presentation final - children and family futures abuse specialists webinar... · ldk bt demonstrate...
TRANSCRIPT

8/29/2011
1
Welcome
Thank you for joining us today. The webinar will begin in a few moments.
• If you are experiencing technical problems with the
TEXT PAGE
• If you are experiencing technical problems with the GoToWebinar program, contact the GoToWebinar help desk:
1 (800) 263-6317Webinar ID: 839994497
How Do I Ask Questions?
Type and send your questions through the Question and Answer
TEXT PAGE
log located on the bottom half on your panel/dashboard.
A Program of theSubstance Abuse and Mental Health Services
AdministrationCenter for Substance Abuse Treatment
&the Administration on Children, Youth and Families
Children’s BureauOffice on Child Abuse and Neglect
NCSACW Mission:To develop knowledge and provide technical
assistance to Federal, State, local agencies and Tribes to improve outcomes for families with
substance use disorders in the child welfare and family court systems
The Role of Recovery Specialists in Substance Abuse Treatment, Child Welfare and Dependency Courts
August, 2011
Sandy RobinsonSandy RobinsonConsultantConsultant
Children and Family FuturesChildren and Family Futures
4 9 4 0 I r v i n e B l v d , S u i t e 2 0 2 , I r v i n e , C A 9 2 6 2 07 1 4 - 5 0 5 - 3 5 2 5 n c s a c w @ c f f u t u r e s . o r g
h t t p : / / w w w . n c s a c w . s a m h s a . g o v

8/29/2011
2
Agenda
• Purpose of using a substance abuse specialist model
• Roles and responsibilities• Training and supervision• Location and settings• Understanding values and agreements• Funding• Function in the system• Questions
Sometimes Child Welfare and Substance Abuse Treatment are Worlds Apart
Child W lf
Substance Abuse
6
Welfare Treatment
Summary
Substance use disorders are NOT just one more thing
• They are central, critical, and urgent• A thorough response requires strategic
thinking• It requires a strategic multi-year plan• It requires work at all ten bridges of linking
across systems• The best prevention for children remains
treatment for their parents
Purpose Of Utilizing Substance Abuse Recovery Specialists
Reduce costs of out‐of‐home placements and/or reduce time of children in foster care
Remove barriers and improve linkages between CWS and treatment to better serve clients
TEXT PAGE8
Improve the capacity of CWS to serve parents with substance use disorders
Increase collaboration between agencies
Ensure reasonable efforts
8/29/2011
3
Purpose Of Utilizing Substance Abuse Recovery Specialists
Decrease time to assess and enter treatment
Increase compliance with treatment
TEXT PAGE9
Increase 12 month permanent placements
Increase family reunification rates
Decrease time in foster care
Roles and Responsibilities
Case management
Screening, assessment, referral, and engagement into Treatment
Support to parents while in treatment
C d t h i it (CT DE IL S t )
TEXT PAGE
Conduct home visits (CT, DE, IL, Sacramento)
Urine testing (CT, DE, IL, Sacramento, San Diego)
