preferences for an end of life 'premium‘: an examination of framing effects and study design...
TRANSCRIPT

Koonal Shah, Office of Health Economics
International Academy of Health Preference ResearchGlasgow 4 November 2017
Preferences for an end of life 'premium‘:An examination of framing effects and study design considerations

IAPHR Meeting, Glasgow4 Nov 2017, 2
Acknowledgements
• Co-authored by my PhD supervisors, Aki Tsuchiya and Allan Wailoo (both University of Sheffield)
• Study was funded by the National Institute for Health and Care Excellence via its Decision Support Unit
• The views expressed (and any errors or omissions) are of the authors only

IAPHR Meeting, Glasgow4 Nov 2017, 3
• Criteria that need to be satisfied for NICE’s supplementary end of life policy to apply:
NICE end of life policy
C2
The treatment is indicated for patients with a short life expectancy, normally less than 24 months
There is sufficient evidence to indicate that the treatment offers an extension to life, normally of at least an additional three months, compared to current NHS treatment
The treatment is licensed or otherwise indicated, for small patient populations
C3
C1

IAPHR Meeting, Glasgow4 Nov 2017, 4
Findings from literature review
IAPHR Meeting, Glasgow4 Nov 2017, 5
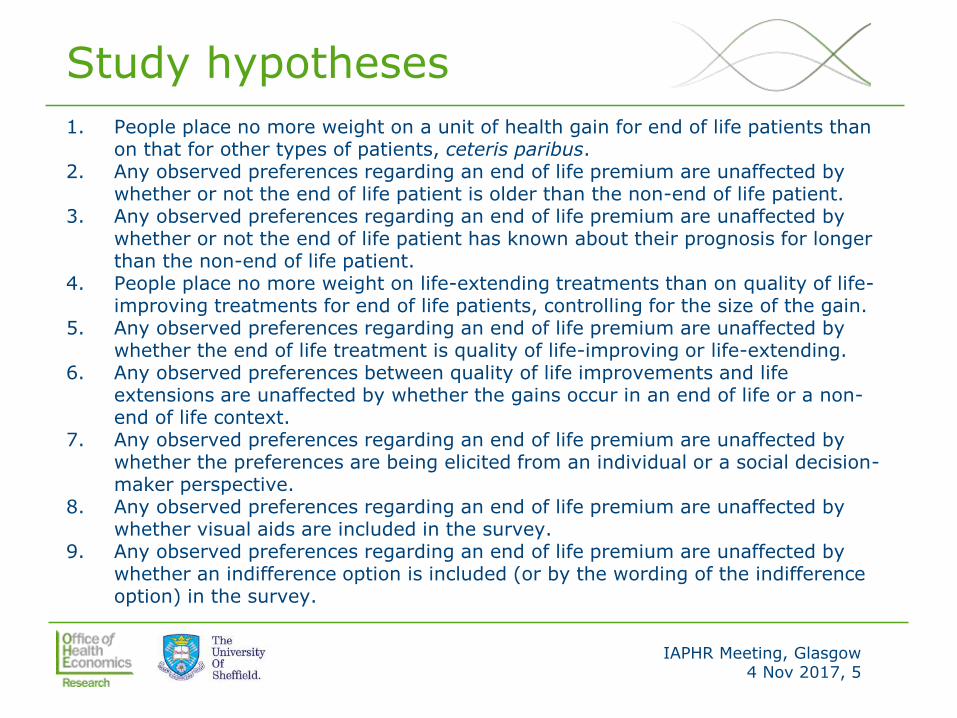
Study hypotheses
1. People place no more weight on a unit of health gain for end of life patients than on that for other types of patients, ceteris paribus.
2. Any observed preferences regarding an end of life premium are unaffected by whether or not the end of life patient is older than the non-end of life patient.
3. Any observed preferences regarding an end of life premium are unaffected by whether or not the end of life patient has known about their prognosis for longer than the non-end of life patient.
4. People place no more weight on life-extending treatments than on quality of life-improving treatments for end of life patients, controlling for the size of the gain.
5. Any observed preferences regarding an end of life premium are unaffected by whether the end of life treatment is quality of life-improving or life-extending.
6. Any observed preferences between quality of life improvements and life extensions are unaffected by whether the gains occur in an end of life or a non-end of life context.
