pre/post dapt in nstemi evidence beyond any dubius · 2016-06-21 · ua/nstemi
TRANSCRIPT
PRE/POST DAPT in NSTEMI evidence beyond
any DUBIUS
Giuseppe Tarantini
University of Padua

Clinical History
Male 71 years old
Risk factors:
Hypertension
Carotid Vasculophaty
COPD
Diabetic (IR)
Admitted because of NSTE ACS in our Hospital

EKG
2D-ECHO: EDV 70 ml/m2, EF 57%, anterior hypokinesia

TIMI Risk Score = 5
Death, MI or uTVR: 26% @ 14 days
Grace Risk Score = 134
In-Hospital Death: 4.6 ---- 6-Months Death 12%
Crusade bleeding Score = 40
In-hospital Major Bleeding: 9.2%
Expected cath 12-24 hrs

Up vs Downstream
DAPT?

Risk-based
approach
Trial-based
approach
Risk-based
approach
1.ACS Trial’s MACE rate has fallen over the past 10 years
2.Risk calculator of old data/old drugs may
Overestimate the contemporary ischemic risk
Underestimate the contemporary bleeding risk
3.Risk score is rarely used in trials as enrollment criteria
4.Highest absolute risk do not always predicts greatest
efficacy
5.NACE risk score are absent
6.RC applied to general population pts not enrolled in
trials, do not ensure that pts selected for Tx are those
who benefit
Risk-based
approach
Trial-based
approach

Evidence (NSTEMI) upstream vs
downstream?
Clopigogrel: Upstream flawed superiority UP vs DOWN
Prasugrel: Downstream > Upstream
Ticagrelor: Downstream > Upstream unsettled
“STEMI no overall advantage”
GPI:
I IIa IIb III
A When coronary anatomy is
not known.
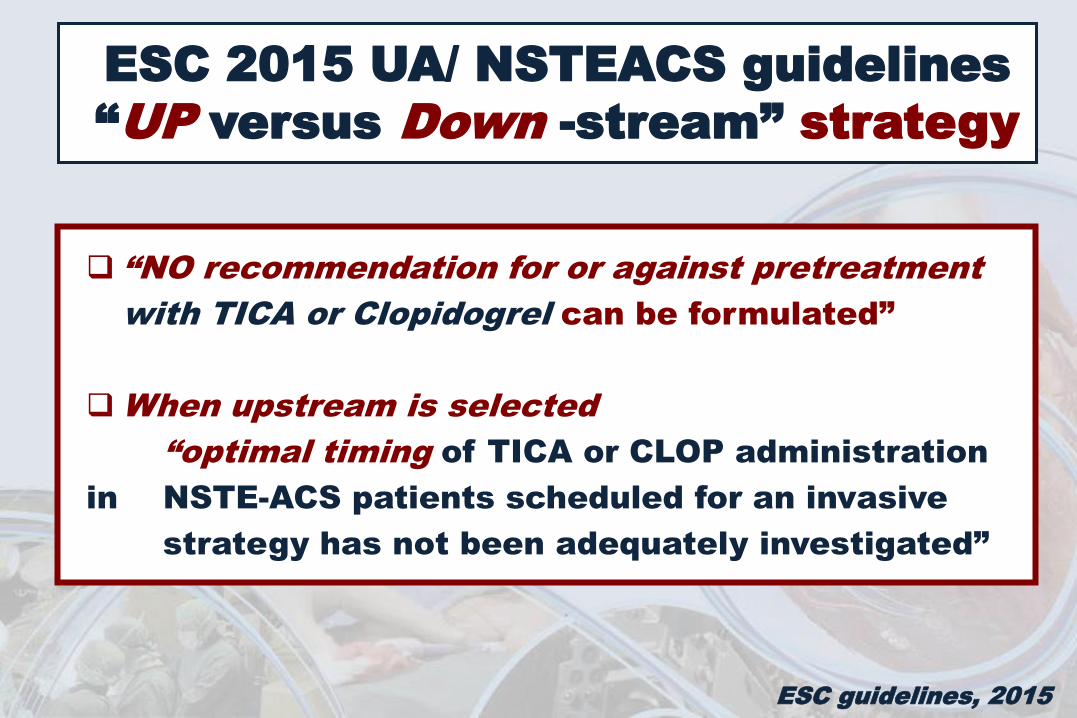
ESC 2015 UA/ NSTEACS guidelines
“UP versus Down -stream” strategy
ESC guidelines, 2015
“NO recommendation for or against pretreatment
with TICA or Clopidogrel can be formulated”
When upstream is selected
“optimal timing of TICA or CLOP administration
in NSTE-ACS patients scheduled for an invasive
strategy has not been adequately investigated”
Up vs Downstream
DAPT?
RANDOMIZE !