Consultation and Information sharing with CW and/or courts
Training to CW and potentially the court
Develop and implement substance abuse capacity building plans for CW (MA)
10
Training and Supervision
Licensed/certified addiction counselor
Licensed clinical SW with addiction certification (CT)
Supervised by child welfare (CT, NH, WA)
Supervised by contracted service provider (IL, S t S Di )Sacramento, San Diego)
Dual supervision (DE, MA)
Regular meetings to maintain program purpose and/or foster collaborative relationships
Receives CW “New Worker Training” (DE, MA, NH)
Participates in cross training
11
Employed by state, county CW agency, community-based AOD treatment agency, contracted service provider or Self-employed and contracted by CW
Location and Settings
12
Area/regional/county/district CW offices (CT, DE, MA, NH, WA)Contracted service provider’s office, near to juvenile court (IL, Sacramento, San Diego)

8/29/2011
4
Underlying Values and Agreements
MOU or other agreement formally outlines joint values and principles for the program (Sacramento, WA)MOU or other agreement outlining joint valuesMOU or other agreement outlining joint values influences the implementation of program, but was not developed for the program, specifically (Sacramento, MA)
MOU or other agreement outlines systems’ and or other programs’ roles in program implementation (CT, DE, IL, San Diego)
13
State funds – CT, DE, MAFederal funds (i.e., Title IV-E, IV-B) – IL and NHM lti l (i ti l t t f di
Funding
14
Multiple sources (i.e., partial state funding, tobacco settlement, agency budget reallocation) – Sacramento, San Diego and Washington
Substance Abuse Specialists
TEXT PAGE
Substance Abuse Specialists
TEXT PAGE

8/29/2011
5
Substance Abuse Specialists
TEXT PAGE
Program Context
Sacramento County population: 1.5 millionBetween Oct 2006 and Sept 2007, there were 1862 child abuse/neglect referrals accepted for investigation gAn estimated 70 to 80% of child welfare cases involve families affected by substance use
Sacramento County Prior to STARS and Dependency Drug Court
Reunification rate about 20-25%Parents unable to access substance abuse treatmentSocial workers, attorneys, courts oftenSocial workers, attorneys, courts often uninformed on parent progressDrug testing not uniform and results often delayed
Sacramento County after STARS and Dependency Drug Court
Reunification rates at 40–45%With Recovery Specialist & Drug Court Graduation, Reunification rates at 75%Reunification is occurring fasterReunification is occurring fasterParents truly have “treatment on demand”All parties involved in the case are informed at every stage of treatmentAll parents receive random observed “instant” drug testing
8/29/2011
6
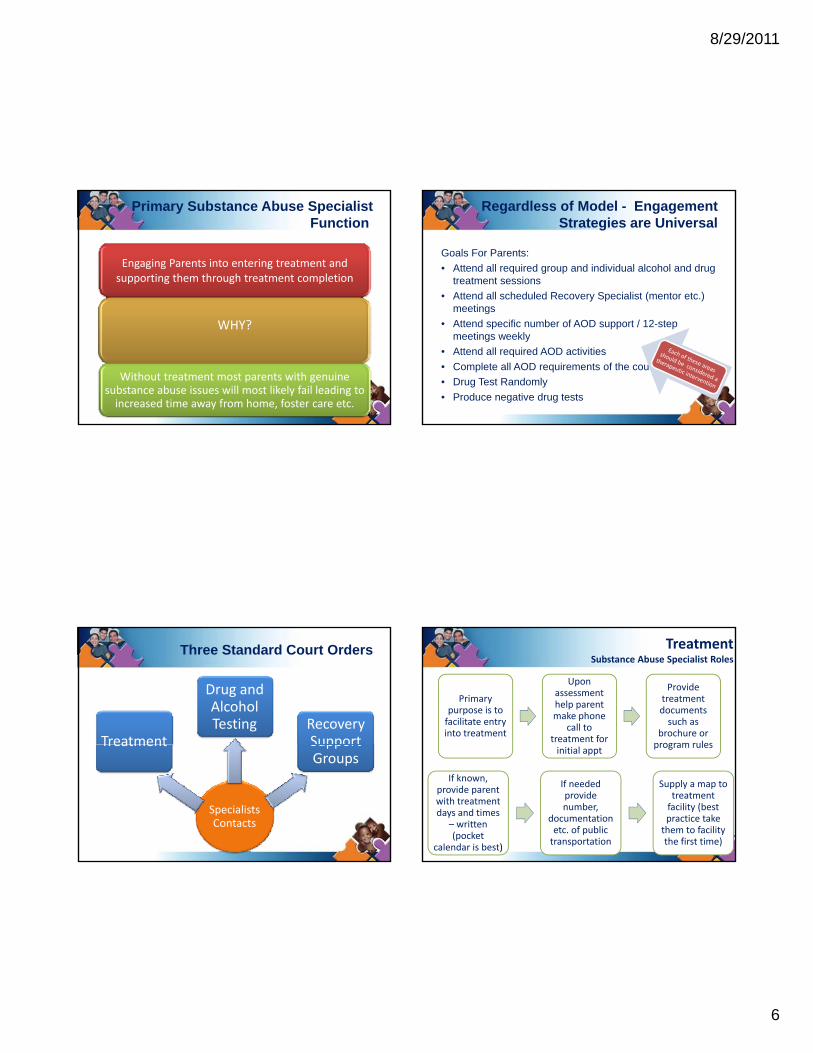
Primary Substance Abuse Specialist Function
Engaging Parents into entering treatment and supporting them through treatment completion
WHY?
Without treatment most parents with genuine substance abuse issues will most likely fail leading to increased time away from home, foster care etc.