7. Any observed preferences regarding an end of life premium are unaffected by whether the preferences are being elicited from an individual or a social decision-maker perspective.
8. Any observed preferences regarding an end of life premium are unaffected by whether visual aids are included in the survey.
9. Any observed preferences regarding an end of life premium are unaffected by whether an indifference option is included (or by the wording of the indifference option) in the survey.
IAPHR Meeting, Glasgow4 Nov 2017, 6
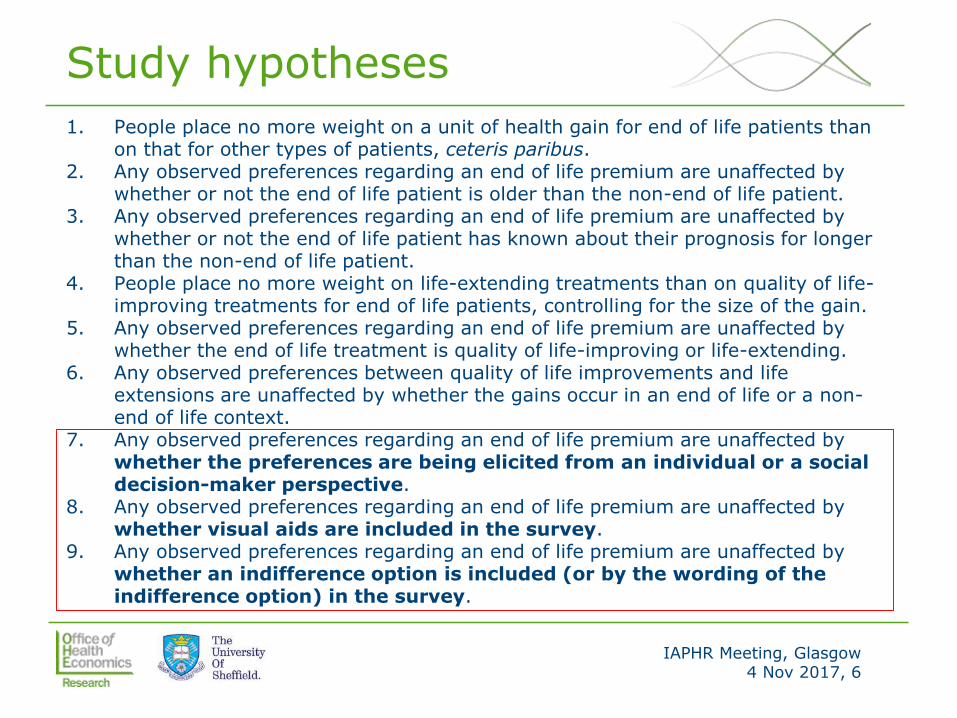
Study hypotheses
1. People place no more weight on a unit of health gain for end of life patients than on that for other types of patients, ceteris paribus.
2. Any observed preferences regarding an end of life premium are unaffected by whether or not the end of life patient is older than the non-end of life patient.
3. Any observed preferences regarding an end of life premium are unaffected by whether or not the end of life patient has known about their prognosis for longer than the non-end of life patient.
4. People place no more weight on life-extending treatments than on quality of life-improving treatments for end of life patients, controlling for the size of the gain.
5. Any observed preferences regarding an end of life premium are unaffected by whether the end of life treatment is quality of life-improving or life-extending.
6. Any observed preferences between quality of life improvements and life extensions are unaffected by whether the gains occur in an end of life or a non-end of life context.
7. Any observed preferences regarding an end of life premium are unaffected by whether the preferences are being elicited from an individual or a social decision-maker perspective.
8. Any observed preferences regarding an end of life premium are unaffected by whether visual aids are included in the survey.
9. Any observed preferences regarding an end of life premium are unaffected by whether an indifference option is included (or by the wording of the indifference option) in the survey.
IAPHR Meeting, Glasgow4 Nov 2017, 7
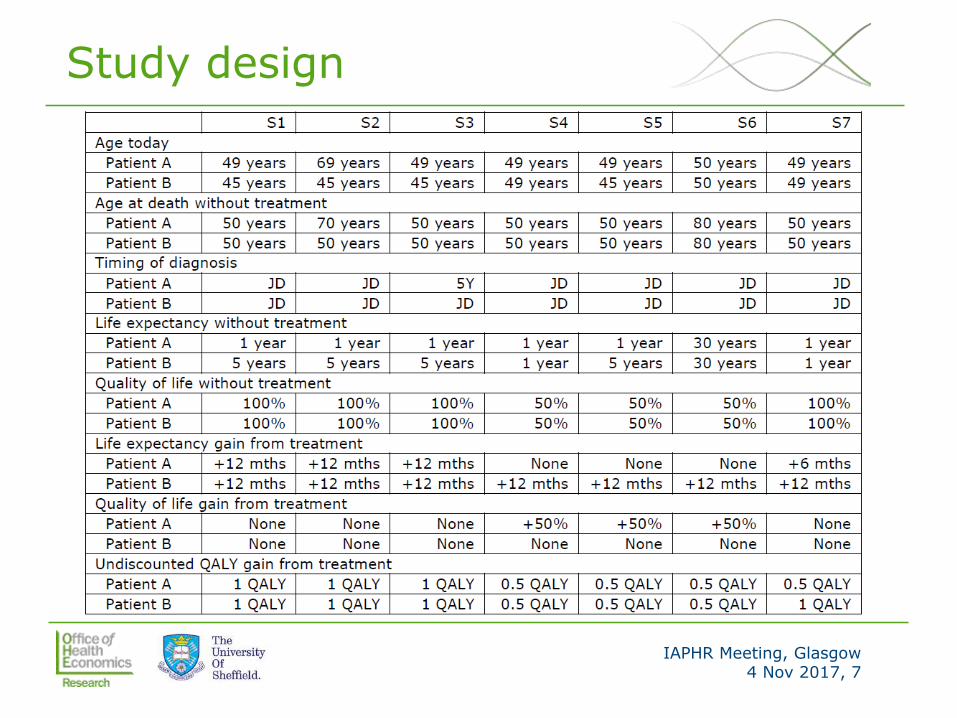
Study design