RANDOMIZED CONTROLLED TRIAL
Downstream versus Upstream strategy for the
administration of P2Y12 receptor Blockers In
non ST elevated acUte coronary Syndromes
with initial invasive indication.
PI G. Tarantini
Co-PI G. Musumeci

Downstream strategy Upstream strategy:
Ticagrelor
if PCI
UA/NSTEMI <72 hours - initial invasive indication
ASA + open label anticoagulants
Randomization
Prasugrel* Ticagrelor
I EP powered for
superiority
II EP powered for
non inferiority
DUBIUS trial n≈ 2528
1st
Primary EP: 30-d NACE (CV death, MI, stroke, BARC 3, 4, 5)
*60 mg oral bolus then 5 mg/die if >75 yrs or < 60 kg
Randomization 2nd II EP powered for
EQUIVALENCE

EQUIVALENCE CALCULATIONS
ASSUMPTIONS: Two-sided equivalence test for rejecting the hypothesis H0: |π2 - π1 |≤ 0.04 (i.e.:
Plasugrel and Ticagrerol will not differ for more than 4% in terms of NACE)
α = 0.05, confidence bounds 0.95
Overall sample size of 1100 patients (550 Prasugrel + 550 Ticagrerol) An incidence rate of rates π1 = 0.05 in Ticagrerol and π2 = 0.085 in Prasugrel (odds ratio
of 1.765) and a true difference in incidence rates of 0.01 between treatment groups
An allocation rate of 1:1
Based on the above assumptions, the power (1 - β) is 0.805.
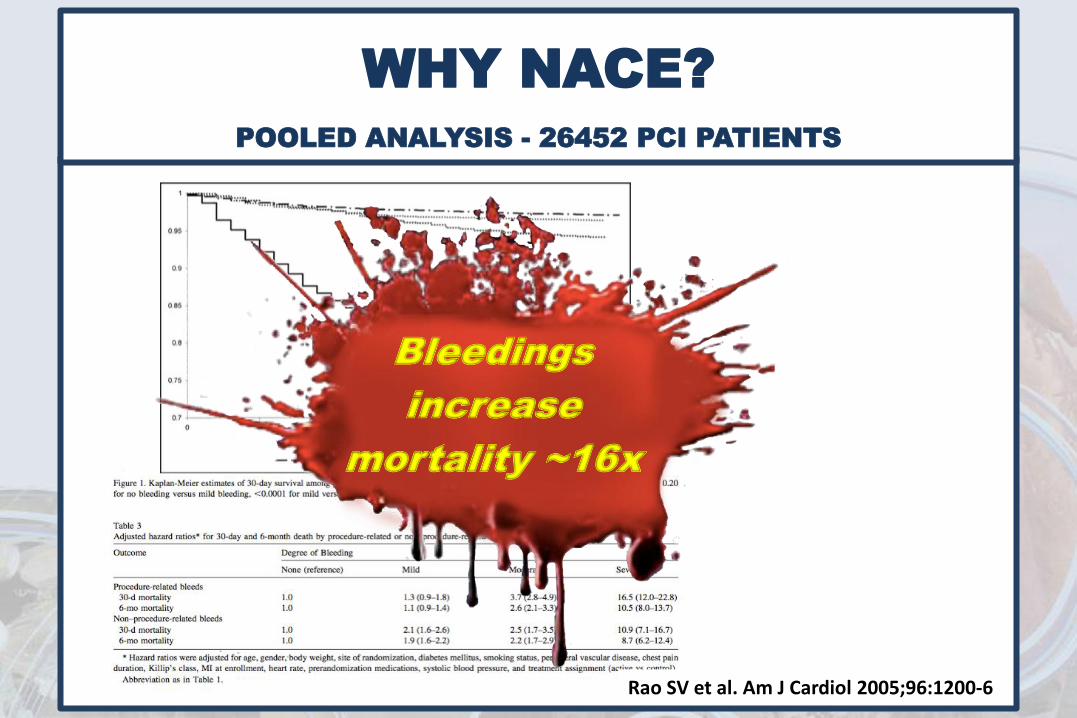
WHY NACE?
POOLED ANALYSIS - 26452 PCI PATIENTS
Rao SV et al. Am J Cardiol 2005;96:1200-6
Bleedings
increase
mortality ~16x