21
Regardless of Model - Engagement Strategies are Universal
Goals For Parents:• Attend all required group and individual alcohol and drug
treatment sessions• Attend all scheduled Recovery Specialist (mentor etc.)
meetingsmeetings• Attend specific number of AOD support / 12-step
meetings weekly• Attend all required AOD activities • Complete all AOD requirements of the court• Drug Test Randomly• Produce negative drug tests
22
Three Standard Court Orders
Treatment
Drug and Alcohol Testing Recovery
Support
Specialists Contacts
Treatment Support Groups
23
Primary purpose is to facilitate entry into treatment
Upon assessment help parent make phone
call to treatment for
Provide treatment documents such as
brochure or program rules
TreatmentSubstance Abuse Specialist Roles
initial appt program rules
24
If known, provide parent with treatment days and times
– written (pocket
calendar is best)
If needed provide number,
documentation etc. of public transportation
Supply a map to treatment facility (best practice take them to facility the first time)
8/29/2011
7
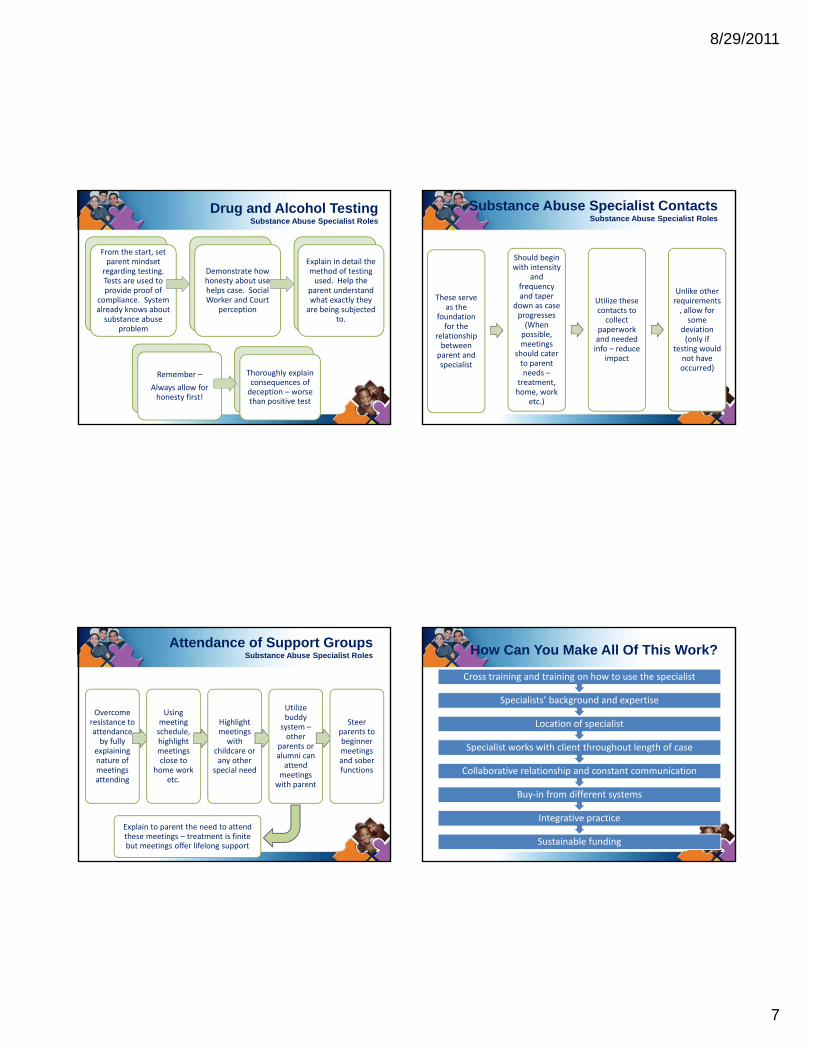
Drug and Alcohol TestingSubstance Abuse Specialist Roles
From the start, set parent mindset regarding testing. Tests are used to provide proof of
compliance. System l d k b t
Demonstrate how honesty about use helps case. Social Worker and Court
ti
Explain in detail the method of testing used. Help the
parent understand what exactly they
b i bj t dalready knows about substance abuse
problem
perception are being subjected to.
25
Remember –
Always allow for honesty first!
