see section 9).
• Suture removal (price per patient)This is a service required from PMS practices to mitigate the risk of patients going to hospital tohave sutures removed. Suture removal is not currently in the community services contract butis offered by GMS practices under a Local Incentive Scheme.
• Housebound visiting (price per patient)This is an important service for a vulnerable group of patients. Local engagement found thatpractices were eager to keep housebound visiting within the PMS contract to enable them toset aside time for housebound visiting in the context of the growing pressures in the surgery.Currently, 23 of Bromley 24 PMS practices provide this service (96%). Further engagement will
50

be undertaken with practices following commissioning intention development up to 31st March to understand how housebound populations vary and agree if necessary an updated definition of ‘housebound’ and service specification.
• Additional reception time outside of core hours (price per patient)This is currently an optional service within the PMS contract that patients have come to expectand that improves access to primary care. Practices felt that removing this incentive could leadto ‘taking a backwards step’ towards better patient access. Currently, 19 of Bromley 24 PMSpractices provide this service (79%). The CCG will support those practices not currentlyoffering this service to agree a way forward
• Additional nurse time outside of core hours (price per patient)As above re: reception time. Also, additional nurse time out of hours can alleviate the pressureon GPs and walk-in centres/UCCs. Currently, 13 of Bromley 24 PMS practices provide thisservice (54%). The CCG will support those practices not currently offering this service to agreea way forward
• Practice development investment (specification)This specification will be asking practices to sign up to producing and implementing a practicedevelopment plan, including plans for long term sustainability of the workforce, training andeducation needs, improved appraisal arrangements, peer review participation, service andresource sharing and other measures to improve how the practice is adapting to meet patientneeds. This comes in response to a clear message from Bromley GP practices that the biggestrisk to patient care is the threatening unsustainability of primary care as it is currentlyoperating.
The first stage of offering this service to practices to support their long term sustainability willbe an in-depth scoping of the main challenges faced by practices and their needs in order to beable to deliver high quality, full coverage services to the population of Bromley. A tailored planfor practice development will be required from each practice, which will require up to threemonths to develop. Appraisal, peer support and development sessions will need to be includedin the plan, as well as plans for additional nurse and GP time. Larger practices will need toproduce a development plan commensurate with their list size, in recognition of the additionalfunding they will receive as a price per weighted patient. This approach is subject to furtherdevelopment.
It is anticipated that the practice development investment element of the PMS offer will requirea lead in time of up to six months from when the new PMS contract is approved (31st March)and will therefore not be on offer until quarter 3 (1st October) of 2016/17. The plan is expectedto outline practice development over the three year period up to March 2019.
The additional investment required to support practice development will be made availablethrough a significant amount of the PMS premium being allocated to this element of the newcontract. The risk exists that despite undertaking this process, the impact on general practice islimited and workforce and other organisational challenges continue to threaten patient care.This will be mitigated through the CCG taking a collaborative approach with practices to fullyunderstand their individual risks, and by investing on a sufficient scale to be able to drivechange.
• Transformational specifications to deliver Integrated Care Networks (specification and KPIs)This will be linked to delivery of Integrated Care Networks in Bromley and will comprise:
o Signing up to the ICN Memorandum of Understanding and committing to work withcommunity and other services within the Network structure
o Participation in Integrated Case Management scheme to deliver improved care planningand support to at-risk patients through multi-disciplinary team working. Cases will beidentified through a combination of risk stratification and clinical opinion, the latter being
51
important for identifying the deteriorating cases that are not yet in the top 2% but require input before their problems escalate. Further definition of the Integrated Case Management scheme will be agreed at a clinical round table discussion with local GPs on 17th February
o Actively working with care coordinators and navigators for a minimum number of hours orreferrals per week (based on list size), also to be confirmed at the clinical round table on17th February. The care coordinator and navigator roles (clinical and non-clinicalrespectively) will be commissioned by the CCG as part of the investment into supportingprimary care and integrating with other parts of the health system, social care and thevoluntary sector. Engaging with care coordinators and navigators might be undertaken bythe GP, practice nurse, practice manager and/or other staff and might take placeelectronically, by telephone or in person at the practice
o Increasing identification and support to carers including: maintaining a carers register actively promoting Health Checks to carers distributing advice and information materials from the practice referring as appropriate to non-clinical care navigators to support the carer holistically inviting known carers to carer participation groups /forums held either by the practice
or shared by several practices across the Network
The inclusion of ICN participation within the PMS contract will be developed over coming months in line with the wider out-of-hospital transformation strategy to establish three ICNs, and associated new ways of working, in Bromley. Practices have been engaged in the transformation plans through commissioner events in July and January and through the cluster meetings, and so should be familiar to greater or lesser degrees with these concepts and the direction of travel. Further refinement of the specifications for this element of the PMS contract will be developed to complement changes afoot in the wider health and social care system. It is anticipated that the transformational element of the PMS offer will require a lead in time of up to six months from approval and will therefore not be on offer until quarter 3 (1st October) of 2016/17.
The risk exists that some practices will not take up the specification to deliver ICNs and thus there will be inconsistency of services and patient care. This presents a risk to the population that will be mitigated by continued ongoing dialogue with practices, a focused and achievable implementation plan for ICNs and supported by the CCG and wider healthcare partners to bring about improvements together.
4 Engagement
Please give details as to what engagement has taken place with practices, patients or other third party services to complete your PMS commissioning intentions:
In addition to internal engagement across the CCG’s directorates and with Clinical Leads and lay members, the CCG has undertaken the following external engagement:
• Engagement with GPs and other practice staff through the January cluster meetings. Thisincluded presentation of the London Offer and in-depth discussion and debate about localpriorities. This directly shaped the CCG commissioning intentions
• Informal discussions with individual practices prior to and after the cluster meetings to gatherwider views recognising that not all attendees speak at the cluster meetings
• Informal discussions with the Bromley LMC at the commencement of the process and topresent the draft commissioning intentions following GP engagement at cluster meetings
• No patient engagement has yet been undertaken specifically on the PMS contract changes;however, this will be part of the out-of-hospital transformation plans which will be partlydelivered through the PMS contract transformational specifications
52
Conflict of interest of CCG Clinical Leads has been managed by:
• CCG Clinical Leads have been engaged as commissioners at two meetings with governingbody members and at the Primary Care Programme Board where the clinical merit ofchanges to the PMS contract were discussed
• In-depth financial discussions about how we allocate the PMS premium have not includedClinical Leads and were between managerial staff only
• Clinical Leads have explicitly stated (out loud) their conflicts of interest at the beginning ofany meeting covering the PMS review
• Any presentations to the Clinical Leads with notional prices next to each service (e.g. the‘London Offer’ slide) were not the subject of debate and it was made explicitly clear thatthese pricings were indicative only, subject to allocations and negotiations
• The CCG engaged on the PMS review with it’s member practices, thus diluting the Conflictof Interest risk from just the Clinical Leads and offering a more robust approach
Conflict of interest of CCG member practices was managed by making it clear at the beginning of all cluster meetings that this is a commissioning subject (the cluster meetings are commissioning meetings) and keeping the conversations to clinical merit of services as strictly as possible.
5 Impact assessments on practice stability following PMS contract changes
Has the CCG completed any impact studies on services that potentially will need to cease in practices, or if funding will cease that currently may financially support clinicians in practices and to ensure that practice stability can be maintained throughout the transition? Please give details:
The majority of services offered through the current PMS contract will continue to be offered through the new contract. The only exceptions to this are patient choice to access advice (although email and possibly telephone access will be offered through the additional technology use service specification) and guaranteed same day clinical response (also supported through additional technology use, enhanced hours and access hubs).
Where practices feel they cannot take up all of the PMS services and/or there is a risk that the practice will revert to a GMS contract, the CCG will work closely with these practices to agree what is achievable and aspirational, and how they might be supported through other means, e.g. through the Bromley GP Alliance.
6 Transition
Two years of transition is allowable for practices in line with national guidance. Following further national clarification, it is confirmed that a longer transitional period can be considered by regional teams with CCGs on a case by case basis as part of negotiations but this will not be considered on a CCG wide basis. All transitional periods must end by March 2020/21.
CCG to give full explanation as to how they will transition to new services they have advised they will be commissioning above. This should include as a minimum how it will be rolled out across the CCG. Length of time it will take to be up and running, any risks or additional costs involved.
Not applicable.
53
7 Equalisation
Equalisation to GMS in 2016/17 should be delivered where strategically and financially possible. In cases where this is not possible, CCG areas will be required to set out their plans for equalisation in their commissioning intentions submission in February and show strategic plans for achieving it as part of Sustainability and Transformation plans submitted in June 2016. Plans will need to show equalisation before 2021 to ensure equalisation is achieved in the planning period. Note that as a minimum, where CCGs have not achieved funding equalisation within PMS practices this will need to be achieved by 2016/17.
CCG to give explanation of how they will seek to achieve equalisation within the prescribed timeframe. This should include a timescale for implementation, any risks and additional costs involved.
Bromley CCG is committed to offering equalisation of the offer to GMS practices and patients compared with PMS practices and patients. GMS practices comprise 19 of Bromley’s 45 practices and account for 37% of patients.
If the full PMS premium was offered to GMS practices, and uptake was 100%, this would create a cost pressure to the CCG of £1.4 million per annum. The CCG has an option to offer some elements of the PMS contract to GMS practices in 2016/17 and the remainder in 2017/18, the prioritisation of which would be subject to local ongoing discussions with GMS practices and the LMC. However, the CCG is currently undertaking full financial modelling and aspires to offer all GMS practices the option to deliver all PMS services from 1st October 2016. As this is a part year cost pressure that can be mitigated in-year, this would present a preferable situation compared with waiting until April 2017 to offer GMS practices the full complement of services.
The risk exists that the CCG does not know the likely level of uptake of PMS services by GMS practices, which will have a direct impact upon how we model affordability of the whole suite of PMS services being offered to GMS practices. Therefore, once the PMS contract is finalised by 31st March, the CCG will ask for Expressions of Interest from GMS practices about offering the equivalent services in their practices.
Another risk exists that few GMS practices will want to offer few or none of the PMS services. If this transpires to be the case, the CCG will look at other options to provide these services to GMS patients, e.g. through borough wide schemes, potentially provided by the GP Alliance on a 100% population coverage basis. However, if the quantum of what is required to provide all services to all patients is too great, a further risk exists that the GP Alliance will not have the capacity to provide all of the required services. The CCG will consider prioritisation and phasing of the GMS offer if this scenario transpires, working closely with key stakeholders and engaging other potential providers where possible to achieve population coverage as sustainably and quickly as possible.
Both APMS contracts held by NHS England (London) with Bromley practices are being reviewed in synergy with the London offer. NHS England (London) will seek to agree with the two APMS practices that as a minimum, they provide the London Offer being commissioned by the CCG within the existing contract price. Further services offered by APMS practices will be subject to affordability and considered as part of the ongoing equalisation process. However, the CCG is committed to achieving equalisation of both of these practices within the financial year 2016/17.
8 Costs and Investment planning
CCG to give full details of any costs and investment plans they have for the following 2 years, including any impacts this will have on service delivery of the commissioning intentions noted above or any new incentives they may wish to deliver.
54