IAPHR Meeting, Glasgow4 Nov 2017, 8
Study design
Visual aid arm No visual aid arm
Forced choice arm Version 1 Version 4
Indifference arm Indifference option 1 arm Version 2 Version 5
Indifference option 2 arm Version 3 Version 6

IAPHR Meeting, Glasgow4 Nov 2017, 9
No visual aid vs. visual aid

IAPHR Meeting, Glasgow4 Nov 2017, 10
No visual aid vs. visual aid

IAPHR Meeting, Glasgow4 Nov 2017, 11
Forced choice vs. indifference options
If the health service has only enough funds to treat one of the two patients, which of the following describes your view?
o I would prefer the health service to treat patient A
o I would prefer the health service to treat patient B
o I would prefer the health service to treat patient A
o I have no preference (I do not mind which patient is treated)
o I would prefer the health service to treat patient B
o I would prefer the health service to treat patient A
o Both patients should have an equal chance of being treated (tossing a coin would be a fair way to make the choice)
o I would prefer the health service to treat patient B
Forced choice
Indiff. option 1
Indiff. option 2

IAPHR Meeting, Glasgow4 Nov 2017, 12
Follow-up question to identify point of indifference

IAPHR Meeting, Glasgow4 Nov 2017, 13
Examination of perspective
• Scenario S8 included as an individual perspective operationalisation of S1
• Respondents asked to imagine that they could be one of the patients in need of treatment
• Question posed:
• Suppose the health service has enough funds to make either treatment A or treatment B available, but not both. Without knowing which scenario will occur (but knowing that both have an equal chance of occurring), what would you prefer?
• No visual aids; indifference option 2 (for all respondents)
• Preamble for S8 used elements of ‘cheap talk’
IAPHR Meeting, Glasgow4 Nov 2017, 14
Data collection and methods of analysis
• Sample: adult members of UK general public (online panel members); age, gender and social grade quotas – n=2,401
• Draft survey piloted using CAPIs (conducted by author) with convenience sample of non-academic university staff
• Comparisons between arms and between scenarios assessed using Pearson’s chi-squared test
• Support for (life-extending) end of life premium assessed using binomial test
• Multiple logistic regression used to assess impact of respondent background characteristics on likelihood of choosing to treat end of life patient
• Sensitivity analysis: assessed impact of excluding respondents meeting one of two poor quality/engagement indicators