Thoroughly explain consequences of deception – worse than positive test
Substance Abuse Specialist ContactsSubstance Abuse Specialist Roles
These serve as the
Should begin with intensity
and frequency and taper
down as case Utilize these Unlike other requirements
ll fas the foundation for the
relationship between parent and specialist
down as case progresses (When possible, meetings
should cater to parent needs –
treatment, home, work
etc.)
contacts to collect
paperwork and needed info – reduce
impact
, allow for some
deviation (only if
testing would not have occurred)
26
Attendance of Support GroupsSubstance Abuse Specialist Roles
Overcome resistance to attendance by fully
Using meeting schedule, highlight
Highlight meetings with
Utilize buddy system –other
parents or
Steer parents to beginner y y
explaining nature of meetings attending
g gmeetings close to
home work etc.
childcare or any other
special need
parents or alumni can attend
meetings with parent
gmeetings and sober functions
27
Explain to parent the need to attend these meetings – treatment is finite but meetings offer lifelong support
How Can You Make All Of This Work?
S i li t k ith li t th h t l th f
Location of specialist
Specialists’ background and expertise
Cross training and training on how to use the specialist
Sustainable funding
Integrative practice
Buy‐in from different systems
Collaborative relationship and constant communication
Specialist works with client throughout length of case
28
8/29/2011
8
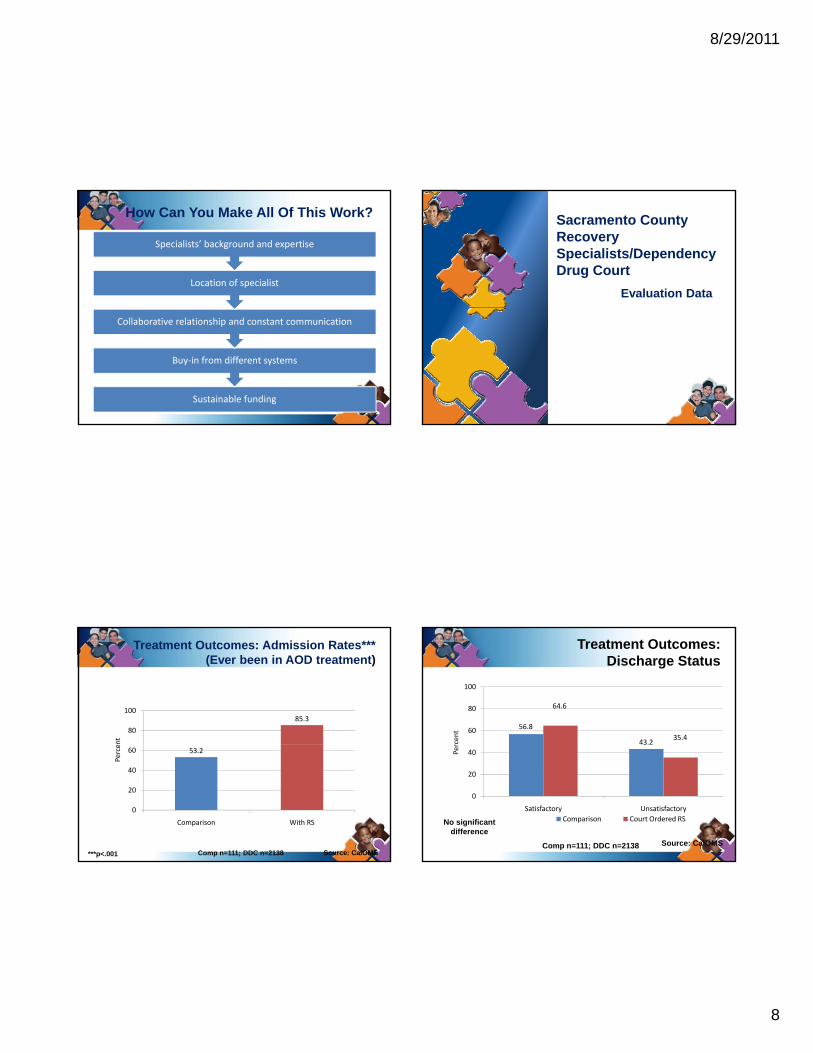
How Can You Make All Of This Work?