The key financial priority for the Bromley health system is to achieve financial sustainability across all providers. The development and investment in primary care is a key priority in achieving that goal as part of the wider transformation of out-of-hospital care.
Bromley CCG is committed to ensuring the total value of the PMS premium does not decrease below the current level of £2.16 million. However, not all practices currently sign up to the full value of the services, set at £12.26 per patient, with the average across all PMS practices being £11.35. Offering the full value of the £12.26 per patent to all PMS practices would cost an additional £167,000, which is made up of two elements. There would be a £25,000 shortfall in the core PMS offer and £142,000 for the increase in PMS premium to those practices currently not at the full value. The CCG however, is aiming to provide this ‘top up’ investment to bring all PMS practices up to the same offer and therefore providing the same services for their patients.
In addition to this, if the full offer of £12.26 was made to GMS practices, the financial modelling indicates that an additional investment of £1.426 million would be required.
Both these additional investments represent a significant cost pressure to the Bromley health economy, currently already under financial pressure with an acute provider in Kings College Hospital reporting a significant underlying deficit and a challenging five year recovery plan.
Allocations for the next three years have now been announced. Bromley CCG will be receiving a 4.3% uplift (2.9% underlying after accounting for national policy changes) in 2016/17 followed by reductions for 2017/18 (2.2%) and 2018/19 (2.5%).
With the additional uplift in 2016/17, there is a key expectation that transformation of the health system is progressed at pace and the areas identified in the PMS contract commissioning intentions are aligned to the wider out-of-hospital objectives.
Wider investment requirements to support the Bromley CCG strategy and targets include the continued investment in acute hospital services to meet statutory requirements, including A&E, RTT and cancer target, as well as quality improvements towards the London standards.
As part of the wider system support and transformation, further investment has been prioritised for the continued development of the Integrated Care Networks, linked to the Memorandum of Understanding to be agreed across all organisations in Bromley. Other investment plans include the continued development of emergency care with the Discharge Bureau and ‘Discharge to Assess’ beds and the continuation of the primary care access hubs set up as a pilot in 2015/16. In line with national guidance and the Parity of Esteem requirements, the CCG will continue to invest further in Mental Health services.
Clearly the value of these commitments are significant and the CCG QIPP savings target for 2016/17 is between £8m to £10m representing between 2% to 2.5% of the CCG allocation. This will need to be delivered to allow these investments to take place.
All investments, including those identified for the PMS premium and GMS equalisation, are subject to affordability and the GMS investment may need to be phased over a two year period before full roll out. These have been factored into the CCG three-year plan.
The costs of APMS changes are still be determined as more contract information is required, particularly as there is already a synergy between the London Offer and the current APMS contracts. However, as with GMS equalisation, this would be subject to affordability but expected to be rolled out on the same timetable as GMS equalisation.
Breakdown of proposed PMS Premium funding The proposed allocation of funding from the PMS premium for each of the component services within these commissioning intentions is set out below. These have been represented as
55

proportions of available funding, given the total quantum of available funding is subject to the circumstances set out in the preceding paragraphs within this section of the template.
London offer Mandatory KPIs (screening, immunisations, patient voice) 27%
Additional technology use 9%
Subtotal: 36%
Local priorities End of Life care planning 4.5%
Bowel screening 3.5%
Breast screening 3.5%
Suture removal 1%
Housebound visiting 3%
Subtotal: 15.5%
Transformational
priorities
Practice development investment 21%
Delivery of Integrated Care Networks 27.5%
Subtotal: 48.5%
Total: 100%
9 Wider Commissioning Intentions
How do the PMS Commissioning intentions described above fit in with the wider CCG commissioning intentions for the following year (2016/2017) where applicable note how this fits in with the Joint Strategic Needs Assessment (JSNA):
Bromley CCG’s PMS contract commissioning intentions are in line with the wider strategic context and aspirations at local, South East London, London and national scales. They support the following wider strategic aims:
• Improving primary care access. Following the Prime Minister’s Challenge Fund, CCGs areunited in the need to improve access to primary care as the first port of call for patients and aslist holders central to local health economies. Not just looking at ‘more access’, but exploringdifferent ways of how can primary care work to meet patient needs is reflected in the CCG’scommissioning intentions relating to technology use, additional reception and nurse time andhome visiting, and participation in ICNs
• A focus on general practice sustainability is a local priority for Bromley CCG given thedemographic of it’s GPs, practice nurses and wider primary care staff and persistent anddeepening workforce challenges. While lack of available clinical staff in many fields includingGPs is a national problem, it is acutely felt in Bromley with increasing numbers of GPs retiringin their 50s and a deficit of practice nurses in particular. The decision to include practicedevelopment investment in the PMS commissioning intentions is therefore a decision andproactive step towards working with general practice to alleviate these pressures and arisingrisks to patients. This supports the work across London as well as that of the Our HealthierSouth East London strategy and locally within the Community Education Provider Network(CEPN) development plan
56

• Bromley’s out-of-hospital transformation plans and ongoing development of Integrated CareNetworks has arisen directly from the Our Healthier South East London out-of-hospitaltransformation strategy. It is consistent with the NHS Five Year Forward View and movementinternationally towards multi-specialty community providers, accountable care organisations,primary and acute care systems and other models of integrated, system wide and shared care.Using the opportunity of the PMS contract review to embed new ways of integrated workinginto general practice will help to drive change locally in the context of the supra-local strategy
• End of Life care is a priority workstream for Bromley CCG as the borough has amongst thehighest proportion of older people in London, and a rapidly growing cohort of patients aged75+, 85+ and 100+. This is associated with higher than average incidence of dementia,multiple and complex long term conditions and social isolation. See the Bromley JSNA formore information. End of Life care is also a South East London high impact (‘big hitter’) priority
• Bowel screening is a local priority for Bromley. The borough has consistently unperformed inthe detection of cancer early at stages 1 and 2 and diagnoses through the two week wait havebeen lower than average which impacts on survival rate. The 2015 JSNA shows that ourpopulation is aging, increasing cancer prevalence of cancer, and also highlights concernsaround obesity (we are the 6th most obese population in London). Cancer causes 30% of alldeath in Bromley and digestive tract cancers accounts for 28.4% of all cancer deaths. Inpatientadmission data shows that bowel cancer in Bromley patients is not being detecting earlyenough and patients are presenting for treatment much later. This reduces survival rates aswell as demanding more intensive intervention
• Breast screening is a local priority for Bromley, as identified in the JSNA. Breast cancer is themost common cancer in Bromley and incidence is higher than the London average. Screeningrates have improved from 74% up to 77% in the last five years, on a par with the nationalaverage and better than the London average, but it still remains a key priority for the Bromleypopulation
10 Other Information
Has the CCG got any other information/documents to support these PMS commissioning intentions?
Definitions and outline specifications of the local commissioning intentions for the following services will be available during the period of negotiations with the LMC and preparation to implement with GP practices:
• End of Life care planning• Bowel screening• Breast screening• Suture removal• Housebound visiting• Additional reception time outside of core hours• Additional nurse time outside of core hours• Practice development investment• Transformational specifications to deliver Integrated Care Networks
Please also note that for additional technology use (provision of electronic consultations) within the London Offer, Bromley CCG proposes that the local definition includes offering email consultations for follow ups and includes telephone consultations.
57
Co-commissioning of Primary Care South East London’s CCGs and NHS England Primary Care Joint Committees
Primary Care Joint Committees (PCJC) Meetings
DATE OF MEETING: 11 February 2016
ENCLOSURE: J
Title: PMS Commissioning Intentions: NHS Greenwich CCG AUTHOR: Jan Matthews, Primary Care Manager (interim)
SUMMARY:
Assessment of local position following the confirmation of the final London offer between NHS England and London LMCs: NHS Greenwich CCG will implement the London Offer with weekend additional capacity through Saturday morning opening for all PMS Practices, the mandatory KPIs and the Tech offer.
Summary of how the remaining funds/premium will be spent: We propose to use our remaining premium to implement the Breast Screening KPI, a KPI for Lung Cancer screening, and a KPI to increase Saturday morning access to GP registration. These are fully in line with our commissioning priorities in Greenwich – improving public health (specifically targeting cancer) and improving GP registration. These priorities have been agreed with the Health & Wellbeing Board.
The current PMS premium will be reinvested in general practice.
KEY ISSUES:
London Transformation programme: As part of the work being undertaken across south east London, we are moving towards implementing the Strategic Commissioning Framework for primary care. This includes the Saturday morning opening for all practices (included in the PMS Premium) and during 2016/17 we will be implementing changes in overall GP access to ensure that there is a Local Care Network focused offer for patients in their locality on Saturday afternoons and Sundays. Locally this initiative is known as “Right Care, First Time” and includes changes to urgent and out-of-hours care that were implemented in 2015.
Impact on GMS and APMS practices: Minimal – we will ensure that similar offers are made to our one GMS practice, and our
58
Annex 6

APMS practices.
Summary of any additional local issues: NHS Greenwich CCG is working closely with local general practice to move to improve access for local patients, and will discuss the detail of these proposals with the local LMC and all practices via our four local Syndicates. These PMS Commissioning Intentions are part of this picture, and relate as well to the improvements in access linked to “Right Care, First Time”.
RECOMMENDATIONS:
The Greenwich Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Greenwich Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Greenwich Local Medical Committee, according to the timetable outlined.
CCG CONTACT: Name: Simon Hall, Deputy Chief Officer E-Mail: [email protected]
AUTHOR CONTACT: Name: Jan Matthews, Primary Care Manager (interim) E-Mail: [email protected]
59

CCG Name NHS Greenwich CCG
London Offer
1 London Standard Key Performance Indicators (KPIs)
Is CCG going to offer? Additional Comments
Cervical screening
Childhood Immunisation ‐ 5‐in‐1 Vaccine by 1 Year
Childhood Immunisation ‐ aged 5 years and over.
Flu Immunisation 65+
Flu Immunisation Under 65 at risk
Pneumococcal Immunisation 65+
Overall Experience
Percentage of patients responding within the 'good' range to the question "Overall, how
would you recommend your experience of your GP Surgery?"
Telephone
Percentage of patients responding within the 'easy' range to the question "Generally,
how easy is it to get through to someone at your GP Surgery on the phone?"
Convenience of appointment
Percentage of patients responding within the 'convenient' range to the question "How
convenient was the appointment you
were able to get?"
Experience of making an appointment
Percentage of patients responding within the 'good' range to the question "Overall, how
would you describe your
experience of making an appointment?"
Yes Focussing on this indicator should drive
up performance overall. Greenwich
CCG remains below the England
average for this indicator. In January
2016 The National GP survey for
Greenwich was at 69% London was
69% and the England average was 74%.
Recommendation
Percentage of patients who would definitely or probably recommend their GP Surgery
Yes Greenwich CCG achieved 73% in the
2016 survey. National average is 78%.
We hope to raise achievement by
focussing on this indicator
Capacity & Access Measures
Average Attendance at local unscheduled care facilities (including WIC, UCC and A&E)
for non‐admitted patients during Core PMS hours
No
2 Premium Access Service Specification
Is CCG going to offer? Additional Comments
Yes
Is CCG going to offer? Additional Comments
Yes
3 Other commissioning intentions
4 Engagement
Patient Voice
Vaccinations and Immunisations
PMS Commissioning Intentions ‐ Which must be completed as a minimum for CCG Commissioning intentions return
documentation.
CCG to confirm that they are going to complete the full Mandatory KPI suite?
CCG to confirm which two patient voice areas they are going to add to their mandatory KPI suite from the below options:
London Standard KPIs
Screening
Yes
What other commissioning intentions are the CCG planning, including any potential out of hospital services, or interpractice services?
CCG must detail any service/s in full, how service will be measured, what the outcomes are/expected, is it equitable across the CCG, is it value for money, how does it meet the needs of the local
population, and does service meet the requirements of the Strategic Commissioning Framework (SCF ‐ Copy available on request)
PROACTIVE: Greenwich CCG have selected KPIs on breast cancer and lung cancer. These are both significant health challenges for the population of Greenwich, and we believe that this push on
screening via primary care will make a significant contribution to early detection and treatment.
ACCESSIBLE: Patients have told us that they find registration with a GP difficult, so we are enabling Saturday registration through one of our KPIs. Additionally (as part of our Long Term
Conditions primary care contract that is already in place) we will be ensuring that all practices are able to share their GP records via Vision 360 enabling practices to work towards Network‐based
access on Saturday afternoons and Sundays. This compliments the Saturday morning offer outlined above.
Greenwich CCG has an overall premium of £10.24. Once the mandatory KPIs of £3.04, the £1.00 for Tech per weighted patient and the Saturday morning £4.00 per registered patient are
deducted we have £2.15 to allocate for our three named KPIs, Breast Cancer screening, Lung cancer screening and Patient registration access.
The CCG intends to deliver patient and public engagement via Health Watch and its Patient Reference Group. A great deal of patient and public engagement has already been done via the OHSEL
events programme on what Greenwich residents wanted to see in Primary Care.
1. Patient Reference Group meeting 17.12.2016
2.Syndicate engagement 6.1.2016 29.1.2016
3.Joint NHSE & CCG PMS workshop 28.10.2015
4. SEL Primary care Joint Committee 28.10.2015
5.Primary care Joint committee 10.12.2015
6. Greenwich wide membership forum 13.1.2016
7. Local LMC pre engagement 8.1.2016 and 4.2.2016
8. The CCG is implementing the PMS review as part of a wider piece of work improving GP access in the borough
Please give details as to what engagement has taken place with practices, patients or other third party services to complete your PMS commissioning intentions :
If the CCG is not planning to offer any of the service specification, please given comment on rationale for this :
Is the CCG going to complete the full access service specification? If answer is Yes ‐ move to question 3, If answer is no, but the
CCG is going to choose some areas from the service specification , complete rows 32‐34 with Yes/No answers. Additional
comments can be added as required.
Premium Access Service Specification
CCG to confirm if they will include the optional KPI on capacity and access:
Improving Access through the use of technology
Weekend Additional Capacity
Premium Access Service Specification ‐ Service areas :
60