NACE Rationale in DUBIUS TRIAL:
Bleeding increases directly and indirectly mortality
FDA RECOMMENDATION
Ischemic (efficacy) and Bleeding (safety) endpoints should be
comparable (hard vs hard)
NACE rate should not derived post-hoc (e.g. TRITON
TIMI 38 and PLATO) but prespecified and powered
19
TIMI
GUSTO
CURE
GRACE
STEEPLE
PLATO
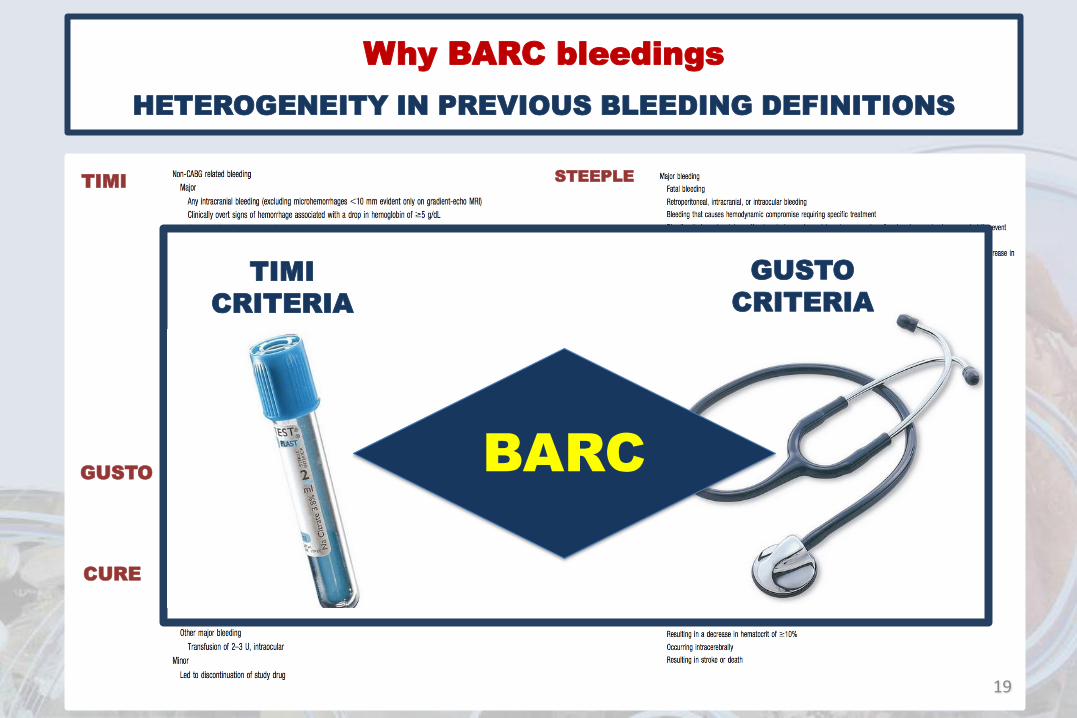
Why BARC bleedings
HETEROGENEITY IN PREVIOUS BLEEDING DEFINITIONS
TIMI
CRITERIA
GUSTO
CRITERIA
BARC

LOMBARDIA - A.O Desio
- AO Vimercate
- A.O. Papa Giovanni XXIII
- A.O. Treviglio
- Centro Cardiologico Monzino
- A.O. Fatebenefratelli
- Policlinico San Matteo
- Ospedale Bassini
- Ospedale Niguarda
- Policlinico San Marco
- A.O.S. Antonio Abate
- San Luca – Milano
- Humanitas
- San Gerardo
- San Donato
- Osp Maggiore
PIEMONTE - Ospedale degli Infermi
- Ospedale Maria Vittoria
- Ospedale San Giovanni Bosco
LIGURIA - Ospedale Galliera
EMILIA ROMAGNA - Ospedale degli Infermi
- Ospedale Maria Vittoria
- Ospedale San Giovanni Bosco
CAMPANIA - A.O.S.G.Moscati
- A.O. Monaldi
- Azienda Ospedaliera
Universitaria Federico II
TOSCANA - A.O. Senese
- Azienda USL 9
- Azienda USL 4
- Ospedale del Cuore
- Azienda USL 6
- Azienda Ospedaliero-
Universitaria Pisana
ABRUZZO - Ospedale Spirito Santo di
Pescara
CALABRIA - A.O. di Cosenza
PUGLIA - Anthea Hospital
- Ospedale Civile Lorenzo
Bonomo
- Ospedale Casa Sollievo Della
Sofferenza
LAZIO - Ospedale Sandro Pertini
- Policlinico Casilino
VENETO - Azienda ULSS 9 Treviso
- Azienda ULSS 13 Mirano
- Ospedale San Giacomo
- Ospedale Civile Santa Maria
della Misericordia
- Azienda ULSS 17 Schiavonia
- Casa di Cura Privata Dott.
Pederzoli
SICILIA - A.O. Universitaria Gaetano
Martino
- Ospedale 'Civile Maria Paternò
Arezzo
- P.S. S.Elia
SARDEGNA - Ospedale San Francesco
- Ospedale Sirai
Coordinating Center: PADOVA
47 centri aderenti