Location of specialist
Specialists’ background and expertise
Sustainable funding
Buy‐in from different systems
Collaborative relationship and constant communication
29
Sacramento County Recovery Specialists/Dependency Drug Court
Evaluation Data
85.3
80
100
ent
Treatment Outcomes: Admission Rates***(Ever been in AOD treatment)
53.2
0
20
40
60
Comparison With RS
Perce
***p<.001 Comp n=111; DDC n=2138 Source: CalOMS
Treatment Outcomes: Discharge Status
56.8
43.2
64.6
35.460
80
100
rcent
No significant difference
Source: CalOMSComp n=111; DDC n=2138
0
20
40
Satisfactory Unsatisfactory
Per
Comparison Court Ordered RS
8/29/2011
9
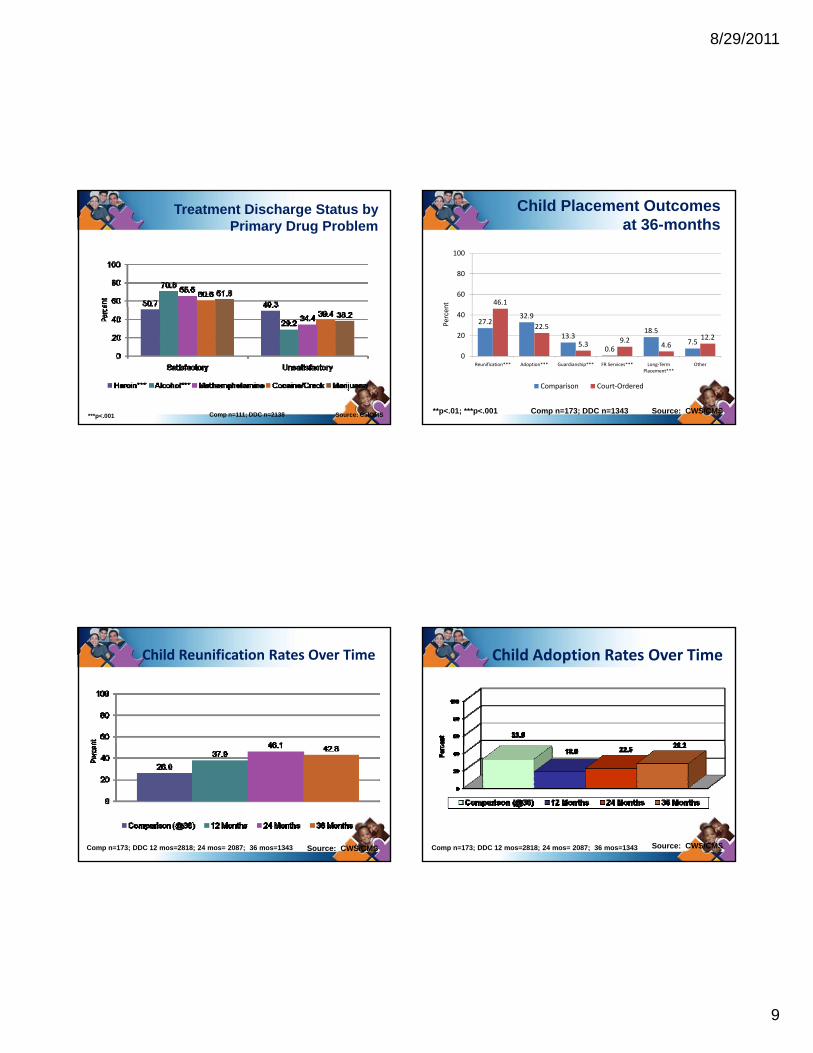
Treatment Discharge Status by Primary Drug Problem
***p<.001 Source: CalOMSComp n=111; DDC n=2138
Child Placement Outcomes at 36-months
46.160
80
100
nt
27.232.9
13.3
0.6
18.5
7.5
22.5
5.3 9.24.6
12.2
0
20
40
Reunification*** Adoption*** Guardianship*** FR Services*** Long‐Term Placement***
Other
Percen
Comparison Court‐Ordered
**p<.01; ***p<.001 Comp n=173; DDC n=1343 Source: CWS/CMS
Child Reunification Rates Over Time