5 Impact assessments on practice stability following PMS contract changes
6 Transition
7 Equalisation
8 Costs and Investment planning
9 Wider Commissioning Intentions
10 Other Information
Has the CCG got any other information/documents to support these PMS commissioning intentions?
Yes (NHS Greenwich CCG Primary Care Strategy, 2015 ‐ 2020). This document is available upon request
Improving Access will be carried out by implementation of the London Saturday access offer. We will be working to improve weekend access as part of a wider workstream , which will be
consulted on to go live in October.
The CCG is implementing the PMS review as part of a wider CCG programme of improvements in GP Access and services. It is anticipated that Saturday morning opening will go live in July with
further access improvements in October once a consultation process has been undertaken.
Our assessment is that the approach to the PMS review will not have an significant negative impact on the financial or operational stability of PMS Practices.
Has the CCG completed any impact studies on services that potentially will need to cease in practices, or if funding will cease that currently may financially support clinicians in practices and
to ensure that practice stability can be maintained throughout the transition? Please give details :
Wider Greenwich commissioning intentions can be broken into the following areas:
1. Transformation plans to changes services significantly (Ageing Well, Improvements to GP access linked to these commissioning intentions)
2. Contract termination/review notices where an alternative provision is available (particularly community services in light of Ageing Well programme, and move to Local Care Networks)
3. Improve efficiency through procurement (e.g. Musculoskeletal Services prime contractor procurement)
4. Payment efficiencies by reviewing contractual values
5. Delivery efficiencies by improving pathways/prevention (in line with Greenwich JSNA)
6. Better Care Fund – improve value
7. Contract to statutory minimum requirements
We have a challenging QIPP programme for 2016/17, as the CCG is facing major financial pressures.
Improvements to GP access include a proposal for consultation to implement the next phase of "Right Care, First Time" replacing the existing GP‐led walk‐in centre facilities with new provision on
a Local Care Network basis covering Saturday afternoons and Sundays ‐ facilitated by shared IT to ensure full GP records are available.
How do the PMS Commissioning intentions described above fit in with the wider CCG commissioning intentions for the following year (2016/2017) where applicable note how this fits in
with the Joint Strategic Needs Assessment (JSNA) :
CCG to give full details of any costs and investment plans they have for the following 2 years, including any impacts this will have on service delivery of the commissioning intentions noted
above or any new incentives they may wish to deliver.
GMS Equalisation : Greenwich has 1 GMS and three APMS Practices. The CCG is committed to funding the equalisation of the GMS Practice ; APMS Practices will move to equalised KPIs over
time. The majority of Practices in Greenwich are PMS and have equalised funding as a result of a previous review.
Equalisation to GMS in 2016/17 should be delivered where strategically and financially possible. In cases where this is not possible, CCG areas will be required to set out their plans for
equalisation in their commissioning intentions submission in February and show strategic plans for achieving it as part of Sustainability and Transformation plans submitted in June 2016.
Plans will need to show equalisation before 2021 to ensure equalisation is achieved in the planning period. Note that as a minimum, where CCGs have not achieved funding equalisation
within PMS practices this will need to be achieved by 2016/17.
CCG to give explanation of how they will seek to achieve equalisation within the prescribed timeframe. This should include a timescale for implementation, any risks and additional costs
involved.
2 years of transition is allowable for practices in line with national guidance. Following further national clarification, it is confirmed that a longer transitional period can be considered by
regional teams with CCGs on a case by case basis as part of negotiations but this will not be considered on a CCG wide basis. All transitional periods must end by March 2020/21.
CCG to give full explanation as to how they will transition to new services they have advised they will be commissioning above. This should included as a minimum how it will be rolled out
across the CCG. Length of time it will take to be up and running, any risks or additional costs involved.
61

Co-commissioning of Primary Care South East London’s CCGs and NHS England Primary Care Joint Committees
Primary Care Joint Committees (PCJC) Meetings
DATE OF MEETING: 11 February 2016
ENCLOSURE: J
Title: PMS Commissioning Intentions: NHS Lambeth CCG AUTHOR: Andrew Parker – Director of Primary Care Development
SUMMARY:
Assessment of local position following the confirmation of the final London offer between NHS England and London LMCs: The total identified PMS cost per weighted patient totals £94.13. Of this, £78.01 is the agreed cost of the core specification which, after the application of £3.04 for London KPI’s and £1.00 for the agreed London technology offer, leaves £12.08 for KPI’s/ Specifications at a local CCG level. This assumes that the Weekend Additional Capacity Saturday Morning opening commitments are met through GP Federation run Extended Access Services Hubs across the borough and not at an individual practice level subject to final local consultation.
Summary of how the remaining funds/premium will be spent: The remaining premium will be allocated proportionately to commissioning intentions associated with enabling the delivery of the CCG Strategy and London Strategic Commissioning Framework as Follows: Accessible care 15%, Proactive Care 30%, Co-ordinated care – 30%, Whole system Integration (LCN’s) 25%. This is subject to the finalisation of consultation regarding the Saturday morning opening model across Federations/with individual practices. The PMS premium will continue to be fully invested in general practice services and any underspend from underachievement of KPI’s will be retained locally for reinvestment and recovery.
KEY ISSUES:
London Transformation programme: The CCG is committed to ensuring that its investments are enabling the delivery of its local strategy, the ‘Our Healthier South East London’ Strategy and the London wide ‘Transforming Primary Care’ Strategic Commissioning Framework.
Impact on GMS and APMS practices: Resources have been set aside to ensure
62
Annex 7

equalisation. for the 4 GMS Practices in the borough. For the 6 APMS practices, we will be consulting with individual practices to incorporate KPIs into existing contractual arrangements.
Summary of any additional local issues: Detailed KPI’s/specifications are subject to final development through a clinically led short life commissioner group scheduled to conclude by end of February. The final Weekend Additional Capacity Saturday morning opening model to be delivered through Extended Access Services Hubs and individual practices is subject to final consultation to the same timescale.
RECOMMENDATIONS:
The Lambeth Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Lambeth Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Lambeth Local Medical Committee, according to the timetable outlined.
CCG CONTACT: Name: Andrew Parker - Director of Primary Care Development E-Mail: [email protected]
AUTHOR CONTACT:
Name: Andrew Parker - Director of Primary Care Development
E-Mail: [email protected]
63
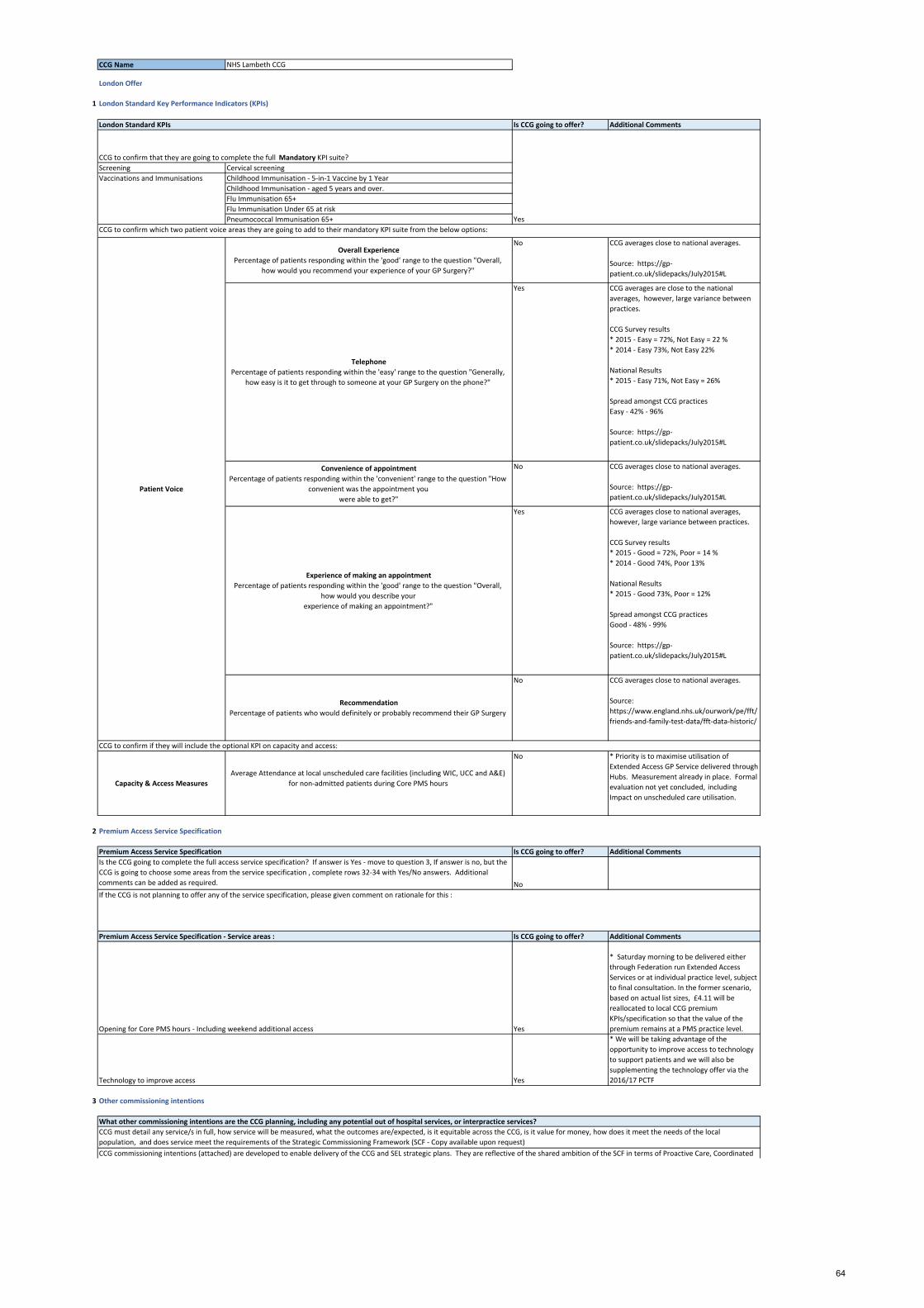
CCG Name NHS Lambeth CCG
London Offer
1 London Standard Key Performance Indicators (KPIs)
Is CCG going to offer? Additional Comments
Screening Cervical screening
Childhood Immunisation ‐ 5‐in‐1 Vaccine by 1 Year
Childhood Immunisation ‐ aged 5 years and over.
Flu Immunisation 65+
Flu Immunisation Under 65 at risk
Pneumococcal Immunisation 65+
Overall Experience
Percentage of patients responding within the 'good' range to the question "Overall,
how would you recommend your experience of your GP Surgery?"
No CCG averages close to national averages.
Source: https://gp‐
patient.co.uk/slidepacks/July2015#L
Telephone
Percentage of patients responding within the 'easy' range to the question "Generally,
how easy is it to get through to someone at your GP Surgery on the phone?"
Yes CCG averages are close to the national
averages, however, large variance between
practices.
CCG Survey results
* 2015 ‐ Easy = 72%, Not Easy = 22 %
* 2014 ‐ Easy 73%, Not Easy 22%
National Results
* 2015 ‐ Easy 71%, Not Easy = 26%
Spread amongst CCG practices
Easy ‐ 42% ‐ 96%
Source: https://gp‐
patient.co.uk/slidepacks/July2015#L
Convenience of appointment
Percentage of patients responding within the 'convenient' range to the question "How
convenient was the appointment you
were able to get?"
No CCG averages close to national averages.
Source: https://gp‐
patient.co.uk/slidepacks/July2015#L
Experience of making an appointment
Percentage of patients responding within the 'good' range to the question "Overall,
how would you describe your
experience of making an appointment?"
Yes CCG averages close to national averages,
however, large variance between practices.
CCG Survey results
* 2015 ‐ Good = 72%, Poor = 14 %
* 2014 ‐ Good 74%, Poor 13%
National Results
* 2015 ‐ Good 73%, Poor = 12%
Spread amongst CCG practices
Good ‐ 48% ‐ 99%
Source: https://gp‐
patient.co.uk/slidepacks/July2015#L
Recommendation
Percentage of patients who would definitely or probably recommend their GP Surgery
No CCG averages close to national averages.
Source:
https://www.england.nhs.uk/ourwork/pe/fft/
friends‐and‐family‐test‐data/fft‐data‐historic/
Capacity & Access Measures
Average Attendance at local unscheduled care facilities (including WIC, UCC and A&E)
for non‐admitted patients during Core PMS hours
No * Priority is to maximise utilisation of
Extended Access GP Service delivered through
Hubs. Measurement already in place. Formal
evaluation not yet concluded, including
Impact on unscheduled care utilisation.
2 Premium Access Service Specification
Is CCG going to offer? Additional Comments
No
Is CCG going to offer? Additional Comments
Yes
* Saturday morning to be delivered either
through Federation run Extended Access
Services or at individual practice level, subject
to final consultation. In the former scenario,
based on actual list sizes, £4.11 will be
reallocated to local CCG premium
KPIs/specification so that the value of the
premium remains at a PMS practice level.
Yes
* We will be taking advantage of the
opportunity to improve access to technology
to support patients and we will also be
supplementing the technology offer via the
2016/17 PCTF
3 Other commissioning intentions
What other commissioning intentions are the CCG planning, including any potential out of hospital services, or interpractice services?
CCG must detail any service/s in full, how service will be measured, what the outcomes are/expected, is it equitable across the CCG, is it value for money, how does it meet the needs of the local
population, and does service meet the requirements of the Strategic Commissioning Framework (SCF ‐ Copy available upon request)
CCG commissioning intentions (attached) are developed to enable delivery of the CCG and SEL strategic plans. They are reflective of the shared ambition of the SCF in terms of Proactive Care, Coordinated
CCG to confirm that they are going to complete the full Mandatory KPI suite?
CCG to confirm which two patient voice areas they are going to add to their mandatory KPI suite from the below options:
Premium Access Service Specification
Is the CCG going to complete the full access service specification? If answer is Yes ‐ move to question 3, If answer is no, but the
CCG is going to choose some areas from the service specification , complete rows 32‐34 with Yes/No answers. Additional
comments can be added as required.
London Standard KPIs
Yes
Patient Voice
Vaccinations and Immunisations
Premium Access Service Specification ‐ Service areas :
Technology to improve access
CCG to confirm if they will include the optional KPI on capacity and access:
If the CCG is not planning to offer any of the service specification, please given comment on rationale for this :
Opening for Core PMS hours ‐ Including weekend additional access
64