IAPHR Meeting, Glasgow4 Nov 2017, 15
Results – modal choice in each arm
Scenario Forced choice
Indiff. 1 Indiff. 2No visual
aidVisual Aid
S1EOL patient (A) vs. non-EOL patient (B)
A I I I B
S2Older EOL patient (A) vs. younger non-EOL patient (B)
B B B B B
S3
EOL patient with more time with knowledge (A) vs. non-EOL patient with less time with knowledge (B)
B I I B I
S4
QOL gain for EOL patient (A) vs. life extension for EOL patient (B)
A A I A A
S5
QOL gain for EOL patient (A) vs. life extension for non-EOL patient (B)
A A A A A
S6
QOL gain at end of normal LE (A) vs. life extension at end of normal LE (B)
A I I A A

IAPHR Meeting, Glasgow4 Nov 2017, 16
Impact of indifference option
• In S1, modal choice in forced choice arm was to treat the end of life patient, whereas for respondents in the indifference arm this was the least common choice
• Significant association between availability of an indifference option and propensity to choose to treat the end of life patient (p<0.01)
• Across all scenarios, indifference was expressed more frequently by respondents in indifference option 2 arm (p<0.01)
• Examination of ordering effects shows that respondents in the indifference arms were increasingly likely to choose the indifference option as they proceeded through the survey

IAPHR Meeting, Glasgow4 Nov 2017, 17
Impact of visual aid
• In S4, S5 and S6, respondents in visual aid arm were more likely than those in the no visual aid arm to choose the life-extending treatment over the quality of life-improving treatment (p<0.01 in S4 and S6; p<0.1 in S5)
• In other scenarios, pattern of responses did not differ greatly between arms (p>0.05)

IAPHR Meeting, Glasgow4 Nov 2017, 18
Impact of perspective
• Significant association between study perspective and propensity to prioritise provision of end of life treatment (p<0.01)
S1 vs. S8
(version 5 only)
S8
A I B Total
S1 A 42 (10.6%) 40 (10.1%) 47 (11.8%) 129 (32.5%)
I 16 (4.0%) 101 (25.4%) 41 (10.3%) 158 (39.8%)
B 9 (2.3%) 24 (6.0%) 77 (19.4%) 110 (27.7%)
Total 67 (16.9%) 165 (41.6%) 165 (41.6%) 397 (100.0%)

IAPHR Meeting, Glasgow4 Nov 2017, 19
Other results of note
• Excluding respondents who met data quality flags strengthensthe finding of lack of support for an end of life premium
• High levels of internal incoherence observed – respondents’ choice task responses were often at odds with their responses to subsequent attitudinal questions
• Respondents who are younger, have children, or have experience of terminal illness in friends/family were more likely than average to choose to treat the end of life patient

IAPHR Meeting, Glasgow4 Nov 2017, 20
Selected discussion points
• Framing effects and study design considerations were found to affect choices, though in no arm were results consistent with an end of life premium
• Very few respondents’ choices were consistent with NICE’s policy (though even fewer were consistent with QALY-max)
• Some findings contrast those of the literature review
• Likelihood of choosing the end of life option lower under the individual perspective
• Likelihood of choosing the end of life option similar in the visual aid and no visual aid arms
• Some evidence that it is not only whether an indifference option is available that matters, but also how exactly that indifference option is framed and mechanised

IAPHR Meeting, Glasgow4 Nov 2017, 21
To enquire about additional information and analyses, please contact Koonal Shah at [email protected]
To keep up with the latest news and research, subscribe to our blog, OHE News
Follow us on Twitter @OHENews, LinkedIn and SlideShare
Office of Health Economics (OHE)
Southside, 7th Floor105 Victoria StreetLondon SW1E 6QT United Kingdom
+44 20 7747 8850 www.ohe.org
OHE’s publications may be downloaded free of charge from our website.
Thank you for listening