Comp n=173; DDC 12 mos=2818; 24 mos= 2087; 36 mos=1343 Source: CWS/CMS
Child Adoption Rates Over Time
Comp n=173; DDC 12 mos=2818; 24 mos= 2087; 36 mos=1343 Source: CWS/CMS
8/29/2011
10
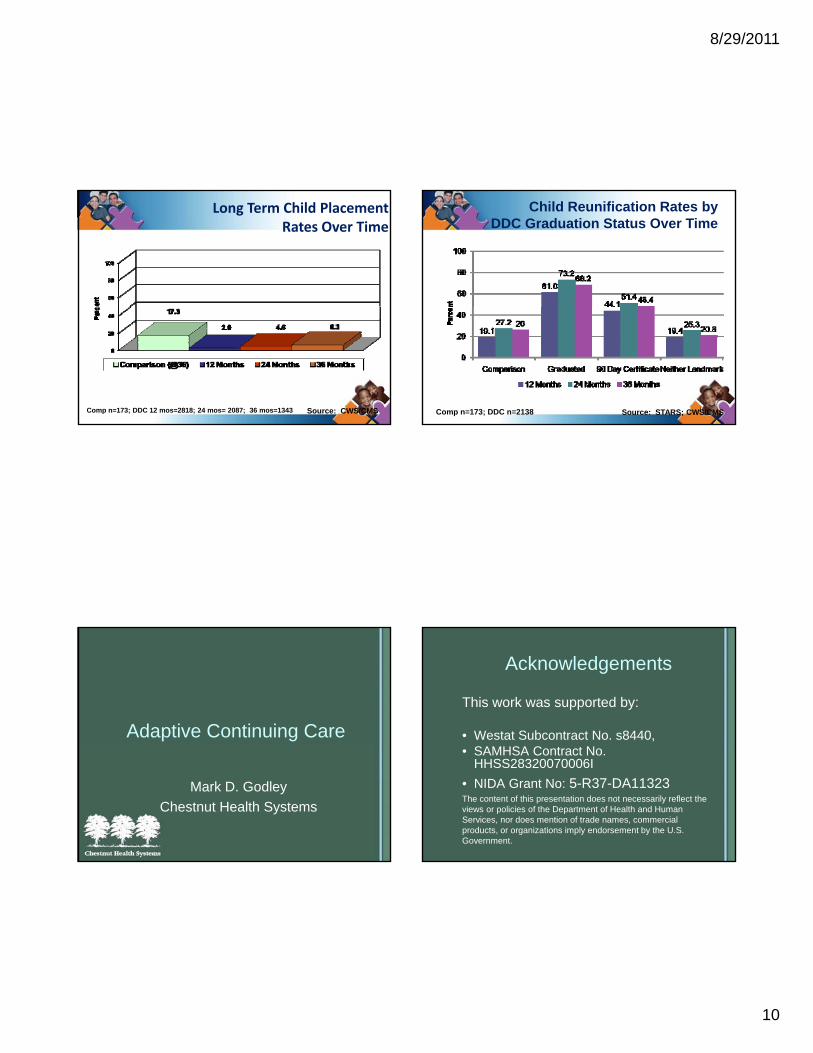
Long Term Child Placement Rates Over Time
Comp n=173; DDC 12 mos=2818; 24 mos= 2087; 36 mos=1343 Source: CWS/CMS
Child Reunification Rates by DDC Graduation Status Over Time
Comp n=173; DDC n=2138 Source: STARS; CWS/CMS
Adaptive Continuing Care
Mark D. GodleyChestnut Health Systems
Acknowledgements
This work was supported by:
• Westat Subcontract No. s8440,• SAMHSA Contract No.
HHSS28320070006I• NIDA Grant No: 5-R37-DA11323The content of this presentation does not necessarily reflect the views or policies of the Department of Health and Human Services, nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S.Government.
8/29/2011
11
Presentation Aims
• What is adaptive continuing care• Key elements of adaptive continuing care• Describe two approaches to adaptive
continuing care• Results
Adaptive continuing care is treatment that is tailored and or modified based on a client’s symptoms, status, and level of functioning.