4 Engagement
5 Impact assessments on practice stability following PMS contract changes
6 Transition
7 Equalisation
8 Costs and Investment planning
9 Wider Commissioning Intentions
10 Other Information
Has the CCG got any other information/documents to support these PMS commissioning intentions?
NHS Lambeth CCG Commissioning Intentions 2016‐17 summary presentation is available upon request.
NHS Lambeth CCG Commissioning Intentions report 2016/17 is available upon request
The CCG is implementing the PMS review at the same time as it is reviewing its investment in the GP Delivery Scheme and the Extended Access Hubs.
The CCG is funding £1.9m for GP Delivery Schemes across a range of commissioned services and these initiatives are being considered in parallel with the PMS work to develop local KPIs through the PMS
review. The CCG has set aside non recurrent funds of approximately £700k in 2016/17 to meet the costs of Holistic Health Care Assessments, previously funded by Guys Charity through Southwark and
Lambeth Integrated Care (SLIC), whilst this service is still being evaluated.
The CCG has a recurrent budget of £1.5m for Extended Access services, to which (subject to final consultation) it is intended to add a further £0.5m to deliver a sustainable model including Saturday
mornings, during 16/17. During 16/17 the existing walk in service will be reviewed and subject to options appraisal, resources will be sprea d across the Extended Access services to further ensure stability
and ensure delivery of SCF Access specification.
NOT APPLICABLE
Care and Accessible care and are developed through our local care programmes. PMS KPIs/specifications will be reviewed and revised annually. PMS premium will continue to be fully invested in general
practice services and any underspend from underachievement of KPIs will be retained locally for reinvestment and recovery.
We are proposing that the disposition of the CCG premium will be as follows:
* Accessible Care ‐ 15%
To include utilisation of best practice clinical pathways (DXS), working with PPG's and vulnerable groups through effective use of extended access services Hub capacity.
* Proactive Care ‐ 30%
To include breast and bowel screening and focus on local public health priorities including for children and mental health service areas.
* Coordinated Care ‐ 30%
To include long term conditions management for Diabetes, Stroke, CHD, & Hypertension.
* Whole system integration ‐ 25%
To support whole system CQUIN and commitment to integration at Local Care Network (LCN) level. focus on 3 or more LTCs/Elderly Frail/mental Health.
The CCG has also traditionally commissioned measurable outcomes via a Local Incentive Scheme (GPDF). KPI's associated with this scheme are being revised and finalised through one process alongside
PMS KPI's and will continue to be contracted separately. It is this alignment that will enable us to commission London Standard, Premium Access and local KPI's coherently to achieve key strategic
outcomes.
* At a higher level financial assessments indicate that practices have the opportunity to receive income to the same levels as at present.
* At a practice level individual impact studies will be completed as NHSE premium costings are finalised, local KPI's are concluded and costed and draft offers are prepared. Main issue will be in respect of
% premium associated with KPI performance assumptions.
* LMC at London meeting and individually with chair
* GP members via 3 locally specific meeting
* Wider stakeholders, including Healthwatch and PPG through Primary Care Programme meetings
* Collective membership at All Practice Event
* NHS England
* CCG Governing Body
* PMS 'Task and Finish Group'; including LMC and GP Federation membership
Please give details as to what engagement has taken place with practices, patients or other third party services to complete your PMS commissioning intentions :
Has the CCG completed any impact studies on services that potentially will need to cease in practices, or if funding will cease that currently may financially support clinicians in practices and to ensure
that practice stability can be maintained throughout the transition? Please give details :
Equalisation to GMS in 2016/17 should be delivered where strategically and financially possible. In cases where this is not possible, CCG areas will be required to set out their plans for equalisation in
their commissioning intentions submission in February and show strategic plans for achieving it as part of Sustainability and Transformation plans submitted in June 2016. Plans will need to show
equalisation before 2021 to ensure equalisation is achieved in the planning period. Note that as a minimum, where CCGs have not achieved funding equalisation within PMS practices this will need to
be achieved by 2016/17.
CCG to give explanation of how they will seek to achieve equalisation within the prescribed timeframe. This should include a timescale for implementation, any risks and additional costs involved.
How do the PMS Commissioning intentions described above fit in with the wider CCG commissioning intentions for the following year (2016/2017) where applicable note how this fits in with the Joint
Strategic Needs Assessment (JSNA) :
A key element relates to CCG whole system strategy for integration and the development of Local Care Networks (LCNS). 25% of the CCG premium will be associated with a whole systems incentive to
support improved management of older people/MH/3 or more LTC's by formulating admission avoidance and early discharge at a LCN level. This mirrors an arrangement agreed with localities and
Southwark CCG. The population focus of this iteration reflects the need identified in the JSNA.
NHS Lambeth CCG Commissioning Intentions 2016‐17 summary presentation is available upon request.
2 years of transition is allowable for practices in line with national guidance. Following further national clarification, it is confirmed that a longer transitional period can be considered by regional teams
with CCGs on a case by case basis as part of negotiations but this will not be considered on a CCG wide basis. All transitional periods must end by March 2020/21.
CCG to give full explanation as to how they will transition to new services they have advised they will be commissioning above. This should included as a minimum how it will be rolled out across the
CCG. Length of time it will take to be up and running, any risks or additional costs involved.
NHS Lambeth CCG has 4 GMS practices and has identified funds in the 2016/17 Operational Plan to enable transition of these practices to PMS in addition to existing funds set aside for this purpose. It is
envisaged that this work will be completed by 30 June 2016. For NHS Lambeth CCG's 6 APMS practices we will be consulting with individual practices to incorporate KPIs into existing contractual
arrangements. This process will be undertaken during 2016/17.
CCG to give full details of any costs and investment plans they have for the following 2 years, including any impacts this will have on service delivery of the commissioning intentions noted above or any
new incentives they may wish to deliver.
65

Co-commissioning of Primary Care South East London’s CCGs and NHS England Primary Care Joint Committees
Primary Care Joint Committees (PCJC) Meetings
DATE OF MEETING: 11 February 2016
ENCLOSURE: J
Title: PMS Commissioning Intentions – Lewisham CCG
AUTHOR: Diana Braithwaite, Director of Commissioning & Primary Care
SUMMARY: The Lewisham Primary Care Programme Board met on 27.01.2016 and agreed to recommend approval of the CCGs Commissioning Intentions for the PMS Review to the Primary Care Joint Committee. The PMS review provides a local opportunity to commence tacking variation in quality and improving appropriate access to GP services, which often results in differential outcomes for our population.
KEY ISSUES: • Delivering the London Strategic Framework: The CCGs commissioning intentions for
the PMS review supports delivery of the Transforming Primary Care in London: StrategicCommissioning Framework.
• London PMS Key Performance Indicators: The CCGs commissioning intentionsreflects the 8 mandatory NHS England PMS KPIs to support standardisation of PMScontracts across London. The CCG is committed to improving patient experience of localservices and has selected two patient voice indicators based on the GP Patient Survey(January 2016), which is supported by our analysis on reducing inequalities for thoseseeking support with managing their long-term condition.
• London PMS Premium Specifications: The CCG intends to commission the ImprovingAccess through the Use of Technology – specifically; (i) making appointments on line; (ii)electronic consultations; and (iii) ensuring patient information is accurate and complete onNHS Choices. This supports our local work on increasing on-line access to enable freeingup capacity for those of our population who need to access their GPs service via thetelephone. The CCG does not intend to commission the Weekend Additional Capacity(WAC) as part of the London PMS Premium. In Lewisham patients are able to accessunscheduled care from a GP through the local Walk-in centre, which is open 7 days perweek 08:00 to 20:00. GP services are also accessible via the Urgent Care Centre, whichhas dedicated local GPs and is also available 7 days per week 08:00 to 20:00. In order todeliver on the Strategic Framework for ACCESS (A3 – Routine Hours Saturday Opening)and provide bookable appointments – in the interim the CCG intends to commission theadditional access from the existing provider from July 2016. In the longer term appropriate
66
Annex 8

additional access will be commissioned through the development of the CCG Integrated Primary & Urgent Care Service, scheduled for 2017/18.
• Local PMS Premium: The CCG Primary Care Programme Board recommendedapproval of the commissioning priorities for the local PMS premium to the Primary CareJoint Committee on 27.01.2016, subject to detailed specifications and KPIs beingfinalised by 16.02.2016. The current PMS premium will be reinvested in general practiceand the funding available to support the premium is £3.359m. The proposals for the localPMS premium are reflective of the CCGs Primary Care Development Strategy and theLewisham Health & Wellbeing Strategy; Accessible, Coordinated and Proactive Care.Supporting sustained primary care models as a part of our Neighbourhood CareNetworks. The commissioning intentions for the PMS premium reflect the shift to outcomebased KPIs. In addition, to commence reducing variation amongst individual practicesthat results in differential outcomes from our population.
• The methodology reflecting KPIs will be based on NHSE banding approach tothresholds/levels of achievement – adjusted to reflect local requirements. Appendix 1provides details of the weighting/ppwp allocated to the KPIs and specifications.
• GMS & APMS: Our local approach is to provide an equivalent offer to GMS (4 inLewisham) and APMS (1 in Lewisham) practices.
• Local Medical Committee: Pre-engagement has taken place with the Chair of the LMC.
RECOMMENDATIONS:
The Lewisham Primary Care Joint is recommended by the Lewisham Primary Care Programme Board to approve the PMS Commissioning Intentions for Lewisham Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Lewisham Local Medical Committee, according to the timetable outlined.
CCG CONTACT: Name: Diana Braithwaite E-Mail: [email protected]
AUTHOR CONTACT: Name: Diana Braithwaite E-Mail: [email protected]
67