Downstream strategy
DUBIUS trial
CURRENT CASE #1
*60 mg oral bolus then 5 mg/die if >75 yrs or < 60 kg
Randomization 1st



PCI
Downstream strategy
Prasugrel*
DUBIUS trial
CURRENT CASE #1
*60 mg oral bolus then 5 mg/die if >75 yrs or < 60 kg
Randomization 1st
Randomization 2nd

After PCI

DISCHARGE DAY 4
TnI peak 0.261 ug/l
2D-ECHO: EDV 72 ml/m2, EF 54%
ASA 100 mg
Prasugrel (10 mg daily)
Norvasc 10 mg, Triatec 5 mg, Torvast 80 mg, Lansoprazolo 30 mg
F-up 4 month – no Events, still on
Prasugrel
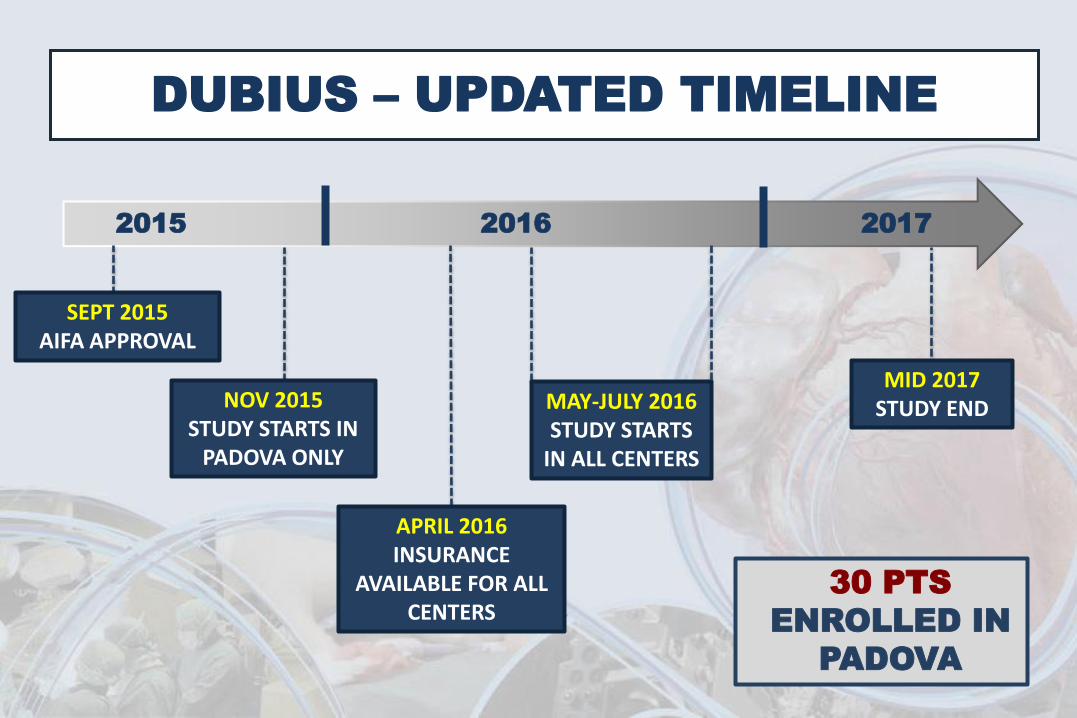
2015 2016
DUBIUS – UPDATED TIMELINE
SEPT 2015 AIFA APPROVAL
APRIL 2016 INSURANCE
AVAILABLE FOR ALL CENTERS
MID 2017 STUDY END
30 PTS
ENROLLED IN
PADOVA
NOV 2015 STUDY STARTS IN
PADOVA ONLY
MAY-JULY 2016 STUDY STARTS
IN ALL CENTERS
2017