Adaptive Continuing Care
Adaptive Continuing Care: Key Elements
• Monitor clients discharged from treatment for substance use disorders at planned intervalsintervals
• Use standardized instrument and approach to client monitoring
• Decrease or increase contact frequency depending on client functioning
• Provide support or stepped up care depending on client functioning
Telephone-based Adaptive Continuing Care for Adolescents
Seattle, WA
Tucson, AZ
Bloomington, IL
Fitchburg, MA

8/29/2011
12
Adaptive Call Structure
• Weekly calls during the first 90 days after discharge from treatment, then monthlyy
• Call frequency increases or decreases depending on how adolescent is doing
• Texting sessions are an option• If adolescent cannot be contacted after
90 days of attempts, the case is closed
Telephone Protocol• Greeting and general conversation• Ask about whether they experienced any “triggers
to use since last call”• If no use but triggers discuss how they overcame,
praise, and ask them how they can generalize p y g• Discuss and agree to recovery goals for the next
period between calls• If use, ask if they are still using and make referral
back to a counselor• Provide assistance with referral (call, arrange
transportation, etc)
Average Length of call by Week in Minutes: Seconds
14:24
16:48
19:12
0:00
2:24
4:48
7:12
9:36
12:00
4/17
/201
0
5/1/
2010
5/15
/201
0
5/29
/201
0
6/12
/201
0
6/26
/201
0
7/10
/201
0
7/24
/201
0
8/7/
2010
8/21
/201
0
9/4/
2010
9/18
/201
0
10/2
/201
0
10/1
6/20
10
Percent of Adolescents Completing Planned Telephone Support Sessions
500
600
700
0
100
200
300
400
500
Bloomington Fitchburg Seattle Tucson
AttemptedCompleted
56%
67%
65% 57%
8/29/2011
13
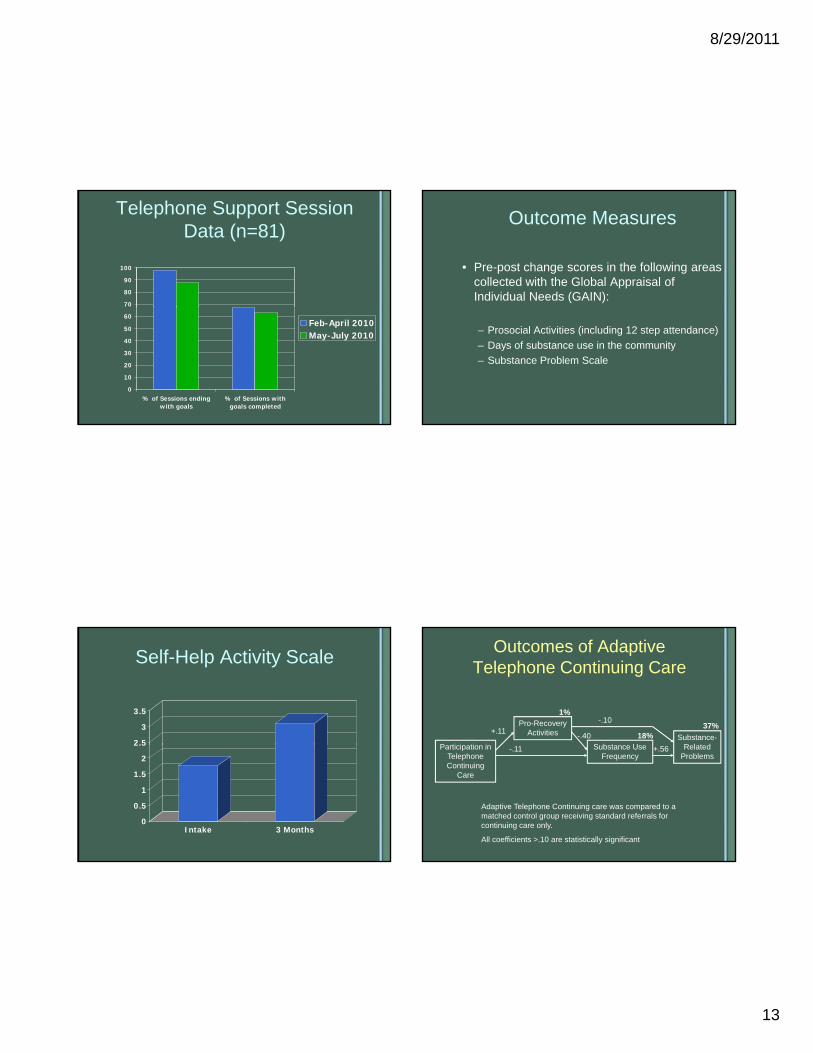
Telephone Support Session Data (n=81)
70
80
90
100
0
10
20
30
40
50
60
% of Sessions endingwith goals
% of Sessions withgoals completed
Feb-April 2010May-July 2010
Outcome Measures
• Pre-post change scores in the following areas collected with the Global Appraisal of Individual Needs (GAIN):
– Prosocial Activities (including 12 step attendance)– Days of substance use in the community– Substance Problem Scale
Self-Help Activity Scale
2.5
3
3.5
0
0.5
1
1.5
2
2.5
Intake 3 Months
Outcomes of Adaptive Telephone Continuing Care
P ti i ti i
Pro-Recovery Activities
S b t USubstance-
R l t d
+.11
1%-.10
-.40 18%37%
Participation in Telephone Continuing
Care
Substance Use Frequency
Related Problems
-.11 +.56
Adaptive Telephone Continuing care was compared to a matched control group receiving standard referrals for continuing care only.