CCG Name LEWISHAM
London Offer
1 London Standard Key Performance Indicators (KPIs)
Is CCG going to offer? Additional Comments
Childhood Immunisation ‐ 5‐in‐1 Vaccine by 1 Year
Childhood Immunisation ‐ aged 5 years and over.
Flu Immunisation 65+
Flu Immunisation Under 65 at risk
Pneumococcal Immunisation 65+
Capacity & Access Measures
Average Attendance at local unscheduled care facilities (including WIC, UCC and A&E) for
non‐admitted patients during Core PMS hoursNo The CCG will review and consider for
2017/18.
Overall Experience
Percentage of patients responding within the 'good' range to the question "Overall, how
would you recommend your experience of your GP Surgery?"
No Lewisham (82%) is above the London
average (80%) as per the GPS January
2016. Therefore, this indicator was not
selected because the primary driver for
recommending your overall experience
is predominantly about whether you can
get an appointment at time that is
convenient for you.
Telephone
Percentage of patients responding within the 'easy' range to the question "Generally, how
easy is it to get through to someone at your GP Surgery on the phone?"
No
For 'ease of getting through to someone
over the phone’ GPS indicator for
Lewisham is below both the London and
England average and the trend is
downwards. It is our intention to
commission the London Premium
Service Specification ‐ Improving access
through the use of technology (including
on‐line booking). The GPS indicator for
on‐line booking in Lewisham has risen
and there has been a decrease in those
booking appointments by phone.
Consequently, there is a correlation
between increasing on‐line booking and
thereby freeing up capacity for over the
phone bookings for those who do not
have access to the internet. Lewisham
intends to adopt a more targeted
approach for individual practices.
Convenience of appointment
Percentage of patients responding within the 'convenient' range to the question "How
convenient was the appointment you
were able to get?"
No Lewisham performance is the same as
the London average (89%) as per the
GPS January 2016. Therefore, this
indicator was not selected as primary
driver for recommending your overall
experience is predominantly about
whether you can get an appointment at
time that is convenient for you.
Experience of making an appointment
Percentage of patients responding within the 'good' range to the question; 'Overall, how
would you describe your experience of making an appointment?'
Yes
Focussing on this indicator should drive
up performance of the other related
'access' indicators e.g. ease of getting
through, awareness etc. The trend for
this indicator is downward for
Lewisham and we remain below the
England average. For the January 2016
National GP Survey Lewisham was at
69%, London 69% and the England
average 74%.
Recommendation
Percentage of patients who would definitely or probably recommend their GP Surgery
No Analysis of this indicator is not
contained in the standard CCG GPS pack
produced by Ipsos MORI. In addition,
practices are required to provide Friends
& Family Tests (FFT) on a monthly basis
and therefore reviewing and proactively
addressing any issues in real time.
The CCG will offer all components of the
mandatory KPIs
Patient Voice
Cervical screening
PMS Commissioning Intentions
CCG to confirm that they are going to complete the full Mandatory KPI suite?
CCG to confirm which two patient voice areas they are going to add to their mandatory KPI suite from the below options:
London Standard KPIs
Screening
YesVaccinations and Immunisations
68
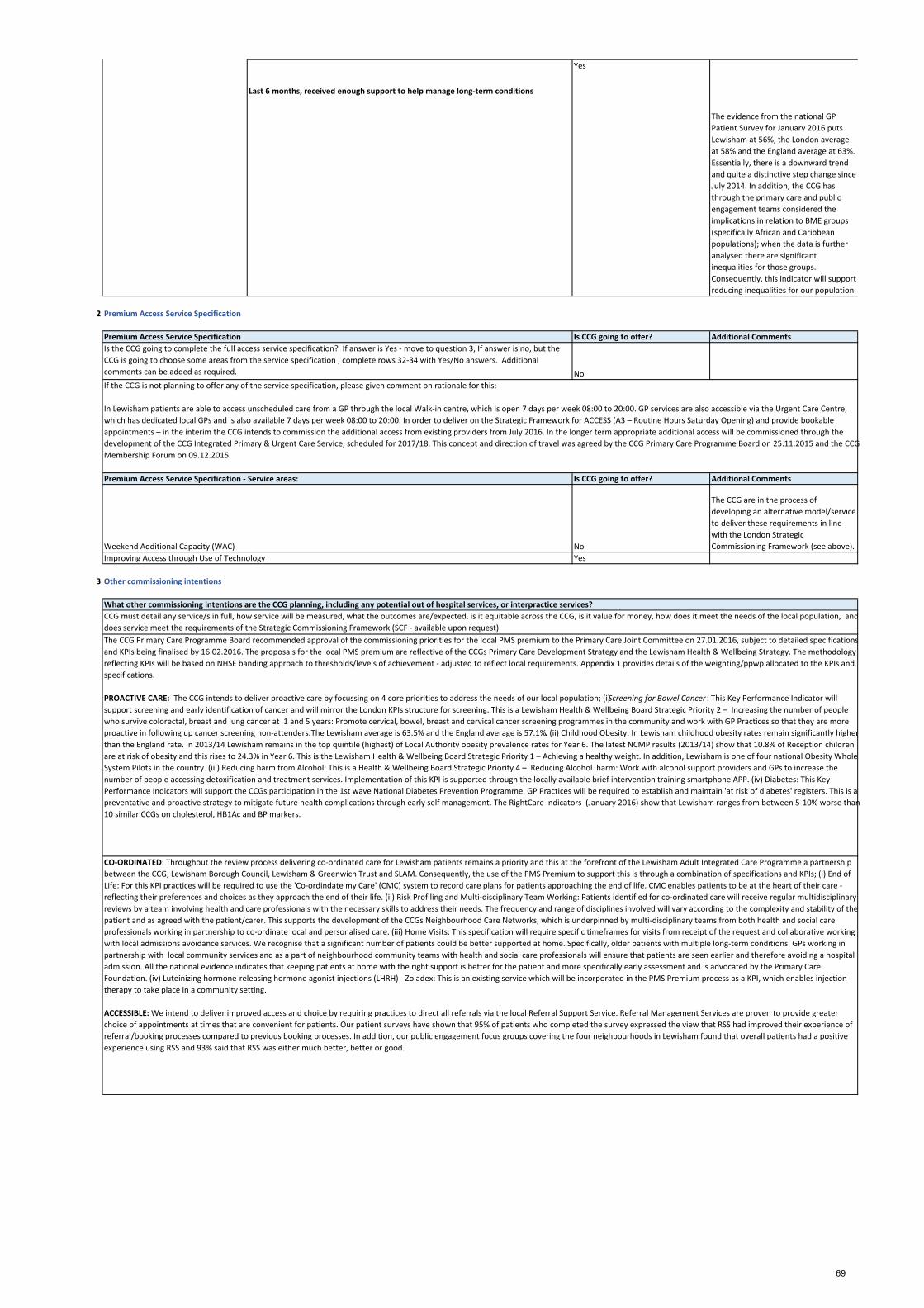
Last 6 months, received enough support to help manage long‐term conditions
Yes
The evidence from the national GP
Patient Survey for January 2016 puts
Lewisham at 56%, the London average
at 58% and the England average at 63%.
Essentially, there is a downward trend
and quite a distinctive step change since
July 2014. In addition, the CCG has
through the primary care and public
engagement teams considered the
implications in relation to BME groups
(specifically African and Caribbean
populations); when the data is further
analysed there are significant
inequalities for those groups.
Consequently, this indicator will support
reducing inequalities for our population.
2 Premium Access Service Specification
Is CCG going to offer? Additional Comments
No
Is CCG going to offer? Additional Comments
No
The CCG are in the process of
developing an alternative model/service
to deliver these requirements in line
with the London Strategic
Commissioning Framework (see above).
Yes
3 Other commissioning intentions
What other commissioning intentions are the CCG planning, including any potential out of hospital services, or interpractice services?
CCG must detail any service/s in full, how service will be measured, what the outcomes are/expected, is it equitable across the CCG, is it value for money, how does it meet the needs of the local population, and
does service meet the requirements of the Strategic Commissioning Framework (SCF ‐ available upon request)
The CCG Primary Care Programme Board recommended approval of the commissioning priorities for the local PMS premium to the Primary Care Joint Committee on 27.01.2016, subject to detailed specifications
and KPIs being finalised by 16.02.2016. The proposals for the local PMS premium are reflective of the CCGs Primary Care Development Strategy and the Lewisham Health & Wellbeing Strategy. The methodology
reflecting KPIs will be based on NHSE banding approach to thresholds/levels of achievement ‐ adjusted to reflect local requirements. Appendix 1 provides details of the weighting/ppwp allocated to the KPIs and
specifications.
PROACTIVE CARE: The CCG intends to deliver proactive care by focussing on 4 core priorities to address the needs of our local population; (i) Screening for Bowel Cancer : This Key Performance Indicator will
support screening and early identification of cancer and will mirror the London KPIs structure for screening. This is a Lewisham Health & Wellbeing Board Strategic Priority 2 – Increasing the number of people
who survive colorectal, breast and lung cancer at 1 and 5 years: Promote cervical, bowel, breast and cervical cancer screening programmes in the community and work with GP Practices so that they are more
proactive in following up cancer screening non‐attenders. The Lewisham average is 63.5% and the England average is 57.1%. (ii) Childhood Obesity: In Lewisham childhood obesity rates remain significantly higher
than the England rate. In 2013/14 Lewisham remains in the top quintile (highest) of Local Authority obesity prevalence rates for Year 6. The latest NCMP results (2013/14) show that 10.8% of Reception children
are at risk of obesity and this rises to 24.3% in Year 6. This is the Lewisham Health & Wellbeing Board Strategic Priority 1 – Achieving a healthy weight. In addition, Lewisham is one of four national Obesity Whole
System Pilots in the country. (iii) Reducing harm from Alcohol: This is a Health & Wellbeing Board Strategic Priority 4 – Reducing Alcohol harm: Work with alcohol support providers and GPs to increase the
number of people accessing detoxification and treatment services. Implementation of this KPI is supported through the locally available brief intervention training smartphone APP. (iv) Diabetes: This Key
Performance Indicators will support the CCGs participation in the 1st wave National Diabetes Prevention Programme. GP Practices will be required to establish and maintain 'at risk of diabetes' registers. This is a
preventative and proactive strategy to mitigate future health complications through early self management. The RightCare Indicators (January 2016) show that Lewisham ranges from between 5‐10% worse than
10 similar CCGs on cholesterol, HB1Ac and BP markers.
Premium Access Service Specification ‐ Service areas:
Improving Access through Use of Technology
CO‐ORDINATED: Throughout the review process delivering co‐ordinated care for Lewisham patients remains a priority and this at the forefront of the Lewisham Adult Integrated Care Programme a partnership
between the CCG, Lewisham Borough Council, Lewisham & Greenwich Trust and SLAM. Consequently, the use of the PMS Premium to support this is through a combination of specifications and KPIs; (i) End of
Life: For this KPI practices will be required to use the 'Co‐ordindate my Care' (CMC) system to record care plans for patients approaching the end of life. CMC enables patients to be at the heart of their care ‐
reflecting their preferences and choices as they approach the end of their life. (ii) Risk Profiling and Multi‐disciplinary Team Working: Patients identified for co‐ordinated care will receive regular multidisciplinary
reviews by a team involving health and care professionals with the necessary skills to address their needs. The frequency and range of disciplines involved will vary according to the complexity and stability of the
patient and as agreed with the patient/carer. This supports the development of the CCGs Neighbourhood Care Networks, which is underpinned by multi‐disciplinary teams from both health and social care
professionals working in partnership to co‐ordinate local and personalised care. (iii) Home Visits: This specification will require specific timeframes for visits from receipt of the request and collaborative working
with local admissions avoidance services. We recognise that a significant number of patients could be better supported at home. Specifically, older patients with multiple long‐term conditions. GPs working in
partnership with local community services and as a part of neighbourhood community teams with health and social care professionals will ensure that patients are seen earlier and therefore avoiding a hospital
admission. All the national evidence indicates that keeping patients at home with the right support is better for the patient and more specifically early assessment and is advocated by the Primary Care
Foundation. (iv) Luteinizing hormone‐releasing hormone agonist injections (LHRH) ‐ Zoladex: This is an existing service which will be incorporated in the PMS Premium process as a KPI, which enables injection
therapy to take place in a community setting.
ACCESSIBLE: We intend to deliver improved access and choice by requiring practices to direct all referrals via the local Referral Support Service. Referral Management Services are proven to provide greater
choice of appointments at times that are convenient for patients. Our patient surveys have shown that 95% of patients who completed the survey expressed the view that RSS had improved their experience of
referral/booking processes compared to previous booking processes. In addition, our public engagement focus groups covering the four neighbourhoods in Lewisham found that overall patients had a positive
experience using RSS and 93% said that RSS was either much better, better or good.
Premium Access Service Specification
Is the CCG going to complete the full access service specification? If answer is Yes ‐ move to question 3, If answer is no, but the
CCG is going to choose some areas from the service specification , complete rows 32‐34 with Yes/No answers. Additional
comments can be added as required.
If the CCG is not planning to offer any of the service specification, please given comment on rationale for this:
In Lewisham patients are able to access unscheduled care from a GP through the local Walk‐in centre, which is open 7 days per week 08:00 to 20:00. GP services are also accessible via the Urgent Care Centre,
which has dedicated local GPs and is also available 7 days per week 08:00 to 20:00. In order to deliver on the Strategic Framework for ACCESS (A3 – Routine Hours Saturday Opening) and provide bookable
appointments – in the interim the CCG intends to commission the additional access from existing providers from July 2016. In the longer term appropriate additional access will be commissioned through the
development of the CCG Integrated Primary & Urgent Care Service, scheduled for 2017/18. This concept and direction of travel was agreed by the CCG Primary Care Programme Board on 25.11.2015 and the CCG
Membership Forum on 09.12.2015.
Weekend Additional Capacity (WAC)
69