All coefficients >.10 are statistically significant
8/29/2011
14
Satisfaction with Telephone Support (n=25)
70%
80%
90%
100%
0%
10%
20%
30%
40%
50%
60%
sometimes-almostalways liked
receiving calls
always/almostalways thought
telephone supportworker was kindand encouraging
never/almost neverthought telephone
support worker wastoo demanding
thought calls werethe right amount of
frequency
thought telephonecalls were the right
length of time
would recommendcalls longer than thefirst 3 months post-
discharge
Early Re-Intervention (ERI) Experiment and Hypotheses
Monitoring and
Early Re-Intervention
Reduce Time to Re-admission
Less Successive Quarters
Using
Less Risk Behaviors, MH and Crime
Source: Dennis et al 2003, 2007; Scott et al 2005, in press
Relative to Control, RMC will reduce the time from relapse to readmission
The quicker the return to treatment, the less successive quarters using in the community
The less quarters using in the community, the less HIV Risk Behaviors, Mental Health and Crime Problems
Recovery Management Checkups (RMC)
• Quarterly monitoring after treatment• Linkage meeting/motivational interviewing to:
– provide personalized feedback to participants about their substance use and related problems,
– help the participant recognize the problem and consider ret rning to treatmentconsider returning to treatment,
– address existing barriers to treatment, and – schedule an assessment.
• Linkage assistance– reminder calls and rescheduling– Transportation and being escorted as needed
• Treatment Engagement Specialist
ERI-2 Time to Treatment Re-Entry at Year 4
mitt
ed 1
+ Ti
mes
50%
60%
70%
80%
90%
100%Time from relapse to
readmission reduce by 78% (45-13 = -32 months; d=-.41) 74% ERI-2 RMC*
(n=198)
48% ERI-2 OM( 195)
RMC increases the odds of re-entering treatment over 4 years by 3.1
Perc
ent R
eadm
Wilcoxon-Gehen statistic (df=1) = 28.60, p<.001
OR=3.1, p<.05
0%
10%
20%
30%
40%
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 45
Months from 1st Follow-up In Need for Treatment,
(n=195)
Source: Scott & Dennis (2009); Dennis & Scott (in press)
The size of the effect grew every quarter
8/29/2011
15
Positive Consequences of Early Readmission
• Checkups and Early Readmission to Treatment were associated with: – Less substance use and problems– Longer periods of abstinence– More attendance and engagement in self
help activitieshelp activities• Above were associated with:
– Fewer HIV risk behaviours– Less illegal activity, arrests, and time
incarcerated– Fewer mental health problems– Less utilization and costs to society
Source: Scott & Dennis (2009); Dennis & Scott (in press)
Practice Implications• Adaptive Continuing Care is “state-of-the-art”
and improves outcomes but must consider:
– What will the frequency of client contact be?– How will regular client contact be maintained?g– Need to have client information system to track and
manage contacts with clients– The longer you plan to retain clients in continuing
care the greater the cost– Costs can be decreased by using trained, well-
supervised volunteers
Questions and DiscussionQuestions and Discussion
Register Now
http://www.cffutures.org/conference2011Gaylord National Resort and Convention Center on the Potomac—National Harbor, MD

8/29/2011
16
Contact Information
Mark D. Godley, Ph.D.Chestnut Health Systems
448 Wylie Dr.
Sandy RobinsonChildren and Family Futures4940 Irvine Blvd, Suite 202
Normal, IL 61761
Email: [email protected]
Irvine, CA 92620
Email: [email protected]