4 Engagement
5 Impact assessments on practice stability following PMS contract changes
6 Transition
7 Equalisation
8 Costs and Investment planning
9 Wider Commissioning Intentions
10 Other Information
Working together for better health, better care, and stronger communities‐ CCG & Lewisham Borough Council Joint Commissioning Intentions: http://www.lewishamccg.nhs.uk/get‐
involved/Commissioning%20intentions%20documents/Summary%20commissioning%20Intentions%20summary.pdf#search=joint%20commissioning%20intentions
Primary Care Development Strategy: http://www.lewishamccg.nhs.uk/about‐us/Who‐we‐are/Governing%20Body%20papers/November%202014%20Governing%20Body%20papers.pdf
Joint Strategic Needs Assessment: http://www.lewishamjsna.org.uk/
Right Care ‐ Commissioning for Value (Lewisham) January 2016: https://www.england.nhs.uk/wp‐content/uploads/2016/01/lewisham‐ccg‐16.pdf
Improving Access – A3: Saturdays routine and A4: Extended access (Estimated) ‐ our plans for addressing both these components in both 2016/17 and 2017/18 have been provided earlier on in the document and
this will be supported additional funding from the CCG. It is our intention to incorporate the Luteinzing hormone‐releasing hormone agonist injections (LHRH): Zoladex Service currently provided by practices in
the PMS premium to support consolidation of contracting processes. This service will to support GP practices proving injection therapy in the community.
Not applicable.
Our assessment is that the approach to the PMS Review will not have any significant negative impact on the financial and operational stability of practices.
The CCG intends to deliver patient and public engagement via its recently formed Public Reference Group and the four Neighbourhood level Patient Participant Groups. Recognising that a great deal of
patient/public engagement has taken place via the OHSEL deliberative events programme on what our population thought was important for primary care.
PMS Working Group (21.10.2015): Review.
Joint NHSE & CCG – PMS Workshop (28.10.2015): Development of Commissioner Priorities.
SEL Primary Care Joint Committee – Workshop (28.10.2015): Review of Commissioner Priorities
Primary Care Programme Board (25.11.2015): Endorse Commissioning Intentions & Priorities for Primary Care.
Primary Care Joint Committee (10.12.2015): Review Commissioner Priorities.
Membership Forum (09.12.2015): Assurance that Commissioner Priorities reflects the CCG Primary Care Development Strategy.
Local LMC (04.11.2015, 20.01.2016 & 04.02.2016): Pre‐engagement on Commissioning Intentions & Priorities.
NHS England: On‐going.
Director of Public Health, LBL (18.10.2016): Health & Wellbeing Board priorities for Primary Care.
Please give details as to what engagement has taken place with practices, patients or other third party services to complete your PMS commissioning intentions:
Has the CCG completed any impact studies on services that potentially will need to cease in practices, or if funding will cease that currently may financially support clinicians in practices and to ensure that
practice stability can be maintained throughout the transition? Please give details :
CCG to give full details of any costs and investment plans they have for the following 2 years, including any impacts this will have on service delivery of the commissioning intentions noted above or any
new incentives they may wish to deliver.
Has the CCG got any other information/documents to support these PMS commissioning intentions?
How do the PMS Commissioning intentions described above fit in with the wider CCG commissioning intentions for the following year (2016/2017) where applicable note how this fits in with the Joint
Strategic Needs Assessment (JSNA) :
Lewisham’s Health and Wellbeing Board has identified nine priority outcomes that form the basis of our 10 year Health & Wellbeing Strategy, which were refreshed in 2015. These nine priorities are based on
JSNA evidence and those which will be reflected and delivery will be supported via the PMS Premium are articulated below;
1. Increase the uptake of immunisations: Uptake of immunisation has been a problem in Lewisham for some time. Uptake of vaccines has been below target, and as a result, significant numbers of children in
Lewisham are not protected against potentially serious infections. Due to the low uptake of MMR vaccine, there was an outbreak of measles in Lewisham in 2008 with a total of 275 confirmed or suspected cases.
Action over recent years has resulted in considerable improvement in uptake but significant challenges remain.
3. Reduce the harm caused by alcohol misuse:
4. Promote Healthy Weight
5. Improving Mental Health & Wellbeing: Prevalence of mental illness is high in Lewisham. Factors such deprivation, a diverse population and being an inner city location all contribute to the high levels of poor
mental health. Severe Mental illness (SMI) describes a range of disorders characterised by psychosis where individuals become apparently detached from reality. These include schizophrenia and bipolar disorder.
About half of these are managed in primary care, with additional support for the remainder available via acute community and in‐patient services. Around 1.1% of the population registered with GPs has a severe
mental illness.
8. Reduce the number of emergency admissions for people with chronic long term conditions: Proactive primary care can support reducing avoidable unplanned admissions amongst patients with complex care
needs.
2 years of transition is allowable for practices in line with national guidance. Following further national clarification, it is confirmed that a longer transitional period can be considered by regional teams with
CCGs on a case by case basis as part of negotiations but this will not be considered on a CCG wide basis. All transitional periods must end by March 2020/21.
CCG to give full explanation as to how they will transition to new services they have advised they will be commissioning above. This should included as a minimum how it will be rolled out across the CCG.
Length of time it will take to be up and running, any risks or additional costs involved.
GMS Equalisation: Lewisham has four GMS and one APMS practices. The CCG has committed to funding in addition to the PMS premium funding for equalisation to GMS/APMS practices from the
commencement of the contract (Jul). PMS Equalisation: The majority of Lewisham practices are PMS. The CCG has committed to equalisation across all PMS practices and expects this to be within the allocated
PMS premium.
Equalisation to GMS in 2016/17 should be delivered where strategically and financially possible. In cases where this is not possible, CCG areas will be required to set out their plans for equalisation in their
commissioning intentions submission in February and show strategic plans for achieving it as part of Sustainability and Transformation plans submitted in June 2016. Plans will need to show equalisation
before 2021 to ensure equalisation is achieved in the planning period. Note that as a minimum, where CCGs have not achieved funding equalisation within PMS practices this will need to be achieved by
2016/17.
CCG to give explanation of how they will seek to achieve equalisation within the prescribed timeframe. This should include a timescale for implementation, any risks and additional costs involved.
70

Lewisham CCG: Summary of the Proposed Commissioning Intentions for the Local PMS Premium - £3.359m
ACCESSIBLE CARE KPI or specification
Proposal Costing (price per weighted patient) of PMS Premium
Costing (%) of PMS Premium
A1. Referral Management KPI Percentage of referrals through local Referral Management processes £1.00 8% PROACTIVE CARE KPI or
specification Proposal Costing (price per
weighted patient) of PMS Premium
Costing (%) of PMS Premium
P1. Childhood Obesity KPI Percentage patients aged 16 or younger with an accurate BMI record; of those recorded as overweight/obese assessed in the preceding 15 months given a brief intervention and/or signposted to local lifestyle interventions.
£2.20 P2. Bowel Cancer Screening KPI Percentage of patients in relevant age cohort during reporting period registered
with the practices that have responded to invitation for screening. 18% P3. Alcohol KPI Practices to identify a percentage of registered patients who are currently
consuming alcohol at higher risk levels using Fast or AUDIT C and deliver brief intervention.
P4. Diabetes Specification At risk of diabetes registers to be established and maintained within practices.
CO-ORDINATED CARE KPI or specification
Proposal Costing (price per weighted patient) of PMS Premium
Costing (%) of PMS Premium
C1. End of Life KPI Use of Coordinate my Care to record care plans for patients at End of Life
£4.90
C2. Risk Profiling and Multidisciplinary Working
Specification Patients identified for coordinated care will receive regular multidisciplinary reviews by a team involving health and care professionals with the necessary skills to address their needs. The frequency and range of disciplines involved will vary according to the complexity and stability of the patient and as agreed with the patient/carer.
41%
C3. Luteinizing hormone-releasing hormone agonist injections (LHRH): Zoladex
Specification Provision of injection therapy in the community.
C4. Home Visits Specification Practices to identify the need for home visits within a specified time frame in relation to the request and action accordingly.
71

NHSE PMS Mandatory KPIs & London PMS Premium Service Specification
KPI or specification
Proposal Costing (price per weighted patient) of PMS Premium
Costing (%) of PMS Premium
NHSE PMS Mandatory KPIs KPI Screening, Immunisations, Vaccinations, Patient Experience £3.04 25%
London PMS Premium Service Specification – Improving access through the use of technology
Specification (a) Practices to make available at least 50% of all appointments available online by 1 April 2017; (b) Practices to offer electronic consultations; (c) Practices to ensure that its pages on NHS Choices are updated regularly, and provide complete and accurate information regarding the practice at all times.
£1.00 8%
Totals £12.14 100%
72

Co-commissioning of Primary Care South East London’s CCGs and NHS England Primary Care Joint Committees
Primary Care Joint Committees (PCJC) Meetings
DATE OF MEETING: 11 February 2016
ENCLOSURE: J
Title: PMS Commissioning Intentions: NHS Southwark Clinical Committee Group
AUTHOR: Caroline Gilmartin, Director of Integrated Commissioning, NHS Southwark Clinical Commissioning Group
SUMMARY:
Assessment of local position following the confirmation of the final London offer between NHS England and London LMCs: Southwark CCG (CCG) has considered the outcome of the formal consultation with NHSE and London-wide LMC. As a result of this the CCG will be delivering the whole of the London offer and has elected to consider a KPI for breast screening as part of its local offer – subject to further work to understand the implications and impact for our population. Two of the possible five patient voice indicators have been selected. As Southwark has invested in access hubs to increase the number of GP appointments available in the area, there is only one key indicator from the access specification, relating to improved technology to support better access that has been selected.
Summary of how the remaining funds/premium will be spent: In the attached paper the key areas for developing KPI’s have been set out. These are subject to formal consultation with Southwark LMC. The proposal is that all remaining premium (indicative funding of £15.80) will be deployed to performance areas that have been clinical agreed, address public health issues and are areas of care that general practice can influence performance and uptake of services.
Any under performance of the current PMS premium will be reinvested in general practice.
KEY ISSUES:
London Transformation programme: The CCG has addressed all the key areas that the LTP has raised, except those where to do so would cause us to be paying twice for a service, e.g. Access to weekend appointments in GP practices.
73
Annex 9

Through mapping of current PMS KPI proposals and the transformation agenda, we are assured that the commissioning intentions do cover the wider strategic commissioning framework for London.
Impact on GMS and APMS practices: The CCG has agreed to invest in GMS and APMS practices (where required) to ensure that they can also delver the full premium offer to their patients
Summary of any additional local issues: None noted
RECOMMENDATIONS:
The Southwark Primary Care Joint Committee is requested to approve the PMS Commissioning Intentions for Southwark Clinical Commissioning Group subject to completion of specifications, KPIs & associated prices; and formal consultation with Southwark Local Medical Committee, according to the timetable outlined.
CCG CONTACT: Name: Caroline Gilmartin E-Mail: [email protected]
AUTHOR CONTACT: Name: Caroline Gilmartin E-Mail: [email protected]
74

CCG Name NHS Southwark CCG
London Offer
1 London Standard Key Performance Indicators (KPIs)
Is CCG going to offer? Additional Comments
Screening Cervical screeningChildhood Immunisation - 5-in-1 Vaccine by 1 YearChildhood Immunisation - aged 5 years and over. Flu Immunisation 65+Flu Immunisation Under 65 at riskPneumococcal Immunisation 65+
Overall ExperiencePercentage of patients responding within the 'good' range to the question "Overall, how
would you recommend your experience of your GP Surgery?"
Yes The CCG held a practice and patient engagement event on 3 February 2016. One of the event aims was to engage on the ‘Patient Voice’ KPIs proposed to ensure our patients had an opportunity to input into which KPIs they felt were most important to them. The outcome of that event is Overall Experience and Experience of making an appointment KPIs have been prioritised by local patients and the CCG therefore proposes these indicators having conducted a process of local engagement.
The CCG recognises the difficultly of conducting full public consultation with the limited time and changes being made to the contract. The CCG has sought service user engagement within this limited timeframe and also utilised the full public and patient engagement we conducted locally last year. We have also considered the recent GP Access Survey Results. The CCG average achievement of questions was that 79% of patients said that their overall experience of their GP practice was either ‘very good’ or ‘fairly good’ against a national average of 85%. Results ranged at a practice level from 50% - 94%.
The CCG proposes to include this indicator in the PMS premium to incentivise practices to focus on the GP Patient Survey results to identify potential improvements to address patient experience.
This has been agreed by NHS Southwark CCG’s Commissioning Strategy Committee and ratified by our Conflict of Interest Panel.
TelephonePercentage of patients responding within the 'easy' range to the question "Generally, how
easy is it to get through to someone at your GP Surgery on the phone?"
No n/a
Convenience of appointmentPercentage of patients responding within the 'convenient' range to the question "How
convenient was the appointment youwere able to get?"
No n/a
Experience of making an appointmentPercentage of patients responding within the 'good' range to the question "Overall, how
would you describe yourexperience of making an appointment?"
Yes The CCG average achievement of questions was that 67% of patients said their experience of making an appointment was either ‘very good’ or ‘fairly good’ against a national average of 73%. (January 2016 results)Results ranged at a practice level from 39% - 90%. The CCG would like for this indicator to be included within the PMS premium as it relates to the extended primary care services that have been commissioned to increased hours that patients can obtain a GP / nurse appointment.
It is therefore recognised that access is a priority area of improvement for the CCG. GP Patient survey results have slightly decreased in the last year despite commissioning the extended primary care services and incentivising practices to agree a neighbourhood Access Policy.
Patients’ experience of making an appointment should be improved by the extended primary care services that have been commissioned 8am – 8pm, 7 days per week and therefore by focusing practices attention on this indicator it also may encourage utilisation of the extended primary care service when appropriate.
The CCG proposition is to include this indicator within the PMS premium to incentivise practices to review their access systems and to deliver a reduction in variation between practice results.
This has been agreed by NHS Southwark CCG’s Commissioning Strategy Committee and ratified by our Conflict of Interest Panel.
RecommendationPercentage of patients who would definitely or probably recommend their GP Surgery
No n/a
2 Premium Access Service Specification
Is CCG going to offer? Additional CommentsCapacity & Access Measures Average Attendance at local unscheduled care facilities (including WIC, UCC and A&E) for
non-admitted patients during Core PMS hoursNo
The NHS Southwark CCG is proposing not to incentivise this access measure as part of the PMS premium. NHS Southwark CCG does not commission a Walk in Centre (WIC).
The NHS Southwark CCG has monitored A&E minors and UCC attendances for a number of years and discusses the outcome of this with local practices using our local dashboard, quality assurance and improvement process. A great deal of focused work has taken place to reduce the impact of A&E attendances on an individual practice level.
The NHS Southwark CCG has commissioned an Extended Primary Care Service (EPCS) to provide additional GP appointments for our local population to improve both access and continuity of care. We are therefore closely monitoring these indicators as part of the EPCS delivery model delivered by our Federations on behalf of member practices, which includes individual practice action plans where appropriate.
A full EPCS evaluation including impact on the system will take place in November 2016. The CCG will specifically want to understand the impact of the additional access on our interdependent services. As the CCG is funding the EPCS locally, to incentivise these indicators on an individual practice level would be risk counteracting the collective working and performance which has been taking place in Southwark to increase access to our population.
No See below.
Is CCG going to offer? Additional CommentsNo The CCG commissions 2 extended primary care services in the borough which the whole registered population
of Southwark access to primary care services 8am – 8pm 7 days per week.The services have been commissioned to ensure this access is equitable for all patients registered with Southwark practices. The extended primary care services provide an additional 116,458 primary care appointments per annum (87,434 face to face appointments). This equates to 5.5 face to face appointments per 1000 patients per week.The service has been commissioned to enable the delivery of the Accessible Care Specification (A1 – A7) of the Transforming Primary Care in London: A Strategic Commissioning Framework. The CCG is working with the GP federations, as the providers, to develop the service specification further to include routine appointments for patients and to increase the utilisation of the service. Incentivising individual practices to open at the weekend would continue to facilitate the continuation of variance in terms of access for patients which does not support the CCG’s principle that services should be commissioned for a population.
Yes
3 Other commissioning intentions
What other commissioning intentions are the CCG planning, including any potential out of hospital services, or interpractice services?CCG must detail any service/s in full, how service will be measured, what the outcomes are/expected, is it equitable across the CCG, is it value for money, how does it meet the needs of the local population, and does service meet the requirements of the Strategic Commissioning Framework (SCF - available upon request)NHS Southwark CCG has an indicative average of £19.84 PMS premium per weighted registered patient. The CCG intends to include local PMS indicators in addition to the London offer. After deducting the estimated premium associated with the NHS England London offer, the CCG
As part of the annual commissioning cycle to review PMS KPIs, the CCG would wish these KPIs to be considered as the phased approach from individual practice to collective incentivisation for performance from 2017/18 onwards in line with the CCG’s Five Year Forward View plan.
They will be offered in full from 2016/17.
Premium Access Service Specification - Service areas :
Technology to improve access
PMS Commissioning Intentions - Which must be completed as a minimum for CCG Commissioning intentions return documentation.
CCG to confirm that they are going to complete the full Mandatory KPI suite?
CCG to confirm which two patient voice areas they are going to add to their mandatory KPI suite from the below options:
Premium Access Service Specification
Is the CCG going to complete the full access service specification? If answer is Yes - move to question 3, If answer is no, but the CCG is going to choose some areas from the service specification , complete rows 32-34 with Yes/No answers. Additional comments can be added as required.
If the CCG is not planning to offer any of the service specification, please given comment on rationale for this : n/a
Opening for Core PMS hours - Including Saturday AM
London Standard KPIs Yes
Patient Voice
Vaccinations and Immunisations
75

Area KPI Focus Rationale Primary Care Strategic Commissioning Framework FundingMental Illness Patients on mental health register with a long term condition given an annual physical
health check.
Advised on self-management of long term condition or signposted to support services.
To improve the physical health of patients with mental illness.
National evidence suggests that SMI patients die 15-20 years younger on average that people who do not have a mental illness mainly from preventable physical causes.
The CCG’s Clinical Effectiveness Group as considering an EMIS Web template to support the delivery.
P3: Personal conversations focused on an individual’s health goals.
C4: Patients supported to manage their health and wellbeing.
To support the primary care proactive management of patients with a long term condition with a focus on patients with mental illness.
To be based on individual achievement in 2016/2017.
Dementia Patients with dementia to have an identified carer who has been referred to the Alzheimer’s Society for carer assessment. If no carer is identified, to ensure dementia patients are linked in to local community support services
To deliver the aims of the National Dementia Strategy, PM’s Challenge and NHSE’s Transforming Dementia Care Framework to enable ‘living well with dementia’ by encouraging good quality management of dementia in the community by maintaining carer health and wellbeing.
P2: Developing assets and resources for improving health and wellbeing.
To support primary care to work with others and use resources to empower people to remain healthy; and to feel connected to others and to be supported in their local community.
To be based on individual achievement in 2016/2017.
Childhood Obesity Identify children who are overweight and obese through proactive measure e.g. when mum is in the surgery.
‘Brief intervention’ helping parents recognise they child is overweight and thinking about how they might address this as a family.
Signpost to free gym and swim for children to get more active
Refer to services that will help families become more active where they need extra help and advice.
Formalise link with schools to share data to identify patients for support. Link with the national child measurement programme for 4-5 year old and 10-11 year olds.
Currently within the current PMS contract as a self-certification standard.
28% of children aged 4 and 5 are overweight or obese significantly above the England average.
44% of 10-11 year olds in Southwark are overweight or obese, significantly higher than the England average.
P3: Personal conversations focused on an individual’s health goals.
To support the primary care proactive identification and offer of brief interventions.
To be based on individual achievement in 2016/2017.
Wound Management Primary care management of non-complex wounds in line national guidance. To support the delivery of a primary care wound management service and to facilitate equitable access for patients to a primary care nursing service
Nursing services are currently in the PMS contract as a self-certification standard.
To support equal access for patients to a non-complex wound high quality management service in primary care.
To be based on the collective performance of practices.
Hypertension Optimising blood pressure control for patients with hypertension A KPI is within the current PMS contract. This will be reviewed in line with National and Local Guidance, performance and appropriateness for primary care delivery.
C1: Case finding and review.
To support the proactive management of patients with LTCs and enable practices to identify those who may be, or are at risk of, experiencing an exacerbation of their condition but who have not reached a crisis point to seek treatment.
To be based on the collective performance of practices.
Stroke Optimising cholesterol control for patients who are at high risk of a stroke A KPI is within the current PMS contract. This will be reviewed in line with National and Local Guidance, performance and appropriateness for primary care delivery.
C1: Case finding and review.
To support the proactive management of patients with LTCs and enable practices to identify those who may be, or are at risk of, experiencing an exacerbation of their condition but who have not reached a crisis point to seek treatment.
To be based on the collective performance of practices.
Coronary Heart Disease Optimising cholesterol control for patients with Coronary Heart Disease (CHD) A KPI is within the current PMS contract. This will be reviewed in line with National and Local Guidance, performance and appropriateness for primary care delivery.
C1: Case finding and review.
To support the proactive management of patients with LTCs and enable practices to identify those who may be, or are at risk of, experiencing an exacerbation of their condition but who have not reached a crisis point to seek treatment.
To be based on the collective performance of practices.
Diabetes
Optimising cholesterol control and minimising CVD risk of patients with diabetes. A KPI is within the current PMS contract. This will be reviewed in line with National and Local Guidance, performance and appropriateness for primary care delivery.
C1: Case finding and review.
To support the proactive management of patients with LTCs and enable practices to identify those who may be, or are at risk of, experiencing an exacerbation of their condition but who have not reached a crisis point to seek treatment.
To be based on the collective performance of practices.
Breast Screening Percentage of females in relevant age cohort during reporting period registered with the practice that have defaulted and subsequently attend the breast screening service
The CCG is proposing to include this KPI within the PMS premium.
In 2014/2015 and 2015/2016 the CCG incentivised practices through the Neighbourhood Development Plan (NDP) to work in neighbourhood groups to develop a call and recall system to improve quality and to reduce unwarranted variation in outcomes. The continuation of this work will support practices in the delivery any KPI in this area.
P5: Patients not currently accessing primary care services
Primary care teams will also design approaches to follow up those patients who might be attending the practices from time to time but are not taking up invitations for services such as screeningand vaccinations.
To be based on individual achievement in 2016/2017.
The shared system wide incentive.
4 Engagement
Date / Forum Purpose2 September 2015 - Locality Patient Participation Group (South)
To present the PMS review principles and local context
25 September 2015 – All practice event To present the PMS review principles and local context
4 November 2015 - Locality Patient Participation Group (South)
To present the PMS review principles and local context
19 November 2015 - Presentation to Engagement and Patient Experience Committee
To present the PMS review principles and local context
estimates £15.80 is available for local commissioning intentions. This funding will be distributed across the KPIs and specifications outlined in the local commissioning intentions. The CCG PMS local indicators will be equitable across all practices. The CCG has completed a local action plan to deliver the 3 specifications of accessible, proactive and coordinated care from the Transforming Primary Care in London: A Strategic Commissioning Framework. The CCG aims to deliver these specifications through a combination of partnership working through our Local Care Networks, the PMS KPIs and the EPCS. This will be supported by non-recurrent investment to support Federation infrastructure and organisational development, and for co-ordinated care; a shared system wide incentive across PMS, acute and mental health contracts.
Southwark’s local PMS proposed indicators include the current PMS clinical outcome areas for patients with long term conditions (LTC). In addition to these, the CCG also proposes a number of priority areas which have been identified as priorities in our JSNA and as patient demand pressures. Some of the areas are also within the current PMS contract as a self-certification standard, which the CCG is proposing to develop in to measurable KPIs.
The CCG is proposing of the £15.80 allocated to local commissioning intentions that means ultimately 50% will be assigned to collective performance and 50% for individual performance. Collective performance will support the delivery of more equitable services to patients in Southwark. This is in line with the NHS Southwark CCG’s Primary and Community Care Strategy to reduce variation in patient outcomes and improve service value by commissioning services for our collective registered population. It also meets the national requirements for strategic alignment and reducing inequalities through the PMS premium. Where there is collective performance, an agreed percentage of that funding will be based on performance of KPIs across general practice, and the remaining will relate to performance in relation to a shared system-wide incentive to deliver care coordination as part of a Local Care Network (LCN). This system-wide incentive recognises and supports the central role practices have within the system generally and an LCN specifically. In particular, the approach delivered under this incentive will support delivery of the coordinated care elements of the Framework (C1 – C5). Practices will need to work together to determine how they deliver the collective incentivised KPIs and system wide incentive. The PMS premium funding will still be paid to individual practices in line with PMS contract requirements. NHS Southwark CCG has both GP federations and a developing Local Care Network which may be used to support collective performance delivery.
From 2016/2017, will be a step change period, which may include transition from shadow to full implementation of KPIs, over a number of months/years to support the delivery of the new and revised KPIs and the transition from individual performance to full collective performance. The CCG has engaged with our local member practices and federations on what this could look like to inform the formal consultation with the LMC when they receive full mandate from our local practices. The CCG proposes that the KPIs will be reviewed annually and that the proportion of indicators based on collective performance will increase annually. The rate of change expectation will form part of the formal consultation process with the LMC and discussion with our federations given proposed role in supporting practices deliver collective performance. This may include a number of ways to ensure that the KPIs are deliverable, including shadowing, and will be dependent on each proposed KPI where there may already be a formal service delivery structure in place through local funded initiatives i.e. collective call and recall process.Any funding lost to practices because of underperformance will be reinvested back in to general practice upon receipt of an agreed recovery plan. This funding will be aligned to clear specifications and work plans that will be linked to improving quality and reducing variation in primary care. The areas of focus for the CCG’s commissioning intention are below.
The commissioning intentions have been developed within input from CCG Clinical leads and public health colleagues to ensure that they are focused on key priority areas for Southwark. The CCG have engaged with practices and patients at the following events during the development of the commissioning intentions.
Please give details as to what engagement has taken place with practices, patients or other third party services to complete your PMS commissioning intentions :
The shared system-wide incentive is to support practices to work as part of Local Care Networks to deliver the types of care coordination described in the Transforming Primary Care: Strategic Commissioning Framework (SCF) (standards C1-to-C5).The SCF sets out five things (C1-C5) that need to happen as part of care coordination: C1 Case Finding | C2 Named Professional | C3 Care Planning | C4 Self-management | C5 MDT working
In the first six months the CCG is asking providers to take part in their LCN (and probably to work across LCNs) to agree their approach in relation to each of these requirements. This will also be supported by a dedicated piece of work across the Lambeth and Southwark Strategic Transformation Partnership (a partnership of local commissioners and providers) in relation to data analysis and information governance. This is a significant change in the way that people work across the system, but it builds upon the integrated care work in general practice and links to the additional community support that has been developed through Southwark and Lambeth Integrated Care (SLIC) to date (e.g. the Enhanced Rapid Response Service and @home models of care).
The CCG will want the different providers within an LCN to give specific emphasis to those people with high complexity, probably signalled by the number of LTCs (3+ or 5+) and other markers of need such as being in receipt of social care, having an SMI diagnosis, living alone etc… and other markers of a change i.e. increasing risk score or use of services e.g. risk of falls/frailty index).
In addition the CCG will ask providers to propose appropriate outcome measures to baseline (probably including things like emergency bed days, total outpatient appointments, admission to residential care, time spent at home, or one or more ‘I’ statements). Commissioners’ increasing focus on outcomes will mean that the detail of the case finding will be for LCN members to agree, although our phased approach intends to support this over the next 6-12 months in practice.
76
20 January 2016: presentation local commissioning intentions to Council of Members
To present the local commissioning intentions to practices in their commissioner roles to further develop and receive feedback on the specific areas to be adopted as part of the PMS premium in 2016/2017.
28 January 2016 presentation local commissioning intentions to Council of Members at Locality meetings
To recap the position and aims of the PMS review and provide further opportunity for members to comment on the clinical priority areas being proposed and to give members an opportunity to share views on the contribution general practices can make in addressing those areas.
3 February 2016 : Provider and patient event
To present the local commissioning intentions to practices, in their provider role, and patient to engage on the: • Purpose and principles of the PMS review
• KPI focus areas and their views on which KPIs should be prioritised for 2016/17
• Process for consultation and PMS KPI focus for 2017/18 and beyond.
5 Impact assessments on practice stability following PMS contract changes
6 Transition
7 Equalisation
8 Costs and Investment planning
9 Wider Commissioning Intentions
10 Other Information
The CCG has supported practice and Federation development to date through non-recurrent funding via the Neighbourhood Development Plan Incentive Scheme and investment in Federation business plans for 2016/17. Going forward, the CCG will align transformation funding (via Federation business plans) to enable Federations to develop their collective infrastructure to be best placed to support practices to deliver existing GP Federation contracts, work with LCN partners to deliver shared priorities such as the system wide incentive, and where agreed with practices -collective delivery/ways of working to support achievement of PMS KPIs. The CCG commissions 2 local contracts through the 2 federations (covering the north and south of the borough), EPCS and Population Health Management Contract. These are a combined annual cost of £3.9m. The EPCS has will be fully reviewed in November 2016 to identify if this is fully delivering the Accessible Care Specification (A1 – A7) of the Transforming Primary Care in London: A Strategic Commissioning Framework.
Practices in Southwark had the value of their PMS Contract equalised in a PMS review in 2012/2013 following a previous PMS contract review. It is not proposed that practices will need transition support in line with national guidance. The CCG will ensure that pace of change is stepped to ensure delivery in 2016/2017 and not to destabilise general practice.
Practices in Southwark had the value of their PMS Contract equalised in a PMS review in 2012/2013 following a previous PMS contract review.
The CCG’s commissioning intentions are not proposing to cease services currently provided by practices.
It is noted that there may be a risk to practices as payments for the collective KPIs and system wide incentive will be reliant on other practices / providers.
Payment incentives for KPIs based on collective achievement will be structured to mitigate this risk and we will review and agree a pace of change towards full collective incentivisation to minimise destabilisation. The CCGs intention is to move practices to a mode of delivery that increases the stability of their income, through introducing the lever to enable different models of delivery to be supported. Any underperformance against KPI’s will be reinvested back to in general practice at a collective (at this point in time this means through federations,) or other equivalent model support by practices for use to support the delivery of the PMS premium KPIs for the following year. Therefore no money will be lost to general practice primary care.
Has the CCG completed any impact studies on services that potentially will need to cease in practices, or if funding will cease that currently may financially support clinicians in practices and to ensure that practice stability can be maintained throughout the transition? Please give details :
CCG to give full details of any costs and investment plans they have for the following 2 years, including any impacts this will have on service delivery of the commissioning intentions noted above or any new incentives they may wish to deliver.
Has the CCG got any other information/documents to support these PMS commissioning intentions?
How do the PMS Commissioning intentions described above fit in with the wider CCG commissioning intentions for the following year (2016/2017) where applicable note how this fits in with the Joint Strategic Needs Assessment (JSNA) :
NHS Southwark CCG will update and consult the premium KPIs on an annual basis to ensure that they continue to be focused on the priorities for the population of Southwark. The NHS Southwark CCG will ensure that there is a phased transition to collective delivery which is demonstrable. In line with the Five Year Forward View and population based commissioning, transition from individual performance to collective, the CCG will develop the KPIs and outputs in to patient outcomes linked to the work of Local Care Network. NHS Southwark CCG will ensure the PMS premium complies with the Our Healthier South East London (OHSEL) Community Based Care.
The CCG broader commissioning intentions for primary care in 2016/2017 are:
• To fully deliver and embed extended primary care access capacity in GP practices through the EPCS significantly reducing wait for access GP services improving patient experience (accessible care). Through engagement with practices as part of the PMS review process these sites have
been identified by practices as possible enablers for delivery of the PMS indicators that will be based on collective performance, such as wound care.
• Implement the joint NHSE/CCG local primary care work plan using the PMS review and local contracts to work with individual and groups of GP practices and other community providers to deliver:
- Transforming Primary Care in London: A Strategic Commissioning Framework accessible, coordinated and proactive careThe CCG has ensured that the PMS review commissioning intentions are linked to the Proactive and Coordinated care specifications within the Strategic Commissioning Framework. The CCG is working with the GP federations, as providers of the
extended primary care services to development the services provided at the two services to increase the utilisation and to support the delivery of the Accessible Care specification.
- Quality improvement Framework Reducing variationAs part of the CCG’s quality improvement workplan, the CCG’s Primary Care Dashboard indicators will be reviewed to focus on the PMS KPIs. The dashboard will allow member practices and federations to identify, benchmark and oversee work to improve
patients outcomes that are listed within the PMS commissioning intentions.
• Align all population health management related contracts and incentives for community delivered services including transformational funding.
2 years of transition is allowable for practices in line with national guidance. Following further national clarification, it is confirmed that a longer transitional period can be considered by regional teams with CCGs on a case by case basis as part of negotiations but this will not be considered on a CCG wide basis. All transitional periods must end by March 2020/21.CCG to give full explanation as to how they will transition to new services they have advised they will be commissioning above. This should included as a minimum how it will be rolled out across the CCG. Length of time it will take to be up and running, any risks or additional costs involved.
PMS equalisation This is not a critical issue in Southwark due to the PMS Contract review undertaken in 2011 which achieved PMS premium funding equalisation across all PMS practices from 2012/2013. GMS equalisation (3 contracts)To provide an equality of funding opportunity to all GP practices in Southwark and to enable the delivery of population based services, the CCG will offer all GMS practices to ability to earn the PMS premium offer depending on affordability.APMS equalisation (6 contracts)All APMS contracts in Southwark will be renegotiated by 30 June 2017 when there is a suitable break in their contract or they expire. The CCG would ask that NHS England negotiate that APMS Contracts from 1 April 2016 include PMS premium services and standard to enable the delivery of population based services. It is recognised that finances may not be able to be negotiated until contract end dates in 31 March 2013 and 30 June 2017. There are two APMS contracts in Southwark which receive less money per patient than the current PMS contract offer. The CCG would look to offer these practices the ability to earn the PMS premium offer depending on the affordability and expect that NHS England will negotiate the new KPIs into future APMS contract negotiation.
Equalisation to GMS in 2016/17 should be delivered where strategically and financially possible. In cases where this is not possible, CCG areas will be required to set out their plans for equalisation in their commissioning intentions submission in February and show strategic plans for achieving it as part of Sustainability and Transformation plans submitted in June 2016. Plans will need to show equalisation before 2021 to ensure equalisation is achieved in the planning period. Note that as a minimum, where CCGs have not achieved funding equalisation within PMS practices this will need to be achieved by 2016/17. CCG to give explanation of how they will seek to achieve equalisation within the prescribed timeframe. This should include a timescale for implementation, any risks and additional costs involved.
77